Back to Journals » Clinical Interventions in Aging » Volume 14
Randomised Controlled Trial Of The Effect Of Tai Chi On Postural Balance Of People With Dementia
Authors Nyman SR ![]() , Ingram W
, Ingram W ![]() , Sanders J
, Sanders J ![]() , Thomas PW
, Thomas PW ![]() , Thomas S
, Thomas S ![]() , Vassallo M
, Vassallo M ![]() , Raftery J, Bibi I
, Raftery J, Bibi I ![]() , Barrado-Martín Y
, Barrado-Martín Y ![]()
Received 28 August 2019
Accepted for publication 26 September 2019
Published 19 November 2019 Volume 2019:14 Pages 2017—2029
DOI https://doi.org/10.2147/CIA.S228931
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Walker
Video abstract presented by Samuel R Nyman.
Views: 446
Samuel R Nyman,1 Wendy Ingram,2 Jeanette Sanders,2 Peter W Thomas,3 Sarah Thomas,3 Michael Vassallo,4 James Raftery,5 Iram Bibi,1 Yolanda Barrado-Martín1
1Department of Psychology and Ageing & Dementia Research Centre, Faculty of Science and Technology, Bournemouth University, Poole House, Talbot Campus, Poole, Dorset BH12 5BB, UK; 2Peninsula Clinical Trials Unit, Peninsula Medical School, University of Plymouth, Plymouth, Devon PL4 8AA, UK; 3Bournemouth University Clinical Research Unit, Faculty of Health and Social Sciences, Bournemouth University, Royal London House, Lansdowne Campus, Bournemouth, Dorset BH1 3LT, UK; 4Centre of Postgraduate Medical Research and Education, Faculty of Health and Social Sciences, Bournemouth University, Royal London House, Lansdowne Campus, Bournemouth, Dorset BH1 3LT, UK; 5Faculty of Medicine, University of Southampton, Highfield Campus, Southampton, SO17 1BJ, UK
Correspondence: Samuel R Nyman
Department of Medical Science and Public Health, Faculty of Health and Social Sciences, Bournemouth University, Poole House, Talbot Campus, Poole, Dorset BH12 5BB, UK
Tel +44 1202 968179
Email [email protected]
Purpose: To investigate the effect of Tai Chi exercise on postural balance among people with dementia (PWD) and the feasibility of a definitive trial on falls prevention.
Patients and methods: Dyads, comprising community-dwelling PWD and their informal carer (N=85), were randomised to usual care (n=43) or usual care plus weekly Tai Chi classes and home practice for 20 weeks (n=42). The primary outcome was the timed up and go test. All outcomes for PWD and their carers were assessed six months post-baseline, except for falls, which were collected prospectively over the six-month follow-up period.
Results: For PWD, there was no significant difference at follow-up on the timed up and go test (mean difference [MD] = 0.82, 95% confidence interval [CI] = −2.17, 3.81). At follow-up, PWD in the Tai Chi group had significantly higher quality of life (MD = 0.051, 95% CI = 0.002, 0.100, standardised effect size [ES] = 0.51) and a significantly lower rate of falls (rate ratio = 0.35, 95% CI =0.15, 0.81), which was no longer significant when an outlier was removed. Carers in the Tai Chi group at follow-up were significantly worse on the timed up and go test (MD = 1.83, 95% CI = 0.12, 3.53, ES = 0.61). The remaining secondary outcomes were not significant. No serious adverse events were related to participation in Tai Chi.
Conclusion: With refinement, this Tai Chi intervention has potential to reduce the incidence of falls and improve quality of life among community-dwelling PWD [Trial registration: NCT02864056].
Keywords: accidental falls, clinical trial, cognitive impairment, exercise, intervention
Introduction
Falls are a major public health issue among older people.1 They are of even more concern among people with dementia (PWD), who are more than twice as likely to fall and twice as likely to experience injurious falls as their cognitively intact peers.2,3 PWD admitted to hospital with a fall injury are more likely to experience adverse health outcomes during their stay and after discharge such as hospital readmission, institutionalisation, and mortality.4,5
There is robust evidence for interventions, and in particular exercise-based interventions, to prevent falls and fall-related injuries among community-dwelling people without cognitive impairment.6–8 However, to date, only three exercise trials have been conducted with community-dwelling PWD,9–11 of which only one reported outcomes up to a 12-month follow-up.9 This latter study used an intensive provision that may be too expensive for some health services, including the UK. Thus, there is a need for more evidence-based fall prevention interventions for PWD.
Tai Chi is an ancient form of Chinese mind–body exercise, where participants carry out smooth and continuous body movements along with deep breathing and mental concentration;12 equivalent to moderate-intensity exercise and quiet meditation.13 This form of exercise is particularly suited for PWD with its use of slow and repetitive movements.14 Tai Chi has been found to provide numerous health benefits,15 though most of the relevant research to date has focused on balance outcomes among healthy older people.16
We conducted a trial to test the effect of Tai Chi on improving postural balance among PWD. It was also a feasibility study for a subsequent definitive trial to test the effect of Tai Chi on preventing falls among PWD. Systematic reviews have shown that Tai Chi is an effective exercise-based intervention for preventing falls among older people,8 frail and at-risk older adults,17,18 and older people with Parkinson’s disease and stroke.19 We report the first randomised controlled trial to test if Tai Chi can improve postural balance among PWD, and the future definitive trial will be the first to test if Tai Chi can prevent falls among PWD.
Materials And Methods
Design
We conducted a randomised, assessor-blind, two-arm, parallel group, superiority trial. The trial is registered (ClinicalTrials.gov ID no: NCT02864056, first posted August 11th, 2016), and was preceded by a pilot intervention phase.20 The trial was approved by the West of Scotland Research Ethics Committee 4 (reference: 16/WS/0139) and the Health Research Authority (IRAS project ID: 209193). A summary of the protocol is available along with details to access the full protocol and dataset.21 We randomised dyads, comprising a PWD and their informal carer, to either a control group (usual care) or an intervention group (usual care plus the TACIT Tai Chi intervention) in a 1:1 ratio at three recruitment sites in the south of England (see Figure 1). Randomisation was stratified by site, and we used minimisation within each site by treatment condition and 12-month fall history at baseline (fallen/not fallen). Randomisation was processed via a centralised web-based randomisation system designed and maintained by the UKCRC-registered Peninsula Clinical Trials Unit. After completion of the baseline home visit, a member of the trials unit randomised dyads and sent them a letter to advise their treatment allocation. During the trial, to aid recruitment, we made the following protocol amendments: reduced the eligibility criteria to a minimum age of 18 years and minimum Mini Addenbrooke’s Cognitive Examination (M-ACE) score of 10, and reimbursed participants for their travel (intervention group) and participation (control group).
