Back to Journals » Advances in Medical Education and Practice » Volume 13
Qualitative Study of Medical Doctors on Their Experiences and Opinions of the Characteristics of Exceptionally Good Doctors
Authors Schnelle C ![]() , Jones MA
, Jones MA
Received 15 April 2022
Accepted for publication 4 June 2022
Published 17 July 2022 Volume 2022:13 Pages 717—731
DOI https://doi.org/10.2147/AMEP.S370980
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Christoph Schnelle, Mark A Jones
Institute for Evidence-Based Healthcare, Bond University, Robina, QLD, 4226, Australia
Correspondence: Christoph Schnelle, Institute for Evidence-Based Healthcare, Bond University, 14 University Drive, Robina, QLD, 4226, Australia, Email [email protected]
Background: It is generally accepted that there is a therapist effect in psychotherapy, with master therapists being studied using qualitative methods. There are surgeons with exceptionally positive patients’ physical health outcomes, and qualitative research on what makes good doctors. However, characteristics of exceptionally good doctors are less studied and understood.
Objective: To qualitatively study the opinions of physicians on exceptionally good doctors.
Methods: Thirteen semi-structured interviews of English-speaking medical doctors of any specialty were conducted. Recruitment was achieved through the authors’ network; contacting authors of relevant research papers; and Bond University’s General Practitioner recruitment program. Their opinion was sought on what makes an exceptionally good doctor, whether they have met such a person, what was their experience of that person, and whether they consider themselves as exceptionally good doctors.
Analysis: A six-phase thematic analysis in an experiential framework, as per Braun and Clarke, was implemented to identify themes and their details in an inductive approach with a realist epistemological position, ie, assuming truthful knowledge on what makes exceptionally good doctors can be obtained.
Results: Each interviewee had met and been inspired by exceptionally good doctors. Descriptions covered six themes: character traits; other characteristics; patient relationships; peer and health care system relations; education; and treatment examples. Exceptionally good doctors were found to have up-to-date extensive medical knowledge and skills, relate well with patients, and have excellent diagnostic abilities. They tend to be humble, approachable, inspiring, and are long-remembered role models. However, they may not always be appreciated by their peers and their health care system because of their exceptional abilities.
Discussion and Conclusion: Exceptional doctors are beneficial for their peers, their patients, and their health care system. Identifying, acknowledging, and making such doctors more accessible to medical students and junior doctors could have a positive impact on medical practice.
Keywords: qualitative study, thematic analysis, doctors’ performance
Plain Language Summary
Given there are billions of doctor-patient interactions every year, it could be impactful to study whether some doctors are exceptionally good and if so, why they are exceptionally good. However, to date, there has been little research on this topic. Previous research has reported that good doctors deal well with people, are competent, and ethical. This study report outlines the results of interviews with medical doctors on their opinions of what makes an exceptionally good doctor. Analysis of their responses suggest exceptionally good doctors have up-to-date extensive medical knowledge and skills, relate well with patients and are excellent at diagnosing diseases and conditions. They are humble, approachable, inspiring, and are long-remembered role models for other doctors. However, they may not always be appreciated by their peers and their health care system. Exceptional doctors, if they can be identified, could be a potentially important resource in terms of mentoring junior doctors.
Background
In 2018, there were over 800 million visits to doctors of medicine in the United States,1 and in the countries that are part of the Organization for Economic Co-operation and Development (OECD), the annual number of doctor visits per capita ranged from 2.3 in Mexico to 17.2 in South Korea. It has been reported that the most frequently used “drug” in general practice is the doctor himself.2,3 Taking such billions of medical doctor visits each year into consideration, there is a surprisingly limited amount of research on what makes a good doctor, and much less on exceptionally good doctors, or even whether a doctor, on his or her own, makes a difference in patients’ physical health after all known factors are accounted for.
In 2002, the British Medical Journal (BMJ) due to popular demand4 published a special edition titled “What’s a good doctor and how do you make one?” with the lead article written by Hurwitz and Vass,4 summarizing the confusion on the issue as “The varieties of good, poor, and bad doctors are diverse and may sometimes coexist in the same individual”, and an unnamed editor, considering the articles published in that volume, suggested that defining a good doctor is impossible.5
In the same edition, two senior administrators of medical schools, McCrorie and Cumming, were optimistic that they can train medical students to be good doctors; however, they did not define such doctors in any detail beyond requiring clinical and interpersonal abilities,6,7 while Pringle et al8 in the same issue argued that the public and managers need to know which are the good doctors so they can protect themselves from the bad ones. They also reported that data on effectiveness, safety, acceptability, and efficiency can identify good doctors better than the anecdotal approach, and provided 12 attributes of quality measures, in addition to the benefits and dangers of using them; however, such data only enables one to measure aspects of performance. The citation gap for Balint’s 1955 paper2 of 86 Scopus9 but 4800 Google Scholar citations suggests that doctors’ performance may be more important to the general public than researchers. Jeremy Holmes10 has described the good doctors as the ones who can bring their good and bad parts together to be good enough doctors, for which they should be content, whereas Paice et al11 stated that “excellent role models will always inspire, teach by example, and excite admiration and emulation.” Still, this does not add to the evidence about what a good doctor is, since they also stated that “being a role model is serendipitous; there is no training program, appointment panel, or certificate”.
More recently, it has been recognized that doctors can at least be described in terms of patients’ physical health outcomes, which subsequently represents some of the doctors as positive outliers, ie, they have substantially better patient health outcomes than the average doctor, even after accounting for all known variables such as patient’s and doctor’s demographics, hospital factors, or patient risk.12–21 In other words, there are exceptionally good doctors in terms of patient outcomes.
However, there may be other characteristics or criteria for exceptionally good doctors besides patient outcomes. This was investigated by Steiner-Hofbauer et al22 who performed a systematic review of stakeholders’ opinions on what makes a good doctor, adding interpersonal skills, ethics, medical management, teaching, and research to medical skills. In their systematic review, there were 6 studies on what makes a good doctor from the peers’ perspective (other medical doctors), but none that addressed exceptionally good doctors.
Herzig et al23 analyzed a set of 83 general interviews called “life pictures” (“Lebensbilder”), published in the German medical weekly journal (DMW), of doctors who, in the majority, were in academic leadership positions. Each doctor was asked “When is a doctor a good doctor?”. The responses were assigned into nine categories, from which, the most common responses were having sufficient knowledge and empathy, though these attributes were only mentioned by 23% and 21% participants, respectively. Other related characteristics such as sufficient practical ability and caring for patients were mentioned by 9% and 12% participants. Except for life-long learning (10%), no other characteristics had a double-digit percentage, showing that there was little agreement among participants.
