")
Back to Journals » Orthopedic Research and Reviews » Volume 14
Radiation in Adolescent Idiopathic Scoliosis Management: Estimated Cumulative Pre-Operative, Intra-Operative, and Post-Operative Exposure
Authors Duke A , Marchese R, Komatsu DE, Barsi J
Received 29 August 2022
Accepted for publication 17 December 2022
Published 30 December 2022 Volume 2022:14 Pages 487—493
DOI https://doi.org/10.2147/ORR.S387369
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Alexander Duke, Richard Marchese, David E Komatsu, James Barsi
Department of Orthopaedics and Rehabilitation, Stony Brook University Hospital, Stony Brook, NY, USA
Correspondence: Alexander Duke, Stony Brook University Hospital, Health Sciences Center T18-089, Stony Brook, NY, 11794, USA, Tel +1 631 972-8324, Fax +1 631 444-3502, Email [email protected]
Background: Adolescent Idiopathic Scoliosis (AIS) is the most common type of scoliosis affecting adolescents, with approximately 2– 4% of children being diagnosed. Crucial to the diagnosis and management are radiographic imaging, which allow physicians to assess and treat – from initial visits through surgical planning and post-operative management. While initial stages require low levels of exposure to radiation, via x-rays, as patients progress in disease severity exposure becomes larger with pre-operative, intra-operative and post-operative CT scans. While many studies have evaluated exposure during AIS treatment, few have assessed the cumulative radiation exposure adolescents receive during their evaluation. The purpose of our study is to complete a comprehensive review on cumulative radiation exposure and determine what stages in AIS treatment expose patients to the highest level of radiation over a duration of 2 years.
Methods: A retrospective chart review of 109 AIS cases (29M, 80F), mean age 14.9 ± 2.3 years was completed to assess and quantify each imaging modality used. Employing a radiation detector, each imaging modality was then assessed, and estimated radiation exposures were determined. Statistical analysis was completed utilizing averaged patient exposures during each selected period in AIS management.
Results: Mean estimated radiation doses (StDev) were 60.94 mrem (± 0.609 mrem) for two x-rays (full-length AP and lateral radiograph of the entire spine), 12.92 mrem (± 1.292 mrem) for each fluoroscopy exposure, and 1340.60 mrem (± 13.406 mrem) per CT scan. Based on these values, estimated subject exposures were calculated. The total estimated radiation exposure over a 2-year period was 5572.74 mrem (± 1428.88 merm) or 2786.37 mrem (± 714.43 mrem) per year.
Conclusion: The two-year cumulative radiation exposure is below the recommended exposure by Nuclear Regulatory Commission and OSHA. As expected, CT exposure presents the largest radiation exposure to patients with AIS throughout their operative management.
Level of Evidence: III, retrospective study.
Keywords: scoliosis, radiation, adolescent idiopathic scoliosis
Introduction
Adolescent idiopathic scoliosis (AIS) is the most common type of scoliosis, affecting 2% to 4% of adolescents.1 Moderate curves are followed radiographically with serial x-rays to monitor curve progression.2 Surgical patients potentially can be exposed to more ionizing radiation with intra-operative fluoroscopy and Computed Tomography (CT). Post-operatively, spinal alignment is assessed radiographically.3 The combination of these procedures increases patient exposure to radiation, a factor which physicians must consider in the treatment process. One study reported that the typical AIS patient will be evaluated with 22 radiographs in a 3-year period.4 Another study reported that intra-operative fluoroscopy contributes to 78% of radiation exposure in AIS management.5
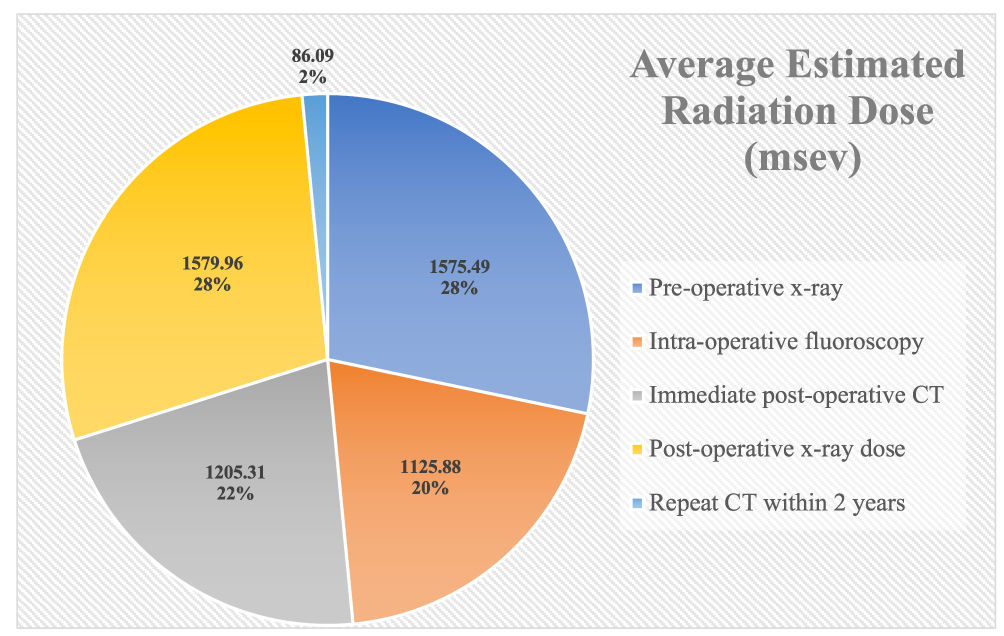 |
Figure 1 Estimated average radiation doses during dedicated periods in AIS management. Total average estimated cumulative dose 5572.74 mrem (55.72mSv). |
