")
Back to Journals » International Journal of General Medicine » Volume 15
Public Awareness of Alzheimer’s Disease: A Cross-Sectional Study from Saudi Arabia
Authors Alorfi NM
Received 14 June 2022
Accepted for publication 12 August 2022
Published 28 September 2022 Volume 2022:15 Pages 7535—7546
DOI https://doi.org/10.2147/IJGM.S373447
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Nasser M Alorfi
Department of Pharmacology and Toxicology, College of Pharmacy, Umm Al-Qura University, Makkah, Saudi Arabia
Correspondence: Nasser M Alorfi, Department of Pharmacology and Toxicology, College of Pharmacy, Umm Al-Qura University, Makkah, Saudi Arabia, Tel +966500644261, Email [email protected]
Background: Alzheimer’s disease is considered the most common neurodegenerative and progressive illness. It is also a common type of dementia characterized by brain atrophy, neuronal tissue loss, and the formation of amyloid plaques. Mild memory loss is a commonly expected start of the disease, which can progress to loss of capacity to carry on a conversation and react to certain situations.
Objective: This study aimed to measure knowledge about Alzheimer’s disease in Saudi Arabia through the use of the Alzheimer’s Disease Knowledge Scale (ADKS) and measure the association between the ADKS with relevant demographic variables.
Methods: A pre-validated questionnaire containing 30 questions was distributed electronically to anyone older than 18 years old living in Saudi Arabia. Items regarding socio-demographic characteristics and the Alzheimer’s Disease Knowledge Scale (ADKS) were also included.
Results: Participants did not have a high enough mean score to be regarded as appropriately knowledgeable (mean = 17.35). Higher knowledge scores on Life impact, Risk factors, Assessment and diagnosis, Caregiving, Treatment and management, and ADKS were associated with the female gender. Higher knowledge of caregiving was associated with a postgraduate academic qualification. Higher knowledge on Assessment and Diagnosis was associated with higher age. Higher knowledge on risk factors was associated with having relatives diagnosed with Alzheimer’s disease. Higher knowledge on life impact was associated with having newspaper and journal articles as the source of medical information.
Conclusion: National awareness campaigns for the community and continuing education courses for caregivers must be placed to aid in increasing awareness regarding Alzheimer’s disease.
Keywords: Alzheimer’s, dementia, neurodegenerative diseases, knowledge, awareness
Introduction
The most prevalent neurodegenerative disorder, Alzheimer’s disease (AD), is characterized by the loss of neuronal tissue, the formation of amyloid plaques in the brain, and the emergence of neurofibrillary tangles within neurons, leading to brain atrophy, cognitive impairment, and ongoing neurodegeneration.1,2 AD is a type of dementia that progresses at a fast rate with increasing age, family history, and as a result of traumatic brain damage.3–6 Specifically, advancing age is the most well-known of all the aforementioned risk factors for Alzheimer’s disease.7
The exact etiology and pathophysiology behind Alzheimer’s disease remain not fully understood, and the condition is still considered to be incurable.8 As such, there is no cure for Alzheimer’s disease currently available. However, certain medications can slow symptoms’ worsening, such as Cholinesterase inhibitors, N-methyl-D-aspartate (NMDA) receptor antagonists, and selective serotonin reuptake inhibitors (SSRI).9,10
Memory impairment, cognitive decline, disorientation, and generalized confusion are the major clinical symptoms, with reduced free recall that does not improve with cueing and indications of social or occupational function disruption.11–13 Several warning signs are associated with AD such as language difficulties, sleep disturbance, personality changes, and progressive changes in mood.14,15
Alzheimer’s disease is responsible for over two-thirds of incidences of progressive cognitive decline in the geriatric population in Saudi Arabia, in which a total prevalence of AD accounts to approximately 130.000.16 Since Alzheimer’s is a prevalent neurodegenerative disorder, it is supposed necessary that the general population are knowledgeable about the said condition; however, awareness of its etiology, pathophysiology, risk factors, assessment, diagnosis, and symptoms has not yet been assessed using a thorough scientific approach. As such, this study aimed to measure knowledge about AD in Saudi Arabia through the use of the ADKS, as well as to measure the association between the ADKS with relevant demographic variables.
Methodology
A cross-sectional research design was employed in this study in which a self-administered ADKS questionnaire was distributed electronically and sent via emails and via other social media to the population. Eligible participants in this study include those above 18 years old and those residing in Saudi Arabia. On the other hand, unqualified participants include those living outside the kingdom. The study took place in April-May 2020.
Informed consent forms were also distributed before data collection, noting that the responses from participants would be treated with the greatest confidentiality and that participants have the option to withdraw at any moment throughout the survey. Furthermore, this study was approved by the biomedical research ethics committee of Umm Alqura University (Approval No. HAPO-02-K-012-2022-04-1058).
Statistical Methodology
IBM SPSS version 23 (IBM Corp., Armonk, N.Y., USA) was used to analyze the results of this study. The characteristics of the research variables were defined using simple descriptive statistics in the form of counts and percentages as well as in the form of mean and standard deviations for categorical and nominal variables and continuous variables, respectively.
Instrumentation
This study adopted the use of the Alzheimer’s Disease Knowledge Scale (ADKS) questionnaire containing 30-items and employing a true or false scale format.17 The translated version was used in Arabic language. It would take approximately five to ten minutes to complete. Risk factors, evaluation and diagnosis, symptoms, course, life effect, caregiving, and therapy and management are the seven subdomains covered under this questionnaire. These subdomains, together with the primary domain were calculated by using a simple additive method. Furthermore, several preliminary findings substantiate that the ADKS questionnaire has sufficient reliability with test-retest and internal consistency, as well as adequate content, predictive, concurrent, and convergent validity.
