Back to Journals » Medical Devices: Evidence and Research » Volume 19
Quantifying Changes in Balance, Gait, Fall Risk, and Sensory Reweighting in Older Adults Following Multi-Session Electrical Vestibular Stimulation Therapy
Authors Ralston JD ![]() , Stanley S, Roper JM, Darici O, Peters RM
, Stanley S, Roper JM, Darici O, Peters RM
Received 19 December 2025
Accepted for publication 12 March 2026
Published 21 March 2026 Volume 2026:19 590344
DOI https://doi.org/10.2147/MDER.S590344
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Mohamad Bashir
John D Ralston,1 Scott Stanley,2 Joshua M Roper,1 Osman Darici,1,3 Ryan M Peters1,3– 5
1Neursantys Inc., Cupertino, CA, 95014, USA; 2Caring Hands Caregivers, Cupertino, CA, 95014, USA; 3Faculty of Kinesiology, University of Calgary, Calgary, Alberta, Canada; 4Department of Biomedical Engineering, University of Calgary, Calgary, Alberta, Canada; 5Hotchkiss Brain Institute, University of Calgary, Calgary, Alberta, Canada
Correspondence: John D Ralston, Email [email protected]
Objective: To assess the utility of digital biomarkers derived from a head-mounted wearable physiological vibration acceleration (phybrata) sensor for quantifying changes in balance, gait, fall risk, and sensory reweighting in older adults undergoing multi-session electrical vestibular stimulation therapy (eVST).
Methods: Data were collected and analyzed from 32 residents aged 60– 98 yrs from a continuing care retirement community before, during, and after the administration of an 18-session eVST treatment protocol delivered over a 4– 6-week period. Each session included subthreshold wideband stochastic electrical vestibular stimulation (swsEVS) for 20 minutes delivered using a wearable device. Balance performance, sensory reweighting, and fall risk were assessed immediately before and after treatment using a head-mounted phybrata sensor. Two additional standard balance tests, along with wearable-sensor-based gait assessments, were administered before the 1st and after the 18th treatment session.
Results: 30 of the 32 participants demonstrated significantly improved balance and gait performance and reduced fall risk following the 18-session eVST treatment protocol. Phybrata sensory reweighting profiles for the study participants as a group revealed significant recovery of vestibular balance regulation and decreased reliance on proprioception. Phybrata biomarkers were found to identify the 2 non-responders in the study population within the first 2 treatment sessions. The number of participants classified as “high fall risk” decreased from 19 to 4 following treatment. Significant stabilization of head movement was observed following eVST treatment using head-mounted sensors during gait tests over distances as short as 7.6m, with the largest reductions observed in the medial-lateral direction. Head-acceleration based gait biomarkers were found to be more sensitive to eVST-induced improvements than stride-to-stride gait parameters measured using foot-mounted sensors.
Conclusion: Phybrata digital biomarkers enable rapid objective assessment of changes in balance, gait, fall risk, and sensory reweighting in older adults before, during, and after a multi-session eVST treatment protocol.
Keywords: presbystasis, presbyvestibulopathy, age-related balance decline, electrical vestibular stimulation, phybrata, vestibular, proprioception, sensory reweighting, wearable sensor, biomarkers of aging, balance restoration, fall risk
Introduction
Declining balance and mobility, clinically referred to as presbystasis,1 significantly degrades overall health, increases the risk of falls, and hinders the ability of older adults to live actively, independently, and productively. Although many age-related changes contribute to presbystasis, studies of balance aging have identified vestibular dysfunction, clinically known as presbyvestibulopathy,2 and the resulting central nervous system sensory reweighting,3 as primary underlying causes of balance decline in older adults. The economic burden exceeds $280 billion annually in the U.S., with over $50 billion in direct medical expenses for falls4 and $230 billion in additional costs for post-acute care services, long-term care, productivity loss for patients and unpaid caregivers, and diminished quality of life.5 Despite this enormous economic impact, quantitative clinical evaluations of vestibular balance and mobility impairments require specialized laboratory equipment that most older adults and their care providers do not have access to, so they are limited to subjective, inconsistent, and outdated methods to assess functional decline.6–8 And even when vestibular dysfunction is diagnosed accurately, non-surgical restorative interventions are lacking.
The complex neuroplastic learning and development processes that enable human balance and locomotor stability continue into the teenage years.9 The central nervous system (CNS), which includes the brain and spinal cord, integrates visual, vestibular, and proprioceptive/somatosensory sensory inputs to generate motor control outputs. These signals are then transmitted to the musculoskeletal system via the peripheral nervous system (PNS) to enable standing upright, walking steadily, keeping objects in visual focus during head movements, and performing complex actions without losing balance. Progressive loss of functioning of all these systems with increasing age contributes to balance deficits.
More than 35% of U.S. adults over 40 years of age already suffer from age-related dysfunction in the vestibular balance system,10 often long before symptoms begin to be observed.11 Vestibular dysfunction has been identified as the primary cause of balance decline in more than 55% of adults over age 50, or around 70 million people in the U.S.12–15 Vestibular disorders significantly increase the risk of clinically significant outcomes such as falls, with studies revealing that individuals with diagnosed vestibular balance impairments had a 12-fold increase in the odds of falling, while individuals with non-specific balance dysfunction had a 2.6-fold increase in the odds of falling.10 The vestibular system consists of the peripheral vestibular balance organs, the vestibular nerve that transmits motion signals to the brain, the vestibular nucleus in the brainstem, and multiple brain regions that utilize this information. The wide distribution of vestibular sensory information throughout the CNS reflects its important role in supporting not just balance, but also many other physiological, cognitive, and psychological processes16,17 Presbyvestibulopathy in aging adults can include dysfunction in both the peripheral vestibular organs in the inner ear and central vestibular processing in the brain,18 significantly disrupting balance,14,19 gait,13 and vestibulo-ocular reflexes,11 increasing fall risk,20 and contributing to the onset and progression of cognitive decline.21,22
Loss of vestibular hair cells is a consequence of normal aging, weakening sensory outputs from the vestibular organs and triggering atrophy effects in other components of the vestibular system.15,18,23–26 These atrophy effects include decrease in the gain of the synapses between vestibular hair cells and the vestibular nerve, along with decreased neuronal excitability and axonal transmission along the vestibular nerve, all three of which further weaken the signals received by the brain. These weaker signals can in turn lead to decrease in the gain of the synapses in the vestibular nuclei and atrophy in those parts of the CNS that integrate and process sensory input and motor control output signals.
A key element of balance-related CNS processing is sensory reweighting (SR), a feature of neuroplasticity that allows the brain to continually assess the reliability and recalibrate the utilization of signals from various sensory systems.27,28 SR can occur dynamically (eg, in response to changing environmental factors such as poor lighting or unstable surfaces) or gradually over time (eg, in response to physiological changes such as vestibular hair cell loss, vision decline, or proprioceptive signal degradation). Reduced response time or accuracy of the SR process significantly increases fall risks.29 Evaluating SR is important to identify potential underlying causes of balance decline. In a previous study3 we have demonstrated that digital biomarkers derived from balance assessments using a wearable physiological vibration acceleration (phybrata) sensor can be used to quantify declining postural stability, underlying impairments across multiple balance system components, the resulting sensory reweighting, and increased fall risks in older adults. The results demonstrated clear progressive trends in declining balance performance and sensory reweighting, with decreased vestibular function offset by increased reliance on proprioception,30 across a wide range of age and balance performance.
The phybrata sensor is essentially a very sensitive seismometer for the human body, used to detect and analyze involuntary micro-movements of the head and body during standing balance and walking gait tests. The head-mounted design and tiny mass of the phybrata sensor enable the detection of unique spatial-, time-, and frequency-domain feature sets, including the separate contributions that each of the different physiological systems in the body make to the biomechanical stabilization of the head and eyes that enables stable balance and movement, by mapping them to specific vibrational frequency bands in the phybrata data.3
The current standard treatment for older adults diagnosed with vestibular decline, as well as many patients with other vestibular disorders or injuries, is vestibular rehabilitation therapy (VRT).31,32 VRT is an exercise-based regimen typically delivered by physical and occupational therapists who have specialized vestibular training. The mechanisms behind VRT include habituation to normalize the brain’s reaction to movements or visual environments that trigger dizziness; adaptation to recalibrate the brain’s response to remaining vestibular function and minimize discrepancies between vision and inner ear sensation; and substitution to help patients compensate for weakened vestibular inputs by relying more on vision and proprioception. However, VRT does not restore degraded vestibular function or prevent further deterioration. Prescription medications, known as vestibular suppressants, are available to alleviate acute symptoms such as dizziness, nausea, and vertigo.33,34 However, these drugs come with significant side effects and are usually prescribed for only a few days to manage acute symptoms. Since they have no prophylactic or therapeutic role, they are unsuitable for long-term treatment for older adults without acute symptoms, or as preventative interventions, and some have been shown to increase subsequent fall risk.35 Vestibular implants36,37 represent the only current option to restore vestibular function, but these experimental devices require a high-risk invasive surgical procedure and are limited to patients with severe damage or loss of their vestibular organs. Consequently, they are not expected to become a widely available or economically viable solution for normal age-related balance decline. When fall risks become critical, the most common solution offered to older adults is some combination of mobility assistive devices such as canes, walkers, or wheelchairs. However, these interventions may be counterproductive, since they can potentially exacerbate vestibular dysfunction and further degrade quality of life.38
A growing body of research suggests that non-invasive low-level noisy electrical vestibular stimulation (nEVS) is a promising approach to enhancing or restoring age-related decline in vestibular function, with potential diagnostic applications, therapeutic benefits, and mechanisms of action that are well documented.39–54 EVS stimulates vestibular hair cells and the vestibulocochlear nerve, and at amplitudes exceeding the human perceptual threshold (typically 0.5mA or greater) can evoke vestibular reflexes. Early applications included assessing neuromotor impairments in astronauts exposed to microgravity55 and reducing motion sickness in pilots training in flight simulators.56 Whereas EVS delivered at amplitudes above the perceptual threshold can degrade vestibular performance, nEVS has emerged as a promising safe and non-invasive restorative treatment for balance deficits,53,57 including in older adults.43,48–51 nEVS involves delivering imperceptible electrical currents to the vestibular organs and afferent neurons, typically via electrodes placed over the left and right mastoids. Multiple studies indicate that nEVS can restore both peripheral and central vestibular functions by inducing neuroplastic changes at the cellular level and in the connectivity of neural circuits.45–47,50,52 Changes in peripheral vestibular function may include regeneration of motion-sensing hair cells (stereocilia), enhanced synaptic transmission between stereocilia and the vestibular nerve, and enhanced neuronal excitability and axonal transmission along the vestibular nerve, all of which strengthen motion-related signals delivered to the brain.58–60 Changes in central vestibular function include increased synaptic gain in the vestibular nuclei and multiple forms of neuroplasticity that partially restore functional performance across sensory integration and motor control systems.61 These changes not only stabilize balance and movement but also enhance neuromotor control and sensory reweighting. It has also been proposed that low levels of noise applied to the vestibular system can enhance the detection of sub-threshold signals via a stochastic resonance mechanism,43,44,48,50,53,57 where the addition of noise enhances the detection of a signal that would otherwise be undetectable.
