")
Back to Journals » Psychology Research and Behavior Management » Volume 17
Psychosocial Correlates of Motivation for Abstinence Among People Who Used Drugs After Community Rehabilitation Treatment in China: A Structural Equation Modelling
Authors Ruan S, Wang X, Zhao C, Li Q, Li WM, Zhang G, Pan J, Yang X
Received 18 September 2023
Accepted for publication 7 December 2023
Published 4 January 2024 Volume 2024:17 Pages 39—50
DOI https://doi.org/10.2147/PRBM.S440876
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Songli Ruan,1,* Xin Wang,2,* Chengjia Zhao,3,* Qian Li,2 Wing Ming Li,2 Guohua Zhang,4,5 Jianshe Pan,4 Xue Yang2
1Mental Health Education and Guidance Center of College Students, Henan University of Urban Construction, Pingdingshan, People’s Republic of China; 2JC School of Public Health and Primary Care, The Chinese University of Hong Kong, Hong Kong, People’s Republic of China; 3School of Mental Health, Wenzhou Medical University, Wenzhou, People’s Republic of China; 4Department of Psychiatry, The Affiliated Kangning Hospital, Wenzhou, People’s Republic of China; 5Zhejiang Provincial Clinical Research Center for Mental Disorders, The Affiliated Wenzhou Kangning Hospital, Wenzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xue Yang, JC School of Public Health and Primary Care, The Chinese University of Hong Kong, Hong Kong, People’s Republic of China, Email [email protected]
Background: Enhancing abstinence motivation of drugs is an effective strategy for the rehabilitation of people who used drugs and prevention of drug use relapse. However, little is known about its risk and protective factors. This study aimed to examine the potential intrapersonal (ie, impulsivity, depression, anxiety, sleep quality) and interpersonal factors (ie, perceived social support) of abstinence motivation among people who completed the community rehabilitation treatment.
Methods: A total of 222 participants (mean age = 43; male = 89.2%) were recruited from eleven communities located in Wenzhou, China. Data were collected using a self-reported questionnaire in counselling room settings between April and June 2021.
Results: The proportions of participants with depression, anxiety, and poor sleep quality were 38.8%, 19.5%, and 21.2%, respectively. Age and family history of physical disease were significant background factors of abstinence motivation. Impulsivity, depressive symptoms, anxiety symptoms, and poor quality of sleep were negatively associated with abstinence motivation. Perceived social support from family and important others was positively associated with abstinence motivation. Structural equation modeling fitted the data well in which impulsivity and perceived social support were both associated with abstinence motivation indirectly through mental health problems.
Conclusion: The identified psychosocial factors should be addressed in community rehabilitation treatment and follow-up service to enhance abstinence motivation and the long-term effectiveness of the treatment.
Keywords: abstinence motivation to drugs, mental health problems, personality, social support, community-based rehabilitation treatment, Chinese people who used drugs
Introduction
Drug Dependence and Relapse in China and Globally
Drug dependence has been a global public health issue that brings negative impacts on social stability and economic development for centuries.1,2 While drugs such as opium and heroin are considered “traditional drugs”, there has been an upsurge in new drug use, such as methamphetamine, ketamine and ecstasy.3 According to the World Drug Report,4 there were around 275 million people who use drugs worldwide in 2021, a 22% increase from 2010. Furthermore, illicit drug use can be addictive. Drug use relapse after detoxification treatment is common.5 Globally, studies in Iran reported almost 90% relapse within a year of rehabilitation.6 A study in Norway followed 374 illicit substance users and reported a relapse rate of 37% after inpatient substance use treatment by three-month follow-up.7 Drug use caused almost half a million deaths in 2019.4 The negative impact caused by the COVID-19 pandemic is also likely to affect global drug use patterns. The crisis has pushed more than 100 million people into extreme poverty and has greatly exacerbated unemployment and inequalities, making more people susceptible to drug use.8
In China, the prevalence of drug dependence significantly increased in the late 1980s, spreading into 2102 counties and cities, comprising 76.3% of regions of China by 2004.9 Although people who use drugs have decreased for two consecutive years in China, there are still 2.14 million of them nationwide.10 Drug use relapse rates within the first year after discharge from treatment in China could be as high as 80% to 95%.11,12
Abstinence Motivation for Drug Use
Abstinence motivation refers to the motivation to engage in and abstain from drug use.13 It is a key determinant in the interdiction of psychological addiction.7,13 Numerous researchers have emphasized the importance of motivation in shaping patterns and outcomes related to substance use and relapse.14,15 Abstinence motivation is also one of the strongest predictors of positive treatment outcomes of substance use.13,16 Thus, exploring the psychosocial factors associated with abstinence motivation is important to prevent relapse behaviour. The identified factors can also guide the development of effective treatment services for people who use drugs.
Factors of Abstinence Motivation
Previous studies have found that intrapersonal factors, such as life satisfaction, positive self-concept, and adaptive coping styles, interpersonal factors, such as the number of network members in recovery, and low levels of stigma (eg, self-stigma or public stigma) could enhance abstinence motivation of drug use.16–18 However, few studies have investigated the roles of impulsivity, social support, and mental health problems in abstinence motivation.
Impulsivity
Impulsivity refers to the inability to inhibit behaviours that may have negative consequences and be inconsiderate of outcomes before acting.19 High impulsivity is also characterised by a preference for delay reward discounting. Impulsive individuals tend to perform more risk-taking behaviours, be impatient, and have a lack of attention span.19 Impulsivity is a risk factor of drug use and relapse.20 Abstaining from drugs requires active and sustained response suppression to resist the temptation of rewarding effects and pleasure of drugs.21 Thus, impulsivity may enhance one’s craving for drugs and weaken the abstinence motivation after the rehabilitation treatment.
