Back to Journals » Risk Management and Healthcare Policy » Volume 19
Public-Access Defibrillation in Megacities: Structural Barriers and Systemic Opportunities in Shanghai, China
Received 6 January 2026
Accepted for publication 4 May 2026
Published 19 May 2026 Volume 2026:19 590419
DOI https://doi.org/10.2147/RMHP.S590419
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Keon-Hyung Lee
Yu Gao,1 Xin Zhou,1 Li Luo1,2
1Shanghai Institute of Infectious Disease and Biosecurity, Fudan University, Shanghai, People’s Republic of China; 2School of Public Health, Fudan University, Shanghai, People’s Republic of China
Correspondence: Li Luo, School of Public Health, Fudan University, Shanghai, People’s Republic of China, Email [email protected]
Background: Despite nationwide efforts to expand public-access defibrillation (PAD) in China, the use of automated external defibrillators (AEDs) remains extremely low. Although spatial disparities in AED deployment have been widely reported, less is known about the structural, procedural, and behavioral factors that hinder effective use in real-world emergencies. This study explored multilevel barriers and opportunities within Shanghai’s PAD system.
Methods: Guided by the Social Ecological Model, we conducted in-depth semi-structured interviews with 42 participants involved in AED financing, deployment, management, maintenance, training, digital platform development, and emergency response. Interviews were conducted between December 2024 and June 2025, with data transcription, checking, and preliminary analysis continuing until July 2025. Data were analyzed using inductive and deductive thematic analysis. Themes were organized across system, organizational, community, and individual levels.
Results: Shanghai’s PAD system is shaped by interacting barriers across multiple levels. At the individual level, limited emergency knowledge, fear of causing harm, and uncertainty about legal protection reduced bystanders’ willingness to act. At the organizational and system levels, fragmented governance, inconsistent maintenance standards, restricted venue access, non-standard signage, and disconnected digital platforms limited AED visibility, accessibility, and timely activation. At the same time, several opportunities emerged. High-willingness population groups could be targeted through scenario-based, recurrent training. Data-informed AED siting and hybrid fixed-plus-mobile deployment models using taxis or delivery riders may help reduce spatial inequities. Participants also highlighted the need for a centralized, government-led AED information platform linked to emergency dispatch and device management.
Conclusion: AED installation alone is insufficient to deliver effective PAD. In Shanghai, PAD performance is constrained less by device availability itself than by fragmented governance, weak system integration, and persistent behavioral barriers. Strengthening legal protection, improving cross-sector coordination, integrating AED information with dispatch systems, and promoting activation-oriented public training may help translate AED availability into lifesaving action.
Keywords: public-access defibrillation, automated external defibrillator, out-of-hospital cardiac arrest, qualitative research
Introduction
Out-of-hospital cardiac arrest (OHCA) is one of the most time-critical medical emergencies worldwide and is associated with high mortality and disability.1,2 In China, more than one million OHCA events are estimated to occur annually, yet the reported bystander cardiopulmonary resuscitation (CPR) rate is only 4.8%, and the survival-to-discharge rate is as low as 0.35%.3,4 Early cardiopulmonary resuscitation and defibrillation before the arrival of emergency medical services (EMS) can substantially improve survival after OHCA,5–7 and immediate defibrillation using an on-site automated external defibrillator (AED) has been associated with survival rates of 50–74% in shockable cases.8,9 For this reason, increasing AED availability in public settings has become a major strategy for strengthening the early links in the chain of survival.
Following growing evidence of the value of public-access defibrillation (PAD), the American Heart Association issued its first PAD recommendations in 1992,9 followed by the European Resuscitation Council in 1998.10 Since then, many countries have expanded AED deployment in locations considered at elevated risk of OHCA and have promoted community training in AED use. At the same time, subsequent studies have shown that many cardiac arrests occur in private residences and that limiting AED deployment to public places yields only modest rates of early defibrillation.11,12 This mismatch between where OHCAs occur and where AEDs are placed highlights that PAD effectiveness depends not only on device placement, but also on whether devices can be identified, accessed, retrieved, and used rapidly in real emergencies.
China released national guidelines for AED deployment in public places in 2021, relatively later than many high-income countries.13,14 Although AED deployment has accelerated in recent years, PAD utilization remains low, and real-world accessibility remains limited.13,14 This gap reflects not only differences in AED coverage, but also broader contextual factors, including variation in urban form, public-place characteristics, population density, governance arrangements, and sociocultural conditions. As a result, PAD strategies developed in high-income settings cannot be directly transferred to China without contextual adaptation.
Shanghai was among the first cities in China to introduce local policies supporting AED installation in public places and has made visible progress in expanding deployment since the release of the national guidelines.15 However, important questions remain about how AEDs are governed, distributed, signposted, maintained, located, retrieved, and activated in actual emergency situations. Existing international research offers valuable lessons, but much of that evidence comes from settings with more mature EMS systems, higher bystander CPR rates, and better-established maintenance and coordination mechanisms. In contrast, PAD implementation in China is shaped by fragmented financing arrangements, uneven public preparedness, and limited integration across institutions and emergency response systems. Moreover, most existing studies in China remain quantitative, focusing primarily on spatial distribution16 or cost-effectiveness,17 while paying far less attention to the organizational, procedural, and behavioral mechanisms that determine whether an AED can be successfully used during an emergency.
PAD implementation is therefore shaped by interacting influences across multiple levels, including policy and administration, organizations and venues, community settings, and individual bystanders. Yet few studies have examined these barriers from the perspectives of the diverse actors involved in AED financing, deployment, management, maintenance, training, platform development, and emergency response. Addressing this gap is essential for developing context-specific strategies to strengthen PAD performance in China. Therefore, this study aimed to explore the multilevel barriers to PAD implementation in Shanghai from the perspectives of health administrators, EMS personnel, venue managers, digital platform developers, and other key actors, and to identify feasible strategies for improving public-access defibrillation within the current policy and resource context.
Methods
Conceptual Framework
This study was guided by the Social Ecological Model (SEM), a framework widely used to examine the multilevel determinants of health-related decision-making and behavior. SEM facilitates understanding of how individual factors interact with interpersonal, community, organizational, and policy environments to shape emergency response behaviors.18,19 Within this framework, public health interventions can be examined not only in terms of outcomes, but also in relation to the structural and behavioral processes that influence their implementation.
In the context of public-access defibrillation (PAD), SEM was particularly appropriate because it enabled simultaneous examination of macro-level structures, such as legislation, financing arrangements, governance mechanisms, and information systems, alongside micro-level factors, including bystanders’ knowledge, skills, perceptions, and behavioral barriers. This multilevel perspective helped explain the persistent gap between AED availability and actual use in emergency situations. SEM also informed the development of the interview guide and the thematic organization of the analysis by structuring inquiry across system, organizational, community, and individual levels.
