Back to Journals » International Journal of General Medicine » Volume 16
Pulmonary Function Assessment in Myasthenia Gravis Patients in a National Referral Hospital in Indonesia
Authors Octaviana F ![]() , Safri AY
, Safri AY ![]() , Wiratman W, Indrawati LA, Fadli N, Hakim M
, Wiratman W, Indrawati LA, Fadli N, Hakim M
Received 11 July 2023
Accepted for publication 25 September 2023
Published 3 October 2023 Volume 2023:16 Pages 4477—4483
DOI https://doi.org/10.2147/IJGM.S426321
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Fitri Octaviana,1,2 Ahmad Yanuar Safri,1,2 Winnugroho Wiratman,1– 3 Luh Ari Indrawati,1,2 Nurul Fadli,1,3 Manfaluthy Hakim1,2
1Department of Neurology, Faculty of Medicine, Universitas Indonesia, Jakarta, Indonesia; 2Department of Neurology, Cipto Mangunkusumo General Hospital, Jakarta, Indonesia; 3Universitas Indonesia Hospital, Depok, Indonesia
Correspondence: Fitri Octaviana, Email [email protected]
Purpose: Myasthenia gravis (MG) can cause respiratory muscle weakness and the need of ventilator support. Spirometry as the gold standard for pulmonary function examination has limited availability, especially in our hospital which is only available in outpatient clinic during work hours (not in emergency room or patient room). Furthermore, all primary healthcare in Indonesia do not have spirometry equipment, thus other alternatives are required. This study aimed to analyze the relationship between a single breath counting test (SBCT), peak flow meter (PFM), and spirometry to assess pulmonary function in MG patients in a national referral hospital in Indonesia.
Patients and Methods: A single-center, cross-sectional study was conducted and SBCT, PFM, and spirometry examination were performed in MG patients and healthy controls.
Results: Seventy patients, aged 47.7 ± 13.4 years old, participated in this study. SBCT, forced vital capacity first second (FVC1), and forced expiratory volume first second (FEV1) value between MG patients and healthy controls showed a significant difference, in which healthy controls have higher SBCT, FVC1, and FEV1 values (p = 0.000, p = 0.000 and p = 0.001 respectively). There was a significant difference between PFM with SBCT and FVC1 value in MG patients. Strong correlation was found between SBCT and FVC1 in MG patients.
Conclusion: MG patients had worse pulmonary function compared to healthy controls. SBCT and PFM examination have a significant correlation with FVC1 in MG patients. Therefore, SBCT and PFM can be used as a bedside tool to detect respiratory impairment in MG patients.
Keywords: myasthenia gravis, peak flow meter, single breath counting test, spirometry
Introduction
Myasthenia gravis (MG) is an autoimmune disease characterized by fluctuating weakness of the extraocular, bulbar, and proximal muscles.1 Autoantibodies against the postsynaptic nicotinic acetylcholine receptor can be found in the serum of about 85% of patients and provide confirmation of the diagnosis.2 Muscle weakness will be worsened with activity and improved after resting.3
Approximately 15–20% of patients with MG experience a myasthenic crisis in the first 2 years after diagnosis.4 Myasthenia crisis can result from weakness of the upper airway muscles leading to obstruction and aspiration or weakness of the respiratory muscles that reduce the tidal volume or from the weakness of both muscle groups. Common precipitating factors for myasthenia crisis include respiratory infection, aspiration pneumonia, sepsis, surgical procedures, initiation of treatment with high-dose corticosteroids, and exposure to some drugs.5,6
Spirometry has been widely used in neuromuscular disease worldwide as a predictor of the need for mechanical ventilation and the incidence of respiratory failure.7 Peak expiratory flow and vital lung capacity in spirometry are components that contribute to this. The first signal measured on spirometry is the volume or air rate as a function of the lung at that time.1 There are several measurements, namely forced vital capacity (FVC), where the volume expelled during a full expiration as hard as possible starting from a full inspiration, and forced expiratory volume (FEV), where the expiratory volume is calculated from the two words/ second of the FVC maneuver.8
The Single Breath Counting Test (SBCT) is the maximum measurement of serial number counting, which is performed with a normal voice after maximal inhalation. Previous studies have shown that SBCT has a good correlation with gold standard measurements of pulmonary function test (PFT), peak expiratory flow rate (PEFR), and FEV in the first second (FEV1).9 SBCT can also effectively replace the complex laboratory measurements of PFT.