Electrical vestibular stimulation is also unique among sensory neuromodulation62 techniques because it targets the vestibular sensory organ to activate the brain’s endogenous neural pathways rather than forcing artificial currents directly into brain tissue, allowing the stimulation to be naturally transformed and integrated within regional neuronal dynamics and oscillatory networks. This access to broad, multisynaptic vestibular projections throughout brainstem, cerebellar, subcortical, and cortical systems offers potential therapeutic applications across diverse neurological conditions, trauma-related dysfunction, and age-related decline in balance, cognition, and motor control. Clinical applications of nEVS that have been explored include Meniere’s disease, vestibular neuritis, bilateral vestibular disorders, vestibular schwannoma, Parkinson’s disease, stroke, motor myelopathies, anxiety, cognitive disorders, memory disorders, insomnia, obesity, type 2 diabetes, and age-related balance decline.41,44,47,52,63–65
However, the above studies have shown that the effectiveness of EVS can vary widely, and not all choices of stimulation parameters are effective for improving postural control. Sensitivity to EVS is also known to differ between the sexes66 and change as a function of age.67 Two previous studies of nEVS stimulation in older adults demonstrated reductions in center of pressure motion and postural sway measured using force plates following a single treatment session, indicating improvement in postural stability, which persisted for several hours after stimulation.48,49 Two other previous studies have investigated the cumulative impact of repetitive EVS treatment sessions.51,54 One of these studies51 combined nEVS with a 6-week exercise-based treatment program in a cohort of 150 older adults (age 66±4 years), and demonstrated a significant improvement in balance and reduction in risk of falls in both the exercise-only group (N=50) and exercise+nEVS group (N=50) compared to the placebo group (N=50), and the treatment benefits were significantly larger when nEVS was included. However, the persistence of these effects was not assessed. The second of these studies54 combined EVS with a 4-week vestibular rehab therapy (VRT) in a cohort of 40 patients (age 43±8 years) diagnosed with unilateral peripheral vestibular weakness. The EVS+VRT group (N=20) demonstrated significantly larger improvements in both vestibular function (measured using videonystagmography) and postural stability (measured using computerized dynamic posturography) than the VRT-only group (N=20). The persistence of these effects was again not assessed.
nEVS has also been investigated to enhance human gait performance. Several studies have demonstrated that imperceptible nEVS can reduce stride-to-stride variability, improve bilateral coordination, and enhance dynamic walking stability in both healthy adults68 and patients with bilateral vestibulopathy.69 Others have reported increases in gait velocity and stride length with nEVS in healthy and vestibular-impaired participants,70 as well as reductions in step-width variability and improvements in trunk stability during balance-challenged walking tasks.71 Similar benefits have been observed in more demanding locomotor contexts such as treadmill walking with lateral perturbations72 and head-turning tasks under visual deprivation.73 While these findings support the potential of EVS to facilitate improvements in gait control, the interventions were generally limited to single-session or short-duration applications, with outcomes assessed only within the experimental session.
Despite a wide range of promising diagnostic and therapeutic applications, EVS has not yet been widely commercialized due to the challenge of assessing individual responses across a wide range of potential stimulation parameters. We have been able to overcome this challenge by utilizing phybrata sensors and biomarkers to monitor changes in test subjects’ balance performance, sensory reweighting, and fall risk in response to varying EVS waveforms and dosing regimens.74,75 This capability led to the development of a subthreshold (±0.35 mA) wideband (0 to 300 Hz) stochastic (noisy) EVS waveform (swsEVS) and an electrical vestibular stimulation therapy (eVST) treatment protocol (eighteen 20-minute swsEVS treatment sessions delivered over a 4-6-week period) that has produced significant and long-lasting increases in balance performance in study populations from 50–95 years of age.76–78 In a pilot randomized control trial (RCT) we have demonstrated persistence of 6 months or longer for eVST treatment group participants but not for sham control group participants.78 Pilot deployments in multiple senior living communities and physical therapy/neuro rehab clinics have demonstrated that eVST treatments are comfortable, well-tolerated, have no adverse side effects, and can be administered by medical staff with minimal training in any senior care location, including at-home care and in remote communities with limited healthcare access.78,79
Our previous eVST studies have been limited to the use of laboratory stimulation equipment and phybrata assessments of changes in static balance performance measures in a clinical setting. The present study expands the use of phybrata biomarkers to quantify changes in balance, gait, fall risk, and sensory reweighting in older adults following the above 18-session eVST treatment protocol delivered in a real-world senior living setting using a Neurvesta bioelectronic stimulation device79 (Neursantys Inc, Cupertino, CA). Changes in balance were also assessed using two standard balance tests: standing on 1 leg, a validated assessment of overall balance-related mortality risk;80 and standing on a foam pad with feet together and eyes closed to assess vestibular balance function.81 Changes in gait performance were assessed using 3 time-synchronized IMUs — 2 attached to the shoes and one attached to the mastoid — while patients walked distances of 7.6 m (25 feet) and 20 m on a hard surface wearing shoes. Gait biomarkers derived from the head-mounted sensor were compared with standard gait metrics derived from IMUs attached to the feet in terms of their sensitivity to eVST-induced performance changes. The present study does not include a sham control group. However, comparisons with our recent RCT indicate that the eVST-induced improvements observed here significantly exceed the small practice effects typically observed for sham participants.78
Methods
Participants
32 participants aged 83.7 ± 6.8 yrs (min 60 yrs, max 98 yrs, 23 female, 9 male) from a continuing care retirement community (The Forum at Rancho San Antonio, Cupertino, California) enrolled in and completed the 18-session study. Individuals with an implanted electronic device (pacemaker, cochlear implant), neurological disorder, vestibular disorder, or musculoskeletal condition that significantly impaired balance or mobility were excluded from the study. Participants were also required to have normal or corrected-to-normal vision.
Ethical Considerations
The study protocol is published on ClinicalTrials.gov (NCT06846047). The study was conducted in accordance with the Declaration of Helsinki with research ethics approval under the University of Calgary’s Conjoint Health Research Ethics Board (IRB Study Number REB22-1006), and written informed consent was obtained for all participants in the study. Participants provided written informed consent for publication of the images in Figures 1 and 2.
 |
Figure 1 Phybrata sensor attached to the mastoid using an adhesive patch. |
 |
Figure 2 NEURVESTA device attached using disposable electrodes. |
Test and Treatment Procedures
All balance and gait tests and eVST treatments were administered by research team members and trained home care providers in dedicated clinical office space at the Caring Hands Caregivers study site. Each of the 18 study sessions included 20 minutes of swsEVS dosing. During the first, second, 6th, and 18th sessions, 2-minute phybrata balance assessments were carried out for all participants immediately before and after the swsEVS dosing. During the first session, clinical staff at each center measured and recorded each participant’s date of birth, height, weight, and leg-length. Gait assessments and the two additional standard balance tests described above were also administered prior to the first treatment session and following completion of the 18th treatment session.
Phybrata balance testing was carried out on a hard floor with footwear removed as previously reported,3 with the test subject and administrator alone in a separate quiet windowless room to minimize distractions and resulting anomalous patient movements, and avoid the need for manual data cleaning.78 Tests with artefacts from anomalous patient movement can be readily identified by test administrators via visual inspection of the raw acceleration time series data presented by the mobile app. Less than three percent of all tests in this study were flagged — these tests were repeated immediately, and test data with motion artefacts was excluded from the analysis. The phybrata sensor was attached to the patient’s mastoid using a disposable medical adhesive, as shown in Figure 1, while standing still for 60 sec with eyes open (Eo) and then again for 60 sec with eyes closed (Ec). As in previous studies using the phybrata sensor, participants were instructed to stand upright in a relaxed position with their feet together and their arms at their sides while maintaining their gaze in a straight-ahead direction focused on a visual target mounted on the wall 10 feet away at eye level. Patients were also instructed not to talk or move during testing. The test administrator always stood by the subjects: (1) to monitor subjects’ postural sway throughout the trial; and (2) so that the subjects had no fear of falling during eyes-closed testing. Testing was repeated if any anomalous patient movement was observed during phybrata testing.
A smartphone app connects to the phybrata sensor via a Bluetooth low-energy (BLE) wireless link to configure and run tests, collect data, and interface with cloud-based data storage, analytics, and reporting services. The phybrata IMU includes a 3-axis accelerometer to record x (anterior-posterior (AP), or front-back), y (vertical), and z (medial-lateral (ML), or left-right) acceleration time series data in units of g. During each 60 sec test, data is recorded at a sampling rate of 100 Hz, generating a total of 6000 samples for each of the 3 axes (x, y, z). The accelerometer signals are filtered to remove drift, as in our previous studies with the same device,3,82–85 using a recursive high-pass filter with a 0.02 Hz cutoff frequency.
After the initial phybrata balance assessment, a Neurvesta bioelectronic stimulation device (Neursantys Inc, Cupertino, CA) was placed over the participant’s shoulders and attached to 2 pairs of disposable pre-gelled electrodes (Ambu Blue Sensor SP, Ballerup, Denmark) placed on both mastoid processes and on both sides of the back of the neck beside the spine at the level of the C4 vertebrae (Figure 2). The skin was cleaned with an alcohol swab before attaching the electrodes. Electrode impedance between each mastoid-C4 pair bilaterally was typically between ~3-8 kΩ. Neurvesta balance treatments were administered in a larger communal room, typically with groups of 2–4 participants at a time. Participants were seated and not required to complete any specific physical tasks during the 20 minutes of swsEVS dosing. Immediately after treatment, the Neurvesta device and electrodes were removed, and participants waited 5 minutes before repeating phybrata balance assessments.
During each of the 18 eVST treatment sessions, participants received 20 minutes of continuous swsEVS dosing (±0.35 mA peak-to-peak amplitude, 0 to 300 Hz), as in our previously reported RCT.78 The uniform white noise signal was band-pass filtered (4th order Butterworth) between 0.001 and 300 Hz, and output at a rate of 5 kHz from the Neurvesta device. Previous research has indicated that individuals typically begin to perceive vestibular sensations around 0.9–1.0 mA, with cutaneous sensations such as tingling or prickling occurring at similar or slightly lower intensities (0.85 mA).66 The eVST protocol uses ±0.35 mA to maximize participant comfort, and recent studies have shown that this amplitude is sufficient to activate vestibulospinal pathways despite the user being perceptually unaware of the stimulation.86 Brain imaging studies have shown that broadband nEVS, relative to narrow-band or sinusoidal EVS, is more effective at activating vestibular cortical areas.46,87 A bandwidth of 0–300 Hz was chosen because recent primate studies indicate that 300 Hz is the highest frequency vestibular afferents are capable of encoding.46,88 Participants also received a low-amplitude current pulse (“tap”) at the electrodes at the beginning of the stimulation interval to alert them that the session had started.
Two additional standard balance tests were also administered before the 1st and after the 18th treatment session: standing on 1 leg to asses overall balance;80 and standing on a foam pad with feet together and eyes closed to assess vestibular balance function.81 Similar to the phybrata tests, these two additional balance tests were carried out with the test subject and administrator alone in a separate quiet windowless room to avoid any distractions.
Gait performance was also measured before the 1st and after the 18th treatment session using 3 time-synchronized IMUs, 2 of which were attached to the shoes, and one attached to the mastoid. Patients walked 2 different distances — 7.6 meters and 20 meters — on a hard surface wearing shoes. Gait performance over each distance was measured twice before and after the eVST treatment. We chose 20 meters because it is long enough to see changes in acceleration patterns of the body and head in healthy89 and impaired90 study populations. We chose 7.6 meters (25 feet) because the 25-foot walk test is convenient and typical distance used for gait testing in clinical settings.91
Data Processing
For each pair of standing balance tests (60 sec Eo followed by 60 sec Ec), Eo and Ec phybrata powers (in watts) were calculated as previously described3,78,82,83 by summing over the time series data using the combined magnitude of the accelerations along all three axes (accelx,y,z) and assuming a reference mass moving under these accelerations,82 providing a direction-independent measure of postural stability:
Phybrata power = Σt (accelx,t2 + accely,t2 + accelz,t2) * mB * Δt * g2
where mB = 1.3kg is the reference mass undergoing the measured acceleration (average mass of the human brain82), Δt = 0.01sec is the accelerometer sampling interval, and g = 9.81m/sec2 is the gravitational constant (to convert accelerometer output in units of g into units of m/sec2), which gives phybrata power in units of kg m2/sec3 = watts.
Sensory reweighting profiles were derived for each participant as previously described3,83,92,93 by using a Fast Fourier Transform (FFT) of the raw accelerometer data to derive the Acceleration Spectral Density (ASD) for each of the directional components. For the FFT calculation, zero-padding was added to increase the number of acceleration signal data points to the next power of 2. Relative reliance on specific mechanisms of postural control was quantified by calculating the normalized sum of the three directional components across five frequency bands in the phybrata ASD frequency spectra: 0.02–0.1 Hz (visual regulation); 0.1–0.5 Hz (vestibular regulation); 0.5–1 Hz (CNS participation, both cerebellar and cortical); 1–10Hz (spinal reflexive loops, proprioception, multi-joint and muscle activity); 10–25 Hz (vestibulocollic head stabilization).