Study Design
We conducted a qualitative study using in-depth, semi-structured interviews to explore the experiences and perspectives of actors involved in AED financing, deployment, management, maintenance, training, digital platform development, and emergency response. This approach was chosen because it is well suited to generating rich, contextualized accounts of how public-access defibrillation functions in practice and where implementation barriers arise.
This study followed the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist (Appendix S2).20 Guided by the SEM, the study aimed to examine how multilevel factors shape the real-world functioning of PAD in Shanghai, including how institutional and individual conditions influence the ability to locate, access, retrieve, and use AEDs during emergencies, and what strategies may strengthen PAD performance within the current policy and resource context.
Study Setting and Participant Recruitment
Public-access AED deployment in Shanghai began around 2015. Using a Python-based web crawler, we identified 4313 publicly registered AEDs listed on a WeChat AED information platform, yielding a density of approximately 1 AED per 5760 residents based on Shanghai’s permanent resident population of approximately 24.87 million. One registered AED was linked to a municipal vehicle and was located outside the Shanghai metropolitan area at the time of data collection (Figure 1).
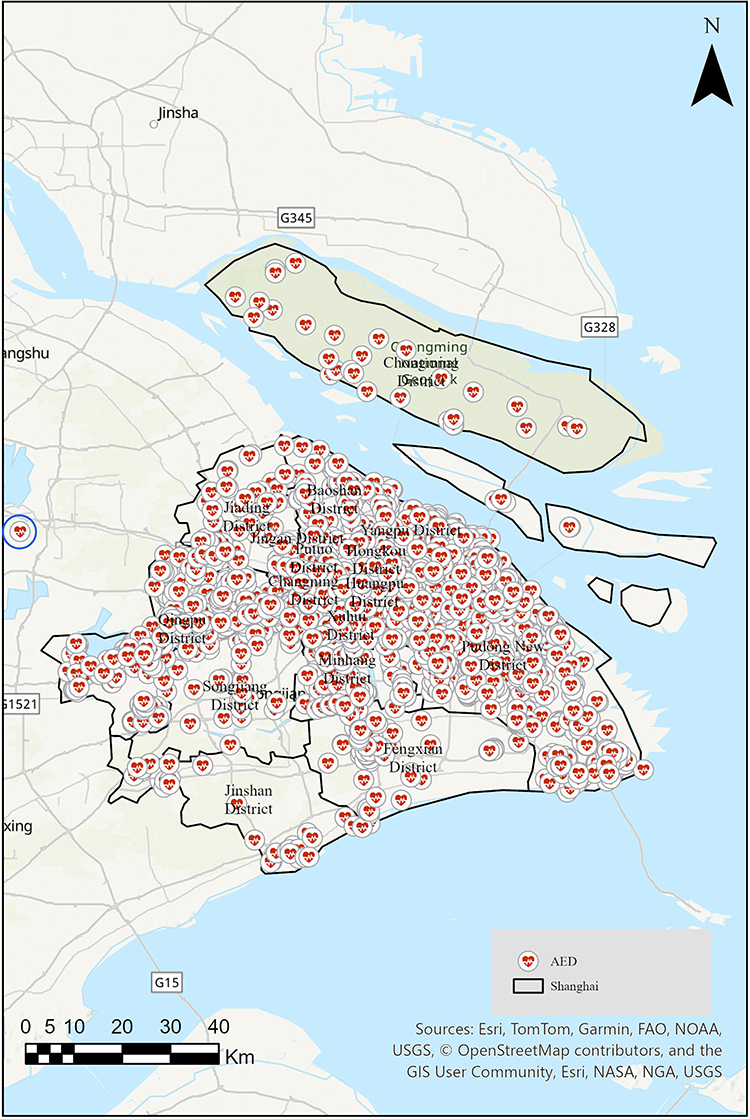 |
Figure 1 Spatial distribution of publicly registered automated external defibrillators (AEDs) in Shanghai, China, identified from a WeChat AED information platform. |
At the district level, AED distribution was highly uneven. Pudong New Area had the largest number of AEDs (n=1816; 53.38 per 100,000 residents), likely reflecting the legacy of public health investment associated with the World Expo. Qingpu District had the highest per-capita density (576 AEDs; 104.14 per 100,000 residents) and was the only district meeting the benchmark of 100 AEDs per 100,000 population, although kernel density analysis indicated that its AEDs were concentrated in the central area, with peripheral coverage remaining limited. By contrast, densely populated central urban districts such as Xuhui, Yangpu, Jing’an, Minhang, and Putuo had fewer than 274 AEDs each, with per-capita densities ranging from 11.73 to 30.42 per 100,000 residents. Outer suburban districts including Jinshan, Songjiang, and Chongming had the lowest densities (6.33–6.60 per 100,000 residents). Table 1 presents the full district-level AED distribution.
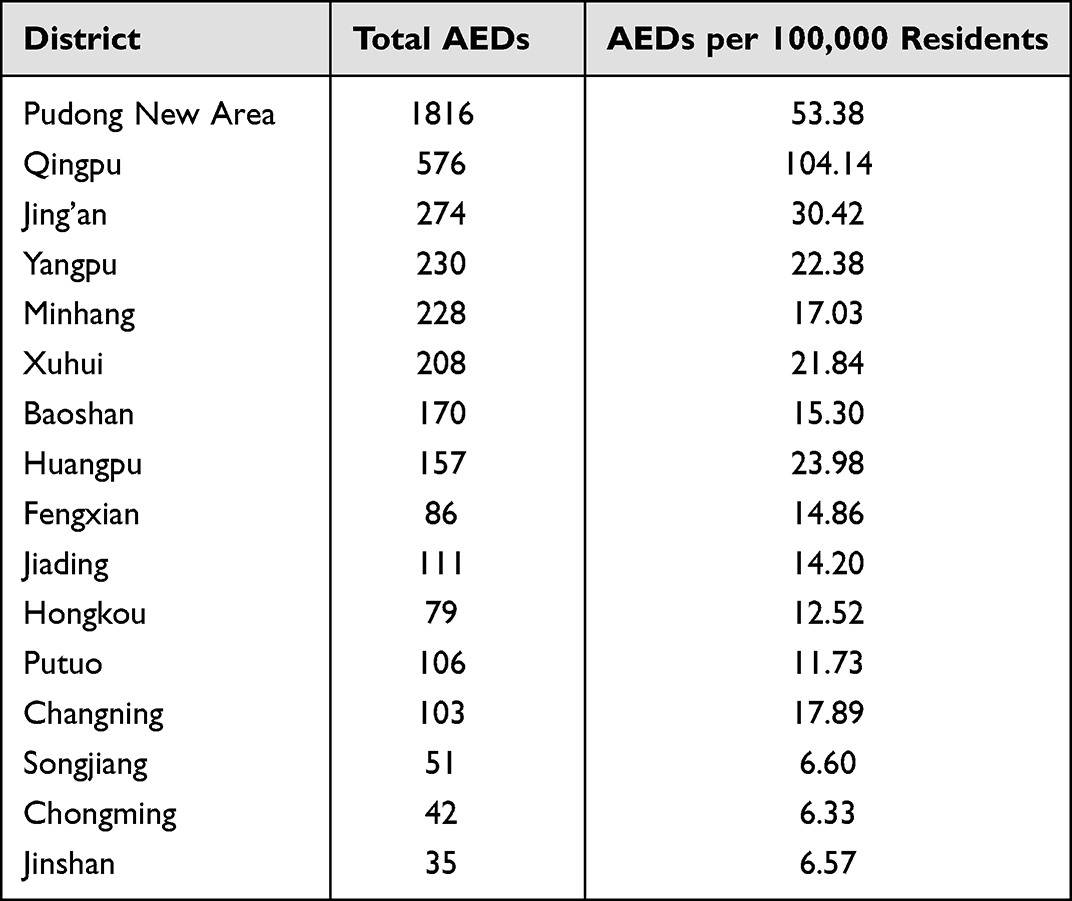 |
Table 1 District-Level AED Distribution and per-Capita Density in Shanghai (by 2025) |
To obtain a comprehensive understanding of PAD implementation, we used purposive sampling to recruit participants from stakeholder groups directly involved in PAD-related planning, implementation, coordination, or operational support. Sampling sought to capture variation across institutional roles rather than representativeness in a statistical sense. Participants were recruited from municipal- and venue-level organizations, including the Health Commission, the Red Cross Society, the prehospital emergency medical center, public venue managers, and AED information platform developers.
