Back to Journals » Risk Management and Healthcare Policy » Volume 16
Public’s Willingness to Perform COVID-19 Self-Testing During the Transition to the Endemic Phase in Malaysia – A Population-Based Cross-Sectional Study
Authors Ng DLC, Bin Jamalludin MA, Gan XY, Ng SY, Bin Mohamad Rasidin MZ ![]() , Felix BA, Jagang NM, Sindeh W, Bin Mohd Abdul Rahim MAH, Tan SB
, Felix BA, Jagang NM, Sindeh W, Bin Mohd Abdul Rahim MAH, Tan SB ![]() , Chai CS
, Chai CS
Received 9 September 2023
Accepted for publication 16 November 2023
Published 21 November 2023 Volume 2023:16 Pages 2505—2519
DOI https://doi.org/10.2147/RMHP.S439530
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gulsum Kaya
Diana-Leh-Ching Ng,1 Mohd Amirulikhmar Bin Jamalludin,2 Xhi-Yan Gan,3 Siew-Yoong Ng,3 Muhammad Zulhusni Bin Mohamad Rasidin,4 Beverlyn Anak Felix,1 Nicholas M Jagang,5 Woweham Sindeh,6 Mohd Abdul Hafiz Bin Mohd Abdul Rahim,7 Seng-Beng Tan,8 Chee-Shee Chai1
1Department of Medicine, Faculty of Medicine and Health Science, University Malaysia Sarawak, Kota Samarahan, Malaysia; 2Department of Emergency and Trauma, Sarawak General Hospital, Kuching, Malaysia; 3Department of Medicine, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia; 4Department of Obstetrics and Gynaecology, Hospital Raja Perempuan Zainab II, Kota Bharu, Malaysia; 5Membakut Health Clinic, Ministry of Health, Beaufort, Malaysia; 6Telupid Health Clinic, Ministry of Health, Beluran, Malaysia; 7Department of Medicine, Sungai Buloh Hospital, Sungai Buloh, Malaysia; 8Palliative Care Unit, Subang Jaya Medical Center, Subang Jaya, Selangor, Malaysia
Correspondence: Chee-Shee Chai, Department of Medicine, Faculty of Medicine and Health Science, University Malaysia Sarawak, Kota Samarahan, Malaysia, Tel +6019-8188265, Email [email protected]
Introduction: Malaysia entered the transition to the endemic phase of Coronavirus 2019 (COVID-19) on 1st April 2022. This study aims to determine the public’s willingness to perform COVID-19 self-testing. Factors that influenced their willingness were also assessed.
Methods: A nationwide, cross-sectional, and population-based study was conducted online in Malaysia from 28th April 2023 to 4th June 2023. Individuals aged 18 years and above were enrolled through the snowball sampling method. Data were analyzed by using the Chi-Square test, independent t-test, and binary logistic regression.
Results: One thousand four hundred fifty-three responses were included in the analysis. Of these respondents, 89.3% were willing, 4.1% were reluctant, and 6.6% remained hesitant to perform COVID-19 self-testing, The common reasons given by those willing to perform COVID-19 self-testing included being able to self-isolate (99.0%) and seek treatment (96.3%) earlier if tested positive. The common reasons against COVID-19 self-testing included the belief that COVID-19 is equivalent to the common flu (91.7%) and having received the COVID-19 vaccine (78.3%). The isolation policy for COVID-19 was the most significant consideration for those who were still hesitant (85.4%). Women [adjusted odds ratios (OR): 2.1, 95% confidence intervals (95% CI): 1.44– 3.00, p < 0.001], individuals with tertiary education (OR: 2.1, 95% CI: 1.32– 3.26, p = 0.002), those vaccinated against COVID-19 (OR: 8.1, 95% CI: 2.63– 24.82, p < 0.001), and individuals with prior experience of COVID-19 self-testing (OR: 4.2, 95% CI: 2.84– 6.12, p < 0.001) showed a significantly higher willingness to engage in COVID-19 self-testing.
Conclusion: The public exhibited a high willingness to perform COVID-19 self-testing during the transition to the endemic phase in Malaysia. Future strategies to promote COVID-19 self-testing uptake in Malaysia should focus on vulnerable groups, address the common concerns among those hesitant and reluctant, and highlight the advantages of COVID-19 self-testing.
Keywords: COVID-19, self-testing, endemic, willingness, hesitant, Malaysia
Introduction
The Coronavirus 2019 (COVID-19) pandemic is the worst-ever global health emergency, leading to a catastrophic loss of human lives and economic recession.1 As of 2nd September 2023, COVID-19 has infected 695 million people worldwide, leading to 6.9 million deaths.2 The aggressive global immunization rollout for COVID-19 since 2021 has finally revealed light at the end of the pandemic tunnel.3 On 5th May 2023, the World Health Organization declared that COVID-19 was no longer a public health emergency of international concern.4
In Malaysia, the first case of COVID-19 was detected in January 2020.5 To date, a total of 5.1 million cases and thirty-seven thousand deaths have been reported.2 Public health measures implemented during the initial phase of the pandemic included nationwide lockdown,6 contact tracing facilitated by the mobile application “MySejahtera”,7 and adherence to the “3C3W” principle (avoiding Crowds, Confined spaces, Close conversation; practicing Wear masks, Washing hands, Warning of disease) as standard operating procedures.6 The National COVID-19 Immunization Program was subsequently initiated, starting in February 2021 for adults, September 2021 for adolescents, and February 2022 for children.8
On 1st April 2022, Malaysia entered the transition to the endemic phase of COVID-19, prompted by the effectiveness of these public health measures.9 While most of the restrictive measures were gradually lifted, COVID-19 testing within communities was further strengthened via the “TRIIS” strategies (self-Testing if symptomatic, Report if positive, Isolate, Inform close contact, Seek treatment).10 A total of forty-three antigen-detection rapid diagnostic tests (Ag-RDTs) were conditionally approved by the authorities and made readily available to the public over the counter at an affordable cost, aiming to promote self-testing.11
Self-testing refers to an in-vitro test of body materials by individuals without health consultation with the aim to detect a disease or risk.12 In addition to pregnancy, self-testing has been widely used to detect infectious diseases, metabolic disorders, and cancers.13 Self-testing empowers individuals, granting them autonomy and self-management over their health.13,14 Compared to clinical laboratory testing, self-testing offers advantages such as convenience, cost-saving, and confidentiality.15 Additionally, the use of self-testing in combating the COVID-19 pandemic has demonstrated substantial benefits, including reduced community transmission through early isolation and contact tracing,16 accelerated access to treatment,17 and decongested clinical testing facilities.18
Understanding the willingness of the public to engage in COVID-19 self-testing can aid in designing and implementing policies that enhance test uptake. However, the existing data on the public’s willingness to perform COVID-19 self-testing primarily stem from studies conducted during the early or midst of the pandemic. Studies have shown the willingness of the public to engage in self-testing varies at different stages of public health crises, influenced by factors such as government testing policies, community infection rates, and health literacy.19 Moreover, at the onset of the transition to the endemic phase, one in two Malaysians reported experiencing COVID-19 pandemic fatigue.20 Two-thirds of them expressed tiredness to test for COVID-19 even when it was indicated.20 Therefore, as the transition to the endemic phase progresses, declining motivation for COVID-19 self-testing over time could emerge as a major concern.
