")
Back to Journals » International Journal of Women's Health » Volume 15
Qualitative Exploration Study of Perceptions of Women and Nurse-Midwives on Antenatal Care Information and Communication in Tanzania
Authors Heri R , Mselle LT , Malqvist M
Received 22 November 2022
Accepted for publication 5 May 2023
Published 5 June 2023 Volume 2023:15 Pages 927—941
DOI https://doi.org/10.2147/IJWH.S398710
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Rashidi Heri,1 Lilian Teddy Mselle,2 Mats Malqvist3
1Department of Nursing Management, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania; 2Department of Clinical Nursing, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania; 3Department of Women’s and Children’s Health, Uppsala University, Uppsala, Sweden
Correspondence: Rashidi Heri, Email [email protected]
Background: Antenatal health information enables pregnant women to make informed choices for their health during pregnancy and childbirth. Worldwide, evidence shows inadequate coverage of the information provided to women during antenatal care visits. Interaction between women and providers is important to ensure effective information exchange. This study aimed to explore women’s and nurse midwives’ perceptions of their interactions and the information they shared about care during pregnancy and childbirth in Tanzania.
Methods: Formative explorative research using in-depth interviews was conducted with eleven Kiswahili-speaking women who had normal pregnancies and had more than three antenatal contacts. Also, five nurse-midwives who worked in the ANC clinic for a year or more were included in the study. A thematic analysis based on descriptive phenomenology guided the analysis of data that was informed by the WHO quality of care framework.
Results: Two major themes emerged from the data, enhancing communication and respectful delivery of ANC information and receiving information about pregnancy care and safe childbirth. We found that women felt free to communicate and interact with midwives. Some women feared interacting with midwives and other midwives were difficult to approach. All women acknowledge receiving antenatal care information. However, not all women reported receiving all ANC information as per national and international guidelines. Inadequate staffing and time were the reasons for poor prenatal care information delivery.
Conclusion: Women did not report most of the information provided during ANC contacts as per the national ANC guidelines. The inadequate number of nurse-midwives, increased number of clients, and insufficient time were reported to contribute to inadequate provision of information during antenatal care. Strategies for effective provision of information during antenatal contacts should be considered including using group antenatal care and information communication technology. Further, nurse-midwives should be sufficiently deployed and motivated.
Keywords: antenatal care, health information, pregnant women, maternal and infant mortality, Tanzania
Background
Antenatal care (ANC) helps early identification of high-risk pregnancies and educates women for positive labour outcomes. In ANC, women are provided with education and counselling, screening of diseases, and treatment to ensure better outcomes for the mother and fetus.1–3 Antenatal care is intended to reduce infant and maternal mortality rates, as well as stillbirths.2,3 Globally, the provision of antenatal health information has become a common component of antenatal care.
Maternal and infant mortality in Tanzania have remained high over the years despite various measures to reduce it. In 2016, maternal deaths accounted for 556 per 100,000 women.4 The trends of MMR have been changing from 578 in 2004, 454 in 2010, 556 in 2015,4 and 432 in the 2012 national census.5 Also, neonatal, infant and under-five deaths remained high. For example, in 2015, there were 39 perinatal, 25 neonatal, 43 infants, and 67 under-five deaths per 1000 live birth.4 Despite these changes, the rates of maternal and neonatal deaths, women’s attendance to ANC is continuously growing.4 For example, in 2010, almost all pregnant women (98%) received antenatal care from skilled personnel at least once during their pregnancy.4 Although the coverage of ANC attendance has increased, the quality of maternal and child health care is still inadequate.4,6
Tanzania government has implemented various interventions to reduce maternal and neonatal mortality rates. In 1971, maternal and reproductive health services were established which was followed by several approaches and programs including Expanded Program on Immunization,7,8 the Safe motherhood initiative 19898 and Integrated Management of Child Illness 1996.9 In 2002, the government adopted the focused antenatal care (FANC) approach following the World Health Organization recommendations.10 The FANC model integrates interventions such as health promotion, detection of diseases and treatment and it recognizes the antenatal period as a key entry point for pregnant women into the health system.6 FANC consisted of four contacts with health facilities and eight for the current WHO recommendations on antenatal care for a positive pregnancy experience.11 In each contact, the pregnant woman should be assessed, screened for risks, given education and counseling to improve her health and that of the fetus.12,13
The FANC model emphases on woman’s contact with health care provider focusing more on the number of contacts the woman makes and time when the first visit to ANC is made. The new guidelines, however, underscore the need to move from counting the woman’s contacts as a measure of success and focus on the content and process of care pregnant woman follows in antenatal care.14 The process involves the interaction between women and providers throughout the continuity of care15 and the content of education about antenatal care women receive during ANC contacts. In the WHO quality of maternal and newborn care framework, the process of care is divided into two main categories, the provision of care and experience of care. The provision of routine evidence-based care includes management of complications, actionable information and efficient referral system. The experience of care focuses on effective communication, provision of dignified and respectful care and emotional support.15 These elements of care and support are important in ensuring that women seek skilled care in the health care. It also fosters an environment conducive for learning and changing behavior for positive pregnancy outcomes. This paper is informed by the WHO quality of maternal and newborn care framework, focusing primarily on the experience of the care.
Effective communication between nurse-midwives and pregnant women ensures positive relationships, fosters a sense of reassurance, comfort and warmth. The positive relationship reduces negative emotion and may promote health practices among pregnant women.16 Effective communication is a tool for useful information delivery.
Evidence shows inadequate coverage of information and counselling provided in antenatal care clinics.17–21 A few similar studies conducted in Tanzania have addressed women’s knowledge of danger signs22 and the quality of counselling on danger signs.23 These studies have reported limited knowledge of danger signs by women and that many women were not informed about any danger signs during antenatal care visits. Other studies in Africa19 and the USA20 have reported the significance of health information during antenatal care and acknowledged inadequate coverage and quality of education and counselling provided in antenatal care clinics.21,24 Communication as a tool for effective information provision is problematic all over the world. However, a few studies in Tanzania have reported about experiences of communication and information provided to women during pregnancy. This study, therefore, explored women’s and nurse midwives’ perceptions of communication and information provision in the ANC clinic.
The rationale of this study was to examine the women’s and midwives’ perceptions of the communication and information provision in antenatal care in Tanzania. The findings identified the way women and nurse midwives view the communication process and care, elicit gaps and challenges involved in care interaction, and suggest ways to improve communication during the care process in an antenatal clinic. The relevance of addressing this question of how pregnant women and nurse midwives in Tanzania feel about communication and getting information and care at the ANC clinic is to ensure that we get evidence-based information to enable the improvement of communication and interaction during antenatal care, an area that is problematic in Tanzania. This paper therefore describes women’s and nurse midwives’ perceptions of their interaction and information shared during antenatal care.
Methods
Study Design and Setting
A formative descriptive qualitative research design25 using thematic analysis based on descriptive phenomenology was employed to explore women’s and nurse midwives’ perceptions of health information provided during antenatal contacts. The study was conducted in two districts of the Coast region of Tanzania, Kibaha and Bagamoyo districts. These districts were purposefully selected for the feasibility of group antenatal care intervention. In addition, Kibaha district was a semi-urban and Bagamoyo district was a rural setting, and both are close to Dar es Salaam commercial city of Tanzania. Specifically, the study was conducted in three health centres, Mkoani and Mlandizi in Kibaha District and Kerege in Bagamoyo District. The three health centres were chosen because of their high rates of ANC attendance. Monthly average antenatal attendance was 430 at Mkoani Health Center, 580 at Mlandizi Health Center, and 180 at Kerege Health Center.