Under the Life Impact subdomain, the following questions were included: (1) People with Alzheimer’s disease are particularly prone to depression, (2) Most people with Alzheimer’s disease live in nursing homes, and (3) it is safe for people with Alzheimer’s disease to drive, as long as they have a companion in the car at all times. Under Risk Factors, the following questions were included: (1) It has been scientifically proven that mental exercise can prevent a person from getting Alzheimer’s disease, (2) People in their 30s can have Alzheimer’s disease, (3) Having high cholesterol may increase a person’s risk of developing Alzheimer’s disease, (4) Prescription drugs that prevent Alzheimer’s disease are available, (5) Having high blood pressure may increase a person’s risk of developing Alzheimer’s disease, and (6) Genes can only partially account for the development of Alzheimer’s disease. Under the Course subdomain, the following questions were included: (1) After symptoms of Alzheimer’s disease appear, the average life expectancy is 6 to 12 years, (2) In rare cases, people have recovered from Alzheimer’s disease, (3) A person with Alzheimer’s disease becomes increasingly likely to fall down as the disease gets worse, (4) Eventually, a person with Alzheimer’s disease will need 24-hour supervision. Under Assessment and Diagnosis, the following questions were included: (1) When a person with Alzheimer’s disease becomes agitated, a medical examination might reveal other health problems that caused the agitation, (2) If trouble with memory and confused thinking appears suddenly, it is likely due to Alzheimer’s disease, (3) Symptoms of severe depression can be mistaken for symptoms of Alzheimer’s disease, and (4) Alzheimer’s disease is one type of dementia. Under Caregiving, the following questions are included: (1) People with Alzheimer’s disease do best with simple instructions given one step at a time, (2) When people with Alzheimer’s disease begin to have difficulty taking care of themselves, caregivers should take over right away, (3) If a person with Alzheimer’s disease becomes alert and agitated at night, a good strategy is to try to make sure that the person gets plenty of physical activity during the day, (4) When people with Alzheimer’s disease repeat the same question or story several times, it is helpful to remind them that they are repeating themselves, and (5) Once people have Alzheimer’s disease, they are no longer capable of making informed decisions about their own care. Under Treatment and management, the following questions are included: (1) People whose Alzheimer’s disease is not yet severe can benefit from psychotherapy for depression and anxiety, (2) Poor nutrition can make the symptoms of Alzheimer’s disease worse, (3) When a person has Alzheimer’s disease, using reminder notes is a crutch that can contribute to decline and (4) Alzheimer’s disease cannot be cured. Under Symptoms, the following questions are included: (1) Tremor or shaking of the hands or arms is a common symptom in people with Alzheimer’s disease, (2) Trouble handling money or paying bills is a common early symptom of Alzheimer’s disease, (3) One symptom that can occur with Alzheimer’s disease is believing that other people are stealing one’s things, and (4) Most people with Alzheimer’s disease remember recent events better than things that happened in the past.
An independent t-test and One-way ANOVA, with Least Significant Difference (LSD) as a post hoc test, were employed to demonstrate an association between the domains and demographical data represented by two group means and more than two groups, respectively. The standard distribution hypothesis was used in these analyses. A Pearson’s correlation coefficient was employed to correlate variables that were both represented by means. Welch’s t-test for two group means was employed as a backup. Finally, the null hypothesis was rejected if such p-value was less than 0.05.
Results
As seen in Table 1, a total of 575 responses were obtained in the study. It is important to note that the majority of the respondents were female (65.2%, n = 375), university graduates (67.7%, n = 389) and between the ages 18–25 (84.3%, n = 485). In addition, more than half of the individuals did not have any relatives diagnosed with Alzheimer’s disease (76.9%, n = 442) and got their medical information from health care providers (68.0%, n = 391).
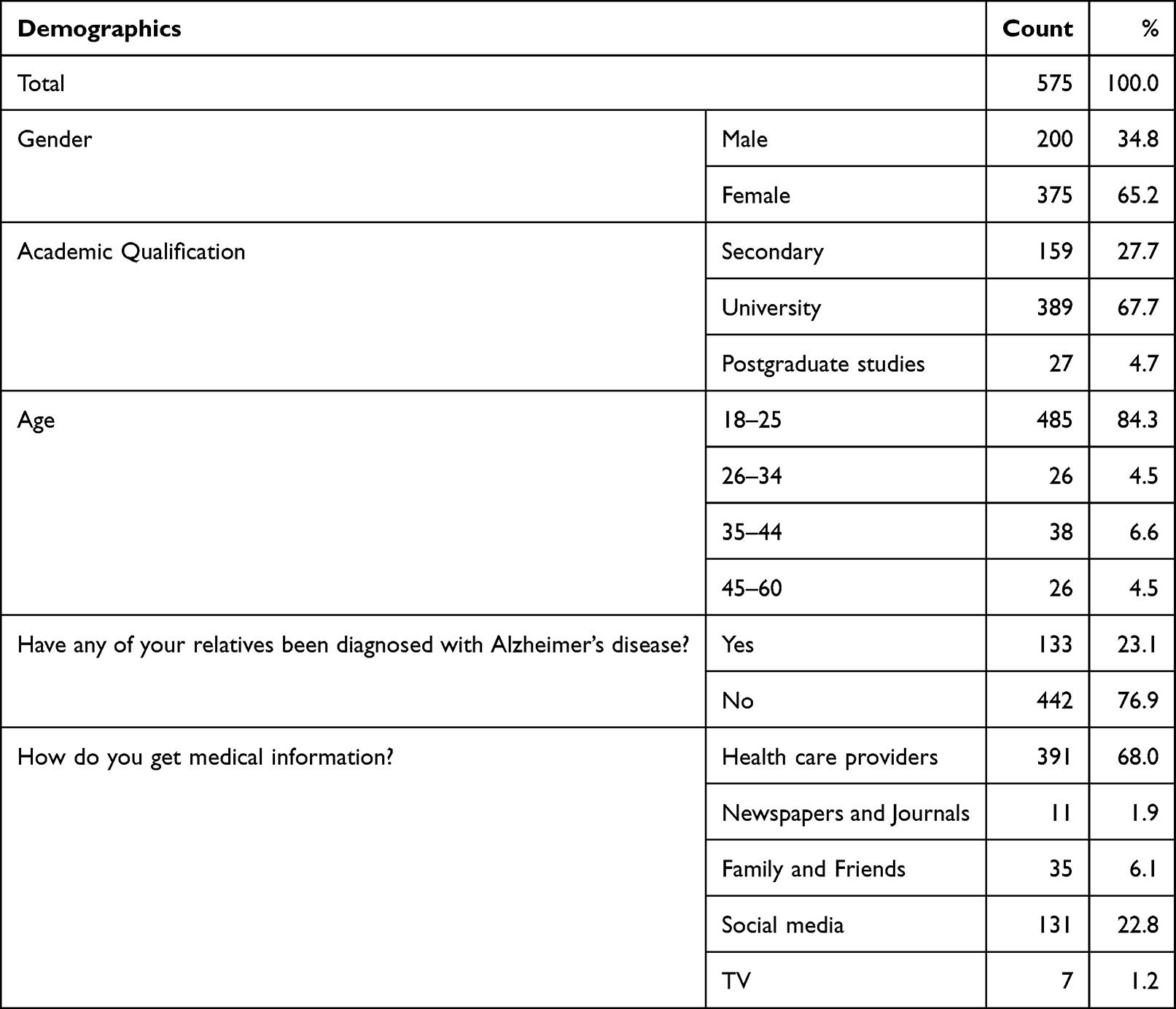 |
Table 1 Demographic Characteristics of the Study Population |
Table 2 presents the results of the Alzheimer’s Disease Knowledge Scale questionnaire, whereas Table 3 represents the percentage of correct responses. The majority of the responses were correct under the Life Impact subdomain wherein a relatively more significant portion of the respondents answered True to the item indicating that people with Alzheimer’s disease are particularly prone to depression (71.3%, n = 410), as well as answered False to the items stating that (1) most people with Alzheimer’s disease live in nursing homes (60.9%, n = 350) and (2) it is safe for people with Alzheimer’s disease to drive, as long as they have a companion in the car at all times (61.0%, n = 351).