This study aims to determine the public’s willingness to perform COVID-19 self-testing one year after the transition to the endemic phase in Malaysia. The sociodemographic and clinical factors that influenced their willingness, as well as the reasons behind their decision, were also assessed. The findings of this study will enable authorities to refine their strategies and response plans for more effective COVID-19 control in anticipation of the endemic phase.
Materials and Methods
Study Design and Respondents
A nationwide, cross-sectional, and population-based study was conducted in Malaysia from 28th April 2023 to 4th June 2023. The inclusion criteria were any individuals aged 18 years and above, who stayed in Malaysia since the transition to the endemic phase and were willing to provide informed consent. Individuals who were unable to read in English, Malay, or Mandarin were excluded from the study. A minimum sample size of 255 subjects was required, calculated using the formula for cross-section study - sample size = Z1-α 2p(1 - p)/d2.21 Z represented the confidence interval at 95%, d denoted the margin of error at 5%, and p referred to the proportion of COVID-19 self-testing refusal and hesitancy in the previous study at 21%.17 All respondents provided online informed written consent before participating in the study. This study had been granted ethics approval from the Medical Research Ethics Committee of the University Malaya Medical Center (MREC ID No. 2022312–11071) and was conducted in accordance with the Declaration of Helsinki.
Procedure
This study was conducted online using the snowball sampling recruitment method to obtain responses from a broader population. Firstly, the advertisement and survey questionnaire in the format of a Google Form were sent to the researchers’ contacts who met the study criteria through mobile WhatsApp. Secondly, agreeable contacts were asked to complete an online consent form after confirming that they understood the study’s purpose. Thirdly, respondents were instructed to independently complete the anonymous study questionnaire, which was available in either English, Malay, or Mandarin. Fourthly, respondents were encouraged to share the study with their contacts who also met the study criteria. A similar recruitment process was repeated until an adequate sample was achieved. No incentives were provided to the respondents.
Tools Development
The survey questionnaire was developed by a group of experts in COVID-19 control based on post-literature reviews and discussions,10,22–24 taking into account local health policies and the COVID-19 situation.25–27 To ensure face validity and content validity of the questionnaire, feedback was obtained through a pilot study involving 80 laymen and a group of clinicians experienced in health surveys. The questionnaire consisted of three parts, 1. Sociodemographic and clinical characteristics of the respondents, 2. Practices of COVID-19 self-testing among respondents since the transition to the endemic phase, 3. The willingness of the respondents to perform COVID-19 self-testing and the reasons behind their decision.
Operational Definition
The sociodemographic characteristics of the respondents included age, gender, marital status, region of residence, education level, household income, employment status, healthcare worker status, and whether they lived together with the elderly, someone with chronic illness, or young children. The clinical characteristics of the respondents included the presence of chronic illness, history of significant contact with someone who had COVID-19, COVID-19 diagnosis, and COVID-19 vaccination status. The region of residence was categorized into five regions: Central region (Kuala Lumpur, Selangor, and Putrajaya), Southern region (Johor, Melaka, and Negeri Sembilan), Northern region (Perak, Penang, Kedah, and Perlis), East Coast (Pahang, Kelantan, and Terengganu), and Borneo Island (Sarawak, Sabah, and Labuan). The household income was classified into three categories: B40 – bottom 40% (less than RM 6200 per month), M40 – middle 40% (RM 6200 – RM 13,000 per month), and T20 – top 20% (more than RM 13,000 per month).28
Survey Questionnaire
COVID-19 self-testing practices were assessed by capturing the types of Ag-RDTs used and the indications for their self-testing. Eleven indications were provided, including one regarded symptom, two regarded contacts, four regarded requirements, and four regarded self-surveillances (Supplementary File). For respondents’ willingness to perform COVID-19 self-testing, response options included “Yes”, “No”, and “Hesitate”. A list of fifteen reasons was provided for respondents who were willing to perform COVID-19 self-testing to choose from, including two regarded management, three regarded perceived risks, six regarded strengths of Ag-RDTs, and four regarded self-reassurance. For respondents who were not willing to perform COVID-19 self-testing, a list of fifteen reasons was also provided, including three regarded psychological fears, four regarded perceived risks, three regarded disease beliefs, and five regarded weaknesses of Ag-RDTs. For respondents who were still hesitant to perform COVID-19 self-testing, fourteen factors that could affect their future decision were listed, including three regarded management, one regarded public perception, three regarded perceived risks, four regarded properties of Ag-RDTs, one regarded COVID-19 situation, and two regarded recommendations.
Statistical Analysis
The statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS for Windows version 25.0, SPSS Inc, Chicago, IL, USA). Continuous variables were presented as mean ± standard deviation (SD) while categorical variables were presented as percentages. The respondents were divided into two groups based on their willingness to perform COVID-19 self-testing - those who were willing versus those who were hesitant or not willing. Between groups differences were compared using an independent t-test for continuous variables and a Chi-Square test for categorical variables. A two-sided p-value of less than 0.05 was considered statistically significant in this study. For multivariate analysis, variables that showed significant two-sided p-values in the univariate analysis were included as covariates in the binary logistic regression. The analysis aimed to obtain odds ratios (OR), 95% confidence intervals (95% CI), and two-sided p-values.