While many studies have evaluated radiation exposure in patients during AIS assessment, few have estimated and assessed the cumulative radiation exposure throughout AIS management and during different stages of treatment.5–9 Some studies report that intra-operative radiation during scoliosis surgery is within safe limits.9–11
Increased exposure to ionizing radiation has been shown to increase cancer rate. AIS patients have up to a 4.3% increased risk of cancer, involving breast and thyroid cancers.5,12 It has also been reported that surgically treated AIS patients have higher than baseline risks for leukemia, breast cancer, or a heritable defect; 0.8%, 2.1%, and 3.0%, respectively.13 Endometrial and breast cancer were found to be the most frequent in AIS patients and occurred at levels five times greater than those in an age-matched population.12
This study was designed to estimate the cumulative magnitude of radiation exposure throughout AIS management in patients managed surgically during the pre-operative, intra-operative, and post-operative period. The post-operative period was designated as a period of 2 years. This information is intended to allow surgeons to better weigh the clinical benefits of imaging techniques with the adverse effects of radiation exposure.5
Materials and Methods
This study was a retrospective chart review that was approved by the Stony Brook University Institutional Review Board. Inclusion criteria were patients with ages of 10–18 and a diagnosis of AIS that underwent posterior spinal fusion by a single board-certified pediatric orthopaedic surgeon. Informed consent was not obtained prior to study commencement as this was a retrospective review. All patient data was de-identified. Exclusion criteria included patients older than 18, patients with non-idiopathic curves, and patients with previous spinal surgery procedures. All patients meeting inclusion criteria between the dates of January 1, 2006, and December 31, 2013, were included in this study.
Demographic and radiographic exposure data were collected from the patients’ electronic medical records. For radiation exposure, we collected the following information on each patient: number of pre-operative x-rays prior to posterior spinal fusion, number of intra-operative fluoroscopy images during surgery, whether the patient had a post-operative CT, number of levels fused during surgery, number of post-operative x-rays up to 2 years following surgery, number of post-operative CTs up to 2 years following surgery, and if the patient returned to the OR prior to 2 years following the initial procedure.
In order to quantify the radiation doses associated with different imaging modalities, nanodot dosimeters (Landauer Inc., Glenwood, IL) were placed in the imaging path of each instrument. Each modality was assessed five times using different dosimeters. To account for background radiation, unexposed control dosimeters were kept in the same location as the experimental dosimeters. At the conclusion of each case, the doses (mrem) were measured using MicroStar InLight Reader portable dosimeter (Landauer).
To estimate radiation exposure each modality was assessed in standard fashion for the prescribed diagnostic modality. For x-ray assessment, two exposures were made to simulate a full-length AP and a Lateral radiograph view using a Philips Diagnostic Alivas model x-ray machine. Settings for both exposures were 75kVp, 20mAs, 250mA, and 80ms. Fluoroscopy exposure was estimate through five AP (88kVp, 1.2mA, 1s) and five lateral exposures (104kVp, 3.5mA, 1s) utilizing an OEC MinView 6800 (2005 model). Fluoroscopy, on the other hand, with its variable angles, adjustable distances between detector and patient, readily modified kVp and mA, presents challenges that require some assumptions for a “best fit” calculation. General factors that were standardized included distance from detector and body weight. Tissue weighting factors were then utilized and an average weighting factor was used to calculate effective dose based on incident radiation (mGy) for fluoroscopy and the dose length product for the intraoperative CT. The CT scan assessment was completed utilizing a single scan from a GE 64 Slice (2007 model).