Perceived Social Support
Social support is a well-documented stress buffer and protective factor against drug use and relapse.6,22 A study conducted in the United States reported that positive interpersonal interactions, such as getting along with family members and helping each other, significantly decreased the chance of relapse among substance abusers at a post-treatment 6-month follow-up.23 Another study following 535 drug abusers at compulsory rehabilitation treatment for 6 months in China found that greater social support predicted a lower risk of relapse.24 Drug users who perceive social support and warmth especially from family and important others may have more coping resources for stress.25 Thus, they do not need to rely on drugs for stress coping. Perceiving social support may also reduce depression, loneliness and enhance the sense of belongingness and motives of being healthy,26–28 thus enhancing abstinence motivation of drug use.
Mental Health Problems
Depression, anxiety and sleep problem are common mental health problems that can lead to various behavioral problems including drug use and relapse.29–31 Drug use is often used as a coping behavior to relieve or escape from negative emotions and stress.32 Theories of addiction also suggest that acute and chronic stress could increase vulnerability to drug use and relapse. For example, the stress-coping model of addiction suggests that drug is used as a maladaptive coping strategy to reduce negative affect and increase positive affect.33 Drug addicts may find relapse to substances a way to deal with their sleep problems and negative feelings. Mental health problems may also affect risk-related expectations and decision-making which would lead to drug use and relapse.34 Sleep and emotional difficulties during abstinence can lead to aggression, irritability, and restlessness.35 In a study with 102 cannabis-dependent patients, those with poor sleep quality had less reduction in cannabis use during the course of a 6-month self-guided cessation attempt compared to those with good sleep quality;36 among 55 patients who finished treatment, poor sleep quality predicted relapse within the first 2 days after treatment.37 However, we have not identified any studies testing whether poor sleep quality would reduce the abstinence motivation of people who use drugs. We only identified one recent study which found that anxiety was negatively associated with drug abstention motivation in Chinese males with substance use disorders.38
The Mediation Model of Abstinence Motivation
Furthermore, mental health problems may play as a proximal mediator that can explain why impulsivity reduces and social support enhances abstinence motivation. The risk effect of impulsivity and the protective effect of social support on mental health problems have been well documented in people who use drugs and general populations.39,40 Impulsivity is a distinct personality factor that may contribute to stress,41 suicide,40 and the onset of emotional problems,42 while social support can provide individuals with a sense of belonging, reduce feelings of isolation and loneliness, and increase coping resources during difficult times which is particularly important for those who are experiencing mental health challenges.43 Thus, it can be expected that impulsivity and social support may affect mental health problems which in turn contribute to abstinence motivation of drug use.
The Present Study
We only identified one study testing the role of anxiety in abstinence motivation of drug use;38 no study tested the roles of depression, sleep problems, impulsivity, and social support in abstinence motivation. We did not find any study testing the mediation effects of mental problems on the relationships from impulsivity and social support to abstinence motivation. To fill these research gaps, the present study aims to investigate the prevalence/levels of depression, anxiety, sleep quality, impulsivity, and social support and their associations with abstinence motivation of drug use among Chinese drug use patients after community-based rehabilitation treatment. It is hypothesized that higher levels of depression, anxiety, poor sleep quality, and impulsivity would be associated with lower abstinence motivation, while greater social support would be associated with higher abstinence motivation.
In China, a 2-year isolated compulsory drug rehabilitation is the most common service for people who use drugs. Since the Anti-Drug Law of the People’s Republic of China was enacted in 2007, local governments have been encouraged to provide residents with community-based drug rehabilitation and recovery programmes. Individuals who register voluntarily are arrested due to illicit drug abuse, or have completed isolated compulsory drug rehabilitation treatment are required to join community-based rehabilitation programs.44 The current study included a sample of those who completed such rehabilitation programs.
Materials and Methods
Participants and Data Collection
Participants were recruited from 11 communities located in Wenzhou City, Zhejiang Province, China. The inclusion criteria of this study were: 1) Chinese residents with a history of drug dependence; 2) who completed the community-based drug rehabilitation treatment. The exclusion criteria included: 1) non-Chinese speakers; and 2) being physically and/or cognitively unfit for the interview. The community social workers, who worked for the community-based drug rehabilitation and recovery programmes, invited 254 participants by phone and made an appointment for an individual interview. During the interview, 230 participants completed a structural and anonymous questionnaire in a counselling room in the community and with the assistance of a well-trained research assistant and a social worker. Each participant was informed that their participation was voluntary, and refusal to participate would not result in any negative consequences on their received community service. Data confidentiality was guaranteed, and only the researchers of this study could access the data. The data were collected from April to June 2021. Of the 230 participants who completed the survey, eight (6.5%) were excluded from the data analysis because more than 20% of the data were missing from one or more scales of the key study variables. The remaining 222 (93.5%) were used for the final analysis. No significant differences in socio-demographic characteristics were found between participants included and excluded from the data analysis (P > 0.0.5).
Ethics Approval and Consent to Participate
The study was approved by the Ethics Committee of the affiliated Kangning Hospital, Wenzhou Medical University (Reference No. KNLL-20201011002). Participants signed informed consent. Participation was voluntary and anonymous. The study was conducted according to the Declaration of Helsinki.