Lambe and Bristow,24 in a Delphi survey of 10 clinicians, asked participants to rank, in three rounds, 20 characteristics of good doctors on a 5-point Likert scale. The 10 most important were: patient care; probity; communication and listening skills; recognizing own and others’ limits; empathy and being non-judgmental; adaptability; lifelong improvement; compassion; commitment and motivation; and being a team player. However, the study is limited by having only 9 males and one female participant, and by the participants’ inability to add or modify any of the proposed characteristics. Yazdi et al25 conducted a qualitative study asking patients open-ended questions about a “good physician”, from which they obtained a similar list of characteristics but with the addition of the physician’s appearance, grooming and personal characteristics. Such responses were then used to construct a questionnaire for 150 Iranian physicians, of which 100 responded, who largely agreed with the patients’ point of view, except that they put a much lower value on appearance and personal characteristics. Fones et al26 compiled a list of characteristics of a good doctor from a Medline search and three focus groups, then developed Likert questions for a survey of 274 doctors and 400 members of the public in Singapore. Good general agreement in ranking the characteristics between doctors and members of the public was achieved, with the public rating cognitive qualities and communication abilities more highly, while doctors rating ethics more highly.
Schenck and Churchill27,44 interviewed 40 doctors, and 10 complementary and alternative practitioners, for a book on how to become an “expert healer”, summarized as: 1) do the little things, ie, good manners; 2) take time and listen; 3) be open (be vulnerable, brave, face the pain, observant); 4) find something to like, to love about the patient; 5) remove barriers, ie, practise humility; 6) let the patient explain; 7) share authority; and 8) be committed and trustworthy. There was no mention of medical, organizational, or other competences. Apart from Schenck and Churchill’s work, there is little research on the relationship between medical doctors and healing. However, there are systematic reviews and meta-analyses exploring the relationship between medical doctors and patients’ physical or mental health outcomes.29–32
Summarizing, the editor of the BMJ reflected in 2002 that defining what a good doctor could be is nearly impossible. And after twenty years, there is still limited research approaching this subject. In terms of quantitative measures, previous systematic reviews and meta-analyses indicate that patients’ physical health outcomes and other performance indicators can be used to determine good doctors and exceptionally good doctors. However, looking from a qualitative approach, previous literature can be divided into reported qualities by patients, other health care workers, and medical doctors (peers). For the context of this study, the following qualities encompass what other medical doctors have considered that a “good doctor” should have, based on the reviewed literature:
- Personal characteristics (empathy, manners, be open, non-judgmental, compassion, adaptability, motivation, humility, team player).
- Good physician-patient relationships and caring for patients as people.
- Communication and listening abilities (taking time for listening, letting the patient explain).
- Medical competence and knowledge in diagnosis and interventions to apply.
- Ethics.
- Life-long learning (continuous education, research).
- Ability to liaise with others in the treatment of their patients, ie, management capability.
The qualitative characteristics of a good doctor were heterogeneous, particularly in how each author labelled them, though there were similarities. For example, Steiner-Hofbauer et al,22 used the term “Medical competence”, which may have similar meanings to what Herzig et al,23 named “sufficient knowledge and sufficient practical ability”, and Fones et al26 “cognitive domain.” While empathy23,24 could be part of the “general interpersonal qualities”,22 “physician-patient relationship”,25 or refer to “find something to like, to love about the patient.”27
The Present Study
The authors of this study have previously systematically reviewed studies reporting doctors’ effects on patients’ physical health outcomes beyond those explained by known factors such as doctor experience.33,47,48 Results showed there are doctors that have exceptional patient outcomes that are not explained by known factors, suggesting exceptional doctors exist. The aim of the present study is to qualitatively study the opinions of medical doctors on their experiences of exceptional doctors and what made these doctors exceptionally good.
Methods and Study Design
Study Design
The present study design is a qualitative approach involving an in-depth, exploratory data collection and thematic analysis. We conducted semi-structured interviews with medical doctors that spoke English. The study design is further explained in detail in the published protocol.34
Each of the interviewees was asked three questions:
- What, in your opinion, makes an exceptionally good doctor?
- Do you have an experience with such a doctor, and how was that experience?
- Do you consider yourself to be an exceptionally good doctor?
The interviewer summarized at times during the interviews what had been said and asked the interviewee whether the summary was accurate, in addition to asking for more details to answers already given, if further clarification was needed. All interviews took place via zoom,35 by distance, apart from one case where the interviewer and interviewee were in the same room. Zoom was used for recording in the single same-room interview due to its integration with otter.ai,36 which was used for live transcription, from which the transcript was then revised and edited by a transcription typist, according to the saved audio recording. For accuracy, the interviewer re-reviewed the transcripts for any errors. NVivo software37 was used to mark up the transcripts with codes that later were used to identify themes, as per the procedures outlined for thematic analysis. The interviewees received a copy of their transcript and were offered to freely edit it.
Participants and Recruitment
The participant inclusion criteria were medical doctors of any specialty, currently working in the public or private sectors, who speak English. Participants were recruited through professional acquaintances of the authors, contacting 216 authors of relevant research papers, and the GP recruitment program of the Institute of Evidence-based Healthcare of Bond University.
The sample size was determined by data saturation38 which was achieved with 10 interviews, with the next three interviewees confirming and repeating concepts and characteristics of exceptionally good doctors that were already introduced by earlier interviewees. The sample size was also guided by the concept of information power39 which indicates that when the aim of the study is broad, as in our case, the selection of participants should be specific, to help keeping the information relevant for the actual study topic.
Taking into consideration that the participants are medical doctors who had an opinion and experience of exceptionally good doctors, the quality of the dialogue was expected to be high. In addition, the interviewer was experienced, and the analysis strategy required sufficient variation among the answers. Thereby, the estimate of interviewees needed was 10–25 doctors, with saturation expected once no new themes were introduced in three successive interviews, which was the case after 13 interviews.
As there is no established theory on what makes an exceptionally good doctor or what their impact is, this study also has a strong exploratory element.39
Bias
According to Braun and Clarke, “Bias as a concept does not apply as a valid critique of qualitative research”40 as the researchers’ personal history, assumptions and perspectives do affect the research, making it subjective. This subjectivity, according to Braun and Clarke, is seen as a strength by most qualitative researchers. However, to reduce bias, the interviews were done by a non-clinician (CS) who is experienced in interviews as a part of his profession as a financial adviser. CS limited his interviewing to only asking what the interviewees’ opinions and experiences of exceptionally good doctors are, whether the interviewee considers him or herself to be an exceptionally good doctor, and to summarize points or ask for clarification or expansion of anything unclear.