Peak Expiratory Flow Rate (PEFR) is a lung function test tool that is widely used because it is very easy and often encountered in daily practice. It is defined as the maximum flow rate that forces air out of the lungs in L/min. PEFR is a sensitive and accurate index for measuring airway obstruction and respiratory muscle strength. PEFR can be assessed using a peak flow meter (PFM) and a spirometer. PFM is a simple and inexpensive tool; therefore, it is relatively easy to measure PEFR with PFM.9
Spirometry as the gold standard for pulmonary function examination has limited availability especially in our hospital which is only available in outpatient clinic during work hours (not in emergency room or patient room). In addition, all primary care facilities in Indonesia do not have spirometry equipment, thus further alternatives are required. This study aimed to analyze the correlation between SBCT, PFM, and spirometry to assess pulmonary function in MG patients.
Materials and Methods
We performed an observational analytic study with a case–control design. The case group consisted of MG patients in the outpatient clinic, Emergency Room (ER), and inpatient ward in a National Referral Hospital in Indonesia from January to December 2019. The inclusion criteria were MG patients aged more than 18 years old. Patients were excluded if they suffered from chronic obstructive pulmonary disease due to infection, post lung infection due to tuberculosis, and other neurological diseases in the central and peripheral nervous systems such as cerebrovascular disease, intracranial tumor, and peripheral neuropathy. The sample size was determined with single proportional sample formula and the minimal sample of this study was 64 subjects. The control group consisted of healthy control volunteers recruited from the outpatient clinic who had no history of pulmonary and neurological diseases and had normal physical examinations. Because there were no established normal values of SBCT in our hospital, we introduced a control group analysis to this study. We used a 4:1 ratio of the case–control number of subjects unmatched for age and sex. The minimal number of healthy controls that were needed was 16.
Data collection was done through the interviews, medical records, and physical and pulmonary examinations (SBCT, PFM, and spirometry) results, then recorded in the research form. The interview and physical test performed on the same day by the same examiner. The patient’s age, disease duration, medication use, and complaints were all elicited during the interview in order to identify the patient’s MG type and MGFA classification during the study period. In this study, we used the spirometry normal curve/nomogram in our hospital to assess the spirometry results. The normal curve is determined according to age, gender and height. A peak flow meter was also used as a device for monitoring lung function. Peak flow meters determined by one’s personal best or typical peak flow, and could be classified as green, yellow, and red zone. Green zones were set if PFM showed between 80% and 100%. While the yellow zone represents as PFM 51% up to 80% personal best and red zone displays 50% or less of a personal best. Peak flow measurements in this range suggest the possibility of a major airway obstruction.10
SBCT, and PFM were not normally distributed, while predicted PFM, FVC1, and FEV1 were normally distributed in MG patients. SBCT, PFM, predicted PFM, FVC1, and FEV1 in MG patients with a history of crisis were normally distributed. While in healthy controls, SBCT, PFM, predicted PFM, FVC1, and FEV1 values had a normal distribution. Chi-square or Fisher test was performed for categorical data analysis, while the independent Student’s t-test or Mann–Whitney test was employed for numerical data analysis. Statistical analysis used the SPSS version 26.0 program. This research has been approved by the ethics committee of the Faculty of Medicine, Universitas Indonesia (KET-670/UN2.F1/ETIK/PPM.00.02/2019). All data and examination results were kept confidential.
Results
Characteristics of Patients
Seventy MG patients and 16 healthy controls were included in this study. The proportion of males and females was 1:2.5 in case group, ranging from 18 to 72 years old. MG patients and healthy controls showed a greater proportion of female, but there was no significant difference between sex in MG patients and healthy controls (p =0.560). MG patients have higher mean age than healthy controls. Age characteristics in MG patients and healthy controls showed significant difference (p = 0.007). There was no significant difference in body height between MG patients and healthy controls (p = 0.569), despite the fact that the features of body height in healthy controls indicated a greater mean than in MG patients (Table 1).
 |
Table 1 Characteristics of MG Patients and Healthy Controls |
Generalized symptoms (51.4%) were the most common early symptoms compared to ocular symptoms in MG patients. Patients with early onset MG showed dominance in this study. The proportion of ocular and generalized MG patient classification was almost the same. The median duration of illness of the MG patients was 3 years (Table 1).