Figure 3 shows sample Eo and Ec x, y, z phybrata time series signals for a study participant prior to the first eVST treatment session (Figure 3a) and following completion of the 18th eVST treatment session (Figure 3b). The three acceleration traces illustrate the raw AP, vertical, and ML head-motion signals, respectively, used to quantify balance performance. After treatment, the overall amplitude and variability of the acceleration signals are visibly reduced, particularly along the medial-lateral axis, indicating improved postural stability and finer control of head motion during quiet stance.
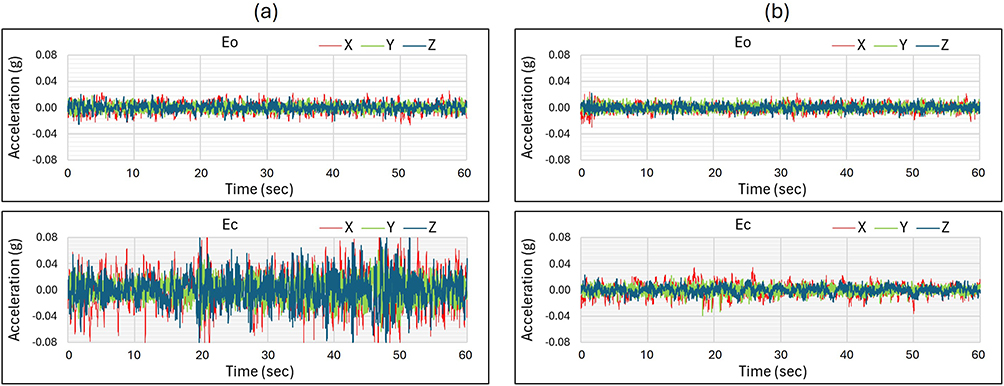 |
Figure 3 Sample raw x (anterior-posterior (AP), or front-back), y (vertical), and z (medial-lateral (ML) or left-right) phybrata acceleration time series data for a test subject during 60-second eyes open (Eo) and eyes closed (Ec) standing balance tests (a) before beginning and (b) after completing the 18-seesion eVST treatment. |
Figure 4 presents the corresponding AP/ML phybrata spatial scatter plots and phybrata power bar graphs for the same study participant as in Figure 3 during 60-second Eo and Ec standing balance tests, prior to the first eVST treatment session (Figure 4a) and following completion of the 18th eVST treatment session (Figure 4b). The two-dimensional acceleration distributions (anterior–posterior vs. medial-lateral) show a tighter, more centralized cluster of data points after treatment, reflecting reduced sway excursions for both Eo and Ec. The accompanying bar graphs in Figure 4a and b confirm a marked reduction in total phybrata power from pre- to post-eVST, quantitatively consistent with improved balance performance.
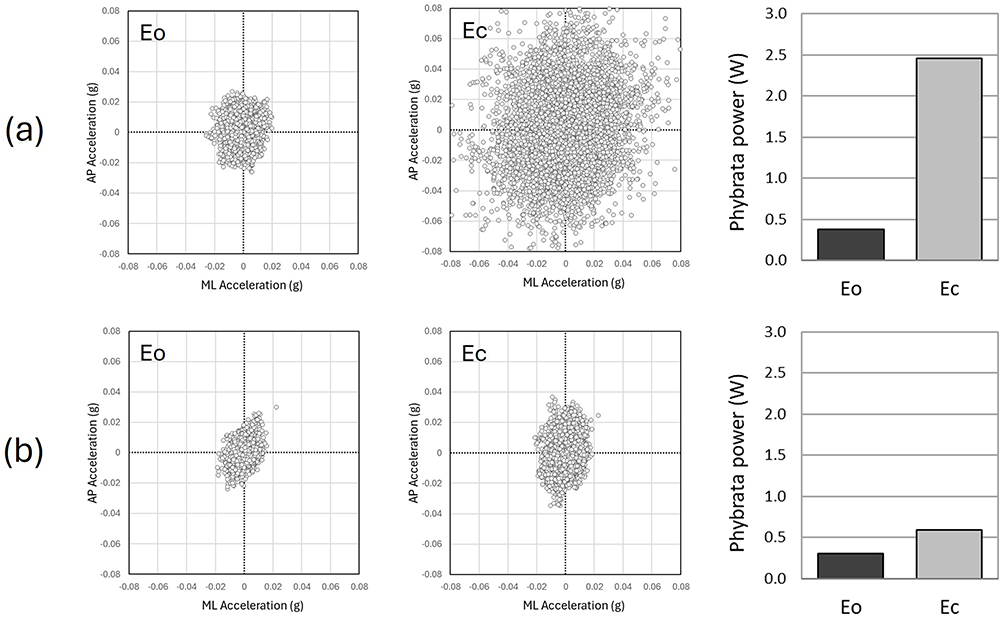 |
Figure 4 Sample phybrata anterior-posterior (AP) / medial-lateral (ML) acceleration spatial scatter plots and total phybrata powers for the same test subject as in Figure 3 during 60-second eyes open (Eo) and eyes closed (Ec) standing balance tests (a) before beginning and (b) after completing the 18-seesion eVST treatment. |
Figure 5 presents the Ec sensory-reweighting profiles derived from the same participant’s acceleration spectral density distributions prior to the first eVST treatment session and following completion of the 18th eVST treatment session. The post-treatment SR profile reveals increased power within the vestibular band and decreased power within the proprioceptive band, signifying a functional shift toward enhanced vestibular regulation and reduced reliance on proprioceptive control. This representative example captures the characteristic redistribution of sensory weighting observed across participants following repeated eVST dosing, essentially reversing the impact of age-related vestibular loss on SR that we have previously reported.3
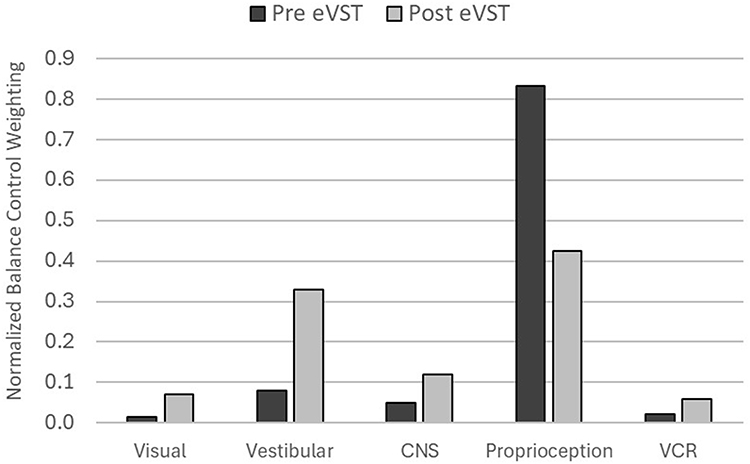 |
Figure 5 Eyes closed sensory reweighting profiles derived from acceleration spectral density distributions for the same test subject as in Figures 3 and 4, prior to beginning and following completion of the 18-session eVST treatment. |
Gait speed, stride length and width, and step time were calculated from the IMU’s on the feet using inertial navigation techniques that we have previously reported.94–96 Foot trajectories were computed from an IMU mounted on top of each foot. Gravity-compensated accelerations were integrated to yield foot velocity by assuming that each foot comes briefly to rest when it is flat on the ground during each footfall. These midstance instances were used to correct the integrated foot velocity to zero during each stride and the foot position was calculated by integrating the corrected velocity. Given that our gait assessments are restricted to straight walking and the absolute heading of the IMU’s are not known, the forward walking direction was estimated from a linear fit of seven successive footfall locations. We then rotated each foot path to align it to the estimated forward direction. The forward direction and gravity vector together define the local lateral direction. Stride length is then defined as the distance between two discrete footfall (midstance) instants of the same foot along the forward direction, and stride time is defined as the time duration between these footfall instances. Stride width is defined as the lateral deviation of the foot from the forward trajectory path. Step time is defined as the time difference between subsequent left and right footfalls. The variabilities of stride length, stride width, stride time, and step time are defined as the standard deviation of the corresponding parameters. The trial time for each run was calculated as the time difference between the instances when the acceleration magnitude of the foot that takes the first step exceeds a threshold of 1 m/sec2 (relative to gravity) and the acceleration magnitude of the foot that takes the last step drops below the same threshold. The trial distance was calculated as the average integrated forward distance travelled by both feet at the end of the trial assuming their initial position is zero. The average gait speed for each trial was calculated by dividing the trial distance by the trial time.
For the head IMU, we corrected the gravity compensated acceleration to have zero mean, based on the assumption that the head IMU began moving from zero speed and ended at zero speed. We then integrated this acceleration to find head speed and integrated the head speed to estimate head position. As was the case for the foot-mounted IMU’s, we did not know the absolute heading, but unlike the feet, the head-mounted IMU does not have well-defined midstance rest durations that can be used to correct integration errors in the head position calculated by integrating head velocity. Nevertheless, a principal component analysis (PCA) showed that more than 99% of the variability in head position was explained by the first PCA vector. In other words, the direction of the head remained constant along this principal direction during our straight walking gait trials, allowing us to assume that the first PCA component represents the forward direction of the head. We then rotated the gravity compensated and zero mean head acceleration to be aligned with the forward direction, allowing us to use the forward direction and gravity vector to determine the lateral head direction. From the head acceleration in forward, lateral, and vertical acceleration we calculated the root mean square (RMS) variability in total head power and head powers in each direction, to assess changes due to the eVST treatment.
Statistical Analysis
All statistical analysis were performed in R, fitting separate linear mixed effects models (LMMs) using the “lmer” function in the “lme4” package. For both balance and gait, the eVST treatment is the main effect. For the standing balance data, we analyzed separate LMMs for Eo and Ec conditions, both with “Session” (sessions 1, 2, 6, and 18) as a fixed factor, and subject as a random factor. For the gait data, we quantified the significant gait differences of the treatment by fitting two separate LMMs for each walking distance, 7.6m and 20m, with “Session” (session 1 vs 18) as a fixed factor, and subject as a random factor. When we had a significant effect of eVST treatment, we performed a post-hoc analysis on the estimated marginal means using Bonferroni correction. The confidence intervals (CI) for significant post-hoc comparisons are reported as CI_L (CI low) and CI_H (CI high). All statistical analyses were performed with R Statistical Software (version 2025.05.1+513), using an alpha level of 0.05.
An a priori power analysis was performed for the primary balance metrics based on effect sizes observed in our prior sham-controlled EVS balance study78 using comparable phybrata-derived metrics. Using those previously reported between-session reductions in total phybrata power for the stimulation group we performed a power analysis for the Ec condition and concluded 22 subjects is enough to provide 80% power to detect similar within-subject treatment effects at α = 0.05. For gait outcomes, however, this investigation represents the first multi-session (18-session) EVS study assessing longitudinal effects on gait stability; therefore, no directly comparable effect size estimates were available to inform an a priori calculation. As such, gait analyses should be considered exploratory and hypothesis-generating. To address potential false-negative risk and improve interpretability, we report effect sizes and 95% confidence intervals for all primary and secondary outcomes. Future randomized controlled trials with larger samples will use the present gait effect size estimates to perform fully powered a priori sample size determinations.