Analysis
The analytical approach used consisted of thematic analysis as an experiential framework, inspired by Braun and Clarke,40–42 described in detail in the published protocol.34
To summarize, this is a qualitative study of semi-structured interviews that seeks to understand doctors’ thinking and experiences of exceptionally good doctors. The approach is inductive without a prior coding frame or the authors’ “analytical preconceptions”.43 From the transcript, a number of themes emerged, together with relevant quotations from the interviews in an inductive process using a realist epistemological perspective, a perspective which assumes that truthful knowledge about exceptionally good doctors can be obtained.
Results
Thirteen medical doctors were eligible and consented to be interviewed and have their anonymized responses published. Six were recruited through professional acquaintances of the authors, three (out of 216 contacted) were authors of relevant research papers, and four were from the GP recruitment program of the Institute of Evidence-based Healthcare of Bond University. Five of the 13 participants were females; age groups ranged from the 30s to the 80s.
Four doctors were primary care specialists, four were other specialists, three served as primary care specialists and medical researchers, one was a specialist and medical researcher, and one was a clinician and medical educator. Eight interviewed doctors have practiced in Australia, two in the US and UK, and one each in Egypt, The Netherlands and South Africa. Seven considered themselves as exceptionally good doctors, while the other six did not. All interviewed doctors have practiced as clinicians and, except for three, are still currently practicing. Demographic details are provided in Table 1.
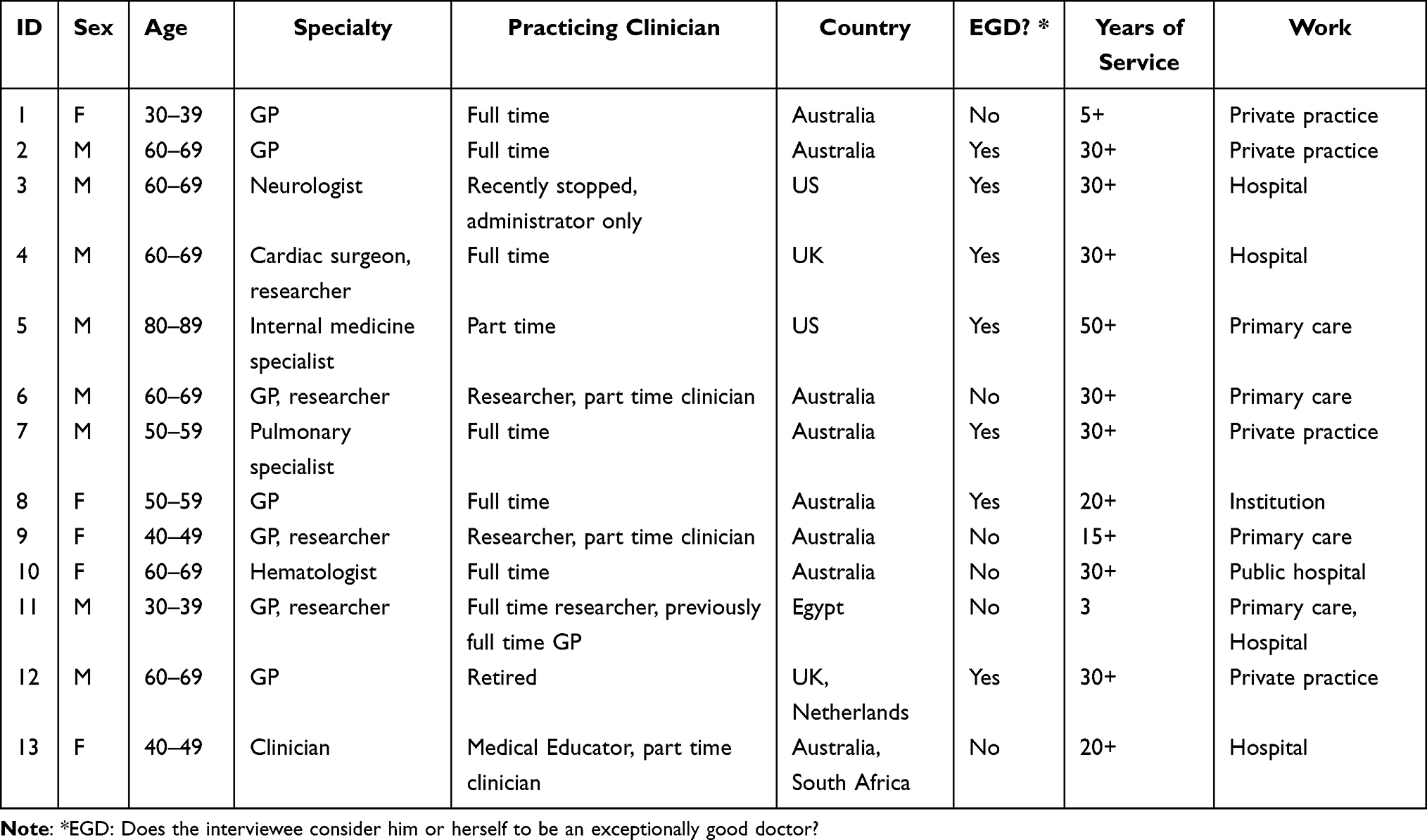 |
Table 1 Descriptive Details of Interviewees |
A very commonly expressed opinion, explicitly mentioned by 11 of the 13 interviewees, was that it takes multiple traits to be an exceptionally good doctor, most importantly to have both in-depth medical knowledge and the ability to communicate with patients. This requirement was expressed in different ways, with the common thread being that you cannot be an exceptionally good doctor unless you have excellent medical knowledge, ability, and understanding, however, this needs to be accompanied by the ability to speak and listen to the patient so that they feel taken care of and looked after. Some interviewees mentioned an exception to those dual requirements, with regards to surgeons with very outstanding surgical skills but not necessarily great communication skills. Otherwise, the consensus was that it takes multiple skills to be an exceptionally good doctor.
We generated six themes from the transcribed data (Table 2):
- Character traits, ie, what type of personality do exceptionally good doctors have?
- Characteristics other than character traits: how do exceptionally good doctors act?
- Patients, how do exceptionally good doctors treat patients and do their outcomes differ?
- Their relationships with their peers and the health care system they work in.
- Education and exceptionally good doctors.
- Treatment examples of exceptionally good doctors.
