Back to Journals » Breast Cancer: Targets and Therapy » Volume 17
Radiation-Based Multi-Modal Therapy Combining with Immunotherapy to Develop a Vaccine-Like Effective Treatment for Triple-Negative Breast Cancer
Authors Dai M, Tian Z, Xu F, Yao B, Liang H, Li D, Wang J, Rong J, Liu T, Tang H, Lu H ![]() , Zhang W
, Zhang W
Received 21 January 2025
Accepted for publication 21 May 2025
Published 10 June 2025 Volume 2025:17 Pages 483—496
DOI https://doi.org/10.2147/BCTT.S518625
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Robert Clarke
Mengyan Dai,1,2,* Zuhong Tian,2,3,* Fanyuan Xu,2 Bang Yao,2,4 Hongxia Liang,1,2 Dongyan Li,1,2 Jiangang Wang,5 Junyan Rong,2 Tianshuai Liu,2 Haili Tang,5 Hongbing Lu,2 Wenli Zhang2
1The College of Life Sciences, Northwest University, Xi’an City, 710069, People’s Republic of China; 2School of Biomedical Engineering, Shaanxi Provincial Key Laboratory of Bioelectromagnetic Detection and Intelligent Perception, The Fourth Military Medical University, Xi’an, Shaanxi, 710032, People’s Republic of China; 3State Key Laboratory of Holistic Integrative Management of Gastrointestinal Cancers and Xijing Hospital of Digestive Diseases, Fourth Military Medical University, Xi’an, 710032, People’s Republic of China; 4School of Materials Science and Engineering, Shaanxi University of Science and Technology, Xi’an, Shaanxi, 710021, People’s Republic of China; 5Department of General Surgery, The Second Affiliated Hospital of the Fourth Military Medical University, Xi’an, 710038, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wenli Zhang, School of Biomedical Engineering, The Fourth Military Medical University, 169th Changle West Road, Xi’an, Shaanxi, 710032, People’s Republic of China, Email [email protected] Hongbing Lu, School of Biomedical Engineering, The Fourth Military Medical University, 169th Changle West Road, Xi’an, Shaanxi, 710032, People’s Republic of China, Email [email protected]
Background: Triple-negative breast cancer (TNBC) is an aggressive malignancy with high metastasis and recurrence rates. Current treatments like chemotherapy and immunotherapy face challenges due to chemotherapy side effects, limited immunotherapy applicability, and TNBC’s immunosuppressive microenvironment.
Purpose: To achieve a more effective treatment for TNBC, a novel therapeutic strategy has been developed, which uses X-ray excited photodynamic therapy (X-PDT) to activate the tumor immune microenvironment following with the immunotherapy of Anti-CTLA4.
Methods: Base on the 4T1 tumor mouse model, this study initially investigated the regulatory effects of X-PDT on the tumor immune microenvironment. Subsequently, the therapeutic efficacy of combining X-PDT with Anti-CTLA4 was evaluated for its inhibitory effects on primary, metastatic, and recurrent tumors. The underlying mechanisms were further elucidated through comprehensive techniques including flow cytometry, ELISA, and immunofluorescence assays.
Results: The synergistic strategy can effectively ablate the primary tumor while inhibiting metastasis and preventing recurrence like a vaccine. It enhances intratumoural dendritic cells (DCs) maturation (from 25.7% to 58.3%, P < 0.05) and immune T cell infiltration activating a strong anti-tumor immune response. The anti-tumor efficacy of synergistic therapy is enhanced by 2.5 times comparing with immunotherapy alone, while the tumor metastasis has been inhibited significantly. The maturation level of mature dendritic cells was increased from 26.7% to 86.3% (P < 0.01). The intratumoural CD8+/CD4+ T cells were increased from 0.51% and 1.54% to 15.4% and 23.1% (P < 0.0001), respectively. The synergistic therapy exerts a powerful vaccine-like long-term immune memory function to prevent tumor recurrence with the elevated level of effector memory T (Tem) cells (from 12.8% to 33.3%, P < 0.05).
Conclusion: Based on the 4T1 mouse model, developed an effective vaccine-like therapeutic strategy combining X-PDT with Anti-CTLA4, which can effectively ablate tumors, inhibit metastasis, and prevent tumor recurrence. This work may provide a novel effective therapeutic modality for the clinical treatment of TNBC.
Keywords: combination therapies, cancer vaccine, X-ray excited photodynamic therapy, immunotherapy, nanodrugs
Introduction
In 2022, the global incidence of new breast cancer cases reached 2.31 million, representing nearly one-fourth of all female cancer diagnoses. The mortality attributed to breast cancer was 666,000, constituting approximately 15.4% of total cancer deaths in women.1,2 Breast cancer can be categorized into four subtypes: Luminal A, Luminal B, human epidermal growth factor receptor 2 (HER-2) overexpressing, and Triple Negative Breast Cancer (TNBC).3 TNBC exhibits insensitivity to both endocrine and targeted therapies due to the negative of estrogen receptor (ER), progesterone receptor (PR), and HER-2 expression. This subtype is characterized by high malignancy, a propensity for metastasis, frequent recurrence, and an overall poor prognosis.4–6 At present, the standard clinical interventions for TNBC predominantly include surgical resection, radiotherapy (RT), and systemic chemotherapy. However, the emergence of drug resistance frequently results in recurrence and metastasis of TNBC.7
Immune checkpoint inhibitors (ICIs) are a class of anticancer drugs that activate the immune system by blocking immune checkpoint molecules, thereby enhancing its ability to attack tumor cells. The introduction of ICIs has generated significant optimism for TNBC patients and represents a focal point in the field of immunotherapy.8 Currently, the ICIs approved for clinical use primarily including Anti-CTLA4, Anti-PD-1, and Anti-PD-L1 agents. Notably, Anti-PD-1 has been utilized as an adjuvant therapy for TNBC, and reduced the mortality rate by 34% successfully.9,10 In a concurrent trial assessing the combination of PD-L1/CTLA-4 dual antibodies with albumin-bound paclitaxel in advanced TNBC, the objective response rate and clinical benefit rate were reported at 44% and 52%,11 this regimen has received FDA approval to proceed to a Phase II clinical trial in the United States.12 Although ICIs have shown some progress, only a small proportion of TNBC patients are suitable for ICIs therapy and it is not effective in suppressing the metastasis and recurrence of TNBC,5 because TNBC is characterized as a “cold” tumor with low immunogenicity.13–15 The immunosuppressive microenvironment of TNBC significantly limits the efficacy of ICIs.16,17 It is essential to develop therapeutic strategies that enhance the immunogenicity of TNBC, reduce drug resistance, and effectively inhibit metastasis and recurrence.
