Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Pulmonary Arterial Pressure Changes Under Dobutamine Stress Echocardiography in Non-Anemic Iron Deficient COPD Subjects
Authors Wanderley Xavier AC, Koch R, Steinhorst Goelzer L, Muller PT ![]()
Received 10 March 2022
Accepted for publication 25 June 2022
Published 24 August 2022 Volume 2022:17 Pages 1943—1949
DOI https://doi.org/10.2147/COPD.S365461
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Ana Christina Wanderley Xavier,1,2 Rodrigo Koch,1 Leandro Steinhorst Goelzer,1 Paulo T Muller1
1Federal University of Mato Grosso do Sul (UFMS)/Maria Aparecida Pedrossian Hospital (HUMAP), Laboratory of Respiratory Pathophysiology (LAFIR), Campo Grande, Mato Grosso do Sul, MS, Brazil; 2Echocardiography Unit, Maria Aparecida Pedrossian Hospital (HUMAP), Campo Grande, Mato Grosso do Sul, MS, Brazil
Correspondence: Paulo T Muller, Laboratory of Respiratory Pathophysiology (LAFIR), Respiratory Division of University Hospital, Federal University of Mato Grosso do Sul (UFMS), Filinto Müller S/N, Vila Ipiranga, Campo Grande, CEP:79080-090, Brazil, Tel +55-67 33453149, Fax +55-67 33453049, Email [email protected]
Purpose: Non-anemic iron deficiency (NAID) is common in COPD, and could induce functional/structural changes in the pulmonary vascular bed. Thus, we aimed to study, during resting and ambient oxygen conditions, the systolic pulmonary arterial pressure (sPAP) changes during dobutamine stress echocardiography (DSE) for NAID+ compared to NAID- subjects with COPD.
Patients and Methods: We analyzed 24 patients with COPD and evaluated their clinical parameters, including lung function and serum iron profile, followed by the changes in the sPAP under DSE.
Results: Ten subjects with NAID+ were compared with fourteen NAID- subjects for sPAP measurement. At baseline, only left atrial volume was significantly different between groups (30± 4 vs 23± 5 mL*m2), respectively (p-value=0.002). For the right side, tricuspid annular plane systolic excursion (TAPSE) was similar between-groups (22± 2 vs 20± 4, p-value > 0.05), at baseline. The sPAP (mmHg) changes were also not significantly different between groups (pre 32± 14 vs peak 48± 14 for NAID+ and pre 29± 7 vs peak 43± 10 for NAID-, Group p-value=0.400, Time p-value < 0.0001, and Interaction p-value=0.606).
Conclusion: COPD subjects with NAID do not show increased sPAP responses during DSE, compared with iron-replete subjects.
Keywords: COPD, iron deficiency, pulmonary hypertension, stress echocardiography
Introduction
Non-anemic iron deficiency (NAID) is a common metabolic disorder, affecting between 18% and 48% of subjects with chronic obstructive pulmonary disease (COPD).1,2 Among the known pulmonary vascular effects of NAID are intracellular oxidative stress dysregulation,3 pulmonary arterial smooth muscle proliferation,4 and hyperreactive hypoxic pulmonary vasoconstriction (HPV).5 Thus, NAID could be associated with increased systolic pulmonary arterial pressure (sPAP) under resting conditions in COPD subjects.6 Hypoxia (and iron deficiency) could stabilize the hypoxia induced factor 1-α and trigger HPV.4,5 In spite of this, little attention has been given to the hemodynamic effects involved in the pulmonary vascular bed in COPD subjects with NAID; in fact, COPD subjects are prone to abnormal increases in sPAP under certain conditions, eg, exacerbations, sleep-associated hypoxemia or exercise.7
NAID has been associated with lower physical activity and exercise capacity in COPD.2,8 Moreover, iron supplementation led to increased exercise capacity.9 In “healthy” people with NAID, iron supplementation led to a reduction in sPAP during exercise, independently of hypoxia.5 As pulmonary arterial bed regulation has an important role for exercise performance, the impact of NAID for sPAP responses under increased pulmonary blood flow conditions is critical to expand our knowledge in this field.