For each subject, the number of x-rays, fluoroscopic images, and CT scans were multiplied by the empirically calculated doses to estimate patient exposure. Data was then categorized into pre-operative, intra-operative, and 2-year post-operative periods.
All data are reported as mean ± standard deviation.
Results
A total of 109 cases met the inclusion criteria. The mean age was 14.9 ± 2.3 years. Mean radiation doses (StDev) were 60.94 mrem (±0.609 mrem) for two x-rays, 129.18 mrem (±1.29 mrem) for 10 fluoroscopy exposures, and 1340.60mrem (± 13.406 mrem) for each CT scan. Based on these values, subject exposures were calculated. The total radiation exposure over a 2-year period was 5572.74 mrem (±1428.88 merm) or 2786.37 mrem (±714.43 mrem) per year. A break down of the average estimated radiation dose obtained during pre-operative, intra-operative, and post-operative examination is highlighted in Figure 1.
All patients received intra-operative fluoroscopy during their respective posterior spinal fusion surgeries. Ninety-eight patients (89.91%) underwent an immediate post-operative CT scan. Within the first 2 years post-operatively, 5 patients underwent repeat CT scans. Four patients had persistent pain at their surgical sites, and CT was obtained to evaluate hardware. One patient returned to surgery one week following the initial procedure secondary to hardware malposition; subsequently three separate CT scans were completed within two years of the initial procedure. Data are presented in Tables 1 and 2.
