Back to Journals » Clinical Ophthalmology » Volume 19
Quantitative Anterior Segment SD-OCT Assessment of the Iridocorneal Angle in Chinese Patients with Open-Angle Glaucoma or Ocular Hypertension: An Observational Study
Authors Penzner J, Sun X ![]() , Wang YX, Li N, Issa M, Lai H, Ho Q, Lee SS, Robinson MR
, Wang YX, Li N, Issa M, Lai H, Ho Q, Lee SS, Robinson MR
Received 23 May 2025
Accepted for publication 14 October 2025
Published 16 December 2025 Volume 2025:19 Pages 4725—4735
DOI https://doi.org/10.2147/OPTH.S536846
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Jeff Penzner,1 Xinghuai Sun,2 Ya Xing Wang,3 Ni Li,4 Masara Issa,1 Hongxin Lai,1 Quoc Ho,1 Susan S Lee,1 Michael R Robinson1
1AbbVie, Irvine, CA, USA; 2Eye & ENT Hospital of Fudan University, Shanghai, People’s Republic of China; 3Beijing Institute of Ophthalmology, Beijing Tongren Hospital, Capital Medical University, Beijing, People’s Republic of China; 4West China Hospital, Sichuan University, Chengdu, People’s Republic of China
Correspondence: Jeff Penzner, Allergan, an AbbVie company, 2525 Dupont Drive, Irvine, CA, 92612, USA, Tel +1 (714) 246 3828, Email [email protected]
Purpose: We evaluated iridocorneal angle biometrics using anterior segment spectral-domain optical coherence tomography (SD-OCT) compared with Shaffer grade clinical assessments in Chinese patients with open-angle glaucoma (OAG) or ocular hypertension (OHT) to determine which method is most suitable for preoperative angle assessment.
Methods: This noninterventional, prospective study enrolled 206 patients with OAG or OHT in both eyes and Shaffer grade > 1 iridocorneal angles at 3 sites in China. Shaffer grades and SD-OCT 5-line raster scans (Zeiss Cirrus HD-OCT 4000) of the inferior angle were obtained under dark conditions. Images were evaluated for visualization of Schwalbe’s line, the superior iris surface, and angle recess. ImageJ software was used to measure the angle-opening distance at Schwalbe’s line (SL-AOD) in gradable images.
Results: Almost all study eyes had Shaffer grade 4 (91.0%) or grade 3 (8.3%) angles. Mean (standard deviation) SL-AOD was 0.75 (0.33) mm (median 0.73, range 0.051– 1.9, n=322). The SL-AOD was < 0.635 mm (the tube outer diameter of the Ahmed glaucoma valve and Baerveldt glaucoma implant) in 37.6% of the eyes. SL-AOD values did not differ significantly between OAG and OHT diagnoses or between phakic and pseudophakic eyes.
Conclusion: Iridocorneal angle biometrics derived from SD-OCT images in Chinese patients with OAG or OHT showed large variation in the SL-AOD in eyes with open angles on gonioscopy. Over one-third of patients had SL-AOD too small to safely accommodate commonly used glaucoma tube shunts. Expanded preoperative use of SD-OCT could potentially be beneficial to detect angles at risk for corneal complications and inform device selection.
Keywords: Asia, biometrics, glaucoma, ocular hypertension, optical coherence tomography, iridocorneal angle
Introduction
Glaucoma is the leading cause of irreversible blindness globally, affecting over 60 million people 40–80 years of age, and is projected to affect 111.8 million people by the year 2040.1,2 Asia accounts for 60% of glaucoma cases worldwide, with an estimated 33.5 million and 11.7 million cases of primary open-angle glaucoma (OAG) and primary angle-closure glaucoma (ACG), respectively.3 Assessment of iridocorneal angle width is important for the identification of angles at increased risk of closure, and also to identify appropriate angle size for safe use of glaucoma tube shunts.4,5 Placement of a device in an inadequate space may lead to contact with the corneal endothelium, resulting in risk of vision impairment from corneal edema and corneal endothelial cell loss.6 Progressive loss of corneal endothelial cells can be significant and lead to corneal decompensation and vision loss, which may ultimately require surgical intervention.7
In clinical practice, iridocorneal angle width is typically evaluated on gonioscopy using a gonioscopy lens and a standard grading system such as the Shaffer grading system.8 Although gonioscopy is the gold standard for angle assessment, this technique is subjective and does not provide quantitative information needed to accurately assess angle measurements.4,9 Alternative approaches to iridocorneal angle assessment include ultrasound biomicroscopy and anterior segment optical coherence tomography (AS-OCT). Both methods can generate detailed images of anterior segment structures including the iridocorneal angle.4 However, ultrasound biomicroscopy is time consuming, requires direct contact with the eye, and is less reproducible because results can be influenced by the operator.4 AS-OCT is a noncontact imaging modality and has several advantages over ultrasound biomicroscopy for angle assessment, including faster image acquisition and generation of images with higher resolution.4 AS-OCT has been used in numerous studies to better understand iridocorneal angle biometrics in patients with glaucoma.10–13
Angle parameters determined from AS-OCT include the angle-opening distance (AOD), which is a surrogate for gonioscopic angle measurement in eyes with open angles.14 Historically, images from time-domain OCT instruments were low resolution, and Schwalbe’s line could not be reliably identified.15 As a result, the scleral spur was used as the primary anatomical landmark, with the AOD measured at a distance of 500 or 750 µm anteriorly, approximating the location of Schwalbe’s line.15 With the later generation higher-resolution spectral-domain OCT (SD-OCT) instrument, visualization of Schwalbe’s line is enhanced in the images, and no scleral spur–based approximation of its location is required.15 Therefore, with SD-OCT, enhanced visualization of Schwalbe’s line has allowed the determination of novel angle biometrics based on this location including the angle-opening distance at Schwalbe’s line (SL-AOD), which has shown high levels of repeatability (intraclass correlation coefficient [ICC] of ≥0.997 for measurements from the same image) and reproducibility between instruments, graders, and image acquisitions (ICC of 0.961 between the Cirrus and Spectralis instruments, ≥0.929 between graders, and ≥0.989 between sequential image acquisitions), leading to standardization of this biometric.16