Photodynamic therapy (PDT), which relies on the generation of reactive oxygen species (ROS) via light-activated photosensitizers to eradicate tumor cells, offers significant advantages, including reduced toxicity and fewer side effects compared to multi-drug chemotherapy, as well as the notable absence of drug resistance, which has shown advantages in tumor management, such lung cancer, bladder cancer and esophageal carcinoma.18,19 Research indicates that PDT can directly induce cytotoxicity in tumor cells, augment tumor immunogenicity, and activate anti-tumor immune responses.20 PDT could effectively target local primary tumors, combat metastatic tumors, and prevent tumor recurrence in the conjunction with immunotherapy.21,22 However, PDT encounters the challenge of limited penetration depth of the excitation light source.23 X-ray excited photodynamic therapy (X-PDT) addresses this limitation by utilizing X-rays, commonly employed in radiotherapy, as the excitation “light” source. This approach is considered as a combination therapy of radiotherapy (RT) and PDT, demonstrating significant potential in enhancing tumor immunogenicity and activating anti-tumor immune responses by producing tumor-associate agents from ablated tumor cell residues.24–26 Given the propensity of TNBC to metastasize and recurrence, our research has demonstrated that X-PDT effectively inhibits the migration and invasion of 4T1 tumor cells, as well as the lung metastasis of 4T1 tumors, by impeding the epithelial-mesenchymal transition (EMT) process.27 However, there remains a certain risk of recurrence.28 X-PDT is anticipated to function as a “vaccine-like” in conjunction with ICIs Anti-CTLA4, and thus improve the immune microenvironment of TNBC, achieving an effective synergistic therapeutic effect as well as inhibiting the metastasis and recurrence.
Thus, we constructed 4T1 mouse tumor models and using NaYF4-based nanoparticles, which possess ultra-strong X-ray excited optical luminescence (XEOL),29 as the X-ray to light energy transducer unit, coupling with FDA-approved photosensitizer Rose Bengal for efficient X-PDT. To identify if X-PDT could trigger anti-tumor immune responses, the proportion of intratumoural dendritic cells (DCs) maturation as well as infiltrating CD8+ T cell were quantified first by flowcytometry as well as immunofluorescence. On this basis, a synergistic treatment combining X-PDT and Anti-CTLA4 was performed to investigate the effectiveness of primary tumor suppression and metastasis inhibition. To investigate the mechanism of effective therapeutic outcomes achieved by the synergistic therapy, by flowcytometry, immunofluorescence as well as ELISA, DCs in the tumor-draining lymph nodes, tumor infiltrated CD8+/CD4+ T cells, regulatory T(Treg) cells expression, the expression levels of TNF-α and IL12-p70 was quantified. To identify the vaccine-like efficacy of the synergistic therapy upon tumor rechallenging, a distant tumor was inoculated 30 days post-treatment, and the tumor growth and effector memory T (Tem) cells were monitored and quantified.
It was found that this combination strategy elevated dendritic cells in the tumor-draining lymph nodes of 4T1 mice by 3 times, and the intratumourally infiltrated CD8+/CD4+ T cells by 30/15 times, and effectively suppressed the Treg cells expression and elevated the secretion levels of TNF-α and IL12-p70 by 3/6 times. In addition, we found that X-PDT combined with Anti-CTLA4 significantly reduced the number of lung metastases in 4T1 mice. Additionally, X-PDT achieved excellent anti-tumor effects in the face of tumor re-challenge, demonstrated an excellent vaccine-like immune memory effect, and in combination with Anti-CTLA4, this vaccine-like function was even more effectively boosted, which was able to efficiently protect the organism from tumor recurrence.
Materials and Methods
Cell Culturing
Mouse mammary carcinoma 4T1 cells were obtained from the Cell Bank of the Chinese Academy of Sciences. The cell lines were cultured in Dulbecco’s modified Eagle’s medium high glucose (DMEM-high glucose, D5796, Sigma‒Aldrich) supplemented with 10% fetal bovine serum (FBS, 100941C, Gibco) and 5% penicillin‒streptomycin (P1400, Solarbio, Beijing) at 37 °C with 5% CO2 and 95% humidity. Cells were passaged when they reached 70–80% confluence. The cells were passaged using 0.25% trypsin-EDTA (T1300, Solarbio).
Tumor Animal Models
All animals were provided by the Animal Center of the Fourth Military Medical University. All animal experiments were approved by the Animal Experiment Administration Committee of the Fourth Military Medical University and were carried out in accordance with the National Institutes of Health Guide for the Care and Use of Laboratory Animals. The hair of female Balb/c mice aged 6–8 weeks was shaved off the right lower limb. A mouse model of breast cancer was established by subcutaneously injecting 3×106 4T1 cells. The mice were kept under a 12 h light/dark cycle. The tumor volume was calculated according to the following formula:

In vivo X-PDT Therapy and Immunotherapy Treatment
When the tumor size reached 70–100 mm3, random block grouping was performed. 100 μL of PBS was injected into the NC group, while 100 μL of 10 mg/mL of NaYF4: 10%Tb3+@NaYF4 NPs@AEP-RB solution was intratumorally injected in the NPs-RB group and the X-PDT groups. After 12 h, for the X-PDT and RT groups, the tumor was exposed to X-rays, and the rest of the body was shielded by a 3 mm thick lead plate. The other groups of mice were not radiated. The weight and tumor volume of all the mice were monitored every other day beginning on the day of injection of NPs-RB (the tumor volume and mouse body weight at the time of the first X-ray irradiation were recorded as the starting data). For immunotherapy treatment, mice were i.p. injected with 10 μg Anti-CTLA4 in 100 μL PBS on day 1, 4 and 7, after their primary visible tumors were removed by X-PDT. Anti-CTLA4 used in vivo was obtained from Bioxcell. Three mice from each group were euthanized to evaluate the anti-tumor immune response in vivo, and euthanasia was performed using CO2 asphyxiation.
Flow Cytometry Analysis
To analyze the immune cells in tumors, those tumors were harvested from mice and digested using 1500 U/mL collagenase (Sigma), 1000 U/mL hyaluronidase (Sigma) and Sigma DNase (Sigma) at 37°C for 30 min. Cells were filtered through nylon mesh filters and washed with PBS containing 2% FBS. The single cell suspension was incubated with anti-CD3-FITC (Biolegend, Clone:17A2), anti-CD8-eFluor450 (Biolegend, Clone:53–6.7), anti-CD4-PE (Biolegend, Clone: GK1.5) antibodies. Afterwards, those cells were washed with PBS containing 2% FBS and analyzed using flow cytometry analysis. To analyze the mature DCs in Tumor-draining lymph nodes, cells were filtered through nylon mesh filters and washed with PBS containing 2% FBS. The single cell suspension was incubated with anti-CD11c-FITC (Biolegend, Clone: N418), anti-CD86-APC (Lianke, Clone:GL-1), anti-CD80-PE (Lianke, Clone:6–10A1) antibodies. To analyze Tem cells, spleen cells harvested from mice after various treatment were stained with anti-CD3-FITC (Biolegend, Clone:17A2), anti-CD8-eFluor450 (Biolegend, Clone:53–6.7), anti-CD62L- PerCP/Cyanine5.5 (Biolegend, Clone: MEL-14) and anti-CD44-PE (Lianke, Clone:IM7) antibodies. Data analysis was carried out by using FlowJo V10.8.1 software.
Cytokine Detection
Serum samples were isolated from mice after various treatments and diluted for analysis. TNF-α and IL-12p70 were analyzed with ELISA kits according to vendors’ protocols.
Histological Examinations
For H&E staining, the heart, liver, spleen, lungs, kidneys, and tumor were fixed in 4% paraformaldehyde (BL539A, Biosharp, Beijing) for 48 h and embedded in paraffin. Then, the paraffin sections were stained with H&E and imaged under an inverted fluorescence microscope (CKX53, Olympus, Guangzhou).