Results
Sociodemographic and Clinical Characteristics of the Respondents
Of the 1527 study responses received, 1480 (96.9%) respondents agreed to participate in the study. The final sample consisted of 1453 (95.2%) respondents after excluding 27 (1.8%) of them who were below 18 years old. Table 1 shows the sociodemographic and clinical characteristics of the respondents.
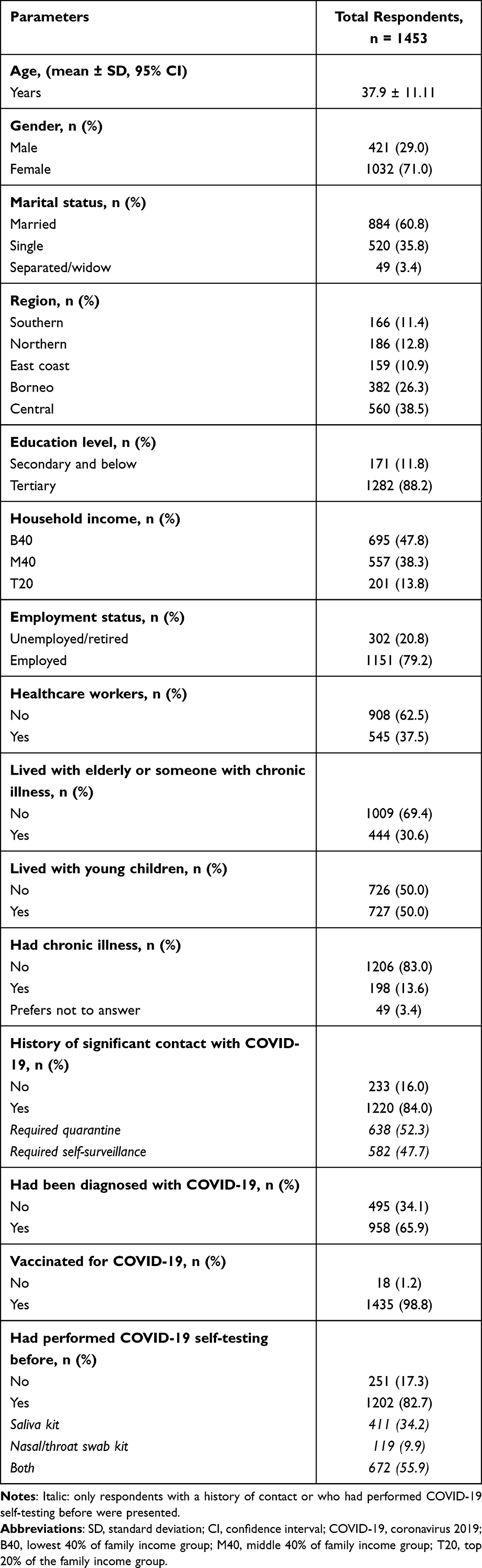 |
Table 1 Sociodemographic and Clinical Characteristics of the Respondents |
The respondents had a mean age of 37.9 ± 11.11 years. The majority of them were female (71.0%), married (60.8%), had tertiary education (88.2%), currently employed (79.2%), and were non-healthcare workers (62.5%). Geographically, 38.5% of the respondents were from the Central region, 26.3% were from Borneo Island, 12.8% were from the Northern region, 11.4% were from the Southern region, and 10.9% were from the East Coast. In terms of family income, 47.8% of them were categorized as B40, 38.3% as M40, and the remaining 13.8% as T20.
Half of the respondents had young children at home, while 30.6% were living with the elderly or someone with a chronic illness. Only 13.6% of the respondents reported having a chronic illness, with another 3.4% refusing to disclose further. The majority of the respondents had a history of significant contact with someone diagnosed with COVID-19 (84.0%) or had been diagnosed with COVID-19 (65.9%). Almost all respondents (98.8%) had received the COVID-19 vaccine.
Practices of COVID-19 Self-Testing Since the Transition to the Endemic Phase
During the transition to the endemic phase, 82.7% of the respondents reported having performed COVID-19 self-testing. Among those who self-tested, 34.2% used saliva Ag-RDTs, 9.9% used nasal/throat swab Ag-RDTs, and 55.9% used both saliva and nasal/throat swab Ag-RDTs.
The two most common indications for performing COVID-19 self-testing were having symptoms of COVID-19 (64.5%) and close contact with someone diagnosed with COVID-19 (58.3%) (Figure 1). Other common indications included casual contact with someone diagnosed with COVID-19 (33.8%) and the requirement to return to the workplace or school (30.1%).
 |
Figure 1 Indications to perform COVID-19 self-testing. |
Willing to Perform COVID-19 Self-Testing and the Reasons Behind
89.3% of the respondents were willing to perform COVID-19 self-testing (Table 2). The majority of the respondents agreed with all the reasons provided in the survey (51.1–99.0%) as the rationale behind their willingness to perform COVID-19 self-testing (Figure 2), except for the reason that they were at high risk of severe COVID-19 (39.6%). The most common reasons cited by respondents for their willingness to perform COVID-19 self-testing were related to disease management. For example, respondents expressed that they would be able to self-isolate (99.0%) and seek treatment (96.3%) earlier if they tested positive for COVID-19. Other reasons included self-reassurance (85.4% to 91.1%), the perceived strengths of Ag-RDTs (62.4% to 98.1%), and perceived risks (39.6% to 55.1%). A few respondents also mentioned that they were willing to perform COVID-19 self-testing because they were not eligible to receive the COVID-19 vaccine due to health problems.
