Back to Journals » Advances in Medical Education and Practice » Volume 11
Quality and Impact of Survey Research Among Anesthesiologists: A Systematic Review
Authors Geyer ED ![]() , Miller R
, Miller R ![]() , Kim SS
, Kim SS ![]() , Tobias JD
, Tobias JD ![]() , Nafiu OO, Tumin D
, Nafiu OO, Tumin D
Received 25 April 2020
Accepted for publication 24 July 2020
Published 25 August 2020 Volume 2020:11 Pages 587—599
DOI https://doi.org/10.2147/AMEP.S259908
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Emily D Geyer,1 Rebecca Miller,1 Stephani S Kim,1 Joseph D Tobias,1,2 Olubukola O Nafiu,1 Dmitry Tumin3
1Department of Anesthesiology and Pain Medicine, Nationwide Children’s Hospital, Columbus, OH, USA; 2Department of Anesthesiology & Pain Medicine, The Ohio State University, Columbus, OH, USA; 3Department of Pediatrics, East Carolina University, Greenville, NC, USA
Correspondence: Stephani S Kim Kim
Department of Anesthesiology and Pain Medicine, Nationwide Children’s Hospital, 700 Children’s Drive, Columbus, OH 43205, USA
Tel +1 614 722-2675
Fax +1 614 722-4203
Email [email protected]
Abstract: New technology has facilitated survey research of anesthesia professional society members. We evaluated prevailing metrics of quality and impact of published research studies based on surveys of anesthesiologists. We hypothesized that adherence to recommended practices (such as use of reminders) would be associated with increased survey response rates, and that higher response rates would be associated with higher article impact. Using the MEDLINE database, we identified 45 English-language research articles published in 2010– 2017 reporting original data from surveys of anesthesiologists. The median response rate was 37% (IQR: 25– 46%). Recommended survey practices, including the use of reminders (p = 0.861) and validated questionnaires (p = 0.719), were not correlated with response rates. In turn, survey response rates were not associated with measures of article impact (p = 0.528). The impact of published research based on surveys of anesthesiologists, as measured by citation scores (p = 0.493) and Altmetrics (p = 0.826), may be driven primarily by the novel data or questions raised using survey methodology, but does not appear to be associated with response rates. Improving reporting of survey methodology and understanding possible sources of non-response bias are important for future studies in this area.
Keywords: survey methodology, anesthesiologist, response rate, survey research, systematic review
Introduction
Survey research has been used by investigators for studying clinical, educational, and professional topics in the field of anesthesiology. The feasibility of such research has been facilitated by the prevalence of computer technology, the increased ease of communication via the internet, the development of online survey questionnaires, and the availability of e-mail lists from various organizations for participant recruitment. However, the validity of survey data is reduced by low response rates, missing data points, and poorly designed questionnaires.1 The importance of appropriate survey design for enhancing inference from survey data is increasingly recognized among clinical researchers.2,3 Recent guidelines for survey research on clinical topics have emphasized the need for reducing potential sources of bias by using validated questions, pre-testing survey questionnaires, and using incentives or reminders to enhance response rates.4–6 However, the value of adopting these “best practices” of survey research has not been examined for studies recruiting the participation of anesthesiologists. Understanding the quality and impact of data that can be generated from surveys of anesthesiologists can support development of higher-quality surveys among members of the profession and increase the value of members’ participation in surveys.
In this systematic review, we identified published survey research sampling anesthesiologists and evaluated the quality and impact of these studies. The primary measure of quality was the survey response rate.6 Measures of impact included article citations, publication in high impact factor journals, Altmetric scores, and mention of studies in educational materials, news media, and professional society publications (other than academic journals). We hypothesized that adherence to recommended practices of survey design was associated with higher survey response rate and higher article impact. Our secondary aim was to determine which survey characteristics were associated with improved survey response rate, or greater impact, of surveys conducted among anesthesiologists.
Methods
IRB approval was not necessary for this study because it was a review of published research articles. In April and May of 2018, we conducted a systematic search of the MEDLINE database for English-language peer-reviewed research articles published in 2010–2017, which reported original data generated by surveying anesthesiologists based on their membership in one of the following professional societies: American Society of Anesthesiologists, ASA; Association of Anaesthetists of Great Britain and Ireland, AAGBI; Canadian Anesthesiologists’ Society, CAS; Australian and New Zealand College of Anaesthetists, ANZCA; Society for Pediatric Anesthesia, SPA; Association of Paediatric Anaesthetists of Great Britain and Ireland, APAGBI; Canadian Pediatric Anesthesia Society, CPAS; and Society for Pediatric Anaesthesia in New Zealand and Australia, SPANZA. Search keywords included “survey” and “anesthesia” or “anesthesiologist”/“anesthetist” (using British and American spelling, as well as plural and singular nouns). We used PubMed to search for articles, filtering results according to journal indexing in MEDLINE.
We identified titles and abstracts of articles and evaluated each for potential inclusion in the systematic review. We obtained full texts for original research articles (full length or brief communication formats) meeting our inclusion criteria. We screened each paper for original survey research of individual anesthesiologists responding on their own behalf. We excluded studies that sampled institutions or asked respondents to participate in their study on behalf of an institution (eg, studies that targeted fellowship program directors), and qualitative research using entirely unstructured surveys or interviews. We resolved disagreements regarding whether an article met inclusion criteria through discussion among the investigators. The lead investigator reviewed articles selected for inclusion, and coded the pre-specified fields shown in Table 1. All studies meeting inclusion criteria were planned to be included in the analysis, and no a priori power calculation was performed. Survey characteristics and quality outcomes which we expected would be commonly reported, and which would be suitable for objective assessment, were pre-selected to be included in the review. Data that were deemed unlikely to be reported in published studies, such as questionnaire visual design, were not included.