TUNEL and Ki67 staining were performed by IF staining. TUNEL assay was performed by TUNEL labeling kit (11684817910, Roche, Basel, Switzerland) according to manufactures instruction. Ki67 positive cells were stained by Alexafluo594 labeled Ki-67 (D3B5) Rabbit mAb (#9129, CST, Boston, USA).
All slides were scanned by using Pannoramic-250 Flash II slide-scanner (3D-Histech, Budapest, Hungary) and analyzed by Case viewer software (3D-Histech, Budapest, Hungary). The TUNEL apoptotic index and Ki67 proliferation index were calculated by quantifying the ratio of the fluorescence intensity of positive cells to the area of total cells.
Statistical Analysis
GraphPad Prism 8 (GraphPad Software, San Diego, CA, USA) was used for all data analyses and for graph plotting. Multiple groups were compared using one-way analysis of variance (one-way ANOVA) with Tukey’s multiple comparison test, and tumor growth curves were analyzed using two-way analysis of variance (two-way ANOVA). Quantitative results are expressed as the mean ± SEM. A threshold of P < 0.05 was considered to indicate statistical significance, and further confidence is indicated by asterisks (*P < 0.05; **P < 0.01; ***P < 0.001; ****P < 0.0001).
Results
X-PDT Promotes Intratumoural Dendritic Cell Maturation and CD8+ T Cell Infiltration
To investigate whether X-PDT could trigger anti-tumor immune responses, we performed X-PDT treatment by constructing a 4T1 subcutaneous loaded tumor model of female Balb/c mice (Figure 1a and b), which was divided into a negative control (NC) group that did not receive any treatment, an RT group that was irradiated with X-rays only, and an X-PDT treatment, followed by close monitoring of the health status of the mice. Tumor tissues were harvested after five days of X-PDT, and single-cell suspensions of tumor tissues as well as tumor sections were prepared. The maturation level of DCs (CD11c+, CD86+, and CD80+) in the tumors, as one of the most important classes of antigen-presenting, was quantified by flowcytometry (The flow lap-gate program for mature DCs is show in the Figure S1), as well as the infiltration of intratumor CD8+ T cells by immunofluorescent (IF) microscopy. As shown in Figure 1c and e, the statistical analysis of the flowcytometry results as well as their quantitative results showed that there was no significant difference of the mature DCs in tumors between the NC and RT groups, whereas the maturation level in the tumors of the X-PDT-treated mice was increased significantly (from 25.7% to 58.3%, P < 0.05). The infiltration of intratumor CD8+ T cells, which was quantified by IF, showed only a few CD8+ T cells infiltrating the tumor in the NC group and the RT group (Figure 1d and f), which demonstrated that the immunogenicity of 4T1 tumors was poor. On the other hand, the infiltration of CD8+ T cells in X-PDT-treated tumors was significantly increased comparing which in the NC and RT groups (P < 0.01). The elevated maturation level of DCs and the increase of infiltrating CD8+ T cells in tumors indicated that X-PDT could indeed trigger anti-tumor immune responses and manipulate the tumor immune microenvironment.
 |
Figure 1 X-PDT’s immune-stimulation abilities. (a and b) Schematic of X-PDT treatment; (c and e) Quantification of maturation levels of intratumoral dendritic cells (n=3; *, P < 0.05); (d) Immunofluorescence images of CD8 expression in the tumor (DAPI, blue; CD8+ T cells, green; scale bar: 50 μm); (f) Semi-quantitative analysis of immunofluorescence results from c (n=3-5; *, P < 0.05; **, P < 0.01). All data is reported as the means ± SEM. |
X-PDT Plus Anti-CTLA4 Blockade Inhibits Tumor Growth and Metastatic
On the basis of X-PDT activating anti-tumor immune response, the in vivo tumor suppression effect of X-PDT combining with the immune checkpoint inhibitor Anti-CTLA4 treatment was investigated (Figure 2a). Firstly, Balb/c mice-bearing subcutaneous 4T1 tumors were divided into the following groups: (1) NC, (2) RT, (3) X-PDT, (4) Anti-CTLA4, (5) RT+Anti-CTLA4, and (6) X-PDT+Anti-CTLA4. Tumor size was monitored closely one day before treatment, and then tumor size and body weight of mice were monitored every two days. As illustrated in Figure 2b and c and Figure S2, the synergistic treatment of X-PDT combining with Anti-CTLA4 demonstrated a robust tumor-suppressing effect comparing with all other treatment groups (P < 0.01). Both the RT+Anti-CTLA4 and X-PDT treatment groups showed better tumor suppression effects comparing with NC, RT, and Anti-CTLA4 groups (P < 0.01), which also side by side showed the advantages of X-PDT treatment comparing with RT. Meanwhile, the Anti-CTLA4 group showed a trend of rapid tumor growth after eight days of treatment, indicating that the therapeutic effect of Anti-CTLA4 alone was not satisfactory (P > 0.05), while the combination treatment with X-PDT or RT could achieve better tumor suppression effect due to the immune system activation by X-PDT. On the 14th day after treatment, the tumor tissues were harvested for H&E, TUNEL and Ki67 staining (Figure 2d–f). The H&E staining outcomes revealed that all treatment groups effectively suppressed tumor cell growth to varying degrees, causing nuclear crumpling. Notably, the combined treatment groups and the X-PDT group demonstrated more pronounced tumor destruction, suggesting a heightened anti-tumor efficacy among these three groups. The TUNEL staining results indicated a more pronounced enhancement of DNA damage and apoptosis in tumor cells within the X-PDT+Anti-CTLA4 group, which notably accelerated the apoptotic process of tumor cells (P < 0.0001). Ki67 staining results showed that the X-PDT+Anti-CTLA4 group and RT+Anti-CTLA4 group had a robust ability to inhibit tumor proliferation, and X-PDT also showed a better tumor proliferation inhibition ability comparing with NC, RT and Anti-CTLA4 groups (P < 0.0001). Meanwhile, we performed H&E staining of the heart, liver, spleen, and kidney of the mice (Figure S3), and the staining results did not show any obvious tissue damage and lesions, and the body weight of the mice remained stable during the monitoring period (Figure S4), suggesting that the therapeutic strategy of X-PDT based on NaYF4: 10% Tb@NaYF4-RB and the immune checkpoint inhibitor Anti-CTLA4 has a bravo biosafety.
 |
Figure 2 Anti-tumor effects of X-PDT combining with Anti-CTLA4 treatment in Balb/c mice-bearing subcutaneous 4T1 tumors. (a) Schematic of X-PDT plus Anti-CTLA4 combination therapy; (b) Tumor growth curve (*, P < 0.05; **, P < 0.01); (c) Tumor weight (*, P < 0.05; **, P < 0.01; ****, P < 0.0001); (d) Tumor H&E, TUNEL and Ki-67 staining images (scale bar: 100 μm); (e and f) TUNEL and Ki-67 staining statistical analysis (*, P < 0.05; **, P < 0.01; ****, P < 0.0001). The data are reported as the means ± SEM of n=8-10 (a–c) and n=3 (e and f) independent experiments. |
To gain deeper insights into the therapeutic efficacy of X-PDT and Anti-CTLA4 synergistic treatment in suppressing metastatic tumor progression, we established a 4T1-derived metastatic tumor model (Figure 3a), leveraging the inherent propensity of 4T1 tumors to metastasize to the lungs. On day 14, we collected lung tissues from each group for photographing as well as H&E staining (Figure 3c). The presence of lung metastatic foci was evident and prominent in the NC group, as well as in the RT group and the Anti-CTLA4 group (P > 0.05). However, the X-PDT group, Anti-CTLA4 group, and RT+Anti-CTLA4 group were able to inhibit lung metastasis (P < 0.05), although large lung nodules still appeared. The X-PDT+Anti-CTLA4 synergistic treatment significantly inhibited the lung metastasis of 4T1 tumors, and the average number of lung metastatic sites (P < 0.01) (Figure 3b), suggesting that the synergistic therapy could effectively inhibit the metastatic tumors of 4T1.