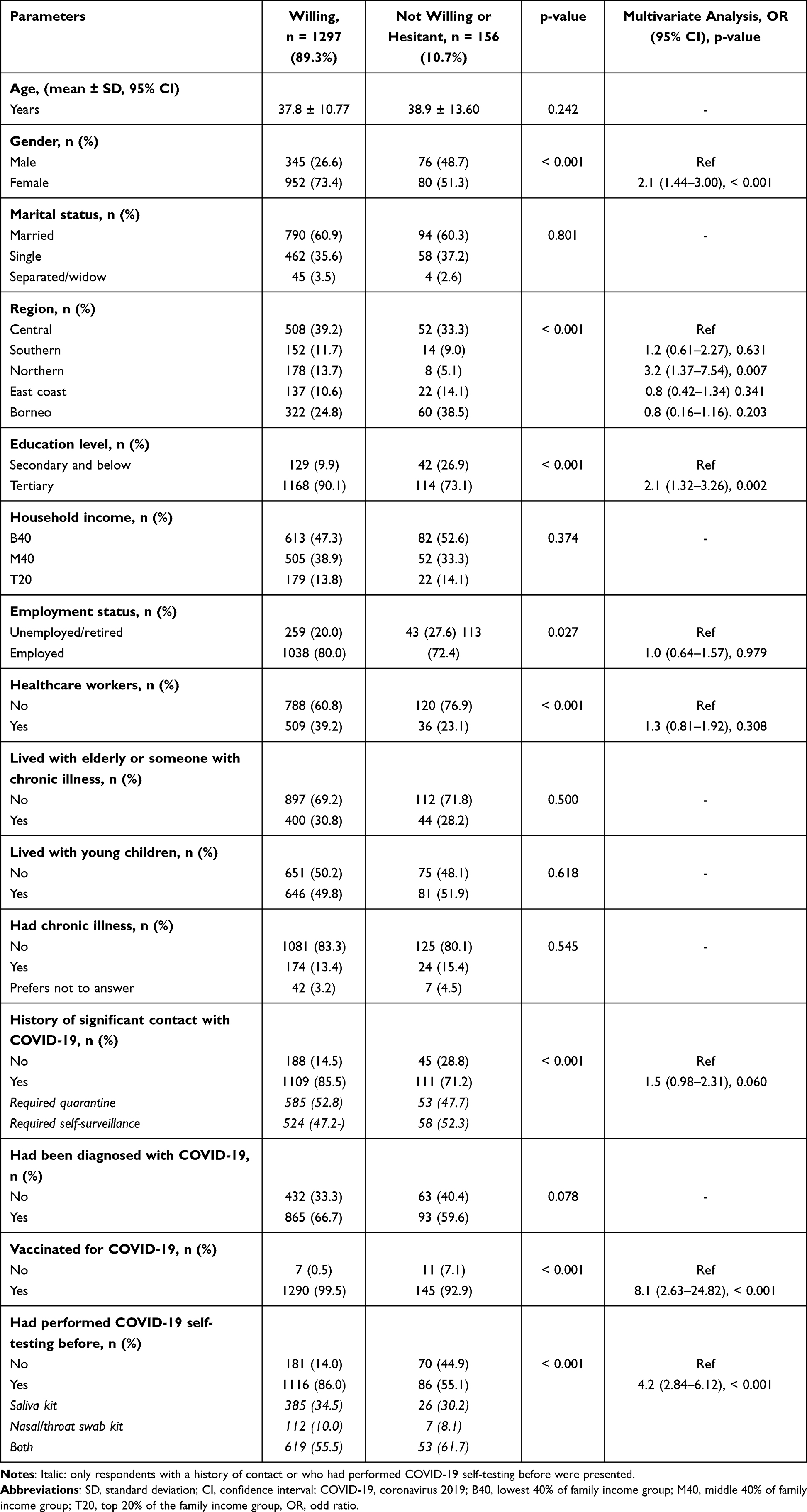 |
Table 2 The Willingness of the Respondents to Perform COVID-19 Self-Testing |
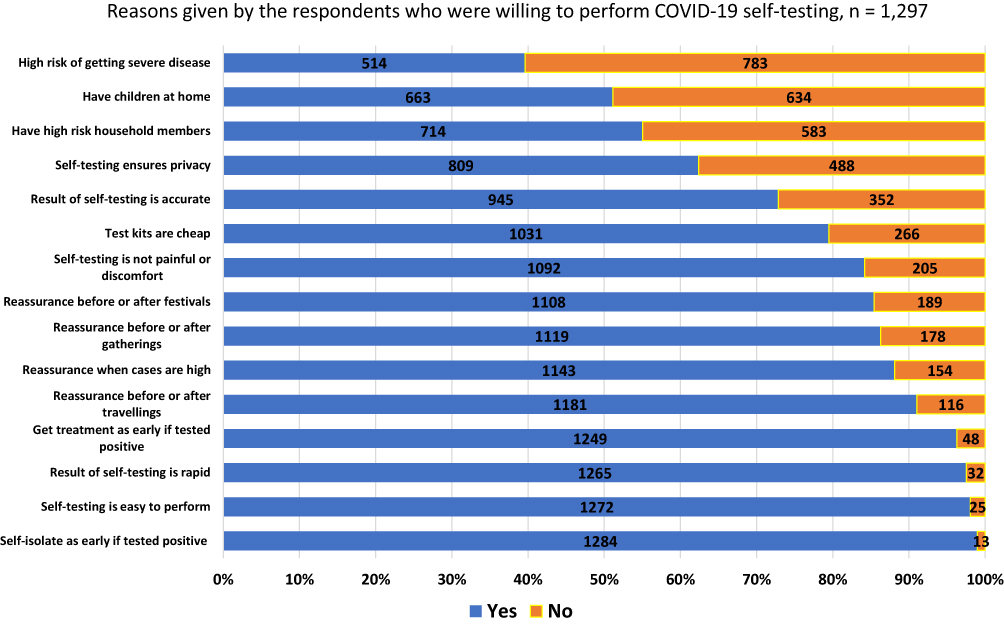 |
Figure 2 Reasons given by the respondents who were willing to perform COVID-19 self-testing. |
Not Willing to Perform COVID-19 Self-Testing and the Reasons Behind
Only 4.1% of respondents stated that they were not willing to perform COVID-19 self-testing. The common reasons given by these individuals included the belief that COVID-19 is equivalent to the common flu (91.7%), having received the COVID-19 vaccine (78.3%), autonomy not to be tested (76.7%), and considering themselves to be at low risk of severe COVID-19 (75.0%) (Figure 3). Only 3.3% of them were unaware that COVID-19 could be self-tested. No additional reasons were mentioned by this group.
 |
Figure 3 Reasons given by the respondents who were not willing to perform COVID-19 self-testing. |
Hesitant to Perform COVID-19 Self-Testing and the Reasons Behind
Another 6.6% of the respondents were still hesitant to perform COVID-19 self-testing. Apart from the price of the Ag-RDTs kit (47.9%), these respondents indicated that they would take into account all the factors listed in the survey (58.5–85.4%) before deciding whether to perform COVID-19 self-testing (Figure 4). The isolation policy for COVID-19 was the most significant consideration for this group (85.4%). No additional concerns were mentioned by these respondents.