Thus, the current study was performed primarily to explore sPAP responses in COPD with or without NAID, under dobutamine stress echocardiography (DSE), with the main hypothesis of a significantly higher increase in sPAP under DSE in the NAID group compared to the iron-replete group. The secondary endpoint was baseline left and right ventricular performance differences between the groups.
Methods
This is an observational, single-center, parallel-group and prospective study, including patients from March to December 2021. The subjects were recruited at the COPD clinic from the University Hospital (HUMAP) after local Ethics Committee on Research Involving Human Beings approval, from the Federal University of Mato Grosso do Sul (number 20527619.2.0000.0021), and all patients provided written informed consent. Subjects were invited to participate during two visits. The first visit was intended to verify inclusion/exclusion criteria, blood analysis, and lung function tests. The second visit was scheduled for the DSE.
Inclusion criteria were COPD subjects with at least two months stable disease and with optimized bronchodilator therapy. Exclusion criteria included chronic oxygen therapy, previous myocardial infarction, anemia (<12 g% for woman and <13 g% for men),10 serious cardiac arrhythmia, non-effective increase in heart rate during DSE, and intercurrent comorbidities, such as bronchial asthma, thyroid pathology, heart failure, neoplasia, lung resection, uncontrolled hypertension, or diabetes. The criteria for NAID in COPD subjects are controversial and there is no global consensus.2,6,10 Notwithstanding, we used the most accepted criteria for COPD, including functional and definitive NAID; Definitive NAID was defined as a ferritin level lower than 100 ng/mL and functional NAID included subjects with a ferritin level between 100 and 299 ng/mL and transferrin saturation (TS) <20%. Lung function included pre- and post-bronchodilator spirometry and the carbon monoxide diffusion capacity, both following the ERS/ATS criteria11 and Brazilian predictive values.12,13
The standard and stress echocardiography were performed in a climatized room; two-dimensional, M-mode, and Doppler echocardiography were performed according to the American Society of Echocardiography.14 The subjects were admitted during the morning and under food fasting. A venous line catheter was inserted in the median basilic vein. Images and parameters were collected with a standard device (EPIQ 7C, Philips, USA). The initial examination consisted of the left ventricular (LV) measures, including the left atrial indexed volume (LAV). LV ejection fraction was measured by the Teichholz and Simpson methods. In addition, LV diastolic function was performed by tissue and pulsed-Doppler echocardiography. Detailed methods for assessment of LV diastolic function have been previously published,15 and included: (i) peak velocity of early diastole (E), peak atrial contraction velocity (A), and the E/A ratio, obtained by pulsed-wave Doppler on the mitral valve; (ii) Tissue pulsed-wave Doppler of the septal and lateral portions of the mitral annulus in diastole (E´) and the E/E´ ratio. The baseline and peak tricuspid reflux velocity (TRV) were obtained through continuous-wave Doppler at the right ventricle (RV) inlet, and the sPAP was measured by the peak gradient between the RV and the right atrium from the peak TRV, after right atrium pressure (RAP) acquisition and using the Bernoulli equation (sPAP = (TRV)2 + RAP). RAP was estimated from the inferior vena cava diameter and collapsibility. Right ventricular systolic function was assessed at baseline with the tricuspid annular plane systolic excursion (TAPSE). All patients underwent continuous dobutamine infusion, under continuous monitoring of systemic arterial pressure (SAP), heart rate (HR), and peripheral oximetry (SpO2) (DIXTAL DX 25215, Dixtal, 2008). Dobutamine was increased at increments of 5 μg· kg−1·min−1 at 3-min intervals up to a maximum of 40 μg·kg−1·min−1, seeking to achieve 85% of the maximal predicted HR. In order to reach the predicted submaximal HR, we also used handgrip exercise and atropine (up to a maximum dose of 2 mg), from the dobutamine dose of 20 μg·kg−1·min−1.16 The echocardiography was performed by a cardiologist-sonographer, blinded for blood analysis results, with wide experience in COPD echocardiograms. Thus, all records were considered technically acceptable.
All data are presented as mean±SD. For prediction of the minimum sample size, we used recently published data on reliability of sPAP through DSE.17 Considering a between-subjects average ferritin difference of 100 ng/mL, and a within-subject mean ± SD difference of −1.2±8.0 mmHg for peak sPAP, 10 subjects in each group are necessary to reach a power of 0.8, in a two-tailed study, with significance adjusted for a p-value <0.05, in a two-way repeated measure ANOVA design. Categorical variables were submitted to the Fisher statistical approach and the Shapiro–Wilks method was used to evaluate the distribution profile of the sample. In addition, the Student t or Mann–Whitney U-tests were performed where appropriate for group comparisons.