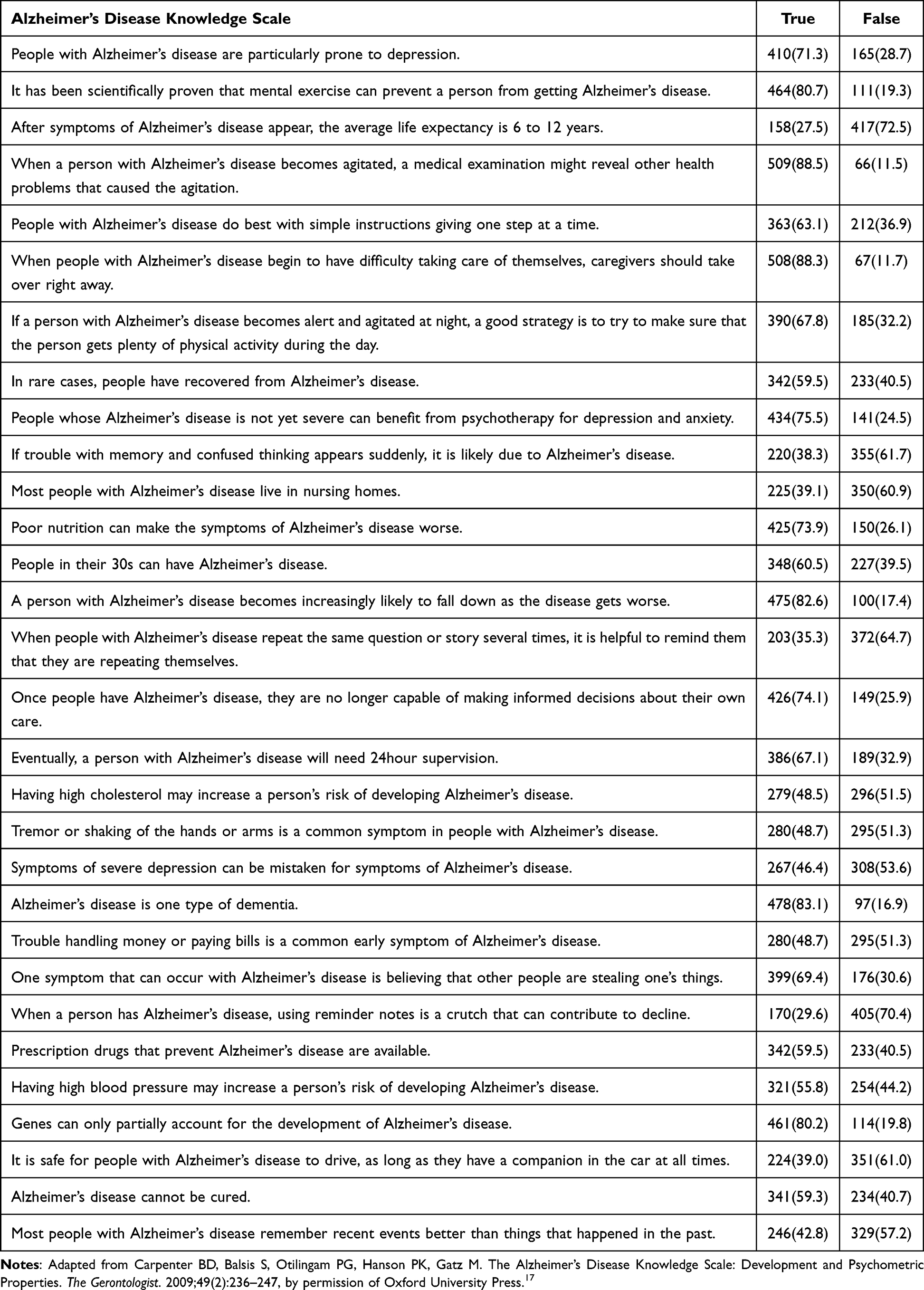 |
Table 2 Results of the Alzheimer’s Disease Knowledge Scale |
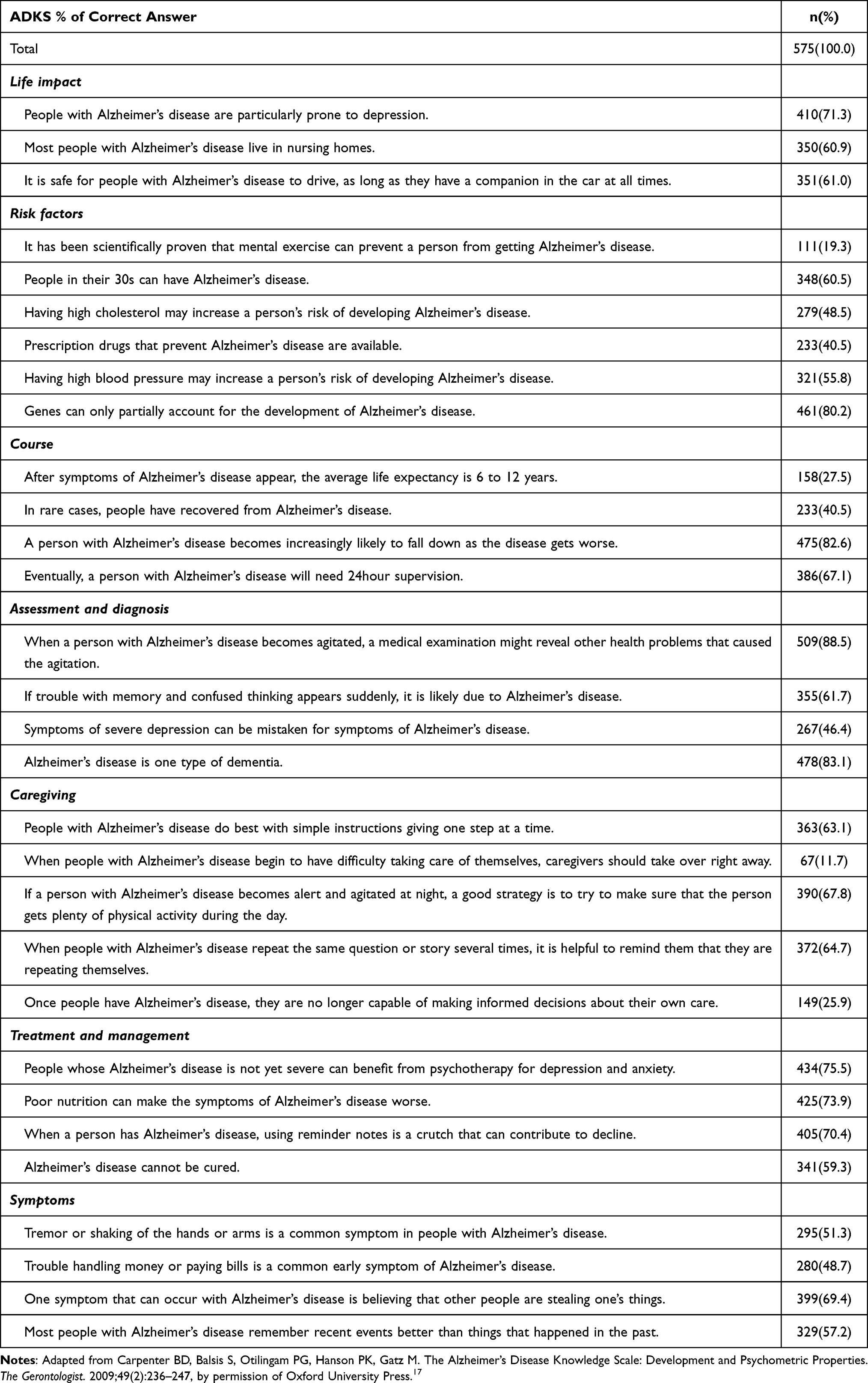 |
Table 3 Percentage of Correct Responses from the Alzheimer’s Disease Knowledge Scale Questionnaire |
Half of the items recorded under Risk Factors appeared to show that most of the respondents were correct. That is, a relatively large percentage of the respondents answered True to the items indicating that (1) people in their 30s can have Alzheimer’s disease (60.5%, n = 348), (2) having high blood pressure may increase a person’s risk of developing Alzheimer’s disease (55.8%, n = 321), and (3) genes can only partially account for the development of Alzheimer’s disease (80.2%, n = 461). Meanwhile, the other 50% of the items under the same subdomain appeared to show that substantially less than half of the respondents were correct in answering False to the items indicating that (1) it has been scientifically proven that mental exercise can prevent a person from getting Alzheimer’s disease (19.3%, n =111), and that (2) Prescription drugs that prevent Alzheimer’s disease are available, as well as in answering True to the item indicating that having high cholesterol may increase a person’s risk of developing Alzheimer’s disease (48.5%, n = 279).
More than half of the items under the Course subdomain appeared to show that the majority of the respondents were correct in answering True to the statements indicating that (1) a person with Alzheimer’s disease becomes increasingly likely to fall down as the disease gets worse (82.6%, n = 475) and (2) eventually, a person with Alzheimer’s disease will need 24-hour supervision (67.1%, n = 386). On the contrary, substantially lower correct responses were recorded in the remaining two items, in which respondents answered True to the item indicating that the average life expectancy is 6 to 12 years, after the appearance of the symptoms of Alzheimer’s disease (27.5%, n = 158), as well as answered False to the item indicating that people have recovered from Alzheimer’s disease, in rare cases (40.5%, n = 233).
Similarly, more than half of the responses under the Assessment and Diagnosis subdomain showed that the majority of the participants were correct in answering True to the items indicating that (1) a medical examination might reveal other health problems that could have caused agitation in a patient with Alzheimer’s disease (88.5%, n = 509) and that (2) Alzheimer’s disease is one type of dementia (83.1%, n = 478), as well as in answering False to the item indicating that if trouble with memory and confused thinking appears suddenly, it is likely due to Alzheimer’s disease (61.7%, n = 355). On the other hand, less than half of the respondents were correct in answering True to the item, indicating that the symptoms of severe depression can be mistaken for symptoms of Alzheimer’s disease (46.4%, n = 267).