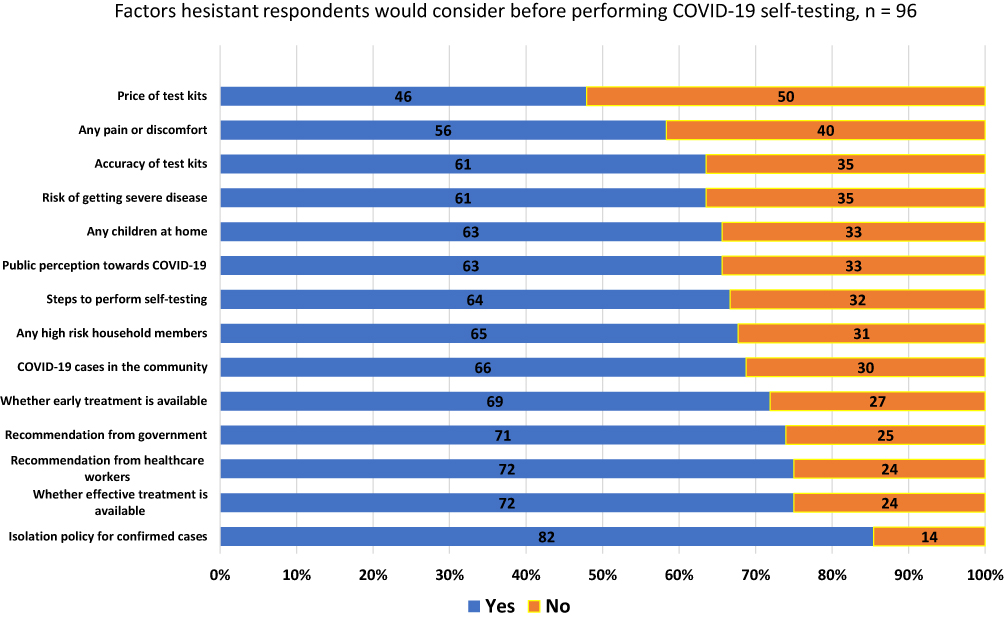 |
Figure 4 Factors hesitant respondents would consider before performing COVID-19 self-testing. |
Factors Influencing Willingness to Perform COVID-19 Self-Testing - Association and Logistic Regression
Factors that influenced respondents’ willingness to perform COVID-19 self-testing included their gender (p < 0.001), region of residence (p = 0.001), education level (p < 0.001), employment status (p = 0.027), whether they were healthcare workers (p < 0.001), history of significant contact with someone who had COVID-19 (p < 0.001), COVID-19 vaccination status (p < 0.001), and whether they had previously performed COVID-19 self-testing (p < 0.001).
Multivariate analysis of binary logistic regression showed that respondents who were female (OR: 2.1, 95% CI: 1.44–3.00, p < 0.001), had tertiary education (OR: 2.1, 95% CI: 1.32–3.26, p = 0.002), vaccinated against COVID-19 (OR: 8.1, 95% CI: 2.63–24.82, p < 0.001), and had performed COVID-19 self-testing before (OR: 4.2, 95% CI: 2.84–6.12, p < 0.001) were significantly more willing to perform COVID-19 self-testing. Additionally, respondents from the Northern zone (OR: 3.2, 95% CI: 1.37–7.54, p = 0.007) were significantly more willing to perform COVID-19 self-testing than those from the Central zone.
Discussion
General Discussion
To date, only one study has assessed the public’s willingness to perform COVID-19 self-testing during the transition to the endemic phase. In this study, 87.3% of the population in China who had never been infected by COVID-19 expressed their willingness to undergo COVID-19 self-testing.29 Other studies conducted during the early or midst of the COVID-19 pandemic reported varying levels of willingness to perform COVID-19 self-testing among their respective populations. For instance, a higher willingness rate was reported in South Africa (90.4%),30 Nigeria (84.1%),31 Kenya (81.4%),32 and Greece (79.0%).17 A slightly lower willingness rate was reported in the United Arab Emirates (70.3%),33 while an even lower rate was reported in Indonesia (60.8%) and Brazil (49.1%),34,35 respectively. In comparison to these studies, our population reported a higher willingness to perform COVID-19 self-testing (89.3%). This could be attributed to various government initiatives aimed at promoting self-testing since Malaysia entered the transition to the endemic phase. These include enhancing health literacy regarding COVID-19 self-testing via constant information and education provision, as well as ensuring the easy availability, accessibility, and affordability (3As) of test kits.11 Furthermore, the adoption of new health behaviours that encourage Malaysians to live with COVID-19 and get tested when indicated may explain this higher willingness.36
Several factors have been identified to be associated with a higher willingness to perform COVID-19 self-testing in previous studies. A higher education level was reported in five studies,17,29,31,34,35 full-time employment was reported in four studies,31,33–35 residents of the rural area was reported in three studies,30,32,34 and older age,29,33 female gender,29,33 previously investigated for COVID-19,29,31 and higher perceived risk of COVID-19 infection were reported in two studies,29,31 respectively. Additionally, one study each reported that individuals who stayed with the elderly,29 previously diagnosed with COVID-19,33 had been vaccinated against COVID-19,33 and possessed better knowledge about COVID-19 were more willing to perform COVID-19 self-testing.29 Those with lower income, limited internet access, and recent experience with non-pharmacological intervention to mitigate COVID-19, such as quarantine, however, were shown to be more reluctant to perform COVID-19 self-testing.29 Our study indicates that females, individuals with higher education levels, those who have received COVID-19 vaccinations, and those with prior experience in COVID-19 self-testing displayed a greater willingness to participate in self-testing, were aligned with the findings of some of these studies.