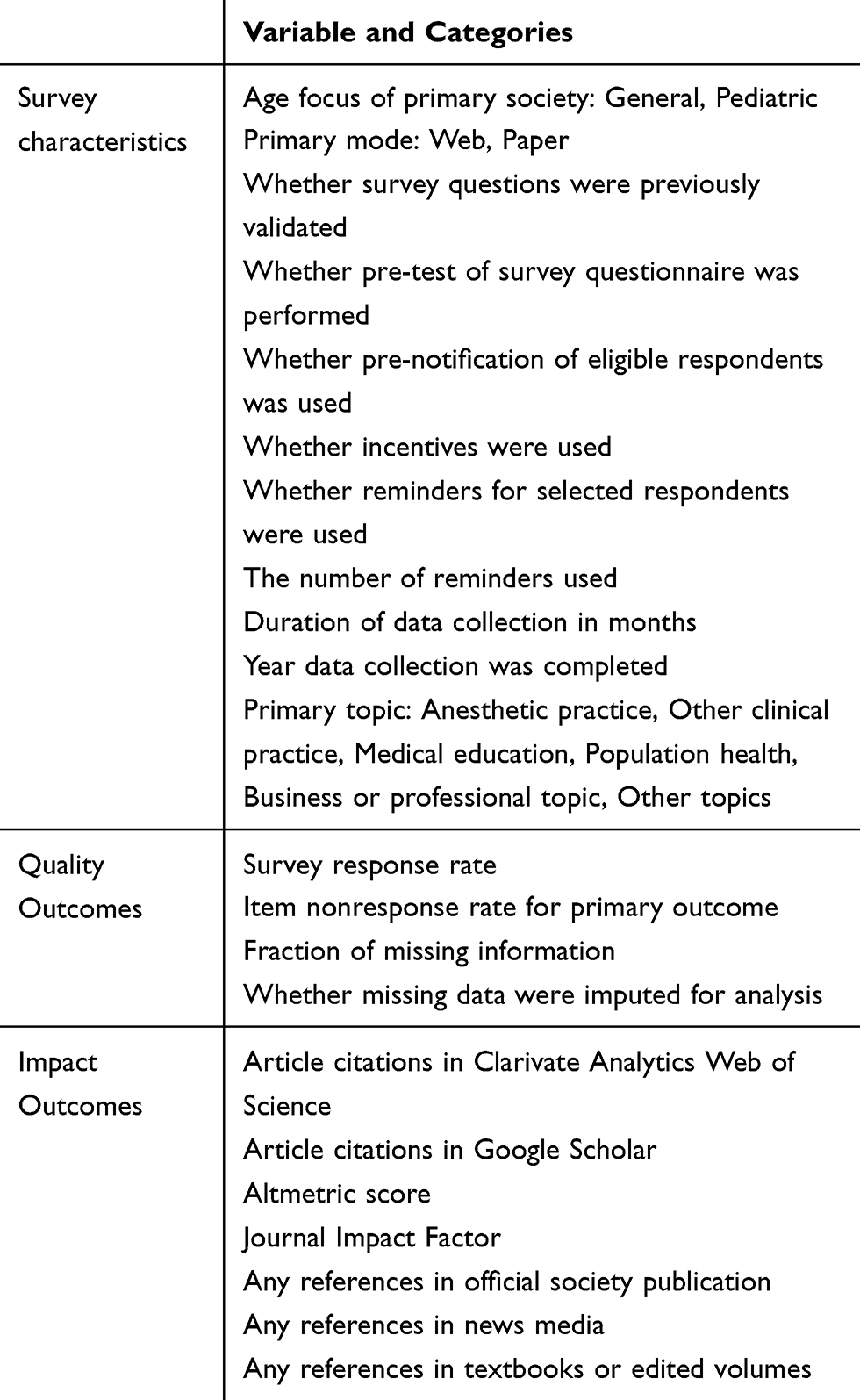 |
Table 1 Pre-Specified Fields Coded for Each Manuscript |
The primary quality outcome in this review was the reported survey response rate, defined as the number of completed responses out of the number of potential respondents who were invited to participate. Partially completed surveys were included in the response rate if they were described as part of the number of completed responses in the original studies. Secondary quality measures included the item non-response rate for the primary study outcome, if one was specified, and the fraction of missing information. The item non-response rate was calculated as the number of responses missing data on the primary study outcome out of the total number of survey responses. The fraction of missing information was defined as the number of surveys with any incomplete data on study variables, out of the total number of complete surveys. We also noted whether the studies used multiple imputations to complete any items missing data for analysis. Article impact outcomes were assessed at the time of the review and included article citation counts from Web of Science and Google Scholar; the Altmetric score of news media and social media mentions; and the impact factor of the journal in which the article was published. These characteristics have been used in prior bibliometric research assessing the impact of publications in medicine and life sciences.7–9 Additionally, we used a Web search (Google) to determine whether articles were mentioned in news media, textbooks or edited volumes, or official publications of professional societies, excluding academic journals.
Characteristics of survey design included the use of validated questions, survey pre-testing, use of incentives for survey completion, pre-notification of invited respondents, and use of reminders, reflecting general recommendations for improving survey research on clinically relevant topics.4–6 Additional characteristics of surveys that may have influenced the response rate, such as survey mode and duration of data collection, were coded as summarized in Table 1.10 The study was not powered for a specific primary hypothesis test but explored a range of plausible associations among survey characteristics, survey response rate, and study impact. Response rates and impact measures were compared against survey characteristics using Spearman correlation coefficients and rank-sum tests. We did not assess the risk of bias because the surveys described included studies that evaluated a diverse range of topics, so bias in the estimation of a specific quantity or association was not an area of focus for our review. Data analysis was performed using Stata/IC 14.2 (College Station, TX: StataCorp LP) and two-tailed P<0.05 was considered statistically significant.
