Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Pyoderma Gangrenosum with Pseudoepitheliomatous Hyperplasia Histopathologically Misdiagnosed as Squamous Cell Carcinoma: A Case Report and Brief Literature Review
Authors Pan J, Qian J, Li X, Wang Y, Huo N
Received 23 April 2026
Accepted for publication 28 May 2026
Published 3 June 2026 Volume 2026:19 619529
DOI https://doi.org/10.2147/CCID.S619529
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Monica K. Li
Jinru Pan,1– 6,* Jiandan Qian,1,* Xiangyan Li,1 Yan Wang,1 Na Huo1
1Department of Infectious Diseases, Peking University First Hospital, Beijing, People’s Republic of China; 2Renal Division, Department of Medicine, Peking University First Hospital, Beijing, People’s Republic of China; 3Institute of Nephrology, Peking University, Beijing, People’s Republic of China; 4Key Laboratory of Renal Disease, Ministry of Health, Beijing, People’s Republic of China; 5Key Laboratory of Chronic Kidney Disease Prevention and Treatment (Peking University), Ministry of Education, Beijing, People’s Republic of China; 6Beijing Key Laboratory of Precision Medicine and New-Drug/Equipment Development for Severe Kidney Disease, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yan Wang, Department of Infectious Diseases, Peking University First Hospital, Beijing, People’s Republic of China, Email [email protected] Na Huo, Department of Infectious Diseases, Peking University First Hospital, Beijing, People’s Republic of China, Email [email protected]
Abstract: Pseudoepitheliomatous hyperplasia (PEH), a rare histopathological manifestation of pyoderma gangrenosum (PG), closely resembles squamous cell carcinoma (SCC) and leads to misdiagnosis, yet relevant reported cases remain limited. We report a 71-year-old female who developed abdominal pain and persistent fever after tooth extraction. Subsequent erythema, ulcerative necrotic lesions occurred on her left dorsal hand following frequent intravenous infusion, and lesions paradoxically expanded after surgical debridement. Initial biopsy and pathological consultation suggested SCC with positive surgical margins. However, the rapid progression of the lesion was inconsistent with SCC. Finally, a repeat biopsy confirmed diffuse neutrophilic infiltration with benign PEH, confirming the diagnosis of PG. The patient received systemic immunosuppressive therapy with oral prednisolone and sulfasalazine, systemic symptoms resolved and cutaneous lesions healed completely without recurrence during follow-up. This case highlights that while PEH is a known variant of PG, its potential to mimic malignancy remains a significant diagnostic pitfall that is often underrecognized in clinical practice. Comprehensive evaluation of distinctive clinical manifestations and a repeat biopsy when necessary are crucial for confirming PG, so as to prevent diagnostic delay and unnecessary surgical interventions.
Keywords: neutrophilic dermatosis, pyoderma gangrenosum, squamous cell carcinoma, pseudoepitheliomatous hyperplasia
Introduction
Pyoderma gangrenosum (PG) is a rare autoinflammatory neutrophilic dermatosis that typically occurs on the legs and is most common among middle-aged females.1 It typically presents as a single or multiple papules or nodules that progress to painful ulcers with violaceous borders and surrounding erythema.1 Importantly, unlike postsurgical PG, for which several recurrent clinical clues and characteristic patterns have progressively been recognized,2 the diagnosis of classic PG remains particularly challenging due to the lack of specific clinical, laboratory, and histopathological features. Although validated scoring frameworks such as the PARACELSUS score and Delphi criteria have been developed to address this diagnostic uncertainty, their modest concordance and variable diagnostic yield leave substantial room for subjective interpretation and diagnostic delay. The exact etiology remains unclear, but more than half of the PG patients are associated with systemic conditions, including inflammatory bowel disease (IBD), autoimmune disorders, and certain hematologic diseases.3 Furthermore, it may arise spontaneously or be triggered by pathergy after minor or surgical trauma.1,2,4
Notably, the histopathological landscape of PG can be confounded by pseudoepitheliomatous hyperplasia (PEH), a benign but exuberant epidermal proliferation that can mimic well-differentiated squamous cell carcinoma (SCC), leading to the misdiagnosis of malignancy and subsequent mismanagement.5 Here, we report a case of PG on the left dorsal hand presenting PEH histopathologically, initially misdiagnosed as SCC.