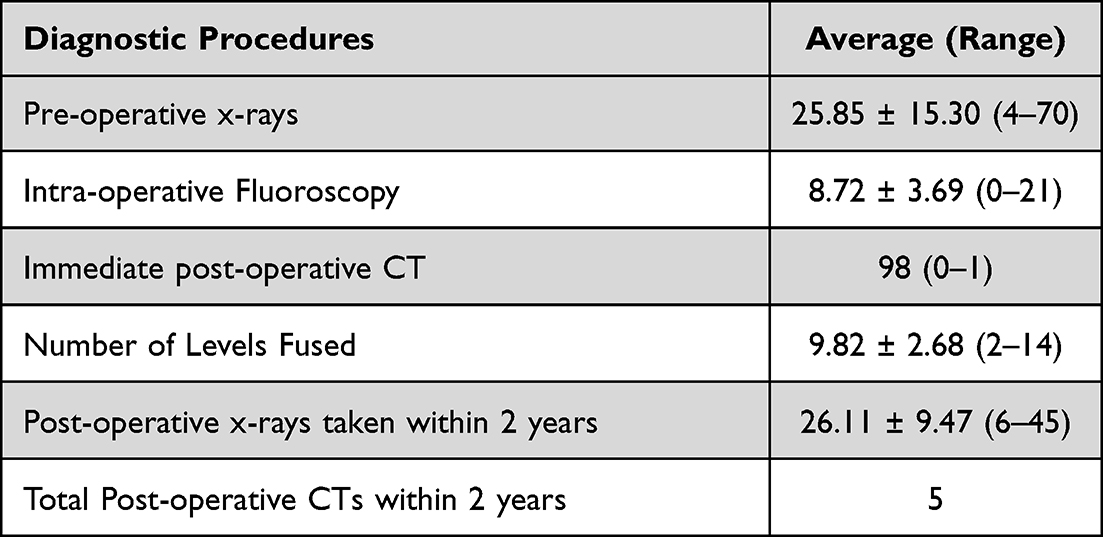 |
Table 1 Diagnostic Procedures During Dedicated Periods in AIS Management |
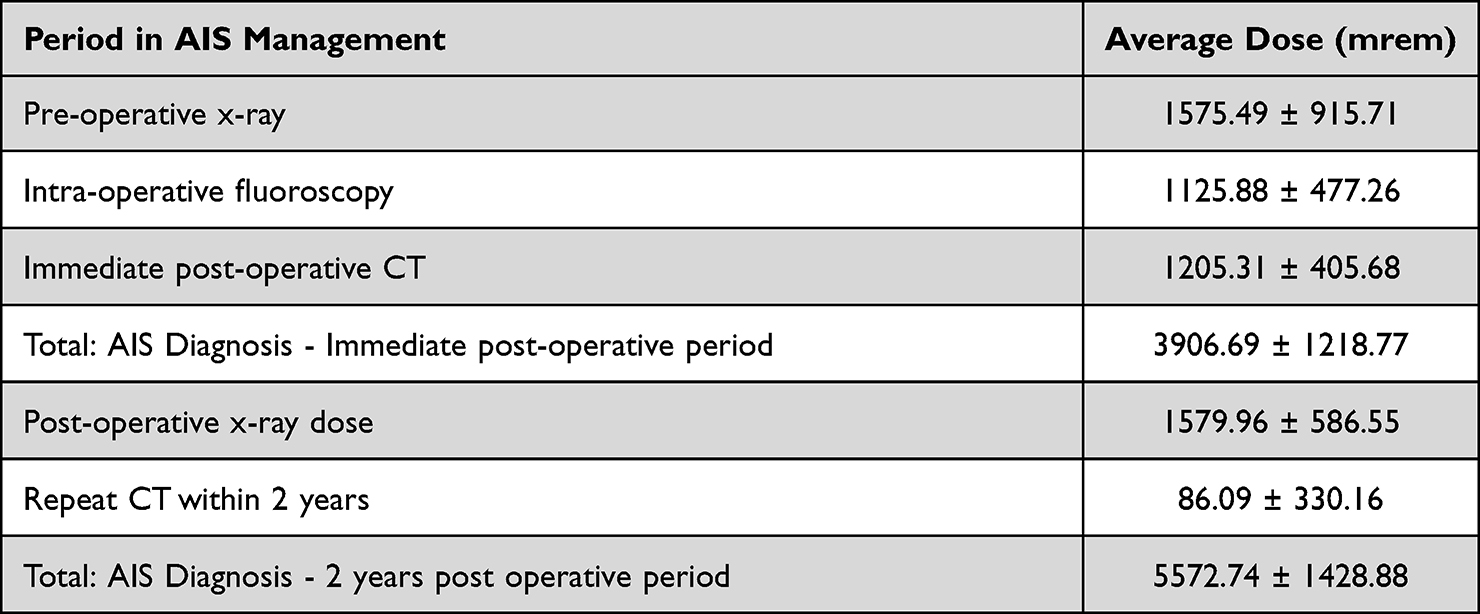 |
Table 2 Average Estimated Radiation Dose (Mrem) During Dedicated Periods in AIS Management |
Discussion
Patients with AIS require a radiography to assess and guide treatment. While it is a necessary component, it places pediatric patients at a heightened risk of cancer from radiation exposure. Pediatric tissues are more sensitive to the effects of radiation than those of adults and the longer life expectancy of pediatric patients gives them a greater potential to manifest the adverse effects of radiation.14 This increased risk of cancer among pediatric patients demands justification of radiological procedures and utilization of the minimal effective dose.14,15 This study was designed to better understand the estimated cumulative radiation exposure of AIS patients from assessment through surgical treatment. The aim of this study is to establish estimated radiographic exposures and assist physicians in making informed decisions to minimize patient radiation exposure.