Participants were eligible if they: (1) had at least three years of involvement in PAD-related work, such as AED financing, site selection, management, training, maintenance, or emergency response; and (2) currently held operational responsibilities related to PAD. A total of 42 participants met these criteria and agreed to take part. An initial briefing session was used to introduce the study objectives and interview procedures. Potential participants were then approached individually, and one-on-one interviews were arranged at their workplaces to protect confidentiality, minimize disruption to their responsibilities, and support candid discussion.
Data Collection
In-depth semi-structured interviews were conducted in Mandarin between December 2024 and June 2025 by two trained qualitative researchers, YG (PhD candidate) and XZ (Master of Public Health). Data transcription, checking, and preliminary analysis continued until July 2025. Both interviewers had academic backgrounds related to emergency care and health systems and had no prior personal or professional relationships with participants.
Before each interview, the researchers introduced themselves, explained the purpose of the study, and obtained informed consent. Participants were informed that their responses would be anonymized and that anonymized quotations could be used in academic publication. Interviewees were also invited to briefly describe their professional background and their involvement in OHCA response, AED planning, deployment, management, or operational support.
The interview guide was informed by the SEM and used open-ended questions to explore barriers and opportunities across different stages of PAD implementation, including financing, siting, accessibility, use, and maintenance. Example questions included: “What challenges does your organization encounter when participating in PAD?”; “Do you think the current quantity and distribution of AEDs are sufficient or reasonable?”; “What opportunities do you see for diversifying AED deployment strategies, such as mobile AED models?”; and “What do you believe are the main reasons for China’s low per-capita AED utilization?”
Interviews lasted approximately 30–40 minutes and were audio-recorded and transcribed verbatim. Data collection and preliminary analysis proceeded iteratively. Thematic saturation was considered to have been reached when successive interviews no longer generated substantively new themes or altered the developing thematic framework, and when recurring patterns were observed across stakeholder categories. A saturation tracking table is provided in Appendix S1. No field notes were taken, and transcripts were not returned to participants for member checking. To protect confidentiality, all transcripts were anonymized, assigned numerical identifiers, and stored in password-protected files accessible only to the research team.
Data Analysis
We used thematic analysis, combining inductive coding with deductive guidance from the SEM. All transcripts were imported into NVivo 11 (QSR International, Victoria, Australia). Two researchers (YG and XZ) independently read the transcripts repeatedly to familiarize themselves with the data and then conducted initial line-by-line coding. Preliminary codes were developed both from the conceptual framework and from issues emerging directly from the data.