Case Report
A 71-year-old woman, previously in good health, presented with fever and abdominal pain after tooth extraction. After a local professional dentist ruled out dental-care-related complications, screening for detailed etiologies was further initiated. Initial laboratory tests revealed mild anemia, elevated inflammatory markers, and an increased erythrocyte sedimentation rate. Contrast-enhanced abdominal computed tomography (CT) showed edema and thickening of the small intestinal wall in the mid-lower abdomen, with adjacent mesenteric thickening and haziness, prompting consideration of small intestinal infection or inflammatory bowel disease. Subsequent gastrointestinal endoscopy identified benign colonic polyps and non-atrophic gastritis, but no definitive source of infection. Besides, there were no abnormalities detected in autoimmune antibody test and tumor markers. After combined antibiotic therapy with intravenous levofloxacin (0.5g/d) and piperacillin-tazobactam (4.5 g, every 8 hours), her abdominal pain improved, and a repeat abdominal CT demonstrated no significant abnormalities in the small or large intestine. However, her fever persisted, and she was transferred to our department for further evaluation and treatment.
Following nearly 20 days of repeated intravenous infusion with same antibiotic regimen at our and local hospital, erythema and papules appeared at the injection site on her left dorsal hand, accompanied by significant edema, surface ulceration, necrosis and purulent exudate. The surrounding skin exhibited subcutaneous hemorrhage, with edges showing creeping expansion (Figure 1A). Microbiological studies, including bacterial cultures, mycobacterial polymerase chain reaction, and broad-spectrum pathogen detection via targeted Next-Generation Sequencing of the purulent fluid were all negative. Moreover, after daily debridement and dressing changes, the lesion progressively enlarged, eventually involving the distal forearm (Figure 1B). Therefore, we performed the first biopsy at the ulcer edge. Both of the initial histopathological examination and secondary pathology consultation suggested well-differentiated squamous cell carcinoma (SCC) with positive margins (Figure 2A). To further evaluate for SCC, Positron Emission Tomography-CT (PET-CT) was performed, revealing diffuse fluorodeoxyglucose-avid soft tissue swelling in the left hand with a maximum standardized uptake value of 18.4, without bone erosion or metastatic lesions. Given the undermined edge of the ulcer, extensive local lesions without regional lymphadenopathy, and rapid progression inconsistent with SCC, a multidisciplinary discussion including Burn and Plastic Surgery Department and Dermatology Department raised the suspicion of PG, and surgery is contraindicated for this condition. Consequently, antibiotic therapy was discontinued, and empiric immunosuppressive therapy was initiated with oral prednisolone at an initial dose of 35 mg/d (0.5 mg/kg/d), which was subsequently tapered by 5 mg per week to a maintenance dose of 5 mg/d for a total treatment duration of 3 months, combined with sulfasalazine. The patient’s temperature gradually normalized, followed by gradual resolution of edema.