Ethnic Chinese people have smaller iridocorneal angles relative to White people because of differences in eye anatomy, including a smaller anterior chamber width and thicker irises,17–19 and thus are at higher risk of ACG18 and corneal contact with devices in the angle. Even when angles appear to be open, the AOD in Chinese eyes may be smaller than in non-Asian eyes,18 and too small to accommodate a glaucoma tube shunt. A study comparing AS-OCT and gonioscopy assessments of angle size in a Chinese-American population demonstrated large variability in AOD 750 measurements of angle width among eyes with Shaffer grade 3 and grade 4 angles.20
The purpose of the current study was to quantitatively assess Schwalbe’s line–based iridocorneal angle biometrics with SD-OCT in a Chinese population with OAG or ocular hypertension (OHT). We compared SD-OCT measurements with clinical assessment of the angle width by Shaffer grading to determine which method might be most suitable for the preoperative assessment of whether the angle can safely accommodate a tube shunt. The AS-OCT images from some of the patients were used previously in a study evaluating the maximum implant fit, a novel biometric of angle size.21
Methods
This noninterventional, prospective study was conducted at 3 academic research institutions in China to quantitatively assess the iridocorneal angle width in patients with OAG or OHT (ClinicalTrials.gov identifier: NCT01781962). Research was carried out in accordance with the Declaration of Helsinki and Chinese and local privacy requirements, and the study protocol and key documents were approved by an Independent Ethics Committee (Ethics Committee of West China Hospital, Sichuan University, Sichuan, China; Ethics Committee of Beijing Tongren Hospital, Beijing, China; or Ethics Committee of the Eye and ENT Hospital of Fudan University, Shanghai, China) at each site prior to study initiation. All patients provided written informed consent.
The study population included male and female patients, 18 years of age or older, with a diagnosis of OAG (primary OAG, pseudoexfoliation glaucoma, or pigmentary glaucoma) or OHT in both eyes. An additional key entry criterion was Chinese ancestry, defined as self-reported Chinese lineage from all 4 grandparents of the patient. Phakic and pseudophakic eyes were included.
Patients were excluded from study participation if they had a history of a narrow angle (Shaffer grade ≤1) or angle closure, angle recession, abnormal anterior segment anatomy due to surgery or trauma, or other ocular abnormalities that would preclude accurate OCT assessment; a known history of peripheral anterior synechiae in the inferior angle; intraocular surgery within 3 months prior to the examination day; uncontrolled systemic disease; or allergy to the diagnostic agents used in the study. Patients with an angle abnormality affecting angle anatomy in the inferior angle in either eye, including but not limited to aqueous bypass shunts, Trabectome procedures, or congenital ocular disease, were also excluded. However, the study protocol did not specify examination for plateau iris configuration or exclusion of affected patients.
SD-OCT Image Acquisition
SD-OCT was performed using the Zeiss Cirrus HD-OCT 4000 and software version 4.5 or higher (Carl Zeiss AG, Oberkochen, Germany). SD-OCT images were acquired in dark examination rooms, and consistent dark conditions for the examinations were confirmed using a light meter. The 5-line raster scan protocol was rotated to the vertical position and centered on the pupil to image the inferior angle (6 o’clock position). Qualified OCT operators optimized patient and instrument positioning to obtain clear visualization of Descemet’s membrane, corneal endothelium, and trabecular meshwork, which in turn allowed for high confidence in identifying Schwalbe’s line (Figure 1). Additionally, visualization of the anterior iris surface was necessary for proper measurement of angle biometrics.
 |
Figure 1 Anterior segment spectral-domain optical coherence tomography image of iridocorneal angle showing Descemet’s membrane (DM, white line), corneal endothelium (CE), Schwalbe’s line (SL, yellow circle), trabecular meshwork (TM), and superior iris surface (IRIS). Clear visualization indicates proper instrument positioning and a gradable image. |
Shaffer Grading
Gonioscopy was performed following SD-OCT in a dark room. Shaffer grades were determined using a Goniometric MV200 lens (Ocular Instruments, Inc, Bellevue, WA, USA) to observe the inferior iridocorneal angle at approximately the 6 o’clock position, corresponding to the SD-OCT measurement procedures.
SD-OCT Image Grading and Peer Review
A single grader initially reviewed all SD-OCT images for quality (eg, noise, artifacts) and ability to visualize the inferior angle, including the key landmarks highlighted in Figure 1, such that accurate measurements were possible. Identification of Schwalbe’s line at the termination of Descemet’s membrane was critical. Two additional graders reviewed any images of suboptimal quality for angle visualization, and a consensus among the graders was required to keep or discard these images from the dataset.
Image Analysis
The SL-AOD, defined as the length of the line perpendicular to the corneal endothelium between Schwalbe’s line and the superior iris surface,22 was measured on calibrated SD-OCT images using ImageJ 1.49v software (National Institutes of Health, Bethesda, MD, USA, and Laboratory for Optical and Computational Instrumentation, University of Wisconsin, Madison, WI, USA) as described previously.15,16 This software allows a line to be drawn on an image to measure the distance between two points. For the analysis of SL-AOD, the grader (an author) identified the location of Schwalbe’s line and drew a line from Schwalbe’s line perpendicular to the corneal endothelium to the point where it met the superior surface of the iris; the length of this line was determined to be the SL-AOD (Figure 2).