The antenatal clinics in Tanzania have the following facilities for pregnant women’s care: waiting areas, registration, physical examination, and consultation room.12,26 The ANC services were divided into units including registration, education and counseling, physical examination and test, family planning, Prevention of Mother to Child Transmission (PMTCT) of HIV and postnatal care follow-up. The antenatal contacts were scheduled from 7.30 am to 3.30 pm. Because of shortage of staff, each unit was served by only one nurse midwife. Kerege health center antenatal clinic was highly understaffed with three midwives, while Mkoani health center antenatal clinic had 8 midwives and Mlandizi 7 nurse-midwives. Health education is the first activity provided in the health centre before other services begun, which was commonly done to all women who will be present during the time. After health education, women will head to receive other services including physical examination and laboratory tests. Understanding the impact of ANC information provided by nurse midwives in the context of increased number of clients and shortage of providers, especially nurse midwives,27 the authors wanted to learn from the participants the content of ANC information and communication between nurse midwives and women, and identify barriers to effective communication for designing strategies ensuring that appropriate and relevant content of ANC information is well understood by women hence improved experiences of childbirth and positive birth outcomes.
Participants and Recruitment
Participants for this study were purposively recruited.28 To be included in the study, women had to have made three or more scheduled antenatal contacts, had a normal pregnancy, and spoke Kiswahili. It was expected that women who have made more antenatal contacts are likely to have had adequate information about antenatal care. To gain diverse experiences women with varied characteristics in age, parity and level of education were considered. Nurse-midwives were either enrolled or registered with Tanzania Nursing and Midwifery Council (TNMC) and worked in ANC clinic for more than a year. Enrolled nurse-midwives in Tanzania are those with a certificate in nursing and midwifery education and registered nurse midwives have at least a diploma in nursing and midwifery.29 The researcher worked with the in-charge of antenatal clinics to identify eligible nurse-midwives and women. All participants provided written informed consent after they understood the purpose of the study, issues of confidentiality and voluntary nature of their participation in the study. In addition, participants were informed that their interviews would be audio recorded and agreed for their anonymous quotes to be used in publication.
Data Collection
We conducted 16 face-to-face in-depth interviews (IDI),30 eleven with pregnant women and five with nurse-midwives using an IDI guide. The IDI guide included topics and questions on ANC information gained from the literature review and the tools were extensively reviewed by the research team before use. During interviews, women shared their perspectives on ANC information they received from nurse-midwives including health promotion messages, how they interacted with providers and feedback on care they received. On the other hand, nurse-midwives reported their perspectives on ANC information they provided to women, interactions they have had with women during antenatal care. Interviews took place within the health centers’ premises, in a quiet room and out of reach of other participants and clients. Interviews were conducted by the first author, a male nurse with a master’s degree and experience in conducting health research, and a research assistant who was a female registered midwife specialist. Both were assistant lecturers in a public University. Interviews were conducted in Kiswahili and were audio recorded using a Sony digital recorder except for one interview with a nurse midwife who did not consent for her interview to be recorded. At the end of each interview, the researchers listened to the recorded conversations and reflected on them and made sure that emerged themes were followed up with subsequent interviews. After 16 interviews, it was considered that the knowledge saturation was reached as per other researchers’ recommendations that 12 interviews are required to achieve saturation.31 Nevertheless, the sample size for qualitative studies depend on the complexity of the research questions, the purpose of the research study, the diversity of the sample, the nature of the analysis and what can be done with available time and resources.32 The interview sessions with women lasted within 40 minutes while that of nurse-midwives took between 30 and 50 minutes.
Analysis
We analyzed data using thematic analysis,33–35 a flexible method of data analysis that allows researchers with various methodological backgrounds to participate. The recorded interviews were transcribed verbatim in Kiswahili by the first author (RH) then a few transcriptions were cross-checked by other members of the research team.36 The analysis was done using the English translated transcripts. However, before coding the English translated transcripts were back translated into Kiswahili to ensure accuracy and completeness of translations against the original notes. A few observed discrepancies in translation were corrected accordingly. Transcripts were then read repeatedly to gain the sense of the information about pregnancy care and childbirth that was provided by the nurse-midwives and that reported by the women to have received during their visits to antenatal clinics. A list of potential and initial codes was generated, discussed and agreed on by the research team. Throughout the analysis process, the relevant texts were compared, checked, and rechecked for similarities and differences between the codes to form categories that reflected the manifest content of the text. The naming of categories was reflected and revised accordingly.
Results
The social and demographic characteristics of the pregnant women are presented in Table 1.
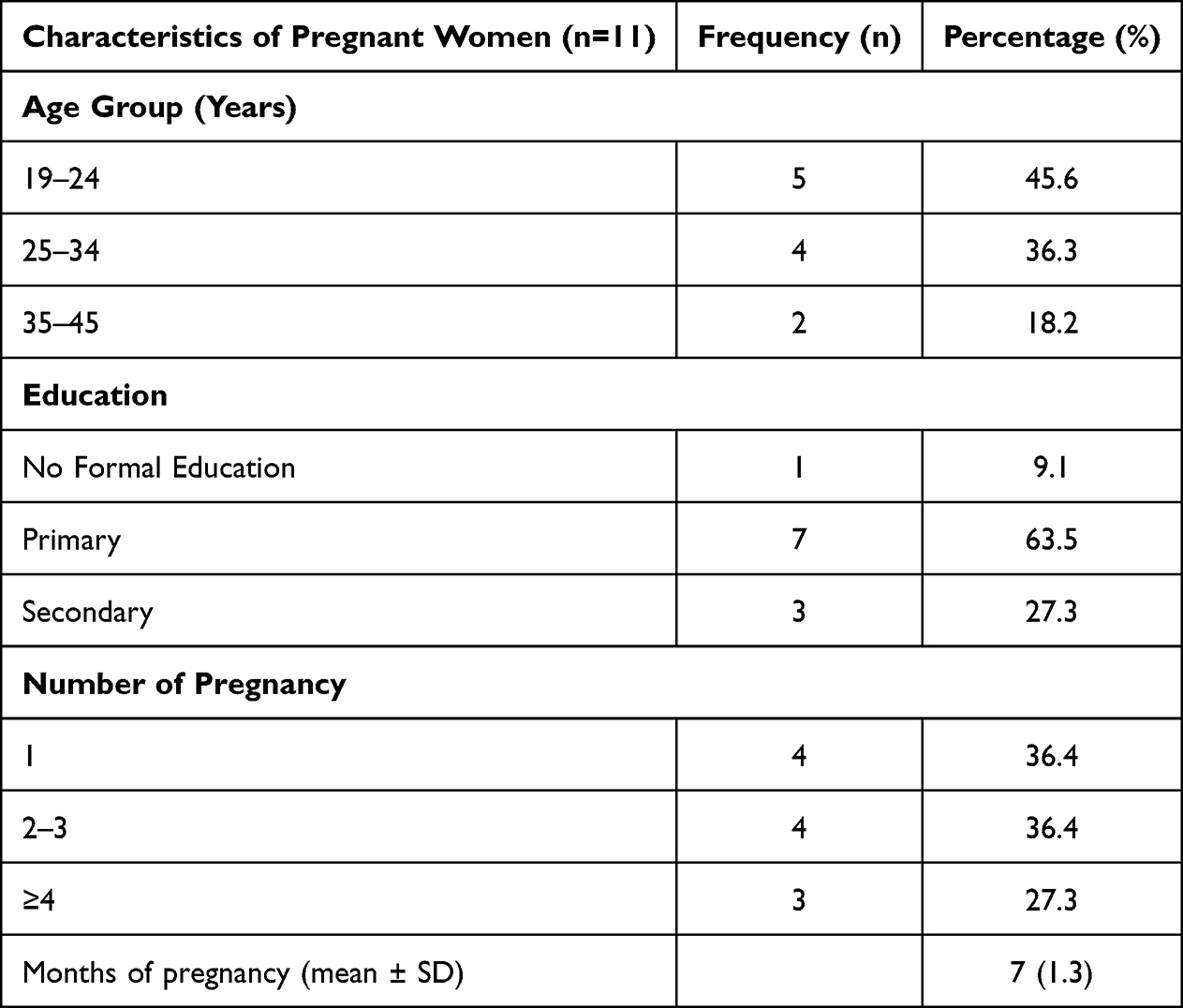 |
Table 1 Characteristics of Pregnant Women |
Nurse-midwives were between the age of 30–59 with a median of 53 years. Two-third of nurse-midwives were enrolled and the rest were registered with diploma in nursing. Nurse midwives had worked at ANC between 2 and 28 years.