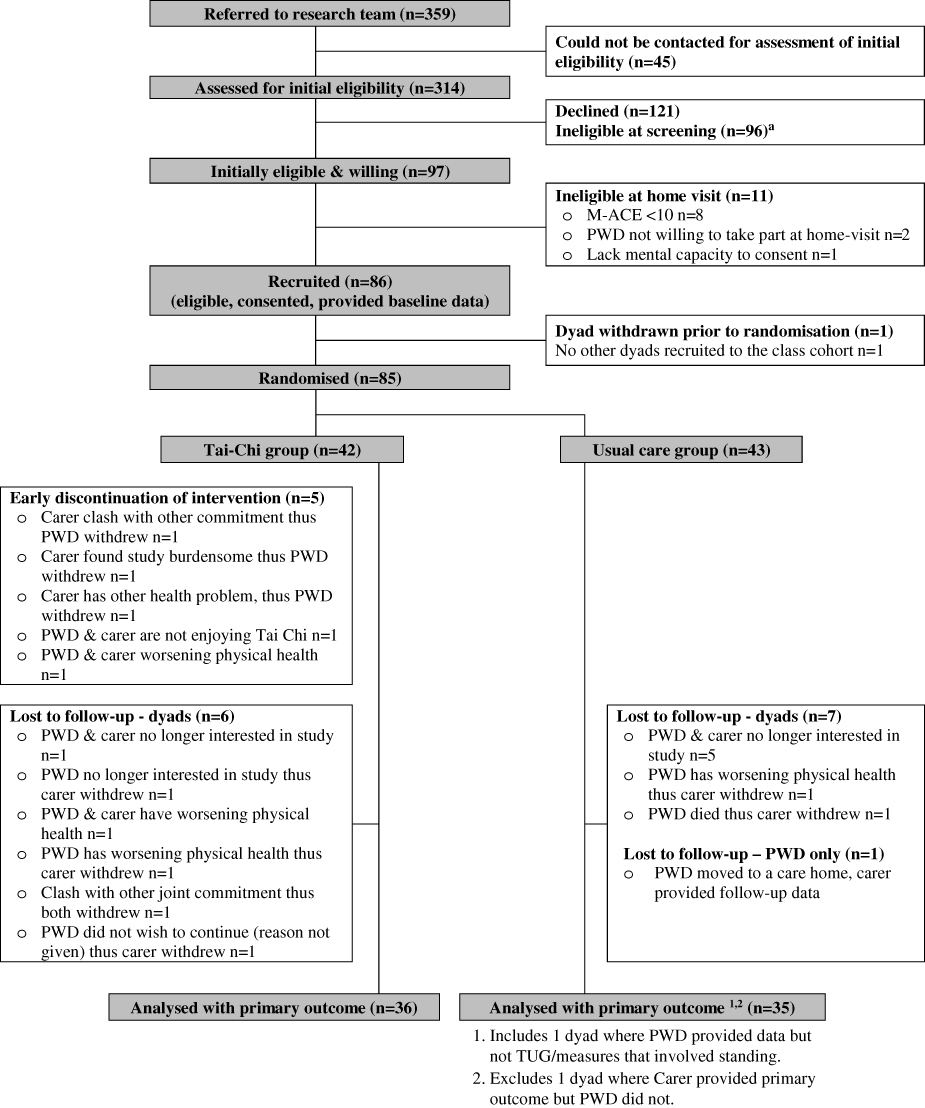 |
Figure 1 Flow diagram of study participation.Note: See Supplementary Figure S1 for details. |
Participants
Participants were identified and recruited via various sources, including National Health Service research/clinic databases, memory assessment services, local charities, and self-referral. Both the person with dementia and their informal carer were required to consent to participate. After referral, a member of the research team checked eligibility and then arranged a home visit to the dyad. At the visit, they took informed consent and then administered the M-ACE to confirm eligibility.22 PWD were included if they met the following criteria: aged 18 or above, living at home, had a diagnosis of dementia (indicated on their medical record held by the National Health Service or general practitioner), physically able to do standing Tai Chi, and willing to attend weekly Tai Chi classes. PWD were excluded if they met any of the following criteria: living in a care home, in receipt of palliative care, had severe dementia (baseline M-ACE score of ≤9),22 had a Lewy body dementia or dementia with Parkinson’s disease, had severe sensory impairment, were currently practising or had been practising within the past six months Tai Chi or similar exercise (Qi Gong, yoga, or Pilates) on average once a week or more, were currently under the care of or had been referred to a falls clinic for assessment, currently attending a balance exercise programme (eg Otago classes), or lacked mental capacity to provide informed consent. Informal carers were included if they met the following criteria: living with the PWD or could visit at least twice per week, were able to support the PWD by participating in data collection throughout the trial and in the intervention components (if randomised), able to do standing Tai Chi, and willing to attend weekly Tai Chi classes. Carers were excluded if they met any of the following criteria: had severe sensory impairment or lacked mental capacity to provide informed consent.
Intervention
Both groups received usual care. This may have included prescribed medicine and signposting to services for information and opportunities to socialise and receive peer support, but no exercise prescription. The intervention group also received a Tai Chi intervention comprising 3 components: (1) Tai Chi classes, (2) home-based Tai Chi practice, and (3) behaviour change techniques (see Table S1). The intervention was designed for participants to accrue 50 hrs or more Tai Chi in line with evidence that higher doses of exercise lead to greater reductions in falls.7 Classes were held once a week in suitable venues (eg, church halls). Each session was booked for 90 mins, with 45 mins instructor-led group Tai Chi followed by up to 45 mins informal discussion. Dyads were encouraged to participate in the informal discussions each week to foster mutual peer support, and provide opportunity for ongoing advice from the Tai Chi instructor in relation to the home-based practice. Up to 10 dyads were recruited per class. The approach to teaching at each class was the repetition of movements and positive reinforcement. This approach capitalises on PWD’s capacity to continue to learn and remember motor tasks with the use of procedural or kinaesthetic memory, ie, through making behaviours automatic, despite impaired ability to explicitly recollect such memories.23
The 20-week course was delivered by either a lead instructor with experience in teaching PWD or an additional instructor. Both instructors were experienced in teaching Tai Chi and had qualifications at senior instructor level for public Tai Chi classes. The lead instructor observed the other instructor teach a class for one of their first cohorts to ensure fidelity and provided minor adjustment to their teaching style. Five percent of classes were observed by a researcher who completed a fidelity checklist.
Outcomes
After demographic data were collected at baseline, the majority of measures were taken at baseline and repeated at six months post-baseline in dyads’ homes by a researcher kept blind to treatment condition. Dyads were reminded prior to the home visit to conceal their treatment allocation. Full details of the outcome measures used have been reported previously.21
Primary Outcome
For dynamic balance, we measured PWD’s mean timed up and go (TUG) score.24 This is a measure of how many seconds it takes for a participant to transition from a seated position to stand, walk 3 metres, turn, walk back, and be seated again.
Secondary Outcomes: PWD
For functional balance, we measured Berg balance score.25 For static balance, we measured postural sway while standing on the floor and on a foam mat,26 using total (anteroposterior + medio-lateral) normalised path length of the acceleration sway trace of the pelvis. This was recorded digitally using a Balance Sensor (THETAmetrix), mounted over the upper sacrum.