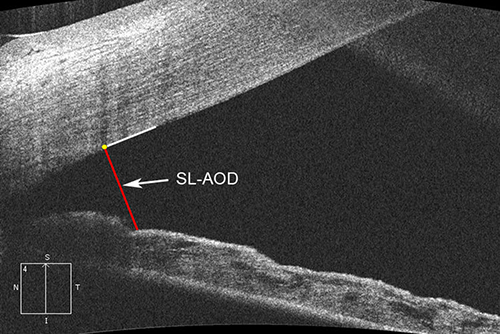 |
Figure 2 Anterior segment spectral-domain optical coherence tomography image illustrating the Schwalbe’s line–based angle-opening distance (SL-AOD, red line). Yellow circle, Schwalbe’s line; white line, corneal endothelium. |
Statistical Analysis
The statistical analysis used SAS version 9.4 software (SAS Institute, Cary, NC, USA). Patient demographics, SL-AOD measurements, and Shaffer grades were summarized with descriptive statistics. Mixed model repeated measures (MMRM) modeling was also applied for the analysis of SL-AOD and for subgroup analysis of SL-AOD by demographic and clinical parameters to adjust for the correlation between eyes, with observations from the right and left eye treated as repeated measures in the MMRM models.
Results
SD-OCT images of both eyes in 206 patients were acquired. Demographic and clinical characteristics of the patients and eyes are listed in Table 1. Patients were all Chinese and primarily diagnosed with OAG. Most of the study eyes were phakic (92.5% phakic, 6.3% pseudophakic) and had Shaffer grade 4 angles.
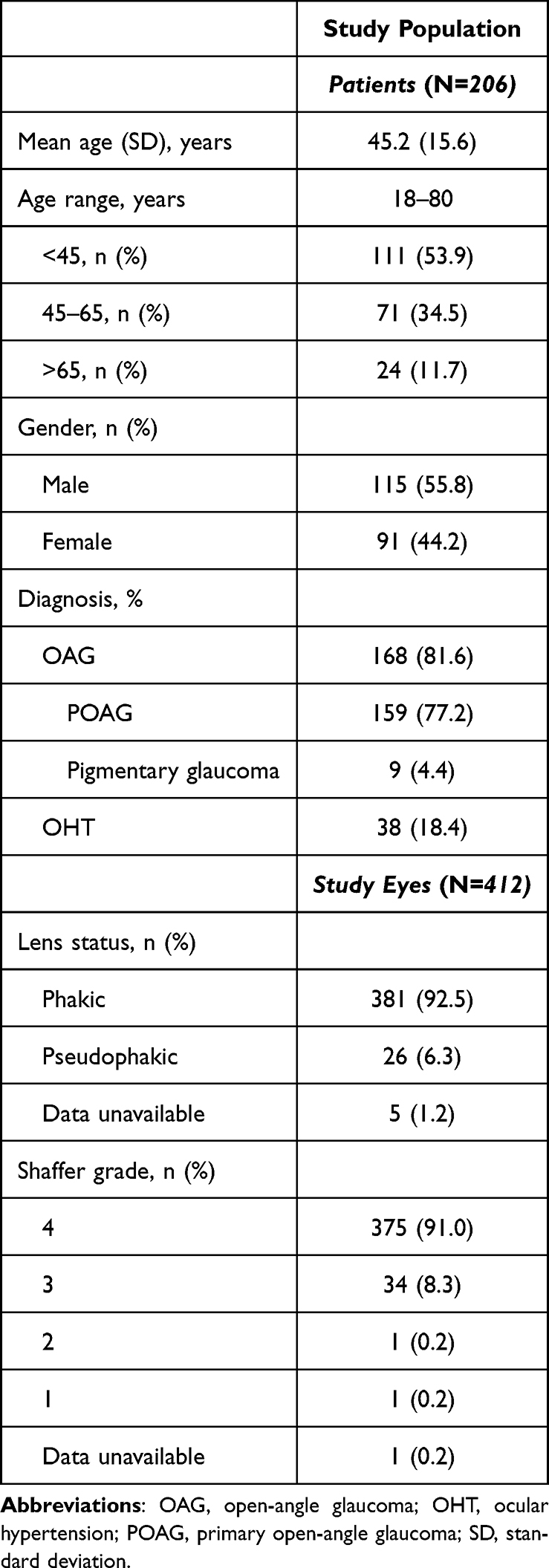 |
Table 1 Study Population Demographics and Clinical Characteristics |
Images that were gradable (ie, suitable for analysis of iridocorneal angle biometrics) were subsequently identified and used for analysis. The criteria for gradable images were clear visibility of Schwalbe’s line, the corneal endothelium, and the superior iris surface. In most of the images that were ungradable, the iris was out of the field of view or there was excessive image noise.
Figure 3 shows the distribution of SL-AOD values in eyes with gradable images (322 eyes of 178 patients). Large variability in the SL-AOD values was evident within eyes with open angles on gonioscopy (Figure 3). The mean (standard deviation) SL-AOD was 0.75 (0.33) mm (95% confidence interval [CI]: 0.71–0.79; median 0.73; range 0.051–1.9; n=322 eyes). There was a weak positive correlation between SL-AOD values and Shaffer grades (rs = 0.13; 95% CI: 0.02–0.24; P = 0.019). The SL-AOD was <0.635 mm in 37.6% (121/322) of the eyes with gradable images, including 57.1% (16/28) of the eyes with Shaffer grade 3 inferior angles and 35.3% (103/292) of the eyes with Shaffer grade 4 inferior angles.