Two major themes emerged from the data: Enhancing communication and respectful delivery of ANC Information and Receiving information about pregnancy care and safe childbirth. See Table 2. The findings are illustrated by the participants’ quotations abbreviated as “PW” for pregnant woman followed participant’s age and parity. Nurse-midwives’ quotations are abbreviated as “NM” followed by the professional registration category, “RNM” for registered nurse midwife and “ENM” for the enrolled nurse-midwife. Also, it is followed by age and working experience.
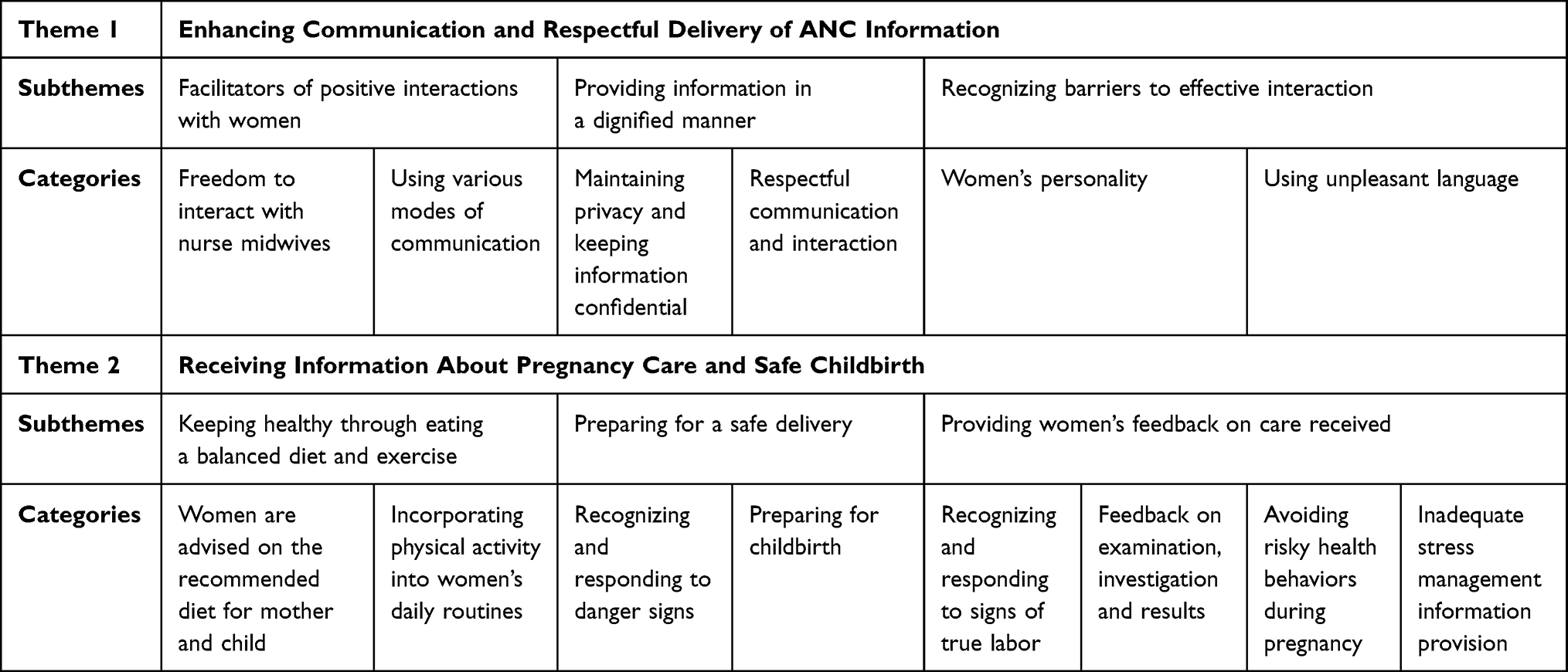 |
Table 2 Theme, Subthemes and Categories from the Perceptions of Women and Nurse-Midwives on Antenatal Care Information and Communication |
Enhancing Communication and Respectful Delivery of ANC Information
This theme has three subthemes and six categories. The themes describe perspectives of women and nurse midwives’ interaction and exchange of information during ANC contact. Also, it describes how respect and dignity were observed and maintained during interactions, as well as the need for an environment free of abuse.
Facilitators of Positive Interactions with Women
Freedom to Interact with Nurse Midwives
Women freedom to communicate is key for the providers to understand their needs and concerns and support them appropriately, women reported that during ANC care, they were free to ask questions, talk and interact with nurse midwives and other care providers at any time.
I am so free here, let me tell no lie; I am free to ask anything, talk, and get good service. (PW: Age 30, Multipara: Para 2)
Other women thought that nurse-midwives were too busy for a productive interaction, and some were not easily approachable.
Nurses are very busy, when you come; you give them your card, they say, “wait, we will call you”, and you are called, examined, and released to go home (PW: Age 30, Multi: Para 8)
Using Various Modes of Communication
Although face-to-face was the primary mode of communication between women and care providers, other modes of communication were also used to facilitate women’s interactions with nurse midwives during care. Some women used telephone to communicate with the nurse-midwives or visited nurses’ homes when need arise.
…I have seen this nurse taking care of me very nicely. I decided to request her telephone number; so that if I have something to ask, I can ask. In truth, she gave me the number. That is the nurse now I am close with, and in case of any problem, I will be able to ask her (PW: Age 43, Multipara: Para 3)
Nurse-midwives gave women their telephone numbers so that they are able to effectively and continuously provide answers to women’s questions and support them promptly.