Results
30 of the 32 participants demonstrated significantly improved balance and gait performance and reduced fall risk following the 18-session eVST treatment protocol (“responders”). 2 of the 32 participants demonstrated no significant changes (“non-responders”). No adverse events were reported during the study. Figure 6 presents box-whisker plots illustrating the changes in Eo and Ec phybrata powers for the 30 responders. Both Eo (F3,87 = 28.15, p = 8.11e-13) and Ec (F3,87 = 32.43, p = 3.61e-14) phybrata head accelerometer powers decreased significantly with the eVST treatment sessions. Overall, the Eo phybrata power decreased 35.80% (p = 3.29e-12, CI_L = 0.116, CI_H = 0.226, ES = 1.16) between the first and the 18th eVST treatment sessions. The Eo phybrata power decreased 17.48% (p = 4.87e-04, CI_L = 0.029, CI_H = 0.138, ES = 1.00) between the first and second eVST treatment sessions and 15.25% (p =0.022, CI_L = 0.005, CI_H = 0.114, ES = 0.74) between the second and 6th treatment sessions. The difference between the 6th and 18th treatments was not significant. Overall, the Ec phybrata power decreased 62.02% (p = 9.53e-14, CI_L = 0.585, CI_H = 1.070, ES = 1.12) between the first and the 18th eVST treatment sessions. The Ec phybrata power decreased 35.78% (p = 4.77e-6, CI_L = 0.235, CI_H = 0.720, ES = 1.05) between the first and second eVST treatment sessions, and 69.08% (p = 0.0011, CI_L = −0.592, CI_H = −0.107, ES = 0.89) from the second to the 18th treatment session. The changes between the second and the 6th treatment sessions, and between the 6th and the 18th treatment sessions were not significant.
 |
Figure 6 Eo and Ec phybrata power box-whisker plots for 30 responders. Note: *p ≤ 0.05. |
Figure 7 presents phybrata sensory reweighting plots for study participants as a group prior to beginning and after completing the 18-session eVST treatment protocol. Separate plots are shown for Eo (Figure 7a) and Ec (Figure 7b). Relative changes in reliance on specific mechanisms of postural control were quantified by calculating relative changes within the five frequency bands in the normalized phybrata ASD frequency spectra defined above, corresponding to visual regulation, vestibular regulation, CNS participation, proprioceptive regulation, and vestibulocollic head stabilization. The normalized sensory reweighting plots in Figure 7 are calculated by integrating over time and frequency in each of the five ASD frequency bands for each individual and then averaging each band over all 32 study participants. Figure 7 reveals a significant eVST-induced redistribution across the five spectral bands following the 18-session treatment, with restoration of vestibular balance regulation and a decreased reliance on proprioceptive balance control. For Eo, we found significant effects of the treatment for the vestibular (F1,31 = 41.8, p = 3.28e-7), proprioceptive (F1,31 = 21.25, p = 6.55e-5), and CNS processing (F1,31 = 28.76, p = 7.57e-6) frequency bands. Specifically, the vestibular (54.14%, CI_L = 0.094, CI_H = 0.181, ES = 1.14) contribution to postural stabilization increased, whereas CNS processing (−31.52%, CI_L = −0.047, CI_H = −0.021, ES = 0.94) and the proprioceptive (−23.22%, CI_L = −0.13661450, CI_H = −0.05280862, ES = 0.81) contribution decreased. Similarly, for the eyes closed condition, we found significant effects of the treatment for the vestibular (F1,31 = 44.83, p = 1.72e-7), proprioceptive (F1,31 = 18.08, p = 0.00018), and CNS processing (F1,31 = 28.34, p = 1.72e-7) frequency bands. Specifically, the vestibular contribution (50.92%, CI_L = 0.095, CI_H = 0.179, ES = 1.18) increased, while the CNS processing (−32.24%, CI_L = 0.066, CI_H = −0.029, ES = 0.94) and the proprioceptive (−24.48%, CI_L = −0.163, CI_H = −0.057, ES = 0.75) contribution to postural stabilization decreased.
 |
Figure 7 (a) Eyes open and (b) Eyes closed phybrata sensory reweighting plots for study participants as a group prior to beginning and following completion of the 18-session eVST treatment. Note: *p ≤ 0.05. |
Figure 8 presents gait performance measured with sensors on the head at the start and end of the 18-session eVST treatment for the 30 responders. The two trials at the start and again at the end were averaged for each subject and are shown as a single data point. We found significant effects of the treatment in head acceleration for both 20-meter and 7.6-meter trials. For the 20-meter walk, the total RMS head acceleration power on average decreased 17.04% (F1,89 = 23.38, P = 5.5e-6, CI_L = −0.024, CI_H = −0.0102, ES = 0.55). The average forward, lateral and vertical RMS head acceleration powers all decreased: forward −19.15% (F1,89 = 6.69, P = 0.011, CI_L = −0.009, CI_H = −0.001, ES = 0.21); lateral −26.78% (F1,89 = 23.98, P = 4.3e-6, CI_L = 0.008, CI_H = −0.003, ES = 0.74); vertical −14.16% (F1,89 = 17.28, P = 7.4e-5, CI_L = −0.01, CI_H =−0.005, ES = 0.45), respectively. For the 7.6-meter walk, the total RMS head acceleration power on average decreased 10.25% (F1,89 = 9.95, P = 0.0021, CI_L = −0.011, CI_H = −0.002, ES = 0.30). The average lateral and vertical RMS head acceleration powers decreased significantly: lateral −19.38% (F1,89 = 15.99, P = 0.00013, CI_L = −0.004, CI_H = −0.001, ES = 0.67); vertical −7.81% (F1,89 = 5.03, P = 0.027, CI_L = −0.007, CI_H = −0.0004, ES = 0.22), respectively. The forward RMS head acceleration power also decreased, but not significantly: forward −12.79% (F1,89 = 3.79, P = 0.054, CI_L = −0.004, CI_H = 0.00004, ES = 0.11). Significant changes were also observed in some of the gait parameters derived from the foot-mounted IMUs. Step time variability and stride width variability on average decreased 19.58% (F1,89 = 8.93, P = 0.0036, CI_L = −0.020, CI_H = −0.004, ES = 0.44) and 11.08% (F1,89 = 6.72, P = 0.011, CI_L = −0.007, CI_H = −0.001, ES = 0.36), respectively for the 20-meter walk. For the 7.6-meter walk, stride width variability on average decreased 14.12% (F1,89 = 4.09, P = 0.046, CI_L = −0.010, CI_H = −0.00009, ES = 0.52) but the step time variability was not significantly different.
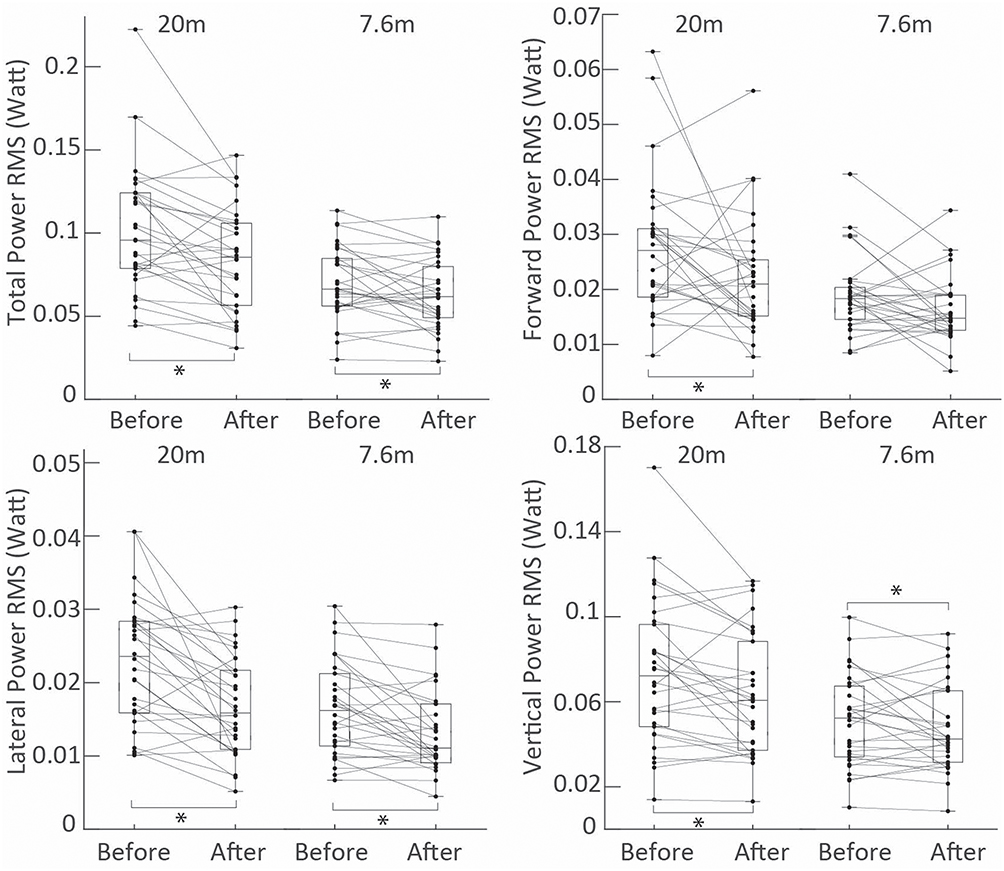 |
Figure 8 Gait performance for the 30 responders measured over 20m and 7.6m with sensors on the head prior to beginning and following completion of the 18-session eVST treatment. Significant decreases in the total RMS head acceleration power and all three directional components (lateral, forward, and vertical) are observed over 20m, and in the total and lateral RMS head acceleration powers over 7.6m. Note: *p ≤ 0.05. |
Figure 9 summarizes results of the additional balance performance tests and fall risk assessments for all 32 study participants. A McNemar’s chi-square test with continuity correction was conducted to evaluate the statistical significance of the changes observed for the 32 participants. The number of participants able to stand for a full minute on a foam balance pad with eyes closed increased from 14 to 27 (χ2(1) = 11.08, p = 0.001), demonstrating substantial recovery of vestibular balance function. Those capable of maintaining a single-leg stance for at least 10 seconds with eyes open on a hard floor increased from 6 to 17 for the left leg (χ2(1) = 9.09, p = 0.003)) and from 8 to 19 for the right leg (χ2(1) = 9.09, p = 0.003), indicating significant improvements in unilateral balance control. The number of participants classified as “high fall risk” based on their Ec phybrata performance3 was reduced from 19 to 4 after treatment (χ2(1) = 13.07, p = 0.0003). These results indicate statistically significant (α = 0.01) improvements in balance performance and fall risk. Many participants also self-reported immediate improvements in balance and walking within the first two treatment sessions, consistent with the results presented in Figure 6.
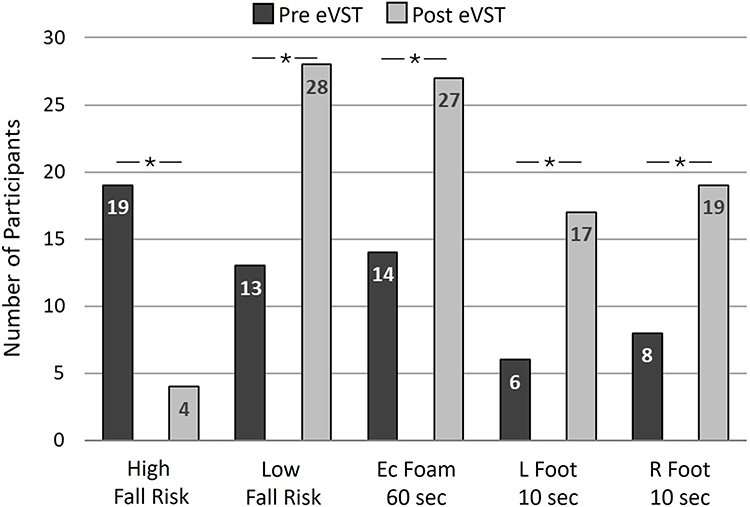 |
Figure 9 Summary of changes in fall risk and balance performance measures for all 32 pilot participants. Note: *p ≤ 0.05. |
Figure 10 presents Eo and Ec phybrata powers for the 2 non-responders. Figure 11 presents sensory reweighting profiles for the 2 non-responders, derived from phybrata test data captured prior to the first eVST treatment session. These results reveal that non-responders can be identified in the first two treatment sessions by a combination of 3 phybrata biomarkers:
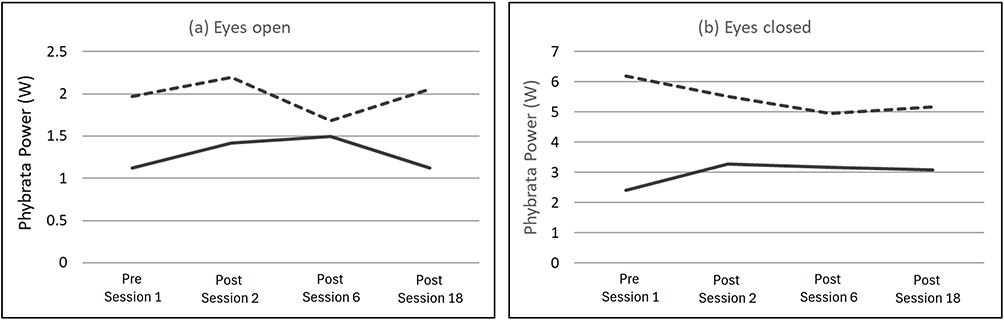 |
Figure 10 (a) Eyes open (Eo) and (b) eyes closed (Ec) phybrata powers for 2 non-responder study participants, illustrating Eo and Ec powers above a threshold of 2W. |
 |
Figure 11 Phybrata sensory reweighting profiles derived from phybrata test data captured prior to the first eVST treatment session for 2 non-responder study participants, illustrating (a) large reduction in vestibular contribution to balance control, (b) a decrease in the vestibular contribution from eyes open (Eo) to eyes closed (Ec) testing. |
(i) Eo (Figure 10a) and Ec (Figure 10b) Phybrata powers above a threshold of 2W (Figure 10), indicating seriously impaired balance.