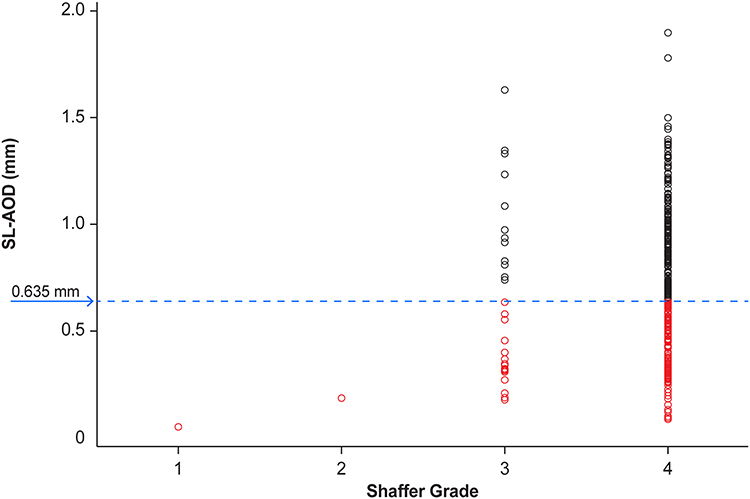 |
Figure 3 Distribution of SL-AOD values in eyes of Chinese patients with OAG or OHT. Blue arrow and dashed line show the 0.635 value. Red circles indicate values <0.635 mm. Abbreviations: OAG, open-angle glaucoma; OHT, ocular hypertension; SL-AOD, Schwalbe’s line–based angle-opening distance. |
There was a significant relationship between patient age and angle width, with SL-AOD larger (P<0.001) in the eyes of patients younger than 45 years than in older patients (Table 2). A significant relationship between patient gender and angle width was also observed (Table 2). Eyes of male patients had significantly larger angles than those of female patients (P=0.003), with least-squares mean SL-AOD of 0.829 mm and 0.677 mm in male and female patients, respectively. No significant difference in SL-AOD was seen between eyes diagnosed with OAG and those diagnosed with OHT, or between pseudophakic and phakic eyes (Table 2).
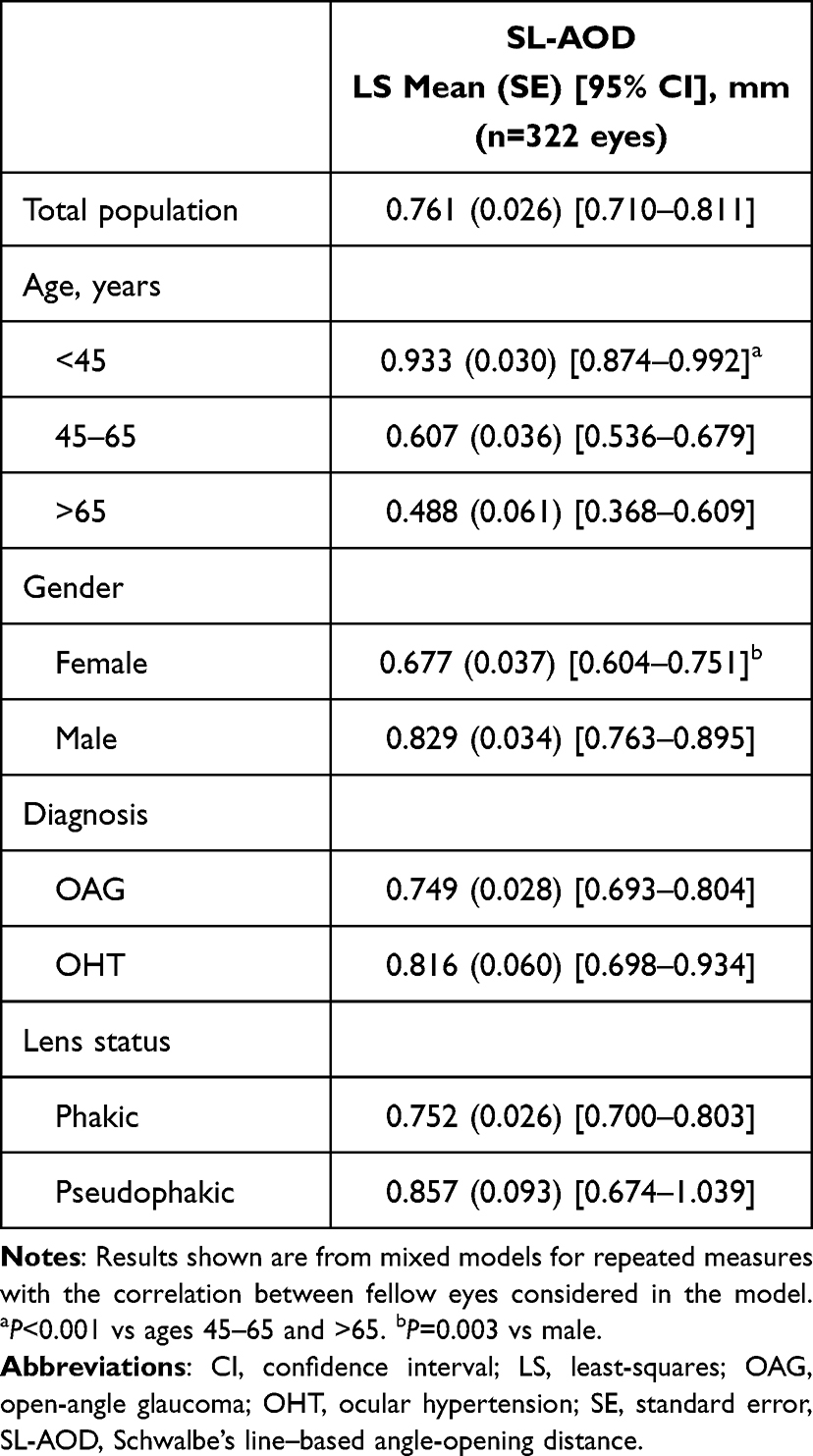 |
Table 2 Angle Biometrics in the Total Population and Subgroups |
Discussion
In this study, we used SD-OCT images and gonioscopy to assess the iridocorneal angle in eyes of Chinese patients with OAG or OHT. We evaluated the SL-AOD, a standard biometric for angle size, in all patients to allow comparison of the AOD to literature values and to the tube diameter of commonly used glaucoma drainage devices. The results showed large variability in the SL-AOD among eyes with wide open angles on gonioscopy. In a substantial proportion of the eyes, commonly used glaucoma tube shunts would be unable to fit within the angle without contacting the corneal endothelium.