Results
Twenty-four subjects were eligible and performed all the tests. Ten NAID+ and fourteen NAID- subjects were evaluated for primary and secondary endpoints. The subjects (mean±SD) were aged 65±11 vs 66±9 years, respectively, and were similar for gender, body mass index (BMI), Charlson Comorbidity Index (CCI), and smoking status (p-value >0.05 for all, Table 1). Similarly, FEV1 (47±19 vs 48±13%predicted) and frequency of comorbidity/medication use were not significantly different between groups (p-value >0.05 for all, Table 1).
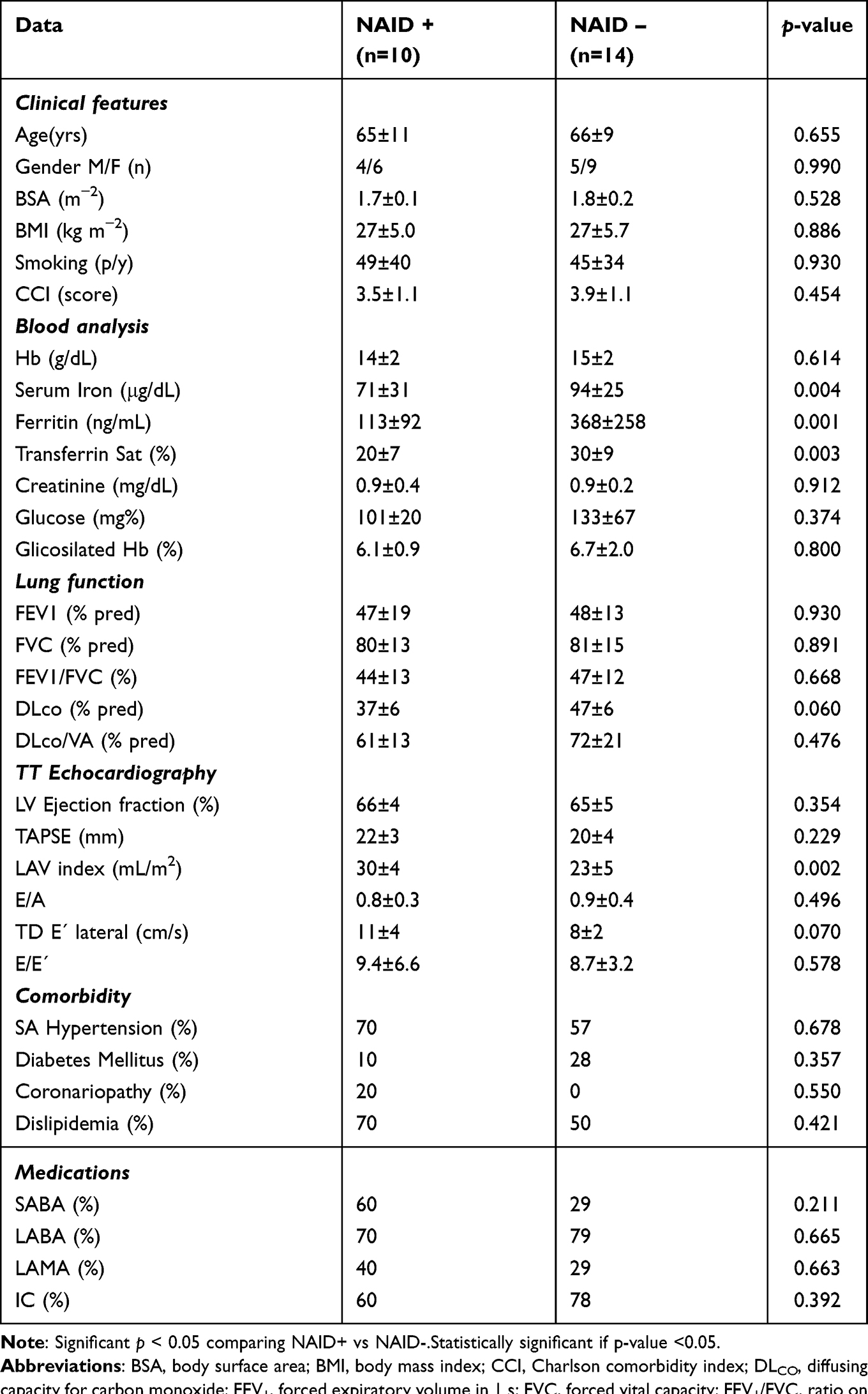 |
Table 1 Clinical Features, Blood Analysis, Lung Function, and TT Echocardiography for Selected Data. Comparative Data Between COPD with and without NAID |