Under the subdomain, Caregiving, the majority of the respondents were correct in answering True to the statements indicating that (1) People with Alzheimer’s disease do best with simple instructions given one step at a time (63.1%, n = 363), and that (2) if a person with Alzheimer’s disease becomes alert and agitated at night, a good strategy is to try to make sure that the person gets plenty of physical activity during the day (67.8%, n = 390) as well in answering False to the item indicating that when people with Alzheimer’s disease repeat the same question or story several times, it is helpful to remind them that they are repeating themselves (64.7%, n = 372). On the other hand, the minority of the respondents were correct in answering False to the statements indicating that (1) caregivers should take over right away when people with Alzheimer’s disease begin to have difficulty taking care of themselves (11.7%, n = 67), ad that (2) once people have Alzheimer’s disease, they are no longer capable of making informed decisions about their own (25.9%, n = 149).
In terms of the Treatment and management subdomain, the majority of the respondents were correct in answering True to the following items: (1) People whose Alzheimer’s disease is not yet severe can benefit from psychotherapy for depression and anxiety (75.5%, n = 434), (2) Poor nutrition can make the symptoms of Alzheimer’s disease worse (73.9%, n = 425), and (3) Alzheimer’s disease cannot be cured n = 59.3%, n = 341). The majority of the respondents were also correct in answering False to the item indicating that using reminder notes is a crutch that can contribute to decline when a person has Alzheimer’s disease (70.4%, n = 405).
With regards to the Symptom subdomain, the majority of the respondents were correct in answering True to the statements indicating that (1) one symptom that can occur with Alzheimer’s disease is believing that other people are stealing one’s things (69.4%, n = 399) and that (2) trouble handling money or paying bills is a common early symptom of Alzheimer’s disease (48.7%, n = 280). Likewise, the majority of the respondents were correct in answering False to the items indicating that (1) most people with Alzheimer’s disease remember recent events better than things that happened in the past (57.2%, n = 329) and that (2) tremor or shaking of the hands or arms is a common symptom in people with Alzheimer’s disease (51.3%, n = 295).