(ii) Normalized vestibular sensory reweighting contributions below a threshold of 0.15 (Figure 11a), indicating very little remaining vestibular contribution to balance control.
(iii) A decrease in the vestibular sensory reweighting contribution from Eo to Ec testing (Figure 11b) that is accompanied by a large increase in proprioceptive balance control, indicating that the CNS has already adapted to rely on proprioception rather than vestibular balance control when visual input is reduced.
These behaviors essentially identify individuals whose balance impairment is already very large, and their vestibular function has deteriorated too far to respond to the standard eVST treatment protocol.
Discussion
We have previously demonstrated that digital biomarkers derived from a single head-mounted phybrata sensor during Eo and Ec standing balance tests provide objective assessments of progressive age-related balance impairments and sensory reweighting, underlying physiological contributions, and related intrinsic fall risks in older populations.3 The present study uses these same phybrata balance tests and biomarkers, and additional gait tests and biomarkers, to quantify the corresponding restoration of balance and mobility and reduction of fall risk in older adults resulting from an 18-session eVST treatment protocol. Phybrata sensory reweighting biomarkers reveal a corresponding recovery of vestibular balance regulation that is offset by decreased reliance on proprioceptive balance control.
eVST-Induced Improvements in Balance
The magnitude and consistency of the observed reductions in phybrata power across the eighteen treatment sessions demonstrate that cumulative eVST dosing produces progressive stabilization of head motion during quiet stance. These findings are consistent with our recent RCT trial in older adults utilizing a prototype eVST electronics module (Neursantys Inc, Cupertino, CA), in which significant reductions in postural phybrata power were observed beginning within the first week of treatment and persisting for up to six months following treatment completion.78 The present community-based pilot extends those findings by confirming that similar improvements can be achieved outside laboratory settings, using home-care providers and a portable non-invasive wearable neurostimulation device to deliver eVST treatments. Importantly, the improvements were evident in both eyes-open and eyes-closed conditions, implying that eVST can enhance vestibular contributions to balance even when visual information is available. The accompanying changes in sensory reweighting profiles—characterized by increased weighting of vestibular balance control and reduced reliance on proprioception—may indicate a functional recovery of vestibular regulation. Together, these results provide evidence that repeated eVST sessions promote recalibration of sensory integration networks, allowing older adults to depend more effectively on vestibular cues for postural stability during static balance tasks.
eVST-Induced Improvements in Gait
In addition to static balance, the present findings demonstrate significant improvements in gait performance following the 18-session eVST treatment protocol. Head-acceleration-based biomarkers are observed to be sensitive to eVST-induced improvements even in short (7.6m) clinical walking tests, whereas longer walking distances (20m) are required to capture changes in stride-to-stride gait parameters measured using foot-mounted IMUs. Head acceleration power decreased across all directions during both short (7.6 m) and long (20 m) walks, with the largest reductions in the medial-lateral direction. This is a significant result because, among gait acceleration components, medial–lateral acceleration has been shown to be most strongly associated with fall risk in older adults, reflecting impaired lateral balance control during walking.97 Balance control during walking relies heavily on controlling side-to-side motion of the body’s center of mass. Aging is associated with declines in hip abductor strength, sensory integration, and neuromuscular coordination, all of which are critical for mediolateral stability. Increased variability or magnitude of medial–lateral head acceleration reflects poorer dynamic balance and reduced ability to respond to perturbations. Anterior–posterior acceleration is more related to gait speed and propulsion; while informative, it is less predictive of falls. Vertical acceleration reflects step impact and leg stiffness but shows weaker and less consistent associations with fall risk.
Reductions in stride-to-stride variability of step time and stride width during the longer 20 m walks further indicate enhanced dynamic balance and gait consistency. The absence of significant variability changes in the shorter 7.6 m gait test results using foot-mounted IMUs is likely due to the limited number of strides available for analysis, but the head-based IMU metrics were nonetheless able to capture eVST-related improvements even in these short, clinically feasible protocols. The combination of head biomarkers over short walking distances and stride-level improvements over longer walks highlights both the mechanistic impact of eVST on gait control and the practical potential for monitoring clinical changes with brief, accessible gait tests.
The present findings extend the growing body of work showing that subthreshold noisy EVS can acutely improve walking performance in both healthy individuals and patients with vestibular impairment. Previous studies have demonstrated reduced gait variability and enhanced dynamic stability in healthy individuals,68,72 increased gait velocity and stride length in both normals and patients with bilateral vestibulopathy,70 and improved coordination and reduced stride variability in bilateral vestibulopathy patients.69 Others have reported reductions in trunk sway and step-width variability in balance-challenged walking tasks71 and improvements in stability under visual deprivation.73 However, these studies were limited to short, single-session exposures, with transient in-session effects measured only during or immediately after stimulation. Our structured, multi-week protocol and longitudinal study design provide evidence that repeated eVST sessions not only elicit immediate improvements but also lead to persistent adaptations in head and gait stability, likely reflecting cumulative neuroplastic changes within vestibular and sensorimotor pathways. The combined evidence from the present study and our previous RCT78 suggests that eVST may promote both immediate improvements due to stochastic resonance while the stimulation is being applied (and potentially short-lasting after-effects) and longer-term neural adaptations that consolidate improved balance and gait performance.
Possible Mechanisms
Several mechanisms may underlie these improvements. At the peripheral level, subthreshold EVS likely modulates vestibular afferent firing from both otolith and semicircular canal hair cells,45 enhancing the encoding of small head movements98 and compensating for age-related reductions in hair-cell sensitivity.50 Repeated stimulation may also support limited regeneration or functional recovery of vestibular hair cells and synaptic transmission, as suggested by histological evidence of residual regenerative capacity in older human utricles.99
At the central level, cumulative eVST dosing may induce neuroplastic changes within the vestibular nuclei, cerebellum, and associated cortical regions.41 Evidence from animal and human studies has shown changes in the expression of AMPA and NDMA receptors within the vestibular nuclei following repeated stimulation, suggesting neuroplasticity has occurred.46,100 The observed persistence of balance and gait improvements months after treatment cessation reported in our previous RCT78 further supports a neuroplastic mechanism rather than transient stochastic resonance alone. Such adaptations likely enhance the efficiency of vestibulospinal reflexes and improve the dynamic weighting of vestibular inputs during complex postural and locomotor tasks.
Clinical Significance
Research into aging has identified many biomarkers that can quantify biological age and monitor underlying molecular and physiological changes in older adults.101–103 However, progress has been much slower in translating these findings into clinically effective interventions that extend healthspan.104 The 2015 World Health Organization report on “World Health and Aging”105 highlighted the importance of minimizing the rate of decline in multiple domains of intrinsic capacity that impact healthspan. Interventions that can turn back epigenetic clocks or reduce inflammatory markers are only a preliminary step towards enhancing key domains of intrinsic capacity in older adults.102 Vestibular dysfunction is now known to trigger a downward spiral that impacts multiple domains of intrinsic capacity, including sensory, locomotion, cognition, and psychological capacity.18,21,106
The results presented here address key challenges that have impeded access to widely available diagnosis and treatment for declining vestibular function. From a translational perspective, the ability to track age-related vestibular decline and eVST-induced improvements using a single head-mounted phybrata sensor offers a practical, scalable approach for quantifying physiological aging and recovery. The phybrata biomarkers used here are sensitive enough to detect treatment responses after only two sessions and could distinguish non-responders early in the intervention, which limits costs and unproductive time for payers, providers, and patients alike. Compared to traditional balance and gait assessments, these phybrata metrics provide high-resolution quantitative insight into sensory reweighting and neural recovery, supporting the development of personalized neuromodulation therapies for fall prevention. The significant improvements in balance performance and reductions in fall risk illustrated in Figure 9 further highlight the functional and clinical benefits of combing phybrata assessments and eVST treatments.
Given the substantial healthcare costs associated with falls and fall-related injuries, effective strategies for early detection and treatment of balance decline could yield significant patient-centered and system-level benefits. Balance decline contributes to fear of falling, activity restriction, and progressive deconditioning, creating a self-reinforcing cycle of functional loss.107 Detecting impairment before this cascade becomes entrenched allows clinicians to intervene when adaptive capacity and neuroplastic potential remain relatively preserved. The present findings suggest the possibility of shifting from purely compensatory approaches toward interventions that more directly target underlying sensory dysfunction. This proactive approach aligns with current models of preventive geriatrics and supports maintenance of mobility, participation, and quality of life. A recent health economics assessment of the current eVST solution108 quantified the substantial unmet clinical need for better diagnosis and management of vestibular dysfunction and highlighted how the present phybrata and eVST innovations address these inefficiencies through proactive detection and functional restoration of declining balance in older adults.
The potential scalability of wearable diagnostic and therapeutic technologies further enhances their clinical relevance. Together with the simplicity and safety of the wearable stimulation system, the results reported here position eVST as a feasible intervention that can be deployed in outpatient, rehabilitation, senior living, long-term-care, home-based, and community settings. Combining phybrata and eVST can expand access to balance assessment and intervention, particularly for older adults with limited mobility or access to specialty care.
Combining phybrata and eVST can also enable a closed-loop stimulation approach, which is a rapidly evolving research area in non-invasive brain stimulation.109 Since the optimal swsEVS stimulus to deliver may depend on the current balance impairment profile, changes in this profile throughout treatment can impact patient response. Together with our previous balance impairment studies,3 the current results, demonstrate that phybrata sensory reweighting profiles can be using to quantify each patient’s unique balance impairment profile at the outset of treatment and unique response trajectory throughout treatment. We have recently developed a machine learning classifier that processes phybrata sensor data during eVST therapeutic treatment sessions to assess the effectiveness of each individual treatment session and the cumulative response over multiple treatment sessions.110 The resulting phybrata response biomarkers establish the foundation for a closed-loop, adaptive, hyper-personalized eVST therapy framework that optimizes treatment parameters based on continuous objective monitoring of individual patient response.
The Importance of Head Stabilization
An additional clinically important implication of our work is the emphasis on head stabilization as a core mechanism underlying both standing balance and walking gait stability. The results discussed here indicate that age-related vestibular decline impairs the ability to stabilize the head in space, which not only reduces postural stability, but also disrupts gaze control, trunk alignment, and step-to-step consistency during locomotion. Because vestibular signals are referenced to head motion, inadequate head stabilization increases sensory noise during gait, forcing greater reliance on visual and proprioceptive/somatosensory inputs that are frequently degraded in older adults. This destabilization is particularly evident during walking, when rhythmic head movements must be precisely regulated to maintain visual acuity and dynamic equilibrium.
These findings have important gait-specific clinical implications, especially in situations that challenge attentional and sensory integration demands. During dual-task walking, older adults with vestibular impairment often demonstrate disproportionate increases in head motion, gait variability, and instability,111 reflecting limited capacity to allocate attentional resources to head and postural control simultaneously. This helps explain why dual-task gait assessments are strong predictors of fall risk112 and why interventions that improve head stabilization may enhance performance under cognitively demanding conditions. Improved head control may also enhance visual sampling and environmental awareness during ambulation, further reducing fall susceptibility.
Head stabilization also has direct relevance to the use and prescription of assistive devices. While canes and walkers may improve base of support, they do not directly address head–trunk coordination and may, in some cases, promote downward gaze or altered head posture that further degrades vestibular input. Interventions such as eVST that target vestibular function and head stabilization could complement assistive device use by improving upright head posture, gaze stability, and confidence during walking, thereby optimizing overall mobility rather than compensating solely at the level of the lower extremities.