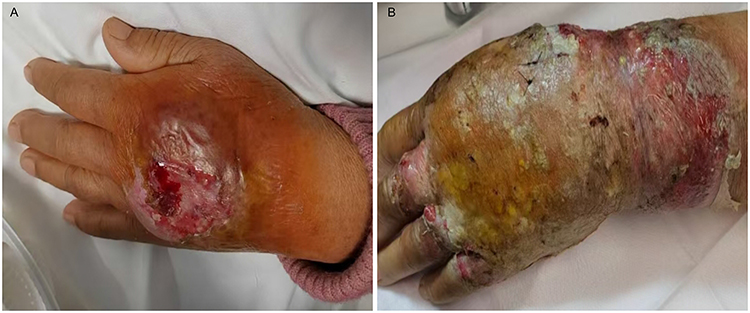 |
Figure 1 The lesion of the left hand. (A) The initial lesion of the left dorsal hand. (B) The lesion progressively extended to the left forearm. |
 |
Figure 2 Histopathological features of the left dorsal hand skin biopsy. (A) First biopsy: epidermal hyperplasia, dermal acute and chronic inflammatory cell infiltration with granuloma formation, focal epithelial-like cell nests, mild cellular atypia, considered as well-differentiated squamous cell carcinoma (H&E, ×200). (B) Second biopsy: epidermal pseudoepitheliomatous hyperplasia, diffuse neutrophil infiltration throughout the dermis, with scattered plasma cells and numerous histiocytes, no significant granulomatous changes observed, consistent with neutrophilic dermatosis (H&E, ×200). |
To further clarify the diagnosis, a repeat biopsy of the edge of newly developed lesions demonstrated epidermal PEH, with diffuse neutrophilic infiltration throughout the dermis, consisting with neutrophilic dermatosis (Figure 2B). Ultimately, the diagnosis of PG was confirmed. The patient was transferred to dermatology department for continued the prescribed prednisolone and sulfasalazine therapy, supplemented with ozonated hydrotherapy and wound care. The lesions healed completely approximately one month after treatment leaving raised scars (Figure 3), and no recurrences were observed during the 6-month follow-up period.
 |
Figure 3 Lesion healed after 1-month treatment leaving raised scars. |
Discussion
PG is a rare, non-infectious autoinflammatory neutrophilic dermatosis.1 Owing to the absence of definitive clinical and histopathological features, its diagnosis is frequently delayed. We report a complex diagnostic journey involving a case of PG on the left dorsal hand, which was initially misdiagnosed as SCC due to the histopathological presence of PEH.
At onset, the patient presented with fever, abdominal pain, and intestinal wall thickening. PG is often associated with underlying systemic conditions, most notably IBD.3 Although initial endoscopy failed to confirm a typical IBD diagnosis, abdominal CT revealed small bowel edema. Furthermore, following corticosteroid therapy, the patient’s systemic fever subsided concurrently with lesion’s improvement. This parallel response suggests a systemic inflammatory process sensitive to immunosuppression, though a shared pathophysiological mechanism between the cutaneous and gastrointestinal manifestations cannot be definitively established.
The occurrence of PEH in the histopathology of PG is rarely reported. PEH is a benign, reactive irregular proliferation of the epidermis and adnexal epithelium that closely mimics the invasive epithelial cords of SCC.5 A brief review of previously published similar cases indicates that these patients are generally elderly, with lesions occurring at various anatomical sites, with or without comorbid systemic diseases (Table 1).6–10 In this case, the rapid, undermining expansion of the skin ulcer and extensive local lesions without regional lymphadenopathy was inconsistent with the clinical course of SCC. The diagnosis of PG was ultimately confirmed by the rapid improvement of lesions following empirical immunosuppressive therapy and the characteristic diffuse neutrophilic infiltration observed in a repeat biopsy. This underscores the critical importance of a clinicopathologic-therapeutic correlation.