The two coders compared and refined the coding structure through iterative discussion. Coding discrepancies were resolved through consensus, and related codes were grouped into broader categories and themes. Throughout the analytic process, we examined patterns, similarities, and differences across interviews and stakeholder categories to assess the breadth of theme representation and whether certain issues were emphasized more strongly by particular participant groups. Final themes were organized into challenges and opportunities at the individual, organizational, environmental, and system levels related to AED financing, deployment, use, and maintenance. Representative extracts illustrating the coding and analytic process are presented in Table 2.
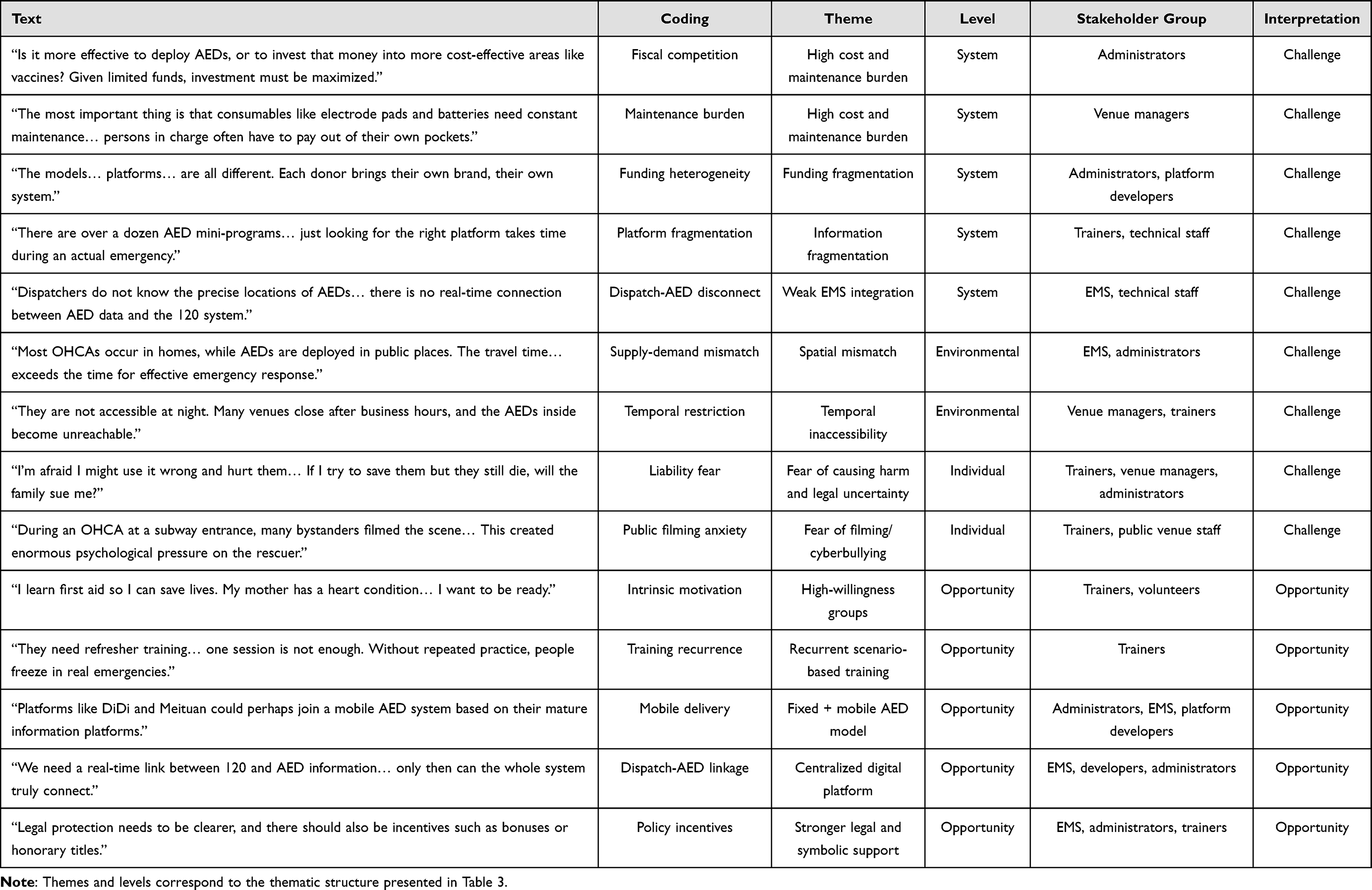 |
Table 2 Example of Content Analysis Process |
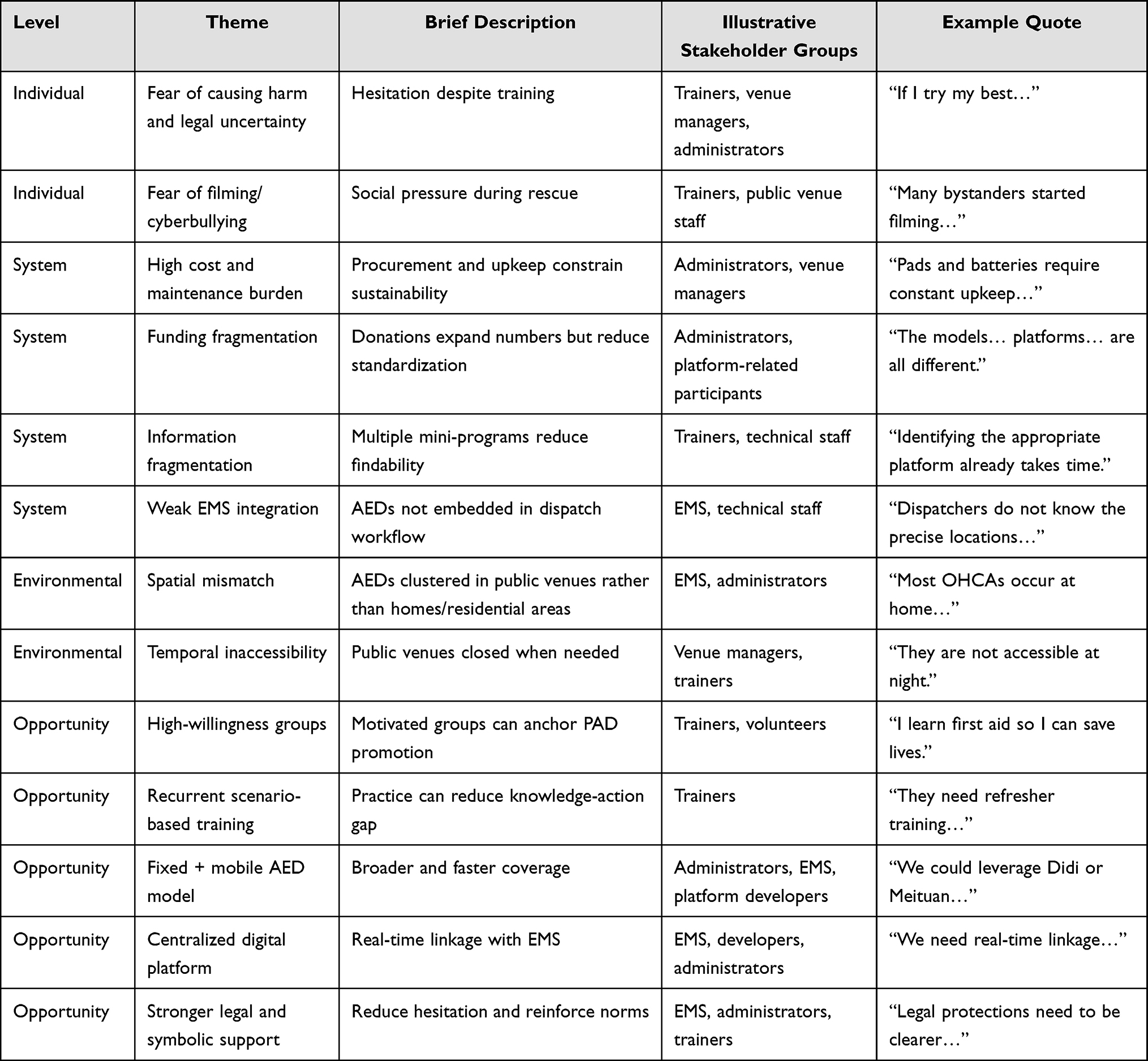 |
Table 3 Summary of Main Themes, Levels, Stakeholder Groups, and Illustrative Quotes |
Results
Participant Characteristics and Overview of Themes
All 42 interviews were completed as scheduled, with no repeated interviews or participant dropouts. Of the participants, 17 were female and 25 were male, with a mean age of 43.74 years. Participants included 16 health administrative or institutional officials, 15 operational or technical support personnel, and 11 venue managers or instructors involved in prehospital emergency training. Across these stakeholder categories, participants described interrelated barriers and opportunities spanning individual, organizational, environmental, and system levels. While the broad thematic structure was highly consistent across groups, certain themes were emphasized more strongly by specific participants: legal hesitation and psychological pressure were more frequently discussed in relation to bystander behavior and training contexts, whereas fragmented governance, maintenance burdens, and platform interoperability were especially emphasized by administrative, technical, and EMS-related participants. Table 3 summarizes the main themes and their representation across stakeholder groups.
Challenges in Public-Access Defibrillation
Individual-Level Barriers: Fear, Legal Uncertainty, and Social Pressure
A prominent barrier identified across interviews was the gap between knowing and acting. Even when citizens had received first-aid training, many participants reported that bystanders often remained reluctant to use AEDs during actual emergencies. Fear of causing harm, uncertainty about legal consequences, and concern about being blamed were repeatedly described as key deterrents. These concerns suggest that technical knowledge alone is insufficient to ensure action in emergency situations.
One participant stated, “I’m afraid I might use it incorrectly and end up hurting them… I’ve never operated one before” (Participant 32, Shanghai Hongqiao Railway Station). Another asked, “If I try my best to save someone but they still die, could the family sue me?” (Participant 21, Municipal Metro Station).