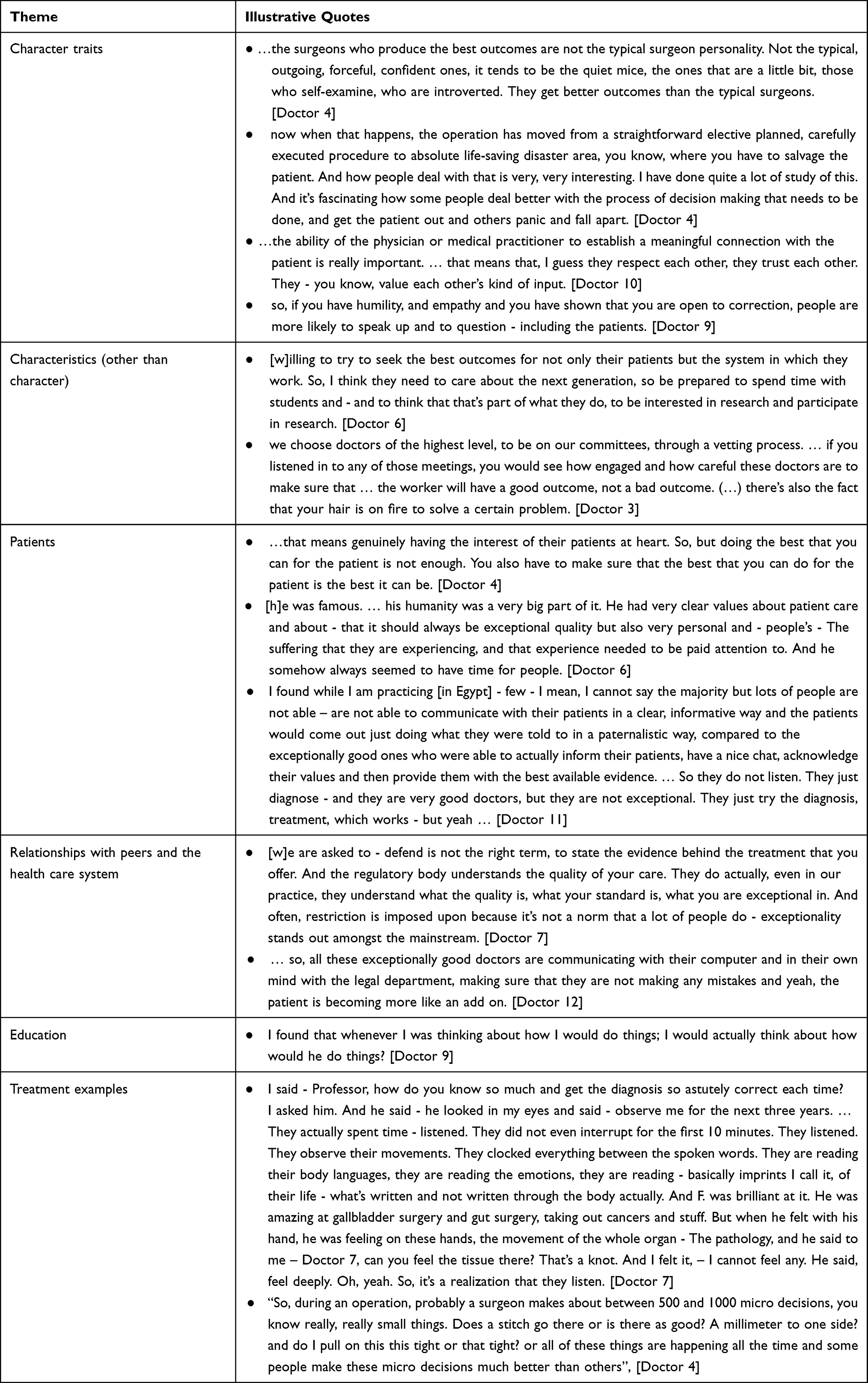 |
Table 2 Themes and Illustrative Quotes of “What Makes an Exceptionally Good Doctor?” |
Table 2 “Themes and Illustrative Quotes of ‘What makes an exceptionally good doctor?” is also a table of thematic analysis.
Character Traits
All the respondents mentioned character traits of exceptionally good doctors by painting a picture of a humble person who is a good communicator, adaptable, personable, with self-awareness and honesty. Three doctors each also mentioned confidence, being incorruptible, having integrity, being open minded, and having will, and drive or determination.
Nine of the doctors mentioned humility, which manifested itself in many ways, eg, “they don’t have ownership over that particular diagnosis” (Doctor 1), or an exchange reported by a GP (Doctor 2) where a cardiologist treated him as an equal. Similarly, Doctor 6 stated: “So they’re basically perfectly ready to be wrong multiple times with a patient until everything actually fits” and “they are happy to be wrong”.
Humility was also quoted in ways beyond patient diagnostics, in terms of how they relate to their colleagues, as Doctor 7 relates:
F. (…), for example, was a head of a major hospital in Hong Kong and US. But you know what; when you chat to him, he’s like a next-door neighbor, a brother. And he was amazingly humble - although super qualified. And the other two were the same. Super qualified, father of medicine, father of respiratory medicine, but you can have a barbecue with him … and say, ‘Paul, Doctor 7, Tom’ - by first name basis. I mean, where do you find that? Amazing, isn’t it?
Another aspect of humility, as per Doctor 10, is of these doctors doing things “Where they are outside of their comfort zone”, as she stated: “So that they are experiencing what it’s like to not be the best” and proceeded
the ability to see the humanity in another person no matter how broken or scarred that humanity may look and recognize that I am no better. … So, I have no right to judge that person or to put them down.
Such humility reflects the description of Schenck and Churchill,27,44 though none of the interviewees mentioned any religious aspect to that humility but considered it more of a trait rather than something to “practice”. The only other report we have found regarding humility was in a qualitative study of medical students on the “good doctor”.45
Congruent with previous qualitative studies, eight interviewees mentioned that being a good communicator is necessary.
In terms of being adaptable, Doctor 4 reports:
But, more important than all of the technical aspects is the ability to make good decisions. So, I think that is much more important in order to make a good surgeon that gets good outcomes for their patients than technical skills.
An example of adaptability, humility, listening to the patient and thoroughness is given by Doctor 7:
Every patient, every person, every being is different. Every person has a different reading. So how can you be generalized into a sample or whatever, a random whatever. So that makes exceptional physicians more humble because you can’t let go - be complacent. … I got books everywhere. … But when I’m with a patient, I’m totally dedicated to listening - by listening I don’t know - something comes up, an impress is given, the whole package of treatment comes through - more and more than ever before. And that’s what [three famous and exceptionally good doctors] did all the time.
Finally, Doctor 9 argued on the effects of the personality of exceptional doctors:
[I]t’s actually the doctors that do get listened to are the ones who shout the loudest and complain the most, not necessarily - which is almost the opposite of what we’ve been discussing. You know, the importance of humility and patience and almost by definition, an exceptional doctor is not going to be pushy and demanding and insist on change the way that they want it because that’s not really within their - their personality or this - The way that they’ve developed their skill sets.