Measures
Depressive Symptoms
The 20-item Self-rating Depression Scale (SDS)45 was used to assess depression over the past week. It is rated on a 4-point Likert scale (1 = never to 4 = always), with a higher score implying higher levels of depression. The standard raw total score (raw total score * 1.25) was used to calculate the prevalence of depression, and the cut-off points of 53, 63, and 73 represent the thresholds for mild, moderate, and major depression, respectively.46 The scale has been validated in Chinese populations.47 (Cronbach’s α=0.86 in the current sample)
Anxious Symptoms
The 20-item Self-rating Anxiety Scale (SAS)48 was used to assess anxiety. It has been validated among the Chinese population.47 Items were rated on a 4-point Likert scale (1 = never to 4 = always). A higher score implies a higher level of anxiety. The standard raw total score was used to calculate the prevalence of anxiety; the cut-off points of 50, 60, and 70 represent the thresholds for mild, moderate, and severe anxiety, respectively.47 (Cronbach’s α=0.86 in the current sample)
Quality of Sleep
The 18-item Pittsburgh Sleep Quality Index was used to evaluate sleep quality in the past month.49 Items are rated on a 4-point Likert scale (0 = Not during the past month to 3 = Three or more times a week). The total score ranges from 0 to 21, with higher scores representing lower sleep quality. The cut-off points of 5 and 7 represent the thresholds for the general and poor sleep quality, respectively. This scale has been used in Chinese populations.50 (Cronbach’s α=0.93 in the current sample)
Impulsivity
Impulsivity was assessed by the 30-item Chinese-version Barratt impulsivity Scale.51 It is rated on a 5-point Likert scale (1 = never to 5 = always). The total score ranges from 30 to 150, with higher scores representing a higher level of impulsivity. (Cronbach’s α=0.89 in the current sample)
Perceived Social Support
Perceived social support was measured by the 12-item Perceived Social Support Scale, which contains three subscales, including social support from family, friends, and significant others.52 The scale is rated on a 7-point response scale (1 = strongly disagree to 7 = strongly agree), with a higher total score indicating a higher level of perceived social support. This scale showed good reliability in Chinese populations.53 (Cronbach’s α=0.92 for Family Support, 0.92 for Friends Support, and 0.91 for Significant Others Support in the current sample)
Abstinence Motivation to Drugs
The 36-item Abstinence Motivation Scale was used to measure participants’ abstinence motivation to drugs.54 Items are rated on a 5-point Likert scale (1 = totally disagree to 5 = totally agree). Total scores range from 36 to 180. A higher score indicates higher levels of internal and external motivation and confidence for abstinence. The scale has been validated among the Chinese population.54 (Cronbach’s α=0.99 in the current sample)
Statistical Analysis
Descriptive statistics were conducted for all the variables. Univariate linear regression models were used to examine the association between each background factor and abstinence motivation. Univariable and multivariable linear regression models were applied to investigate the associations between psychosocial factors (ie, depressive symptoms, anxious symptoms, quality of sleep, impulsivity and perceived social support) and abstinence motivation after adjusting for the significant background factors.
Structural equation modelling (SEM) was conducted to test the proposed mediation model. Scores of depression, anxiety, and poor sleep quality were used as indicators for mental problems (latent variable). The items of impulsivity and abstinence motivation to drugs were randomly bundled into three parcels for the latent variables, respectively. The measurement model was tested using confirmatory factor analysis (CFA). The structural model was tested by SEM. χ2/df ≤3, the Comparative Fit Index (CFI) >0.95, the Tucker-Lewis Index (TLI) >0.95, the Root Means Square Error of Approximation (RMSEA) and the Standardized Root Mean Square Residual (SRMR)<0.08 were considered as good model fit.55,56 The 95% confidence interval (CI) of the indirect effects was based on 5000 bias-corrected bootstrap samples. The magnitude of the effect sizes was assessed by the standardized coefficients (β). β = 0.10, 0.30 and 0.50 were considered as small, medium, and large effect sizes for direct path coefficients,57 and β = 0.01, 0.09 and 0.25 as small, medium, and large effect sizes for indirect path coefficients.58 According to 10 observations per indicator variable in setting a lower bound of an adequate sample size for SEM,59 our sample size was sufficient for these analyses. The analyses were conducted by SPSS 23.0 and Mplus 7.4. The significance level was set at p < 0.05.
Results
Descriptive Characteristics
Participants were primarily male (89.2%), without a family history of mental disorder (96.8%) or physical disease (88.0%). Around 16.7% of the participants were 35 years old or younger, and 44.1% were between 36 and 45 years. The whole sample’s average years of school attainment were 7.61 (SD = 2.89). Nearly half (53.2%) of the participants were married. About 23.3% of participants were gamblers, and 94.3% were tobacco users (Table 1).
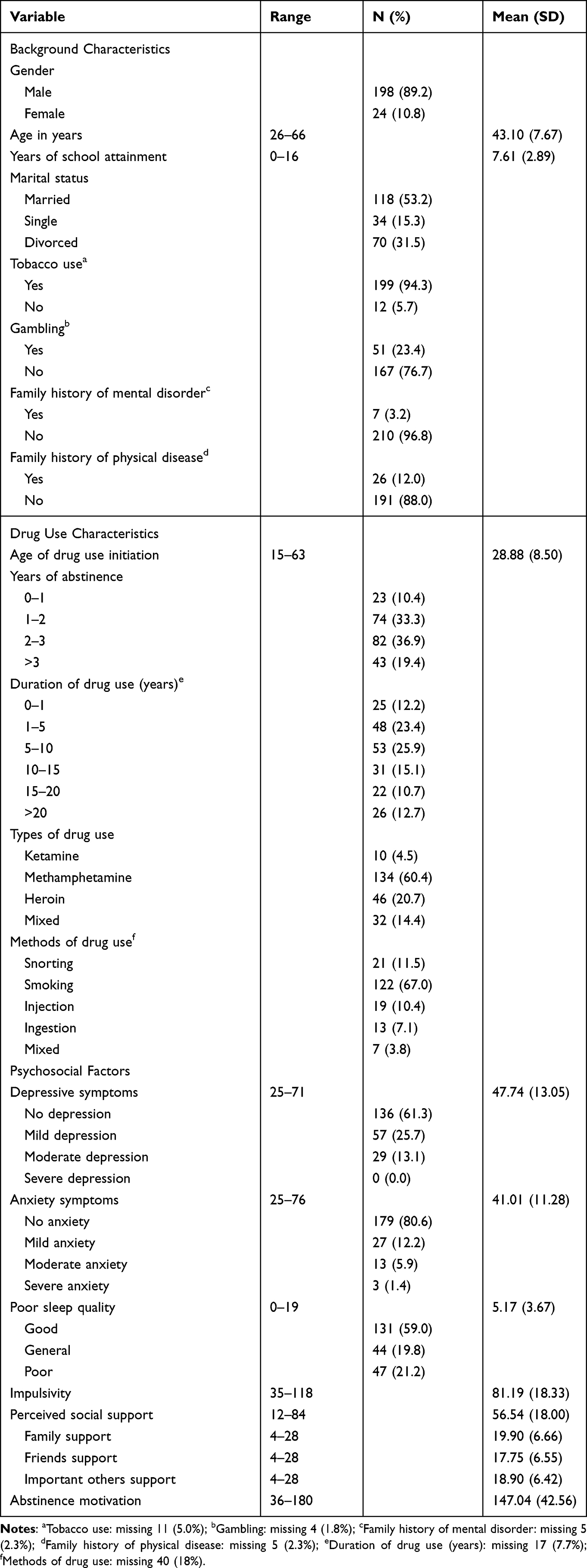 |
Table 1 Description of Background Characteristics, Psychosocial Factors, and Abstinence Motivation of the Participants (N = 222) |
Before the treatment, Methamphetamine was the most popular type of drug (60.4%), followed by Heroin (20.7%) in this sample. The methods of drug use were smoking (67.0%), snorting (11.5%), injection (10.4%) and ingestion (7.1%). On average, the participants had used the drugs for 10 years (SD = 7.74). And the mean of years abstaining from the drugs was 2.85 (SD = 1.71). The mean score of abstinence motivation was 20.42 (SD = 5.92).