For the LV evaluation, only the LAV index (mL*m2) was significantly different for NAID+ vs NAID- subjects (30±4 vs 23±5 respectively, p-value=0.002, Table 1). Tissue Doppler E´ lateral (cm/s) was marginally non-significant between-groups (11±4 vs 8±2, p-value=0.07, Table 1). For the right side, TAPSE (mm) was similar between-groups at baseline (22±2 vs 20±4, p-value >0.05, Table 1). The sPAP changes (baseline-to-peak, mmHg) were also not significantly different between-groups (pre 32±14 vs peak 48±14 for NAID+ and pre 29±7 vs peak 43±10 for NAID-, Group p-value=0.400, Time p-value <0.0001, and Interaction p-value=0.606, Table 2 and Figure 1B). HR, TRV, and SAP responses were also not significantly different (p > 0.05 for both, Table 2 and Figure 1A, C and D). Of note, SpO2 increased significantly for the two groups over time (p-value <0.0001, Table 2).
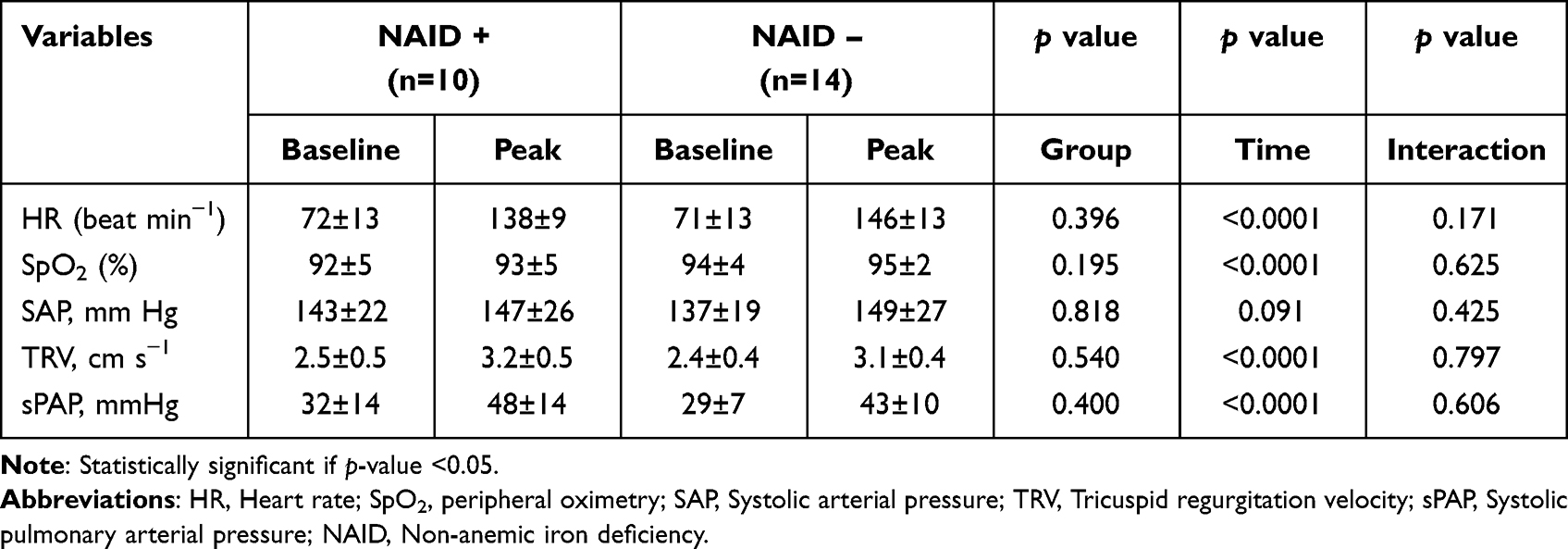 |
Table 2 Cardiovascular and Oxygenation Results for Dobutamine Stress Echocardiography |