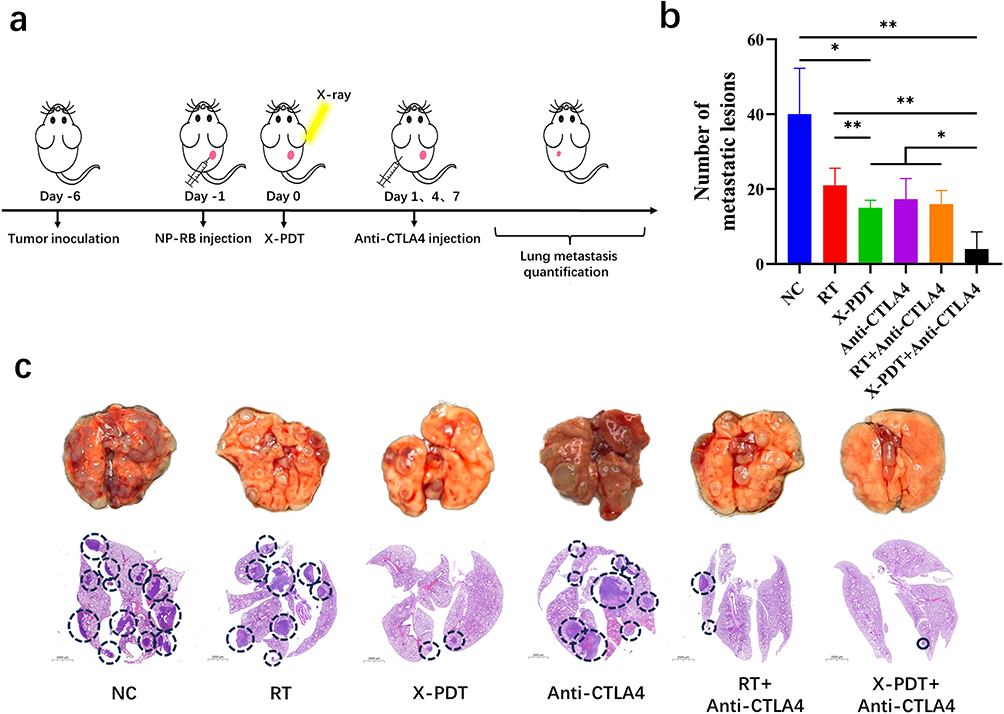 |
Figure 3 Inhibitory effect on lung metastasis. (a) Schematic diagram of lung metastasis evaluation; (b) The statistic results of metastatic foci in the lungs (*, P < 0.05; **, P < 0.01); (c) Representative white light images of the lungs and H&E staining of lungs (The circled sections indicate the locations of metastatic lesions). Data were reported as means ± SEM of n=8-10 (a) and n=3 (b and c) independent experiments. |
The Anti-Tumor Mechanism Investigation of X-PDT Combined with the Immunotherapy
DCs are the most powerful type of cells in the body for antigen presentation, presenting tumor antigens and initiating T cell-mediated adaptive immune responses, which in turn activate the body’s anti-tumor immune response. And the hallmark of DCs maturation is the upregulation of co-stimulatory molecules (CD86+ and CD80+) (Figure 4a and c). The tumor-draining lymph nodes were investigated after 14 days of treatment and quantified the expression of mature DCs by flowcytometry. The flow lap-gate scheme for mature DCs in tumor-draining lymph nodes was shown in the Figure S5. The proportion of DCs maturation in the X-PDT+Anti-CTLA4 group was significantly elevated to 86.3%, surpassing all other groups by a notable margin, which in turn activates T cells to boost immune responses (P < 0.01). The maturation rate of DCs in the X-PDT group (61.9%) demonstrated a comparable level to that of the RT+Anti-CTLA4 group (68.1%) (P > 0.05), underscoring the immune-stimulatory potential of X-PDT.
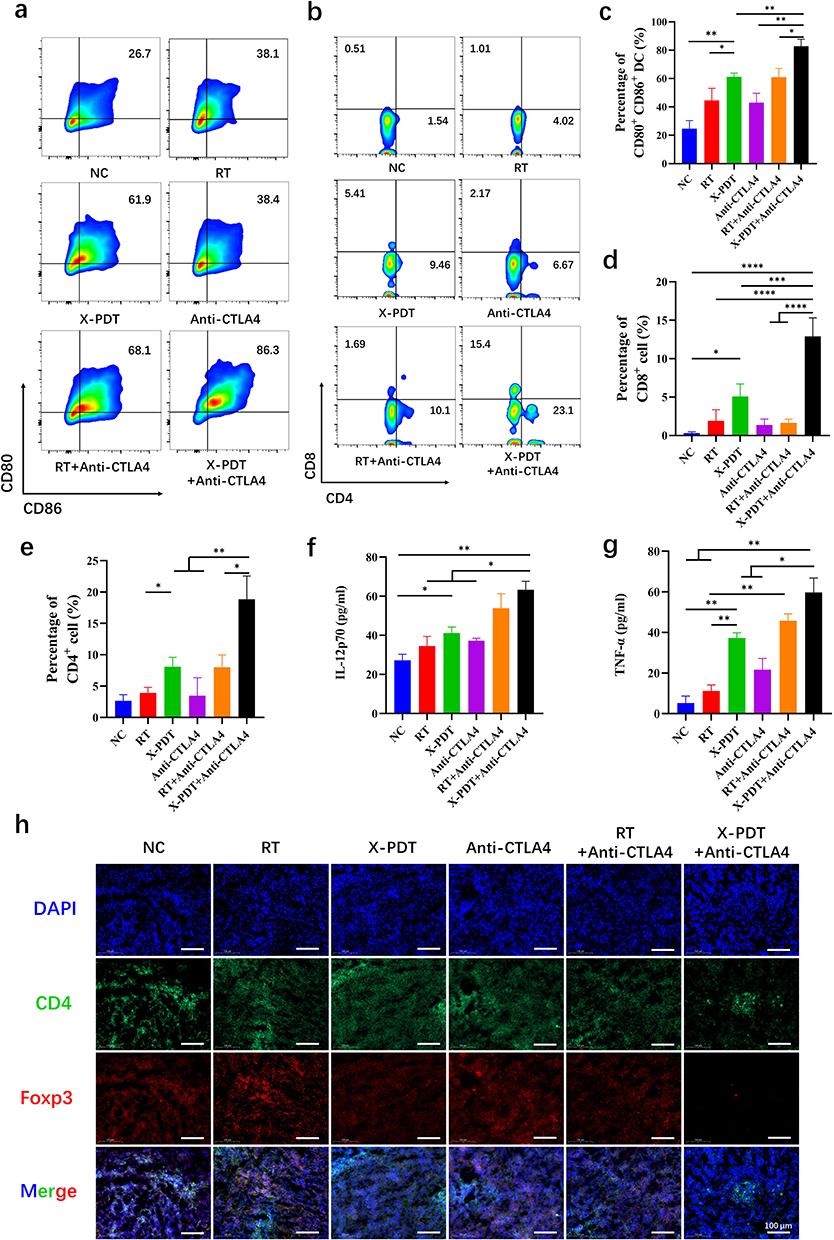 |
Figure 4 The mechanism study. (a and c) Flowcytometry quantification of DCs maturation in tumor-draining lymph nodes (*, P < 0.05; **, P < 0.01); (b, d and e) Flowcytometry quantification of intratumoral CD8+/CD4+ T cell infiltration (*, P < 0.05; **, P < 0.01; ****, P < 0.0001); (f and g) Monitoring of cytokine levels in serum (*, P < 0.05; **, P < 0.01); (h) Immunofluorescence images of intratumoral Treg cells expression (Scale bar: 100 μm). Data were reported as means ± SEM of n=3 (a, b, f and g) independent experiments. |
The key to the generation of the tumor immune response was the proportion of immune cells, mainly cytotoxic T cells (CD3+ and CD8+) as well as the proportion of helper T cells (CD3+ and CD4+) (Figure 4b, d and e). The proportion of CD8+ and CD4+ T cells infiltrating in tumors were quantified by flowcytometry (Figure S6). The proportion of CD8+ T cells in the NC group was as low as 0.51%, which indicated the low immunogenicity of the 4T1 tumors. The proportions of CD8+ T cells in both the RT group (1.01%) and the Anti-CTLA4 group (2.17%) were marginally increased in comparison to the NC group (0.51%), implying that the immune response triggered solely by RT or Anti-CTLA4 therapy was relatively feeble (P > 0.05). The X-PDT group significantly increased the proportion of tumor-infiltrating CD8+ T cells to 5.41%, while also elevating the proportion of CD4+ T cells from 1.54% to a notable 9.46%, when compared to the NC group (P < 0.01). The RT+Anti-CTLA4 treatment group showed a weak elevation of CD8+ T cells infiltrated in the tumor (1.69%) (P > 0.05), in the contract, the proportion of CD4+ T cells was elevated from 1.54% to 10.1% (P < 0.05). Compared to the RT alone group, the combination of Anti-CTLA4 boosted the proportion of CD4+ T cells by 2 times. And the combined treatment strategy of X-PDT and Anti-CTLA4 enhanced the proportion of intratumorally infiltrating CD8+/CD4+ T cells substantially from 0.51%/1.54% to 15.4%/23.1% compared with the NC group, respectively (P < 0.0001).