I just give them (clients) my phone number. For those who do not have a phone, I tell them, even if you find me on the street, just stop me. If you have a problem, tell me. (RNM, Age 50 with 28 years of experience)
Providing Information in a Dignified Manner
Maintaining Privacy and Keeping Information Confidential
Nurse-midwives ensured that information is provided to women respectfully and with dignity to build trustworthiness which is important in health care. Midwives reported that they never shared women’s information with non-concerned people.
(…) the information they provide is kept confidential, the information women provide to us remains with us and women will not hear them on the street or elsewhere (…). (NM: RNM, Age 32 with 7 years of experience)
Respectful Communication and Interaction
Nurse midwives believed that their interaction and communication with women was done in a respectful manner. Although they were unsure whether what they were doing was perceived by women as respect.
(…), It is difficult to know if you are respecting women or not. It is the pregnant women as they perceive the nurse-midwife. It depends on how the pregnant woman perceives you. (NM: ENM, Age 55 with 28 years of experience)
Women reported elements that show respectful treatment and dignified care. These included being humble, responding to questions, welcoming, being patient when talking to them and not yelling at them.
(…) she (nurse midwife) is not disregarding women, not discriminating, when you ask questions she responds well, sits down, and listens to you, giving you good advice and clarifying issues until you understand. (PW: Age 27, Multi: Para 2)
Recognizing Barriers to Effective Interaction
Women’s Personality
Although nurse midwives reported having good interactions with women, they believed that women’s personalities could be a facilitator and a barrier to effective communication and interaction when receiving care.
Some women are free, but it depends on one’s personality. Some women are free, and if they have something to say, they come directly to you, but some are fearful, thinking, what answer will I get if I ask? It is how a person thinks, if she is ready to talk, I am open to talk. (ENM, Age 55 with 28 years of experience)
Using Unpleasant Language
Women in this study also acknowledged receiving verbal abuse from the nurse midwives that interfered effective communication and care provision. Other women, however, perceived verbal abuse as the outcome of circumstances nurse-midwives are going through, which may have led to using unpleasant language:
Some nurses are harsh. If you try to ask a question, they harass you verbally. I am not free to ask questions because some midwives may reply badly. I am afraid to ask questions. (PW: Age 19, Nullipara)
You know, the days are not the same, you may find one day she may be harsh to patients, but another day, she is relaxed with a sense of humility. Every person is not perfect, you see. I can wake up in the morning and become very harsh with my children until they ask themselves what is happening to their mum. But on another day, I am very humble to my children, so this is how we live with our nurses. (PW: Age30, Multi: Para 8)
Receiving Information About Pregnancy Care and Safe Childbirth
Women were given ANC information to help them care for their pregnancies, prepare for labor and delivery and care for their children. They received information about nutrition, physical activity, examination results, danger signs during pregnancy and labour, risky health behaviors, stress management and preparation for delivery.
Keeping Healthy Through Eating a Balanced Diet and Exercise
Women are Advised on the Recommended Diet for Mother and Child
Women reported that information about the importance of eating a balanced diet was commonly emphasized in the first ANC contacts. Women were encouraged to eat plenty of vegetables and fruits, less fat and salt and drink plenty of water.
They (Nurse-midwives) informed us that we need to eat a balanced diet. We were informed during the first visit, … They recommend stiff porridge, vegetables, fish, meat, and things like that; eat plenty of vegetables because they help to increase blood and enough fruits, yes like that. (PW: Age 30, Multi: Para 2)
Nurse midwives encouraged women to eat more frequently during pregnancy, eating foods that are available in their areas and using nutrition supplements:
We tell them to eat mixed foods especially vegetables to increase the blood levels. Also, we give them FEFO (Iron and Folic acid) supplements. (NM: RNM, Age 32 with 7 years of experience)
Although most women acknowledged receiving information about nutrition during pregnancy, other women reported that they did not receive information about food and nutrition during ANC contacts.
Ever since I started this clinic, I have never been told anything about what I should eat or not eat. (PW: Age19, Nullipara)
Both pregnant women and nurse midwives reported that child nutrition education and care was mostly provided during postnatal care. The ANC guidelines direct nutrition education to be provided in late antenatal contacts. This may be due to the increased number of women in ANC compared to number of ANC staff. It was, however, reported that information about child nutrition and the importance of exclusive breast-feeding was always provided to women who were HIV positive.
We talk less about child nutrition. Much emphasis is placed on HIV positive women; we inform them that after the child is born, they will be given drugs and then the mother should continue to breastfeed without giving the child anything else to prevent HIV infection; but for women with normal pregnancy, we don’t talk much about child nutrition, we don’t take it seriously. (NM: RNM, Age 32 with 7 years of experience)
After delivery, the mother is instructed to exclusively breastfeed the child for six months, after that time the baby could be given soft foods like porridge. (PW: Age 30, Multi: Para 2)
Incorporating Physical Activity into Daily Routines
Physical exercises during pregnancy help women to remain active and therefore nurse midwives informed women to continue with their domestic chores as part of exercises and do other simple physical exercises:
A pregnant woman is supposed to do her routine chores if she does not have any problems. Do her simple activities like cooking, washing dishes, and household chores that do not use a lot of energy. We tell her it is part of the exercise (NM: RNM, Age 32 with 7 years of experience)
Some women, however, acknowledged not receiving information about the importance of doing exercise during pregnancy. And others relied on their friends and parents who had experience of giving birth.
I was not given information about exercise, and I don’t have experience, my mother instructs me; I do exercise like walking, fetching water (…). (PW: Age 20, Nullipara)
Preparing for a Safe Delivery
Recognizing and Responding to Danger Signs
Women recalled being informed about danger signs and what to do if they experienced each one of them. They were told to go to the nearby health facility if they had a foul-smelling vaginal discharge, vaginal bleeding, severe headache, dizziness, swollen legs or abdominal pain.
They informed me that danger signs include bad smell vaginal discharge, severe headaches, and a baby who is not playing and when I experience them, I should go to the hospital. (PW: Age 24, Multi: Para 1)
Women’s partners were also involved during the talk.
So, we try to talk to both (woman and her partner) so that they both understand the danger signs that may happen and what to do. (NM: RNM, Age 30 with 2.5 years of experience)
Preparing for Childbirth
Women reported being informed about delivery preparation including identifying someone to take care for the woman’s family in her absence; identifying at least two blood donors; preparing funds for transport and identifying a decision-making family member to accompany a woman during labor. The element that was mostly recalled by women was the preparation of essential items needed for a clean birth.
When we came for the first time, we were informed of the need to prepare delivery supplies like, ten pairs of khanga, a bucket of water, and other things that need to be on standby at home. (PW: Age27, Multi: Para 2)
However, other women were not told to prepare transport.
I was not told to prepare the transport, I just used common sense. (PW: (Age24, Multi: Para1)
Recognizing and Responding to Signs of True Labor
Understanding the signs of true labor is one of the key information to ensure that women get to the health facility timely and increase the chances of women giving birth in the health facilities. However, women received this information from their mothers and friends. The women explained how they understood the signs of labor.