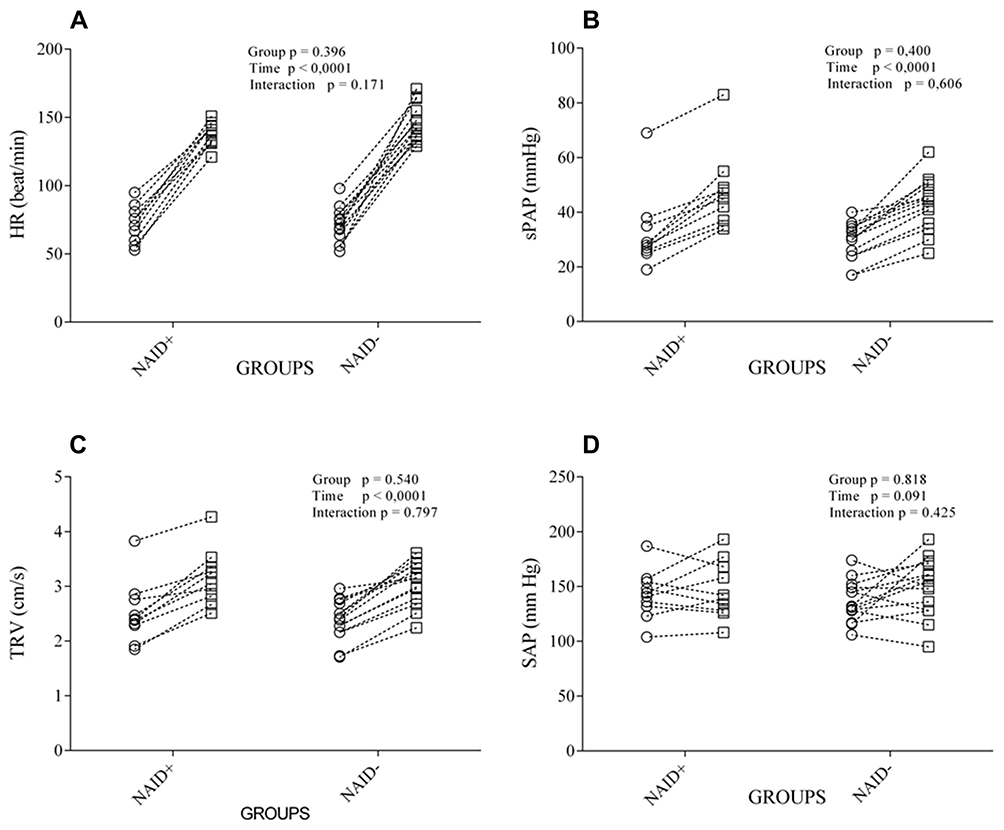 |
Figure 1 Baseline-to-peak DSE results for heart rate (HR, (A)), systolic pulmonary arterial pressure (sPAP, (B)), tricuspid regurgitation velocity (TRV, (C)), and systemic blood pressure (SAP, (D)) according to the groups. Circles=baseline and squares=peak. |
Discussion
To the best of our knowledge, this is the first study to assess sPAP changes under DSE in COPD subjects with NAID. Our preliminary results do not support a role for NAID in increases in sPAP under clinically stable, ambient oxygen, and resting conditions. Further evaluations during exercise are warranted to understand the role of NAID in the pulmonary vascular bed as a limiting factor for exercise intolerance, independently of well-established peripheral muscle impairment due to NAID.