Table 4 shows the mean scores for the subdomains namely, life Impact (μ = 1.93, sd = 0.9), risk factors (μ = 3.05, sd = 1.2), course (μ = 2.18, sd = 0.9), assessment and diagnosis (μ = 2.80, sd = 0.8), caregiving (μ = 2.33, sd = 1.0), treatment and management (μ = 2.79, sd = 0.9), symptoms (μ = 2.27, sd = 0.9), as well as the main domain, Alzheimer’s Disease Knowledge Scale (μ = 17.35, min = 8, max = 27, sd = 3.1).
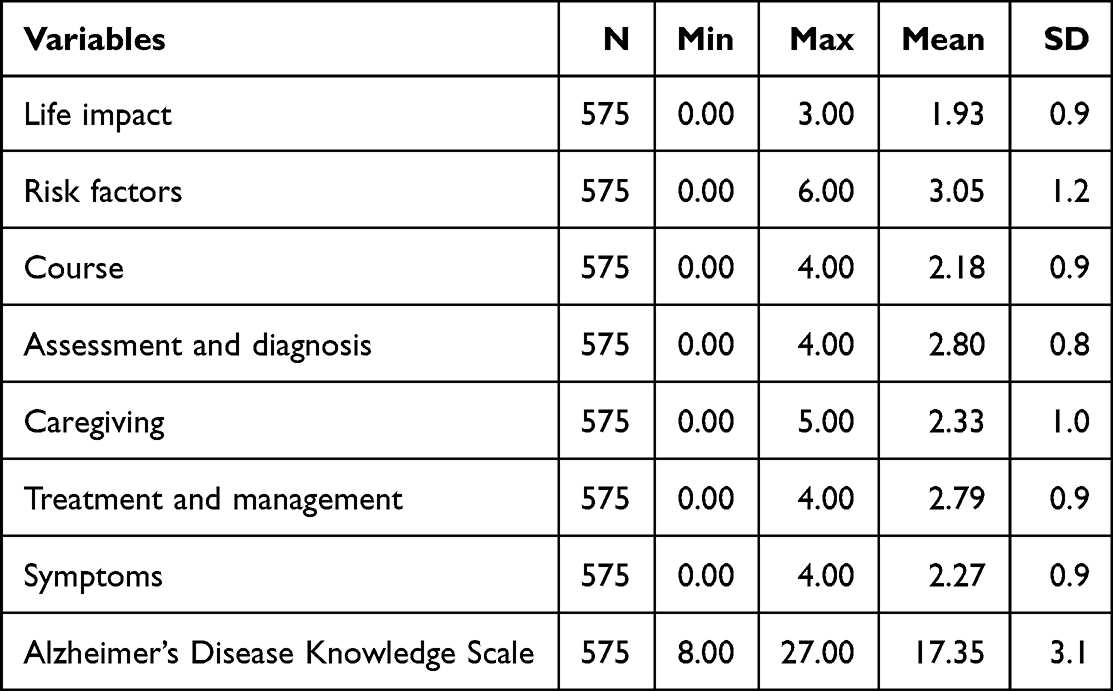 |
Table 4 Mean Scores per Sub-Domain |
Table 5 presents the correlations between the Alzheimer’s Disease Knowledge Scale and its subdomains as well as the correlation between each subdomain. Interestingly, the Alzheimer’s Disease Knowledge Scale was determined to be significantly associated with all of the indicated subdomains namely, (1) Life impact (p value = <0.001), (2) Risk factors (p value = <0.001), (3) Course (p value = <0.001), (4) Assessment and diagnosis (p value = <0.001), (5) Caregiving (p value = <0.001), (6) Treatment and management (p value = <0.001), and (7) Symptoms (p value = <0.001).
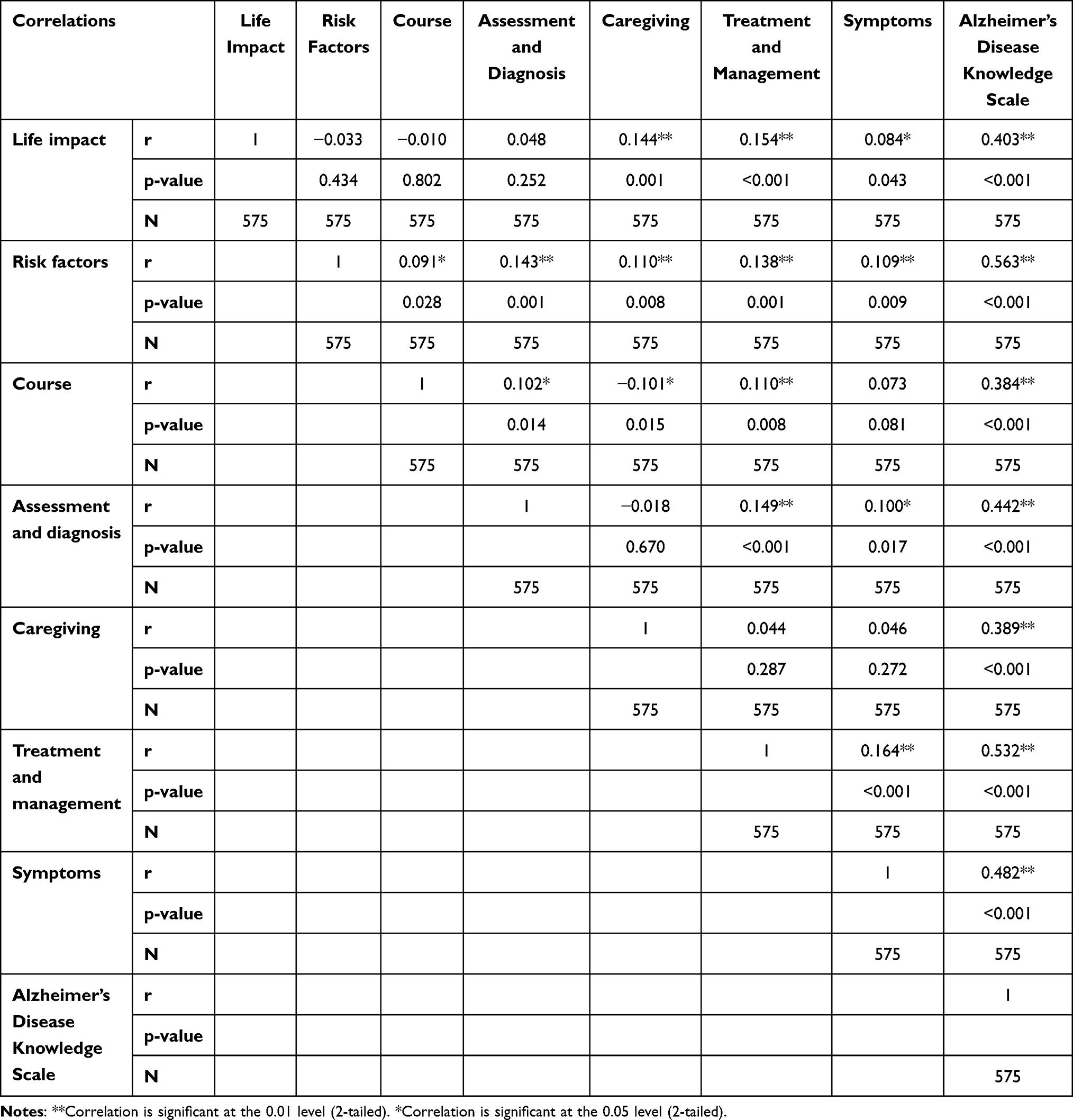 |
Table 5 Correlations Between Alzheimer’s Disease Knowledge Scale and Its Subdomains |
Significant associations were determined between Life Impact and the following subdomains: (1) Caregiving (p value = 0.001), (2) Treatment and Management (p value = <0.001), and (3) Symptoms (p value = 0.043). Risk Factors was also found to have a significant association with (1) Course (p value = 0.028), (2) Assessment and Diagnosis (p value = 0.001), (3) Caregiving (p value = 0.008), (4) Treatment and Management (p value = 0.001) and (5) Symptoms (p value = 0.009); meanwhile, Course was determined to have a significant association with (1) Assessment and Diagnosis (p value = 0.014), (2) Caregiving (p value = 0.015), and (3) Treatment and management (p value =0.008). In line with this, a significant association was found between Assessment and Diagnosis and the following subdomains: (1) Treatment and management (p value = <0.001) and (2) Symptoms (p value = 0.017). Lastly, Treatment and management also showed a significant association with Symptoms (p value <0.001).