Focal corneal edema near the tube shunt progressing to complete corneal decompensation and leading to vision loss is a well-recognized, frequent complication of glaucoma drainage devices.23–26 During 5 years of follow-up in the Tube Versus Trabeculectomy Study, 12.1% of patients who received the Baerveldt glaucoma implant had persistent corneal edema associated with loss of at least 2 lines of vision, and 5.6% required penetrating keratoplasty.27 Similarly, in the Ahmed Baerveldt Comparison Study, the 5-year cumulative rate of device-related corneal edema was approximately 12% with each device, and the 5-year incidence of corneal transplant procedures was 2.1% with the Ahmed glaucoma valve and 3.0% with the Baerveldt glaucoma implant.28 It has been suggested that corneal damage may be caused by intermittent contact with the device during hard blinks or eye rubbing.29 Peripheral corneal endothelium damage caused by tube contact is thought to lead to localized corneal edema,23–25 and eventually, central endothelial cell loss with total corneal decompensation and vision loss in some patients.7,26 Consistent with this concept, studies have shown that the proximity of glaucoma drainage devices to the corneal endothelium is related to corneal endothelial cell loss.30,31
As the tube outer diameters of the Ahmed glaucoma valve (New World Medical, Rancho Cucamonga, CA, USA) and the Baerveldt glaucoma implant (Johnson & Johnson Vision, Jacksonville, FL, USA) are 0.635 mm,32 we deduce that the SL-AOD in eyes receiving these drainage devices needs to be wider than 0.635 mm to prevent contact between the tube and the corneal endothelium. In our study population of Chinese patients with OAG and OHT, 37.6% of eyes had an SL-AOD <0.635 mm and would be at high risk of corneal complications with these glaucoma tube shunts. The XEN 45 gel stent (AbbVie, North Chicago, IL, USA; hydrated outer diameter 0.22 mm) used in minimally invasive glaucoma surgery can likely be safely used in eyes with a broader range of SL-AODs.
Several previous studies have evaluated angle biometrics in Chinese individuals with open angles.16,33–35 In a study using scleral spur–based OCT methodology, the mean AOD measured 500 µm and 750 µm anteriorly to the scleral spur in a population of predominantly Chinese patients with gonioscopically confirmed open angles was 0.28 mm and 0.38 mm, respectively.33 These values are smaller than the Schwalbe’s line–based AOD measurements in our cohort; however, the relationship between scleral spur– and Schwalbe’s line–based AOD is unknown. A 2015 study by Dastiridou et al34 in 20 healthy individuals with open angles who were predominantly Asian reported an average SL-AOD value of 0.75 mm, and another study in a comparable population of 21 predominantly Asian individuals by Marion et al16 reported an average SL-AOD value of 0.68 mm. These results are consistent with those in our Chinese OAG/OHT population (mean SL-AOD, 0.75 mm). Similar to our study, both of these studies excluded participants with angles of Shaffer grade ≤1 and were conducted in relatively young populations; the average patient age was 32 years in the study by Dastiridou et al34 and 35 years in the study by Marion et al.16 However, these studies examined populations of mixed Asian ethnicities, whereas our study included only patients of Chinese descent. Another study by Dastiridou et al35 compared angle biometrics of healthy Caucasian and Chinese volunteers and found significantly larger SL-AOD values in the Caucasian group (0.464 mm in Caucasian volunteers versus 0.344 mm in Chinese volunteers).35 Interestingly, the mean SL-AOD values in both the Caucasian and Chinese groups35 were substantially smaller than those observed in the Chinese population with OAG/OHT in this study. Potential explanations for the difference in mean iridocorneal angle biometrics between these studies may be related to differences in the study populations, ie, patients with OAG/OHT in this study versus healthy volunteers in the other study,35 and to the potential inclusion of participants with a Shaffer grade of <2 in the inferior angle assessed with SD-OCT in the study by Dastiridou et al.35
Our study findings are applicable to Chinese individuals with demographic and clinical characteristics similar to those of the study population. The mean age of patients in our study (45.2 years) was younger than typically seen in studies involving patients with OAG and OHT in the western world. However, the prevalence of primary OAG is less age-dependent in Asian populations than in White populations.36 The trend of decreasing SL-AOD with increasing age (shown in Table 2) observed in our study may be related to the increase in equatorial diameter of the lens with age37,38 and narrowing of the angle; therefore, the younger patients likely had thinner lenses, resulting in larger angle biometrics. Finally, the gender difference in angle biometrics in this study, where male patients had a larger SL-AOD than female patients, is consistent with previous reports39 and is thought to be related to the higher prevalence of angle closure in female patients.
Angle size is determined by anatomical characteristics such as iris thickness and lens vault that vary by race and ethnicity.19,40 Iris thickness is increased and the prevalence of angle-closure glaucoma is higher in Chinese, Hispanic, and African-American populations compared with White populations.19 Further, there is abundant evidence that Chinese populations have smaller angles than White populations.17–19 However, the mean SL-AOD in the Chinese patients in this study was relatively large (0.75 mm), most likely because the study eligibility criteria excluded patients with a history of narrow or closed angles, the study population was relatively young, and the prevalence of myopia (which is associated with deeper angles) in Asia is growing.41
Although Shaffer grading has been the gold standard for categorizing iridocorneal angle size8 and provides categorical angle values, SD-OCT biometrics may be helpful in providing continuous values and a more quantitative and precise evaluation of angle size. The biometrics in our study population were broadly distributed, and the results showed wide variability in SL-AOD within the categorical Shaffer grades of 3 and 4. An SD-OCT–based biometric such as SL-AOD might be most valuable at the margins (eg, for the smallest of grade 4 angles) in determining the appropriateness of a glaucoma tube shunt. Additionally, since SD-OCT visualizes Schwalbe’s line more effectively than time-domain devices, SD-OCT–based measurements might provide a more accurate assessment of the risk of a device contacting and damaging the corneal endothelium than measurements based on scleral spur–based estimations of Schwalbe’s line. Assessment of angle width in the target quadrant with the objective measurement of SL-AOD could be used along with conventional assessments to help guide device selection and improve the safety of intracameral glaucoma treatments. SD-OCT evaluation can provide supplementary anatomical insight but should not be used in isolation for preoperative decision making.