I was told when I feel severe groin pain, slippery vaginal discharge, and when the tummy/belly goes down slowly, that is the sign of labor. (PW: Age 24, Multi: Para1)
The nurse-midwives thought that for the women who were pregnant for the first time it was a must to inform them about signs of labor and show them how to give birth.
We tell them about signs of labor, especially women with their first pregnancy; we also tell them how they will notice signs of labor and tell her how she will give birth (…). NM: RNM, Age 32 with 7 years of experience
Providing Women’s Feedback About Care Received
Feedback on Examination and Investigation Results
Nurse-midwives claimed to inform women about the test results. They informed the women if their blood level was good or bad or if the baby’s heartbeat was good or bad. Sometimes reagents or kits for routine tests were lacking; therefore, women were advised to do the tests in a private laboratory. If the blood-increasing supplements were not available, women were advised to obtain them from a private pharmacy.
I had my blood level tested. They told me my blood level is low. They gave me blood-increasing tablets. Today, the midwife told me there are no blood-increasing drugs, I will buy them. Since I have not tested my blood level and therefore I do not know my blood level. (PW: Age30, Multi: Para 8)
So, if the tests reveal no problems, you should give them the information. “We tested you today, but we found no problems. In testing urine for sugar and protein, we found you have no problem”. Sometimes the reagents are not available, but for the first visit of a pregnant woman, you can advise the mother to go does it somewhere else. We ask them to do it in the neighboring laboratories, which are private. (NM: ENM, age 55 with 25 years of experience)
Avoiding Risky Health Behaviors
Avoiding risky behaviors and reducing pregnant women’s involvement in activities that may jeopardize the pregnancy’s progress and fetal development are critical issues that need to be constantly emphasized. This meant testing for and talking about possible risks to pregnancy and how to fix them. It also meant not drinking alcohol, smoking cigarettes, using illegal drugs, taking medications without a doctor’s supervision, or having unsafe sex. Although women recalled not being informed about risk behaviors during pregnancy, they knew that using cigarettes, alcohol, marijuana, and other illicit drugs could harm them and their unborn child. Other women reported receiving advice about risky behaviors from the elderly, friends, and family members.
They may be talking about risk behaviors, but I have never been informed by them (providers); I know it is not good to use alcohol or cigarettes during pregnancy. (PW: Age39, Multi: Para 4)
(…) Some pregnant women believe that beer increases blood, and when we were outside today, we were debating about beer being able to increase blood. (PW: Age 27, Multi: Para 2)
My parents said that if you continue using alcohol and cigarette, your child will also use alcohol and cigarette in the future. (PW: Age 30, Multi: Para 2)
Nurse-midwives acknowledged they rarely talked about risk behaviors during antenatal contact.
We do not talk much about risk behaviors during pregnancy that is not our priority, perhaps we should start now. (NM: RNM, Age 32 with 7 years of experience)
Nurse midwives commonly inform women to avoid sexually transmitted infections to protect their babies from acquiring those diseases. However, they only focus on discussing HIV but not other sexually transmitted infections (STIs).
We tell them (the woman and her partner) it is important to protect themselves from sexually transmitted infections (STIs), to use condoms, and if they are diagnosed with STIs, they should be treated. We also tell them about the effects of having these diseases. A baby can be born with these diseases. (NM: RNM, age 32, with 7 years of experience)
Other women never heard about other STIs except HIV.
They do not talk about other diseases acquired through sexual intercourse, when you are tested for HIV, you are only told your blood is safe just be careful. (PW: Age 24, Multi: Para 1)
The use of medicine was also discussed, as it may cause adverse effects if used without medical advice. Women recalled being informed not to use medicine without medical advice. Nonetheless, a few were told that they could use nonprescription drugs such as Panadol and blood increasing medications, but they needed to seek medical advice for drugs that required a prescription. They did not recall talking about the use of alternative medicine, which is a common thing in our setting, where different herbs can be used during pregnancy.
… we were told not to take any drug without a doctor’s instructions, you can use blood-increasing drugs and others, but you are not allowed to take any drug without a doctor’s advice. (PW: Age 30, Multi: Para 2)
Inadequate Stress Management Information Provision
One of the problems that need to be monitored during pregnancy is stress, which may lead to depression if not well managed. Stress during pregnancy is a risk factor for both the mother and child’s adverse outcomes. Anxiety in pregnancy is associated with shorter gestation and has an adverse effect on fetal neurodevelopment and child outcomes.34,37 According to ANC guidelines, pregnant women need to be informed about how to identify signs of stress and depression and how to cope with them. Women were not informed about coping with stress and its management. Other women, however, received this information from nurse-midwives as well as from their relatives or prayed for God’s mercy.
… We were not told about stress management that stress affects someone if they have problems and do not have someone to share them with, and you leave it to God. You may decide to go and tell someone and end up getting bad advice. (PW: (Age 43, Multi: Para3)
Midwives acknowledged talking about stress and depression rarely
I am not sure if we have ever talked about pregnancy-related stress and depression. (NM: RNM, Age 30 with 2.5 years of experience)
Discussion
We conducted this study to describe women and nurse midwives’ perceptions of interactions and antenatal care information provision in Tanzania’s Coastal Region. We found that women perceived their communication and interaction with midwives to be free throughout, and nurse midwives thought that women were free to ask questions. Both midwives and women reported personality differences as both facilitators and barriers to effective communication, as some women feared interacting with midwives and some midwives were difficult to approach. Nurse-midwives believed that communicating with women respectfully and with dignity was important in building trustworthiness. All women were given information about antenatal care, but not all women recalled receiving all the information as per national and international guidelines. Inadequate numbers of staff and inadequate time for the provision of information to the substantial number of pregnant women attending the ANC clinic were perceived to contribute to poor antenatal care information delivery. Friends and relatives were indicated to complement the lack of ANC information. However, some of the information concerning antenatal care given by them was misleading.
Effective communication and interactions between nurse-midwives and pregnant women is the key to delivering adequate and useful health information. It ensures positive relationships, fosters a sense of reassurance, comfort, and warmth. The resultant positive relationship reduces negative emotions and may promote health practices among pregnant women.15
Most pregnant women believed that interaction with nurse-midwives was good, and they were free to communicate. However, some women thought that some nurse midwives were difficult to interact with due to their busy schedule. Some midwives also thought that some women were shy and did not like to interact with them. Despite this contradictory view, it is possible that some women were afraid of verbal abuse, for instance, if they asked tough questions. They always interacted face to face, and midwives were willing to share their phone number with women, but there was a sense that women were afraid to ask for the midwife’s number. This may be due to the client’s and health worker culture of not being too close to each other and focusing more on formal contacts during scheduled ANC visits. Or it may be due to women’s fear of getting a harsh or negative response when requesting the telephone number from midwives. A study in the Netherlands also found that women were allowed to call midwives if they had questions, but some hesitated to call, thinking that their questions were minor.38 Due to the increased number of women attending ANC clinics, telephone and other electronic communication systems may be used to lessen the burden of women and nurse midwives of having to meet face-to-face for consultation even when women do not have a major problem. This may be facilitated by telling the women about midwives’ availability for telephone and other digital platform interaction and encouraging them to ask any questions, even minor ones.38
Respecting women and taking care of them with dignity is an important aspect in ensuring good interactions with women. Respect and dignity are universal human needs. Pregnant women want a friendly and trustful relationship with their midwife and also midwives who can make them feel at ease, who are friendly, respectful, supportive of their choices, treat them well and seriously, give them sufficient time, clarify information for them, and act professionally.38 Women who took part in this study thought that nurse midwives should be humble, friendly, and patient, and not scold women. A study done in Iran also raised the issue of respect, compassion, sympathy, being friendly, paying attention, and intimacy as important in ANC care.39 Women also reported issues of harsh language and nagging. The problem of hash language and mistreatment of women is even higher during labor and delivery.40 The issues of respect and provision of care with dignity and ensuring confidentiality are the cornerstones of enabling women to continue using the health care service and be satisfied with care. They need a lot of emphasis.