Results
Our initial MEDLINE search identified 1448 publications which were reviewed for potential inclusion in the study. Based on title and abstract review, 1403 publications were excluded, and full texts were obtained for the remaining 45 publications. Bibliographic data and study characteristics for the included studies are summarized in Table 2. Twenty surveys were primarily conducted in the United States (US), compared to 16 in Australia/New Zealand, 5 in Canada, and 4 in Great Britain and Ireland. Sample sizes ranged from 84 to 8178, for a total of 35,177 responses among the articles that reported sample size. Most surveys elicited respondents’ opinion about various anesthetic practices, such as the use of laryngeal mask airways, the prevalence of general anesthesia without intravenous access, perioperative management of patients with obstructive sleep apnea, and use of a difficult airway cart.
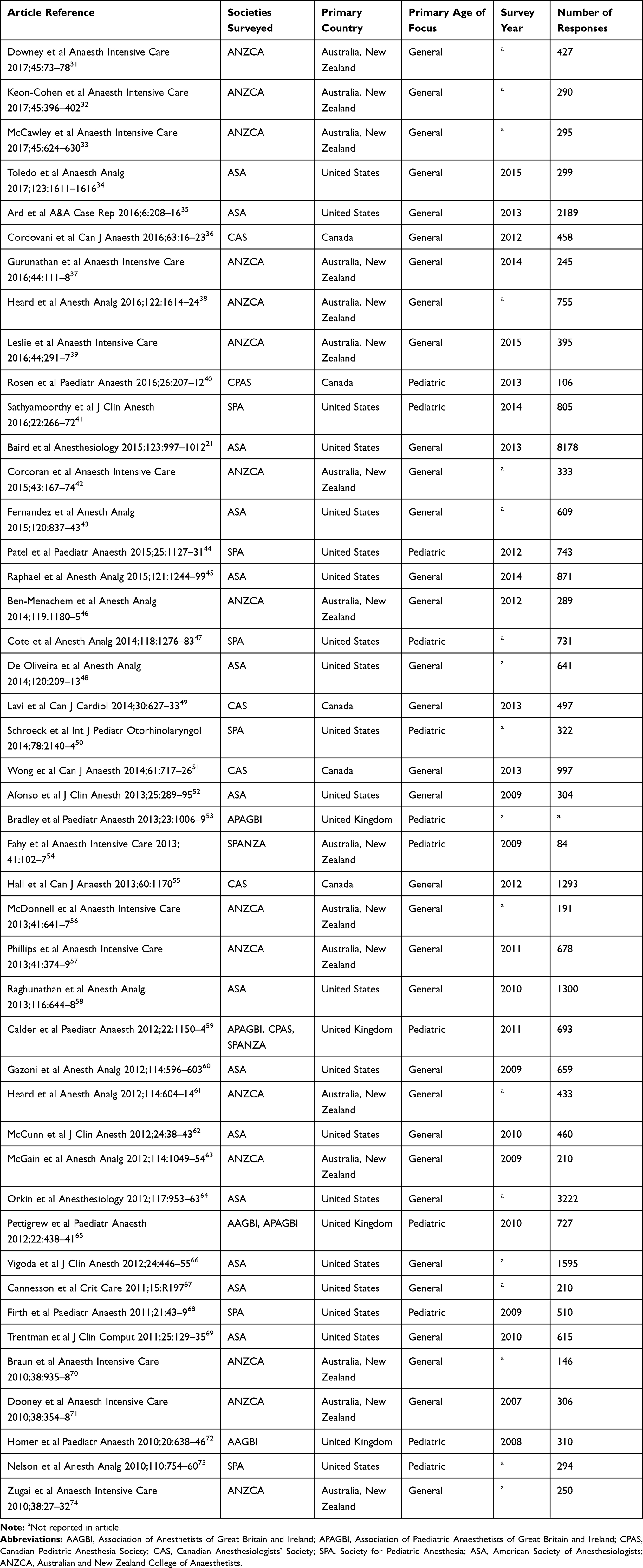 |
Table 2 Bibliographic Data and Study Characteristics for the Included Studies |
Survey methodologies for included studies are summarized in Table 3. Most surveys were completed online, although five surveys used paper questionnaires. Reported methods to ensure survey validity included using validated questions (12/45) and pre-testing the survey questionnaire (23/45). Only one survey reported using both a pre-notification and incentives to increase participation, while 4 surveys reported using incentives alone. By contrast, most surveys used one or more reminders to increase participation (33/45, using a median of 2 reminders). Survey response rates, summarized in Table 4, ranged from 7% to 95% (median [IQR]: 37% [25%, 46%]), although the highest response rate attained on an online survey was 67%. Two studies reported the nonresponse rate for the primary outcome (1.4% and 19.1%, respectively), and 12 studies reported an overall fraction of missing information, ranging from 1.3% to 9.3% (median: 5%; IQR: 2%, 6%).