Our study compared gonioscopic and SD-OCT measurements of the inferior angle primarily because the angle in the inferior quadrant can be easily and reliably imaged with SD-OCT.42 Retraction of the lower lid provides clear access to the inferior angle, and inferior angle assessments are generally used in clinical studies and clinical practice because of the consistent image quality. In contrast, imaging of the superior angle can be challenging because of the positioning of the upper eyelid, and image quality can vary.42 Importantly, in a study that evaluated angle size by gonioscopy in all four quadrants in the eyes of subjects of European, African, and east Asian descent, the mean grade for angle size was significantly higher (more open) in the inferior quadrant than in the nasal, temporal, and superior quadrants.43 Further, a study evaluating Schaffer grades of the angle in all four quadrants reported that mean Schaffer grades varied by race or ethnicity, but for subjects of each race or ethnicity, mean Schaffer grades were similar among quadrants and numerically slightly lower for the inferior angle compared with the superior angle.19 These results suggest that inferior angle measurement could potentially be useful as a conservative surrogate measurement of the angle in other quadrants. We acknowledge, however, that individual-level data on variability in angle size among quadrants are lacking, and presurgical evaluation for every patient should include evaluation of the angle at the planned site of device use.
There were several limitations of this study. Approximately one-fifth of eyes had ungradable SD-OCT images, and the number of patients with Shaffer grades <4 was relatively small. Additional studies are needed to validate the findings. Myopia is rapidly increasing in prevalence41 and is associated with increased risk of developing OAG,44 yet a potential effect of myopia on angle biometrics could not be evaluated because of the lack of refractive error data. Similarly, no data on iris thickness were collected. Future studies will be required to test the hypothesis of a relationship between myopia and angle biometrics as well as the hypothesis of a relationship between iris thickness and angle biometrics in Chinese patients with OAG or OHT. Also, the scope of this study was limited to assessment of the inferior angle, yet glaucoma shunts are often placed in the superotemporal or superonasal iridocorneal angle. The variability in space availability across other quadrants should be considered when evaluating the angle for shunt use.
Conclusions
Chinese patients differ from non-Asian patients in the anatomy of the eye and lens. For this reason, Chinese patients have increased risk of ACG and may also be more likely to have small, open angles that make them unsuitable candidates for glaucoma tube shunts. The Chinese patients with OAG or OHT in this study were relatively young and on average had wide inferior iridocorneal angles as measured by the SL-AOD, yet a substantial proportion of the patients had small SL-AODs and would be prone to having corneal complications with commonly used glaucoma tube shunts. The small angles were not detected on gonioscopy with Shaffer grading. As angle devices are being increasingly used for glaucoma treatment, expanded use of SD-OCT to evaluate angle biometrics could potentially be beneficial to detect angles at risk for corneal complications of these devices and inform device selection.
Abbreviations
ACG, angle-closure glaucoma; AOD, angle-opening distance; AS-OCT, anterior segment optical coherence tomography; OAG, open-angle glaucoma; OCT, optical coherence tomography; OHT, ocular hypertension; SD, standard deviation; SD-OCT, spectral-domain optical coherence tomography; SL-AOD, Schwalbe’s line–based angle-opening distance.
Acknowledgments
The authors thank Xu Liang for contributions to the study and the manuscript development. Medical writing support was provided by Evidence Scientific Solutions, Inc. (Raleigh, NC, USA) and funded by AbbVie.
Data Sharing Statement
AbbVie is committed to responsible data sharing regarding the clinical studies we sponsor. This includes access to anonymized, individual, and study-level data (analysis data sets), as well as other information (eg, protocols, clinical study reports, or analysis plans), as long as the studies are not part of an ongoing or planned regulatory submission. This includes requests for study data for unlicensed products and indications.
These data can be requested by any qualified researchers who engage in rigorous, independent, scientific research, and will be provided following review and approval of a research proposal, Statistical Analysis Plan (SAP), and execution of a Data Sharing Agreement (DSA). Data requests can be submitted at any time after approval in the US and Europe and after acceptance of this manuscript for publication. The data will be accessible for 12 months, with possible extensions considered. For more information on the process or to submit a request, visit the following link: https://www.abbvieclinicaltrials.com/hcp/data-sharing/.
Funding
Allergan (prior to its acquisition by AbbVie) and/or AbbVie funded this study and participated in the study design, research, analysis, data collection, interpretation of data, and reviewing and approval of the publication.
Disclosure
Xinghuai Sun, Ya Xing Wang, and Ni Li have no financial relationships to disclose. Jeff Penzner, Masara Issa, Hongxin Lai, Quoc Ho, Susan S. Lee, and Michael R. Robinson are employees of AbbVie and may hold stock.
References
1. Tham Y-C, Li X, Wong TY, Quigley HA, Aung T, Cheng C-Y. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090. doi:10.1016/j.ophtha.2014.05.013
2. Cheng JW, Cheng SW, Ma XY, Cai JP, Li Y, Wei RL. The prevalence of primary glaucoma in mainland China: a systematic review and meta-analysis. J Glaucoma. 2013;22(4):301–306. doi:10.1097/IJG.0b013e31824083ca
3. Chan EW, Li X, Tham YC, et al. Glaucoma in Asia: regional prevalence variations and future projections. Br J Ophthalmol. 2016;100(1):78–85. doi:10.1136/bjophthalmol-2014-306102
4. Riva I, Micheletti E, Oddone F, et al. Anterior chamber angle assessment techniques: a review. J Clin Med. 2020;9(12):3814. doi:10.3390/jcm9123814
5. Stein JD. Preoperative Evaluation for Glaucoma Drainage Device Surgery. In: Kahook’s Essentials of Glaucoma Therapy. Available from https://www.keogt.com/Preoperative_Evaluation_for_Glaucoma_Drainage_Device_Surgery.