Among 222 participants, 57 (25.7%) of them reported a mild level of depressive symptoms while 29 (13.1%) of them reported a moderate level of symptoms. In addition, the number of participants with mild, moderate, and severe anxious symptoms were 27 (12.2%), 13 (5.9%) and 3 (1.4%), respectively. It was also shown that 47 (21.2%) participants had poor sleep quality.
Background Factors Associated with Abstinence Motivation
Age was negatively associated with abstinence motivation (βu=−0.20, p < 0.01). Having a family history of physical disease was positively associated with motivation for abstaining from drugs (βu=0.14 p < 0.05). Other background factors did not significantly affect abstinence motivation.
Psychosocial Factors Associated with Abstinence Motivation
Depressive symptoms (βa=−0.28, p < 0.001), anxiety symptoms (βa=−0.24, p < 0.001), poor sleep quality (βa=−0.23, p < 0.01), impulsivity (βa=−0.29, p < 0.001) were negatively associated with abstinence motivation, respectively. Perceived family support (βa=0.17, p < 0.05) and perceived important others support (βa=0.16, p < 0.05) were positively associated with abstinence motivation, respectively. When adjusting for other psychosocial factors, only impulsivity was still significantly associated with abstinence motivation (βa=−0.19, p < 0.001; Table 2).
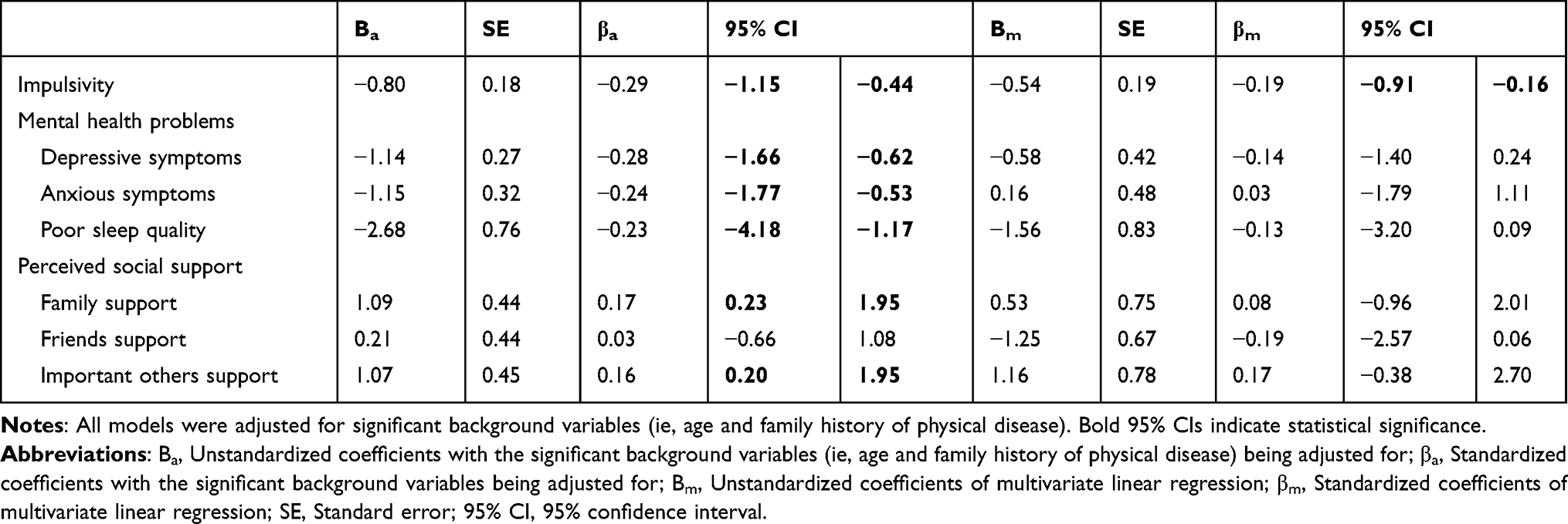 |
Table 2 Associations Between Psychosocial Factors and Abstinence Motivation (N = 222) |
Structural Equation Modelling
The measurement model yielded a good fit: χ2/df = 1.78, CFI = 0.98, TLI = 0.97, RMSEA = 0.06 (95% CI = 0.04, 0.08), SRMR = 0.04. All the parcel indicators were significantly loaded on the latent variables, with standardized factor loading ranging from 0.50 to 0.99 (all p < 0.001). The structural model fitted the data well: χ2/df=1.75, CFI = 0.98, TLI = 0.97, RMSEA = 0.06 (95% CI = 0.04, 0.08), SRMR = 0.05. As shown in Figure 1, the direct effect of impulsivity (β= −0.21, 95% CI = −0.35, −0.06) on abstinence motivation was significant. Mental problems significantly mediated the associations between impulsivity (βindirect = −0.08, 95% CI = −0.16, −0.02)/perceived social support (βindirect = 0.04, 95% CI = 0.01, 0.11) and abstinence motivation.
