")
Back to Journals » International Journal of General Medicine » Volume 17
Pulmonary Manifestations of Systemic Lupus Erythematosus Among Adults in Aseer Region, Saudi Arabia
Authors Alhammadi NA, Alqahtani HS, Mahmood SE , Alshahrani AA, Alahmari AMA, Alshahrani ARS, Badawi ASA, Alqahtani AMA, Alsalem ATA, Alqahtani MSMA, Gazzan MA
Received 24 November 2023
Accepted for publication 6 February 2024
Published 15 March 2024 Volume 2024:17 Pages 1007—1015
DOI https://doi.org/10.2147/IJGM.S449068
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Woon-Man Kung
Nouf A Alhammadi,1,* Hanan Saeed Alqahtani,2,* Syed Esam Mahmood,3,* Abdulrahman Arif Alshahrani,4,* Abdullaziz Motlaq A Alahmari,4,* Abdullah Rashid Safer Alshahrani,4,* Abdullah Saeed A Badawi,4,* Ali Mohammed Ali Alqahtani,4,* Abdullah Thabet A Alsalem,4,* Mohammed Saeed M Alsultan Alqahtani,4,* Mohammed Ali Gazzan4,*
1Department of Medicine, College of Medicine, King Khalid University, Abha, Saudi Arabia; 2Department of Internal Medicine and Rheumatology, Aseer Central Hospital, Abha, Saudi Arabia; 3Department of Family and Community Medicine, College of Medicine, King Khalid University, Abha, Saudi Arabia; 4College of Medicine, King Khalid University, Abha, Saudi Arabia
*These authors contributed equally to this work
Correspondence: Syed Esam Mahmood, Department of Family and Community Medicine, College of Medicine, King Khalid University, Abha, 62529, Saudi Arabia, Email [email protected]
Background: Nearly half of the Systemic lupus erythematosus (SLE) patients develop lung involvement. The study assessed the extent of pulmonary involvement among SLE patients and to identify the associated factors in the population.
Methodology: This retrospective cohort study was conducted at Aseer Hospital and Khamis Myshat Hospital in the Southern region of Saudi Arabia. The study spanned from January 1, 2016, to June 3, 2023. Patient inclusion criteria encompassed individuals who received a definitive diagnosis and classification as per American College of Rheumatology criteria, while patients under 18 years of age and those with mixed connective tissue diseases were exclude.
Results: A total of 247 participants were included. 41.7% (n=103) aged 41 years and older, 95.1% (n = 235) were females. Around 10.10% had diabetes mellitus and 17.00% had hypertension and hypothyroidism. Lupus Nephritis was in 15.40%. Chest involvement was reported in 21.9%, in the form of pleuritis (6.10%), pleural effusion (4.00%), and lupus pneumonitis (4.00%), interstitial lung disease (4.00%), pulmonary embolism (3.60%) of individuals, and pulmonary hemorrhage (2.80%). The respiratory symptoms reported by SLE were; dyspnea, cough, and chest pain each having a prevalence of around 18.0%. Palpitations have a relatively high occurrence at 13.80%. Meanwhile, hemoptysis (blood coughing) has a lower prevalence of 1.20%, and fever is reported at 2.80%. Having chronic kidney disease and hypertension were significantly associated with having pulmonary involvement; (χ 2=3.308, p=0.027) and (χ 2=7.782, Fisher’s p=0.002) respectively. The seropositivity for antiphospholipid Abs, anti-CCP, and antids-DNA were significantly associated with pulmonary involvement (χ 2=3.239, =p=0.049), (χ 2=4.621, Fisher’s p=0.023), and (χ 2=8.248, p=0.010) respectively.
Conclusion: The study found that 21.9% of SLE patients experience chest involvement, with varying degrees of pulmonary symptoms. Factors such as chronic kidney disease, hypertension, antiphospholipid antibodies, Anti-CCP positivity, and seropositivity for Anti-dsDNA were found to be significant associations with lung involvement, contributing to our understanding of SLE.