Finally, impaired head stabilization during gait may serve as a valuable biomarker for fall prediction. Excessive or irregular head motion during walking has been associated with reduced dynamic stability and increased fall risk in older adults.97 By highlighting improvements in balance outcomes linked to vestibular-focused interventions, the present results underscore the potential utility of head-motion metrics—captured via wearable sensors—as clinically actionable indicators of fall risk and treatment response. Collectively, these findings position head stabilization not as a secondary byproduct of improved balance, but as a central diagnostic and therapeutic target for enhancing balance and gait stability and reducing falls in aging populations.
Limitations and Future Studies
While the present study describes innovations in both diagnostics and treatments and reports promising outcomes, several limitations should be acknowledged.
Generalizability of Pilot Data
The absence of a sham control group prevents us from fully isolating stimulation-specific effects; however, comparisons with our recent RCT78 indicate that improvements observed here significantly exceed the small practice effects typically seen in sham conditions. The sample size of 32 was modest and the participants were predominantly female, precluding robust subgroup analyses by sex or age. Larger and more diverse samples are needed to confirm these findings, examine dose-response relationships, and explore how stimulation parameters (eg, frequency content, amplitude, or duration) influence outcomes. The present study was also carried out in a single senior living location — replicating the results in more diverse settings and including more comprehensive functional baselines will be important extensions of the study. The ability to identify potential non-responders early in the treatment process is of significant potential value, but the ability to generalize this result is limited by the small sample size and post-hoc identification of corresponding phybrata biomarkers. Larger controlled trials will be required to determine the degree to which the combination of phybrata biomarkers identified in the current study can serve as the basis for a prospectively testable rule. Moreover, this study focused on standing balance and straight-line walking and did not assess dynamic gait adaptability, obstacle negotiation, and real-world mobility to fully characterize the therapeutic benefits of eVST. Larger controlled trials will also be required for confirmation and external validation of the present results, including ecologically valid tasks to assess changes in fall risk.
Mechanistic Understanding
EVS is unique among sensory neuromodulation techniques in terms of the large number of vestibular projections that can be accessed throughout brainstem, cerebellar, subcortical, and cortical systems.62 As a result, it has diagnostic and therapeutic applications across diverse neurological conditions, trauma-related dysfunction, and age-related decline in balance, cognition, and motor control. Phybrata digital biomarkers and IMU gait metrics both show functional improvements following eVST treatment, and these changes are consistent with a hypothesized recalibration of sensory integration, favoring increased vestibular contribution. However, underlying physiological mechanisms were not assessed directly in the present study. The precise biological mechanisms by which electrical stimulation induces enduring neuroplastic recovery in vestibular systems — particularly in the context of age-related degeneration — require deeper exploration.
The assignment of frequency bands to specific neural systems in the present sensory reweighting analysis relies primarily on indirect associations between control latencies and spectral content in previously reported studies, rather than direct neural recordings from these pathways. While some studies have demonstrated correlational relationships between sensory manipulations and frequency shifts, direct evidence that specific frequency bands exclusively reflect particular neural systems remains limited. Although the results presented here are consistent with widely reported trends in sensory, CNS, and neuromotor contributions to postural stabilization, future studies should investigate in more detail the potential overlap between these frequency bands, variations across study populations, and individual variations as a function of time, impairments, and interventions.
Technology Adoption Barriers
Wearable sensors and bioelectronic devices, while more accessible than traditional lab equipment, still require integration into routine clinical practice, reimbursement pathways, and clinician training. There may be variability in uptake across care settings, especially in resource-limited contexts.
To build on these early findings, future studies should include:
Larger-scale, sham-controlled, double-blinded, multi-site clinical trials with longer follow-up and direct fall/outcomes tracking to evaluate the longer-term efficacy and cost-effectiveness of wearable diagnostic tools and multi-session bioelectronic treatments compared with standard care, across broader demographic and clinical subgroups.
Mechanistic research investigating how neuroplastic changes induced by eVST interact with aging neural circuits to restore balance control, and how these changes correlate with clinical outcomes like fall rates and functional independence. Previous studies of the oculomotor responses to EVS113 have shown that the resulting eye-movement is the sum of the contributions of the oculomotor drive of all the vestibular end organs. Compared with healthy individuals, patients with a variety of clinical vestibular conditions showed systematic differences in EVS-induced eye-movement patterns that were consistent with the reduction or absence of oculomotor contributions from the specific end organs impacted by their particular vestibular condition. Future studies should add comprehensive vestibular excitatory response testing2,114 (VNG/VOR, VEMP, vHIT, fHIT, caloric testing, rotary chair testing) to assess and distinguish between age-related decline and eVST-related changes that are specific to peripheral vestibular functions (otoliths vs. semi-circular canals) vs. central vestibular processing. Future studies investigating eVST-induced changes in the neural mechanisms underlying postural stability115,116 are also warranted. Future studies should also investigate eVST-induced changes in the critical vestibular balance stabilizing mechanisms that accompany transitions between motor states that link balance and gait, such as between quiet standing and locomotion, between different standing postures, and during locomotion termination.117
Implementation science studies focusing on best practices for integrating these technologies into primary care, rehabilitation, and community-based settings, including evaluation of clinician training models, patient adherence, and health system barriers to real-world implementation.
Comparative effectiveness research examining how emerging noninvasive treatments perform relative to or synergistically with established therapies such as VRT or multicomponent fall prevention programs.
Conclusions
The present study demonstrates that multi-session eVST produced significant and durable enhancements in both balance and gait among older adults, mediated by improved vestibular regulation and sensory reweighting. These findings, consistent with controlled laboratory results, provide new evidence that eVST can restore vestibular function and enhance locomotor stability in older adults, with head-motion-based phybrata biomarkers offering a practical means of detecting treatment effects even in short, clinically feasible walking tests compatible with ecologically valid, community-based environments. The combination of wearable sensor and stimulation technologies offers a practical pathway toward accessible, personalized, and data-driven interventions to mitigate age-related balance decline and fall risk.
Abbreviations
Phybrata, physiological vibration acceleration; EVS, electrical vestibular stimulation; eVST, electrical vestibular stimulation therapy; swsEVS, subthreshold wideband stochastic EVS; nEVS, noisy EVS; Eo, eyes open; Ec, eyes closed; ASD, acceleration spectral density; IMU, inertial motion unit; CNS, central nervous system; PNS, peripheral nervous system; SR, sensory reweighting; VRT, vestibular rehabilitation therapy; RCT, randomized control trial; BLE, Bluetooth low energy; AP, anterior-posterior; ML, medial-lateral; PCA, principal component analysis; RMS, root mean square; LMM, linear mixed effects models; ES, effect size; VNG, Videonystagmography; VOR, Vestibulo-Ocular Reflex; VEMP, Vestibular-Evoked Myogenic Potentials; vHIT, video Head Impulse Test; fHIT, functional Head Impulse Test.
Data Sharing Statement
All data are included in this article.
Acknowledgments
The authors wish to thank: the staff and residents at the Forum at Rancho San Antonio (Cupertino, CA) senior living communities for their support in scheduling and coordinating on-site phybrata testing; the team members at Caring Hands Caregivers (Cupertino, CA), and Neursantys Inc. (Cupertino, CA) who supported data collection; and Andreas Hauenstein for support in developing and maintaining the mobile app and cloud data platform used in this study. PROTXX Inc. provided the phybrata sensors, mobile app, and cloud data platform used in this study. Neursantys provided the Neurvesta bioelectronic stimulation devices used in this study.
Disclosure
John Ralston is the co-founder and CEO of Neursantys and has a financial interest in the company. Josh Roper is the co-founder and Vice President of Operations at Neursantys and has a financial interest in the company. Ryan Peters is the Chief Science Officer of Neursantys and has a financial interest in the company. Osman Darici is the Director of Biomechanics at Neursantys. Scott Stanley is the CEO of Caring Hands Caregivers, and a member of the Neursantys Advisory Board. In addition, John Ralston and Ryan Peters have a USPTO patent 17/671,176 pending to Neursantys Inc., and John Ralston, Ryan Peters, and Osman Darici have a USPTO patent application 19/368,983 pending to Neursantys Inc. The authors report no other conflicts of interest in this work. The authors also declare that steps taken to reduce potential bias include the use of a standardized study protocol and objective sensor metrics, along with independent test and treatment delivery vs. statistical analysis and verification responsibilities.
References
1. Teggi R, Familiari M, Battista RA, et al. The social problem of presbystasis and the role of vestibular rehabilitation in elderly patients: a review. Acta Otorhinolaryngol Ital. 2023;43(4):227–24. doi:10.14639/0392-100X-N1908
2. Agrawal Y, Van de Berg R, Wuyts F, et al. Presbyvestibulopathy: diagnostic criteria consensus document of the classification committee of the Bárány Society. J Vestib Res. 2019;29(4):161–170. doi:10.3233/VES-190672
3. Ralston JD, Stanley S, Roper JM, Ralston AB. Phybrata digital biomarkers of age-related balance impairments, sensory reweighting, and intrinsic fall risk. Med Devices. 2025;18:319–336. doi:10.2147/MDER.S522827
4. Florence CS, Bergen G, Atherly A, Burns E, Stevens J, Drake C. The medical costs of fatal falls and fall injuries in older adults. J Am Geriatr Soc. 2018;66(4):693–698. doi:10.1111/jgs.15304
5. Agrawal Y, Pineault KG, Semenov YR. Health-related quality of life and economic burden of vestibular loss in older adults. Laryngoscope Investig Otolaryngol. 2017;3(1):8–15. doi:10.1002/lio2.129
6. Beck Jepsen D, Robinson K, Ogliari G, et al. Predicting falls in older adults: an umbrella review of instruments assessing gait, balance, and functional mobility. BMC Geriatr. 2022;22(1):615. doi:10.1186/s12877-022-03271-5
7. Newman-Toker DE, Cannon LM, Stofferahn ME, Rothman RE, Hsieh YH, Zee DS. Imprecision in patient reports of dizziness symptom quality: a cross-sectional study conducted in an acute care setting. Mayo Clin Proc. 2007;82:1329–11340. doi:10.4065/82.11.1329
8. Pardasaney PK, Slavin MD, Wagenaar RC, Latham NK, Ni P, Jette AM. Conceptual limitations of balance measures for community-dwelling older adults. Phys Ther. 2013;93(10):1351–1368. doi:10.2522/ptj.20130028
9. Steindl R, Kunz K, Schrott-Fischer A, Scholtz AW. Effect of age and sex on maturation of sensory systems and balance control. Dev Med Child Neurol. 2006;48(6):477–482. doi:10.1017/S0012162206001022
10. Agrawal Y, Ward BK, Minor LB. Vestibular dysfunction: prevalence, impact and need for targeted treatment. J Vestib Res. 2013;23(3):113–117. doi:10.3233/VES-130498