DSE is underused for evaluation of the sPAP responses in COPD. Recently, DSE has been used to detect occult pulmonary arterial hypertension in the presence of normal sPAP under standard echocardiography, with satisfactory diagnostic accuracy compared to invasive methods.18 DSE has the advantage that it can be administered to patients unable to perform exercise. However, in the COPD population, exercise has the advantage of triggering (I) unambiguous hypoxemia, or, at least, (II) a fall in the pO2 of venous blood during exercise, that might act as a stimulus to HPV, which is possibly exacerbated in the presence of iron deficiency.5
Our study was not designed to detect the incidence of PAH in COPD with NAID; thus, the small sample of our study preclude conclusions that could confirm the results of Plesner et al with regard to the increased frequency of PAH in COPD with NAID under standard echocardiography and resting conditions.6 Considering a TRV > 2.90 m/s diagnostic for PAH,6 both groups had the same frequency of baseline PAH (~20%). We should consider, however, that in the Plesner et al study, the authors included only COPD subjects with definitive NAID (Ferritin <100 ng/mL).6
The finding of an increased LAV in the NAID+ group is difficult to evaluate, considering the small number of subjects and absence of invasive measurements. Although iron deficiency could induce myocardial energetic disturbance secondary to mitochondrial dysfunction, inducing reduced ventricular reserve,19 a previous study did not show abnormal cardiac filling pressures in NAID+ subjects.20 Moreover, TAPSE, SAH frequency, and LV diastolic function were all similar in both groups. As limitations of this study, we point out the small number of subjects, and the possibility of overestimation of NAID diagnosis owing to the inclusion of functional NAID.6 In addition, pharmacologically induced maximal heart rate under DSE does not characterize the complex mechanisms of exercise intolerance. However, a tachycardia-related increase in sPAP under DSE could predict occult pulmonary arterial hypertension,21 eventually even highly correlated with invasive methods.18 Of note, subjects with “early” pulmonary arterial hypertension but yet with normal or near-normal resting hemodynamics, could present with an abnormal PAP when stressed by an increase in pulmonary blood flow.22,23
As a preliminary conclusion, NAID in COPD subjects does not induce increased sPAP responses under resting conditions and during dobutamine stress echocardiography. Future studies should include exercise with invasive or non-invasive methods for better understanding of the impact of NAID on pulmonary arterial resistance and its contribution to exercise limitation.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval
This study follows ethical standards recommended by the revised statement of Helsinki and the Ethics Committee on Research Involving Human Beings from the Federal University of Mato Grosso do Sul (Approval number 20527619.2.0000.0021). All patients provided written informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Post-Graduate Program on Health and Development in West Central Region at Federal University of Mato Grosso do Sul (Brazil) and was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nickol AH, Frise MC, Cheng HY, et al. A cross-sectional study of the prevalence and associations of iron deficiency in a cohort of patients with chronic obstructive pulmonary disease. BMJ Open. 2015;5(7):e007911. doi:10.1136/bmjopen-2015-007911
2. Barberan-Garcia A, Rodríguez DA, Blanco I, et al. Non-anaemic iron deficiency impairs response to pulmonary rehabilitation in COPD. Respirology. 2015;20(7):1089–1095. doi:10.1111/resp.12591
3. Pérez-Peiró M, Martín-Ontiyuelo C, Rodó-Pi A, et al. Iron replacement and redox balance in non-anemic and mildly anemic iron deficiency COPD patients: insights from a clinical trial. Biomedicines. 2021;9(9):1191. doi:10.3390/biomedicines9091191
4. Lakhal-Littleton S, Crosby A, Frise MC, et al. Intracellular iron deficiency in pulmonary arterial smooth muscle cells induces pulmonary arterial hypertension in mice. Proc Natl Acad Sci U S A. 2019;116(26):13122–13130. doi:10.1073/pnas.1822010116
5. Cheng HY, Frise MC, Curtis MK, et al. Intravenous iron delivers a sustained (8-week) lowering of pulmonary artery pressure during exercise in healthy older humans. Physiol Rep. 2019;7(13):e14164. doi:10.14814/phy2.14164