Interleukin 12p70 (IL-12p70), a crucial cytokine stimulating the generation of immune-responsive T cells, is primarily secreted by dendritic cells and antigen-presenting cells, notably macrophages. The quantification of IL-12p70 is achieved through ELISA, utilizing serum samples meticulously collected from individual mouse groups.30 As demonstrated in Figure 4f, compared with the NC group, X-PDT treatment elevated the mean concentration of IL-12p70 in mouse serum from 26.6 (pg/mL) to 41 (pg/mL). And there was no statistically significant difference observed between the RT group, the Anti-CTLA4 group, and the NC group (P > 0.05). Both the RT+Anti-CTLA4 and X-PDT+Anti-CTLA4 groups significantly enhanced the levels of IL-12p70, with the X-PDT+Anti-CTLA4 treatment demonstrating the utmost efficacy (P < 0.01). Tumor Necrosis Factor-α (TNF-α) possesses the capacity to elicit inflammatory responses and directly eradicate tumor cells, thereby serving as a pivotal regulator in immune system functionality.31 As illustrating in Figure 4g, there was a slight increase in the secretion level of TNF-α in the RT group and the Anti-CTLA4 group comparing with that of NC group, whereas there was a greater increase in the X-PDT group (P < 0.01), the RT+Anti-CTLA4 group (P < 0.05), and the X-PDT+Anti-CTLA4 group, especially in the case of the X-PDT+Anti-CTLA4, where the secretion level of TNF-α increased most significantly (P < 0.01).
Since CTLA4 is mainly expressed on regulatory T (Treg) cells, which inhibit the production of immune T cells in turn suppressing anti-tumor immune responses, and is one of the main factors creating a tumor immunosuppressive microenvironment.32 We explored the expression of Treg cells (CD4+ and Foxp3+) in tumors by immunofluorescence staining of tumor sections from each group. Immunofluorescence assay results showed (Figure 4h) that X-PDT+Anti-CTLA4 treatment significantly suppressed the expression of Treg cells (CD4+Foxp3+) compared to all other groups.
Long-Term Immune Memory Effects of Synergistic Therapy
TNBC has a high recurrence rate and poor prognosis, which seriously jeopardizes patients’ lives. To investigate the potential for the synergistic treatment to act as a vaccine like in scenarios of tumor recurrence, we devised a model of tumor recurrence through the secondary inoculation of tumors on the 30th day subsequent to initial treatment. Subsequently, we closely monitored the tumor size and body weight of the mice to assess the efficacy of the treatment (Figure 5a). Illustrating in Figure 5b,c and Figure S7, the X-PDT+Anti-CTLA4 synergistic therapy showed an effective vaccine-like efficacy upon tumor recurrence (P < 0.0001). In the contract, The RT group and the Anti-CTLA4 group were both ineffective in restraining the growth of recurrent tumors (P > 0.05), whereas the combined treatment of RT+Anti-CTLA4 exhibited a notable recurrent tumor-suppressing effect. Notably, the X-PDT group demonstrated a moderate tumor suppression in the face of tumor recurrence (P < 0.05). Furthermore, H&E staining of recurrent tumor tissues revealed that the X-PDT plus anti-CTLA-4 combination group exhibited significantly larger necrotic areas compared to other treatment groups, demonstrating the potent synergistic effect of this combinatorial therapy in suppressing recurrent tumor growth (Figure S8). Mouse general body weight remained stable during the test period (Figure S9).