Table 6 reveals that having a female gender was significantly associated with higher knowledge scores in terms of Life impact (p value = 0.006), Risk factors (p value = 0.021), Assessment and diagnosis (p value = 0.001), Caregiving (p value = 0.003), Treatment and management (p value = <0.001), as well as the overall in the ADKS (p value = <0.001). It was also revealed that having a postgraduate academic qualification was significantly associated with more knowledge on Caregiving (p value = 0.047). Knowledge the Assessment and Diagnosis of the disease increases with advancing age (p value = 0.045). Meanwhile, having relatives diagnosed with Alzheimer’s disease was also found to be associated with more knowledge on risk factors (p value = 0.019). Lastly, having newspaper and journal articles as the source of medical information was found to be associated with the knowledge on life impact (p value = 0.033).
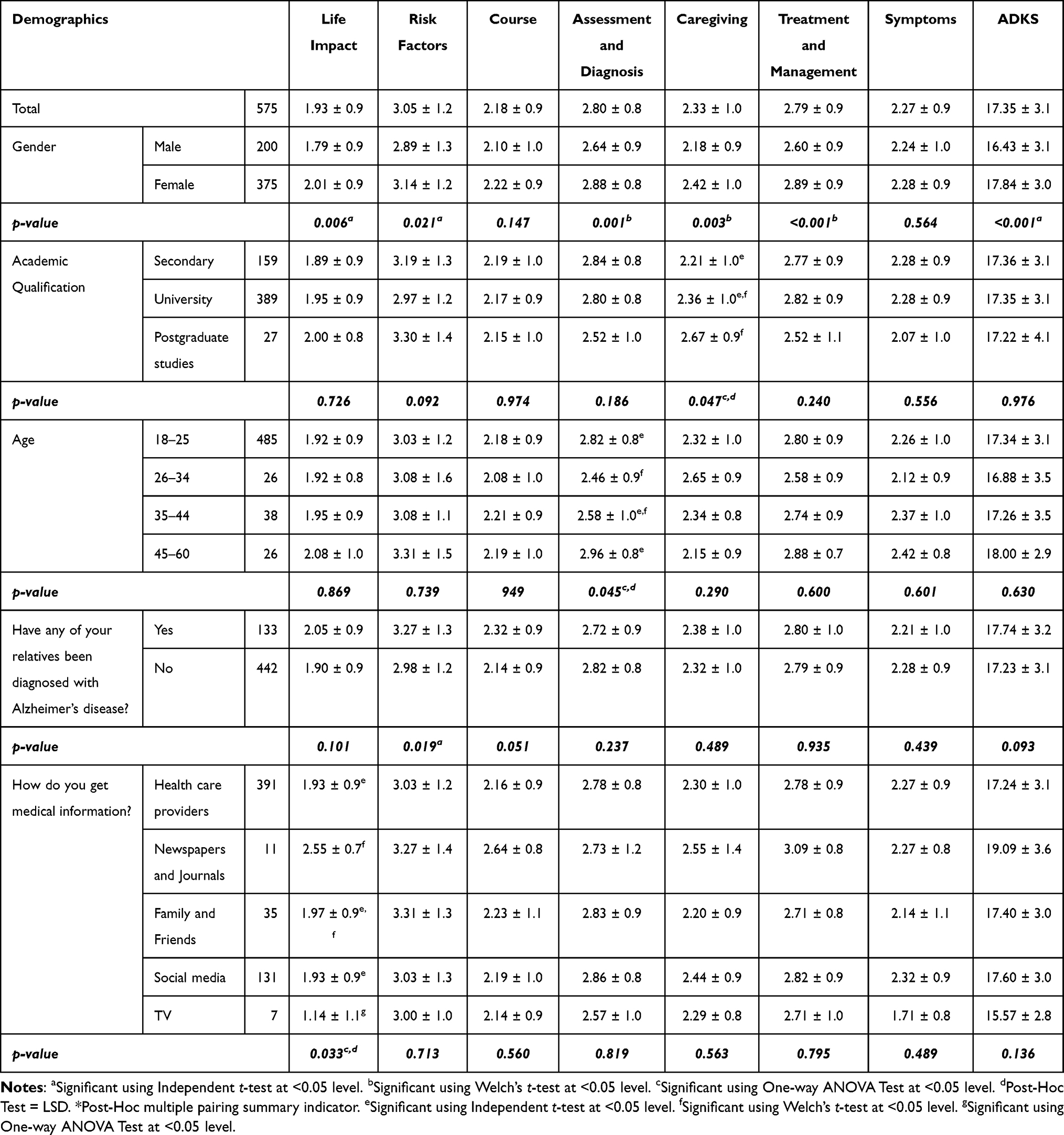 |
Table 6 Association of the Demographic Characteristics of the Sample with the Alzheimer’s Disease Knowledge Scale and Its Subdomains |
Discussion
This research is considered to be the first investigation of the general Saudi population’s knowledge regarding Alzheimer’s disease on the basis of the Alzheimer’s Disease Knowledge Scale questionnaire. While there are a lot of studies tackling Alzheimer’s Disease Knowledge within Saudi Arabia, no one has used this tool. All the articles were created in validated questionnaires based on authors’ expertise. The psychometric properties of the ADSK scales were analyzed in different languages and to evaluate the effectiveness of educational interventions among caregivers, health-care professionals, and the general population.18,19
This study shows that the participants know enough about Alzheimer’s Disease with lowest and highest scores being 8.00 and 27.00, respectively, and with a mean score of 17.35 out of 30 (Table 4). The sample, however, does not have a high enough mean score to be regarded as appropriately knowledgeable. This is consistent with the findings of a Malaysian study employing the ADKS in which a mean score of 18.5 and 19.05 out of 30 was revealed from pharmacists in public hospitals and health clinics, respectively20 Meanwhile, an Australian study which also assessed health professionals revealed a mean score of 23.6.21 This mean score is relatively higher than the present study’s findings, which could be attributable to the fact that healthcare professionals were not identified in the study.