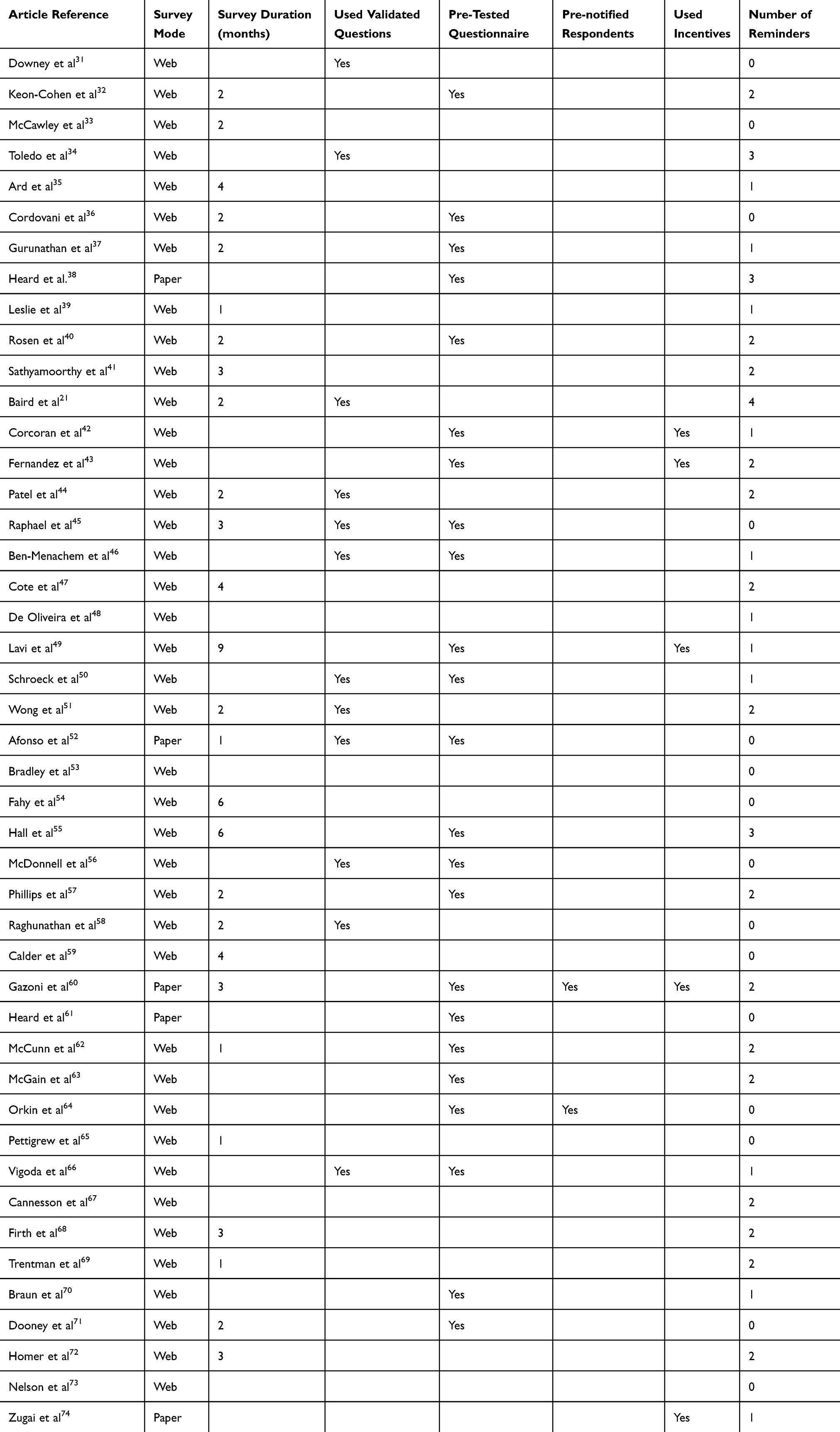 |
Table 3 Reported Characteristics of Survey Methodologies for Selected Studies |
 |
Table 4 Survey Quality and Impact Metrics |
Considering the use of reminders, incentives, pre-notification, questionnaire pre-testing, and use of validated questions, we identified 30 studies which used at least one of these methods, and 15 studies which used none of these methods. The survey response rates did not significantly differ between these two groups (median: 37% vs 36%, p = 0.544). Considering other survey characteristics, median response rates were lower in US surveys compared to non-US surveys (26% vs 39%; 95% confidence interval [CI] of difference: 2%, 23%; p = 0.021), and higher for paper surveys compared to web surveys (55% vs 30%; 95% CI of difference: 13%, 42%; p=0.002). There were not enough data to compare secondary quality outcomes, such as the fraction of missing information.
Other study impact metrics include article citation counts, which ranged from 0 to 218 in Google Scholar (median [IQR]: 10 [4, 20]), and from 0 to 135 in Web of Science (median [IQR]: 5 [2, 14]). Among 16 articles from publishers reporting Altmetric scores, these scores ranged from 0 to 105 (median [IQR]: 2 [1, 6]). All except one of the surveys were published in journals with an assigned 2016 impact factor, with scores ranging from 1.2 to 5.8. Thirteen of the surveys have been referenced in official society publications, 15 in textbooks, and nine in news media. The survey response rate was not correlated with article citations on Google Scholar (ρ = −0.17, p = 0.251) citations on Web of Science (ρ = −0.12, p = 0.450), Altmetric scores (ρ = 0.06, p = 0.826) or journal impact factor (ρ = −0.005, p = 0.976). Survey response rates did not differ between studies that were referenced in official society publications, textbooks, or news media (median [IQR]: 36% [26%, 42%]) and studies that were not (median [IQR]: 38% [25%, 51%]; p = 0.544).
Discussion
Increased feasibility of administering surveys has prompted many groups to conduct survey research of anesthesiology professional societies, in order to gather novel data on clinical practices and to explore professional issues in the field. While recent overviews have brought attention to important aspects of survey design, empirical data remain scarce on what defines high-quality research involving surveys of anesthesiologists. To address this, we reviewed published surveys of large English-language professional anesthesia societies, focusing on variation and correlation in measures of survey quality and impact. Our review identified limited reporting of survey characteristics and a wide variability in survey response rates (7–95%). Other than the use of paper surveys, there were no evident associations between elements of survey design and survey response rates.
Response rate is the primary metric used to assess the quality of survey research.11,12 Specifically, 23 of the articles reviewed (reporting response rates of 8–55%) cited a low response rate as one of their study limitations. Current research suggests that a response rate of 50–60% could minimize the risk of non-response bias, although 35 of the 45 surveys that were published and were included in our study did not meet this threshold.13 The low response rates in many of the surveys reviewed may be due to lower response rates seen in online surveys as compared to paper surveys.14,15 Nevertheless, the median response rate among surveys included in our review was similar to that found in Sheehan’s meta-analysis, which indicated a median response rate of 37% for web-based surveys.16 Efforts to increase response rates may include financial incentives, advance letters, attempts to convert respondents who refuse to participate, and follow-up reminders. However, while these techniques have produced higher response rates in some experimental settings, their use has not been definitively associated with a reduction in non-response bias.17 Thus, high response rates to a survey may be necessary, but not sufficient to assure survey validity.18 Although our study did not overtly measure non-response bias, it was notable that no survey characteristics other than survey mode were correlated with the response rate. Given the generally high and variable non-response rates in the studies reviewed, we speculate that non-response in this setting could often be caused by anesthesiologists choosing to participate in a given survey primarily based on the topic of the research and its relevance to their practice and interests.