Comparison of Pulmonary Functional Characteristics
SBCT values of MG patients and healthy controls had a significant difference, whereas healthy controls had higher SBCT values. A significant difference was also found in spirometry examination, namely on FVC1 and FEV1 between MG patients and healthy controls, where healthy controls have higher FVC1 and FEV1 values (Table 2). Our study showed a similar proportion of ocular and generalized MG types, so we further explored the characteristics of pulmonary function in these MG types. However, based on the analysis, there was no significant difference of these examinations in ocular and generalized MG types (Table 3). This demonstrates that the respiratory function might be already impaired in MG ocular patients, although they have not shown any respiratory symptoms. On the other hand, it may be that the current ocular MG patient has experienced generalized MG before which has impaired their respiratory muscle function.
 |
Table 2 Comparison of Pulmonary Functional Characteristics Between MG Patients and Healthy Controls |
 |
Table 3 Comparison of Pulmonary Functional Characteristics in Ocular and Generalized MG Patients |
MG patients with a history of the crisis showed no significant differences from those without a history of the crisis in all examination results either SBCT, PFM, or spirometry (Table 4). No significant differences were reported between spirometry with SBCT and PFM examinations (Table 5). This result shows abnormal spirometry values do not necessarily result in abnormal SBCT and PFM values in MG patients. Significant differences were found between PFM with SBCT and FVC1 examinations (Table 6). Abnormal spirometry values do not necessarily result in abnormal SBCT and PFM values in MG patients. This means that abnormal spirometry results may not always reflect respiratory impairment due to respiratory muscle weakness in MG patients.
 |
Table 4 Comparison of Pulmonary Functional Characteristics in MG Patients with and without Crisis |
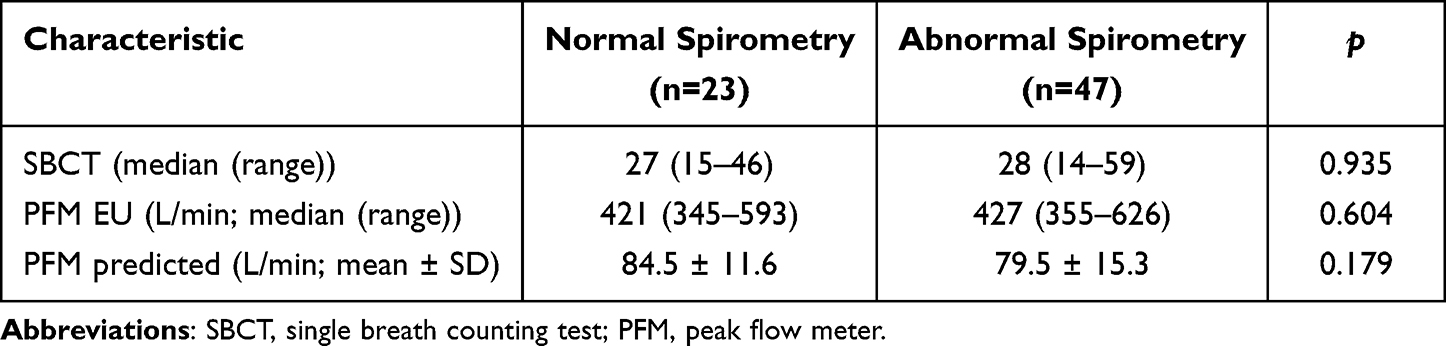 |
Table 5 Association Between Spirometry with SBCT and PFM in MG Patients |
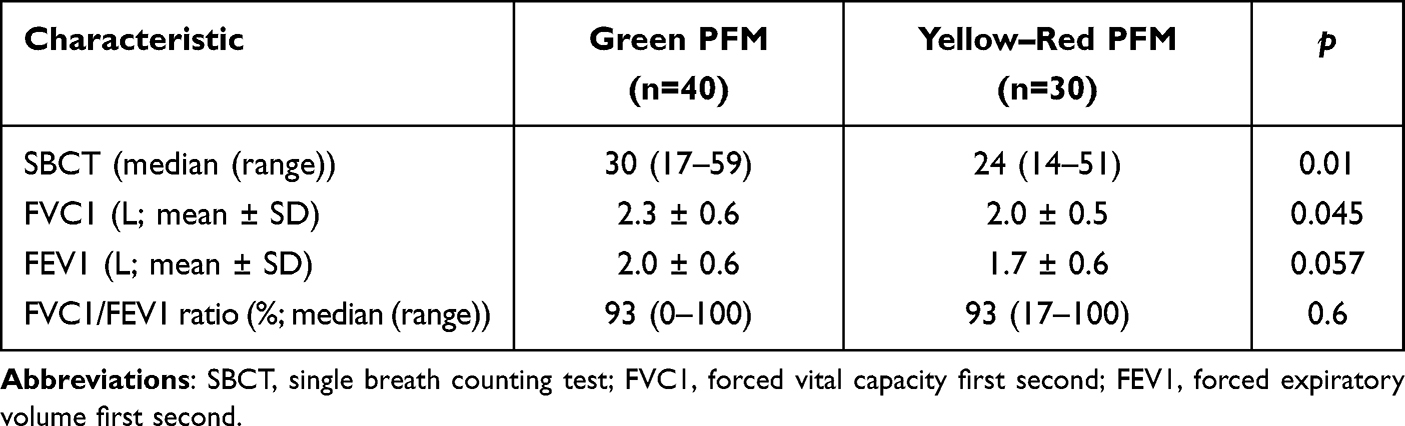 |
Table 6 Association Between PFM with SBCT, FVC1, and FEV1 in MG Patients |
Correlation analyses of each pulmonary function characteristics in all subjects, healthy controls, and MG patients were also performed (Table 7). Correlation analysis of SBCT-FVC1, SBCT-FEV1, PFM EU-FVC1 and PFM EU-FEV1 all showed significant correlations. The correlation of these variables in the overall subject shows a strong correlation level. Correlation analysis of these variables in healthy controls showed a very strong level of correlation. Correlation analysis in MG patients between SBCT and FVC1, SBCT and FEV1, PFM-EU and FEV1 showed a moderate correlation, while correlation between SBCT and FVC1 showed a strong level of correlation.
 |
Table 7 Correlation of Each Pulmonary Functional Characteristics* |
Discussion
The average age of the research subjects was ≤50 years with a higher proportion in females (2.5:1) and early onset MG. These results are similar to previous studies that showed early onset MG was more common in females.11 Males were found in high proportion in late-onset and very late-onset MG in a study conducted in Spain.12