Associations between the subdomains were also established in this study; that is, Life Impact was found to be associated with Caregiving, Treatment and Management, and Symptoms; Risk Factors were found to be associated with Course, Assessment and Diagnosis, Caregiving, Treatment and Management, and Symptoms; Course was found to be associated with Assessment and Diagnosis, Caregiving and Treatment and management; Assessment and Diagnosis was found to be associated with Treatment and management and Symptoms; lastly, Treatment and management were found to be associated with Symptoms. Since the intervention for Alzheimer’s Disease is multidisciplinary, it is worth noting that depending on these subdomains, the patient’s well-being would be directly affected.22
Chinese study revealed that older and female participants had more retention of AD information relative to the male population.23 In contrast, a study in Nepal revealed no significant association between gender and the level of knowledge regarding Alzheimer’s disease.24 Moreover, the present study revealed that advancing age as well as having a postgraduate academic qualification was found to be significantly associated with more knowledge on Assessment and Diagnosis of the disease (p value = 0.045) and Caregiving (p value = 0.047), respectively. Interestingly, this finding shows an interesting similarity and contrast to the study conducted by Amado and Brucki in 2018.25 According to the results of the said study, having higher educational attainment and having a relatively younger age is linked to better awareness and higher knowledge with regards to AD diagnosis, management, and therapeutic interventions.
Furthermore, Amado and Brucki25 also demonstrated that even with relatives and caregivers of patients diagnosed with Dementia, there remains a persistent unawareness and limited knowledge concerning Alzheimer’s disease. Meanwhile, it was shown in the present study that more knowledge on risk factors (p value = 0.019) is associated with having relatives diagnosed with Alzheimer’s disease. Other study suggested that there is a need to increase the knowledge and attitude of the caregivers of people with dementia.26
As per the Ministry of Health, Saudi Arabia made a remarkable transformation to becoming recognized as a part of the Group 20 countries.27 In line with this, the recent years have paved way for several changes in the Saudi community, including the widespread use of the internet and social media, as well as a decline in the demand and attention placed on print-based information sources such as traditional books, commercial journals and newspapers28 with significant increase of scientific research.29 This is similar to the findings of the present study where it was substantiated that a relatively large portion of the respondents utilize social media to acquire medical information (N = 131). Meanwhile, newspapers and journal articles were found to be significantly associated with knowledge on life impact; hence it also remains to be an important source of medical information among the sample population (p value = 0.033). Additionally, with the existence of greater than five hundred hospitals in Saudi Arabia, a significant improvement in healthcare was observed. Hence, this could be a factor as to why the majority of the sample respondents acquire their medical knowledge from healthcare providers (N = 391).
With the significant association between ADKS and all its subdomains, determination of the knowledge gaps that must be bridged to increase the public’s understanding of the disease. Per subdomain, all of the mean scores exhibit greater than 50% correct responses except for the Caregiving category (max = 5.00, μ = 2.3). This is notable because the particular lack of knowledge on caregiving may potentially delay the consistency in terms of the management and interventions given among patients diagnosed with AD and hence affect their quality of life. Furthermore, it is recommended that efforts on calibrating standards and proliferating educational interventions must be placed on this subdomain as well as all other subdomains. This is to aid in increasing the awareness regarding Alzheimer’s Disease, especially for healthcare workers who are considered to be one of the major sources of healthcare information.30
Limitation
This study is among the few that have evaluated the level of knowledge regarding Alzheimer’s Disease in Saudi Arabia. While it depicts significant gaps in knowledge regarding the AD disease, it does not exclude the presence of response bias which is out of the researcher’s control. This study is also limited to making associations rather than establishing causation with a cross-sectional research design. Larger sample will provide more reliable results with greater precision and power. Nonetheless, the findings of this study would be relevant in advancing the current body of knowledge regarding Alzheimer’s Disease.
Conclusion
In this study, the following are revealed: female gender was significantly associated with higher knowledge on Life Impact, Risk Factors, Assessment and diagnosis, Caregiving, Treatment and management, as well as the overall in the ADKS; having a postgraduate academic qualification was associated with higher knowledge on Caregiving; higher age is associated with higher knowledge on the Assessment and Diagnosis of the disease; having relatives diagnosed with Alzheimer’s disease was associated with higher knowledge on risk factors; and lastly, having newspaper and journal articles as the source of medical information was associated with higher knowledge on life impact. National awareness campaigns for all parts of the community is essential to enhance the awareness about AD. Also, continuous educational courses to all health care providers must be placed to aid in increasing the awareness regarding AD nationally.
Ethical Consideration
This work was carried out following the guidelines for ethical scientific research at Umm Alqura University. Approval from the biomedical research ethics committee of Umm Alqura University (Approval No. HAPO-02-K-012-2022-04-1058) was obtained. This research was carried out in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki 2013) for experiments involving humans. Appropriate consents were secured from all studied subjects.
Acknowledgment
The author would like to express deepest appreciation to Professor Brian D Carpenter, Washington University in St Louis, USA, for his valuable support of this work.
Funding
This research received no external funding.
Disclosure
The author declares no conflicts of interest in relation to this work.
References
1. Aisen PS, Jimenez-Maggiora GA, Rafii MS, Walter S, Raman R. Early-stage Alzheimer disease: getting trial-ready. Nat Rev Neurol. 2022;2022:1–11.