Keywords: Systemic lupus erythematosus, pulmonary manifestation, Anti-dsDNA antibodies, ANA
Introduction
Systemic lupus erythematosus is a chronic autoimmune illness characterized by a variety of clinical and immunological abnormalities.1 SLE-related complications can affect all compartments of the lungs and include pleuritis, interstitial lung disease (ILD), alveolar hemorrhage, shrinking lung syndrome (SLS), pulmonary hypertension (PH), airways disease, and thromboembolic disease.2 Clinicians awareness of SLE-related pulmonary symptoms and the development of more sensitive techniques capturing lung involvement have led to the realization that subclinical lung involvement occurs more frequently than clinically discernible involvement.3,4
Clinical evaluations of SLE patients should usually include a comprehensive examination for respiratory problems.4,5 Some asymptomatic patients may present with incidental findings of abnormal chest imaging or lung function tests.6 Serological indications such as elevated erythrocyte sedimentation rate (ESR), low complement, and increased double-stranded DNA (dsDNA) antibody titers, urge further need to evaluate whether the new respiratory symptoms are caused by lupus.7,8
It has been reported that around 20 to 90% of SLE patients develop the lung involvement.7,9 However, it has lately been proposed that this figure is closer to 50–70%.10 Older age and anti-RNP antibodies are predictors of progression to earlier irreversible lung damage.11 The pulmonary manifestations of SLE related mortality varies depending on the type and level of lung involvement observed.12 Chronic lung disease associated with SLE can have a negative impact on the well-being, physical performance, and quality of life of patients.13 Respiratory manifestations can be acute or chronic, primary (directly caused by the disease) or secondary (due to concomitant complications such as infections). Interestingly, acute manifestations may be associated with generalized lupus disease activity, while chronic complications may progress independently to general disease activity.14 Respiratory manifestations of SLE are associated with a variable mortality rate, depending to the type of involvement, its extension, and the presence of comorbidities.13 Therefore, the assessment and treatment of lung involvement in patients with SLE should be performed promptly. CXR, HRCT, and PFT are recommended as diagnostic work-up. Moreover, exact diagnostic criteria for lung involvement in SLE remain elusive. Thus, more attention should be paid to the active surveillance and management of pulmonary manifestations of SLE.15
The existing clinical and therapeutic trial data specifically focused on respiratory manifestations of SLE are scarce. The current study hypothesized that the prevalence of pulmonary involvement among patients with SLE is significantly high, with a tendency toward severe complications. The objective of this study was to assess the extent of pulmonary involvement among SLE patients and to identify the factors that are associated with the occurrence and severity of such involvement. Understanding these factors is essential to providing comprehensive care to patients with SLE, as it can help identify those at higher risk and potentially guide interventions to mitigate severe complications.
Methods
Study Design and Patient Selection
This retrospective cohort study was conducted at Aseer Hospital and Khamis Myshat Hospital in the Southern region of Saudi Arabia. The study spanned from January 1, 2016, to June 3, 2023. Patient inclusion criteria encompassed individuals who received a definitive diagnosis and classification according to the American College of Rheumatology criteria, while patients under 18 years of age and those with mixed connective tissue diseases were excluded.
Data Collection
Demographic information, including age, gender, nationality, and chronic diseases, was systematically extracted from patient records. Patients were asked about the duration of SLE suffering in parallel with the collection of the following laboratory data; Serum complement (C3 and C4), antiphospholipid antibodies (Antiphospholipid, ACL Ab), Anti-CCP (Cyclic Citrullinated Peptide) Antibodies; Anti-Smith Antibodies; Rheumatoid factor; Anti-dsDNA Antibodies (Anti-double-stranded DNA): Anti-dsDNA antibodies are highly specific to SLE and are often linked to lupus nephritis, a kidney complication of SLE.
Assessment of pulmonary manifestations: chest symptoms were recorded and two senior radiologists independently reviewed chest radiographs and high-resolution computed tomography (HRCT) scans to reach diagnosis consensus. Pulmonary manifestations were meticulously documented, which included pleural thickening/effusion, pericardial effusion, pneumonia, pneumonitis, interstitial lung disease, bronchiectasis, diaphragmatic dysfunction, pulmonary embolism (PE), adult respiratory distress syndrome (ARDS), diffuse alveolar hemorrhage (DAH), cryptogenic organizing pneumonia (COP) and pulmonary edema.
Statistical Analysis
Statistical analysis was carried out using R software version 4.2. Categorical variables were expressed as frequencies and percentages. The chi-square test was used to determine if there is a significant association between categorical variables. The Fisher’s Exact Test was used to determine the significance of the association between two categorical variables if the assumption of the Chi square test was violated. Phi coefficient of association was used to determine the strength and direction of association between two binary (dichotomous) variables for the 2*2 table. Cramer’s V was used to measure the association between two categorical variables in a contingency table more than 2*2. We set the p-value below 0.05 to be statistically significant.
Ethical Approval
To maintain ethical standards, the research diligently sought approval (IRB log No: REC-07-08-2022) from the Directorate of Health Affairs, Aseer Region Research Ethics Committee, and Ministry of Health Saudi Arabia. Throughout the research process, the principles outlined in the Helsinki Declaration were strictly followed.
Results
Table 1 summarizes the key demographic characteristics of a sample of 247 people. The age distribution of the sample reveals a significant prevalence of people 41 years of age and older (41.7%). The gender makeup is highly biased toward women (95.1%). Nationality data show that nearly all participants are Saudi, with one single Indian. A considerable proportion of patients (61.9%) reported having other comorbid diseases, while 38.1% did not.