 |
Figure 1 A structural equation modeling model explaining the mediating role of mental health problems in the associations between impulsivity, perceived social support and abstinence motivation. Notes: The standardized path coefficients were shown in the figure. The background variables having associations with abstinence motivation with p < 0.05 (ie, age and having a family history of physical disease) were controlled for. **p < 0.01, ***p < 0.001. The dashed arrow means p ≥ 0.05; the solid arrow means p <0.05. |
Discussion
This study is the first attempt to investigate multiple psychosocial factors of abstinence motivation in ex-drug use patients who have completed community rehabilitation treatments in China. The results generally support our hypotheses, while unexpected findings were also identified.
Our results showed that, after the community-based drug rehabilitation treatment, the prevalence of depression, anxiety and poor sleep quality among the participants were 38.8%, 19.5%, and 21.2%, respectively. With the same assessment tools, the prevalence of depression and anxiety was higher than those reported in general Chinese population (depression ranged from 16.3% to 31%; anxiety ranged from 1.5% to 8.7%),60–63 while the prevalence of poor sleep quality was comparable with those reported in the general Chinese population (26.4%).64
Furthermore, we demonstrated that these mental health problems were negatively associated with abstinence motivation of drug use and mediated the effects of impulsivity and social support on abstinence motivation. Drug use has been a well-documented maladaptive coping behaviour to stress and mental difficulties.65 Individuals who rely on drugs as a means of coping with these emotional and mental problems would be less likely to have motivation to abstain from drugs. The findings suggest that effective treatment (eg, cognitive behavioural treatment (CBT)) and follow-up service targeting mental health problems for people who used drugs should be helpful for reinforcing their abstinence motivation and preventing relapse of drug use.
Individuals with high impulsivity and low social support would be more vulnerable to mental health problems. We found that social support was positively associated with abstinence motivation in regression and indirectly via mental health problems in SEM. Enhancing social support is an effective strategy in addiction treatment.66 It is also a well-documented protective factor of help-seeking and treatment adherence for addictive behaviors (eg,67,68). Proper emotional and instrumental support, encouragement, and help, especially from family members and other significant others (eg, healthcare professionals), could give patients a sense of inclusion, security and belongingness, which aids them in coping with distress and difficulties, and develop positive prospect in life69 and thus enhances drug abstinence self-efficacy and commitment. Our findings corroborate previous studies on drug use treatment11 and suggest that rehabilitation services should enhance proper interpersonal social support of people who used drugs and provide a supportive interpersonal system to enhance their abstinence motivation and maintain the treatment effect. However, friend support was not significantly correlated with abstinence motivation in this sample. Previous studies have discussed the complex role of friends and peers in drug use and relapse. For example, a longitudinal study with 206 males testing the relationship between adolescence and adulthood’s peer influence and substance use reported that adulthood substance use was affected by peers in adolescence, specifically deviant friendships.70 The number of network members in recovery was positively associated with abstinence motivation.17 Hence, it is important to further explore which kinds of friends provided support and what types of support they provided to understand the role of friend support better.
It is worth noting that impulsivity showed robust associations with abstinence motivation in both univariate and multivariate models and SEM (both directly and indirectly). It is theorised that impulsivity leads to risk-taking and poor decisions, making it a major risk for drug use and relapse under conditions that impair an individual’s inhibition responses, such as stressful events or cues to substance use.71–73 It has been documented that people with higher impulsivity are more likely to engage in drug use behaviours.74 This study is the first to further extend our understanding of the effect of impulsivity on abstinence motivation which may affect one’s treatment intention and adherence and future relapse. The significant direct effect of impulsivity in SEM suggests that in addition to mental health problems, there may exist other mediators between impulsivity and abstinence motivation, such as sensation-seeking and craving for drugs. Future studies may explore these potential mediators. Rehabilitation interventions should take this intrapersonal factor into account and teach them skills to cope with patients’ rash-spontaneous behaviours, enhance their self-control, and guide them to explore alternative rewards that are healthier (eg, physical activity). Mindfulness-based interventions have been found to effectively redress impulsive patterns derived from inhibitory motor control or planning capacity deficits and benefit mental health. Cognitive behavioral therapy that provides training for patients’ self-regulation skills and motivational interviewing that aims to enhance patients’ self-change motivation may also be helpful.
The participants who were older and had no family history of physical disease had lower levels of abstinence motivation and should be paid particular attention. However, it is inconsistent with the previous finding that younger people are more likely to relapse than older people.75 One plausible reason is that the survey was conducted during COVID-19, which might increase the risk of relapse among older people because they experienced more stress (eg, worrying about health, finance and job and social isolation), were more difficult to adjust, and had fewer coping resources than younger people.76 In addition, older people may have a longer history of drug use and heavier dependence on drugs, which would also reduce their abstinence motivation. People with a family history of physical disease may concern more about their health and have greater motivation to adopt healthy lifestyles,77 which, in turn, motivates them to abstain from drugs.