Characteristics Other Than Character Traits
All respondents mentioned characteristics with regard to how exceptionally good doctors act. The most mentioned was having up-to-date and in-depth knowledge, the ability to understand evidence, and the commitment to good medical practice. Further characteristics were the ability to minimize errors and, if necessary, go beyond the guidelines. Six of the doctors mentioned time management and being able to network, ie, build good personal and professional relationships. Five mentioned the ability to not over-diagnose, over-prescribe, or to use drugs and medicines as a last resort. Four participants have experienced exceptionally good doctors as being excellent teachers; excellent diagnosticians; doctors with excellent technical skills; such doctors not being defined by their work; and having patience with people. In addition, wisdom, charitable or volunteer work, compassion, and perfectionism were independently mentioned three times. These characteristics are consistent with studies cited earlier,24,27,44 however, the interviewees in this study have provided further details.
With regard to commitment to good medical practice, Doctor 1 spoke about going beyond the individual
But the bigger picture focus as well, I think, also support some doctors to have that focus because they really care about, you know - Yeah, people on a broader scale.
In addition, Doctor 3 considered that a commitment to good medicine takes resilience:
They’re able to recognize the perverse incentives in the system in the health system they work in among his colleagues, among the doctors, he’s referring patients to, the drug and device companies which are out there constantly. The drug companies are sending drug reps into their offices all the time. You have to be able to recognize all this stuff and basically say, that’s not good medicine. I’m not going to do that.
Patients
Exceptionally good doctors relate well with patients and work on those relationships; care for patients and respect them; see them as a whole person, not just a lesion, illness, or collection of symptoms; ask patients to do their part; know them well and comprehensively assess and investigate them. All these items were mentioned by at least eight out of the 13 interviewed doctors. Moreover, seven mentioned doctors being good listeners, trusted by their patients, and giving patients sufficient time irrespective of the time pressure on the doctors. Empathy was mentioned by four doctors.
Caring was described by Doctor 1:
it was really the baseline for this particular doctor to really delve into everything to see where there might be some sort of nook or cranny where there could be pathology coming from or, you know, some way to support the person.
Furthermore, Doctor 5 explained caring in the form of the doctors who make themselves available:
a good doctor, an exceptional doctor will say, you know, I’m a busy person. But here’s my number. Here’s my card. Here’s my email. Here’s my text. … So, get in touch with me if you need to. Not many doctors are like that.
Doctor 1 had received feedback from multiple patients about exceptional colleagues who described their caring:
[P]eople have really raved about them. So, they’ve sort of experiences - and one of them [exceptionally good doctors] I think, she allows people a lot of time to sort of, you know, do what they need to do and provides really good follow up of care as well. I think that might sometimes be to her detriment, but, you know, for her patients, that’s, that’s, you know, everything.
Doctor 6, considered a wider view of care:
You might be an exceptionally talented technician, but you won’t be an exceptional doctor unless you can translate that into the way you practice medicine, and in the way you show care for your patients and the way you are - also interact with your colleagues and with other staff.
Doctor 13 described caring in the same way but worded it slightly differently “ … it was more than just doing her job. She had sensitivity and a skill that I think was pretty, you know, unusual and exceptional”. Doctor 9 also agreed with the other interviewed doctors:
[T]he most exceptional doctors that I have seen are doctors who genuinely appreciate and listen to their patients in a humble way that validates the patient’s perspective.
Relationships with Peers and the Health Care System
Here the differences between doctors that range from acceptable or good to exceptionally good are most pronounced. Those who spoke about their experiences or the experiences of exceptional doctors that they observed, reported that exceptionally good doctors can be celebrated and supported but just as likely are being attacked by their peers and by the health care system in which they work, with little difference to how the poorest doctors are treated. Doctor 7 provides several points on this theme: “[Y]ou don’t really accept yourself as an exceptional physician until there’s enough collegial support”, and
When you keep getting constantly attacked and complained about, as one of my colleagues said to me - a surgeon, top surgeon - retired - while saying you must be doing okay, because I had the same thing, and we’re doing amazing work and they keep going after you, because really - when you’re at the forefront of medicine, or science or whatever, you brush off a lot of jealousy and comparison - all that. And so, when you’re leading forefront, you attract attention, that’s the way it is.
Doctor 7ʹs message in a further quote (Table 2) is both hopeful and sobering in that regulatory bodies do know when a doctor is exceptionally good but may impose restrictions anyway because the doctor is different from the standard. Doctor 8 talking about a colleague described the exceptional as “he was very courageous in this kind of world of medical legal fear”. Doctor 9 contrasts private and public practice:
“So as a general practitioner, if you are exceptional - because we are private practitioners, you’re going to do well because it’s essentially like having an exceptional business. … So, it will mean that you have no problems having or sourcing patients”, versus
[W]hen it comes to then working within a system like the public healthcare system, I think that I have seen exceptional doctors really struggle there and interesting that you point that out, because I think what I have seen is that bureaucracy kind of leans towards mediocrity. … And exceptional doctors are not always necessarily appreciated by their peers either because they can show what can be done. So, depending on how ambitious their peers are - as their peers, rather than seeing them as a mentor, see them as a threat. I have certainly seen doctors undermine the exceptional amongst them because they feel they don’t want to be shown up. That’s within the public health system.
In contrast, Doctor 12 (Table 2) and Doctor 2, respectively, have a bleak view, and a significant concern:
Yeah, I think most of the angst in my life comes from those two things. The risk of litigation because I work outside the current prevailing paradigm, as flawed as it is and two, Medicare looks at algorithms. Medicare, persecutes the very bad and the very good … Once Medicare highlights you as being a problem, when you go to the tribunal, no matter how much evidence you’ve put in to the contrary, no one’s won.
Education and Exceptionally Good Doctors
Only one of the previously published qualitative studies considered education in the context of good doctors44 advocating teaching interpersonal skills to improve the healing ability of practitioners, while the editors of the BMJ special edition on what makes a good doctor4–8,10,11 were aware that doctors could be trained to a certain, unspecified standard but did not expect to do better than that.
Doctor 7 was very clear about the importance of education:
So, the thing about exceptional doctors is that the exceptional doctors are trained by exceptional teachers, who are also doctors and teachers, … for example, in my case, I was mentored by three exceptional professors of medicine and surgery, and they were renowned … So, you will find that exceptional physicians actually have this lineage of exceptionality of teachers who are also equally exceptional. There are exceptions of course, there are people who come out of nowhere, become exceptional, but they’re uncommon. Because to be exceptional, you need a role model, you need reflection, you need inspiration.