Our review presents new data on the state of survey research in anesthesiology but is subject to some limitations. First, we have focused on surveys of anesthesiology professional society members, which are facilitated by the availability of society mailing lists, and the probable interest of society members in contributing to academic research. Therefore, our conclusions may not be generalizable to surveys of other populations, such as patients or caregivers. We also excluded surveys that sample institutions (eg, surveys of fellowship program directors about characteristics of their fellowship program), as response rates to these surveys tend to be very high, possibly owing to respondents’ perceived responsibility to complete the survey on behalf of their institution.19,20 Furthermore, we evaluated quality and impact metrics among published studies, but did not analyze which survey characteristics influenced the likelihood of publication and did not include surveys reported only in the “grey literature” (eg, non-peer-reviewed reports) or surveys conducted internally within professional societies. An additional limitation of examining impact metrics is that only a small number of articles receive scholarly and public attention more than the typical article, such as the Baird et al paper.21 Our review was further limited to publications in MEDLINE-indexed journals. Among the societies included in the study, all affiliated journals (eg, Anaesthesia, Anesthesiology, Canadian Journal of Anaesthesia, and Anaesthesia and Intensive Care) are indexed in MEDLINE, and some studies have described using MEDLINE as a “white list” of high-quality medical journals.22 Therefore, our review did not address the possibility that some surveys with methodological issues may have been published in journals not indexed in MEDLINE, and may not have captured articles that were published ahead of print during the review period, but not indexed in PubMed, as of May 2018. Lastly, we observed no statistically significant associations and weak correlations for a wide range of plausible of associations among survey characteristics, survey response rate, and study impact. This supports our conclusions regarding the unpredictability of response rates, and an evident lack of association between survey response rates and study impact.
In this study, we utilized bibliometric analyses to quantify the attention scientific articles receive.7–9,23 One of the better-known aspects of bibliometrics is citation analysis.24 Our review included several highly cited articles, yet we found that the survey response rate was not correlated with the number of citations. Thus, while survey response rates may influence journals’ decision to publish an article, this study characteristic does not appear to influence academic audiences’ subsequent judgment of the study’s importance. Rather, Falagas et al determined that characteristics such as article length and journal impact factor influence citation counts.25 While citation counts are a classic tool of bibliometrics, alternative metrics are gaining popularity for assessing the impact of research outside of academia. The Altmetric score of a research article indicates the amount of online attention it has received by combining information from multiple data sources, such as social media and news mentions.24 In this review, one article had a very high Altmetric score while the rest of the studies received little attention according to this metric. As with citation counts, the response rate was not correlated with the Altmetric scores. This further suggests that the value of survey research in anesthesiology professional societies may be to raise novel questions or present data unobtainable in other ways, but not necessarily to generate precise and unbiased estimates dependent on a high response rate.
In previous studies, aspects of survey methodology were often reported inconsistently and only partially.26 Reviewing articles in anesthesiology journals, Story et al found that the reporting of survey methods was inconsistent and potentially compromised the transparency and reproducibility of surveys.27 Many sources, including but not limited to review articles published in the anesthesiology literature, outline good practices in conducting and reporting survey research, such as robust testing and development of the research instrument.1–6 Kelley et al emphasize the importance of reporting the details of primary data collection, such as how participants were selected, as well as how data were analyzed and whether any adjustments were made to account for nonresponse, missing data, or differential probability of response.28 Additionally, Davern et al have discussed the importance of estimating nonresponse bias, such as by comparing the survey with other sources, analyzing para-data, or analyzing external data sources.12 Halbesleben et al discussed specific formulas to calculate nonresponse bias based on the response rate, proportion of non-respondents, and characteristics of non-respondents.29 Despite these recommendations, one study in this review did not report the number of participants, while only 12 studies reported using previously validated questions and 23 studies reported pre-testing surveys. Only three studies used statistical weights to account for differential probability of response, and only two studies reported primary outcome nonresponse rates.
Techniques such as weighting and imputation, used in survey data analysis to address potential bias and non-response, appear to be under-used in surveys of anesthesia professional societies. Based on this review, several recommendations for survey practice can be made. Investigators should report essential information regarding data collection and analysis, such as the population targeted, the sampling frame, and whether the sampling frame included the entire society, a random subsample, or a non-random subsample (eg, attendees at a conference). Studies should also describe the development of survey research tools, the source of survey questions, the response rate, the primary outcome nonresponse rate, and the fraction of missing information, using established definitions from the survey methodology literature as appropriate. Additionally, researchers should attempt to analyze nonresponse bias, which can be significant even in the presence of high response rates.12,29 It is particularly important to consider using weighting or analysis of nonresponse bias in the presence of low response rates. Lastly, in surveys of smaller societies, survey data analysis may utilize finite population correction when estimating standard errors of estimates, as many survey samples in our review represented significant proportions of the total society membership. Statistical guidelines on this technique recommend using a finite population correction, which deflates the standard error in proportion to the population fraction surveyed, when the sample size is more than 5% of the total population.30 These recommendations could be incorporated into the development and evaluation of survey research for future studies in this area.
In summary, many surveys of anesthesiology professional societies have been conducted to study clinical, educational, and professional topics in the field. Technology has increased the ease of survey administration, as many survey invitations are distributed to all society members via email to complete on-line, with repeat reminders sent as often as once a month. Notwithstanding the ease of survey administration, response rates were often low even in published survey research. Investigators’ use of reminders and other aspects of survey methodology were not associated with higher response rates in published surveys of anesthesia professional societies. Furthermore, despite a high variability in response rates, the survey response rate was not associated with article impact as measured by article citations, Altmetric score, journal impact factor, or references in society publications, textbooks, or news media. Improving reporting of survey methodology and validating techniques for increasing the response rate specifically among members of anesthesiology professional societies may aid in increasing the quality of survey research in this area, and improve understanding of possible sources of nonresponse bias. Our findings provide a baseline for initiatives to improve survey research in anesthesiology professional societies, and a point of comparison for readers or reviewers assessing the quality of surveys in this population.