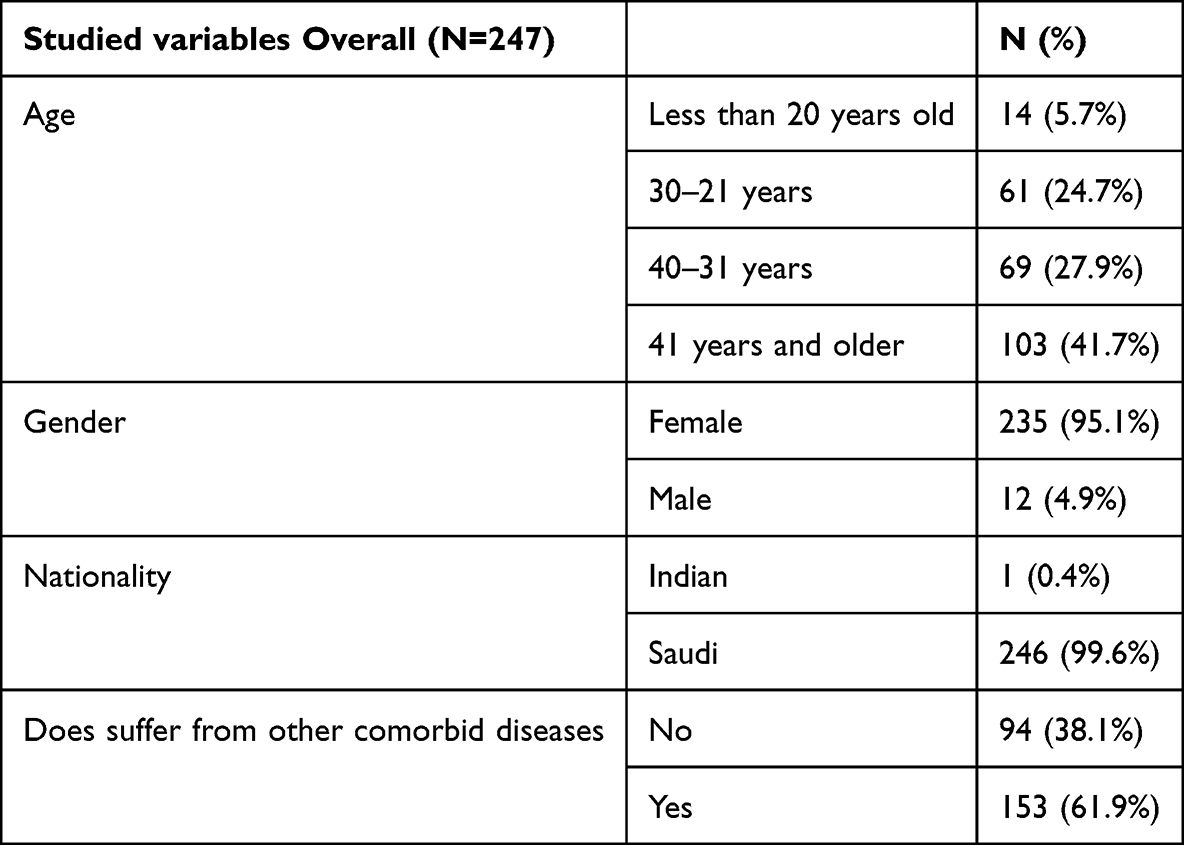 |
Table 1 Sociodemographic Characteristics of the Studied Population |
Figure 1a and b depicts the linked comorbid medical disorders in SLE patients. Among this group, the prevalence rates of associated conditions were as follows, 15.40% for Lupus nephritis, 0.40% for autoimmune hemolytic anemia (AIHA), 4.50% for pulmonary embolism (PE), 6.10% for chronic kidney disease (CKD), 6.50% for rheumatoid arthritis (RA), and 8.90% for deep vein thrombosis (DVT). The prevalence of comorbidities was as follows, 1.20% for bronchial asthma (BA), 10.10% for diabetes mellitus (DM), 17.00% for hypertension, and 17.00% for hypothyroidism.