Doctor 5 similarly reported: “Why shouldn’t exceptional doctors, the experts on being exceptional, why shouldn’t they share their expertise?”.
Treatment Examples
The interviewees provided more than 50 quotes on examples of exceptionally good doctors in action. It seems that there is a strong offer of learning from such doctors when another doctor observes an exceptionally good doctor in action.
Doctor 3 commented on medication prescribing:
So, if you’re, if you have somebody on opioids, or a potentially dangerous drug, do you track their pain and function to see if they’re getting better, or not getting better from using those medications or documenting any improvement in function and not just using them you know, to feel better? … [T]hey use other best practices like they stay away from more dangerous practices like high opioid doses. You know, they much more carefully use potentially dangerous substances. … they could also be characterized by what they don’t do.
Doctor 4 gives a treatment example at the bottom of Table 2 on the difference between surgeons in the quality of their work stated, and speaks about responding to patients, coupled with humility:
[Surgery] patients will have been extremely anxious and very jumpy and threatening to go out of the hospital and not wanting to be treated. All I need to do is to speak to them for two minutes. And I can see the reassurance in that my voice carries gravitas, but that doesn’t necessarily mean that I have gravitas.
Doctor 6 described a truly exceptional surgeon:
[T]here was a surgeon there, who came from Africa … He was so fast and so little bleeding - so accurate, he made it all just easy. Like - how is he doing this, it’s like magic – and I think he just had so much experience cause he had been a surgeon for this hospital, he did orthopedics, he did neurosurgery, he did - while he was in Africa, he even did obstetrics. He just did all the surgery for this hospital. For whatever thousand population. And so just the degree of surgical experience he had was vast, a lot more than most of the British surgeons - who had a lot of experience but they just weren’t in the same league. Seemed to me and you can see it, he just moves right. You can see it. And the consultants could too. Yeah, you could see it - so that was a technical expertise. And he could sort of come and solve problems when things went wrong. Occasionally did some stitches - he would come in and he would just sort it out. … [in a vulvectomy] the consultants were doing one side and he was doing the other, and he was doing his side much faster and much better, with minimal bleeding, compared to the consultant. You could see these two surgeons - you don’t often see that, both doing basically the same procedure just on one side of the body versus the other side, and how much better that one was than that. … [H]e would have had such a big case load that you would need to go fast as well. Not hurry, but fast. And I think exceptional technicians manage to do things with minimal movements. There’s not - there’s a real economy of movements. They don’t do - they don’t fluff around. They actually just do things in a - everything is done, that’s necessary to be done. There are not lots of extra stuff.
Doctor 13 considered that the doctor does well when the work matches their skillset:
I think you can be a good doctor and be very different beings. It’s more about, you know - The skill set matching the job and the situation that you’re working in. So, I think when there’s a good match, it’s amazing.
She gave two specific examples of exceptionally good doctors:
“She made it about people and understanding each other and she focused on resolving the distress and the conflict, which is what was better for everybody in that situation. It was better for the staff and for the family. And it’s - it took a lot of the stress out of it and it resolved things in a way that seemed a lot healthier to me, and it was very compassionate. There was a lot of compassion and caring and understanding within that.”,
And so the situation tends to escalate quite quickly and when this particular anesthetist - just as soon as he walked in the room, it’s like everything kind of calmed down, and he - he was in charge.
Doctor 12 mentioned a seemingly small change using solution focused conversation technique or solution focused brief therapy (SFBT) that has made him, as a GP, much more effective, which also shows the importance of communication:
Because, at first if a person came in very stressed, I was really doing my best - so why don’t you go do some fishing or so or go play some golf and then they said - ah! I don’t like fishing or don’t like - but if you ask, again, what sort of things helped you in the past and they may say, well, in the past I just went for fishing and whatever. So, they provide the answers. So, you need to have a good, good way of asking things. And so that’s I think, an essential part that needs to get into general practice training.
Doctor 11 describing an exceptional good doctor in Egypt, stated:
What made him very exceptional is that he dedicates one day per week for the poor, free of charge, free consultation and he is specialized in kidney diseases - and this is - like, giving one day per week, that’s - if you transfer it in money - that’s lots of money to do. Like he’s not getting any money out of it, which is amazing. He continues to publish lots of research articles along with his clinical work. He does work in a hospital for free as well beside his other day outside the hospital and he has his own private clinic where he sees patients and he always accepts referral from like communities whenever someone is not able to pay, he always provides a consultation.
Additionally, two personal examples from doctor 10:
My mom’s orthopedic surgeon that did her shoulder replacements for her. He was technically like, he’s probably the best surgeon in [an Australian state] for that, but he was just so humble and kind of, you know, just connected sort of with mom and treated her so well.
And ultimately, the palliative care team was really the main team that actually truly sat down with us and listened to what dad wanted, and I thought that was - you know, their care was exceptional and was so like, we just felt it so valuable because they allowed him to have some control over what was happening to you.
Strengths and Limitations of This Study
- One strength of this work is that the concept and design were informed by the recent experience of the authors in systematically reviewing over 10,000 studies on doctors’ or surgeons’ effect on patients’ physical health.
- A limitation is that this is a survey of respondents who speak English and was limited to doctors who have worked in Australia, the US, UK, South Africa, the Netherlands, and Egypt, hence this survey may not be representative of medical doctors worldwide.
- A further limitation is the small sample size of the study and therefore further studies need to potentially interview a larger sample of doctors with different backgrounds and characteristics to make the results more generalizable.
- Another limitation is that only three interviewees have a background outside the Anglo-American culture, ie, Egypt, The Netherlands, and South Africa and none of the three is still living in those countries. The concept of an exceptionally good doctor may differ substantially in other cultures and patient well-being might also differ in its definition.
- Finally, due to the heterogeneity regarding medical/surgical specialties, types of interventions, and types of outcomes relevant to different interventions, there may be differing criteria on what makes an exceptionally good doctor for different medical/surgical specialties.
Discussion
Each of the 13 interviewed medical doctors had an opinion on what makes an exceptionally good doctor and experienced at least one such doctor. All considered their encounter with such a doctor to be a valuable and inspirational experience, especially when they met them during their studies or early in their careers. Twelve of the 13 interviewed doctors associated being an exceptionally good doctor with better patient health outcomes, while the 13th associated it with better patient care. In addition, exceptionally good doctors, according to our sample, are valuable to patients, other doctors, medical education, and medicine overall.
This study is providing two types of characteristics that have previously not been mentioned in the literature or only in a limited way: The education of exceptionally good doctors, ie, how they can be made, and their relationships with their peers and the health care system. Further, we are not aware of treatment examples by such doctors, nor a distinction between good and exceptionally good doctors in the existing literature.