There are several explanations for the factors influencing respondents’ willingness to perform COVID-19 self-testing in this study. Firstly, individuals who have received the COVID-19 vaccine were more motivated for COVID-19 self-testing because they had higher perception of disease risks and precautionary methods benefits.37 This aligns with the Health Belief Model, which stated that an individual’s health-related action or behaviours are often influenced by their beliefs.38 Secondly, previous studies have shown that health behaviours during the COVID-19 pandemic are often shaped by the past experiences.39 Therefore, those who have previously undergone COVID-19 self-testing were more likely to repeat the test. Thirdly, women were more willing than men to engage in COVID-19 self-testing due to better health awareness. Women have shown greater enthusiasm for seeking health information, participating in health screenings, and adopting health prevention strategies even prior to the pandemic.40 During the pandemic, they were also more likely to perceive COVID-19 as a serious threat and were more inclined to adopt infection-preventive measures.41 Fourthly, a higher level of education is often associated with improved economic status, social-psychological support, and better access to healthcare.42 Those with higher education levels tend to be more proactive in disease detection and are likely to make safer health choices.43 Consequently, their higher willingness to engage in COVID-19 self-testing can be attributed to these factors.
To the best of our knowledge, only two studies have explored the reasons behind the willingness of the public to engage in COVID-19 self-testing. The first study involved Black/African Americans,44 while the second study included Indonesian decision makers for the COVID-19 self-testing program.45 In both studies, reasons for willingness to perform COVID-19 self-testing include the ease of use, convenience, and enable early detection of disease.44,45 Conversely, the first study identified concerns regarding the cost, accuracy, and reliability of the test kits;44 while second study revealed fears of being isolated, social stigma, and the belief that COVID-19 does not exist as barriers to adopting self-testing.45 Despite our respondents expressing similar reasons for being willing to engage in COVID-19 self-testing, their reasons against it were mainly due to false belief that COVID-19 vaccines prevent infection and COVID-19 is equivalent to common flu. Our study was conducted when majority of the population had already received vaccines and COVID-19 cases presented with milder symptoms, explained this divergence in concerns. The cost and test accuracy did not emerge as significant barrier among our respondents, likely owing to the government 3As strategy for test kits.11
Strategies for Interventions
One-tenth of the respondents in this study expressed hesitancy or reluctance to engage in COVID-19 self-testing, which could be a concern. With the anticipation of Malaysia soon entering the endemic phase, where individuals will be required to self-monitor, self-test, and self-manage, we propose several strategies to enhance adoption of COVID-9 self-testing. Firstly, future strategies to promote COVID-19 self-testing uptake should focus on the most vulnerable group - individuals who have not yet received COVID-19 vaccine. Identifying this group can be achieved through sources like “MySejahtera” that keeps immunization records of Malaysians,6 or social media platforms such as Facebook and WhatsApp groups where misleading vaccine information tends to circulate.46 The benefits of COVID-19 self-testing along with supporting evidence should be conveyed to them. Secondly, individuals who have never tried COVID-19 self-testing can be encouraged to start doing the test via practical demonstrations. Offering simple and clear instructions supported by visual aids can facilitate the learning process and make it more convenient for new users. Additionally, providing free test kits and testing incentives can prove beneficial in promoting new uptake.23 Thirdly, false beliefs that act as barriers to COVID-19 self-testing should be addressed. Specifically, the public should be informed that individuals infected with COVID-19 face a higher risk of hospitalization, mortality, and long-term complications when compared to those affected by the common flu.47 Additionally, it is essential to emphasize that the COVID-19 vaccine is designed to reduce the severity of the disease but does not prevent against infection.48 Fourthly, addressing public concerns about the isolation policy for COVID-19 could help to alleviate hesitations. These include considering a shorter duration, permitting flexibility, and providing both financial and emotional support.49 Lastly, the advantages of COVID-19 self-testing should be constantly highlighted as part of the educational efforts.
Strengths and Limitations
This is the first study in Malaysia that assessed the public’s willingness to perform COVID-19 self-testing. This study had a large sample size, potentially could represent the general population in Malaysia as the distribution of respondents’ geographical location and family income align with those reported in the national population census. This study also comprehensively explores reasons behind the respondents’ willingness to perform COVID-19 self-testing.
This study has several limitations. Firstly, the use of snowball sampling, a non-probability method, may introduce potential bias due to the reliance on participants referrals.Secondly, this study only limited to adults with internet access, potentially excluded individuals who were older, had lower education levels, and resided in rural that tend to have lower health literacy.43 Thirdly, this cross-sectional study assessed participants’ responses at a specific point in time, limiting the ability to capture changes in willingness to perform COVID-19 self-testing over time and its association with participant characteristics. Fourthly, the survey questionnaire was not tested for construct validity, criterion validity, and reliability. Lastly, the respondents’ knowledge of COVID-19 self-testing was not assessed, despite its potential influence on their attitudes and practices related to precautionary measures.50
Conclusions
The public exhibited a high willingness to perform COVID-19 self-testing one year after the transition to the endemic phase in Malaysia. Women, individuals with tertiary education, those vaccinated against COVID-19, and individuals with prior experience of self-testing were significantly more willing to engage in COVID-19 self-testing. The future strategies to promote COVID-19 self-testing uptake in Malaysia should focus on vulnerable groups, address the common concerns among those hesitant or reluctant, and highlight the advantages of COVID-19 self-testing.
Abbreviations
COVID-19, Coronavirus 2019; Ag-RDTs, antigen-detection rapid diagnostic tests; B40, lowest 40% of family income group; M40, middle 40% of family income group; T20, top 20% of the family income group; OR, odds ratios; CI, confidence intervals; SD, standard deviation; 3 As, availability, accessibility, and affordability.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The ethics approval for this study was obtained from the University of Malaya Medical Centre Medical Research Ethics Committee (MREC ID No. 2022312-11071). The study was conducted according to the Declaration of Helsinki. Written informed consent was obtained from all of the participants.
Acknowledgments
We would like to express our gratitude to all the participants in the study. The authors wish to thank Universiti Malaysia Sarawak for the financial support of this project.
Author Contributions
All authors – DLCN, MABJ, XYG, SYN, MZBMR, BAF, NMJ, WS, MAFBMAR, SBT, and CSC made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Open Access funding provided by the Universiti Malaysia Sarawak. Otherwise, this study did not receive funding from any other sources.