6. Weinlander E, Meijome T, Shah M. The impact of glaucoma drainage devices on the cornea. Curr Ophthalmol Rep. 2020;8:159–164. doi:10.1007/s40135-020-00234-0
7. Beatson B, Wang J, Boland MV, et al. Corneal edema and keratoplasty: risk factors in eyes with previous glaucoma drainage devices. Am J Ophthalmol. 2022;238:27–35. doi:10.1016/j.ajo.2021.12.017
8. Radhakrishnan S, See J, Smith SD, et al. Reproducibility of anterior chamber angle measurements obtained with anterior segment optical coherence tomography. Invest Ophthalmol Vis Sci. 2007;48(8):3683–3688. doi:10.1167/iovs.06-1120
9. Lin SC. Assessing the angle: which method is best? Available from: https://www.reviewofophthalmology.com/article/assessing-the-angle-which-method-is-best.
10. Dada T, Sihota R, Gadia R, Aggarwal A, Mandal S, Gupta V. Comparison of anterior segment optical coherence tomography and ultrasound biomicroscopy for assessment of the anterior segment. J Cataract Refract Surg. 2007;33(5):837–840. doi:10.1016/j.jcrs.2007.01.021
11. Perera SA, Ho CL, Aung T, et al. Imaging of the iridocorneal angle with the RTVue spectral domain optical coherence tomography. Invest Ophthalmol Vis Sci. 2012;53(4):1710–1713. doi:10.1167/iovs.11-8159
12. Ni Ni S, Tian J, Marziliano P, Wong HT. Anterior chamber angle shape analysis and classification of glaucoma in SS-OCT images. J Ophthalmol. 2014;2014:942367. doi:10.1155/2014/942367
13. Sihota R, Kamble N, Sharma AK, et al. ‘Van Herick Plus’: a modified grading scheme for the assessment of peripheral anterior chamber depth and angle. Br J Ophthalmol. 2019;103(7):960–965. doi:10.1136/bjophthalmol-2018-312132
14. Xu BY, Pardeshi AA, Burkemper B, et al. Quantitative evaluation of gonioscopic and EyeCam assessments of angle dimensions using anterior segment optical coherence tomography. Transl Vis Sci Technol. 2018;7(6):33. doi:10.1167/tvst.7.6.33
15. Pan X, Marion K, Maram J, et al. Reproducibility of anterior segment angle metrics measurements derived from Cirrus spectral domain optical coherence tomography. J Glaucoma. 2015;24(5):e47–51. doi:10.1097/ijg.0000000000000136
16. Marion KM, Maram J, Pan X, et al. Reproducibility and agreement between 2 spectral domain optical coherence tomography devices for anterior chamber angle measurements. J Glaucoma. 2015;24(9):642–646. doi:10.1097/ijg.0000000000000303
17. Leung CK, Palmiero PM, Weinreb RN, et al. Comparisons of anterior segment biometry between Chinese and Caucasians using anterior segment optical coherence tomography. Br J Ophthalmol. 2010;94(9):1184–1189. doi:10.1136/bjo.2009.167296
18. Wang D, Qi M, He M, Wu L, Lin S. Ethnic difference of the anterior chamber area and volume and its association with angle width. Invest Ophthalmol Vis Sci. 2012;53(6):3139–3144. doi:10.1167/iovs.12-9776
19. Lee RY, Huang G, Porco TC, Chen YC, He M, Lin SC. Differences in iris thickness among African Americans, Caucasian Americans, Hispanic Americans, Chinese Americans, and Filipino-Americans. J Glaucoma. 2013;22(9):673–678. doi:10.1097/IJG.0b013e318264ba68
20. Xu BY, Pardeshi AA, Burkemper B, et al. Differences in anterior chamber angle assessments between gonioscopy, EyeCam, and anterior segment OCT: the Chinese American Eye Study. Transl Vis Sci Technol. 2019;8(2):5. doi:10.1167/tvst.8.2.5
21. Craven ER, Chopra V, Goldberg JL, et al. Comparison of iridocorneal angle assessments in open-angle glaucoma and ocular hypertension patients: anterior segment optical coherence tomography and gonioscopy. Clin Ophthalmol. 2022;16:1301–1312. doi:10.2147/opth.S322962
22. Cheung CY, Zheng C, Ho CL, et al. Novel anterior-chamber angle measurements by high-definition optical coherence tomography using the Schwalbe line as the landmark. Br J Ophthalmol. 2011;95(7):955–959. doi:10.1136/bjo.2010.189217
23. Dada T, Gupta R, Tinwala SI, Sobti A, Panda A. Repositioning of Ahmed glaucoma valve tube in the anterior chamber with prolene sutures to manage tube-endothelial touch. Nepal J Ophthalmol. 2012;4(2):309–311. doi:10.3126/nepjoph.v4i2.6549
24. Senthil S, Badakare A. Dynamic tube movement after reimplantation of Ahmed glaucoma valve in a child with glaucoma in aphakia. BMJ Case Rep. 2014;2014:1. doi:10.1136/bcr-2013-203197
25. Kumar H, Gupta A, Gupta V. A microinvasive technique for management of corneal edema secondary to glaucoma drainage device tube-corneal touch. Indian J Ophthalmol. 2018;66(6):861–862. doi:10.4103/ijo.IJO_987_17
26. Wang N. Tube Shunt Related Complications of the Cornea. Complications of Glaucoma Surgery. 2020. doi:10.1093/oso/9780195382365.003.0065
27. Gedde SJ, Herndon LW, Brandt JD, Budenz DL, Feuer WJ, Schiffman JC. Postoperative complications in the Tube Versus Trabeculectomy (TVT) study during five years of follow-up. Am J Ophthalmol. 2012;153(5):804–814.e801. doi:10.1016/j.ajo.2011.10.024
28. Budenz DL, Feuer WJ, Barton K, et al. Postoperative complications in the Ahmed Baerveldt Comparison Study during five years of follow-up. Am J Ophthalmol. 2016;163:75–82.e73. doi:10.1016/j.ajo.2015.11.023