Women and midwives also shared their views on various topics covered during ANC contacts, including nutrition education, pregnancy development and monitoring, danger signs and risk behaviors, and preparation for delivery. Nutrition education provides accurate and evidence-based nutrition knowledge to promote healthy eating for pregnant women. Women need this information to make wise food choices that will supply all the required nutrients and provide sufficient energy for the healthy development of their pregnancy.41 Nutrition education increases the likelihood of women eating a balanced diet, exercising, and being healthy.42 It also helps women set proper eating and exercising habits in pregnancy. The WHO guidelines emphasize educating and counseling pregnant women about healthy eating and keeping physically active during pregnancy.43
Women acknowledged receiving nutrition information in general terms that made it difficult for them to make informed nutrition plans according to their needs. Important topics were not covered in detail, but women were just told to eat a balanced diet and increase their intake of fruit and vegetables. Also, only a few nurse midwives acknowledged giving individualized nutrition education only to women with anemia and other nutrition problems. Other studies have also shown that women’s looking healthy was the reason for their receiving less health and nutrition information.38,44 In this study also, the issues of child nutrition were affected by that mindset, as for women with normal pregnancy, less information was given about child nutrition compared to those women who were HIV positive. Other studies also reported that, important specific topics were not covered in detail like vegetables and fruits eating,45,46 leading to inadequate consumption of fruits and vegetables.47,48 A result of a systematic literature review showed that nurse midwives supplied little nutritional information to women internationally.49
Exercise is vital for the well-being of pregnant women, and it is associated with improved mood and physical fitness.50 It also aids in the maintenance of a healthy weight during and after pregnancy, as well as the improvement of mood during and after delivery.50 Despite those benefits, the importance of physical activity was perceived as not being sufficiently emphasized during pregnancy, despite its high benefits. This may have been due to the fact that most women were peasants and active in their activities of daily living and this may have led to midwives giving less emphasis in this area. Another reason may be a lack of enough time to cover the topic.
Enabling pregnant women to recognize danger signs and seek medical help early is one of the important strategies to reduce maternal morbidity and mortality. Women who acknowledged being informed of danger signs were able to mention some of them. Despite many women recalling being informed by midwives of different types of danger signs, previous studies conducted in Tanzania focusing on women’s knowledge of danger signs22 and the quality of counseling services on danger signs,23 reported limited knowledge of danger signs by women and that many women were not informed about any danger signs during antenatal care visits. Also, studies done elsewhere reported women’s low knowledge of danger signs.51,52 Currently, in our setting, danger signs are one of the areas where much emphasis is placed to ensure that women and their partners are aware of danger signs so that they can seek medical health as early as possible in order to reduce maternal morbidity and mortality.
Getting information about nutrition, pregnancy and danger signs are not enough to ensure safe delivery unless the women prepare well for delivery. Poor preparation for delivery may lead to complications and even death due to delays in reaching or getting appropriate skilled care.53 Preparation for delivery involves the pregnant women being given information about birth preparedness and complication readiness. In this strategy women are expected to know their expected delivery date and the importance of delivering in a health facility; Identify a place of birth, someone to care for the woman’s family in her absence, at least two blood donors, a decision-making family member to accompany a woman during labor; Prepare essential items needed for a clean birth, funds for transportation. This information helps women to make the appropriate decision for care seeking and increases the chance of women using health facilities. Most women indicated missing key information on preparation for delivery like identifying a place of birth, someone to care for the woman’s family in her absence; at least two blood donors, a decision-making family member to accompany a woman during labor and preparing funds for transportation. Studies done in Iceland found that birth information was insufficient based on women’s perspective,21 and in Rwanda, women were less prepared for delivery.54
Identification of true signs of labor is the key to making immediate decisions to seek medical services. Many pregnant women were not informed about signs of labor, and they used experience and advice from their mothers and friends. These findings are similar to a study done in Brazil which found that two-thirds of pregnant women were not informed about signs of labor.55 This may affect the early detection of signs of labor and the decision of when to seek care. When this is coupled with transport infrastructure problems and poor preparation due to lack of information, it may cause a delay in seeking the service or in reaching the health facility.
Women who receive feedback on the results of their assessment and examination and those who are aware of pregnancy risk behaviors and danger signs are better able to identify potential problems that may affect the development of the pregnancy and the health of the infant and seek care promptly. Nurse-midwives and pregnant women agreed that explanation of tests and examination procedure and results was done to very few women. HIV test was the only test that was mostly explained to most women. The reason for this may be the presence of many tests and examination results that need to be explained so nurse-midwives have to prioritize which one to talk about. The findings are similar to previous studies done in Tanzania where the reason for clinical examination and physical checkups was not explained to women17 and Uganda where there was a lack of explanation of important clinical and laboratory procedures and linking the tests with preventive information.18
Risk behaviors during pregnancy include cigarette smoking, alcohol use, marijuana use, illicit drug use, and unprotected sex that led to STIs. These affect the development of pregnancy and have an adverse effect on the child’s wellbeing.56 Very few women were told about risk behaviors, their effects, and how to avoid them. This may be caused by nurse midwives assuming that most pregnant women from the coast region do not drink alcohol or smoke cigarettes and it may also be lack of time to cover all the topics. Other issues which were raised very rarely were psychological issues like coping with stress. Despite many pregnant women in developing countries needing more information on psychological issues like coping with stress1,57 very few women in this study were informed about stress management, and nurse midwives did not talk about stress and depression during pregnancy unless if the woman has sign of stress. Relative and friend were reported to play an important part in stress management care. There is a consensus that despite the pregnancy being the normal physiological condition, it is a stressful life event for women.58 Stress during pregnancy is a risk factor for mother and child adverse outcomes. Stress and anxiety in pregnancy are associated with shorter gestation and have an adverse effect on fetal neurodevelopment and child outcomes.37 The issues of stress management during pregnancy need to be given much emphasis during pregnancy to improve the health of the mother and the fetus.
Strengths and Limitations
The qualitative nature of our research gathered both rich and useful information in the study context. Triangulation of sources of information (midwives and women) yields providers and customers opinion of the ANC information. Although the findings of this study were not meant to be generalized, they are relevant to other context that have similar social economic status as that of Tanzania. Further, a quantitative research study that will include larger and more diverse samples, as well more settings or contexts could be conducted to enhance the generalizability of the findings.