The study had several limitations. First, the cross-sectional design could not demonstrate the causal relationships between the psychosocial variables and the outcome. Their relationships can be reciprocal. For example, low abstinence motivation to drugs may lead to relapse and aggravate emotional problems. Longitudinal study design and cross-lagged model to comprehensively investigate their longitudinal relationships are warranted. Future studies should also monitor during and post-treatment changes in the study variables. This would help quantify the impact of rehabilitation services on these areas and inform future service development. Also, the study sample was recruited in one city in China, ensuring the homogeneity of the rehabilitation program the participants attended. However, our findings may not be applicable to people in other geographical locations. Last but not least, we did not include drug use relapse as a variable or confounder although it is closely related to our outcome. It is because it is a sensitive question and almost all the participants chose not to disclose this status.
Conclusions
The high prevalence of mental health problems in people who completed community rehabilitation treatments should be paid attention to and well addressed. Significant risk factors of abstinence motivation included older age, no family history of physical disease, mental health problems, impulsivity, and low perceived social support from family and significant others. Impulsivity was directly and indirectly associated with abstinence motivation via mental health problems, while the indirect effect of social support was significant. Rehabilitation programs and follow-up services should consistently monitor the prevalence of mental health problems and drug use relapse, and address the modifiable psychosocial factors to enhance the abstinence motivation of people who used drugs and the long-term effectiveness of the treatment.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author, X.Y. The data are not publicly available due to their containing information that could compromise the privacy of research participants. No data will be shared which would disclose identifying patient information.
Ethics Approval and Informed Consent
The study was approved by the Ethics Committee of the affiliated Kangning Hospital, Wenzhou Medical University (Reference No. KNLL-20201011002). Participants signed informed consent. Participation was voluntary and anonymous. The study was conducted according to the Declaration of Helsinki. Informed consent was obtained from all subjects involved in the study.
Consent for Publication
All authors listed agree to publish the current study.
Acknowledgments
We sincerely thank all the authors who contributed to this manuscript.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
No funding was received for the study.
Disclosure
The authors declare no conflict of interest.
References
1. Huang Y, Wang Y, Wang H. Prevalence of mental disorders in China: a cross-sectional epidemiological study (vol 6, pg 211, 2019). Lancet Psychiat. 2019;6(4):E11–E. doi:10.1016/S2215-0366(18)30511-X
2. Kivimaki M, Batty GD, Pentti J, et al. Association between socioeconomic status and the development of mental and physical health conditions in adulthood: a multi-cohort study. Lancet Public Health. 2020;5(3):E140–E149. doi:10.1016/S2468-2667(19)30248-8
3. Liu YSX, Fan YL, Huang ZP, et al. Determination of ketamine, methamphetamine and 3,4-methylenedioxymethamphetamine in human hair by flash evaporation-gas chromatography/mass spectrometry. J Chromatogr B. 2020;1153:122275. doi:10.1016/j.jchromb.2020.122275
4. United Nations Office on Drugs and Crime. World drug report 2021; 2021:109.
5. Liu N, Lu ZK, Xie Y. Tracking study on the relapse and aftercare effect of drug patients released from a Compulsory Isolated Detoxification Center. Front Psychiatry. 2022;12. doi:10.3389/fpsyt.2021.699074
6. Atadokht A, Hajloo N, Karimi M, Narimani M. The role of family expressed emotion and perceived social support in predicting addiction relapse. Int J High Risk Behav Addict. 2015;4(1):e21250–e. doi:10.5812/ijhrba.21250
7. Andersson HW, Wenaas M, Nordfjaern T. Relapse after inpatient substance use treatment: a prospective cohort study among users of illicit substances. Addict Behav. 2019;90:222–228. doi:10.1016/j.addbeh.2018.11.008
8. Wasserman D, Iosue M, Wuestefeld A, Carli V. Adaptation of evidence-based suicide prevention strategies during and after the COVID-19 pandemic. World Psychiatry. 2020;19(3):294–306. doi:10.1002/wps.20801
9. Liu Z, Lian ZHI, Zhao C. Drug use and HIV/AIDS in China. Drug Alcohol Rev. 2006;25(2):173–175. doi:10.1080/09595230500538835
10. Office of China National Narcotic Control Commission. Drug situation in China 2019. China; 2020.
11. Rong C, Jiang H, Zhang R, et al. Factors associated with relapse among heroin addicts: evidence from a two-year community-based follow-up study in China. Int J Environ Res Public Health. 2016;13(2):177. doi:10.3390/ijerph13020177
12. Liu L, Chui WH. Rehabilitation policy for drug addicted offenders in China: current trends, patterns, and practice implications. Asia Pac J Soc Work Dev. 2018;28(3):192–204. doi:10.1080/02185385.2018.1482779
13. Moore JP, Hardy SA. Longitudinal relations between substance use abstinence motivations and substance use behaviors in adolescence: a self-determination theory approach. J Pers. 2020;88(4):735–747. doi:10.1111/jopy.12522
14. LeClair A, Kelly BC, Pawson M, Wells BE, Parsons JT. Motivations for prescription drug misuse among young adults: considering social and developmental contexts. Drugs. 2015;22(3):208–216.
15. Starks TJ, Golub SA, Kelly BC, Parsons JT. The problem of “just for fun”: patterns of use situations among active club drug users. Addict Behav. 2010;35(12):1067–1073. doi:10.1016/j.addbeh.2010.07.007
16. Chen M, Zeng X, Chen Y. Self-concept and abstinence motivation in male drug addicts: coping style as a mediator. Soc Behav Person. 2020;48(7):e9334. doi:10.2224/sbp.9334
17. Laudet AB, Stanick V. Predictors of motivation for abstinence at the end of outpatient substance abuse treatment. J Subst Abuse Treat. 2010;38(4):317–327. doi:10.1016/j.jsat.2010.01.007
18. Chang KC, Lin CY, Chang CC, Ting SY, Cheng CM, Wang JD. Psychological distress mediated the effects of self-stigma on quality of life in opioid-dependent individuals: a cross-sectional study. PLoS One. 2019;14(2):e0211033.