Despite the ubiquity of having experienced exceptionally good doctors, there is little research investigating this topic. The available literature is mostly about good doctors, or how to improve doctor performance.22–28
Surprisingly, when reviewing the transcripts, there were many exceptionally good doctors who had been undermined by their peers or the health care system, even when their peers were fully aware that their targets were exceptionally good doctors. Such a cultural trait may be worth further scrutiny and research on how to change this culture, especially since there seem to be very substantial benefits for fellow doctors or medical students encountering exceptionally good doctors and being trained by them. Another concern is that the current culture provides an incentive towards doctors being average rather than exceptional. Presumably, this culture comes with a high cost for patients and health care providers and doctors themselves, who then may not practice medicine to their true potential.
Previous research has shown that there are psychotherapists who have exceptionally good patients’ mental health outcomes46 and surgeons who have exceptionally good patients’ physical health outcomes,33 but none of the studies that identified such surgeons even considered whether it may be worthwhile to study exceptionally good doctors in more detail. In the current study, there was a strong overlap between the opinions expressed: that an exceptionally good doctor needs to have multiple traits to be considered exceptionally good, with the exemption of some surgeons with primarily exceptional surgical skills. However, it was agreed that, at the minimum, such doctors need to have both substantial up-to-date medical knowledge and a high level of communication abilities in dealing with patients. Further, in addition to their high abilities, exceptionally good doctors were humble in accepting that they may need help, or be wrong at any given moment, which means that they are often adaptable, being able to react to the unexpected and therefore, ready, if necessary, to go beyond the guidelines, while giving patients the time they need. A simple example of how exceptionally good doctors differ from other doctors, is that such doctors listen very carefully to the patient and rarely interrupt them in the beginning of the consultation. Such a quality of listening seems eminently able to be developed through practice, or to be passed on as a skill to doctors through teaching, along with many other such transferable skills.
All interviewees admiringly spoke about their encounters with exceptionally good doctors and how they were inspired by them or took them on as role models, with one interviewed doctor unambiguously stating that most exceptionally good doctors are exceptional because they were trained by equally good doctors. Considering this, if such role models could be more accessible to medical students, junior doctors, and perhaps even experienced doctors, then, this would introduce the potential to inspire such students and junior doctors by showing them what is possible despite the constraints they are working under.
Recommendations
We thank one of the anonymous reviewers for the following insights:
- The results can help in the design, implementation or reformulation of curricula aimed at training physicians, towards training exceptionally good doctors.
- The topic discussed in this manuscript is relevant in medical education as well as on the training of other health professionals. Though it might be differences in perceptions about what are exceptionally good doctors across the world due to multiple factors, it will inspire other medical educators in cultivating and on the definition of such exceptionally good doctors.
Further research on exceptionally good doctors that acknowledges cultural differences and sample sizes is needed in order to develop a conceptualization model proposal. Identifying exceptionally good doctors, how to learn from them, increase their number, and change the culture to accept them is recommended. Researching other stakeholders such as patients and administrators on their opinions on and experiences of exceptionally good doctors is also recommended.
Conclusion
Many doctors have met exceptionally good doctors and have learnt from them and were inspired by them. Despite that, there has been little research on exceptionally good doctors and such doctors regularly, though not always, are undermined by their peers and their health care system precisely because of the quality of medicine they practice.
Disclaimer
The views expressed are those of the authors and not necessarily those of Bond University.
Data Storage
Data will be stored in a secured location at Bond University for a period of 5 years after the end of this project as per 601.3/C150 of the Qld Government University Sector Retention and Disposal Schedule in accordance with the guidelines set out by the Bond University Human Research Ethics Committee.
Ethics Approval
Ethical approval Number CS03393 has been received from the Bond University Human Research Ethics Committee on September 27th, 2021.
Consent
All participants have provided their informed consent, including consent for publication of anonymized responses.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation of data, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This review has been funded by the first author as part of his PhD studies. No external funding was received.
Disclosure
All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf, and declare: no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
References
1. National Ambulatory Medical Care Survey. 2018 National Summary Tables; 2018.
2. Balint M. THE DOCTOR, HIS PATIENT, AND THE ILLNESS. Lancet. 1955;265(6866):683–688. doi:10.1016/S0140-6736(55)91061-8
3. Curran J. The doctor, his patient and the illness. BMJ. 2007;335(7626):941. doi:10.1136/bmj.39384.467928.94
4. Hurwitz B. What’s a good doctor, and how can you make one? BMJ. 2002;325(7366):667–668. doi:10.1136/bmj.325.7366.667
5. BMJ. The BMJ's wild goose chase. Br Med J. 2002;325(7366).
6. Cumming A. Good communication skills can mask deficiencies. Br Med J. 2002;325(7366):676. doi:10.1136/bmj.325.7366.676/a
7. McCrorie P. Graduate students are more challenging, demanding, and questioning. Br Med J. 2002;325(7366):676. doi:10.1136/bmj.325.7366.676
8. Pringle M, Wilson T, Grol R. Measuring “goodness” in individuals and healthcare systems. Br Med J. 2002;325(7366):704. doi:10.1136/bmj.325.7366.704