Participants also described how the social environment may intensify hesitation. In particular, the fear of being recorded, criticized, or exposed to online harassment during a rescue attempt was seen as an additional barrier to intervention. This suggests that public scrutiny, amplified by digital media, can further widen the knowledge-action gap. One participant recalled that bystanders began filming during an emergency, which “added enormous pressure-sometimes even more than the rescue itself” (Participant 22, Xujiahui Park).
System-Level Barriers: Cost Burdens, Fragmented Governance, and Weak Digital Integration
At the system level, participants consistently described AED deployment as constrained by high procurement and maintenance costs. Government and venue-based participants noted that AEDs were often viewed as expensive devices competing with other public health priorities, rather than as core emergency infrastructure. Ongoing costs, especially for pads and batteries, were seen as a major challenge to long-term sustainability. In the absence of clearly assigned maintenance responsibilities, some onsite managers reported having to cover costs themselves, contributing to a pattern of devices being installed but not sustainably maintained.
Participants also highlighted funding fragmentation. Although donations from enterprises and charitable organizations had expanded AED availability, the lack of centralized coordination had produced variation in device models, management approaches, and information platforms. According to several interviewees, this uncoordinated expansion risked increasing the number of devices without improving their interoperability or system usability.
A closely related theme was digital fragmentation. Participants reported that multiple AED-related WeChat mini-programs coexisted, often without standardized data structures or real-time updating. This made it difficult for users to identify the correct platform or locate reliable device information during an emergency. EMS-related participants further emphasized that AED data were not effectively integrated with the 120 dispatch system. Dispatchers often lacked real-time information on AED location and operational status, which prevented AED retrieval from being embedded in formal dispatch workflows. As a result, AEDs were present in the environment but not fully actionable within the emergency response chain.
Another functional barrier concerned signage and access restrictions. Participants noted that some earlier-installed AEDs did not use standardized signs, while even newer signs often remained inconspicuous to the general public. Labels such as “for internal use only” further limited real-world accessibility. Together, these problems reduced not only visibility but also the practical usability of AEDs in emergencies.
Environmental Barriers: Spatial Inequality and Limited Temporal Accessibility
Participants consistently reported a mismatch between AED deployment and OHCA risk patterns. They described clear disparities between central and peripheral areas and between public venues and residential communities. In particular, many respondents emphasized that OHCAs often occur at home, whereas AEDs are predominantly concentrated in public settings. This spatial mismatch was consistent with the distribution pattern shown in Figure 1. Furthermore, the district-level data (Table 1) revealed substantial variation in AED density, ranging from 6.33 per 100,000 residents in Chongming to 104.14 per 100,000 in Qingpu, with most densely populated central districts falling well below the benchmark of 100 AEDs per 100,000 population.
Temporal accessibility was also a major concern. Although policies emphasize AED installation in high-footfall settings, many such venues are closed at night, on weekends, or outside business hours. Participants therefore questioned whether nominally public AEDs were truly accessible at the times when they were most needed. Internal-use restrictions in workplaces and schools were cited as further limiting access.
Opportunities for Strengthening Public-Access Defibrillation
Individual-Level Opportunities: High-Willingness Groups and Recurrent Scenario-Based Training
Despite the barriers described above, participants also identified important opportunities. One recurring theme was the presence of high-willingness groups, including first-aid trainers, community health volunteers, and family members of people at elevated cardiac risk. These groups were seen as especially promising entry points for strengthening community-based emergency response capacity. Participants suggested that, rather than relying solely on broad public education campaigns, PAD promotion could more strategically build from individuals who already show strong motivation to intervene.
Participants further emphasized that willingness alone was not enough; repeated practice was necessary to convert willingness into confident action. Scenario-based and recurrent training was viewed as particularly valuable for improving AED operational confidence, reinforcing emergency skills, and reducing hesitation. Several interviewees highlighted the importance of refreshers, simulation-based exercises, and recertification to maintain readiness over time.
System-Level Opportunities: Data-Informed Deployment, Mobile AED Models, and Platform Integration
Participants widely supported more evidence-based AED siting strategies. Suggested approaches included combining OHCA risk patterns with mobility flows, demographic characteristics, and round-the-clock accessibility to identify priority locations. Interviewees frequently mentioned aging communities, ground-floor commercial areas, and 24-hour venues as promising targets for future deployment.
Many participants also supported a hybrid deployment model that combines fixed-site AEDs with mobile AED delivery. Compared with traditional volunteer retrieval models, AEDs carried by taxis, ride-hailing vehicles, or food-delivery riders were perceived as offering broader and more rapid coverage, particularly in dense urban settings. Several interviewees suggested that food-delivery riders may be especially suitable in China because of their spatial dispersion and operational flexibility. These mobile approaches were viewed not as replacements for fixed AEDs, but as complementary mechanisms for addressing persistent spatial inequities.
Digital integration emerged as another major opportunity. Participants strongly supported the establishment of a centralized, government-led AED information platform that would provide real-time device visibility and connect directly with the 120 EMS dispatch system. Such a platform was viewed as essential for improving dispatch accuracy, reducing retrieval delays, and enabling more coordinated AED management. Some interviewees also highlighted the future potential of full-lifecycle digital traceability and improved domestic manufacturing technologies to support higher-quality data integration and management.
Societal and Environmental Opportunities: Legal Protection and Symbolic Incentives
Participants also emphasized broader enabling conditions for PAD activation. Stronger legal protection for bystanders was widely viewed as critical to reducing hesitation and addressing fears of liability. In addition, several interviewees proposed symbolic incentives, such as public recognition, certificates, or honorary awards, as ways to reinforce prosocial norms and encourage intervention. These measures were seen as particularly important for translating high willingness into action in real emergencies.
Cross-Stakeholder Consistency of Themes
Overall, the identified themes were broadly consistent across stakeholder categories, but their emphases differed. Administrative and managerial participants more often highlighted procurement costs, fragmented funding, and governance responsibilities. EMS and technical participants placed greater emphasis on dispatch integration, data quality, and platform interoperability. Venue managers and trainers more frequently discussed public hesitation, signage visibility, access restrictions, and the need for repeated scenario-based training. Taken together, these differences did not suggest competing interpretations; rather, they reflected complementary perspectives on the same implementation gap between AED presence and AED activation. This convergence across groups supports the interpretation that PAD performance in Shanghai is shaped by interacting multilevel barriers rather than by any single isolated problem. This system-level pattern directly informed the discussion of an “activation gap” between AED deployment and actual use.