Disclosure
The authors declare no potential conflicts of interest in respect to the finance, research, authorship, and publication of this article.
References
1. Ciotti M, Ciccozzi M, Terrinoni A, Jiang W-C, Wang C-B, Bernardini S. The COVID-19 pandemic. Crit Rev Clin Lab Sci. 2020;57(6):365–388. doi:10.1080/10408363.2020.1783198
2. Worldometer. COVID-19 Coronavirus Pandemic; 2023. Available from: https://www.worldometers.info/coronavirus/.
3. Watson OJ, Barnsley G, Toor J, Hogan AB, Winskill P, Ghani AC. Global impact of the first year of COVID-19 vaccination: a mathematical modelling study. Lancet Infect Dis. 2022;22(9):1293–1302. doi:10.1016/S1473-3099(22)00320-6
4. Wise J. Covid-19: WHO declares end of global health emergency. BMJ. 2023;381:p1041.
5. Elengoe A. COVID-19 Outbreak in Malaysia. Osong Public Health Res Perspect. 2020;11(3):93–100. doi:10.24171/j.phrp.2020.11.3.08
6. Hashim JH, Adman MA, Hashim Z, Mohd Radi MF, Kwan SC. COVID-19 epidemic in Malaysia: epidemic progression, challenges, and response. Front Public Health. 2021;9:560592. doi:10.3389/fpubh.2021.560592
7. Shah AUM, Safri SNA, Thevadas R, et al. COVID-19 outbreak in Malaysia: actions taken by the Malaysian government. Int J Infect Dis. 2020;97:108–116. doi:10.1016/j.ijid.2020.05.093
8. D-L-C N, Gan -G-G, Chai C-S, et al. The willingness of parents to vaccinate their children younger than 12 years against COVID-19: a cross-sectional study in Malaysia. BMC Public Health. 2022;22(1):1265. doi:10.1186/s12889-022-13682-z
9. The Star. Malaysia will transition into endemic phase from April 1 2022; 2022. Available from: https://www.thestar.com.my/news/nation/2022/03/08/pm-msia-will-enter-endemic-phase-from-april-1.
10. Ministry of Health Malaysia. National COVID-19 testing strategy; 2021. Available from: https://covid-19.moh.gov.my/reopeningsafely/nts/MOH_NTS_22112021_EN_v2.pdf.
11. Medical Devices Authority. Conditional approval list of covid - 19 Test Kit (For Self Test); 2022. Available from: https://mda.gov.my/announcement/1144-conditional-approval-list-of-covid-19-test-kit-for-self-test.html.
12. Grispen JE, Ickenroth MH, de Vries NK, Dinant GJ, Ronda G, van der Weijden T. Improving behaviour in self-testing (IBIS): study on frequency of use, consequences, information needs and use, and quality of currently available consumer information (protocol). BMC Public Health. 2010;10:453. doi:10.1186/1471-2458-10-453
13. Ronda G, Portegijs P, Dinant G-J, Buntinx F, Norg R, van der Weijden T. Use of diagnostic self-tests on body materials among Internet users in the Netherlands: prevalence and correlates of use. BMC Public Health. 2009;9(1):100. doi:10.1186/1471-2458-9-100
14. Ryan A, Ives J, Wilson S, Greenfield S. Why members of the public self-test: an interview study. Fam Pract. 2010;27(5):570–581. doi:10.1093/fampra/cmq043
15. Ickenroth MHP, Ronda G, Grispen JEJ, Dinant G-J, de Vries NK, van der Weijden T. How do people respond to self-test results? A cross-sectional survey. BMC Family Practice. 2010;11(1):77. doi:10.1186/1471-2296-11-77
16. Mina MJ, Parker R, Larremore DB. Rethinking Covid-19 Test Sensitivity — a Strategy for Containment. N Engl J Med. 2020;383(22):e120. doi:10.1056/NEJMp2025631
17. Goggolidou P, Hodges-Mameletzis I, Purewal S, Karakoula A, Warr T. Self-Testing as an Invaluable Tool in Fighting the COVID-19 Pandemic. J Prim Care Community Health. 2021;12:21501327211047782. doi:10.1177/21501327211047782
18. Boum Y, Eyangoh S, Okomo MC. Beyond COVID-19-will self-sampling and testing become the norm? Lancet Infect Dis. 2021;21(9):1194–1195. doi:10.1016/S1473-3099(21)00197-3
19. Alvarez E, Bielska IA, Hopkins S, et al. Limitations of COVID-19 testing and case data for evidence-informed health policy and practice. Health Res Policy Syst. 2023;21(1):11. doi:10.1186/s12961-023-00963-1
20. Abdul Rashid MR, Syed Mohamad SN, Tajjudin AIA, et al. COVID-19 pandemic fatigue and its sociodemographic, mental health status, and perceived causes: a cross-sectional study nearing the transition to an endemic phase in Malaysia. Int J Environ Res Public Health. 2023;20(5):4476. doi:10.3390/ijerph20054476
21. Charan J, Biswas T. How to calculate sample size for different study designs in medical research? Indian J Psychol Med. 2013;35(2):121–126. doi:10.4103/0253-7176.116232
22. World Health Organisation. Antigen-detection in the diagnosis of SARS-CoV-2 infection; 2021. Available from: https://apps.who.int/iris/handle/10665/345948.
23. Embrett M, Sim SM, Caldwell HAT, et al. Barriers to and strategies to address COVID-19 testing hesitancy: a rapid scoping review. BMC Public Health. 2022;22(1):750. doi:10.1186/s12889-022-13127-7
24. Xu J, Kerr L, Jiang Y, et al. Rapid Antigen Diagnostics as Frontline Testing in the COVID-19 Pandemic. Small Science. 2022;2(8):2200009. doi:10.1002/smsc.202200009
25. New Straits Times. Perform Covid-19 TRIIS pre- and post-travel, after attending gatherings; 2022. Available from: https://www.nst.com.my/news/nation/2022/02/768702/perform-covid-19-triis-pre-and-post-travel-after-attending-gatherings.
26. New Straits Times. WHO: take Covid-19 self-test before heading back to hometown; 2023. Available from: https://www.nst.com.my/news/nation/2023/04/901743/who-take-covid-19-self-test-heading-back-hometown.