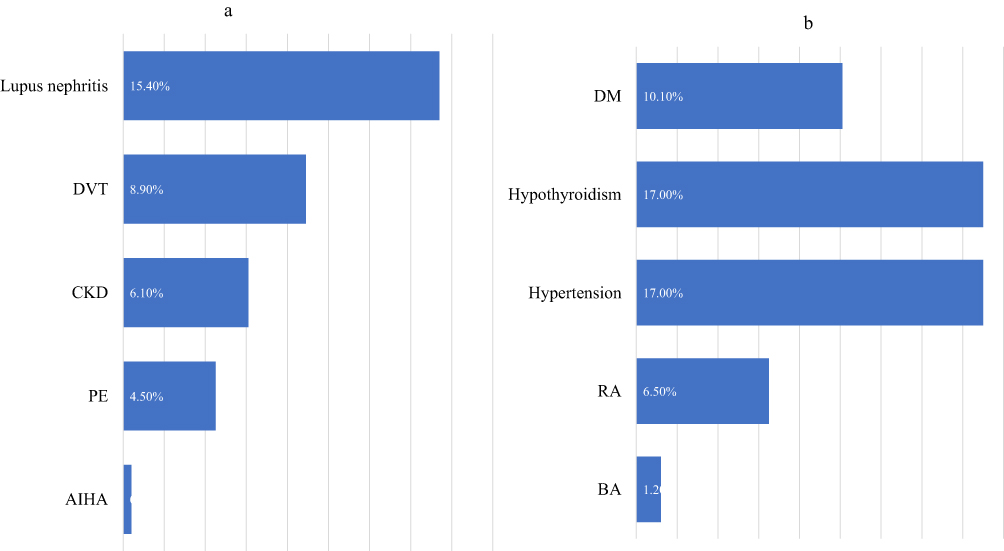 |
Figure 1 (a and b) shows the associated comorbidities associated with SLE. |
In total, 21.9% of SLE reported chest involvement. Figure 2 shows the pattern of pulmonary involvement; pleuritis, affected 6.10% of individuals, pleural effusion was present in 4.00% of cases, lupus pneumonitis, affected 4.00% of individuals, interstitial lung disease affected 4.00% of cases, pulmonary embolism was reported in 3.60% of individuals, and pulmonary hemorrhage, was reported among 2.80%. The respiratory symptoms reported by SLE were as follows; dyspnea (shortness of breath), cough, and chest pain each have a prevalence of around 18.0%. Palpitations have a relatively high occurrence at 13.80%. Meanwhile, hemoptysis (blood coughing) has a lower prevalence of 1.20%. (Figure 3)
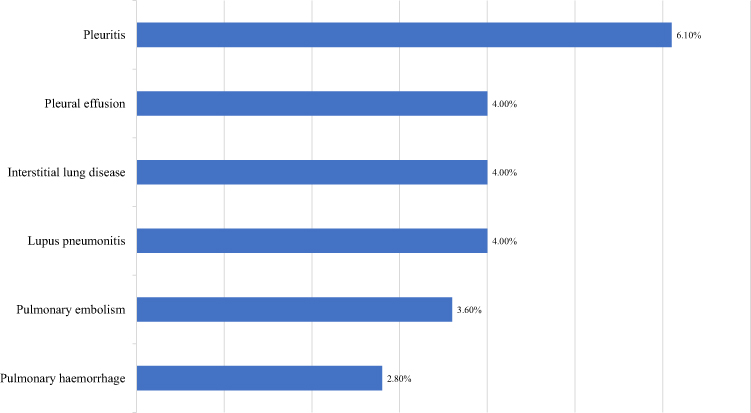 |
Figure 2 Pattern of pulmonary involvement among patients with SLE. |
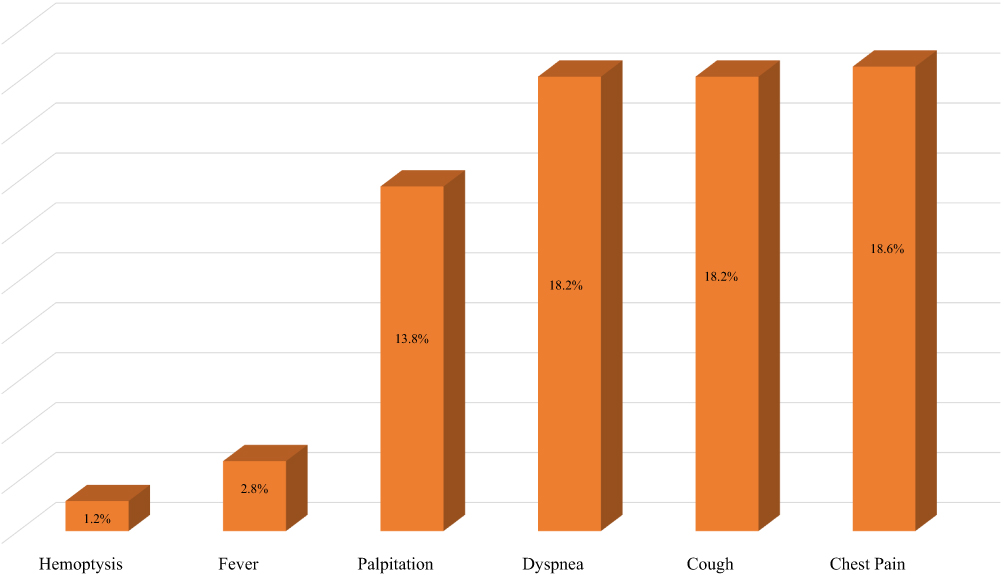 |
Figure 3 The respiratory symptoms that presented with systemic lupus erythematosus. |
Table 2 shows the characteristics of the individuals who had suffered from SLE. Regarding the duration of their SLE experience, 15.4% had experienced the condition for less than 3 years, 42.9% for a period of 3 to 6 years, 25.9% for 6 to 12 years, and 15.8% for more than 12 years. In terms of laboratory findings, serum complement was found to be positive in 3.2% of cases, antiphospholipid in 0.8%, ACL Ab in 4.5%, anti-CCP in 2.4%, anti-Smith in 1.2%, and rheumatoid factor in 17.4%. Additionally, C3 exhibited high levels in 4.5%, low levels in 24.3%, and was negative in 71.3% of cases. Similarly, C4 was observed to be high in 5.3%, low in 18.6%, and negative in 76.1% of cases. Lastly, anti-dsDNA was detected as positive in 47.0% of cases.