19. Perry JL, Carroll ME. The role of impulsive behavior in drug abuse. Psychopharmacology. 2008;200(1):1–26. doi:10.1007/s00213-008-1173-0
20. Davis JP, Barr N, Dworkin ER, et al. Effect of mindfulness-based relapse prevention on impulsivity trajectories among young adults in residential substance use disorder treatment. Mindfulness. 2019;10(10):1997–2009. doi:10.1007/s12671-019-01164-0
21. Poulton A, Hester R. Transition to substance use disorders: impulsivity for reward and learning from reward. Soc Cognit Affective Neurosci. 2020;15(10):1182–1191. doi:10.1093/scan/nsz077
22. Sharma AK, Upadhyaya SK, Bansal P, Sharma MNDK. A study of factors affecting relapse in substance abuse. Indian J Life Sci. 2012;2:28–33.
23. Ellis B, Bernichon T, Yu P, Roberts T, Herrell JM. Effect of social support on substance abuse relapse in a residential treatment setting for women. Evaluat Prog Plann. 2004;27(2):213–221. doi:10.1016/j.evalprogplan.2004.01.011
24. Xiong H, Jia J. Situational social support and relapse: an exploration of compulsory drug abuse treatment effect in China. Int J Offend Ther Compar Criminol. 2018;63(8):1202–1219. doi:10.1177/0306624X18815243
25. Thoits PA. Social support as coping assistance. J Consult Clin Psych. 1986;54(4):416–423. doi:10.1037/0022-006X.54.4.416
26. Draper CE, Grobler L, Micklesfield LK, Norris SA. Impact of social norms and social support on diet, physical activity and sedentary behaviour of adolescents: a scoping review. Child Care Hlth Dev. 2015;41(5):654–667. doi:10.1111/cch.12241
27. Saltzman LY, Hansel TC, Bordnick PS. Loneliness, isolation, and social support factors in post-COVID-19 mental health. Psychol Trauma. 2020;12(S1):S55–S57. doi:10.1037/tra0000703
28. Chang CW, Chang KC, Griffiths MD, Chang CC, Lin CY, Pakpour AH. The mediating role of perceived social support in the relationship between perceived stigma and depression among individuals diagnosed with substance use disorders. J Psychiatr Ment Hlt. 2022;29(2):307–316.
29. Saffari M, Chang KC, Chen JS, et al. Temporal associations between depressive features and self-stigma in people with substance use disorders related to heroin, amphetamine, and alcohol use: a cross-lagged analysis. BMC Psychiatry. 2022;22(1). doi:10.1186/s12888-022-04468-z
30. Liu L, Cao QL. Perceived stress and sleep quality among Chinese drug users: analysis of rumination as a mediator and resilience as a moderator. Int J Ment Health Ad. 2020;20:569–580.
31. Chang KC, Chen HP, Huang SW, et al. Comparisons of psychological distress and self-stigma among three types of substance use disorders receiving treatment-as-usual approaches: real-world data from a 9-month longitudinal study. Ther Adv Chronic Dis. 2022;13:204062232211403. doi:10.1177/20406223221140393
32. Sinha R. The role of stress in addiction relapse. Curr Psychiatry Rep. 2007;9(5):388–395. doi:10.1007/s11920-007-0050-6
33. Wills TA, Shiffman S, editors. Coping and Substance Use: A Conceptual Framework. Academic Press; 1986.
34. Chakravorty S, Vandrey RG, He S, Stein MD. Sleep management among patients with substance use disorders. Med Clin N Am. 2018;102(4):733. doi:10.1016/j.mcna.2018.02.012
35. Budney AJ, Hughes JR, Moore BA, Novy PL. Marijuana abstinence effects in marijuana smokers maintained in their home environment. Arch Gen Psychiatry. 2001;58(10):917–924. doi:10.1001/archpsyc.58.10.917
36. Babson KA, Boden MT, Bonn-Miller MO. The impact of perceived sleep quality and sleep efficiency/duration on cannabis use during a self-guided quit attempt. Addict Behav 2013;38(11):2707–2713. doi:10.1016/j.addbeh.2013.06.012
37. Babson KA, Boden MT, Harris AH, Stickle TR, Bonn-Miller MO. Poor sleep quality as a risk factor for lapse following a cannabis quit attempt. J Subst Abuse Treat. 2013;44(4):438–443. doi:10.1016/j.jsat.2012.08.224
38. Li Y, Zeng X, Zhou H. Relationship between anxiety and drug abstention motivation in men with substance use disorders: a cross-sectional study of compulsory isolation rehabilitation in China. J Ethnic Subs Abuse. 2021;22(1):1–24.
39. Grant JE, Lust K, Chamberlain SR. Problematic smartphone use associated with greater alcohol consumption, mental health issues, poorer academic performance, and impulsivity. J Behav Addict. 2019;8(2):335–342. doi:10.1556/2006.8.2019.32
40. Yuodelis‐Flores C, Ries RK. Addiction and suicide: a review. Am J Addict. 2015;24(2):98–104. doi:10.1111/ajad.12185
41. Kreek MJ, Nielsen DA, Butelman ER, LaForge KS. Genetic influences on impulsivity, risk taking, stress responsivity and vulnerability to drug abuse and addiction. Nat Neurosci. 2005;8(11):1450–1457. doi:10.1038/nn1583
42. Granö N, Keltikangas‐Järvinen L, Kouvonen A, et al. Impulsivity as a predictor of newly diagnosed depression. Scandinavian J Psychol. 2007;48(2):173–179. doi:10.1111/j.1467-9450.2007.00566.x
43. Lambert NM, Stillman TF, Hicks JA, Kamble S, Baumeister RF, Fincham FD. To belong is to matter: sense of belonging enhances meaning in life. Person Soc Psychol Bull. 2013;39(11):1418–1427. doi:10.1177/0146167213499186
44. Liu L, Hsiao SC, Kaplan C. Drug initiation of female detainees in a compulsory drug treatment institution in China. J Psychoactive Drugs. 2016;48(5):393–401. doi:10.1080/02791072.2016.1234088
45. Zung WW. A self-rating depression scale. Arch Gen Psychiatry. 1965;12(1):63–70. doi:10.1001/archpsyc.1965.01720310065008
46. Xiao Y, Xie TJ, Peng JX, et al. Factors associated with anxiety and depression in patients with erectile dysfunction: a cross-sectional study. BMC Psychol. 2023;11(1). doi:10.1186/s40359-023-01074-w