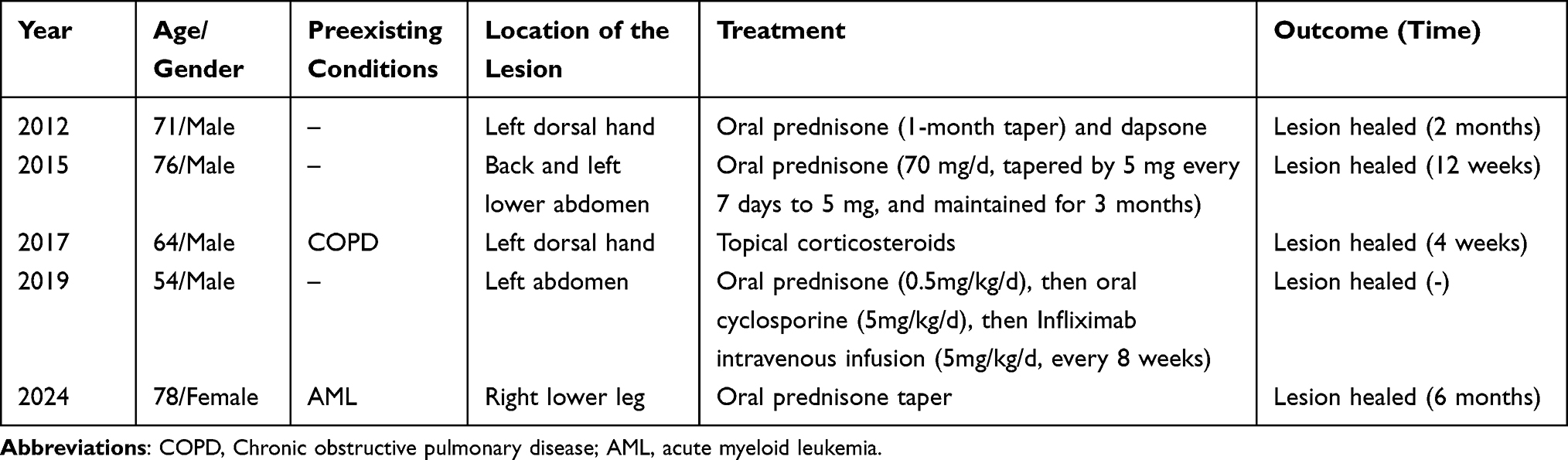 |
Table 1 Literature Review of Reported Pyoderma Gangrenosum with Pseudoepitheliomatous Hyperplasia Histopathologically Mimicking Squamous Cell Carcinoma |
In this patient, the lesion emerged at the site of repeated punctures, which is a classic manifestation of pathergy, a suspicious feature of PG.4 Furthermore, although PET-CT showed significantly increased metabolic activity in the lesions, the absence of bone erosion or metastasis led us to attribute the high tracer uptake to the massive infiltration of activated neutrophils characteristic of PG, rather than malignant proliferation. However, PET-CT is primarily used to screen for underlying malignancies and benign musculoskeletal lesions,11 while the metabolic features of PG lesions remain unreported in current literature. This case firstly describes this phenomenon, which may provide new imaging evidence to improve its diagnostic system.
Regarding treatment, systemic corticosteroids remain the first-line therapy, while topical corticosteroids may be effective for localized or mild PG.12,13 Literature reviews show that most cases achieve complete healing with a corticosteroid-centered regimen (Table 1).6–10 To mitigate the adverse effects of long-term prednisolone use and the risk of relapse upon tapering, we initiated early combination therapy with sulfasalazine. This dual immunosuppressive approach led to rapid wound healing and a favorable prognosis.
Conclusion
This rare case serves as a valuable addition to the literature, aiming to raise clinical awareness and reduce the misdiagnosis of PG. When PG presents histopathologically with PEH, it is highly susceptible to being misdiagnosed as SCC, a diagnostic pitfall that remains insufficiently recognized. Importantly, while histopathology serves as an ancillary tool, its findings can be nonspecific and, as seen in this case, even highly misleading. Consequently, clinicians must integrate clinical features and perform a repeat biopsy when necessary to ensure a timely and accurate diagnosis. Furthermore, PET-CT may serve as a potential reference for the diagnosis of PG in the future. Early initiation of corticosteroid-based immunosuppressive therapy and the avoidance of unnecessary invasive surgical procedures are paramount to improving patients’ outcomes.
Ethics Approval and Consent to Participate
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. Institutional approval for the publication of anonymized case details was granted by Peking University First Hospital. This study was performed in accordance with the Declaration of Helsinki.
Acknowledgments
We would like to express our sincere gratitude to Ping Tu, Yang Wang and Panpan Shang from the Department of Dermatology and Venereology and Li Liang from the Department of Pathology at Peking University First Hospital for their expert guidance and invaluable insights in pathological diagnosis throughout this case.