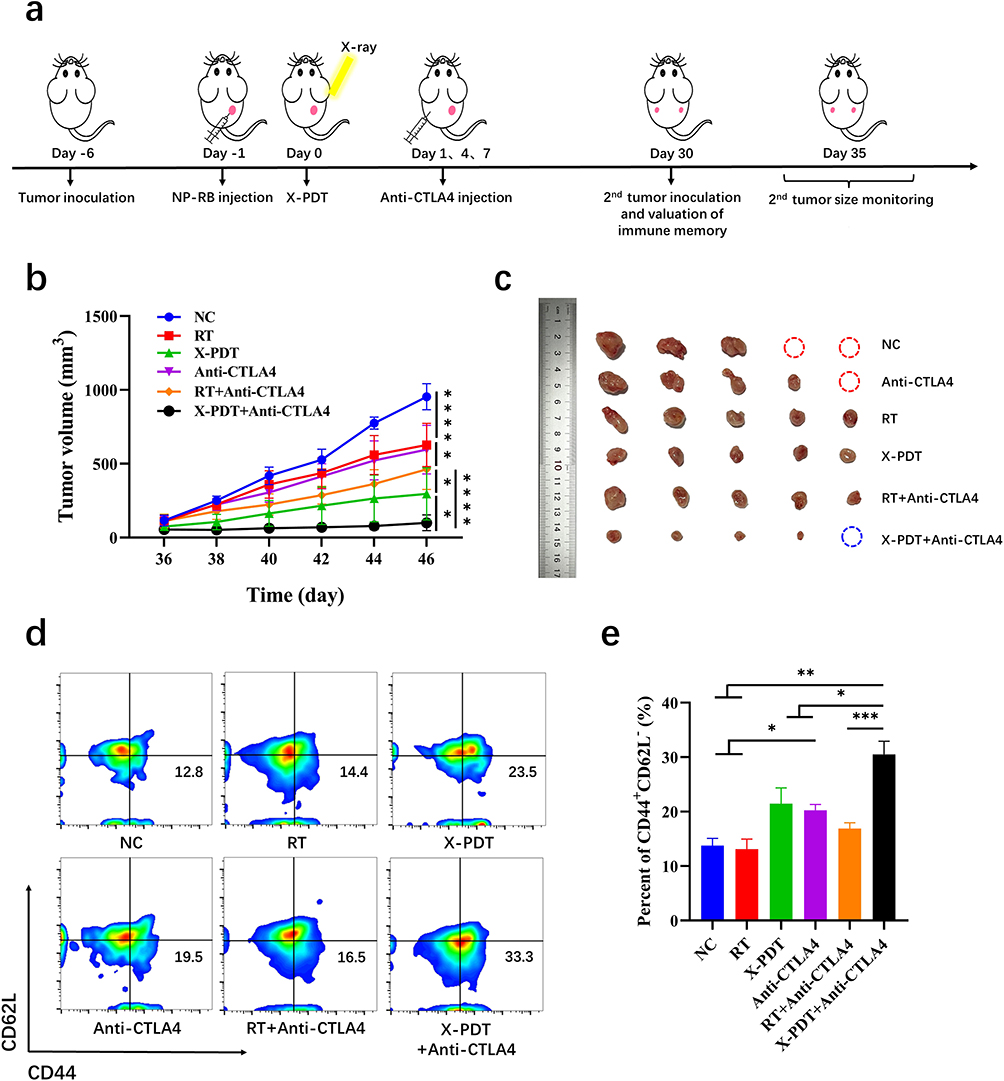 |
Figure 5 Vaccine-like immune memory effect. (a) Schematic diagram of long-term immune memory effect evaluation; (b) Recurrent tumor growth curves (*, P < 0.05; ****, P < 0.0001); (c) Photographs of mice and excised tumor after different treatments; (d and e) Expression of mouse splenic Tem cells quantified by flowcytometry as well as statistical analysis (*, P < 0.05; **, P < 0.01; ***, P < 0.001). Data were reported as means ± SEM of n=5 (a–c) and n=3 (d and e) independent experiments. |
Immune memory T cells play an important role in preventing tumor recurrence, and Tem cells can rapidly produce effector cytokines for immune protection when the body is challenged by tumor again.33,34 And we collected spleens from mice in each group at the experimental endpoint. The proportion of Tem (CD3+ CD8+ CD62L− CD44+) cells in the spleens of mice was detected by flowcytometry, the spleen Tem cells lap-gate scheme is shown in the (Figure S10). And the results showed (Figure 5d and e) that Tem cells expression in the spleens of the NC and RT groups did not differ significantly (P > 0.05), and Anti-CTLA4 treatment elevated Tem cells expression by 6.2% compared with the NC group (P < 0.05), whereas RT+Anti-CTLA4 treatment only elevated it by 3.7% (P > 0.05). X-PDT treatment was able to elevate the expression of Tem cells from 12.8 to 23.5% compared, which is consistent with the anti-tumor efficacy. Notably, X-PDT+Anti-CTLA4 treatment significantly increased Tem cells expression (33.3%), which was 2.6-fold higher compared to the NC group and 2 times higher compared to the RT+AntiCTLA4 group (P < 0.001). Meanwhile, by analyzing the survival of mice during the monitoring period (Figure S11), mice belonging to the NC group commenced dying from day 27 onwards, with the mortality count steadily escalating as time progressed. Compared to the other groups, the survival rate of mice in the X-PDT + Anti-CTLA4 treatment group was the highest.
Discussion
TNBC remains a formidable clinical challenge due to its aggressive metastasis, immunosuppressive microenvironment, and resistance to conventional therapies. The current clinical treatment approach for TNBC primarily revolves around chemotherapy coupling with immunotherapy and radiotherapy serving as supplementary therapies.35 While this integrated approach has witnessed notable advancements in inhibiting tumor growth and extending patients’ survival rates, it nonetheless confronts a myriad of challenges and limitations.36 Our study addresses two critical limitations in current TNBC treatment: (1) the immunosuppressive “cold” tumor phenotype that restricts the efficacy of ICIs such as Anti-CTLA4, and (2) the limited penetration of conventional PDT for deep-seated tumors. By synergizing X-PDT with Anti-CTLA4 immunotherapy, we demonstrate a transformative strategy that not only ablates primary tumors but also establishes systemic anti-tumor immunity to suppress metastasis and prevent recurrence.
The immunosuppressive nature of TNBC, characterized by low DCs maturation and limited cytotoxic T-cell infiltration, has caused ICIs ineffective in most patients.37 Our findings reveal that X-PDT acts as a potent in situ vaccine by generating tumor debris as endogenous antigens, which trigger DC maturation (from 25.7% to 58.3%, P < 0.05) and subsequent boosting CD8+/CD4+T-cell infiltration (30-fold and 15-fold increases, respectively; P < 0.01). This aligns with prior studies showing PDT-induced immunogenicity, but crucially, X-PDT overcomes the penetration limitations of traditional PDT through X-ray excitation, enabling deep-tumor immunomodulation compatible with clinical radiotherapy devices.38
The synergy effect between X-PDT and Anti-CTLA4 lies in their complementary mechanisms: while X-PDT activates the immune system by enhancing antigen presentation, Anti-CTLA4 alleviates immunosuppression by blocking Treg-mediated inhibition. This dual action amplifies pro-inflammatory cytokines, such as TNF-ɑ and IL-12p70 increased by 3-fold and 6-fold, and reduces Treg infiltration, achieving a 2.5-fold improvement in tumor suppression compared to monotherapy. Notably, our strategy outperformed RT+Anti-CTLA4 combinations, highlighting the unique advantage of X-PDT over conventional radiotherapy in activating adaptive immunity.
Current clinical approaches for TNBC, including PD-1/PD-L1 inhibitors and adoptive cell therapies, often face challenges such as high costs, complex manufacturing, and limited patient eligibility.25,39 Our work provides a scalable alternative: the X-PDT/Anti-CTLA4 combination leverages existing radiotherapy infrastructure and avoids the need for personalized antigen selection, addressing both accessibility and efficacy barriers. Unlike whole-cell vaccines requiring tumor resection and ex vivo processing, our in situ vaccine strategy simplifies clinical workflows while achieving comparable immune activation (86.3% DCs maturation, P < 0.01).