In a structured interview, PWD completed the Iconographical Falls Efficacy Scale (Icon-FES, short form)27 and the ICEpop CAPability measure for Older people (ICECAP-O)28 for fear of falls and quality of life, respectively. As noted above, they also completed the M-ACE as a measure of global cognitive functioning.22
Falls among PWD were collected prospectively from baseline until the follow-up home visit.29 We defined a fall as, ‘‘an unexpected event in which the participants come to rest on the ground, floor or lower level”.29 Falls were recorded prospectively by dyads daily, using calendars returned on a monthly basis by post. Telephone calls by an unblinded research assistant were conducted weekly to collect falls data as well,30 along with further information about falls and adverse events from dyads in the intervention group. To ascertain the accuracy of different recall periods, the research assistant conducted telephone calls about fall incidents by the PWD (monthly with the PWD and every 3 months with the carer). Each method of data collection was amalgamated into one overall measure of fall incidence, with duplicates removed (based on dates and description of the fall events).30 Fall injury was recorded by telephone interview when recording falls using existing definitions,31 as was health service use in relation to falls or adverse events. The total cost of providing the intervention to each patient was estimated from weekly registers completed by the Tai Chi instructors.
Secondary Outcomes: Informal Carers
Carers supported PWD in the study with data collection, and in the intervention arm, with their home practice of Tai Chi. To enable carers to facilitate Tai Chi home practise, they attended and participated in the Tai Chi classes along with the PWD. Therefore, we hypothesised that carers would also benefit from the Tai Chi intervention and tested for this. Carers completed the TUG and postural sway tests as described above. They also self-completed, away from the PWD, the ICECAP-O and Zarit Burden Interview (short-form).32
Statistical Analysis
Sample Size
The sample size was based on an estimated smallest detectable change on the TUG of a value of 4,33,34 standard deviation of 9.38,34 and correlation with baseline score of 0.7. Using the above values and a 2-sided 5% significance level, the study would have 90% power with a sample size of 120. Allowing for up to 20% withdrawal/non-completion of outcome measures, we aimed to recruit 150 dyads into the trial (75 per group).
Analysis
Participants were analysed in the group they were randomised to on an intention-to-treat basis. The primary and secondary outcomes were compared between the two trial arms using a mixed (multi-level) model approach to take into account clustering within Tai Chi classes, baseline scores, treatment site, and 12-month falls history. Fall incidence and the proportion of participants who fell were analysed similarly using negative binomial and logistic models, respectively. In addition, we conducted a per protocol analysis that excluded two people who did not have a dementia diagnosis (protocol violations) and participants from the Tai Chi group if they received fewer than 34 hrs. We also conducted a pre-planned subgroup analysis on mean TUG scores at 6-month follow-up according to baseline fall history.
Results
Participants
Dyads were recruited from 06/04/2017 to 17/07/2018, with the final follow-up completed on 30/11/2018. Figure 1 displays the recruitment and retention of participants (see Figure S1 for reasons declined/ineligible). Of the 359 approached, 85 dyads participated (24%), of which 70 (82%) had complete data for the primary outcome variable. Baseline characteristics suggested an even balance across trial arms including medication consumption and other long-term health conditions (see Table 1, and Tables S2–3 for further details).
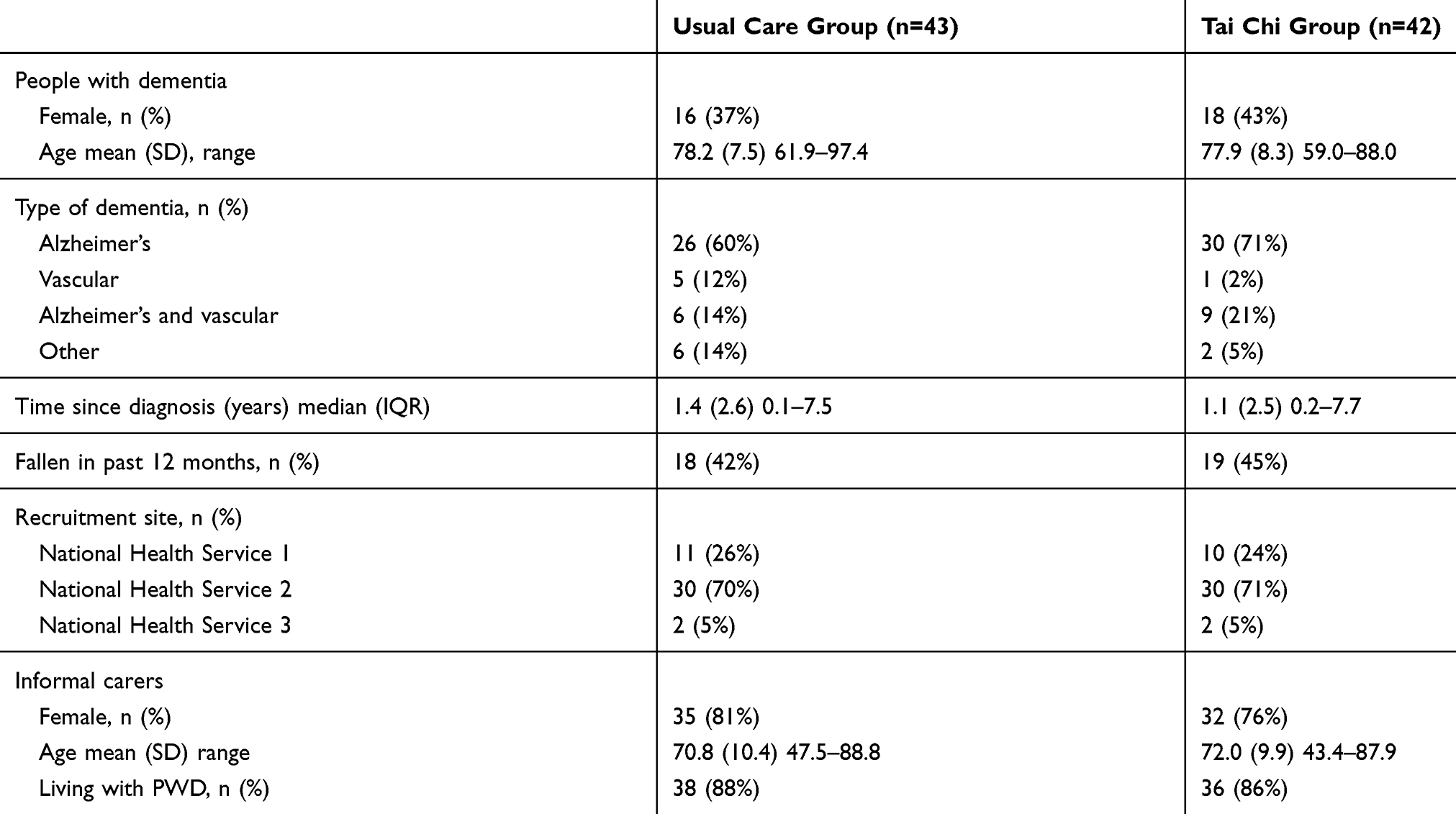 |
Table 1 Baseline Descriptive Statistics |
Fidelity Of Intervention Delivery
Thirty-four classes were observed and almost all aspects of the intervention were consistently delivered. The exceptions were that refreshments were not always provided to encourage socialising after classes, particularly when classes finished late in the afternoon or where parking was restricted. While the instructors emphasised the importance of Tai Chi home practice, they did not emphasise the intended dose of 20 mins per day.
Adherence
Out of a total possible 678 class attendances, there were 457 attendances by PWD and 449 by carers. Mean attendance was 11 classes for both PWD (SD = 6.46, n=41) and carers (SD = 6.68, n =41), or 8.4 and 8.2 hrs, respectively. Mean adherence to home practice was 35% (SD = 30.5, n=38), or 16.5 hrs (SD = 15.14, n=38) for PWD and 17 hrs (SD = 16.55, n=38) for carers. Mean dose of Tai Chi was 23.6 hrs (SD = 19.27, n=41) for PWD and 24.1 hrs (SD = 20.84, n=41) for carers. Three participants (7%) received the intended 50 hrs dose.