Funding
This work is supported by the Fundamental Research Funds for the Central Universities (Peking University Medicine Sailing Program for Young Scholars’ Scientific & Technological Innovation BMU2025YFJHP010).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Ruocco E, Sangiuliano S, Gravina AG, Miranda A, Nicoletti G. Pyoderma gangrenosum: an updated review. J Eur Acad Dermatol Venereol. 2009;23(9):1008–6. doi:10.1111/j.1468-3083.2009.03199.x
2. Caddia G, Voulliaume D, Dettori L, Rubino C, Delay E. Postsurgical Pyoderma Gangrenosum in Breast Surgery: An Updated Systematic Review, Takeaways, and the 6 Commandments. Aesthet Surg J. 2025;45(9):NP142–NP53. doi:10.1093/asj/sjaf095
3. Hadi A, Lebwohl M. Clinical features of pyoderma gangrenosum and current diagnostic trends. J Am Acad Dermatol. 2011;64(5):950–954. doi:10.1016/j.jaad.2010.01.049
4. Anthony Honigman JSK, John WF. Pathergy: a review of potential mechanisms and novel therapeutic targets. Wound Pract Res. 2022;30(1). doi:10.33235/wpr.30.1.55-61
5. Zayour M, Lazova R. Pseudoepitheliomatous hyperplasia: a review. Am J Dermatopathol. 2011;33(2):112–22;quiz23–6. doi:10.1097/DAD.0b013e3181fcfb47
6. Wolfe CM, Green WH, Cognetta AB Jr, Baniahmad O, Hatfield HK. Atypical pyoderma gangrenosum of the dorsal hand mimicking squamous cell carcinoma. J Hand Surg Am. 2012;37(9):1835–1838. doi:10.1016/j.jhsa.2012.06.019
7. Radović T Č, Kostović K, Radoš J, Paštar Z, Pavliša G, Marinović B. Advanced pyoderma gangrenosum previously treated as squamous cell carcinoma. Acta Dermatovenerol Croat. 2015;23(3):208–212.
8. Rostom M, Davidson DM, Biswas AJDH. Pyoderma gangrenosum and pseudoepitheliomatous hyperplasia: a poorly recognized association. Diagn Histopathol. 2017;23(5):229–233.
9. González-Sabín M, Rodríguez-Díaz E, Gonzalvo-Rodríguez P, Astola-Hidalgo I. Pyoderma gangrenosum mimicking a squamous cell carcinoma. Actas Dermosifiliogr. 2019;110(5):400–402. doi:10.1016/j.ad.2018.02.022
10. Hoang M, Maymone MBC, Telang GH, Seo SJ, Robinson-Bostom L. Vegetative pyoderma gangrenosum mimicking squamous cell carcinoma: a poorly recognized diagnostic challenge. Am J Dermatopathol. 2024;47(4):e47–e49. doi:10.1097/dad.0000000000002919
11. Asadoorian M, Matcuk GR Jr, Patel DB, Tomasian A, Wassef HR, White EA. Musculoskeletal pitfalls on fluorodeoxyglucose F 18 PET-computed tomography: pictorial review. PET Clin. 2018;13(4):587–607. doi:10.1016/j.cpet.2018.06.001
12. Moltrasio C, Romagnuolo M, Tavoletti G, Maronese CA, Marzano AV. Pyoderma gangrenosum: pathogenetic mechanisms and their implications for treatment. Semin Immunopathol. 2025;47(1):38. doi:10.1007/s00281-025-01064-7
13. Donnelly H, Boffa MJ. Topical treatment of pyoderma gangrenosum: a systematic review. Indian J Dermatol Venereol Leprol. 2025;91(2):188–195. doi:10.25259/ijdvl_700_2023
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Progressive Facial Ulcer: A Case Report of Pyoderma gangrenosum
Zhang XQ, Tang ZW, Jing J
Journal of Inflammation Research 2024, 17:687-691
Published Date: 3 February 2024