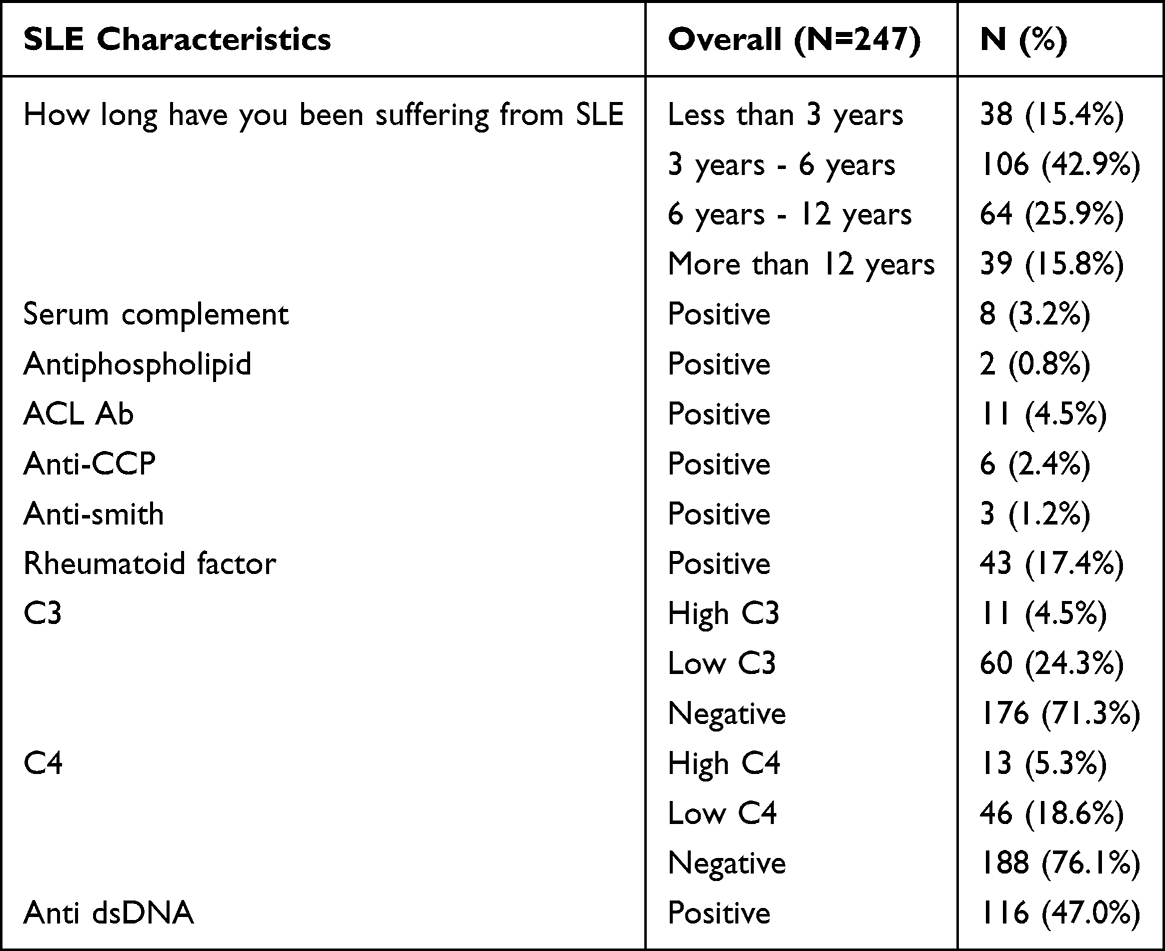 |
Table 2 Characteristics and Laboratory Profiles of Past Systemic Lupus Erythematosus Patients |
Table 3 shows the variables that were significantly associated with lung involvement among patients with SLE. Having CKD was significantly associated with having pulmonary involvement; (p=0.027(. Similarly, hypertension was significantly associated with pulmonary involvement, (p=0.002). The seropositivity for antiphospholipid Abs was significantly associated with pulmonary involvement (p=0.049). Similarly, anti-CCP and antacids-DNA seropositivity were significantly associated with pulmonary involvement (χ2=4.621, Fisher’s p=0.023), and (p=0.010) respectively.