11. Baloh RW, Enrietto J, Jacobson KM, Lin A. Age-related changes in vestibular function: a longitudinal study. Ann N Y Acad Sci. 2001;942:210–219. doi:10.1111/j.1749-6632.2001.tb03747.x
12. Davis LE. Dizziness in elderly men. J Am Geriatr Soc. 1994;42(11):1184–1188. doi:10.1111/j.1532-5415.1994.tb06986.x
13. Iwasaki S, Yamasoba T. Dizziness and imbalance in the elderly: age-related decline in the vestibular system. Aging Dis. 2014;6(1):38–47. doi:10.14336/AD.2014.0128
14. Agrawal Y, Merfeld DM, Horak FB, et al. Aging, vestibular function, and balance: proceedings of a National institute on aging/National institute on deafness and other communication disorders workshop. J Gerontol A Biol Sci Med Sci. 2020;75(12):2471–2480. doi:10.1093/gerona/glaa097
15. Wagner AR, Akinsola O, Chaudhari AMW, Bigelow KE, Merfeld DM. Measuring vestibular contributions to age-related balance impairment: a review. Front Neurol. 2021;12:635305. doi:10.3389/fneur.2021.635305
16. Lopez C, Blanke O. The thalamocortical vestibular system in animals and humans. Brain Res Rev. 2011;67(1–2):119–146. doi:10.1016/j.brainresrev.2010.12.002
17. Kirsch V, Keeser D, Hergenroeder T, et al. Structural and functional connectivity mapping of the vestibular circuitry from human brainstem to cortex. Brain Struct Funct. 2016;221(3):1291–1308. doi:10.1007/S00429-014-0971-X
18. Agrawal Y, Smith PF, Merfeld DM. Dizziness, imbalance and age-related vestibular loss. Senses. 2020;6:567–580. doi:10.1016/B978-0-12-809324-5.23818-2
19. Roman-Liu D. Age-related changes in the range and velocity of postural sway. Arch Gerontol Geriatr. 2018;77:68–80. doi:10.1016/j.archger.2018.04.007
20. Liston MB, Bamiou DE, Martin F, et al. Peripheral vestibular dysfunction is prevalent in older adults experiencing multiple non-syncopal falls versus age-matched non-fallers: a pilot study. Age Ageing. 2014;43(1):38–43. doi:10.1093/ageing/aft129
21. Smith PF. Aging of the vestibular system and its relationship to dementia. Curr Opin Neurol. 2024;37(1):83–87. doi:10.1097/WCO.0000000000001231
22. Obermann M, Gebauer A, Arweiler-Harbeck D, et al. Cognitive deficits in patients with peripheral vestibular dysfunction. Eur J Neurol. 2025;32(1):e15907. doi:10.1111/ene.15907
23. Coto J, Alvarez CL, Cejas I, et al. Peripheral vestibular system: age-related vestibular loss and associated deficits. J Otol. 2021;16(4):258–265. doi:10.1016/j.joto.2021.06.001
24. Madrigal J, Arbelaez-Lelion D, Candelo E, et al. Clinical and otopathologic findings on age-related vestibular loss: state of the art review. Int J Otorhinolaryngol Head Neck Surg. 2023;9(7):602–612. doi:10.18203/issn.2454-5929.ijohns20231822
25. Allen D, Ribeiro L, Arshad Q, Seemungal BM. Age-related vestibular loss: current understanding and future research directions. Front Neurol. 2016;7:231. doi:10.3389/fneur.2016.00231
26. Bergström B. Morphology of the vestibular nerve. II. The number of myelinated vestibular nerve fibers in man at various ages. Acta Otolaryngol. 1973;76(2):173–179. doi:10.3109/00016487309121496
27. Peterka RJ. Sensorimotor integration in human postural control. J Neurophysiol. 2002;88(3):1097–1118. doi:10.1152/jn.2002.88.3.1097
28. Assländer L, Peterka RJ. Sensory reweighting dynamics in human postural control. J Neurophysiol. 2014;111(9):1852–1864. doi:10.1152/jn.00669.2013
29. Zhang S, Xu W, Zhu Y, Tian E, Kong W. Impaired multisensory integration predisposes the elderly people to fall: a systematic review. Front Neurosci. 2020;14:411. doi:10.3389/fnins.2020.00411
30. Pasma JH, Engelhart D, Maier AB, Schouten AC, van der Kooij H, Meskers CG. Changes in sensory reweighting of proprioceptive information during standing balance with age and disease. J Neurophysiol. 2015;114(6):3220–3233. doi:10.1152/jn.00414.2015
31. Deveze A, Bernard-Demanze L, Xavier F, Lavieille JP, Elziere M. Vestibular compensation and vestibular rehabilitation. Current concepts and new trends. Neurophysiol Clin. 2014;44(1):49–57. doi:10.1016/j.neucli.2013.10.138
32. Han BI, Song HS, Kim JS. Vestibular rehabilitation therapy: review of indications, mechanisms, and key exercises. J Clin Neurol. 2011;7(4):184. doi:10.3988/jcn.2011.7.4.184
33. Biswas A. Vestibular sedative drugs – reducing misuse why and how. Available from: https://www.vertigoclinic.in/vestibularsedative-drugs-reducing-misuse-why-and-how/.
34. Viola P, Gioacchini FM, Astorina A, et al. The pharmacological treatment of acute vestibular syndrome. Front Neurol. 2022;13:999112. doi:10.3389/fneur.2022.999112
35. Adams ME, Karaca-Mandic P, Marmor S. Meclizine use and subsequent falls among patients with dizziness. JAMA Otolaryngol Head Neck Surg. 2025. doi:10.1001/jamaoto.2025.2052
36. Guyot JP, Perez Fornos A. Milestones in the development of a vestibular implant. Curr Opin Neurol. 2019;32(1):145–153. doi:10.1097/WCO.0000000000000639
37. Hansen JO, Sass HCR, West NC, Cayé-Thomasen P. Methods and clinical outcomes in vestibular implantation – a systematic literature review. J Vestibular Res. 2025;35(4):172–184. doi:10.1177/09574271251332157
38. Andersen DA, Roos BA, Stanziano DC, Gonzalez NM, Signorile JF. Walker use, but not falls, is associated with lower physical functioning and health of residents in an assisted-living environment. Clin Interv Aging. 2007;2(1):123–137. doi:10.2147/ciia.2007.2.1.123
39. Wuehr M, Decker J, Schniepp R. Noisy galvanic vestibular stimulation: an emerging treatment option for bilateral vestibulopathy. J Neurol. 2017;264(Suppl 1):81–86. doi:10.1007/s00415-017-8481-4
40. Haxby F, Akrami M, Zamani R. Finding a balance: a systematic review of the biomechanical effects of vestibular prostheses on stability in humans. J Funct Morphol Kinesiol. 2020;5(2):23. doi:10.3390/jfmk5020023
41. Dlugaiczyk J, Gensberger KD, Straka H. Galvanic vestibular stimulation: from basic concepts to clinical applications. J Neurophysiol. 2019;121(6):2237–2255. doi:10.1152/jn.00035.2019
42. Herssens N, McCrum C. Stimulating balance: recent advances in vestibular stimulation for balance and gait. J Neurophysiol. 2019;122(2):447–450. doi:10.1152/jn.00851.2018
43. White O, Babič J, Trenado C, Johannsen L, Goswami N. The promise of stochastic resonance in falls prevention. Front Physiol. 2019;9:1865. doi:10.3389/fphys.2018.01865
44. Lajoie K, Marigold DS, Valdés BA, Menon C. The potential of noisy galvanic vestibular stimulation for optimizing and assisting human performance. Neuropsychologia. 2021;152:107751. doi:10.1016/j.neuropsychologia.2021.107751
45. Kwan PAF, Mitchell DE, Blouin J-S, Cullen KE. Neural substrates, dynamics and thresholds of galvanic vestibular stimulation in the behaving primate. Nat Commun. 2019;10(1):1904. doi:10.1038/s41467-019-09738-1
46. Lopez, Cullen KE, Lopez C. Electrical stimulation of the peripheral and central vestibular system. Curr Opin Neurol. 2024;37(1):40–51. doi:10.1097/WCO.0000000000001228
47. de Á. Pires PB, Silva TR, Torres MS, Diniz ML, Tavares MC, Gonçalves DU. Galvanic vestibular stimulation and its applications: a systematic review. Braz J Otorhinolaryngol. 2022;88:S202–S211. doi:10.1016/j.bjorl.2022.05.010
48. Fujimoto, Fujimoto C, Yamamoto Y, et al. Noisy galvanic vestibular stimulation induces a sustained improvement in body balance in elderly adults. Sci Rep. 2016;6(1):37575. doi:10.1038/srep37575
49. Inukai Y, Masaki M, Otsuru N, et al. Effect of noisy galvanic vestibular stimulation in community-dwelling elderly people: a randomised controlled trial. J Neuroeng Rehabil. 2018;15(1):63. doi:10.1186/s12984-018-0407-6
50. Serrador JM, Deegan BM, Geraghty MC, Wood SJ. Enhancing vestibular function in the elderly with imperceptible electrical stimulation. Sci Rep. 2018;8(1):336. doi:10.1038/s41598-017-18653-8
51. Jain A, Sarkar A, Gupta M. Optimizing balance using vestibular electrical stimulation to study its therapeutic effect among elderly. Biosci Biotechnol Res Commun. 2022;15(2):313–320. doi:10.21786/bbrc/15.2.8
52. Marchand S, Langlade A, Legois Q, et al. A wide-ranging review of galvanic vestibular stimulation: from its genesis to basic science and clinical applications. Exp Brain Res. 2025;243:131. doi:10.1007/s00221-025-07079-8
53. Valter Y, Vataksi L, Allred AR, et al. A review of parameter settings for galvanic vestibular stimulation in clinical applications. Front Hum Neurosci. 2025;19:1518727. doi:10.3389/fnhum.2025.1518727
54. Ahmed R, Fahmy EM, Awad AM, et al. Efficacy of transmastoidal galvanic stimulation on recovery outcomes in patients with unilateral peripheral vestibular disorders: a randomized controlled trial. Egypt J Neurol Psychiatry Neurosurg. 2020;56:75. doi:10.1186/s41983-020-00207-x
55. Soto E, Vega R. Use of galvanic vestibular stimulation device as a countermeasure for microgravity effects in spaceflight. Front Space Technol. 2024;5:1422868. doi:10.3389/frspt.2024.1422868
56. Cevette MJ, Stepanek J, Cocco D, et al. Oculo-vestibular recoupling using galvanic vestibular stimulation to mitigate simulator sickness. Aviat Space Environ Med. 2012;83(6):549–555. doi:10.3357/asem.3239.2012
57. McLaren R, Smith PF, Taylor RL, Niazi IK, Taylor D. Scoping out noisy galvanic vestibular stimulation: a review of the parameters used to improve postural control. Front Neurosci. 2023;17:1156796. doi:10.3389/fnins.2023.1156796
58. Huang Y, Mao H, Chen Y. Regeneration of hair cells in the human vestibular system. Front Mol Neurosci. 2022;15:854635. doi:10.3389/fnmol.2022.854635
59. Walters B, Cox B, Stone J. Regeneration of sensory hair cells in mature mammals. Curr Top Dev Biol. 2025;165:307–351. doi:10.1016/bs.ctdb.2025.04.002
60. Gensberger KD, Kaufmann AK, Dietrich H, et al. Galvanic vestibular stimulation: cellular substrates and response patterns of neurons in the vestibulo-ocular network. J Neurosci. 2016;36(35):9097–9110. doi:10.1523/JNEUROSCI.4239-15.2016
61. Mitsutake T, Sakamoto M, Kawaguchi A, Tamari M, Horikawa E. Greater functional activation during galvanic vestibular stimulation is associated with improved postural stability: a GVS-fMRI study. Somatosens Mot Res. 2020;37(4):257–261. doi:10.1080/08990220.2020.1803256
62. Black RD, Rogers LL. Sensory Neuromodulation. Front Syst Neurosci. 2020;14:12. doi:10.3389/fnsys.2020.00012
63. Cheung T, Lam JYT, Fong KH, et al. Evaluating the Efficacy of Electrical Vestibular Stimulation (VeNS) on insomnia adults: study protocol of a double-blinded, randomized, sham-controlled trial. Int J Environ Res Public Health. 2023;20(4):3577. doi:10.3390/ijerph20043577
64. Viirre E, Sittlington J, Wing D, et al. Non-invasive vestibular nerve stimulation (VeNS) reduces visceral adipose tissue: results of a randomised controlled trial. Sci Rep. 2025;15(1):8753. doi:10.1038/s41598-025-92744-9
65. Goothy SSK, McKeown J, Mcgeoch D, et al. Electrical vestibular nerve stimulation as an adjunctive therapy in the management of type 2 diabetes. J Basic Clin Physiol Pharmacol. 2020;32(6):1075–1082. doi:10.1515/jbcpp-2020-0210
66. Nguyen TT, Kang JJ, Oh SY. Thresholds for vestibular and cutaneous perception and oculomotor response induced by galvanic vestibular stimulation. Front Neurol. 2022;13:955088. doi:10.3389/fneur.2022.955088
67. Jahn K, Naessl A, Schneider E, et al. Inverse U-shaped curve for age dependency of torsional eye movement responses to galvanic vestibular stimulation. Brain. 2003;126(Pt 7):1579–1589. doi:10.1093/brain/awg163
68. Wuehr M, Nusser E, Krafczyk S, et al. Noise-enhanced vestibular input improves dynamic walking stability in healthy subjects. Brain Stimulation. 2016;9:109–116. doi:10.1016/j.brs.2015.08.017
69. Wuehr M, Nusser E, Decker J, et al. Noisy vestibular stimulation improves dynamic walking stability in bilateral vestibulopathy. Neurology. 2016;86(23):2196–2202. doi:10.1212/WNL.0000000000002748
70. Iwasaki S, Fujimoto C, Egami N, et al. Noisy vestibular stimulation increases gait speed in normals and in bilateral vestibulopathy. Brain Stimulation. 2018;11(4):709–715. doi:10.1016/j.brs.2018.03.005
71. Piccolo C, Bakkum A, Marigold DS. Subthreshold stochastic vestibular stimulation affects balance-challenged standing and walking. PLoS One. 2020;15:e0231334. doi:10.1371/journal.pone.0231334
72. Mulavara AP, Kofman IS, De Dios YE, et al. Using low levels of stochastic vestibular stimulation to improve locomotor stability. Front Syst Neurosci. 2015;9:117. doi:10.3389/fnsys.2015.00117
73. Chen PY, Jheng Y-C, Wang -C-C, et al. “Effect of noisy galvanic vestibular stimulation on dynamic posture sway under visual deprivation in patients with bilateral vestibular hypofunction. Sci Rep. 2021;11:4229. doi:10.1038/s41598-021-83206-z
74. Ralston JD, Banman CJ, Peters RM. Phybrata-based assessments of sensory reweighting due to postural stability challenges and electrical vestibular stimulation.