Outcomes At Follow-Up: PWD
The outcomes for PWD at follow-up are shown in Tables 2 and 3. There was no significant between-group difference on the TUG in the primary analysis or pre-planned subgroup analysis between those with/without a falls history at baseline. Among the secondary outcomes, PWD in the Tai Chi group had a significantly higher quality of life (medium effect size) and a significantly lower rate of falls (medium effect size, though sensitive to an outlier). The remaining secondary outcomes were not significant with little difference between trial arms. Per protocol analysis obtained similar results.
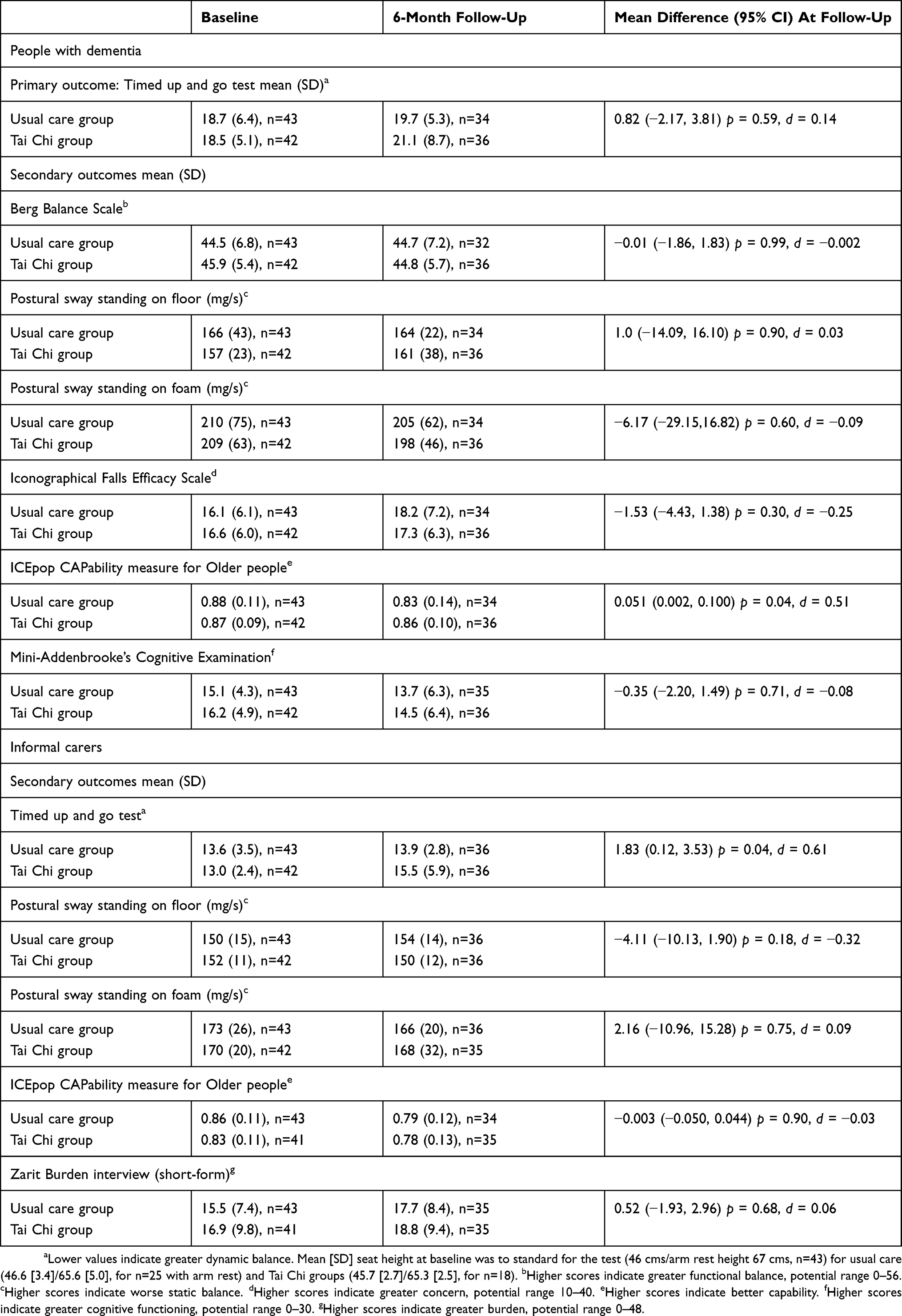 |
Table 2 Continuous Outcomes For People With Dementia And Their Informal Carers |
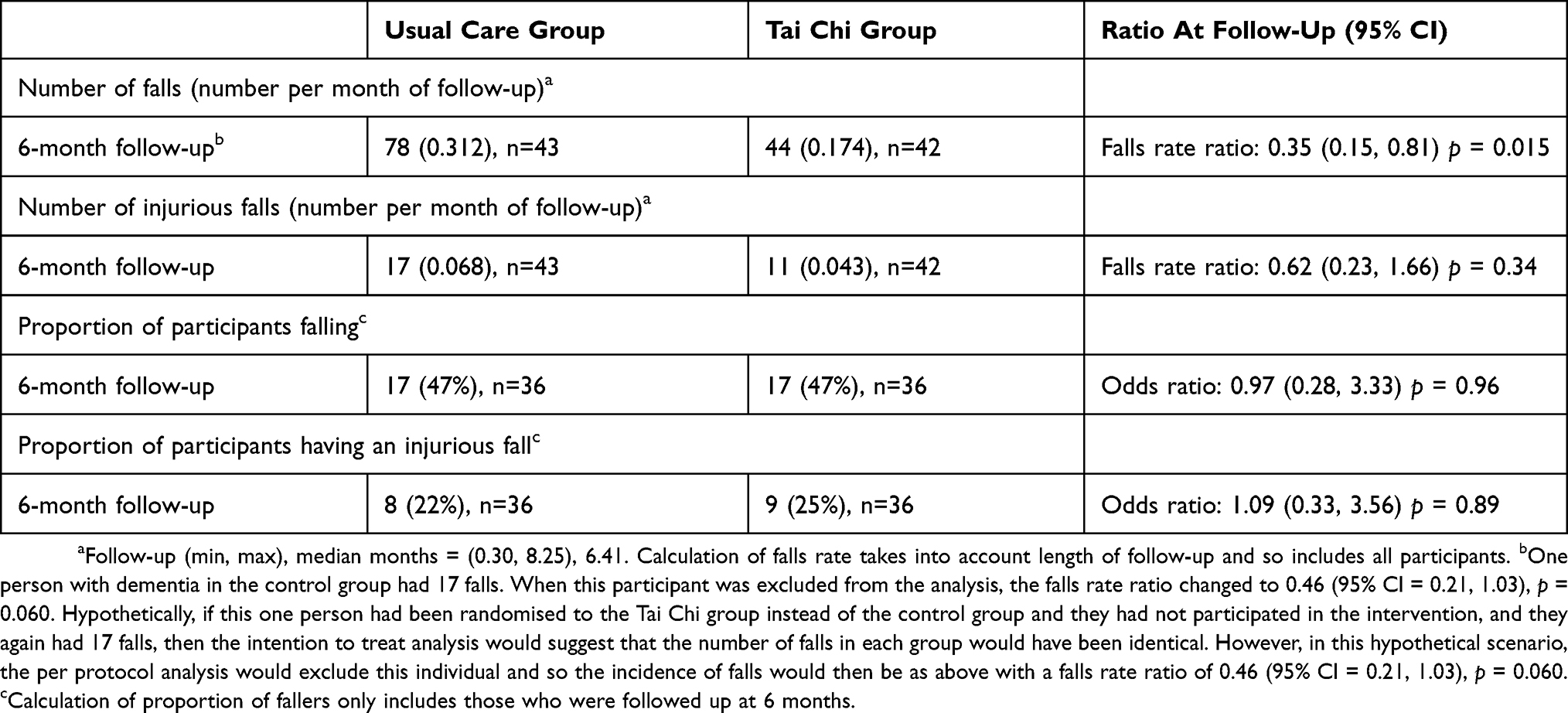 |
Table 3 Falls Outcomes For People With Dementia |
Outcomes At Follow-Up: Informal Carers
The outcomes for carers at follow-up are shown in Table 2. Carers in the Tai Chi group had significantly worse performance on the TUG (medium effect size). The remaining secondary outcomes were not significant with little difference between trial arms. Per protocol analysis obtained similar results.