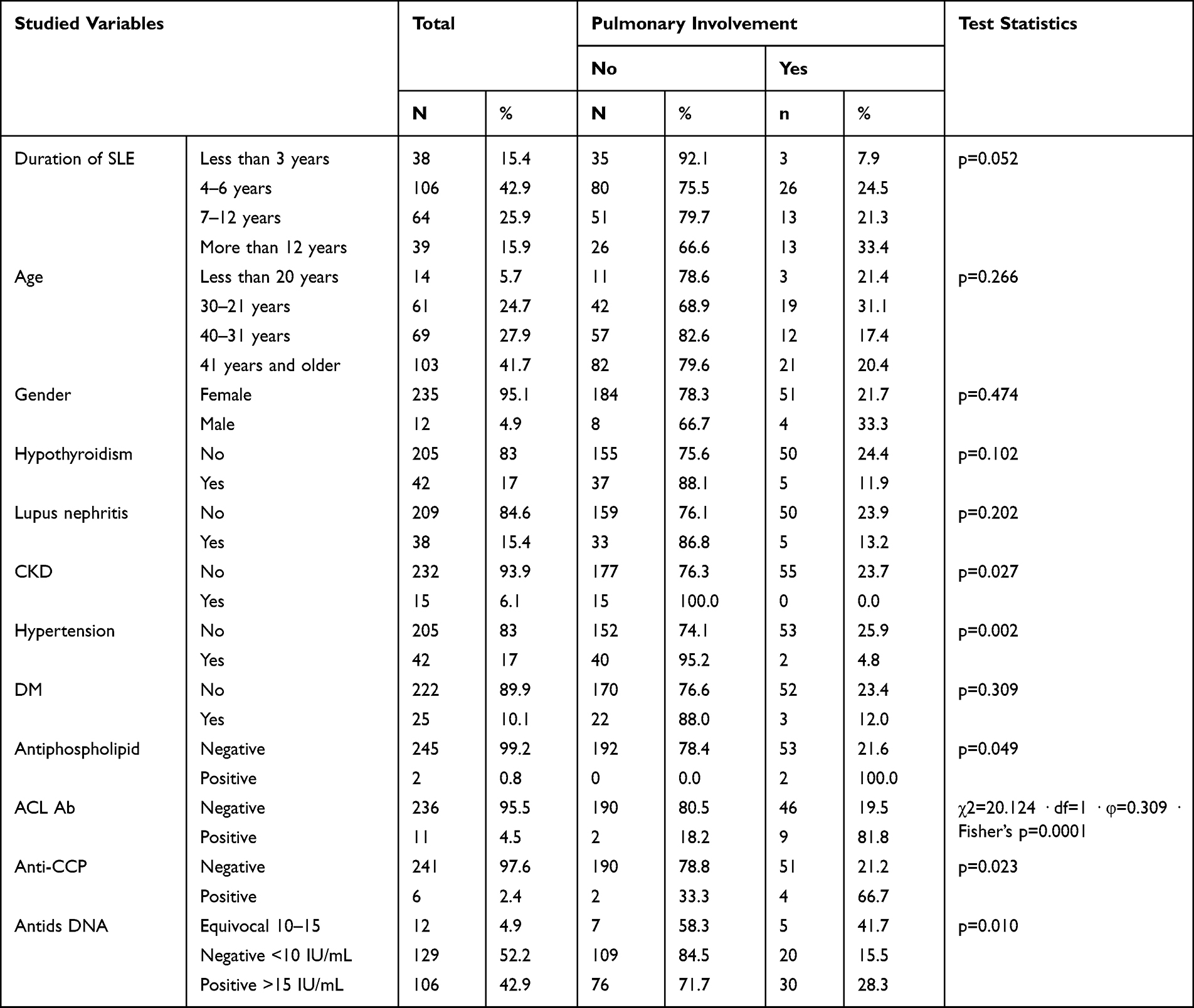 |
Table 3 Factors Associated with the Development of Pulmonary Involvement |
Discussion
In this retrospective study, we aimed to assess the prevalence of pulmonary involvement among SLE. The study found that 21.9% of SLE patients reported chest involvement, with pulmonary involvement varying among cases. Respiratory symptoms included dyspnea, cough, chest pain, palpitations, hemoptysis, and fever. These data provide insight into the prevalence of these symptoms, which are crucial for medical evaluation and diagnosis. Variables that were significantly associated with lung involvement among patients with SLE- were having CKD or hypertension, antiphospholipid Abs, Anti-CCP, and Antids-DNA seropositivity.