75. Ralston JD, King JA, Rempel J, Peters RM, Chima B. Phybrata Biomarker Assessments of Age-Related Balance Impairments and EVS Balance Restoration. In: 2023 Biomarkers of Aging Symposium. Novato, California, USA: Buck Institute for Research on Aging; 2023 Dec 4.
76. Ralston JD, King J, Rempel J, Peters RM. Wearable Bioelectronic Balance Restoration in Older Adults. In AGEWELL Annual Conf. Oct 24-26 2023; Toronto, Ontario.
77. King JA, Banman CJ, Walters N, Clark S, Ralston JD, Peters RM. Electrical vestibular stimulation therapeutics for balance and gait in older adults.
78. King JA, Walters N, Rodrigues N, et al. Electrical vestibular stimulation to improve balance in older adults: a pilot randomized controlled trial. J NeuroEng Rehab. 2025;22(1):231. PMID: 41174737; PMCID: PMC12577125. doi:10.1186/s12984-025-01749-y
79. Ralston JD, King JA, Peters RM. PHYBRATA – novel Neuromotor Systems Biomarkers to Quantify Normal Age-Related Decline in Balance and Mobility, Accelerated Aging Caused by Disease and Trauma, and EVS Balance Restoration. In: 2024 Biomarkers of Aging Symposium. Boston, Massachusetts, USA: Harvard Medical School; 2024 November 1-2.
80. Araujo CG, de Souza E Silva CG, Laukkanen JA, et al. Successful 10-second one-legged stance performance predicts survival in middle-aged and older individuals. Br J Sports Med. 2022;56(17):975–980. doi:10.1136/bjsports-2021-105360
81. Anson E, Bigelow RT, Studenski S, Deshpande N, Agrawal Y. Failure on the foam eyes closed test of standing balance associated with reduced semicircular canal function in healthy older adults. Ear Hear. 2019;40(2):340–344. doi:10.1097/AUD.0000000000000619
82. Grafton ST, Ralston AB, Ralston JD. Monitoring of postural sway with a head-mounted wearable device: effects of gender, participant state, and concussion. Med Devices. 2019;12:151–164. doi:10.2147/MDER.S205357
83. Ralston JD, Raina A, Benson BW, Peters RM, Roper JM, Ralston AB. Physiological Vibration Acceleration (Phybrata) sensor assessment of multi-system physiological impairments and sensory reweighting following concussion”. Med Devices. 2020;13:411–438. doi:10.2147/MDER.S279521
84. Hope A, Vashisth U, Parker M, Ralston AB, Roper JM, Ralston JD. Phybrata sensors and machine learning for enhanced neurophysiological diagnosis and treatment. Sensors. 2021;21:7417. doi:10.3390/s21217417
85. Abdollah V, Dief TN, Ralston JD, Ho C, Rouhani H. Investigating the validity of a single tri-axial accelerometer mounted on the head for monitoring the activities of daily living and the timed-up and go test. Gait Posture. 2021;90:137–140. doi:10.1016/j.gaitpost.2021.08.020
86. Simoneau M, Nooristani M, Blouin JS. Balance control threshold to vestibular stimuli. J Physiol. 2025;603:2783–2799. doi:10.1113/JP288016
87. Mitsutake T, Sakamoto M, Horikawa E. Comparing activated brain regions between noisy and conventional galvanic vestibular stimulation using functional magnetic resonance imaging. NeuroReport. 2021;32(7):583–587. doi:10.1097/WNR.0000000000001629
88. Forbes PA, Kwan A, Mitchell DE, Blouin J-S, Cullen KE. The neural basis for biased behavioral responses evoked by galvanic vestibular stimulation in primates. J Neurosci. 2023;43(11):1905–1919. doi:10.1523/JNEUROSCI.0987-22.2023
89. Menz HB, Lord SR, Fitzpatrick RC. Acceleration patterns of the head and pelvis when walking on level and irregular surfaces. Gait Posture. 2003;18(1):35–46. doi:10.1016/s0966-6362(02)00159-5
90. Latt MD, Menz HB, Fung VS, Lord SR. Acceleration patterns of the head and pelvis during gait in older people with Parkinson’s disease: a comparison of fallers and nonfallers. J Gerontol A Biol Sci Med Sci. 2009;64(6):700–706. doi:10.1093/gerona/glp009
91. Kalinowski A, Cutter G, Bozinov N, et al. The timed 25-foot walk in a large cohort of multiple sclerosis patients. Mult Scler. 2022;28(2):289–299. doi:10.1177/13524585211017013
92. Heydari S, Lacey C, Stewart-Good K, Mayo C, Ralston JD, Gawryluk JR. The relationship between phybrata wearable sensor data and white matter microstructure in people with multiple sclerosis.
93. Lei Y, Rios V, Ji J, Duhon B, Boyd H, Xu Y. Quantifying unsupported sitting posture impairments in humans with cervical spinal cord injury using a head-mounted IMU sensor. Spinal Cord. 2024;62(2):65–70. doi:10.1038/s41393-023-00951-w
94. Ojeda LV, Rebula JR, Kuo AD, Adamczyk PG. Influence of contextual task constraints on preferred stride parameters and their variabilities during human walking. Med Eng Phys. 2015;37(10):929–936. doi:10.1016/j.medengphy.2015.06.010
95. Carlisle RE, Kuo AD. Optimization of energy and time predicts dynamic speeds for human walking. Elife. 2023;12:e81939. doi:10.7554/eLife.81939
96. Darici O, Kuo AD. Humans plan for the near future to walk economically on uneven terrain. Proc Natl Acad Sci U S A. 2023;120(19):e2211405120. doi:10.1073/pnas.2211405120
97. Rispens SM, van Schooten KS, Pijnappels M, Daffertshofer A, Beek PJ, van Dieën JH. Identification of fall risk predictors in daily life measurements: gait characteristics’ reliability and association with self-reported fall history. Neurorehabil Neural Repair. 2015;29(1):54–61. doi:10.1177/1545968314532031
98. Keywan A, Wuehr M, Pradhan C, Jahn K. Noisy galvanic stimulation improves roll-tilt vestibular perception in healthy subjects. Front Neurol. 2018;9:83. doi:10.3389/fneur.2018.00083
99. Taylor RR, Jagger DJ, Saeed SR, et al. Characterizing human vestibular sensory epithelia for experimental studies: new hair bundles on old tissue and implications for therapeutic interventions in ageing. Neurobiol Aging. 2015;36(6):2068–2084. doi:10.1016/j.neurobiolaging.2015.02.013
100. Kim G, Lee S, Kim KS. Repeated galvanic vestibular stimulation modified the neuronal potential in the vestibular nucleus. Neural Plast. 2020;2020:5743972. doi:10.1155/2020/5743972
101. Lu JK, Wang W, Mahadzir MDA, et al. Digital biomarkers of ageing for monitoring physiological systems in community-dwelling adults. Lancet Healthy Long. 2025;6(6):100725. doi:10.1016/j.lanhl.2025.100725
102. Fuentealba M, Rouch L, Guyonnet S, et al. A blood-based epigenetic clock for intrinsic capacity predicts mortality and is associated with clinical, immunological and lifestyle factors. Nat Aging. 2025;5(7):1207–1216. doi:10.1038/s43587-025-00883-5
103. Moqri M, Herzog C, Poganik JR, et al. Validation of biomarkers of aging. Nat Med. 2024;30(2):360–372. doi:10.1038/s41591-023-02784-9
104. Herzog CMS, Goeminne LJE, Poganik JR, et al. Challenges and recommendations for the translation of biomarkers of aging. Nat Aging. 2024;4(10):1372–1383. doi:10.1038/s43587-024-00683-3
105. “World report on ageing and health.” World Health Organization, 2015. Available from: https://www.who.int/publications/i/item/9789241565042.
106. Smith LJ, Pyke W, Fowler R, et al. Impact and experiences of vestibular disorders and psychological distress: qualitative findings from patients, family members and healthcare professionals. Health Expect. 2024;27(1):e13906. doi:10.1111/hex.13906
107. Delbaere K, Crombez G, Vanderstraeten G, Willems T, Cambier D. Fear-related avoidance of activities, falls and physical frailty: a prospective community-based cohort study. Age Ageing. 2010;33(4):368–373. doi:10.1093/ageing/afh106
108. Wen J, Chojecki D, Unsal A, Ueyama M, van Katwyk S. Economic Burden of Vestibular Dysfunction: Executive Report. Edmonton, Alberta: Institute of Health Economics; 2025.
109. Zrenner C, Ziemann U. Closed-loop brain stimulation. Biol Psychiatry. 2024;95(6):545–552. doi:10.1016/j.biopsych.2023.09.014
110. Aziz A, King J, Peters RM, et al. Robust and high precision non-invasive electrical vestibular intervention using earables for balance recovery. Submitted for publication.
111. Loyd BJ, Saviers-Steiger J, Fangman A, et al. Control of linear head and trunk acceleration during gait after unilateral vestibular deficits. Arch Phys Med Rehabil. 2021;102(3):456–462. doi:10.1016/j.apmr.2020.08.005
112. Pavlou M, Costafreda SG, Galsworthy W, Korres G, Bamiou DE. The interplay between cognition, functional and dual-task gait in persons with a vestibular disorder versus healthy controls. Sci Rep. 2023;13(1):10130. doi:10.1038/s41598-023-35904-z
113. MacDougall HG, Brizuela AE, Burgess AM, Curthoys IS, Halmagyi GM. Patient and normal three-dimensional eye-movement responses to maintained (DC) surface galvanic vestibular stimulation. Otol Neurotol. 2005;26(3):500–511. doi:10.1097/01.mao.0000169766.08421.ef
114. Zuniga SA, Adams ME. Efficient use of vestibular testing. Otolaryngol Clin North Am. 2021;54(5):875–891. doi:10.1016/j.otc.2021.05.011
115. Nakamura A, Miura R, Suzuki Y, Morasso P, Nomura T. Discrete cortical control during quiet stance revealed by desynchronization and rebound of beta oscillations. Neurosci lett. 2023;814:137443. doi:10.1016/j.neulet.2023.137443
116. Legrand T, S.j M, Muller L, Naeije G, Ghinst MV, Bourguignon M. Cortical tracking of postural sways during standing balance. Sci Rep. 2024;14(1):1–13. doi:10.1038/s41598-024-81865-2
117. Tisserand R, Dakin CJ, Van der Loos MH, Croft EA, Inglis TJ, Blouin JS. Down regulation of vestibular balance stabilizing mechanisms to enable transition between motor states. Elife. 2018;7:e36123. doi:10.7554/eLife.36123
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Phybrata Digital Biomarkers of Age-Related Balance Impairments, Sensory Reweighting, and Intrinsic Fall Risk
Ralston JD, Stanley S, Roper JM, Ralston AB
Medical Devices: Evidence and Research 2025, 18:319-336
Published Date: 11 June 2025