Acknowledgment
This review was presented in part at the Society for Pediatric Anesthesia 2018 Annual Meeting, March 24, 2018, Phoenix, AZ, USA.
Disclosure
The authors report no conflicts of interest in this work and no external funding.
References
1. Tait AR, Voepel-Lewis T. Survey research: it’s just a few questions, right? Paediatr Anaesth. 2015;25(7):656–662. doi:10.1111/pan.12680
2. Bryson GL, Turgeon AF, Choi PT. The science of opinion: survey methods in research. Can J Anaesth. 2012;59(8):736–742. doi:10.1007/s12630-012-9727-3
3. Sinkowitz-Cochran RL. Survey design: to ask or not to ask? That is the question. Clin Infect Dis. 2013;56(8):1159–1164. doi:10.1093/cid/cit005
4. Jones TL, Baxter MA, Khanduja V. A quick guide to survey research. Ann R Coll Surg Engl. 2013;95(1):5–7. doi:10.1308/003588413X13511609956372
5. Alderman AK, Salem B. Survey research. Plast Reconstr Surg. 2010;126(4):1381–1389. doi:10.1097/PRS.0b013e3181ea44f9
6. Jones D, Story D, Clavisi O, Jones R, Peyton P. An introductory guide to survey research in anaesthesia. Anaesth Intensive Care. 2006;34(2):245–253. doi:10.1177/0310057X0603400219
7. Azer SA. Top-cited articles in problem-based learning: a bibliometric analysis and quality of evidence assessment. J Dent Educ. 2017;81(4):458–478. doi:10.21815/JDE.016.011
8. Araujo R, Sorensen AA, Konkiel S, Bloem BR. Top Altmetric scores in the Parkinson’s disease literature. J Parkinsons Dis. 2017;7(1):81–87. doi:10.3233/JPD-179000
9. La Torre G, Sciarra I, Chiappetta M, Monteduro A. New bibliometric indicators for the scientific literature: an evolving panorama. Clin Ter. 2017;168(2):e65–e71. doi:10.7417/CT.2017.1985
10. Groves RM, Peytcheva E. The impact of nonresponse rates on nonresponse bias - A meta-analysis. Public Opin Q. 2008;72(2):167–189. doi:10.1093/poq/nfn011
11. Cook DA, Wittich CM, Daniels WL, West CP, Harris AM, Beebe TJ. Incentive and reminder strategies to improve response rate for internet-based physician surveys: a randomized experiment. J Med Internet Res. 2016;18(9):e244. doi:10.2196/jmir.6318
12. Davern M. Nonresponse rates are a problematic indicator of nonresponse bias in survey research. Health Serv Res. 2013;48(3):905–912. doi:10.1111/1475-6773.12070
13. Draugalis JR, Plaza CM. Best practices for survey research reports revisited: implications of target population, probability sampling, and response rate. Am J Pharm Educ. 2009;73(8):142. doi:10.5688/aj7308142
14. Cho YI, Johnson TP, Vangeest JB. Enhancing surveys of health care professionals: a meta-analysis of techniques to improve response. Eval Health Prof. 2013;36(3):382–407. doi:10.1177/0163278713496425
15. VanDenKerkhof EG, Parlow JL, Goldstein DH, Milne B. In Canada, anesthesiologists are less likely to respond to an electronic, compared to a paper questionnaire. Can J Anaesth. 2004;51(5):449–454. doi:10.1007/BF03018307
16. Sheehan KB. E-mail survey response rates: a review. J Comput Mediat Commun. 2001;6(2).
17. Groves RM. Nonresponse rates and nonresponse bias in household surveys. Public Opin Q. 2006;70(5):646–675. doi:10.1093/poq/nfl033
18. Fincham JE, Draugalis JR. The importance of survey research standards. Am J Pharm Educ. 2013;77(1):4. doi:10.5688/ajpe7714
19. Benzon HA, De Oliveira GS, Jagannathan N, Suresh S. Selection of subspecialty fellows in anesthesia for pediatric anesthesia: a national survey of program directors in the United States. Pediatr Anesth. 2015;25(5):487–491. doi:10.1111/pan.12608
20. Benzon HA, De Oliveira GS, Hardy CA, Suresh S. Status of pediatric anesthesiology fellowship research education in the United States: a survey of fellowship program directors. Pediatr Anesth. 2014;24(3):327–331. doi:10.1111/pan.12321
21. Baird M, Daugherty L, Kumar KB, Arifkhanova A. Regional and gender differences and trends in the anesthesiologist workforce. Anesthesiology. 2015;123(5):997–1012. doi:10.1097/ALN.0000000000000834
22. Misra DP, Ravindran V, Wakhlu A, Sharma A, Agarwal V, Negi VS. Publishing in black and white: the relevance of listing of scientific journals. Rheumatol Int. 2017;37(11):1773–1778. doi:10.1007/s00296-017-3830-2
23. Eyre-Walker A, Stoletzki N. The assessment of science: the relative merits of post-publication review, the impact factor, and the number of citations. PLoS Biol. 2013;11(10):e1001675. doi:10.1371/journal.pbio.1001675
24. Kolahi J, Khazaei S. Altmetric: top 50 dental articles in 2014. Br Dent J. 2016;220(11):569–574. doi:10.1038/sj.bdj.2016.411
25. Falagas ME, Zarkali A, Karageorgopoulos DE, Bardakas V, Mavros MN. The impact of article length on the number of future citations: a bibliometric analysis of general medicine journals. PLoS One. 2013;8(2):e49476. doi:10.1371/journal.pone.0049476
26. Jewkes R, Bennett C, Khangura S, et al. Reporting guidelines for survey research: an analysis of published guidance and reporting practices. PLoS Med. 2011;8(8):e1001069. doi:10.1371/journal.pmed.1001069
27. Story DA, Gin V, Na Ranong V, Poustie S, Jones D. Inconsistent survey reporting in anesthesia journals. Anesth Analg. 2011;113(3):591–595. doi:10.1213/ANE.0b013e3182264aaf
28. Kelley K, Clark B, Brown V, Sitzia J. Good practice in the conduct and reporting of survey research. Int J Qual Health Care. 2003;15(3):261–266. doi:10.1093/intqhc/mzg031
29. Halbesleben JR, Whitman MV. Evaluating survey quality in health services research: a decision framework for assessing nonresponse bias. Health Serv Res. 2013;48(3):913–930. doi:10.1111/1475-6773.12002