While the present study used uniform equipment and standardized radiographic methods, some limitations persist. These include the limited number of cases and differences between patients (age, gender, follow-up visit intervals). Furthermore, this study assumed that the patients received the dose of radiation reported by the dosimeters. However, radiation scatter creates a difference between emitted and absorbed dose.16 Additionally, any repeat radiographs due to technical errors are not recorded which may result in underestimated radiation exposure. Surgeons may also have varied fluoroscopy use during screw placement, the number of pedicle screws placed, and levels fused. Presciutti and Lee reported that there was no statistical relationship between the operative radiation doses and number of levels fused or pedicle screws placed.5
For our patients, the total estimated radiation exposure over a 2-year period was 5572.74 mrem (±1428.88 mrem) or 2786.37 mrem (±714.43 mrem) per year. These values are below the upper limit of safety, 50mSv per year, as proposed by both the Nuclear Regulatory Commission, reported by Presciutti et al and the Occupational Safety and Health Administration (OSHA).5,17 The “average” American receives about 620 mrem (6.2 mSv) per year from all sources of radiation based on the National Council on Radiation Protection and Measurements published in the NCRP Report No. 160.18 NCRP radiation sources were defined as background radiation, exposure to consumer products, occupational exposures, exposures from industries and exposures due to medical procedures. In 2009, the estimated medical radiation exposure was 2.92 mSvm, in 2016 this number dropped to 2.16 mSv in 2016.19
It has been reported that cancer rate increases by 4.1% per Sievert (Sv); or 0.0041% per mSv.9 In our patient population, exposure level per year was 27.86 mSv compared to the average American medical exposure in 2009 at 2.92 mSv; 9.56 times higher in the same time span. Therefore, the increased risk of cancer in this patient population over a single year is 0.103% vs 0.012%. While this is within safe limits, clinical decisions that diminish the amount of radiation exposure according to the ALARA principle (As Low As Reasonably Achievable) should continue to be made to enhance patient safety.5 This assessment falls in line with recommendations of other studies with similar findings. Law et al17 calculated the radiation exposure from repeated full spine radiographs with postero-anterior and lateral projections in a patient from the age of 5–30 to be 1500 mrem, which is within safe limits and correlates with an increased cancer risk of 0.08–0.17%. This study also found female scoliosis patients to have a higher cancer risk compared to males.17 Despite finding that x-ray radiation exposure was within safe limits, the authors recommended prolongation of the time interval between full spine radiography to enhance patient safety.17
McArthur et al found that the intra-operative radiation dosage for AIS patients falls within safe limits, reporting an average radiation dose of 25.29 mrem (0.2529 mSv), which they reported was equivalent to cancer risk increased by 0.001% per patient.9 This study did acknowledged that, in addition to intra-operative radiation exposure, patients are exposed to radiation throughout AIS management. Based on these statistics, we can extrapolate that our patients have a cumulative 0.0011% increased risk of cancer over a one year period. Our estimated intra-operative fluoroscopy exposure was 12.25 mrem, 55.48% less than the exposure reported by McArthur et al.9 As such, precautions should be taken to reduce radiation exposure.
In concordance with the previous studies, the present study found that the pre-operative, intra-operative, and post-operative management of AIS to be within safe values; the most significant exposure in the peri-operative period. To protect patients from radiation risk, we advocate for that utilizing imaging techniques to minimize radiation exposure. Such techniques include attention to patient position, field size, protective shielding, and reduced fluoroscopy time. Postero-anterior (PA) views emit less radiation exposure compared to the antero-posterior (AP) radiography therefore, PA x-rays should be considered for initial and follow-up evaluations.5,21 A lateral radiograph, which results in higher radiation exposure compared to postero-anterior radiographs, should only be used for curve atypia, neurologic abnormalities, and pre- and post-operative evaluations.5 Low-dose radiography is also now available which can further minimize cumulative radiation exposure for patients.
Several recommendations have been proposed to reduce radiation exposure. CT scans should be adjusted to the patient’s weight and age, with the scanning area minimized, and the number of examinations reduced.14,15 Observed and braced patients are recommended to receive radiographic follow-ups at intervals of at least 6 months, as shorter time intervals were not found to change clinical decisions.5 After 6 months post-operation, follow-up intervals lower than one year were not found to change clinical decisions.5 There are several alternative imaging modalities and emerging technologies that attempt to minimize radiation exposure. Microdose X-rays are now available and provide a substantial dose reduction without compromising image quality.22–26 A second modality, EOS imaging, simultaneously takes full-body AP and lateral images of the skeletal system of a patient in a standing or sitting position, using approximately one-third of the radiation than traditional X-rays or CT scans.20,27
Finally, intra-operative 3D navigation-guided surgery can be used for a variety of spinal procedures, particularly in scoliosis cases where anatomical landmarks are not readily accessible.28,29 The ability to place pedicle screws more accurately with navigation than by freehand, not only minimizes intra-operative fluoroscopy but also the need for routine post-operative CT scans.30,31 Previous studies have shown that one intraoperative spin consisted of approximately 195 images (which is a scan length of approximately 15 cm), set at a low-dose radiation scan (approximately a mean of 207 mGycm, 3.1 mSv).32
This is one of the first papers documenting the estimated cumulative radiation dose that AIS patients receive through their clinical course. A recent study by Meta et al explored radiation dose for both children and adults undergoing spinal deformity treatment; they reported a higher effective radiation dose and estimated risk of cancer in those treated surgically.33 Similarly, we hope that this will encourage further research that will look for ways to minimize radiation exposure and guide treatment in the AIS patient population.