29. Kim CS, Yim JH, Lee EK, Lee NH. Changes in corneal endothelial cell density and morphology after Ahmed glaucoma valve implantation during the first year of follow up. Clin Exp Ophthalmol. 2008;36(2):142–147. doi:10.1111/j.1442-9071.2008.01683.x
30. Koo EB, Hou J, Han Y, Keenan JD, Stamper RL, Jeng BH. Effect of glaucoma tube shunt parameters on cornea endothelial cells in patients with Ahmed valve implants. Cornea. 2015;34(1):37–41. doi:10.1097/ico.0000000000000301
31. Tan AN, Webers CA, Berendschot TT, et al. Corneal endothelial cell loss after Baerveldt glaucoma drainage device implantation in the anterior chamber. Acta Ophthalmol. 2017;95(1):91–96. doi:10.1111/aos.13161
32. Pereira ICF, van de Wijdeven R, Wyss HM, Beckers HJM, den Toonder JMJ. Conventional glaucoma implants and the new MIGS devices: a comprehensive review of current options and future directions. Eye. 2021;35(12):3202–3221. doi:10.1038/s41433-021-01595-x
33. He Y, Baskaran M, Narayanaswamy AK, et al. Changes in anterior segment dimensions over 4 years in a cohort of Singaporean subjects with open angles. Br J Ophthalmol. 2015;99(8):1097–1102. doi:10.1136/bjophthalmol-2014-305816
34. Dastiridou AI, Pan X, Zhang Z, et al. Comparison of physiologic versus pharmacologic mydriasis on anterior chamber angle measurements using spectral domain optical coherence tomography. J Ophthalmol. 2015;2015:845643. doi:10.1155/2015/845643
35. Dastiridou A, Marion K, Niemeyer M, Francis B, Sadda S, Chopra V. Pilot study of the effects of ambient light level variation on spectral domain anterior segment OCT-derived angle metrics in Caucasians versus Asians. Curr Eye Res. 2018;43(7):955–959. doi:10.1080/02713683.2018.1464192
36. Rudnicka AR, Mt-Isa S, Owen CG, Cook DG, Ashby D. Variations in primary open-angle glaucoma prevalence by age, gender, and race: a Bayesian meta-analysis. Invest Ophthalmol Vis Sci. 2006;47(10):4254–4261. doi:10.1167/iovs.06-0299
37. Memarzadeh F, Tang M, Li Y, Chopra V, Francis BA, Huang D. Optical coherence tomography assessment of angle anatomy changes after cataract surgery. Am J Ophthalmol. 2007;144(3):464–465. doi:10.1016/j.ajo.2007.04.009
38. Tai MC, Chien KH, Lu DW, Chen JT. Angle changes before and after cataract surgery assessed by Fourier-domain anterior segment optical coherence tomography. J Cataract Refract Surg. 2010;36(10):1758–1762. doi:10.1016/j.jcrs.2010.05.011
39. Huang W, Gao X, Li X, et al. Anterior and posterior ocular biometry in healthy Chinese subjects: data based on AS-OCT and SS-OCT. PLoS One. 2015;10(3):e0121740. doi:10.1371/journal.pone.0121740
40. Lee RY, Huang G, Cui QN, He M, Porco TC, Lin SC. Association of lens vault with narrow angles among different ethnic groups. Curr Eye Res. 2012;37(6):486–491. doi:10.3109/02713683.2012.669006
41. Spillmann L. Stopping the rise of myopia in Asia. Graefes Arch Clin Exp Ophthalmol. 2020;258(5):943–959. doi:10.1007/s00417-019-04555-0
42. Akil H, Dastiridou A, Marion K, Francis B, Chopra V. Repeatability, reproducibility, agreement characteristics of 2 SD-OCT devices for anterior chamber angle measurements. Can J Ophthalmol. 2017;52(2):166–170. doi:10.1016/j.jcjo.2016.08.019
43. Congdon NG, Foster PJ, Wamsley S, et al. Biometric gonioscopy and the effects of age, race, and sex on the anterior chamber angle. Br J Ophthalmol. 2002;86(1):18–22. doi:10.1136/bjo.86.1.18
44. Marcus MW, de Vries MM, Junoy Montolio FG, Jansonius NM. Myopia as a risk factor for open-angle glaucoma: a systematic review and meta-analysis. Ophthalmology. 2011;118(10):1989–1994e1982. doi:10.1016/j.ophtha.2011.03.012
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Retrospective Analysis of Switching Bimatoprost 0.01% to Bimatoprost 0.03% in Patients with Various Types of Glaucoma and Ocular Hypertension
Xu KM, Cho R, Chan TYB
Clinical Ophthalmology 2022, 16:2385-2390
Published Date: 29 July 2022
Reproducibility of Neuroretinal Rim Measurements Obtained from High-Density Spectral Domain Optical Coherence Tomography Volume Scans
Kim J, Men CJ, Ratanawongphaibul K, Papadogeorgou G, Tsikata E, Ben-David GS, Antar H, Poon LYC, Freeman M, Park EA, Guzman Aparicio MA, de Boer JF, Chen TC
Clinical Ophthalmology 2022, 16:2595-2608
Published Date: 13 August 2022
Glaucoma Diagnosis Through the Integration of Optical Coherence Tomography/Angiography and Machine Learning Diagnostic Models
Kooner KS, Angirekula A, Treacher AH, Al-Humimat G, Marzban MF, Chen A, Pradhan R, Tunga N, Wang C, Ahuja P, Zuberi H, Montillo AA
Clinical Ophthalmology 2022, 16:2685-2697
Published Date: 18 August 2022
Steroid Response Following Dropless Cataract Surgery Using Subconjunctival Triamcinolone
Wu AM, Pitts KM, Pineda R, Chen SH, Wang M, Johnson G, Shen LQ, Margeta MA
Clinical Ophthalmology 2023, 17:2803-2814
Published Date: 22 September 2023
Travoprost Intracameral Implant in Eyes with Glaucoma or Ocular Hypertension: Early Short-Term Real-World Outcomes
Teymoorian S, Kaur J
Clinical Ophthalmology 2025, 19:157-166
Published Date: 16 January 2025