30. Daniel W. Biostatistics: A Foundation for Analysis in the Health Sciences.
31. Downey GB, McDonald JM, Downey RG. Welfare of anaesthesia trainees survey. Anaesth Intensive Care. 2017;45(1):73–78. doi:10.1177/0310057X1704500111
32. Keon-Cohen Z, Myles PS, Story DA. A survey of Australian and New Zealand anaesthetists’ attitudes towards resuscitation orders in the perioperative setting. Anaesth Intensive Care. 2017;45(3):396–402. doi:10.1177/0310057X1704500316
33. McCawley D, Cyna AM, Prineas S, Tan S. A survey of the sequelae of memorable anaesthetic drug errors from the anaesthetist’s perspective. Anaesth Intensive Care. 2017;45(5):624–630. doi:10.1177/0310057X1704500514
34. Toledo P, Duce L, Adams J, Ross VH, Thompson KM, Wong CA. Diversity in the American society of anesthesiologists leadership. Anesth Analg. 2017;124(5):1611–1616. doi:10.1213/ANE.0000000000001837
35. Ard JL
36. Cordovani L, Chung F, Germain G, et al. Perioperative management of patients with obstructive sleep apnea: a survey of Canadian anesthesiologists. Can J Anaesth. 2016;63(1):16–23. doi:10.1007/s12630-015-0512-y
37. Gurunathan U, Berry K, Way M. Intentions and barriers to research activities among Australian and New Zealand anaesthetists: a survey. Anaesth Intensive Care. 2016;44(1):111–118. doi:10.1177/0310057X1604400117
38. Heard GC, Thomas RD, Sanderson PM. In the aftermath: attitudes of anesthesiologists to supportive strategies after an unexpected intraoperative patient death. Anesth Analg. 2016;122(5):1614–1624. doi:10.1213/ANE.0000000000001227
39. Leslie K, Allen ML, Hessian E, Lee AY. Survey of anaesthetists’ practice of sedation for gastrointestinal endoscopy. Anaesth Intensive Care. 2016;44(4):491–497. doi:10.1177/0310057X1604400409
40. Rosen HD, Mervitz D, Cravero JP. Pediatric emergence delirium: Canadian pediatric anesthesiologists’ experience. Paediatr Anaesth. 2016;26(2):207–212. doi:10.1111/pan.12812
41. Sathyamoorthy M, Lerman J, Okhomina VI, Penman AD. Use of cuffed tracheal tubes in neonates, infants and children: a practice survey of members of the society of pediatric anesthesia. J Clin Anesth. 2016;33:266–272. doi:10.1016/j.jclinane.2016.03.013
42. Corcoran TB, Edwards T. A survey of antiemetic dexamethasone administration-frequency of use and perceptions of benefits and risks. Anaesth Intensive Care. 2015;43(2):167–174. doi:10.1177/0310057X1504300205
43. Fernandez PG, Loftus RW, Dodds TM, et al. Hand hygiene knowledge and perceptions among anesthesia providers. Anesth Analg. 2015;120(4):837–843. doi:10.1213/ANE.0000000000000408
44. Patel A, Clark SR, Schiffmiller M, Schoenberg C, Tewfik G. A survey of practice patterns in the use of laryngeal mask by pediatric anesthesiologists. Paediatr Anaesth. 2015;25(11):1127–1131. doi:10.1111/pan.12727
45. Raphael DR, Cannesson M, Rinehart J, Kain ZN. Health care costs and the perioperative surgical home: a survey study. Anesth Analg. 2015;121(5):1344–1349. doi:10.1213/ANE.0000000000000876
46. Ben-Menachem E, Zalcberg D. Depth of anesthesia monitoring: a survey of attitudes and usage patterns among Australian anesthesiologists. Anesth Analg. 2014;119(5):1180–1185. doi:10.1213/ANE.0000000000000344
47. Cote CJ, Posner KL, Domino KB. Death or neurologic injury after tonsillectomy in children with a focus on obstructive sleep apnea: Houston, we have a problem! Anesth Analg. 2014;118(6):1276–1283. doi:10.1213/ANE.0b013e318294fc47
48. De Oliveira GS
49. Lavi S, Jolly SS, Bainbridge D, Manji F, Randhawa V, Lavi R. Sedation, analgesia, and anaesthesia variability in laboratory-based cardiac procedures: an international survey. Can J Cardiol. 2014;30(6):627–633. doi:10.1016/j.cjca.2014.03.034
50. Schroeck H, Healy DW, Tait AR. Airway laser procedures in children and the American society of anesthesiologists’ practice advisory: a survey among pediatric anesthesiologists. Int J Pediatr Otorhinolaryngol. 2014;78(12):2140–2144. doi:10.1016/j.ijporl.2014.09.024
51. Wong DT, Mehta A, Tam AD, Yau B, Wong J. A survey of Canadian anesthesiologists’ preferences in difficult intubation and “cannot intubate, cannot ventilate” situations. Can J Anaesth. 2014;61(8):717–726. doi:10.1007/s12630-014-0183-0
52. Afonso AM, Diaz JH, Scher CS, Beyl RA, Nair SR, Kaye AD. Measuring determinants of career satisfaction of anesthesiologists: validation of a survey instrument. J Clin Anesth. 2013;25(4):289–295. doi:10.1016/j.jclinane.2013.01.007
53. Bradley AE, White MC, Engelhardt T, Bayley G, Beringer RM. Current UK practice of pediatric supraglottic airway devices - a survey of members of the association of paediatric anaesthetists of Great Britain and Ireland. Paediatr Anaesth. 2013;23(11):1006–1009. doi:10.1111/pan.12230