9. Elsevier. Scopus. Elsevier; 2021.
10. Holmes J. Good doctor, bad doctor-a psychodynamic approach. Br Med J. 2002;325(7366):722. doi:10.1136/bmj.325.7366.722
11. Paice E, Heard S, Moss F. How important are role models in making good doctors? Br Med J. 2002;325(7366):707. doi:10.1136/bmj.325.7366.707
12. Begg CB, Riedel ER, Bach PB, et al. Variations in morbidity after radical prostatectomy. New Engl J Med. 2002;346(15):1138–1144. doi:10.1056/NEJMsa011788
13. Bianco FJ
14. Bianco JFJ, Vickers AJ, Cronin AM, et al. Variations among experienced surgeons in cancer control after open radical prostatectomy. J Urol. 2010;183(3):977–983. doi:10.1016/j.juro.2009.11.015
15. Brown EC, Robicsek A, Billings LK, et al. Evaluating primary care physician performance in diabetes glucose control. Am J Med Qual. 2016;31(5):392–399. doi:10.1177/1062860615585138
16. Glance LG, Dick A, Osler TM, Li Y, Mukamel DB. Impact of changing the statistical methodology on hospital and surgeon ranking: the case of the New York State cardiac surgery report card. Med Care. 2006;44(4):311–319. doi:10.1097/01.mlr.0000204106.64619.2a
17. Gossl M, Rihal CS, Lennon RJ, Singh M. Assessment of individual operator performance using a risk-adjustment model for percutaneous coronary interventions. Mayo Clin Proc. 2013;88(11):1250–1258. doi:10.1016/j.mayocp.2013.07.017
18. Harley M, Mohammed MA, Hussain S, Yates J, Almasri A. Was Rodney Ledward a statistical outlier? Retrospective analysis using routine hospital data to identify gynaecologists’ performance. Br Med J. 2005;330(7497):929–932. doi:10.1136/bmj.38377.675440.8F
19. Kunadian B, Dunning J, Roberts AP, Morley R, de Belder MA. Funnel plots for comparing performance of PCI performing hospitals and cardiologists: demonstration of utility using the New York hospital mortality data. Catheter Cardiovasc Interv. 2009;73(5):589–594. doi:10.1002/ccd.21893
20. Landercasper J, Borgert AJ, Fayanju OM, et al. Factors associated with reoperation in breast-conserving surgery for cancer: a prospective study of American society of breast surgeon members. Ann Surg Oncol. 2019;26(10):3321–3336. doi:10.1245/s10434-019-07547-w
21. Rudmik L, Xu Y, Alt JA, et al. Evaluating surgeon-specific performance for endoscopic sinus surgery. JAMA Otolaryngol Head Neck Surg. 2017;143(9):891–898. doi:10.1001/jamaoto.2017.0752
22. Steiner-Hofbauer V, Schrank B, Holzinger A. What is a good doctor? Wien Med Wochenschr. 2018;168(15–16):398–405. doi:10.1007/s10354-017-0597-8
23. Herzig S, Biehl L, Stelberg H, Hick C, Schmeißer N, Koerfer A. What makes a doctor a good doctor? A content analysis of assessments by a sample of doctors. Dtsch Med Wochenschr. 2006;131(51–52):2883–2888. doi:10.1055/s-2006-957216
24. Lambe P, Bristow D. What are the most important non-academic attributes of good doctors a Delphi survey of clinicians. Med Teach. 2010;32(8):e347–e354. doi:10.3109/0142159X.2010.490603
25. Miratashi Yazdi SN, Nedjat S, Majdzadeh R, Arbabi M. Who is a good doctor? Patients & physicians’ perspectives. Letter. Iran J Public Health. 2015;44(1):150–152.
26. Fones CSL, Kua EH, Goh LG. ‘what makes a good doctor?’ - views of the medical profession and the public in setting priorities for medical education. Article. Singapore Med J. 1998;39(12):537–542.
27. Churchill LR, Schenck D. Healing skills for medical practice. Ann Intern Med. 2008;149(10):720–724. doi:10.7326/0003-4819-149-10-200811180-00006
28. Hanyok LA, Hellmann DB, Rand C, Ziegelstein RC. Practicing patient-centered care: the questions clinically excellent physicians use to get to know their patients as individuals. Patient. 2012;5(3):141–145. doi:10.2165/11599530
29. Holt PJE, Poloniecki JD, Gerrard D, Loftus IM, Thompson MM. Meta-analysis and systematic review of the relationship between volume and outcome in abdominal aortic aneurysm surgery. Br J Surg. 2007;94(4):395–403. doi:10.1002/bjs.5710
30. Huo YR, Phan K, Morris DL, Liauw W. Systematic review and a meta-analysis of hospital and surgeon volume/outcome relationships in colorectal cancer surgery. J Gastrointest Oncol. 2017;8(3):534–546. doi:10.21037/jgo.2017.01.25
31. Leow JJ, Leong EK, Serrell EC, et al. Systematic review of the volume–outcome relationship for radical prostatectomy. Eur Urol Focus. 2018;4(6):775–789. doi:10.1016/j.euf.2017.03.008
32. Meagher AP. Colorectal cancer: is the surgeon a prognostic factor? A systematic review. Med J Aust. 1999;171(6):308–310. doi:10.5694/j.1326-5377.1999.tb123665.x
33. Schnelle C, Clark J, Mascord R, Jones MA. Is there a surgeons’ effect on patients’ physical health, beyond the intervention, that requires further investigation? A systematic review. Ther Clin Risk Manag. 2022;Volume 18:467–490. doi:10.2147/TCRM.S357934
34. Schnelle C, Jones MA. Protocol for a qualitative study on doctors’ opinions on and experiences of exceptionally good doctors. Adv Med Educ Pract. 2022;13:103–109. doi:10.2147/AMEP.S343554
35. Inc Z. Zoom Videoconferencing; 2022. Available from: https://zoom.us/.
36. Otter.ai. Record and review in real time. Search, play, edit, organize, and share your conversations from any device; 2022. Available from: https://otter.ai/.
37. NVivo (Version 12); 2018. https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home?_ga=2.258719299.835966230.1648946019-1691335512.1648946019.
38. Braun V, Clarke V. To saturate or not to saturate? Questioning data saturation as a useful concept for thematic analysis and sample-size rationales. Qual Res Sport Exerc Health. 2021;13(2):201–216. doi:10.1080/2159676X.2019.1704846
39. Malterud K, Siersma VD, Guassora AD. Sample size in qualitative interview studies: guided by information power. Qual Health Res. 2016;26(13):1753–1760. doi:10.1177/1049732315617444
40. Braun V, Clarke V. Successful Qualitative Research: A Practical Guide for Beginners. sage; 2013.
41. Braun V, Clarke V. What can “thematic analysis” offer health and wellbeing researchers? Int J Qual Stud Health Well-Being. 2014;926152. doi:10.3402/qhw.v9.26152
42. Clarke V, Braun V. Thematic analysis in “Encyclopedia of critical psychology”. In: Encyclopedia of Critical Psychology. Springer; 2014:1947–1952.
43. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
44. Schenck D, Churchill L. Healers: Extraordinary Clinicians at Work. Oxford University Press; 2011.
45. Cuesta-Briand B, Auret K, Johnson P, Playford D. ‘A world of difference’: a qualitative study of medical students’ views on professionalism and the ‘good doctor’. BMC Med Educ. 2014;14(1):77. doi:10.1186/1472-6920-14-77
46. Lambert MJ. Bergin and Garfield’s Handbook of Psychotherapy and Behavior Change. John Wiley & Sons; 2013.
47. Schnelle C, Jones MA. The doctors’ effect on patients’ physical health outcomes beyond the intervention. A methodological review. Clinical Epidemiology. In Press 2022.
48. Schnelle C, Clark J, Mascord R, Jones MA. Is there a doctors’ effect on patients’ physical health, beyond the intervention and all known factors? A systematic review. Ther Clin Risk Manag. In Press 2022. doi:10.2147/TCRM.S372464
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.