27. The Star. Covid-19 caution: test weekly and treat quickly; 2023. Available from: https://www.thestar.com.my/lifestyle/health/2023/04/16/covid-19-caution-test-weekly-and-treat-quickly.
28. Che Sulaiman NF, Sanusi NA, Muhamad S. Survey dataset of Malaysian perception on rising cost of living. Data Brief. 2020;28:104910. doi:10.1016/j.dib.2019.104910
29. Lu Z, Fu L, Yang L, et al. Hesitancy to Undergo SARS-CoV-2 rapid antigen testing in china: nationwide cross-sectional study. JMIR Public Health Surveill. 2023;9:e43555. doi:10.2196/43555
30. Brumwell AN, Babatunde GB, Wilson MW, et al. Values of COVID-19 Self-Testing among Urban and Rural South Africans: a cross-sectional survey. Prev Med Rep. 2023;32:102114. doi:10.1016/j.pmedr.2023.102114
31. Folayan M, Shilton S, Undelikwo V, et al. People’s willingness to use COVID-19 self-testing in Nigeria: a cross-sectional survey. BMJ Open. 2023;13(1):e063323. doi:10.1136/bmjopen-2022-063323
32. Manguro G, Shilton S, Omenda S, et al. Are Kenyans likely to use COVID-19 self-testing kits? Results from a cross-sectional survey. Int J Public Health. 2022;67:1604918. doi:10.3389/ijph.2022.1604918
33. Jairoun AA, Al-Hemyari SS, Abdulla NM, et al. Knowledge about, acceptance of and willingness to use over-The-counter COVID-19 self-testing kits. J Pharm Health Serv Res. 2022;13(4):370–377. doi:10.1093/jphsr/rmac037
34. Thomas C, Shilton S, Thomas C, et al. Values and preferences of the general population in Indonesia in relation to rapid COVID-19 antigen self-tests: a cross-sectional survey. Trop Med Int Health. 2022;27(5):522–536. doi:10.1111/tmi.13748
35. Martínez-Pérez GZ, Shilton S, Saruê M, et al. Self-testing for SARS-CoV-2 in São Paulo, Brazil: results of a population-based values and attitudes survey. BMC Infect Dis. 2022;22(1):720. doi:10.1186/s12879-022-07706-7
36. New Straits Times. Change and adapt for another new normal; 2022. Available from: https://www.nst.com.my/opinion/letters/2022/03/780375/change-and-adapt-another-new-normal.
37. Nikoloski Z, Bain R, Elzalabany MK, et al. Modelling COVID-19 vaccination status and adherence to public health and social measures, Eastern Mediterranean Region and Algeria. Bull World Health Organ. 2023;101(2):111–120. doi:10.2471/BLT.22.288655
38. Becker MH. The health belief model and personal health behavior. Health Educ Monogr. 1974;2:324–473. doi:10.1177/109019817400200407
39. Bourassa KJ, Sbarra DA, Caspi A, Moffitt TE. Social distancing as a health behavior: county-level movement in the United States during the COVID-19 pandemic is associated with conventional health behaviors. Ann Behav Med. 2020;54(8):548–556. doi:10.1093/abm/kaaa049
40. Deeks A, Lombard C, Michelmore J, Teede H. The effects of gender and age on health related behaviors. BMC Public Health. 2009;9(1):213. doi:10.1186/1471-2458-9-213
41. Galasso V, Pons V, Profeta P, Becher M, Brouard S, Foucault M. Gender differences in COVID-19 attitudes and behavior: panel evidence from eight countries. Proc Natl Acad Sci USA. 2020;117(44):27285–27291. doi:10.1073/pnas.2012520117
42. Zajacova A, Lawrence EM. The relationship between education and health: reducing disparities through a contextual approach. Annu Rev Public Health. 2018;39:273–289. doi:10.1146/annurev-publhealth-031816-044628
43. Jaafar N, Perialathan K, Krishnan M, et al. Malaysian health literacy: scorecard performance from a national survey. Int J Environ Res Public Health. 2021;18(11):5813. doi:10.3390/ijerph18115813
44. Nwaozuru U, Obiezu-Umeh C, Diallo H, et al. Perceptions of COVID-19 self-testing and recommendations for implementation and scale-up among Black/African Americans: implications for the COVID-19 STEP project. BMC Public Health. 2022;22(1):1220. doi:10.1186/s12889-022-13619-6
45. Thomas C, Shilton S, Thomas C, Iye CM, Martínez-Pérez GZ. COVID-19 self-testing, a way to “live side by side with the coronavirus”: results from a qualitative study in Indonesia. PLOS Glob Public Health. 2022;2(10):e0000514. doi:10.1371/journal.pgph.0000514
46. Johnson NF, Velásquez N, Restrepo NJ, et al. The online competition between pro- and anti-vaccination views. Nature. 2020;582(7811):230–233. doi:10.1038/s41586-020-2281-1
47. Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol. 2023;21(3):133–146. doi:10.1038/s41579-022-00846-2
48. Maciuszek J, Polak M, Stasiuk K, Doliński D. Active pro-vaccine and anti-vaccine groups: their group identities and attitudes toward science. PLoS One. 2021;16(12):e0261648. doi:10.1371/journal.pone.0261648
49. The Sun Daily. Covid-19: isolation period reduced to five days from July 5, says Health Minister; 2023. Avaialble from: https://www.thesundaily.my/local/covid-19-isolation-period-shortened-to-five-days-from-july-5-dr-zaliha-BH11167314.
50. Chai C-S, D-L-C N, Chua W-J, et al. Knowledge, attitude, and practices among the general population during the later stage of the COVID-19 pandemic in Malaysia: a cross-sectional study. Risk Manag Healthc Policy. 2022;15:389–401. doi:10.2147/RMHP.S349798
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Willingness to receive the COVID-19 vaccine and associated factors among residents of Southwestern Ethiopia: A cross-sectional study
Jabessa D, Bekele F
Patient Preference and Adherence 2022, 16:1177-1185
Published Date: 3 May 2022
Analysis on the Selection of Herbs in TCM COVID-19 Treatment Protocols Between Malaysia and China
Wang X, Wang J, Pang F
International Journal of General Medicine 2023, 16:3655-3663
Published Date: 21 August 2023