54. Fahy CJ, Costi DA, Cyna AM. A survey of aseptic precautions and needle type for paediatric caudal block in Australia and New Zealand. Anaesth Intensive Care. 2013;41(1):102–107. doi:10.1177/0310057X1304100117
55. Hall R, Bryson GL, Flowerdew G, et al. Drug shortages in Canadian anesthesia: a national survey. Can J Anaesth. 2013;60(6):539–551. doi:10.1007/s12630-013-9920-z
56. McDonnell NJ, Kaye RM, Hood S, Shrivastava P, Khursandi DC. Mental health and welfare in Australian anaesthetists. Anaesth Intensive Care. 2013;41(5):641–647. doi:10.1177/0310057X1304100510
57. Phillips S, Stewart PA, Bilgin AB. A survey of the management of neuromuscular blockade monitoring in Australia and New Zealand. Anaesth Intensive Care. 2013;41(3):374–379. doi:10.1177/0310057X1304100316
58. Raghunathan K, Connelly NR, Friderici J, et al. Unwarranted variability in antibiotic prophylaxis for cesarean section delivery: a national survey of anesthesiologists. Anesth Analg. 2013;116(3):644–648. doi:10.1213/ANE.0b013e318276cf72
59. Calder A, Hegarty M, Davies K, von Ungern-sternberg BS. The difficult airway trolley in pediatric anesthesia: an international survey of experience and training. Paediatr Anaesth. 2012;22(12):1150–1154. doi:10.1111/pan.12058
60. Gazoni FM, Amato PE, Malik ZM, Durieux ME. The impact of perioperative catastrophes on anesthesiologists: results of a national survey. Anesth Analg. 2012;114(3):596–603. doi:10.1213/ANE.0b013e318227524e
61. Heard GC, Sanderson PM, Thomas RD. Barriers to adverse event and error reporting in anesthesia. Anesth Analg. 2012;114(3):604–614. doi:10.1213/ANE.0b013e31822649e8
62. McCunn M, Speck RM, Chung I, Atkins JH, Raiten JM, Fleisher LA. Global health outreach during anesthesiology residency in the United States: a survey of interest, barriers to participation, and proposed solutions. J Clin Anesth. 2012;24(1):38–43. doi:10.1016/j.jclinane.2011.06.007
63. McGain F, White S, Mossenson S, Kayak E, Story D. A survey of anesthesiologists’ views of operating room recycling. Anesth Analg. 2012;114(5):1049–1054. doi:10.1213/ANE.0b013e31824d273d
64. Orkin FK, McGinnis SL, Forte GJ, et al. United States anesthesiologists over 50: retirement decision making and workforce implications. Anesthesiology. 2012;117(5):953–963. doi:10.1097/ALN.0b013e3182700c72
65. Pettigrew T, Adewale L, Morton NS. General anesthesia without intravenous access in children–a survey of current practice among members of the APAGBI and UK regional representatives of the APAGBI and the AAGBI. Paediatr Anaesth. 2012;22(5):438–441. doi:10.1111/j.1460-9592.2011.03787.x
66. Vigoda MM, Behrens V, Miljkovic N, Arheart KL, Lubarsky DA, Dutton RP. Perioperative cardiac evaluation of simulated patients by practicing anesthesiologists is not consistent with 2007 ACC/AHA guidelines. J Clin Anesth. 2012;24(6):446–455. doi:10.1016/j.jclinane.2011.11.007
67. Cannesson M, Pestel G, Ricks C, Hoeft A, Perel A. Hemodynamic monitoring and management in patients undergoing high risk surgery: a survey among North American and European anesthesiologists. Crit Care. 2011;15(4):R197. doi:10.1186/cc10364
68. Firth PG, McMillan KN, Haberkern CM, Yaster M, Bender MA, Goodwin SR. A survey of perioperative management of sickle cell disease in North America. Paediatr Anaesth. 2011;21(1):43–49. doi:10.1111/j.1460-9592.2010.03415.x
69. Trentman TL, Mueller JT, Ruskin KJ, Noble BN, Doyle CA. Adoption of anesthesia information management systems by US anesthesiologists. J Clin Monit Comput. 2011;25(2):129–135. doi:10.1007/s10877-011-9289-x
70. Braun AR, Leslie K, Merry AF, Story D. What are we telling our patients? A survey of risk disclosure for anaesthesia in Australia and New Zealand. Anaesth Intensive Care. 2010;38(5):935–938. doi:10.1177/0310057X1003800520
71. Dooney NM, Osborn KD. Rural anaesthesia practice: attitudes and recruitment following a period of anaesthetic training in rural and regional hospitals. A survey of new consultants. Anaesth Intensive Care. 2010;38(2):354–358.
72. Homer JR, Bass S. Physically restraining children for induction of general anesthesia: survey of consultant pediatric anesthetists. Paediatr Anaesth. 2010;20(7):638–646. doi:10.1111/j.1460-9592.2010.03324.x
73. Nelson KL, Yaster M, Kost-Byerly S, Monitto CL. A national survey of American pediatric anesthesiologists: patient-controlled analgesia and other intravenous opioid therapies in pediatric acute pain management. Anesth Analg. 2010;110(3):754–760. doi:10.1213/ANE.0b013e3181ca749c
74. Zugai BM, Eley V, Mallitt KA, Greenland KB. Practice patterns for predicted difficult airway management and access to airway equipment by anaesthetists in Queensland, Australia. Anaesth Intensive Care. 2010;38(1):27–32. doi:10.1177/0310057X1003800106
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.