Ethical/Copyright Corrections
This manuscript complies with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors have no conflicts of interest to declare with respect to the research, authorship, and/or publication of this article.
References
1. Horne JP, Flannery R, Usman S. Adolescent idiopathic scoliosis: diagnosis and management. Am Fam Physician. 2014;89(3):193–198.
2. Müller M. Secretion of acid hydrolases and its intracellular source in Tetrahymena pyriformis. J Cell Biol. 1972;52(2):478–487. doi:10.1083/jcb.52.2.478
3. Hicks JM, Singla A, Shen FH, Arlet V. Complications of pedicle screw fixation in scoliosis surgery: a systematic review. Spine. 2010;35(11):465–470. doi:10.1097/BRS.0b013e3181d1021a
4. Nash CL, Gregg EC, Brown RH, Pillai K. Risks of exposure to X-rays in patients undergoing long-term treatment for scoliosis. J Bone Joint Surg Am. 1979;61(3):371–374. doi:10.2106/00004623-197961030-00009
5. Presciutti SM, Karukanda T, Lee M. Management decisions for adolescent idiopathic scoliosis significantly affect patient radiation exposure. Spine J. 2014;14(9):1984–1990. doi:10.1016/j.spinee.2013.11.055
6. Pace N, Ricci L, Negrini S. A comparison approach to explain risks related to X-ray imaging for scoliosis, 2012 SOSORT award winner. Scoliosis. 2013;8(1):11. doi:10.1186/1748-7161-8-11
7. Kluba T, Schäfer J, Hahnfeldt T, Niemeyer T. Prospective randomized comparison of radiation exposure from full spine radiographs obtained in three different techniques. Eur Spine J. 2006;15(6):752–756. doi:10.1007/s00586-005-1005-4
8. Dutkowsky JP, Shearer D, Schepps B, Orton C, Scola F. Radiation exposure to patients receiving routine scoliosis radiography measured at depth in an anthropomorphic phantom. J Pediatr Orthop. 1990;10(4):532–534. doi:10.1097/01241398-199010040-00021
9. McArthur N, Conlan DP, Crawford JR. Radiation exposure during scoliosis surgery: a prospective study. Spine J. 2015;15(3 Suppl):S33–36. doi:10.1016/j.spinee.2014.12.149
10. Jones DP, Robertson PA, Lunt B, Jackson SA, Jackson SA. Radiation exposure during fluoroscopically assisted pedicle screw insertion in the lumbar spine. Spine. 2000;25(12):1538–1541. doi:10.1097/00007632-200006150-00013
11. Perisinakis K, Theocharopoulos N, Damilakis J, et al. Estimation of patient dose and associated radiogenic risks from fluoroscopically guided pedicle screw insertion. Spine. 2004;29(14):1555–1560. doi:10.1097/01.BRS.0000131214.57597.21
12. Simony A, Hansen EJ, Christensen SB, Carreon LY, Andersen MO. Incidence of cancer in adolescent idiopathic scoliosis patients treated 25 years previously. Eur Spine J. 2016;25(10):3366–3370. doi:10.1007/s00586-016-4747-2
13. Bone CM, Hsieh GH. The risk of carcinogenesis from radiographs to pediatric orthopaedic patients. J Pediatr Orthop. 2000;20(2):251–254. doi:10.1097/01241398-200003000-00023
14. Khong PL, Ringertz H, Donoghue V, et al. ICRP publication 121: radiological protection in paediatric diagnostic and interventional radiology. Ann ICRP. 2013;42(2):1–63. doi:10.1016/j.icrp.2012.10.001
15. Mathews JD, Forsythe AV, Brady Z, et al. Cancer risk in 680,000 people exposed to computed tomography scans in childhood or adolescence: data linkage study of 11 million Australians. BMJ. 2013;346–360. doi:10.1136/bmj.f2360
16. Zwack LM, McCarthy WB, Stewart JH, McCarthy JF, Allen JG. Radiation dose to workers due to the inhalation of dust during granite fabrication. J Radiol Prot. 2014;34(1):51–62. doi:10.1088/0952-4746/34/1/51
17. Law M, Ma WK, Lau D, Chan E, Yip L, Lam W. Cumulative radiation exposure and associated cancer risk estimates for scoliosis patients: impact of repetitive full spine radiography. Eur J Radiol. 2016;85(3):625–628. doi:10.1016/j.ejrad.2015.12.032