2. Nordberg A. Towards early diagnosis in Alzheimer disease. Nat Rev Neurol. 2015;11(2):69–70. doi:10.1038/nrneurol.2014.257
3. Bendlin BB, Ries ML, Canu E, et al. White matter is altered with parental family history of Alzheimer’s disease. Alzheimers Dement. 2010;6(5):394–403. doi:10.1016/j.jalz.2009.11.003
4. Lye TC, Shores EA. Traumatic brain injury as a risk factor for Alzheimer’s disease: a review. Neuropsychol Rev. 2000;10(2):115–129. doi:10.1023/A:1009068804787
5. Masters CL, Bateman R, Blennow K, Rowe CC, Sperling RA, Cummings JL. Alzheimer’s disease. Nat Rev Dis Prim. 2015;1. doi:10.1038/nrdp.2015.56
6. Newman M, Nik HM, Sutherland GT, et al. Accelerated loss of hypoxia response in zebrafish with familial Alzheimer’s disease-like mutation of presenilin 1. Hum Mol Genet. 2020;29(14):2379–2394. doi:10.1093/hmg/ddaa119
7. Guerreiro R, Bras J. The age factor in Alzheimer’s disease. Genome Med. 2015;7(1):1–3. doi:10.1186/s13073-015-0232-5
8. Pan D, Zeng A, Jia L, Huang Y, Frizzell T, Song X. Early detection of Alzheimer’s disease using magnetic resonance imaging: a novel approach combining convolutional neural networks and ensemble learning. Front Neurosci. 2020;14:259. doi:10.3389/fnins.2020.00259
9. Massoud F, Léger GC. Pharmacological treatment of Alzheimer disease. Can J Psychiatry. 2011;56(10):579–588. doi:10.1177/070674371105601003
10. Long JM, Holtzman DM. Alzheimer disease: an update on pathobiology and treatment strategies. Cell. 2019;179(2):312–339. doi:10.1016/j.cell.2019.09.001
11. Castellani RJ, Rolston RK, Smith MA. Alzheimer disease. Dis Mon. 2010;56(9):484. doi:10.1016/j.disamonth.2010.06.001
12. Moore BA, Barnett JE. Oxford clinical psychology military psychologists ’ desk reference. Case Stud Clin Psychol Sci Bridg Gap. 2015;2015:1–7.
13. Odusami M, Maskeliūnas R, Damaševičius R. An intelligent system for early recognition of Alzheimer’s disease using neuroimaging. Sensors. 2022;22(3):740. doi:10.3390/s22030740
14. Szatloczki G, Hoffmann I, Vincze V, Kalman J, Pakaski M. Speaking in Alzheimer’s disease, is that an early sign? Importance of changes in language abilities in Alzheimer’s disease. Front Aging Neurosci. 2015;7:195. doi:10.3389/fnagi.2015.00195
15. He C, Hu Z, Jiang C. Sleep disturbance: an early sign of Alzheimer’s disease. Neurosci Bull. 2020;36(4):449–451. doi:10.1007/s12264-019-00453-x
16. Ministry of Health. Health days 2020 - World Alzheimer’s day; 2020. Available from: https://www.moh.gov.sa/en/HealthAwareness/healthDay/2020/Pages/HealthDay-2020-09-21.aspx.
17. Carpenter BD, Balsis S, Otilingam PG, Hanson PK, Gatz M. The Alzheimer’s disease knowledge scale: development and psychometric properties. Gerontologist. 2009;49(2):236–247. doi:10.1093/geront/gnp023
18. Leszko M, Carpenter BD. Reliability and validity of the Polish version of the Alzheimer’s disease knowledge scale. Dement Geriatr Cogn Disord. 2021;50(1):51–59. doi:10.1159/000514872
19. Prokopiadou D, Papadakaki M, Roumeliotaki T, et al. Translation and validation of a questionnaire to assess the diagnosis and management of dementia in Greek general practice. Eval Heal Prof. 2015;38(2):151–159. doi:10.1177/0163278712474988
20. Nuri THM, Hong YH, Ming LC, Joffry SM, Othman MF, Neoh CF. Knowledge on Alzheimer’s disease among public hospitals and health clinics pharmacists in the State of Selangor, Malaysia. Front Pharmacol. 2017;8:739. doi:10.3389/fphar.2017.00739
21. Smyth W, Fielding E, Beattie E, et al. A survey-based study of knowledge of Alzheimer’s disease among health care staff. BMC Geriatr. 2013;13(1):1–8. doi:10.1186/1471-2318-13-2
22. Zucchella C, Sinforiani E, Tamburin S, et al. The multidisciplinary approach to Alzheimer’s disease and dementia. A narrative review of non-pharmacological treatment. Front Neurol. 2018;9:1058. doi:10.3389/fneur.2018.01058
23. Sun F, Gao X, Shen H, Burnette D. Levels and correlates of knowledge about Alzheimer’s disease among older Chinese Americans. J Cross Cult Gerontol. 2014;29(2):173–183. doi:10.1007/s10823-014-9229-6
24. Baral K, Dahal M, Pradhan S. Knowledge regarding Alzheimer’s disease among college students of Kathmandu, Nepal. Int J Alzheimers Dis. 2020;2020. doi:10.1155/2020/6173217
25. Amado DK, Brucki SMD. Knowledge about Alzheimer’s disease in the Brazilian population. Arq Neuropsiquiatr. 2018;76(11):775–782. doi:10.1590/0004-282x20180106
26. Parveen S, Mehra A, Kumar K, Grover S. Knowledge and attitude of caregivers of people with dementia. Geriatr Gerontol Int. 2022;22(1):19–25. doi:10.1111/ggi.14304
27. Ministry of Health. Statistical yearbook - statistical yearbook; 2022. Available from: https://www.moh.gov.sa/en/Ministry/Statistics/Book/Pages/default.aspx.
28. Marar SD, Al-Madaney MM, Almousawi FH. Health information on social media. Saudi Med J. 2019;40(12):1294–1298. doi:10.15537/smj.2019.12.24682
29. Zaher WA, Meo SA, Almadi MA, Neel KF. Research productivity of health-care institutions of saudi government: ten-year based bibliometric analysis. J Nat Sci Med. 2018;1(1):13.
30. Wang Y, Xiao LD, Luo Y, Xiao SY, Whitehead C, Davies O. Community health professionals’ dementia knowledge, attitudes and care approach: a cross-sectional survey in Changsha, China. BMC Geriatr. 2018;18(1):1. doi:10.1186/s12877-018-0821-4
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.