Discussion
This study identified multilevel structural, procedural, and behavioral barriers embedded within Shanghai’s public-access defibrillation (PAD) system. Rather than reflecting a simple shortage of automated external defibrillators (AEDs), these barriers point to a broader implementation gap between AED deployment and AED activation in real emergencies. By integrating perspectives from administrative, organizational, technical, venue-based, and training-related participants, this study extends previous research that has primarily focused either on spatial allocation21 (“where AEDs should be placed”) or public knowledge and willingness22 (“whether bystanders are prepared to act”). Instead, our findings highlight a more practical question: under what conditions can AEDs actually be located, retrieved, and used in time-sensitive emergencies? This perspective suggests that PAD effectiveness depends less on device presence alone than on the degree of coordination, governance, accessibility, and behavioral readiness across the wider emergency response ecosystem.21,23,24
A central finding of this study is that sustainable financing is not merely a cost issue, but a governance issue. Previous research has often attributed limited AED coverage to the high costs of procurement and maintenance.25,26 Our findings suggest a deeper structural problem: AEDs have not yet been fully institutionalized as essential public health infrastructure within a unified fiscal and governance framework. In Shanghai, responsibility for procurement, deployment, upkeep, and replacement remains distributed across venues, donors, enterprises, and local administrative actors. This decentralized model has contributed to heterogeneity in device types, maintenance arrangements, and platform registration, while also weakening long-term accountability and standardization. As a result, expansion in AED numbers does not necessarily translate into equitable, sustainable, or well-coordinated system development. Strengthening PAD therefore requires not only more investment, but also clearer public budgeting mechanisms, defined maintenance responsibilities, and more standardized governance arrangements.
Our findings also show that inequities in PAD are shaped by more than simple spatial undercoverage. While earlier studies have documented uneven AED distribution across China, this study indicates that, in Shanghai, deployment is still influenced heavily by administrative directives and convenience-based placement rather than by OHCA risk, population flow, or temporal accessibility. This creates predictable gaps in real-world coverage, particularly given that many OHCAs occur in residential areas and outside routine opening hours. These findings support the need for risk-informed and context-sensitive AED siting strategies, but they also highlight an implementation prerequisite that is often overlooked: optimization cannot function effectively without integrated data systems, shared governance, and cross-sector coordination. In this sense, the barrier is not simply a lack of analytic models, but a lack of the institutional conditions needed to apply them.
Participants’ support for combining fixed-site AEDs with mobile deployment strategies offers an important practical implication for megacities.27–29 Mobile approaches using taxis, ride-hailing services, or delivery networks24,30,31 were viewed as especially promising because they may help address persistent gaps in residential and time-sensitive coverage that fixed public-site deployment alone cannot resolve. Rather than being framed as replacements for conventional AED placement, these approaches should be understood as complementary strategies within a broader PAD system.32,33 For highly mobile and densely populated cities such as Shanghai, a hybrid model may be more realistic than relying exclusively on either static deployment or volunteer-based retrieval. Future PAD planning should therefore consider both place-based and mobility-based access pathways.
Information fragmentation emerged as one of the most consequential procedural barriers identified in this study. Participants described a PAD information environment characterized by multiple platform providers, inconsistent data standards, limited interoperability, and weak linkage with the 120 dispatch system. In practice, this means that even when AEDs are physically nearby, they may remain functionally invisible during an emergency. This finding expands conventional understandings of AED visibility and accessibility. In digitally mediated urban systems, effective PAD depends not only on whether a device exists in a location, but also on whether it can be reliably found, verified, and incorporated into emergency decision-making in real time. This suggests that “findability” should be treated as a core implementation dimension of PAD. From a policy perspective, stronger digital governance is needed, including standardized registration, unified coding and signage,34 real-time status updating, and direct linkage between AED databases and dispatch workflows.
At the behavioral level, our findings suggest that training alone is insufficient to ensure AED use. Participants repeatedly described fear of causing harm,35–37 uncertainty about legal consequences,38–40 and anxiety arising from public scrutiny or filming as major deterrents to action. These concerns persisted even among individuals who had received first-aid instruction, indicating that the gap between learning and action is shaped by emotional and institutional conditions as much as by knowledge deficits. This aligns with international discussions of the “knowledge-action gap”, but our findings also show that such hesitation may be amplified in contexts where legal protections are perceived as unclear and public expectations of lay rescue remain uncertain. Strengthening PAD therefore requires more than technical training. It also requires clearer legal reassurance, stronger social normalization of bystander action, and public messaging that frames AED use as both legitimate and socially supported.
These findings have several practical implications. First, legal protection for bystanders should be clarified and communicated more explicitly in relation to CPR and AED use. Second, PAD governance would benefit from a more centralized coordination mechanism to standardize procurement, maintenance, signage, and data management.41,42 Third, AED information systems should be integrated with dispatch workflows so that devices can become operational assets within the chain of survival rather than passive infrastructure.43,44 Fourth, training strategies should move beyond one-off awareness sessions toward repeated, scenario-based practice designed to reduce hesitation and improve confidence.45,46 Finally, targeted activation strategies for high-willingness groups47-such as family members of cardiac patients, health-related students, trained volunteers, and other motivated lay responders-may provide a practical pathway for building a more responsive community rescue network.48 These groups are not substitutes for broad public preparedness, but they may serve as priority populations for early, scalable intervention.
Several limitations should also be noted. As a qualitative study conducted in Shanghai, the findings are context-specific and may not be directly generalizable to all cities in China or other countries. In addition, although the study included diverse PAD-related stakeholder groups, it did not include all possible actors, such as ordinary laypersons with no prior PAD-related involvement or survivors’ family members outside organized networks. The findings therefore reflect informed system perspectives rather than population-level prevalence of attitudes or behaviors. Nevertheless, the study provides valuable insight into how multilevel barriers interact within a rapidly urbanizing megacity and offers practical directions for improving PAD implementation in similar settings.
Overall, this study suggests that the effectiveness of PAD in Shanghai is constrained less by the mere presence or absence of AEDs than by the conditions that determine whether AEDs can be activated in time. Fragmented financing, weak cross-sector coordination, digital disconnection, restricted accessibility, and persistent behavioral hesitation collectively shape this implementation gap. Improving PAD therefore requires a shift from an installation-oriented approach to an activation-oriented system strategy-one that integrates governance, digital infrastructure, legal support,49 public training, and complementary fixed-plus-mobile deployment models.
Limitations
This study has several limitations. First, it was conducted in Shanghai, a highly developed megacity with relatively strong public health investment, governance capacity, and emergency preparedness, and the findings may not be directly transferable to smaller cities or less-resourced regions. Second, as a qualitative study, the findings are context-specific and reflect participants’ experiences and interpretations rather than population-level prevalence of attitudes or behaviors. Third, although we included diverse PAD-related stakeholder groups, we did not capture all potentially relevant perspectives, such as ordinary laypersons without prior PAD involvement or family members outside organized networks. Future research could extend these findings through comparative studies across cities with different development levels and through quantitative evaluation of proposed interventions, such as integrated AED information platforms, optimized siting strategies, and fixed-plus-mobile deployment models.