Incidence of Pulmonary Complications
In this study, more than one-fifth of patients with SLE had pulmonary involvement. The most reported affection was pleurisy. A similar study conducted in Saudi Arabia based on reviewing records over 10 years involving 184 patients with SLE in the Western Region found that lung manifestations were common in 33% of patients with pulmonary involvement.5 Approximately half of SLE patients have lung involvement, and 4–5% present with pulmonary symptoms.16,17 We found that the most common findings were pleural effusion, consolidation, and atelectasis. Similarly, previous studies reported that the most frequent intrathoracic condition in SLE is pleuritis, which manifests as chest discomfort, cough, dyspnea, and pleural effusion.14,17
The most favorable thoracic location involves the pleura and ranges from an asymptomatic manifestation to pleuritic pain present in around half of the patients.17 The pathologic evidence of pleural fibrosis or pleuritis reported is 50–93%, and pleural effusion in chest radiologic studies is 16–50%.17 Swigris et al18 observed that the entire pulmonary system or any of its components can be damaged in SLE. Several markers, such as higher systemic type 1 interferon (IFN) levels, circulating immune complexes (IC), and neutrophils, are associated with SLE. They appear to play a critical role in promoting lung inflammation, fibrosis, and tissue destruction.19
Duration of the SLE
We found that there was no significant association between the duration of the disease and the incidence of pulmonary complications. Pulmonary abnormalities were significantly higher within the first five years after SLE diagnosis in the study by Alamoudi et al. However, neither disease duration nor Lupus Nephritis was associated with increased risk.5 However, neither disease duration nor LN was associated with increased risk. The study highlights the importance of identifying risk factors for lung involvement in SLE patients.
Disease Complications, Activity, and Autoantibodies
We observed a significant association between having CKD or hypertension and the occurrence of pulmonary lung disease. Antids DNA was also associated with the incidence of pulmonary diseases. Similarly, Alamoudi et al5 found that low complement levels, high Anti-dsDNA levels, and disease activity were all found to be significantly associated with HRCT findings. Furthermore, the presence of pleural effusion, pneumonia, and ground glass attenuation was found to be significantly associated with disease activity. Anti-CCP is not common in SLE and usually indicates an overlap with Rheumatoid arthritis. Interestingly, positive Anti CCP -SLE patients had an increased incidence of lung disease. Whether it’s related to CCP -MUC5B promotor variant and other genetics linked to lung disease in Rheumatoid arthritis or it’s simply a serological marker and a risk factor for lung involvement in SLE, we need more studies with a larger sample size to explore the risk and association.20
Strengths and Limitations
This study encountered several limitations. Firstly, due to its retrospective nature, there is a possibility that certain patient information may have been overlooked, despite the meticulous efforts of the authors to document all relevant details. It is important to note that some data related to specific diagnoses were extracted from patient records, making it impossible to entirely rule out diagnostic errors, especially for closely related conditions. However, this study had many strengths. It was conducted in more than one center, which may reduce the risk of bias in the study’s findings. Furthermore, the sample size was considered sufficient for this study, and the cohort likely consisted of individuals with similar backgrounds, with more than 99% of Saudi nationality.
Conclusions
The study revealed that 21.9% of SLE patients reported experiencing chest involvement, with varying degrees of pulmonary manifestations observed between cases. The respiratory symptoms reported included dyspnea, cough, chest pain, palpitations, hemoptysis, and fever. The prevalence of these symptoms within the SLE population is of significant importance for medical evaluation and diagnostic considerations. In particular, certain variables displayed significant associations with lung involvement among SLE patients, including the presence of CKD or hypertension, the presence of antiphospholipid antibodies, anti-CCP positivity, and seropositivity for Anti-dsDNA. These results provide valuable insights into factors linked to pulmonary involvement in SLE patients and contribute to our understanding of this complex autoimmune condition.
Patient Privacy Protection Statement
We desensitized all the data that can be used to identify patients’ personal information, such as their names, hospitalization IDs, and telephone numbers, to protect the privacy of patients.
Data Sharing Statement
The data that support the results of this study are available from the corresponding author upon reasonable request.