Adverse Events
No serious adverse events were related to participation in the trial (see Table S4).
Health Economics
The cost of Tai Chi instructors came to £26,995, with a mean cost of £631 per intervention group dyad. This was markedly higher than dyads’ willingness to pay (see Table S5).
Assessor Blinding At Follow-Up
The outcome assessor was accidentally unblinded at follow-up by 9 dyads. The assessor was then able to correctly guess their treatment allocation, and guess correctly 63% of treatment allocations (45/72, p=0.044).
Discussion
This randomised controlled trial showed that compared to usual care alone, Tai Chi in addition to usual care did not improve postural balance among PWD. This was evident from both the primary outcome (TUG) and secondary outcomes (Berg balance and postural sway). PWD in the Tai Chi group had a significantly greater quality of life (standardised effect size = 0.51). There was a trend for a reduction in falls among PWD in the Tai Chi group, which became non-significant (p = 0.06) once an outlier was removed. There were no significant improvements for PWD on the other secondary outcomes. For carers, the Tai Chi group had significantly worse TUG scores (standardised effect size =0.61) but no significant change in postural sway. Carrying out and supporting PWD to participate in Tai Chi led to no significant change in their quality of life or carer burden. The above marginal statistically significant secondary outcomes need to be interpreted in the context of 15 secondary outcomes and the risk of type 1 error. While the power for the statistical analysis of the primary outcome was lower than planned due to under-recruitment, the 95% confidence interval did not include the smallest detectable change of 4 and therefore any real difference between groups at follow-up on the TUG is unlikely to be of clinical importance. Tai Chi was found to be safe with no serious adverse events experienced in relation to practising Tai Chi in class or at home.
Primary And Secondary Outcomes: PWD
Our results contrast with previous studies that have found Tai Chi to improve scores on the TUG among older people (weighted mean difference [WMD] = 1.04, 95% CI: 0.67, 1.41)35 and people with Parkinson’s disease when compared to a no-treatment group (WMD = −2.13, 95% CI: −3.26, −1.00).19 In addition, our results contrast with previous findings for Tai Chi to improve Berg balance scores among older people (WMD = 2.86, 95% CI: 1.91, 3.81),35 and improve static balance among those at low but not high risk of falling.36 However, these previous improvements may not be clinically significant,37,38 suggesting that Tai Chi may prevent falls through other mechanisms and not primarily through static and dynamic balance. Given that Tai Chi promotes slow and mindful movement, it may be that the intervention group were walking more mindfully and so at less risk of falls. Further research could examine whether Tai Chi leads to clinically and statistically significant improvements on other outcomes not measured such as leg muscle strength.
We hypothesised that the mechanism for Tai Chi to reduce falls would be via an improvement in postural stability. While we did not observe a significant reduction in the number of fallers, this was less likely as previous exercise interventions have reduced the rate of falls by an average of 23% but the number of fallers by 15%.8 Similarly, we did not observe a significant reduction in injurious falls, as they have a lower event rate and would need a large sample to identify a treatment effect.31 However, we identified a trend for a reduction in the rate of falls among the Tai Chi group. This trend was no longer significant when an outlier with a high rate of falls in the control group was removed (see footnote, Table 3). Future trials of Tai Chi and other exercise-based interventions should examine the mechanism(s) for a reduction in falls. This would build on a trial that found Tai Chi reduced falls more effectively than multi-modal exercise, but no secondary outcomes were different between the two arms to explain the mechanism.39 It would also build on a previous exercise trial that found a reduction in falls without an improvement in the TUG and functional reach tests.40 Other possible mechanisms would include improving leg muscle strength and cognitive motor control to perform everyday activities safely such as stepping onto a curb,41,42 and improving cognition to be more able to complete two tasks at the same time, such as walking while talking.43,44
We found no significant improvement for PWD in the Tai Chi group on fear of falls or global cognitive functioning. While there is weak evidence that exercise reduces fear of falls post-intervention,45 our findings contrast with previous studies that have found Tai Chi to enhance cognitive functioning among those with and without dementia.46 Further research could examine the benefits of Tai Chi using more sensitive and specific measures of cognitive functioning such as executive functioning.
We found quality of life to be significantly higher among PWD in the Tai Chi group. Previous studies have found that Tai Chi improves physical and mental health-related quality of life,12 including depression, anxiety, and psychological well-being.47 However, our results suggest that the Tai Chi group retained their level of quality of life and the control group significantly worsened. It is possible that the worsening in quality of life observed in the control group was associated with their trend for a greater rate of falls. Alternatively, PWD may have retained their quality of life through the benefits of Tai Chi from its use of mindfulness, relaxation, cognitive stimulation, and social interaction.48
While the reporting of adverse events in previous Tai Chi trials has been poor and inconsistent, our study supports the evidence base that Tai Chi does not lead to serious adverse events (eg, a fall resulting in hip fracture) but may be associated with some minor and expected adverse events (eg, knee and backache).49
Secondary Outcomes: Informal Carers
It is unclear why we found carers in the Tai Chi group to have significantly worse TUG scores. Due to unblinding of the assessor early in the trial, we removed questions from the exit interview on exercise conducted outside of the provided intervention. It could be that carers in the control group engaged in more exercise that improved their balance due to disappointment of not being randomised to Tai Chi. Future research should measure physical activity in conjunction with measures of balance and falls to clarify causal effects.50 Alternatively, the intervention may have increased carers’ awareness of the risk of falls and to walk “more mindfully”, and so they may have walked slower but more safely. Future research would benefit from using other measures of physical functioning that do not rely on gait speed.
We found no evidence for change in quality of life or carer burden among carers. This contrasts with previous studies that found improvements in carer burden and quality of life among carers supporting PWD participating in an exercise or cognition-based intervention, respectively;51,52 but greater anxiety and stress among carers supporting PWD with reminiscence therapy.53 Perhaps the lack of change on these variables observed in this study was because the additional demands on carers to facilitate Tai Chi class attendance and home practice were balanced by the enjoyment of these activities. Future research could qualitatively explore this in more detail.