This study showed generalized symptoms (51.4%) were slightly more frequent than ocular symptoms (48.6%). The severity of MG can be seen quantitatively based on the MG composite score and qualitatively based on the MGFA classification. Compared with previous research, ocular MG in our study showed a high proportion.13 The MGFA classification included in this study was MGFA within the last one month. We did not assess the MGFA of patients in a cohort. Therefore, it is possible that the MG patients assessed had already experienced improvement of their generalized MG symptoms.
FVC1 and FEV1 in spirometry and SBCT examination showed significant differences between MG patients and healthy controls, with healthy controls having higher FVC, FEV, and SBCT values. However, no significant differences were found between spirometry with SBCT and PFM examination. This might happen because MG patients have respiratory muscle weakness, not impaired lung function. There was a significant difference between PFM with SBCT and FVC, where FVC is one of the components in spirometry and plays a role in lung capacity related to respiratory muscle strength. Our study showed that in MG patients, there was strong correlation between SBCT and FVC1. Other studies also showed positive correlations between SBCT examination and FVC values.14,15 Therefore, SBCT could reflect the function of vital capacity of the lung. SBCT and PFM examination showed benefits in detecting a respiratory impairment as a bedside tool examination in MG patients.
However, this study has some limitations. In our study, we did not match the characteristics of cases and controls. MG patients and healthy controls showed majority in females. Age greater than or equal to 40 years was found to be more common in MG patients. While healthy controls show a higher mean body height. A study using spirometry discovered those female patients had lower mean values for pulmonary function test parameters than male patients.16 Other study shows that FEV1/FVC is declining by 0.29% per year.17 Additionally, a study discovered that the FEV1 and FVC scores were influenced by age and body height.18 This variation might influence the study’s findings.
Conclusion
FVC1 and FEV1 in spirometry and SBCT examination showed significant differences between MG patients and healthy controls, with MG patients having lower FVC1, FEV1, and SBCT values. There was a significant correlation between SBCT, PFM, and FVC1 values of the spirometry component. Thus, SBCT and PFM examination can be used as a bedside tool to detect respiratory impairment in MG patients.
Research Ethics and Consent
This research has been approved by the ethics committee of the Faculty of Medicine, Universitas Indonesia (KET-670/UN2.F1/ETIK/PPM.00.02/2019) and have been performed in accordance with the principles stated in the Declaration of Helsinki. Prior to conducting the study, all patients were fully informed and signed an informed consent indicating their agreement to participate in the study.