6. Plesner LL, Schoos MM, Dalsgaard M, et al. Iron deficiency in COPD associates with increased pulmonary artery pressure estimated by echocardiography. Heart Lung Circ. 2017;26(1):101–104. doi:10.1016/j.hlc.2016.04.020
7. Blanco I, Piccari L, Barberà JA. Pulmonary vasculature in COPD: the silent component. Respirology. 2016;21(6):984–994. doi:10.1111/resp.12772
8. Martín-Ontiyuelo C, Rodó-Pin A, Sancho-Muñoz A, et al. Is iron deficiency modulating physical activity in COPD? Int J Chron Obstruct Pulmon Dis. 2019;14:211–214. doi:10.2147/COPD.S182700
9. Santer P, McGahey A, Frise MC, et al. Intravenous iron and chronic obstructive pulmonary disease: a randomised controlled trial. BMJ Open Respir Res. 2020;7(1):e000577. doi:10.1136/bmjresp-2020-000577
10. Pizzini A, Aichner M, Sonnweber T, Tancevski I, Weiss G, Löffler-Ragg J. The significance of iron deficiency and anemia in a real-life COPD cohort. Int J Med Sci. 2020;17(14):2232–2239. doi:10.7150/ijms.46163
11. Miller MR, Hankinson J, Brusasco V, et al.; ATS/ERS Task Force. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
12. Pereira CA, Sato T, Rodrigues SC. New reference values for forced spirometry in white adults in Brazil. J Bras Pneumol. 2007;33(4):397–406. doi:10.1590/s1806-37132007000400008
13. Neder JA, Andreoni S, Peres C, Nery LE. Reference values for lung function tests. III. Carbon monoxide diffusing capacity (transfer factor). Braz J Med Biol Res. 1999;32(6):729–737. doi:10.1590/S0100-879X1999000600008
14. Lang RM, Bierig M, Devereux RB, et al.; Chamber Quantification Writing Group; American Society of Echocardiography’s Guidelines and Standards Committee; European Association of Echocardiography. Recommendations for chamber quantification: a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005;8(12):1440–1463. doi:10.1016/j.echo.2005.10.005
15. Muller PT, Utida KAM, Augusto TRL, et al. Left ventricular diastolic dysfunction and exertional ventilatory inefficiency in COPD. Respir Med. 2018;145:101–109. doi:10.1016/j.rmed.2018.10.014
16. Pellikka PA, Nagueh SF, Elhendy AA, Kuehl CA, Sawada SG; American Society of Echocardiography. American Society of Echocardiography recommendations for performance, interpretation, and application of stress echocardiography. J Am Soc Echocardiogr. 2007;20(9):1021–1041. doi:10.1016/j.echo.2007.07.003
17. Pergola V, Previtero M, Lorenzoni G, et al. Feasibility and role of right ventricular stress echocardiography in adult patients. J Cardiovasc Echogr. 2021;31(2):68–72. doi:10.4103/jcecho.jcecho_4_21
18. Rallidis LS, Papangelopoulou K, Makavos G, Varounis C, Anthi A, Orfanos SE. Low-dose dobutamine stress echocardiography for the early detection of pulmonary arterial hypertension in selected patients with systemic sclerosis whose resting echocardiography is non-diagnostic for pulmonary hypertension. J Clin Med. 2021;10(17):3972. doi:10.3390/jcm10173972
19. Martens P, Claessen G, Van De Bruaene A, et al. Iron deficiency is associated with impaired biventricular reserve and reduced exercise capacity in patients with unexplained dyspnea. J Card Fail. 2021;27(7):766–776. doi:10.1016/j.cardfail.2021.03.010
20. Martens P, Verbrugge FH, Nijst P, Dupont M, Mullens W. Limited contractile reserve contributes to poor peak exercise capacity in iron-deficient heart failure. Eur J Heart Fail. 2018;20(4):806–808. doi:10.1002/ejhf.938
21. Lau EM, Vanderpool RR, Choudhary P, et al. Dobutamine stress echocardiography for the assessment of pressure-flow relationships of the pulmonary circulation. Chest. 2014;146:959–966. doi:10.1378/chest.13-2300
22. Kovacs G, Maier R, Aberer E, et al. Borderline pulmonary arterial pressure is associated with decreased exercise capacity in scleroderma. Am J Respir Crit Care Med. 2009;180(9):881–886. doi:10.1164/rccm.200904-0563OC
23. Condliffe R, Kiely DG, Peacock AJ, et al. Connective tissue disease-associated pulmonary arterial hypertension in the modern treatment era. Am J Respir Crit Care Med. 2009;179(2):151–157. doi:10.1164/rccm.200806-953OC
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Beyond Tumors: The Pivotal Role of TRIM Proteins in Chronic Non-Tumor Lung Diseases
Huang X, Yu W, Wei A, Wang X, Chen S
Journal of Inflammation Research 2025, 18:1899-1910
Published Date: 7 February 2025