Conclusion
This study identified a multilevel implementation gap between AED deployment and AED activation in Shanghai. The findings suggest that the effectiveness of public-access defibrillation is constrained less by device availability alone than by fragmented governance, weak digital integration, inconsistent accessibility, and persistent behavioral hesitation. Improving real-world PAD performance therefore requires more than expanding AED numbers. It requires government-led cross-sector coordination, standardized and interoperable AED information systems linked to EMS dispatch, risk-informed and time-sensitive deployment planning, clearer legal protection for bystanders, and repeated scenario-based training to strengthen activation readiness. By framing PAD as a system-integration challenge rather than a device-placement problem alone, this study provides evidence to inform the next stage of AED governance, deployment, and management in China’s megacities.
Data Sharing Statement
The qualitative interview data generated and analyzed during the current study are not publicly available because they contain potentially identifiable information and were collected under conditions of confidentiality. De-identified excerpts are included in the article. Further information may be available from the corresponding author on reasonable request, subject to ethical and institutional approval.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the principles outlined in the Declaration of Helsinki. Ethical approval for this study was obtained from the Ethics Committee for Medical Research of the School of Public Health, Fudan University (Approval No. IRB#2025-01-1199, valid until June 30, 2025), and written informed consent was obtained from all participants. Informed consent was obtained from participants for the publication of their anonymized responses and direct quotes.
Author Contributions
Yu Gao and Xin Zhou conceived and designed the study, developed the interview guide, conducted the interviews, transcribed and coded the data, performed the thematic analysis, and drafted the manuscript. Li Luo critically revised the manuscript for important intellectual content and supervised the study. All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Kiguchi T, Okubo M, Nishiyama C, et al. Out-of-hospital cardiac arrest across the world: first report from the International Liaison Committee on Resuscitation (ILCOR). Resuscitation. 2020;152:39–14. doi:10.1016/j.resuscitation.2020.02.044
2. Danish Heart Stop Register 2020. 2021. Available from: https://hjertestopregister.dk/?page_id=428.
3. Zheng J, Lv C, Zheng W, et al. Incidence, process of care, and outcomes of out-of-hospital cardiac arrest in China: a prospective study of the BASIC-OHCA registry. Lancet Public Health. 2023;8(12):e923–e932. doi:10.1016/S2468-2667(23)00173-1
4. Hou L, Wang Y, Chen B, Ji Y, Wang B. Resuscitation of out-of-hospital cardiac arrest in China: a systematic review and utstein-style data analysis based on the chain of survival. Resuscitation. 2023;193:109974. doi:10.1016/j.resuscitation.2023.109974
5. Hallstrom A, Ornato J, Weisfeldt M, et al; Public Access Defibrillation Trial Investigators. Public-access defibrillation and survival after out-of-hospital cardiac arrest. N Engl J Med. 2004;351(7):637–646.
6. Hasselqvist-Ax I, Herlitz J, Svensson L. Early CPR in out-of-hospital cardiac arrest. N Engl J Med. 2015;373(16):1573–1574. doi:10.1056/NEJMc1509059
7. Coute RA, Mader TJ, Kurz MC. Evaluation of National Institutes of Health cardiac arrest research based on” chain of survival” links. Acad Emerg Med. 2022;29(11):1381–1382. doi:10.1111/acem.14569
8. Valenzuela TD, Roe DJ, Nichol G, Clark LL, Spaite DW, Hardman RG. Outcomes of rapid defibrillation by security officers after cardiac arrest in casinos. N Engl J Med. 2000;343(17):1206–1209. doi:10.1056/NEJM200010263431701
9. Baekgaard JS, Viereck S, Moller TP, Ersboll AK, Lippert F, Folke F. The effects of public access defibrillation on survival after out-of-hospital cardiac arrest: a systematic review of observational studies. Circulation. 2017;136(10):954–965. doi:10.1161/CIRCULATIONAHA.117.029067
10. Bossaert L, Handley A, Marsden A, et al. European Resuscitation Council guidelines for the use of automated external defibrillators by EMS providers and first responders: A statement from the Early Defibrillation Task Force, with contributions from the Working Groups on Basic and Advanced Life Support, and approved by the Executive Committee of the European Resuscitation. Resuscitation. 1998;37(2):91–94. doi:10.1016/s0300-9572(98)00037-9
11. Hansen SM, Hansen CM, Folke F, et al. Bystander defibrillation for out-of-hospital cardiac arrest in public vs residential locations. JAMA Cardiol. 2017;2(5):507–514. doi:10.1001/jamacardio.2017.0008
12. Kiguchi T, Kiyohara K, Kitamura T, et al. Public-access defibrillation and survival of out-of-hospital cardiac arrest in public vs. residential locations in Japan. Circ J. 2019;83(8):1682–1688. doi:10.1253/circj.CJ-19-0065
13. Liao S, Gao F, Feng L, Wu J, Wang Z, Chen W. Observed equity and driving factors of automated external defibrillators: a case study using WeChat Applet Data. ISPRS Int J Geo-Inf. 2023;12(11):444. doi:10.3390/ijgi12110444
14. Zhou Z-Y, Zhang J-Z, Zhao X-Q, et al. Current status of support for Automated External Defibrillators (AEDs) in public places and factors influencing their use in China: a cross-sectional study. J Public Health. 2024;32(11):2105–2120. doi:10.1007/s10389-023-01959-5
15. Wu C, Wu Y, Qiao L. Revealing the decision-making practices in automated external defibrillator deployment: insights from Shanghai, China. BMC Public Health. 2025;25(1):152. doi:10.1186/s12889-025-21341-2
16. Shi Y, Zhang N. Analysis and Optimization of Automated External Defibrillator (AED) configuration in Chinese cities: a case study of Dongcheng District, Beijing. Risk Manag Healthc Policy. 2025;Volume 18:3281–3295. doi:10.2147/RMHP.S502335
17. Groeneveld PW, Kwong JL, Liu Y, et al. Cost-effectiveness of automated external defibrillators on airlines. JAMA. 2001;286(12):1482–1489. doi:10.1001/jama.286.12.1482
18. McLeroy KR, Bibeau D, Steckler A, Glanz K. An ecological perspective on health promotion programs. Health Educ Q. 1988;15(4):351–377. doi:10.1177/109019818801500401
19. Stokols D. Translating social ecological theory into guidelines for community health promotion. Am J Health Promotion. 1996;10(4):282–298. doi:10.4278/0890-1171-10.4.282
20. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
21. Chan TC, Li H, Lebovic G, et al. Identifying locations for public access defibrillators using mathematical optimization. Circulation. 2013;127(17):1801–1809. doi:10.1161/CIRCULATIONAHA.113.001953