Study Limitations
While this was a pragmatic trial and the eligibility criteria were kept as broad as possible, the effect of Tai Chi found in our study may be weaker when applied to the general population of PWD and their informal carers. This trial was limited by a reduction in statistical power due to a lower number of dyads recruited than expected. This is reflective of the broader challenges of recruiting and retaining PWD and their informal carers in research and the need to recruit dyads in groups within the trial design. The reduction in statistical power for detecting differences in all the outcomes, including the TUG from 90% to 69%, means that it is possible the study missed important effects (eg, rate of falls once the outlier was removed). However, we note that the smallest detectable change of a value of 4 s for the TUG was outside the 95% confidence interval (−2.17, 3.81), suggesting our test on the primary outcome was adequately powered.
The study was also limited by the Tai Chi group receiving a lower dose than planned. However, the exact dose needed to prevent falls is unknown. Indeed, current knowledge on intervention dose is drawn from a meta-regression across various interventions and contexts and not specifically, eg, Tai Chi for PWD.7 Class attendance and home practice was comparable to prior exercise trials, though slightly lower in this study given the previous studies excluded PWD.54–56 Further research is required to determine the exact dose required of specific exercise interventions to prevent falls in specific populations. Another limitation is that we did not collect data to confirm the homework sheets were used for the Tai Chi home practice. Future research could collect data to confirm not only the quantity of home practice but also the quality (eg, which exercises were performed each week).
Practice Implications
While practitioners await evidence from future robust definitive trials as to the clinical and cost-effectiveness of Tai Chi for preventing falls among PWD, this study demonstrates that Tai Chi is a safe activity for PWD. This study also suggests that the support required from carers does not decrease their perceived quality of life or increase their perceived carer burden. Indeed, our earlier work found the intervention to be acceptable to PWD and their carers.20 Therefore, qualified Tai Chi instructors are encouraged to provide classes for PWD and their family carers so that PWD may also benefit from this exercise for their general health and wellbeing.57,58
Conclusions
The results suggest that there is potential for Tai Chi as a safe exercise intervention to reduce falls among community-dwelling PWD and improve their quality of life. Also, the intervention did not increase carer burden or reduce quality of life among informal carers. Further work is required to increase adherence to the home-based element of the intervention and identify the mechanism(s) for its potential to reduce falls.
Abbreviations
CI, Confidence Interval; ES, Effect Size; ICECAP-O, ICEpop CAPability measure for Older people; Icon-FES, Iconographical Falls Efficacy Scale; M-ACE, Mini Addenbrooke’s Cognitive Examination; MD, Mean Difference; PWD, People With Dementia; SD, Standard Deviation; TUG, Timed up and Go test; WMD, Weighted Mean Difference.
Ethics Approval And Informed Consent
The trial was approved by the West of Scotland Research Ethics Committee 4 (reference: 16/WS/0139) and the Health Research Authority (IRAS project ID: 209193). After having time to read the participant information sheet and discuss the project with a member of the research team, each participant signed an informed consent form to confirm their voluntary participation in the trial.
Data Availability
The electronic, quantitative trial data will be shared with bona fide researchers intending to use the data for non-commercial research purposes, after an embargo period of approximately 24 months (ending January 2021). Access to the following will be restricted to researchers who sign a confidentiality agreement and confirm their intention to use the data is for secondary data analysis for non-commercial research purposes using a Creative Commons licence: statistical analysis plan; where applicable, statistical code (for final analysis of primary outcome measure); and anonymised participant-level dataset and data documentation. Interested parties may make a formal request to access the electronic dataset, which will be approved/declined by the chief investigator in accordance with the Data Management Plan that will detail management of access, sharing, and preservation of the data. Any use of the electronic data set must be requested via Bournemouth University Library ([email protected]) who will collaborate with the chief investigator with regards to access.
Acknowledgments
The authors acknowledge senior instructor Robert Joyce, Elemental Tai Chi, who designed the 20-week Tai Chi course for this study. The authors thank senior instructor Robert Joyce and instructor Vicki Fludgate for delivering the Tai Chi intervention under the company Elemental Tai Chi. The authors acknowledge the advice received from Dr Shanti Shanker in regard to cognitive testing, Dr Jonathan Williams in regard to objective measurement of static and dynamic balance, and our public and patient involvement group co-led with Helen Allen on our approach to recruitment and data collection. The authors thank the Alzheimer’s Society for their assistance with publicising the study, the General Practice surgeries in Wessex that assisted with recruitment, and the three main recruitment sites: Memory Assessment Research Centre, Southern Health NHS Foundation Trust (Principal Investigator: Brady McFarlane), Memory Assessment Service, Dorset HealthCare University NHS Foundation Trust (Principal Investigator: Kathy Sheret and then Claire Bradbury), and Research and Improvement Team and Older People’s Mental Health Service, Solent NHS Trust (Principal Investigator: Sharon Simpson). We also thank the Trial Steering Committee for their expert input (Independent Chair: Frances Healey, NHS Improvement).
Author Contributions
All authors have approved the final version of the manuscript to be published and have agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of the work are appropriately investigated and resolved. SRN: Chief investigator: Study concept and design, coding of health conditions at baseline and changes in health during the trial, interpretation of data, and preparation of the first draft and final version of the manuscript. WI: Study design, acquisition and interpretation of data, and critical comment on drafts in preparation of the manuscript. JS: Study design, acquisition and interpretation of data, and critical comment on drafts in preparation of the manuscript. PT: Trial statistician: Study design, analysis and interpretation of data, and critical comment on drafts in preparation of the manuscript. ST: Study design, analysis and interpretation of data, and critical comment on drafts in preparation of the manuscript. MV: Trial clinician: Study design, coding of adverse events, coding of health conditions at baseline and changes in health during the trial, interpretation of data, and critical comment on drafts in preparation of the manuscript. JR: Trial health economist: Study design, analysis of health economic data, interpretation, and critical comment on drafts in preparation of the manuscript. IB: Acquisition of data and critical comment on drafts in preparation of the manuscript. YB-M: Acquisition of data and critical comment on drafts in preparation of the manuscript. All authors contributed to the study design/acquisition of data/data analysis, drafting/revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Sponsor’s Role
A representative of Southern Health NHS Foundation Trust was a member of the trial management group and had critical input into the design and management of the trial, including acting as a recruitment site. The Sponsor had no input into the methods, data collection, data analysis, or preparation of the paper.
Funding
This work was funded by the National Institute for Health Research (NIHR) Career Development Fellowship Award to SRN (chief investigator). This paper presents independent research funded by the NIHR’s Career Development Fellowship Programme (grant number CDF-2015-08-030). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care. During the peer-review and interview process, the chief investigator received critical comment on the proposal. However, the funder had no influence on the trial, including: trial design; data collection, analysis, and interpretation; manuscript writing; and dissemination of results including the decision to submit the article. The chief investigator had final decision on these matters.
Disclosure
Dr Samuel R Nyman, Dr Wendy Ingram, Dr Jeanette Sanders, Professor Peter W Thomas, Dr Sarah Thomas, Professor James Raftery, and Dr Yolanda Barrado-Martín report the above grant from the National Institute for Health Research (NIHR) for the conduct of the study. Ms Iram Bibi was funded by Bournemouth University. The authors report no other conflicts of interest in this work.