Statement of Ethics
The study protocol has been reviewed and approved by the Directorate of Health Affairs, Aseer Region Ethics Committee, and Saudi Ministry of Health. Informed consent was obtained from all individuals participating in the study. The patients’ privacy and personal identity information were well protected. The protocol of the study is compliant with Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors extend their appreciation to the Deanship of Scientific Research at King Khalid University for funding this work through large group Research Project under grant number RGP2/263/44.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Bakshi J, Segura BT, Wincup C, Rahman A. Unmet needs in the pathogenesis and treatment of systemic lupus erythematosus. Clin Rev Allergy Immunol. 2018;55(3):352–367. doi:10.1007/s12016-017-8640-5
2. Pines A, Kaplinsky N, Olchovsky D, Rozenman J, Frankl O. Pleuro-pulmonary manifestations of systemic lupus erythematosus: clinical features of its subgroups. Prognostic and therapeutic implications. Chest. 1985;88(1):129–135. doi:10.1378/chest.88.1.129
3. Mittoo S, Fell CD. Pulmonary manifestations of systemic lupus erythematosus. Semin Respir Crit Care Med. 2014;35(2):249–254. doi:10.1055/s-0034-1371537
4. Hellman DB, Kirsch CM, Whiting-O’Keefe Q, et al. Dyspnea in ambulatory patients with SLE: prevalence, severity, and correlation with incremental exercise testing. J Rheumatol. 1995;22(3):455–461.
5. Alamoudi OS, Attar SM. Pulmonary manifestations in systemic lupus erythematosus: association with disease activity. Respirology. 2015;20(3):474–480. doi:10.1111/resp.12473
6. Nakano M, Hasegawa H, Takada T, et al. Pulmonary diffusion capacity in patients with systemic lupus erythematosus. Respirology. 2002;7(1):45–49. doi:10.1046/j.1440-1843.2002.00361.x
7. Aguilera-Pickens G, Abud-Mendoza C. Pulmonary manifestations in systemic lupus erythematosus: pleural involvement, acute pneumonitis, chronic interstitial lung disease and diffuse alveolar hemorrhage. Reumatol Clin. 2018;14(5):294–300. English, Spanish. doi:10.1016/j.reuma.2018.03.012
8. Amarnani R, Yeoh SA, Denneny EK, Wincup C. Lupus and the lungs: the assessment and management of pulmonary manifestations of Systemic lupus erythematosus. Front Med. 2021;7:610257. doi:10.3389/fmed.2020.610257
9. Tselios K, Urowitz MB. Cardiovascular and pulmonary manifestations of Systemic lupus erythematosus. Curr Rheumatol Rev. 2017;13(3):206–218. doi:10.2174/1573397113666170704102444
10. Hannah JR, D’Cruz DP. Pulmonary complications of systemic lupus erythematosus. Semin Respir Crit Care Med. 2019;40(02):227–234. doi:10.1055/s-0039-1685537
11. Bertoli AM, Vila LM, Apte M, et al. Systemic lupus erythematosus in a multiethnic US Cohort LUMINA XLVIII: factors predictive of pulmonary damage. Lupus. 2007;16(6):410–417. doi:10.1177/0961203307079042
12. Kamen DL, Strange C. Pulmonary manifestations of systemic lupus erythematosus. Clin Chest Med. 2010;31(3):479–488. doi:10.1016/j.ccm.2010.05.001
13. Fidler L, Keen KJ, Touma Z, Mittoo S. Impact of pulmonary disease on patient-reported outcomes and patient-performed functional testing in systemic lupus erythematosus. Lupus. 2016;25(9):1004–1011. doi:10.1177/0961203316630818
14. Torre O, Harari S. Pleural and pulmonary involvement in systemic lupus erythematosus. Presse Med. 2011;40(1 Pt 2):e19–e29. doi:10.1016/j.lpm.2010.11.004
15. Shin JI, Lee KH, Park S, et al. Systemic lupus erythematosus and lung involvement: a comprehensive review. J Clin Med. 2022;11(22):6714. doi:10.3390/jcm11226714
16. Vitali C, Bencivelli W, Isenberg DA, et al. Disease activity in systemic lupus erythematosus: report of the Consensus Study Group of the European Workshop for Rheumatology Research. II. Identification of the variables indicative of disease activity and their use in the development of an activity score. The European Consensus Study Group for Disease Activity in SLE. Clin Exp Rheumatol. 1992;10(5):541–547.
17. Crestani B. The respiratory system in connective tissue disorders. Allergy. 2005;60(6):715–734. doi:10.1111/j.1398-9995.2005.00761.x
18. Swigris JJ, Fischer A, Gillis J, Meehan RT, Brown KK. Pulmonary and thrombotic manifestations of systemic lupus erythematosus. Chest. 2008;133(1):271–280. Erratum in: Chest. 2008;133(3):832. Gilles, Joann [corrected to Gillis, Joann]. doi:10.1378/chest.07-0079
19. Lahita RG, Tsokos G, Buyon JP, Koike T, editors.. Systemic Lupus Erythematosus. San Deigo: Academic Press; 2011.
20. Kotschenreuther K, Yan S, Kofler DM. Migration and homeostasis of regulatory T cells in rheumatoid arthritis. Front Immunol. 2022;13:947636. doi:10.3389/fimmu.2022.947636
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.