Moreover, the induction of long-term immune memory Tem cells increased from 12.8% to 33.3%, P < 0.05) positions this approach as a prophylactic measure against recurrence—a critical unmet need in TNBC management. The 60% reduction in lung metastasis (P < 0.01) further underscores its potential to address TNBC’s metastatic propensity, which conventional chemotherapy often fails to control.
While our murine models demonstrate compelling efficacy, translational hurdles must be addressed. The reliance on 4T1 cells, which lack the genomic heterogeneity of human TNBC subtypes, limits generalizability. Future studies should validate these findings in patient-derived xenografts and explore synergies with Anti-CTLA4 inhibitors to broaden applicability across TNBC subtypes. Additionally, optimizing X-ray dosimetry to balance ROS generation and off-target effects will be critical for clinical adoption.
Conclusion
In summary, our findings establish X-PDT combined with Anti-CTLA4 as a transformative strategy for TNBC, capable of ablating primary tumors, suppressing metastasis, and preventing recurrence through durable immune memory. The therapeutic efficacy of X-PDT combined with Anti-CTLA4 treatment in primary and metastatic tumors as well as the advantages demonstrated in the long-lasting immune memory effect can be summarized as follows (Figure 6): (1) X-PDT promotes the maturation of intra-tumor DCs from 25.7% to 58.3% and enhances the CD8+ T-cell infiltration by 3-time to promote the immunogenicity of the tumors; (2) The ICIs Anti-CTLA4 combined with X-PDT treatment can effectively inhibit Treg cells activation, promote CD8+ and CD4+ T cell infiltration by 30-fold and 15-fold, respectively, and enhance the anti-tumor immune response; (3) The Tem cells production can be effectively induced by synergistic therapy, which in turn produces a long-term immune memory effect and prevents tumor recurrence. It provides a new strategy for the clinical treatment of triple-negative breast cancer. This work paves the way for clinical trials integrating radiation-based modalities with immunotherapy to combat TNBC’s recalcitrant biology.
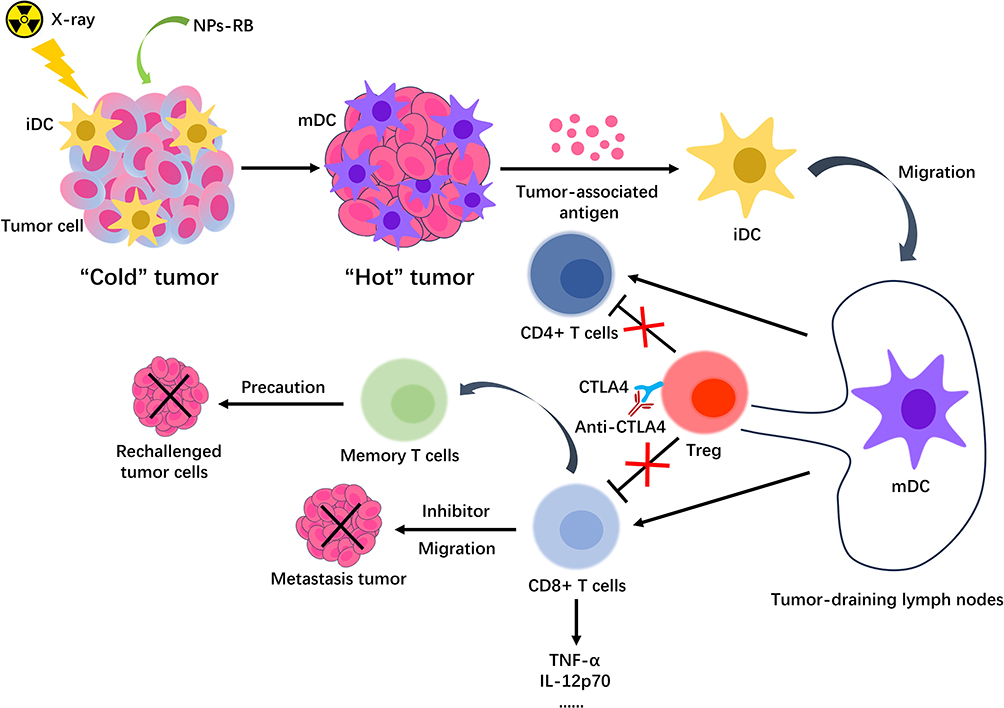 |
Figure 6 Schematic diagram of X-PDT combined with immune checkpoint blockade to induce anti-tumor immune response. |
Acknowledgments
This work was supported by National Key Research and Development Program of China (2023YFF0715400), National Natural Science Foundation of China (12275355, 12305350) and the Foundation of China (23SWAQ58-2).
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Arnold M, Morgan E, Rumgay H, et al. Current and future burden of breast cancer: global statistics for 2020 and 2040. Breast. 2022;66:15–23. doi:10.1016/j.breast.2022.08.010
3. Pareja F, Reis-Filho JS. Triple-negative breast cancers - a panoply of cancer types. Nat Rev Clin Oncol. 2018;15(6):347–348. doi:10.1038/s41571-018-0001-7
4. Karaayvaz M, Cristea S, Gillespie SM, et al. Unravelling subclonal heterogeneity and aggressive disease states in TNBC through single-cell RNA-seq. Nat Commun. 2018;9(1):3588. doi:10.1038/s41467-018-06052-0
5. Chen M, Pockaj B, Andreozzi M, et al. JAK2 and PD-L1 amplification enhance the dynamic expression of PD-L1 in triple-negative breast cancer. Clin Breast Cancer. 2018;18(5):e1205–e1215. doi:10.1016/j.clbc.2018.05.006
6. Iriondo O, Liu Y, Lee G, et al. TAK1 mediates microenvironment-triggered autocrine signals and promotes triple-negative breast cancer lung metastasis. Nat Commun. 2018;9(1):1994. doi:10.1038/s41467-018-04460-w
7. Denkert C, Liedtke C, Tutt A, et al. Molecular alterations in triple-negative breast cancer-the road to new treatment strategies. Lancet. 2017;389(10087):2430–2442. doi:10.1016/S0140-6736(16)32454-0
8. Noor ZS, Master A. Updates on targeted therapy for triple-negative breast cancer (TNBC). Curr Breast Cancer Rep. 2018;10(4):282–288. doi:10.1007/s12609-018-0291-x
9. Li Z, Qiu Y, Lu W, et al. Immunotherapeutic interventions of triple negative breast cancer. J Transl Med. 2018;16(1):147. doi:10.1186/s12967-018-1514-7
10. Cescon DW, Nowecki Z, Gallardo C, et al. Pembrolizumab plus chemotherapy versus placebo plus chemotherapy for previously untreated locally recurrent inoperable or metastatic triple-negative breast cancer (KEYNOTE-355): a randomised, placebo-controlled, double-blind, Phase 3 clinical trial. Lancet. 2020;396(10265):1817–1828. doi:10.1016/S0140-6736(20)32531-9
11. Coward J, Ganju V, Behzadigohar R, et al. Preliminary safety, efficacy, and pharmacokinetics (PK) results of KN046 (bispecific anti-PD-L1/CTLA4) from a first-in-human study in subjects with advanced solid tumors. J Clin Oncol. 2019;37(15_suppl):2554. doi:10.1200/JCO.2019.37.15_suppl.2554
12. Li Q, Liu J, Zhang Q, et al. The anti-PD-L1/CTLA-4 bispecific antibody KN046 in combination with nab-paclitaxel in first-line treatment of metastatic triple-negative breast cancer: a multicenter phase II trial. Nat Commun. 2024;15(1):1015. doi:10.1038/s41467-024-45160-y
13. Liu X, Sun M, Pu F, et al. Transforming intratumor bacteria into immunopotentiators to reverse cold tumors for enhanced immuno-chemodynamic therapy of triple-negative breast cancer. J Am Chem Soc. 2023;145(48):26296–26307. doi:10.1021/jacs.3c09472