Conclusion
Despite pregnant women’s several ANC contacts, not all women recalled receiving all the information as per national and international guidelines. Nurse-midwives’ efforts to provide health information effectively according to national ANC guidelines may have been hindered by inadequate staffing and incentives and the high number of women attending antenatal clinics. The government and other health care providers need to increase the number of midwives, improve their working conditions and incentives. Also, develop policies that encourage the use of technology, like mobile apps, to help healthcare providers and women communicate easily and as a means of communicating health information to clients.
Abbreviations
ANC, Antenatal Care; FANC, Focused Antenatal Care; TDHS, Tanzania Demographic and Health Survey; MoHCDEC, Ministry of Health, Community Development, Gender, Elderly and Children; MMR, Maternal Mortality Ratio; HIV, Human Immunodeficiency Virus; PMTCT, Prevention of Mother to Child Transmission of HIV; WHO, World Health Organization; TNMC, Tanganyika Nursing and Midwifery Council.
Data Sharing Statement
Datasets used and/or analysed during the current study are available from the first author on request.
Ethics Approval and Consent to Participate
Ethical clearance was obtained from the Muhimbili University of Health and Allied Sciences Institutional Review Board. Permissions to collect data were obtained from the Pwani Regional Administrative Secretary, Regional Medical Officers, the Kibaha and Bagamoyo District Executive Directors, and the District Medical Officers, and the facility In-charges.
Acknowledgments
Funding for the study came from Swedish International Development Cooperation Agency (Sida) through bilateral cooperation with the Muhimbili University of Health and Allied Sciences (MUHAS) and Uppsala University (UU). We thank the many individuals who made this study successful, especially the pregnant women and health care providers who participated in our study. We are grateful to Pwani Regional Administrative Secretary, Regional Medical Officers, the Kibaha and Bagamoyo District Executive Directors, and the District Medical Officers, and the facility In-charges for permitting us to conduct the study in their setting.
Disclosure
The authors declare that they have no competing interests.
References
1. Al-Ateeq MA, Al-Rusaiess AA. Health education during antenatal care: the need for more. Int J Women’s Health. 2015;7:239–242. doi:10.2147/IJWH.S75164
2. Lavin T, Pattinson RC. Does antenatal care timing influence stillbirth risk in the third trimester? A secondary analysis of perinatal death audit data in South Africa. BJOG. 2018;125(2):140–147. doi:10.1111/1471-0528.14645
3. Maloni JA, Cheng CY, Liebl CP, Maier JS. Transforming prenatal care: reflections on the past and present with implications for the future. J Obstetr Gynecol Neonatal Nurs. 1996;25(1):17–23. doi:10.1111/j.1552-6909.1996.tb02508.x
4. MoHCDGEC M, NBS, OCGS, and ICF. Tanzania Demographic and Health Survey and Malaria Indicator Survey 2015–2016; 2016. Available from: http://dhsprogram.com/pubs/pdf/FR321/FR321.pdf.
5. National Bureau of Statisctics- Tanzania. 2012 population and housing census; 2012.
6. Kearns A, Hurst T, Caglia J, et al. Focused antenatal care in Tanzania: delivering individualised, targeted, high quality care. Woman Health Initiat. 2014;2014:1–14.
7. Keja K, Chan C, Hayden G, Henderson RH. Expanded programme on immunization. World Health Stat Q. 1988;41(2):59–63.
8. Ministry of Health. The national road map strategic plan to accelerate reduction of maternal, newborn and child deaths in Tanzania 2008–2015; 2008.
9. Robinson D. The integrated management of childhood illness. Afr Health. 1996;18(6):20–21.
10. World Health Organization. WHO Antenatal Care Randomized Trial Manual for the Implementation of the New Model. World Health Organization; 2001.
11. Villar J, Ba’aqeel H, Piaggio G, et al. WHO antenatal care randomised trial for the evaluation of a new model of routine antenatal care. Lancet. 2001;357(9268):1551–1564. doi:10.1016/s0140-6736(00)04722-x
12. MoHCDEC. Antenatal Care Guidelines. Dar es salaam: Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDEC) (Tanzania); 2018.
13. World Health Organization. WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience. Luxebourg: WHO Press; 2016.
14. Lattof SR, Tuncalp O, Moran AC, et al. Developing measures for WHO recommendations on antenatal care for a positive pregnancy experience: a conceptual framework and scoping review. BMJ Open. 2019;9(4):e024130. doi:10.1136/bmjopen-2018-024130
15. Tuncalp Ӧ, Were WM, MacLennan C, et al. Quality of care for pregnant women and newborns-The WHO vision. BJOG. 2015;122(8):1045–1049. doi:10.1111/1471-0528.13451
16. Nicoloro-SantaBarbara J, Rosenthal L, Auerbach MV, Kocis C, Busso C, Lobel M. Patient-provider communication, maternal anxiety, and self-care in pregnancy. Soc Sci Med. 2017;190:133–140. doi:10.1016/j.socscimed.2017.08.011
17. Sarker M, Schmid G, Larsson E, et al. Quality of antenatal care in rural southern Tanzania: a reality check. BMC Res Notes. 2010;3:209. doi:10.1186/1756-0500-3-209
18. Conrad P, De Allegri M, Moses A, et al. Antenatal care services in rural Uganda: missed opportunities for good-quality care. Qual Health Res. 2012;22(5):619–629. doi:10.1177/1049732311431897
19. Dougherty L, Stammer E, Valente TW. Interpersonal communication regarding pregnancy-related services: friends versus health professionals as conduits for information. BMC Pregnancy Childbirth. 2018;18(1):97. doi:10.1186/s12884-018-1729-x
20. Attanasio L, Kozhimannil KB. Patient-reported communication quality and perceived discrimination in maternity care. Med Care. 2015;53(10):863–871. doi:10.1097/MLR.0000000000000411
21. Gottfredsdottir H, Steingrimsdottir T, Bjornsdottir A, Guethmundsdottir EY, Kristjansdottir H. Content of antenatal care: does it prepare women for birth? Midwifery. 2016;39:71–77. doi:10.1016/j.midw.2016.05.002
22. Mwilike B, Nalwadda G, Kagawa M, Malima K, Mselle L, Horiuchi S. Knowledge of danger signs during pregnancy and subsequent healthcare seeking actions among women in Urban Tanzania: a cross-sectional study. BMC Pregnancy Childbirth. 2018;18(1):4. doi:10.1186/s12884-017-1628-6
23. Pembe AB, Carlstedt A, Urassa DP, Lindmark G, Nyström L, Darj E. Quality of antenatal care in rural Tanzania: counselling on pregnancy danger signs. BMC Pregnancy Childbirth. 2010;10(1):35. doi:10.1186/1471-2393-10-35
24. Anya SE, Hydara A, Jaiteh LE. Antenatal care in The Gambia: missed opportunity for information, education and communication. BMC Pregnancy Childbirth. 2008;8:9. doi:10.1186/1471-2393-8-9
25. Colorafi KJ, Evans B. Qualitative descriptive methods in health science research. Herd. 2016;9(4):16–25. doi:10.1177/1937586715614171
26. MoHCDEC. Provider’s Guide Antenatal Care in Tanzania Mainland. Dar es salaam: Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDEC) (Tanzania); 2018.