Acknowledgments
The authors wish to thank the patients, the team of research assistants of Clinical Neurophysiology and Neuromuscular Division, Department of Neurology, Faculty of Medicine Universitas Indonesia/Cipto Mangunkusumo General Hospital, Jakarta, Indonesia.
Funding
This research was funded by Cipto Mangunkusumo General Hospital Operational Research Fund year 2019 (Nota Dinas No. LB.03/2.2/7894/2019). The sponsors had no role in the design, execution, interpretation, or writing of the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Suresh AB, Asuncion RMD. Myasthenia Gravis. StatPearls. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559331/.
2. Meriggioli MN, Sanders DB. Muscle autoantibodies in myasthenia gravis: beyond diagnosis? Expert Rev Clin Immunol. 2012;8(5):427. doi:10.1586/ECI.12.34
3. Jayam Trouth A, Dabi A, Solieman N, Kurukumbi M, Kalyanam J. Myasthenia gravis: a review. Autoimmune Dis. 2012;1(1). doi:10.1155/2012/874680
4. Murthy J. Myasthenic Crisis – comorbidities, Complications, Long-Term Outcomes: the Challenges. Ann Indian Acad Neurol. 2019;22(4):472. doi:10.4103/AIAN.AIAN_472_19
5. Chaudhuri A, Behan PO. Myasthenic crisis. QJM an Int J Med. 2009;102(2):97–107. doi:10.1093/QJMED/HCN152
6. Godoy DA, de Mello LJV, Masotti L, Di Napoli M. The myasthenic patient in crisis: an update of the management in Neurointensive Care Unit. Arq Neuropsiquiatr. 2013;71(9 A):627–639. doi:10.1590/0004-282X20130108
7. Chiang J, Mehta K, Amin R. Respiratory Diagnostic Tools in Neuromuscular Disease. Children. 2018;5(6). doi:10.3390/CHILDREN5060078
8. Graham BL, Steenbruggen I, Barjaktarevic IZ, et al. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am J Respir Crit Care Med. 2019;200(8):e70. doi:10.1164/RCCM.201908-1590ST
9. Kumari A, Malik S, Narkeesh K, Samuel AJ. Single breath count: a simple pulmonary function test using a mobile app. Indian J Thorac Cardiovasc Surg. 2017;33(4):369–370. doi:10.1007/S12055-017-0555-5
10. DeVrieze BW, Bhimji SS Peak Flow Rate Measurement. StatPearls Publishing; 2018. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459325/.
11. Asmail A, Kesler A, Kolb H, Drory VE, Karni A. A tri-modal distribution of age-of-onset in female patients with myasthenia gravis is associated with the gender-related clinical differences. Int J Neurosci. 2019;129(4):313–319. doi:10.1080/00207454.2018.1529669
12. Cortés-Vicente E, Álvarez-Velasco R, Segovia S, et al. Clinical and therapeutic features of myasthenia gravis in adults based on age at onset. Neurology. 2020;94(11):e1171–e1180. doi:10.1212/WNL.0000000000008903
13. Suzuki S, Murai H, Imai T, et al. Quality of life in purely ocular myasthenia in Japan. BMC Neurol. 2014;14(1):142. doi:10.1186/1471-2377-14-142
14. Elsheikh B, Arnold WD, Gharibshahi S, Reynolds J, Freimer M, Kissel JT. Correlation of single-breath count test and neck flexor muscle strength with spirometry in myasthenia gravis. Muscle Nerve. 2016;53(1):134–136. doi:10.1002/mus.24929
15. Aguirre F, Fernández RN, Arrejoría RM, et al. Peak expiratory flow and the single-breath count test as markers of respiratory function in patients with myasthenia gravis. Neurol. 2023;38(6):405–411. doi:10.1016/j.nrleng.2020.09.006
16. Zakaria R, Harif N, Al-Rahbi B, Aziz CBA, Ahmad AH. Gender differences and obesity influence on pulmonary function parameters. Oman Med J. 2019;34(1):44–48. doi:10.5001/OMJ.2019.07
17. Liao SY, Lin X, Christiani DC. Occupational exposures and longitudinal lung function decline. Am J Ind Med. 2015;58(1):14–20. doi:10.1002/ajim.22389
18. Mozun R, Ardura-Garcia C, Pedersen ESL, et al. Age and body mass index affect fit of spirometry Global Lung Function Initiative references in schoolchildren. ERJ Open Res. 2022;8(2). doi:10.1183/23120541.00618-2021
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.