14. Wang H, Ding XH, Liu CL, et al. Genomic alterations affecting tumor-infiltrating lymphocytes and PD-L1 expression patterns in triple-negative breast cancer. J Natl Cancer Inst. 2023;115(12):1586–1596. doi:10.1093/jnci/djad154
15. Meng M, Wu J, Feng Y, et al. A comprehensive strategy based on high clinical translational nanosystem for programmable immunotherapy of triple negative breast cancer. Adv Mater. 2024;36(27):e2314309. doi:10.1002/adma.202314309
16. Khosravi GR, Mostafavi S, Bastan S, et al. Immunologic tumor microenvironment modulators for turning cold tumors hot. Cancer Commun. 2024;44(5):521–553. doi:10.1002/cac2.12539
17. Galon J, Bruni D. Approaches to treat immune hot, altered and cold tumours with combination immunotherapies. Nat Rev Drug Discov. 2019;18(3):197–218. doi:10.1038/s41573-018-0007-y
18. Cheng Y, Cheng H, Jiang C, et al. Perfluorocarbon nanoparticles enhance reactive oxygen levels and tumour growth inhibition in photodynamic therapy. Nat Commun. 2015;6:8785. doi:10.1038/ncomms9785
19. Castano AP, Mroz P, Hamblin MR. Photodynamic therapy and anti-tumour immunity. Nat Rev Cancer. 2006;6(7):535–545. doi:10.1038/nrc1894
20. Kang X, Zhang Y, Song J, et al. A photo-triggered self-accelerated nanoplatform for multifunctional image-guided combination cancer immunotherapy. Nat Commun. 2023;14(1):5216. doi:10.1038/s41467-023-40996-2
21. Liu Z, Xie Z, Li W, et al. Photodynamic immunotherapy of cancers based on nanotechnology: recent advances and future challenges. J Nanobiotechnol. 2021;19(1):1–160. doi:10.1186/s12951-021-00903-7
22. Xu J, Xu L, Wang C, et al. Near-infrared-triggered photodynamic therapy with multitasking upconversion nanoparticles in combination with checkpoint blockade for immunotherapy of colorectal cancer. ACS Nano. 2017;11(5):4463–4474. doi:10.1021/acsnano.7b00715
23. Gao J, Chen Z, Li X, et al. Chemiluminescence in combination with organic photosensitizers: beyond the light penetration depth limit of photodynamic therapy. Int J Mol Sci. 2022;23(20):12556. doi:10.3390/ijms232012556
24. Zhang W, Zhang X, Shen Y, et al. Ultra-high FRET efficiency NaGdF(4): tb(3+)-Rose Bengal biocompatible nanocomposite for X-ray excited photodynamic therapy application. Biomaterials. 2018;184:31–40. doi:10.1016/j.biomaterials.2018.09.001
25. He L, Yu X, Li W. Recent Progress and Trends in X-ray-Induced Photodynamic Therapy with Low Radiation Doses. ACS Nano. 2022;16(12):19691–19721. doi:10.1021/acsnano.2c07286
26. Wang GD, Nguyen HT, Chen H, et al. X-ray induced photodynamic therapy: a combination of radiotherapy and photodynamic therapy. Theranostics. 2016;6(13):2295–2305. doi:10.7150/thno.16141
27. Li R, Gao P, Dai M, et al. Anticancer Effects of radiation dose and dose fractionation on X-ray-induced photodynamic therapy. J Radiation Res Appl Sci. 2024;17(3):100963. doi:10.1016/j.jrras.2024.100963
28. Deepak KGK, Vempati R, Nagaraju GP, et al. Tumor microenvironment: challenges and opportunities in targeting metastasis of triple negative breast cancer. Pharmacol Res. 2020;153:104683. doi:10.1016/j.phrs.2020.104683
29. Pei P, Chen Y, Sun C, et al. X-ray-activated persistent luminescence nanomaterials for NIR-II imaging. Nat Nanotechnol. 2021;16(9):1011–1018. doi:10.1038/s41565-021-00922-3
30. Bontkes HJ, Kramer D, Ruizendaal JJ, et al. Dendritic cells transfected with interleukin-12 and tumor-associated antigen messenger RNA induce high avidity cytotoxic T cells. Gene Ther. 2007;14(4):366–375. doi:10.1038/sj.gt.3302874
31. Cruceriu D, Baldasici O, Balacescu O, et al. The dual role of tumor necrosis factor-alpha (TNF-α) in breast cancer: molecular insights and therapeutic approaches. Cell Oncol. 2020;43(1):1–18. doi:10.1007/s13402-019-00489-1
32. Shan Y, Xie T, Sun Y, et al. Lipid metabolism in tumor-infiltrating regulatory T cells: perspective to precision immunotherapy. Biomark Res. 2024;12(1). doi:10.1186/s40364-024-00588-8
33. Liu Q, Sun Z, Chen L. Memory T cells: strategies for optimizing tumor immunotherapy. Protein Cell. 2020;11(8):549–564. doi:10.1007/s13238-020-00707-9
34. Han J, Khatwani N, Searles TG, et al. Memory CD8+ T cell responses to cancer. Semin Immunol. 2020;49:101435. doi:10.1016/j.smim.2020.101435
35. Okazaki S, Sasaki T, Yasuda S, et al. The feasibility of circulating tumor DNA analysis as a marker of recurrence in triple-negative breast cancer. Oncol Lett. 2021;21(5):420. doi:10.3892/ol.2021.12681
36. Andre F, Zielinski CC. Optimal strategies for the treatment of metastatic triple-negative breast cancer with currently approved agents. Ann Oncol. 2012;23(Suppl 6):i46–i51. doi:10.1093/annonc/mds195
37. Farshbafnadi M, Pastaki KA, Rezaei N. Immune checkpoint inhibitors for triple-negative breast cancer: from immunological mechanisms to clinical evidence. Int Immunopharmacol. 2021;98:107876. doi:10.1016/j.intimp.2021.107876
38. Bianchini G, De Angelis C, Licata L, et al. Treatment landscape of triple-negative breast cancer - expanded options, evolving needs. Nat Rev Clin Oncol. 2022;19(2):91–113. doi:10.1038/s41571-021-00565-2
39. Wang X, Sun W, Shi H, et al. Organic phosphorescent nanoscintillator for low-dose X-ray-induced photodynamic therapy. Nat Commun. 2022;13(1):5091. doi:10.1038/s41467-022-32054-0
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.