27. Kwesigabo G, Mwangu MA, Kakoko DC, et al. Tanzania’s health system and workforce crisis. J Public Health Policy. 2012;33(Suppl 1):S35–S44. doi:10.1057/jphp.2012.55
28. Campbell S, Greenwood M, Prior S, et al. Purposive sampling: complex or simple? Research case examples. J Res Nurs. 2020;25(8):652–661. doi:10.1177/1744987120927206
29. Ministry of Health. The Nursing and Midwifery (Registration, Enrollment and Licencing) Regulations, 2010. Council TNaM, editor. Dar es salaam: Tanzania Goverment Printer; 2010:53.
30. Moridi M, Pazandeh F, Hajian S, Potrata B, Gurgel RQ. Midwives’ perspectives of respectful maternity care during childbirth: a qualitative study. PLoS One. 2020;15(3):e0229941. doi:10.1371/journal.pone.0229941
31. Guest G, Bunce A, Johnson L. How many interviews are enough? An experiment with data saturation and variability. Field Methods. 2016;18(1):59–82. doi:10.1177/1525822x05279903
32. Francis JJ, Johnston M, Robertson C, et al. What is an adequate sample size? Operationalising data saturation for theory-based interview studies. Psychol Health. 2010;25(10):1229–1245. doi:10.1080/08870440903194015
33. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
34. Braun V, Clarke V. Thematic Analysis. Cooper H, Camic PM, Long DL, Panter AT, Rindskopf D, Sher KJ, editors. American Psychological Association; 2012:57–71.
35. Braun V, Clarke V. Reflecting on reflexive thematic analysis. Qualitat Res Sport Exerc Health. 2019;11(4):589–597. doi:10.1080/2159676X.2019.1628806
36. Thurmond VA. The point of triangulation. J Nurs Scholarship. 2001;33(3):253–258. doi:10.1111/j.1547-5069.2001.00253.x
37. Dunkel Schetter C, Tanner L. Anxiety, depression and stress in pregnancy: implications for mothers, children, research, and practice. Curr Opin Psychiatry. 2012;25(2):141–148. doi:10.1097/YCO.0b013e3283503680
38. Baron R, Heesterbeek Q, Mannien J, Hutton EK, Brug J, Westerman MJ. Exploring health education with midwives, as perceived by pregnant women in primary care: a qualitative study in the Netherlands. Midwifery. 2017;46:37–44. doi:10.1016/j.midw.2017.01.012
39. Gheibizadeh M, Abedi HA, Mohammadi E, Abedi P. Iranian women and care providers’ perceptions of equitable prenatal care: a qualitative study. Nurs Ethics. 2016;23(4):465–477. doi:10.1177/0969733015573653
40. Mselle LT, Kohi TW, Dol J. Humanizing birth in Tanzania: a qualitative study on the (mis) treatment of women during childbirth from the perspective of mothers and fathers. BMC Pregnancy Childbirth. 2019;19(1):231. doi:10.1186/s12884-019-2385-5
41. Koehn ML. Childbirth education outcomes: an integrative review of the literature. J Perinat Educ. 2002;11(3):10–19. doi:10.1624/105812402X88795
42. Serçekuş P, Mete S. Turkish women’s perceptions of antenatal education. Int Nurs Rev. 2010;57(3):395–401. doi:10.1111/j.1466-7657.2009.00799.x
43. World Health Organization. WHO Recommendations on Maternal Health Guidelines. Geneva: World Health Organization; 2017.
44. Edvardsson K, Ivarsson A, Eurenius E, et al. Giving offspring a healthy start: parents’ experiences of health promotion and lifestyle change during pregnancy and early parenthood. BMC Public Health. 2011;11(1):936. doi:10.1186/1471-2458-11-936
45. Garnweidner LM, Sverre Pettersen K, Mosdol A. Experiences with nutrition-related information during antenatal care of pregnant women of different ethnic backgrounds residing in the area of Oslo, Norway. Midwifery. 2013;29(12):e130–e137. doi:10.1016/j.midw.2012.12.006
46. Szwajcer EM, Hiddink GJ, Koelen MA, van Woerkum CM. Written nutrition communication in midwifery practice: what purpose does it serve? Midwifery. 2009;25(5):509–517. doi:10.1016/j.midw.2007.10.005
47. Wen LM, Flood VM, Simpson JM, Rissel C, Baur LA. Dietary behaviours during pregnancy: findings from first-time mothers in southwest Sydney, Australia. Int J Behav Nutr Phys Act. 2010;7(1):13. doi:10.1186/1479-5868-7-13
48. Wilkinson SA, Miller YD, Watson B. Prevalence of health behaviours in pregnancy at service entry in a Queensland health service district. Aust N Z J Public Health. 2009;33(3):228–233. doi:10.1111/j.1753-6405.2009.00380.x
49. Lucas C, Charlton KE, Yeatman H. Nutrition advice during pregnancy: do women receive it and can health professionals provide it? Matern Child Health J. 2014;18(10):2465–2478. doi:10.1007/s10995-014-1485-0
50. The American College of Obstetricians and Gynecologists (ACOG). Physical Activity and Exercise During Pregnancy and the Postpartum Period. The American College of Obstetricians and Gynecologists; 2020.
51. Trotman G, Chhatre G, Darolia R, Tefera E, Damle L, Gomez-Lobo V. The effect of centering pregnancy versus traditional prenatal care models on improved adolescent health behaviors in the perinatal period. J Pediatr Adolesc Gynecol. 2015;28(5):395–401. doi:10.1016/j.jpag.2014.12.003
52. Teng SP, Zuo TC, Jummaat FB, Keng SL. Knowledge of pregnancy danger signs and associated factors among Malaysian mothers. Br J Midwifery. 2015;23(11):800–806. doi:10.12968/bjom.2015.23.11.800
53. World Health Organization. WHO Recommendations on Health Promotion Interventions for Maternal and Newborn Health 2015. Geneva: World Health Organization; 2015.
54. Smeele P, Kalisa R, van Elteren M, van Roosmalen J, van den Akker T. Birth preparedness and complication readiness among pregnant women admitted in a rural hospital in Rwanda. BMC Pregnancy Childbirth. 2018;18(1):190. doi:10.1186/s12884-018-1818-x
55. Félix HCR, Corrêa CC, Matias T, Parreira BDM, Paschoini MC, Ruiz MT. The Signs of alert and Labor: knowledge among pregnant women. Revista Brasileira de Saúde Materno Infantil. 2019;19(2):335–341. doi:10.1590/1806-93042019000200005
56. Chung EK, Nurmohamed L, Mathew L, Elo IT, Coyne JC, Culhane JF. Risky health behaviors among mothers-to-be: the impact of adverse childhood experiences. Acad Pediatr. 2010;10(4):245–251. doi:10.1016/j.acap.2010.04.003
57. Nigenda G, Langer A, Kuchaisit C, et al. Women's opinions on antenatal care in developing countries: results of a study in Cuba, Thailand, Saudi Arabia and Argentina. BMC Public Health. 2003;3(1):17. doi:10.1186/1471-2458-3-17
58. Hodgkinson EL, Smith DM, Wittkowski A. Women’s experiences of their pregnancy and postpartum body image: a systematic review and meta-synthesis. BMC Pregnancy Childbirth. 2014;14(1):330. doi:10.1186/1471-2393-14-330
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.