18. Levy AR, Goldberg MS, Mayo NE, Hanley JA, Poitras B. Reducing the lifetime risk of cancer from spinal radiographs among people with adolescent idiopathic scoliosis. Spine. 1996;21(13):1540–1548. doi:10.1097/00007632-199607010-00011
19. Luo TD, Stans AA, Schueler BA, Larson AN. Cumulative radiation exposure with EOS imaging compared with standard spine radiographs. Spine Deform. 2015;3(2):144–150. doi:10.1016/j.jspd.2014.09.049
20. Newton PO, Khandwala Y, Bartley CE, Reighard FG, Bastrom TP, Yaszay B. New EOS imaging protocol allows a substantial reduction in radiation exposure for scoliosis patients. Spine Deform. 2016;4(2):138–144. doi:10.1016/j.jspd.2015.09.002
21. Hui SCN, Pialasse J-P, Wong JYH, et al. Radiation dose of digital radiography (DR) versus micro-dose x-ray (EOS) on patients with adolescent idiopathic scoliosis: 2016 SOSORT- IRSSD “John Sevastic Award” Winner in Imaging Research. Scoliosis Spinal Disord. 2016;11:46. doi:10.1186/s13013-016-0106-7
22. Melhem E, Assi A, El Rachkidi R, Ghanem I. EOS® biplanar X-ray imaging: concept, developments, benefits, and limitations. J Child Orthop. 2016;10(1):1–14. doi:10.1007/s11832-016-0713-0
23. Rehm J, Germann T, Akbar M, et al. 3D-modeling of the spine using EOS imaging system: inter-reader reproducibility and reliability. PLoS One. 2017;12(2):e0171258. doi:10.1371/journal.pone.0171258
24. Dubousset J, Charpak G, Dorion I, et al. A new 2D and 3D imaging approach to musculoskeletal physiology and pathology with low-dose radiation and the standing position: the EOS system. Bull Acad Natl Med. 2005;189(2):287–297.
25. Johnson N. Imaging, navigation, and robotics in spine surgery. Spine. 2016;41(Suppl 7):S32. doi:10.1097/BRS.0000000000001437
26. Rienmüller A, Buchmann N, Kirschke JS, et al. Accuracy of CT-navigated pedicle screw positioning in the cervical and upper thoracic region with and without prior anterior surgery and ventral plating. Bone Joint J. 2017;99-B(10):1373–1380. doi:10.1302/0301-620X.99B10.BJJ-2016-1283.R1
27. Chan A, Parent E, Narvacan K, San C, Lou E. Intraoperative image guidance compared with free-hand methods in adolescent idiopathic scoliosis posterior spinal surgery: a systematic review on screw-related complications and breach rates. Spine. 2017;17(9):1215–1229. doi:10.1016/j.spinee.2017.04.001
28. Allam Y, Silbermann J, Riese F, Greiner-Perth R. Computer tomography assessment of pedicle screw placement in thoracic spine: comparison between free hand and a generic 3D-based navigation technique. Eur Spine J. 2013;22(3):648–653. doi:10.1007/s00586-012-2505-7
29. Su AW, Luo TD, McIntosh AL, et al. Switching to a pediatric dose O-arm protocol in spine surgery significantly reduced patient radiation exposure. J Pediatric Orthop. 2016;36(6):621–626. doi:10.1097/BPO.0000000000000504
30. Mehta JS, Hodgson K, Yiping L, et al. Radiation exposure during the treatment of spinal deformities. Bone Joint J. 2021;103-B(4):1–7. doi:10.1302/0301-620X.103B.BJJ-2020-1416.R3
31. Seibert JA, Morin RL. The standardized exposure index for digital radiography: an opportunity for optimization of radiation dose to the pediatric population. Pediatr Radiol. 2011;41(5):573–581. PMID: 21491197; PMCID: PMC3076558. doi:10.1007/s00247-010-1954-6
32. Schauer DA, Linton OW. NCRP Report No. 160, Ionizing Radiation Exposure of the Population of the United States, medical exposure--are we doing less with more, and is there a role for health physicists? Health Phys. 2009;97(1):1–5. doi:10.1097/01.HP.0000356672.44380.b7
33. National Council on Radiation Protection and Measurements: medical radiation exposure of patients in the United States. NCRP Report No. 184.2019. Bethesda, Maryland: National Council on Radiation Protection and Measurements; 2019.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.