22. Yeung J, Okamoto D, Soar J, Perkins GD. AED training and its impact on skill acquisition, retention and performance–a systematic review of alternative training methods. Resuscitation. 2011;82(6):657–664. doi:10.1016/j.resuscitation.2011.02.035
23. Priori SG, Blomström-Lundqvist C, Mazzanti A, et al. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: the task force for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death of the European Society of Cardiology (ESC) Endorsed by Association for European Paediatric and Congenital Cardiology (AEPC). Europace. 2015;17(11):1601–1687. doi:10.1093/europace/euv319
24. Dahan B, Jabre P, Karam N, et al. Optimization of automated external defibrillator deployment outdoors: an evidence-based approach. Resuscitation. 2016;108:68–74. doi:10.1016/j.resuscitation.2016.09.010
25. Mao RD, Ong MEH. Public access defibrillation: improving accessibility and outcomes. Br Med Bull. 2016;118(1):25–32. doi:10.1093/bmb/ldw011
26. Moran PS, Teljeur C, Masterson S, O’Neill M, Harrington P, Ryan M. Cost-effectiveness of a national public access defibrillation programme. Resuscitation. 2015;91:48–55. doi:10.1016/j.resuscitation.2015.03.017
27. Tsai Y-S, Ko PC-I, Huang C-Y, Wen T-H. Optimizing locations for the installation of automated external defibrillators (AEDs) in urban public streets through the use of spatial and temporal weighting schemes. Appl Geogr. 2012;35(1–2):394–404. doi:10.1016/j.apgeog.2012.09.002
28. Huang C-Y, Wen T-H. Optimal installation locations for automated external defibrillators in Taipei 7-Eleven stores: using GIS and a genetic algorithm with a new stirring operator. Comput Math Methods Med. 2014;2014(1):241435. doi:10.1155/2014/241435
29. Brown TP, Brown T, Andronis L, et al. Optimisation of the deployment of automated external defibrillators in public places in England. Health Soc Care Deliv Res. 2025;13(5):1–179. doi:10.3310/HTBT7685
30. Myerburg RJ, Fenster J, Velez M, et al. Impact of community-wide police car deployment of automated external defibrillators on survival from out-of-hospital cardiac arrest. Circulation. 2002;106(9):1058–1064. doi:10.1161/01.CIR.0000028147.92190.A7
31. Siddiqui FJ, Fook-Chong S, Shahidah N, et al. Technology activated community first responders in Singapore: real-world care delivery & outcome trends. Resusc Plus. 2023;16:100486. doi:10.1016/j.resplu.2023.100486
32. O’Sullivan J, Moore E, Dunn S, et al. Development of a centralised national AED (automated external defibrillator) network across all ambulance services in the United Kingdom. Resusc Plus. 2024;19:100729. doi:10.1016/j.resplu.2024.100729
33. Namee K, Panong N, Polpinij J. Integration of IoT, edge computing and cloud computing for monitoring and controlling automated external defibrillator cabinets in emergency medical service. In:
34. Hansen CM, Wissenberg M, Weeke P, et al. Automated external defibrillators inaccessible to more than half of nearby cardiac arrests in public locations during evening, nighttime, and weekends. Circulation. 2013;128(20):2224–2231. doi:10.1161/CIRCULATIONAHA.113.003066
35. Nielsen AM, Isbye DL, Lippert FK, Rasmussen LS. Can mass education and a television campaign change the attitudes towards cardiopulmonary resuscitation in a rural community? Scand J Trauma Resusc Emerg Med. 2013;21(1):39. doi:10.1186/1757-7241-21-39
36. Moon S, Ryoo HW, Ahn JY, et al. A 5-year change of knowledge and willingness by sampled respondents to perform bystander cardiopulmonary resuscitation in a metropolitan city. PLoS One. 2019;14(2):e0211804. doi:10.1371/journal.pone.0211804
37. Huang EP-C, Chiang W-C, Lu T-C, et al. Barriers to bystanders defibrillation: a national survey on public awareness and willingness of bystanders defibrillation☆. J Formos Med Assoc. 2021;120(3):974–982. doi:10.1016/j.jfma.2020.10.020
38. Cartledge S, Bray JE, Leary M, Stub D, Finn J. A systematic review of basic life support training targeted to family members of high-risk cardiac patients. Resuscitation. 2016;105:70–78. doi:10.1016/j.resuscitation.2016.04.028
39. Tian X, Zhang Y, Dou D. Training experience is an important factor affecting willingness for bystander CPR and awareness of AED: a survey of residents from a province in Central China in 2023. Front Public Health. 2024;12:1459590. doi:10.3389/fpubh.2024.1459590
40. Aedh AI, Abdel-Haliem E, Farid M. Knowledge, attitude, and practice of CPR and willingness to perform it among undergraduate medical students of Najran University, Saudi Arabia: a cross-sectional study. BMC Med Educ. 2025;25(1):772. doi:10.1186/s12909-025-07344-y
41. Smith CM, Lim Choi Keung SN, Khan MO, et al. Barriers and facilitators to public access defibrillation in out-of-hospital cardiac arrest: a systematic review. Eur Heart J Qual Care Clin Outcomes. 2017;3(4):264–273. doi:10.1093/ehjqcco/qcx023
42. Kronick SL, Kurz MC, Lin S, et al. Part 4: systems of care and continuous quality improvement: 2015 American Heart Association Guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132(18 Suppl 2):S397–413. doi:10.1161/CIR.0000000000000258
43. Ringh M, Rosenqvist M, Hollenberg J, et al. Mobile-phone dispatch of laypersons for CPR in out-of-hospital cardiac arrest. N Engl J Med. 2015;372(24):2316–2325. doi:10.1056/NEJMoa1406038
44. Schierbeck S, Hollenberg J, Nord A, et al. Automated external defibrillators delivered by drones to patients with suspected out-of-hospital cardiac arrest. Eur Heart J. 2022;43(15):1478–1487. doi:10.1093/eurheartj/ehab498
45. Sasaki M, Ishikawa H, Kiuchi T, Sakamoto T, Marukawa S. Factors affecting layperson confidence in performing resuscitation of out-of-hospital cardiac arrest patients in Japan. Acute Med Surg. 2015;2(3):183–189. doi:10.1002/ams2.106
46. Greif R, Lockey A, Breckwoldt J, et al. European Resuscitation Council Guidelines 2021: education for resuscitation. Resuscitation. 2021;161:388–407. doi:10.1016/j.resuscitation.2021.02.016
47. Platz E, Scheatzle MD, Pepe PE, Dearwater SR. Attitudes towards CPR training and performance in family members of patients with heart disease. Resuscitation. 2000;47(3):273–280. doi:10.1016/s0300-9572(00)00245-8
48. Mancini ME, Diekema DS, Hoadley TA, et al. Part 3: ethical issues: 2015 American Heart Association Guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132(18 Suppl 2):S383–96. doi:10.1161/CIR.0000000000000254
49. Hou L, Chen G, Kan H, et al. Legislative status of public-access cardiopulmonary resuscitation—China, 2024. China CDC Weekly. 2025;7(21):737–742. doi:10.46234/ccdcw2025.122
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
Cost-Effectiveness of a Community First Responder System for Out-of-Hospital Cardiac Arrest in Poland
Jaskuła J, Medic G, Verma S, Maurer J, Kooy TA, Greef BD
ClinicoEconomics and Outcomes Research 2025, 17:375-386
Published Date: 2 May 2025