47. Zhang Z. Handbook of Behavioral Medicine Scales: China Medical Electronic. Audio-visual Publishing House; 2005.
48. Zung WW. A rating instrument for anxiety disorders. Psychosomatics. 1971;12(6):371–379. doi:10.1016/S0033-3182(71)71479-0
49. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
50. Liu X. Reliability and validity of the Pittsburgh Sleep Quality Index. Chin J Psychiatry. 1996;29:103–107.
51. Li X, Fei L, Xu D, et al. Reliability and validity of the Chinese revised version of Barratt Impulsivity Scale in community and university populations. Chin J Ment Health. 2011;25(08):610–615.
52. Zimet GD, Dahlem NW, Zimet SG, Farley GK. The multidimensional scale of perceived social support. J Person Assess. 1988;52(1):30–41. doi:10.1207/s15327752jpa5201_2
53. Huang Y, Wu R, Wu J, Yang Q, Zheng S, Wu K. Psychological resilience, self-acceptance, perceived social support and their associations with mental health of incarcerated offenders in China. Asian J Psychiatry. 2020;52:102166. doi:10.1016/j.ajp.2020.102166
54. Wu X, Zeng H, Li L, Chen Y. The structure and scale of abstinence motivation. Chin J Drug Depend. 2008;17(6):465–468.
55. Hu LT, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equation Model. 1999;6(1):1–55. doi:10.1080/10705519909540118
56. Kline RB. Principles and Practice of Structural Equation Modeling.
57. Sanders T, Parker PD, Del Pozo-Cruz B, Noetel M, Lonsdale C. Type of screen time moderates effects on outcomes in 4013 children: evidence from the Longitudinal Study of Australian Children. Int J Behav Nutr Phy. 2019;16(1). doi:10.1186/s12966-019-0881-7
58. Kenny D. Effect size of the indirect effect and the computation of power; 2021. Available from: http://davidakenny.net/cm/mediate.htm.
59. Nunnally J, Bernstein I. McGraw-Hill series in psychology. In: Psychometric Theory. New York, NY, US: McGraw-Hill; 1967.
60. Yu B, Gu YQ, Bao X, et al. Distinct associations of computer/mobile devices use and TV watching with depressive symptoms in adults: a large population study in China. Depress Anxiety. 2019;36(9):879–886. doi:10.1002/da.22932
61. Zhang LY, Yin JJ, Cai XF, Li W, Feng LD, Cheng X. Association between eating behaviors and depressive symptoms in Chinese adults: a population-based cross-sectional study. Psychol Health Med. 2022;27(5):1176–1183. doi:10.1080/13548506.2021.1922720
62. Jia ZX, Du X, Du J, et al. Prevalence and factors associated with depressive and anxiety symptoms in a Chinese population with and without cardiovascular diseases. J Affect Disord. 2021;286:241–247. doi:10.1016/j.jad.2021.02.006
63. Zheng D, Liu P, Chen H, Wang X, Li J. Worse psychological traits associated with higher probability of emotional problems during the Omicron pandemic in Tianjin, China. Eur J Psych. 2023;37:84–91 doi:10.1016/j.ejpsy.2022.09.002.
64. Liu RQ, Qian ZM, Trevathan E, et al. Poor sleep quality associated with high risk of hypertension and elevated blood pressure in China: results from a large population-based study. Hypertens Res. 2016;39(1):54–59 doi:10.1038/hr.2015.98.
65. Chen M, Zeng X, Chen Y. Self-concept and abstinence motivation in male drug addicts: coping style as a mediator. Soc Behav Person. 2020;48(7):1–15 doi:10.2224/sbp.9334.
66. Kelly SM, O’Grady KE, Schwartz RP, Peterson JA, Wilson ME, Brown BS. The relationship of social support to treatment entry and engagement: the community assessment inventory. Subst Abuse. 2010;31(1):43–52. doi:10.1080/08897070903442640
67. Westmaas JL, Bontemps-Jones J, Bauer JE. Social support in smoking cessation: reconciling theory and evidence. Nicotine Tob Res. 2010;12(7):695–707. doi:10.1093/ntr/ntq077
68. Marquez B, Anderson A, Wing RR, et al. The relationship of social support with treatment adherence and weight loss in Latinos with type 2 diabetes. Obesity. 2016;24(3):568–575. doi:10.1002/oby.21382
69. Zaidi U. Role of social support in relapse prevention for drug addicts. Int J Innov Creat Change. 2020;13(1):915–924.
70. Dishion TJ, Owen LD. A longitudinal analysis of friendships and substance use: bidirectional influence from adolescence to adulthood. Dev Psychol. 2002;38(4):480–491. doi:10.1037/0012-1649.38.4.480
71. Pattij T, De Vries TJ. The role of impulsivity in relapse vulnerability. Curr Opin Neurobiol. 2013;23(4):700–705. doi:10.1016/j.conb.2013.01.023
72. Adinoff B, Rilling LM, Williams MJ, et al. Impulsivity, neural deficits, and the addictions. J Addict Dis. 2007;26(sup1):25–39. doi:10.1300/J069v26S01_04
73. Reyes-Huerta HE, Dos Santos C, Martínez K. Impulsive mechanisms influencing relapse in alcohol drinking. Med Hypotheses. 2018;112:27–29. doi:10.1016/j.mehy.2018.01.007
74. Dawe S, Loxton NJ. The role of impulsivity in the development of substance use and eating disorders. