Back to Journals » Infection and Drug Resistance » Volume 16
Pulmonary Tuberculosis and Rifampicin Resistant Mycobacterium Tuberculosis in Children and Adolescents using Gene Xpert MTB/RIF Assay in Tigray, Northern Ethiopia
Authors Dejene TA ![]() , Hailu GG, Kahsay AG
, Hailu GG, Kahsay AG ![]() , Wasihun AG
, Wasihun AG
Received 3 August 2023
Accepted for publication 12 October 2023
Published 19 October 2023 Volume 2023:16 Pages 6757—6765
DOI https://doi.org/10.2147/IDR.S433789
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Tsehaye Asmelash Dejene,1,2 Genet Gebrehiwet Hailu,1 Atsebaha Gebrekidan Kahsay,1 Araya Gebreyesus Wasihun1
1Department of Medical Microbiology and Immunology, School of Medicine, College of Health Sciences, Mekelle University, Mekelle, Ethiopia; 2Department of Medical Microbiology, School of Medicine, Aksum University, Axum, Ethiopia
Correspondence: Atsebaha Gebrekidan Kahsay, Department of Medical Microbiology and Immunology, School of Medicine, College of Health Sciences, Mekelle University, P. O. Box: 1871, Mekelle, Tigrai, Ethiopia, Email [email protected]
Background: Tuberculosis (TB) continues to be a global health problem. While childhood TB contributes 10% to the global TB burden, the paucibacillary nature of TB disease in children and the absence of reliable diagnostic methods have made MTB diagnosis in children to be a great challenge. This study aimed to determine the prevalence of MTB and rifampicin-resistant MTB (RR-MTB) among children using Gene Xpert MTB/RIF Assay in Tigray, Ethiopia.
Methods: A retrospective database study was conducted among children in ten governmental hospitals in the Tigray region. Gene Xpert MTB/RIF results of sputum/gastric lavage samples from children with presumptive TB from January 2016 to December 2019 were extracted using a data extraction sheet. Data were collected and analyzed using Statistical Package for the Social Sciences version 21.
Results: The prevalence of bacteriologically confirmed MTB by Gene-Xpert in children with presumptive TB was 7.3% (95% CI: 6.7%− 7.9%) and the proportion of those that were Gene-Xpert MTB positive who also have rifampicin resistance was 10.9% (95% CI: 8.2– 13.6%). Older children aged 11– 15 years [AOR = 1.76; 95% CI = 1.33– 2.33, p < 0.001] and adolescents 16– 17 years [AOR = 2.18; 95% CI = 1.63– 2.92, p < 0.001] were more likely to be MTB positive. Relapse cases [AOR = 1.66; 95% CI = 1.09– 2.51, p = 0.017] and lost/failure cases [AOR = 8.82; 95% CI = 3.94– 19.76, p < 0.001] were more likely to have MTB compared to the new cases.
Conclusion: The proportion of MTB-positive among the TB presumptive patients was 7.3%. The proportion of rifampicin-resistant TB to all positive patients was 10.9%. Female participants had more MTB than males (or younger children). The result highlights the need for due attention in children because it is very helpful in determining the future control of the disease.
Keywords: children and adolescent, presumptive TB, rifampicin resistant, Xpert MTB/RIF, Tigray, Ethiopia
Introduction
Tuberculosis (TB) is one of the leading causes of death worldwide.1 An estimated 10.6 million people fell ill with tuberculosis (TB) worldwide with 1.2 million children as reported in the 2023 World Health Organization fact sheet.2 Given the challenge in diagnosing childhood TB and perception, the burden of TB in children was higher than the estimate,3 indicating that childhood tuberculosis is a public health issue.4 Diagnosis of PTB in children is challenging because of nonspecific clinical or radiologic signs and the paucibacillary nature of the disease.5 To alleviate this diagnostic problem, the WHO recommended Xpert MTB/RIF assay in 2010, a molecular method which is more sensitive and specific.6
Ethiopia is among the TB high-burden countries with a rank of 10th among the high-TB-pandemic and 15th among the 27 high MDR-TB countries. The prevalence and incidence of TB in Ethiopia by 2014 were 211 and 214 per 100,000 population, respectively.7 In 2016, there was an estimated 393.8/100,000 death of TB.8 A systematic review of the epidemiology of MDR-TB in Ethiopia showed that 2.18% of newly diagnosed and 21.07% of previously treated patients had MDR-TB.9 There are limited data on childhood TB and MDR-TB in the nation; however, the estimated contribution of children to the national TB burden reported in 2011 was 16.1%.10
Ethiopia has implemented Xpert since 2015 for the diagnosis of childhood TB. However, there are limited data on TB and RR-TB in children in Ethiopia. A study by Arega et al in Addis Ababa using Gene Xpert assay11 reported a prevalence of 13.6% TB and 7.9% RR-TB in children. Another study from the Oromia region has reported a 31.7% prevalence of TB and 0% for RR-TB using the culture method.12 Except for these couple of studies, data on childhood TB and RR-TB are scant.
It is, therefore, reasonable to conduct a study and provide data on childhood TB and RR-TB to help the regional governments and other stakeholders to help them understand the prevalence, and transmission, and evaluate the effectiveness of TB control programs or forecast future trends of the disease.
Methods
Study Design and Study Population
Tigray Regional State is one of the nine national regional states of Ethiopia. It is the northernmost of Ethiopia located at 12o15’ 4o57’ longitude and 36o27’-39o59’ latitude. According to the 2007 census, Tigray has a population size of 6,960,003 within an area of 54, 572.6 km2. The health facilities in Tigray are one teaching and comprehensive specialized hospital, 14 general hospitals, 20 primary hospitals, 204 health centers, 712 health posts (village clinic), and above 500 private health facilities.
A retrospective database study was conducted among children in ten governmental hospitals in the Tigray region. These include Adwa, St. Mary, Suhul, Kahsay Abera, Adigrat, Wukro, Mekelle, Lemelem Karl, Alamata hospitals and Ayder comprehensive specialized teaching hospital. We purposefully selected the 10 hospitals which started Gene Xpert for the diagnosis of TB in 2016. Directly observed treatment, and short-course (DOTS) TB treatment services are provided in all the health facilities. There are three MDR-TB treatment initiation centers and 52 treatment follow-up centers in the region.
The source population included all children with presumptive TB who had a Gene Xpert MTB/RIF result in the laboratory TB registry book of all included health facilities from January 2016 to December 2019. Our study participants were all children presumptive TB (<18 years) with a complete registry of age, gender, Gene Xpert MTB/RIF results, HIV status, and TB treatment history.
Inclusion Criteria and Variables
We include all presumptive TB children patients (above <18 years) with complete records of age, sex, Xpert-MTB/RIF results, HIV status, and TB treatment history.
Exclusion Criteria
Children with any missing information on age, gender, Xpert MTB/RIF results, invalid, intermediate Xpert MTB/RIF results, HIV status, and TB treatment history were excluded from the study.
Data Collection
Patients’ data such as age, sex, Xpert MTB/RIF results, HIV status, and TB treatment history were collected from registration books using a data extraction sheet.
Sample Collection and Laboratory Processing
A single sputum sample per patient from children who were able to expectorate sputum and gastric lavage samples from younger children who were unable to provide sputum was collected for the diagnosis of all presumptive TB patients using Xpert MTB/RIF assay (Cepheid, Sunnyvale, CA, USA). Briefly, after sputum/gastric lavage was collected, it was mixed with a sample reagent buffer in a 1:2 (sample: sample reagent buffer) volume ratio. Then, it was closed tightly, vortexed for 15 seconds and allowed to stand at room temperature for 10 minutes. It was again vortexed after 10 min and allowed to stand for 5 minutes, a total of 15 minutes. Using the Pasteur pipette provided with the kit >2mL of the (just above 2mL mark on pipette) processed sample was put into the Xpert MTB/RIF cartridge. Then, the cartridge with the specimen was loaded into the Gene Xpert machine, and results were collected from the Gene Xpert machine after two hours.13
Quality Control and Data Analysis
A probe check was performed on every cartridge before initiation of polymerase chain reaction (PCR). During the probe check, fluorescence readings in the reaction tube for each probe were compared to default settings established by Cepheid Company. If the readings did not match the default settings, the assay was terminated. Data were collected from registry books with data extraction sheets. After data completeness is checked, data were entered and analyzed using SPSS Version 21. Frequency, mean, range, and standard deviation were computed. Chi-square and logistic regression analyses were computed to identify the associated factors with RR-TB and MTB. Significant variables in binary logistic regression were analyzed using multiple logistic regressions to identify variables that showed association with MTB and RR-TB at p-value ≤ 0.05.
Ethical Consideration
The Institutional Review Board (IRB) of Aksum University’s College of Health Sciences granted ethical approval for the study; the IRB’s approval number is 152/2019. According to pertinent national, international, and scientific guidelines, the study was conducted. Due to the retrospective nature of the review, Aksum University’s College of Health Science waived the need for parental agreement from the patients and maintained patient data confidentiality in accordance with the Declaration of Helsinki.
Results
Socio-Demographic, Clinical Characteristics, and MTB Results of the Participants
Of the total 8017 children who provided sputum/gastric lavage specimens for TB diagnosis, 7080 (88.3%) had complete data and were included in the study. Males were more dominant (3960, 55.9%) than females, and the age of the patients ranged from 7 months to 17 years, with a mean age of 10.29 (±4.92 SD) years. The majority, 6828 (96.4%) of the study participants were treatment-naive, and the HIV status of 5866 (82.9%) children was not documented. The prevalence of Gene-Xpert-confirmed MTB was 514 (7.3%), and the proportion of rifampicin resistant MTB to the total confirmed MTB was 56 (10.9%). However, the proportion of rifampicin resistant MTB to overall presumptive patients was 56 (0.8%) (Table 1).
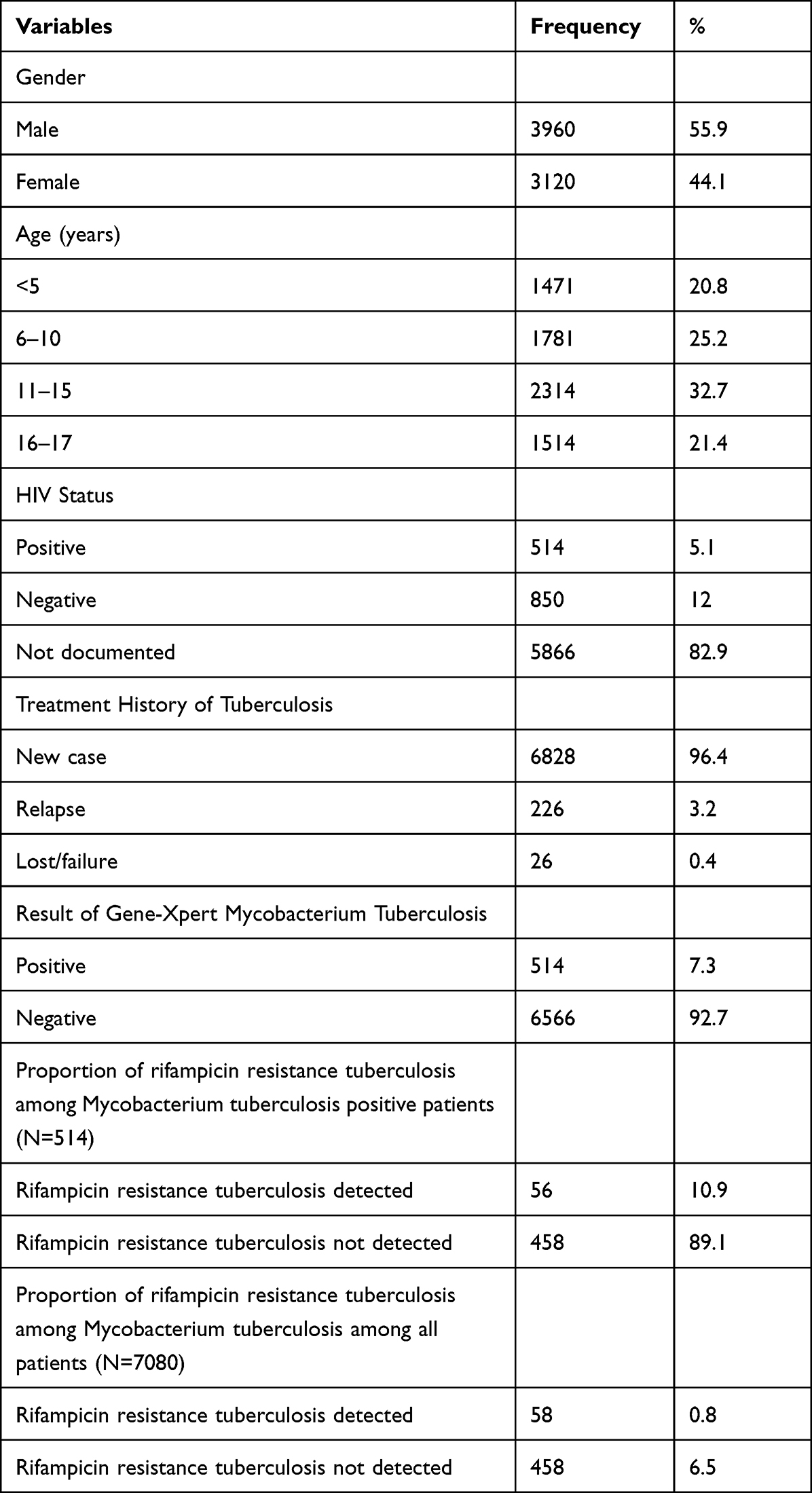 |
Table 1 Socio-Demographic, Clinical Characteristics, and MTB Result Among T Presumptive Children in Tigray, Ethiopia, 2016–2019 (N = 7080) |
Factors Associated with MTB
Female patients were 1.34 times more likely to have TB compared to males [AOR = 1.34; 95% CI = 1.12–1.60, p = 0.002]. Likewise, children aged 11–15 years [AOR = 1.76; 95% CI = 1.33–2.33, <0.001], and 16–17 years [AOR = 2.18; 95% CI = 1.63–2.92, p < 0.001] were more likely to have TB disease compared to those children in the age group of <5 years. Relapse cases [AOR = 1.66; 95% CI = 1.09–2.51, p = 0.017] and lost/failure cases [AOR = 8.82; 95% CI = 3.94–19.76, < 0.001] were more likely to be TB positive compared to the new cases (Table 2).
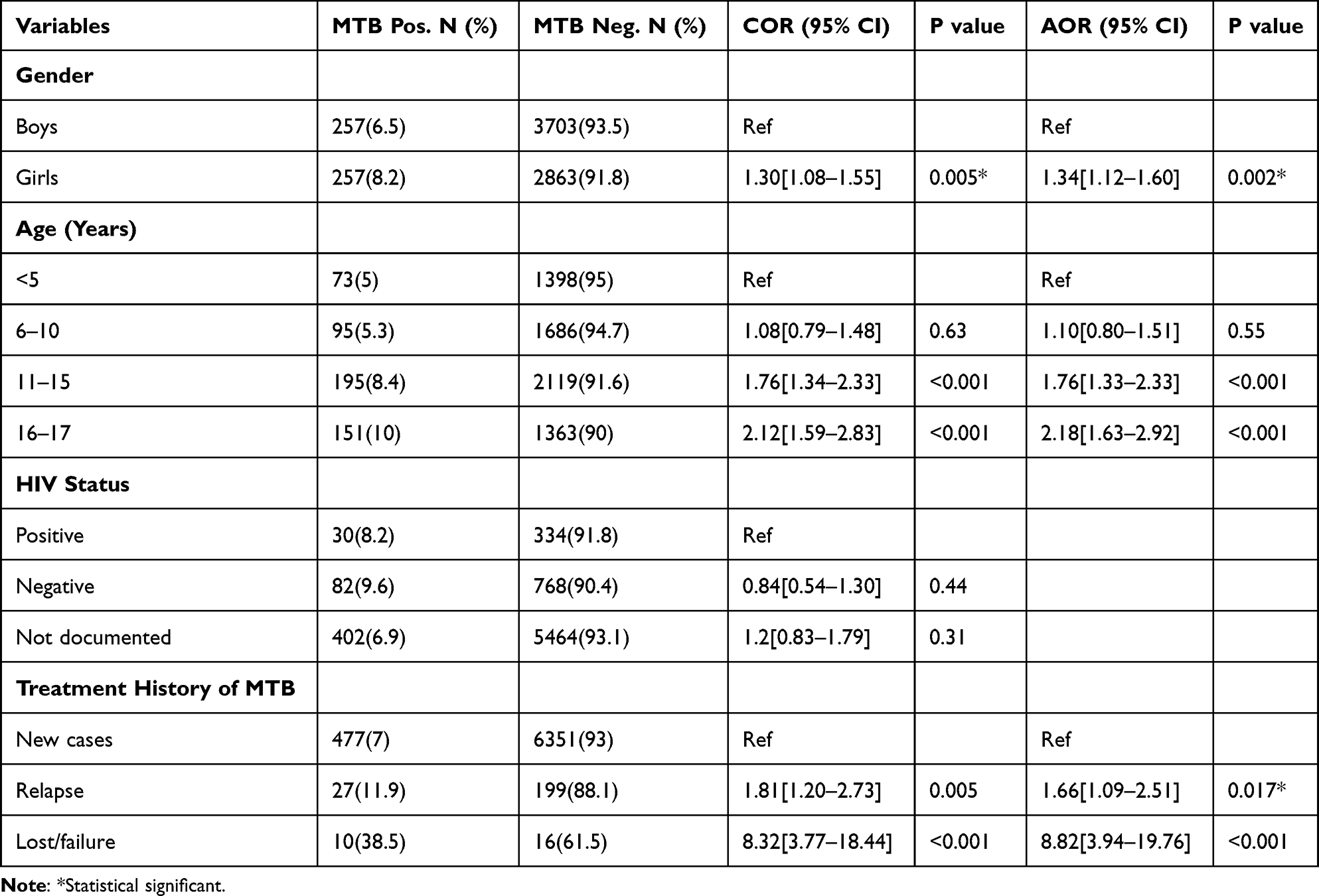 |
Table 2 Factors Associated with MTB Among TB Presumptive Children in Tigray, Ethiopia, 2016–2019 (N = 7080) |
Factors Associated with RR-TB
Out of the total 514 Xpert TB-positive patients, the proportion of RR-TB-positive was 56 (10.9%). Age groups of 6–10 years, 11–15 years, and 16–17 years were, respectively, 2.54, 3.05, and 3.13 times more likely to be RR-TB positive compared to children aged <5 years; this was not, however, statistically significant (p > 0.05). Regarding treatment history and RR-TB, relapse cases were 2.94 times more RR-TB [AOR = 2.94; 95% CI = 1.18–7.36, p = 0.02] positive compared to new cases (Table 3).
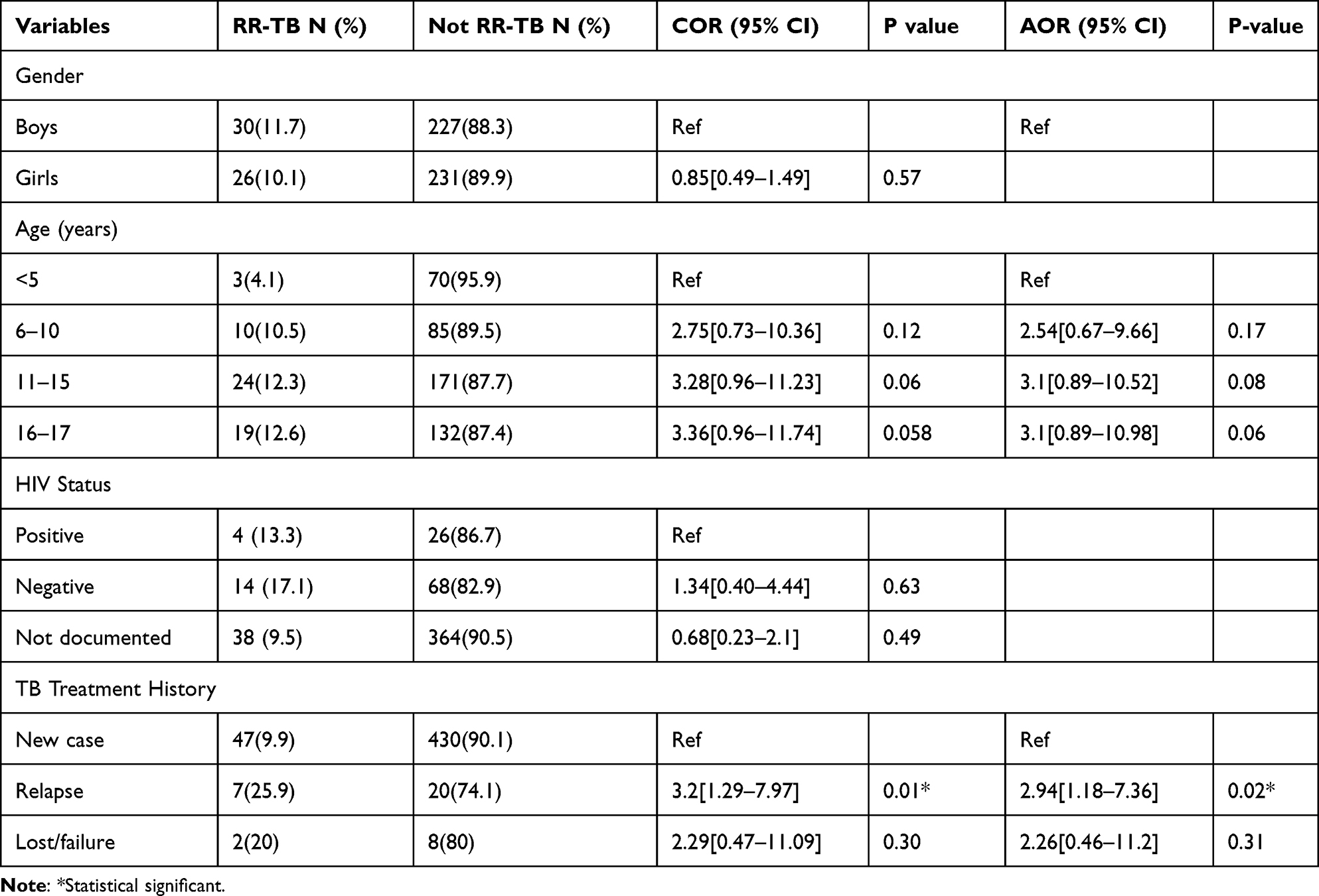 |
Table 3 Factors Associated with RR-TB Among Xpert TB Positive Children in Tigray, Ethiopia, 2016–2019 (N = 56) |
Trends of MTB and RR-TB by Study Years
Figure 1 compares the prevalence of confirmed MTB and the proportion of RR-TB detected among the Xpert TB-positive patients by the study years. Our study revealed that MTB prevalence significantly decreased from 9.6% in the year 2016 to 5.6% in 2018 and then increased to 7.8% in 2019 (p < 0.001). Likewise, the trend of RR-TB has shown a declining trend from 13.4% in 2016 to 7.6% in 2019. This was not, however, statistically significant (p > 0.05).
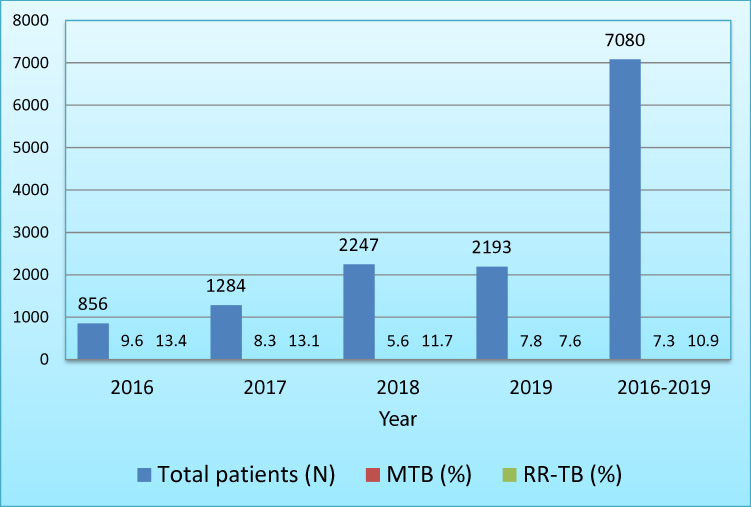 |
Figure 1 Prevalence of MTB and rifampicin-resistant TB among TB presumptive children and adolescent by year in Tigray, Ethiopia, 2016–2019 (N=7080). |
Discussion
Data on childhood tuberculosis are limited owing to the lack of routine case records and the challenge of clinical and bacteriological diagnosis of MTB in children. Thus, epidemiological investigation into childhood MTB is potentially more useful than adult MTB. This is helpful to understand the current transmission and evaluate the effectiveness of MTB control programs or predict future trends in MTB transmission.12 Local data on childhood MTB will help regional, national, and stakeholders to design preventive and control strategies for the disease in these vulnerable groups.
Overall, the prevalence of bacteriologically confirmed MTB was 7.3% and the proportion of those that are Xpert MTB positive who also have RR-TB detected was 10.9%. MTB positive (7.3%) reported by this study was comparable with previous reports from sub-Saharan Africa, 8%,14 Tanzania, 7%,15 and Africa, 7%.16 It is lower than studies conducted in Addis Ababa, Ethiopia, 13.6%,11 Oromia region, Ethiopia,31.7%,12 Sudan, 15.3%,17 South Africa, 19%,18 13%,19 15%,20 Tanzania,17%,21 Uganda, 14%.22
Possible reasons for the variations in the prevalence could be due to differences in methods (culture vs Xpert), sample size, study period, geography, and MTB control and prevention policies. For example, the high MTB prevalence in Ethiopia12,15,16 might be because this study enrolled a small number of children in their study. Besides, the high MTB prevalence in Tanzania21 than our result could be attributed to their study period which was 2011–2014 where Gene Xpert assay was indicated for patients with TB/HIV co-infection and presumptive MDR-TB patients.
Of the total patients aged 7 months to 17 years, the age groups of 11–15 years and 16–17 years were more likely to be MTB positive compared to the younger children (p < 0.05). This is an important finding for public health programmers as this could be due to recent transmission from the children’s caregivers and could hinder future MTB control strategies as infants, and young children are latent reservoirs and potential sources of MTB for the future. Female patients were more likely to be MTB-positive compared to males. This was contrary to the study in the Sudan17 where males were more TB positive.
Positive testing for MTB diseases was significantly high among the new cases compared to previously treated children. This finding was in line with the study in Sudan.17 The high MTB prevalence in the new cases reported by this study could indicate the presence of MTB transmission in the community, calling for coordinated work to prevent and control MTB in the study area.
Given the proportion of RR-TB detected, 10.9% was higher than similar reports from Addis Ababa, Ethiopia, 7.9%,11 Oromia region, Ethiopia, 0%,12 and Uganda, 5.7%.23 We report higher RR-TB positive from relapse cases (p = 0.02) compared to the treatment of naïve patients. While high MDR infection in new cases suggests the important role of ongoing transmission in the occurrence of pediatric MDR-TB, increased infection among relapsed cases implies poor treatment outcomes in the children. This implies that it is a pressing issue for public health in pediatric MTB.24
Our study also assessed the temporal variation in the prevalence of MTB and RR-TB during the years for which retrospective data collected. This study revealed that MTB prevalence significantly decreased from 9.6% in 2016 to 5.6% in 2018. Then, it increased to 7.8% in 2019 (p < 0.001, data not shown). The trend of rifampicin resistance MTB declined from 13.4% in 2016 to 7.6% in 2019 but not statistically significant (Figure 1). Although the decreasing prevalence of childhood MTB in the region is promising, the current problem is still due attention to save children and prevent future MTB-associated morbidities and mortalities.
The strength of this study was its multicenter health facility-based nature and large sample size. This can give updated information on childhood MTB and RR-TB for the regional and national governments and interested stakeholders. However, this study has limitations:
Its result limits the generalizability to the national level as it has conducted in one region, Tigray.
We could not do microbiological confirmation of tuberculosis, phenotypic rifampicin resistance, and resistance to other anti-TB drugs because of the nature of the study.
We did not collect information about contact history of MDR-TB, MTB, education, residence and living conditions of patients. Thus, we could not conduct association between these factors with the outcome variables.
Conclusion
This report shows that 7.3% of the children were bacteriologically confirmed MTB with Xpert; of these, 10.9% were positive for rifampicin resistant-TB. Females (and older children and adolescents, 11–15 and 16–17 years) are more likely to have MTB detected (ie, bacteriological confirmation by Xpert) than males (or younger children). Though childhood MTB showed a decreasing trend over the study period, the prevalence remained a significant problem. The high RR-TB in our report is an indication of recent transmission in the population; suggesting the need for execution of household contact investigations of adults currently under treatment for MDR-TB to prevent the transmission of the disease to the pediatric population. Our results highlight the need for due attention in the study area to save the lives of these populations and control the future burden of the disease and eventually achieve the target “END TB by 2035”.
Abbreviations
HIV, Human immunodeficiency virus; MDR-TB, Multidrug-resistant tuberculosis; RR-TB, Rifampicin resistant tuberculosis; TB, Tuberculosis; WHO, World Health Organization.
Acknowledgments
We would like to thank all the hospital directors and laboratory staff of the study hospitals for their cooperation in giving us access to the records to extract the data.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas, took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Cegielski JP, Dalton T, Yagui M, et al. Extensive drug resistance acquired during treatment of multidrug-resistant tuberculosis. Clin Infect Dis. 2014;59(8):1049–1063. doi:10.1093/cid/ciu572
2. World Health Organization. Tuberculosis report: 2023. Available from: https.//www.who.int/news-room/fact-sheets/detail/tuberculosis.WHO-2023.
3. Tsai K, Chang H, Chien S, et al. Childhood tuberculosis: epidemiology, diagnosis, treatment, and vaccination. Pediatr Neonatol. 2013;54(5):295–302. doi:10.1016/j.pedneo.2013.01.019
4. Dodd PJ, Gardiner E, Coghlan R, Seddon JA. The burden of childhood tuberculosis in 22 high-burden countries: a mathematical modelling study. Lancet Glob Heal. 2012;2(8):e453–e459. doi:10.1016/S2214-109X(14)70245-1
5. Connell TG, Zar HJ, Nicol MP. Advances in the diagnosis of pulmonary tuberculosis in HIV-infected and HIV-uninfected children. J Infect Dis. 2011;204(Suppl 4):S1151–S1158. doi:10.1093/infdis/jir413
6. World Health Organization. Rapid Implementation of the Xpert MTB/RIF Diagnostic Test. Geneva: World Health Organization; 2011.
7. World Health Organization. Ethiopia tuberculosis progress in 2014; 2015.
8. Deribew A, Deribe K, Dejene T, et al. Tuberculosis burden in Ethiopia from 1990 to 2016: evidence from the Global Burden of Diseases 2016 Study. Ethiop J Heal Sci. 2018;28:520–528.
9. Girum T, Muktar E, Lentiro K, et al. Epidemiology of multidrug-resistant tuberculosis (MDR-TB) in Ethiopia: a systematic review and meta-analysis of the prevalence, determinants and treatment outcome. Trop Dis Travel Med Vacc. 2018;4(1):1–12. doi:10.1186/s40794-018-0065-5
10. Seddon JA, Shingadia D. Epidemiology and disease burden of tuberculosis in children: a global perspective. Infect Drug Resist. 2014;7:153–165. doi:10.2147/IDR.S45090
11. Arega B, Menbere F, Getachew Y. Prevalence of rifampicin resistant Mycobacterium tuberculosis among presumptive tuberculosis patients in selected governmental hospitals in Addis. BMC Infect Dis. 2019;19(1):1–5. doi:10.1186/s12879-019-3943-1
12. Workalemahu B, Berg S, Tsegaye W, et al. Genotype diversity of Mycobacterium isolates from children in Jimma, Ethiopia. BMC Res Notes. 2013;6(1):0–6. doi:10.1186/1756-0500-6-352
13. Cepheid. GeneXpertDx System Users’ manual; 2012:2–13.
14. Bates M, O’Grady J, Maeurer M, et al. Assessment of the Xpert MTB/RIF assay for diagnosis of tuberculosis with gastric lavage aspirates in children in sub-Saharan Africa: a prospective descriptive study. Lancet Infect Dis. 2013;13(1):36–44. doi:10.1016/S1473-3099(12)70245-1
15. Reither K, Manyama C, Clowes P, et al. Xpert MTB/RIF assay for diagnosis of pulmonary tuberculosis in children: a prospective, multi-centre evaluation. J Infect. 2015;70(4):392–399. doi:10.1016/j.jinf.2014.10.003
16. Zar H, Workman L, Isaacs W, et al. Rapid diagnosis of pulmonary tuberculosis in African children in a primary care setting by use of Xpert MTB/RIF on respiratory specimens: a prospective study. Lancet Glob Heal. 2013;1(2):e97–e104. doi:10.1016/S2214-109X(13)70036-6
17. Elmadhooun WM. Prevalence of tuberculosis among children in North Sudan: are we only seeing the tip of the iceberg? J Nat Sc Biol Med. 2017;8:114–118. doi:10.4103/0976-9668.198359
18. Nicol MP, Workman L, Isaacs W, et al. Europe PMC Funders Group Accuracy of the Xpert MTB / RIF test for the diagnosis of pulmonary tuberculosis in children admitted to hospital in Cape Town, South Africa: a descriptive study. Lancet Infect Dis. 2014;11(11):819–824. doi:10.1016/S1473-3099(11)70167
19. Heather J, Zar I, Tom G, Connell MN. Diagnosis of pulmonary tuberculosis in children: new advances. Expert Rev Anti Infect Ther. 2010;8(3):277–288. doi:10.1586/eri.10.9
20. Walters E, Gie RP, Hesseling AC, et al. Rapid diagnosis of pediatric intrathoracic tuberculosis from stool samples using the Xpert MTB/RIF Assay: a Pilot Study. Pediatr Infect Dis J. 2012;31(12):1316. doi:10.1097/INF.0b013e318266c21c
21. Rachow A, Clowes P, Saathoff E, et al. Increased and expedited case detection by Xpert MTB / RIF assay in childhood tuberculosis: a prospective cohort study. Clin Infect Dis. 2012;54(10):1388–1396. doi:10.1093/cid/cis190
22. Sekadde MP, Wobudeya E, Joloba ML, et al. Evaluation of the Xpert MTB / RIF test for the diagnosis of childhood pulmonary tuberculosis in Uganda: a cross-sectional diagnostic study. BMC Infect Dis. 2013;13(1):1–8. doi:10.1186/1471-2334-13-133
23. Timire C, Metcalfe JZ, Chirenda J, et al. International Journal of Infectious Diseases Prevalence of drug-resistant tuberculosis in Zimbabwe: a health facility-based cross-sectional survey. Int Soc Infect Dis. 2019;87:119–125. doi:10.1016/j.ijid.2019.07.021
24. Nathavitharana RR, Lederer P, Tierney DB, Nardell E. Treatment as prevention and other interventions to decrease MDR-TB transmission. Int J Tuberc Lung Dis. 2019;23(4):396–404. doi:10.5588/ijtld.18.0276
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.