References
1. World Health Organization. WHO Global Report on Falls Prevention in Older Age. Geneva: World Health Organization; 2007.
2. Taylor M, Delbaere K, Close J, Lord S. Managing falls in older people with cognitive impairment. Ageing Health. 2012;8(6):573–588. doi:10.2217/ahe.12.68
3. Meuleners L, Hobday M. A population-based study examining injury in older adults with and without dementia. J Am Geriatr Soc. 2017;65(3):520–525. doi:10.1111/jgs.14523
4. Dramé M, Fierobe F, Lang P, et al. Predictors of institution admission in the year following acute hospitalisation of elderly people. J Nutr Health Aging. 2011;15(5):399–403. doi:10.1007/s12603-011-0004-x
5. Watkin L, Blanchard M, Tookman A, Sampson E. Prospective cohort study of adverse events in older people admitted to the acute general hospital: risk factors and the impact of dementia. Int J Geriatr Psychiatry. 2012;27(1):76–82. doi:10.1002/gps.2693
6. El-Khoury F, Cassou B, Charles M-A, Dargent-Molina P. The effect of fall prevention exercise programmes on fall induced injuries in community dwelling older adults: systematic review and meta-analysis of randomised controlled trials. BMJ. 2013;347(f6234):Published online 29 October. doi:10.1136/bmj.f6234
7. Sherrington C, Michaleff ZA, Fairhall N, et al. Exercise to prevent falls in older adults: an updated systematic review and meta-analysis. Br J Sports Med. 2017;57:1750–1758. doi:10.1136/bjsports-2016-096547
8. Sherrington C, Fairhall N, Wallbank G, et al. Exercise for preventing falls in older people living in the community (Review). Cochrane Database Syst Rev. 2019;1:Art. No.: CD012424. doi: 012410.011002/14651858.CD14012424.pub14651852. doi:10.1002/14651858.CD012424.pub2
9. Pitkälä KH, Pöysti MM, Laakkonen ML, et al. Effects of the Finnish Alzheimer Disease Exercise Trial (FINALEX): a randomized controlled trial. JAMA Intern Med. 2013;173(10):894–901. doi:10.1001/jamainternmed.2013.359
10. Suttanon P, Hill K, Said C, et al. Feasibility, safety and preliminary evidence of the effectiveness of a home-based exercise programme for older people with Alzheimer’s disease: a pilot randomized controlled trial. Clin Rehabil. 2013;27(5):427–438. doi:10.1177/0269215512460877
11. Wesson J, Clemson L, Brodaty H, et al. A feasibility study and pilot randomised trial of a tailored prevention program to reduce falls in older people with mild dementia. BMC Geriatr. 2013;13:e89. doi:10.1186/1471-2318-13-89
12. Lee LY, Lee DT, Woo J. The psychosocial effect of Tai Chi on nursing home residents. J Clin Nurs. 2010;19(7–8):927–938. doi:10.1111/j.1365-2702.2009.02793.x
13. Li J, Hong Y, Chan K. Tai chi: physiological characteristics and beneficial effects on health. Br J Sports Med. 2001;35(3):148–156. doi:10.1136/bjsm.35.3.148
14. Tadros G, Ormerod S, Dobson-Smyth P, et al. The management of behavioural and psychological symptoms of dementia in residential homes: does Tai Chi have any role for people with dementia? Dementia. 2013;12(2):268–279. doi:10.1177/1471301211422769
15. Solloway M, Taylor S, Shekelle P, et al. An evidence map of the effect of Tai Chi on health outcomes. Syst Rev. 2016;5(1):e126. doi:10.1186/s13643-016-0289-2
16. Rogers C. Tai Chi to promote balance training. Annu Rev Gerontol Geriatr. 2016;36:229–249. doi:10.1891/0198-8794.36.229
17. Lomas-Vega R, Obrero-Gaitán E, Molina-Ortega F, Del-Pino-Casado R. Tai Chi for risk of falls. A meta-analysis. J Am Geriatr Soc. 2017;65(9):2037–2043. doi:10.1111/jgs.15008
18. Del-Pino-Casado R, Obrero-Gaitán E, Lomas-Vega R. The effect of Tai Chi on reducing the risk of falling: a systematic review and meta-analysis. Am J Chin Med. 2016;44(5):895–906. doi:10.1142/S0192415X1650049X
19. Winser S, Tsang W, Krishnamurthy K, Kannan P. Does Tai Chi improve balance and reduce falls incidence in neurological disorders? A systematic review and meta-analysis. Clin Rehabil. 2018;32(9):1157–1168. doi:10.1177/0269215518773442
20. Barrado-Martín Y, Heward M, Polman R, Nyman S. Acceptability of a dyadic Tai Chi intervention for older people living with dementia and their informal carers. J Aging Phys Act. 2019;27(2):166–183. doi:10.1123/japa.2017-0267
21. Nyman S, Hayward C, Ingram W, et al. A randomised controlled trial comparing the effectiveness of Tai Chi alongside usual care with usual care alone on the postural balance of community-dwelling people with dementia: protocol for The TACIT Trial (TAi ChI for people with demenTia). BMC Geriatr. 2018;18:e263. doi:10.1186/s12877-018-0935-8
22. Hsieh S, McGrory S, Leslie F, Dawson K, Ahmed S, Butler C. The mini-addenbrooke’s cognitive examination: a new assessment tool for dementia. Dement Geriatr Cogn Disord. 2015;39(1):1–11. doi:10.1159/000366040
23. Yao L, Giordani B, Alexander NB. Developing a Positive Emotion-Motivated Tai Chi (PEM-TC) exercise program for older adults with dementia. Research Theory Nurs Pract. 2008;22(4):241–255. doi:10.1891/1541-6577.22.4.241
24. Podsiadlo D, Richardson S. The timed up and go – a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991;39(2):142–148. doi:10.1111/j.1532-5415.1991.tb01616.x
25. Berg K, Wood-Dauphine S, Williams JI, Gayton D. Measuring balance in the elderly: preliminary development of an instrument. Physiother Can. 1989;41(6):304–311. doi:10.3138/ptc.41.6.304
26. Taylor M, Delbaere K, Lord S, Mikolaizak A, Brodaty H, Close J. Neuropsychological, physical, and functional mobility measures associated with falls in cognitively impaired older adults. J Gerontol. 2014;69(8):987–995. doi:10.1093/gerona/glt166
27. Delbaere K, Smith ST, Lord SR. Development and initial validation of the iconographical falls efficacy scale. J Gerontol. 2011;66(6):674–680. doi:10.1093/gerona/glr019
28. Coast J, Flynn T, Natarajan L, et al. Valuing the ICECAP capability index for older people. Soc Sci Med. 2008;67(5):874–882. doi:10.1016/j.socscimed.2008.05.015
29. Lamb S, Jørstad-Stein E, Hauer K, Becker C. Development of a common outcome data set for fall injury prevention trials: the prevention of falls network Europe consensus. J Am Geriatr Soc. 2005;53(9):1618–1622. doi:10.1111/j.1532-5415.2005.53455.x
30. Zieschang T, Schwenk M, Becker C, Oster P, Hauer K. Feasibility and accuracy of fall reports in persons with dementia: a prospective observational study. Int Psychogeriatr. 2012;24(4):587–598. doi:10.1017/S1041610211002122
31. Schwenk M, Lauenroth A, Stock C, et al. Definitions and methods of measuring and reporting on injurious falls in randomised controlled fall prevention trials: a systematic review. BMC Med Res Methodol. 2012;12:e50. doi:10.1186/1471-2288-12-50
32. Bedard M, Molloy DW, Squire L, Dubois S, Lever JA, O’Donnell M. The Zarit burden interview: a new short version and screening version. Gerontologist. 2001;41(5):652–657. doi:10.1093/geront/41.5.652
33. Ries J, Echternach J, Nof L, Gagnon Blodgett M. Test-retest reliability and minimal detectable change scores for the timed “up & go” test, the six minute walk test, and gait speed in people with Alzheimer disease. Phys Ther. 2009;89(6):569–579. doi:10.2522/ptj.20080258
34. Blankevoort C, van Heuvelen M, Scherder E. Relibility of six physical performance tests in older people with dementia. Phys Ther. 2013;92(1):69–78. doi:10.2522/ptj.20110164
35. Huang Y, Liu X. Improvement of balance control ability and flexibility in the elderly Tai Chi Chuan (TCC) practitioners: a systematic review and meta-analysis. Arch Gerontol Geriatr. 2015;60(2):233–238. doi:10.1016/j.archger.2014.10.016
36. Song R, Ahn S, So H, Lee E, Chung Y, Park M. Effects of t’ai chi on balance: a population-based meta-analysis. J Altern Complement Med. 2015;21(3):141–151. doi:10.1089/acm.2014.0056
37. Schoene D, Wu SM, Mikolaizak AS, et al. Discriminative ability and predictive validity of the timed up and go test in identifying older people who fall: systematic review and meta-analysis. J Am Geriatr Soc. 2013;61(2):202–208. doi:10.1111/jgs.12106
38. Donoghue D, Stokes EK. How much change is true change? The minimum detectable change of the berg balance scale in elderly people. J Rehabil Med. 2009;41(5):343–346. doi:10.2340/16501977-0337
39. Li F, Harmer P, Fitzgerald K, et al. Effectiveness of a therapeutic Tai Ji Quan intervention vs a multimodal exercise intervention to prevent falls among older adults at high risk of falling: a randomized clinical trial. JAMA Intern Med. 2018. Published online September 10. doi:10.1001/jamainternmed.2018.3915
40. Iliffe S, Kendrick D, Morris R, et al. Multicentre cluster randomised trial comparing a community group exercise programme and home-based exercise with usual care for people aged 65 years and over in primary care. Health Technol Assess (Rockv). 2014;18(49):1–105. doi:10.3310/hta18490
41. van Andel S, Cole MH, Pepping GJ. Associations between gait-related falls and gait adaptations when stepping onto a curb: a prospective falls study. J Aging Phys Act. 2019;27(3):309–315. doi:10.1123/japa.2018-0124
42. Mirelman A, Rochester L, Maidan I, et al. Addition of a non-immersive virtual reality component to treadmill training to reduce fall risk in older adults (V-TIME): a randomised controlled trial. Lancet. 2016;388(10050):1170–1182. doi:10.1016/S0140-6736(16)31325-3
43. Beauchet O, Annweiler C, Dubost V, et al. Stops walking when talking: a predictor of falls in older adults? Eur J Neurol. 2009;16(7):786–795. doi:10.1111/j.1468-1331.2009.02612.x
44. Ellmers TJ, Young WR. Conscious motor control impairs attentional processing efficiency during precision stepping. Gait Posture. 2018;63:58–62. doi:10.1016/j.gaitpost.2018.04.033
45. Kumar A, Delbaere K, Zijlstra G, et al. Exercise for reducing fear of falling in older people living in the community: cochrane systematic review and meta-analysis. Age Ageing. 2016;45(3):345–352. doi:10.1093/ageing/afw036
46. Wayne P, Walsh J, Taylor-Piliae R, et al. Effect of tai chi on cognitive performance in older adults: systematic review and meta-analysis. J Am Geriatr Soc. 2014;62(1):25–39. doi:10.1111/jgs.12611
47. Wang F, Lee E, Wu T, et al. The effects of tai chi on depression, anxiety, and psychological well-being: a systematic review and meta-analysis. Int J Behav Med. 2014;21(4):605–617. doi:10.1007/s12529-013-9351-9
48. Wayne P, Fuerst M. The Harvard Medical School Guide to Tai Chi: 12 Weeks to a Healthy Body, Strong Heart & Sharp Mind. Colorado: Shambhala; 2013.
49. Wayne P, Berkowitz D, Litrownik D, Buring J, Yeh G. What do we really know about the safety of Tai Chi?: a systematic review of adverse event reports in randomized trials. Arch Phys Med Rehabil. 2014;95(12):2470–2483. doi:10.1016/j.apmr.2014.05.005
50. Ramulu P, Mihailovic A, West S, Friedman D, Gitlin L. What is a falls risk factor? Factors associated with falls per time or per step in individuals with glaucoma. J Am Geriatr Soc. 2018. Published online 26 October. doi:10.1111/jgs.15609
51. Vreugdenhil A, Cannell J, Davies A, Razay G. A community-based exercise programme to improve functional ability in people with Alzheimer’s disease: a randomized controlled trial. Scand J Caring Sci. 2012;26(1):12–19. doi:10.1111/j.1471-6712.2011.00895.x
52. Leung P, Orgeta V, Orrell M. The effects on carer well-being of carer involvement in cognition-based interventions for people with dementia: a systematic review and meta-analysis. Int J Geriatr Psychiatry. 2017;32(4):372–385. doi:10.1002/gps.4654
53. Woods R, Bruce E, Edwards R, et al. REMCARE: reminiscence groups for people with dementia and their family caregivers – effectiveness and cost-effectiveness pragmatic multicentre randomised trial. Health Technol Assess (Rockv). 2012;16(48):1–116. doi:10.3310/hta16480
54. McPhate L, Simek EM, Haines TP. Program-related factors are associated with adherence to group exercise interventions for the prevention of falls: a systematic review. J Physiother. 2013;59(2):81–92.
55. Nyman S, Victor C. Older people’s participation in and engagement with falls prevention interventions in community settings: an augment to the Cochrane systematic review. Age Ageing. 2012;41(1):16–23.
56. Simek EM, McPhate L, Haines TP. Adherence to and efficacy of home exercise programs to prevent falls: a systematic review and meta-analysis of the impact of exercise program characteristics. Prev Med. 2012;55(4):262–275. doi:10.1016/j.ypmed.2012.07.007
57. Ginis KA, Heisz J, Spence JC, et al. Formulation of evidence-based messages to promote the use of physical activity to prevent and manage Alzheimer’s disease. BMC Public Health. 2017;17(1):e209. doi:10.1186/s12889-017-4090-5
58. Nyman S, Szymczynska P. Meaningful activities for improving the wellbeing of people with dementia: beyond mere pleasure to meeting fundamental psychological needs. Perspect Public Health. 2016;136(2):99–107. doi:10.1177/1757913915626193
 © 2019 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.
© 2019 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.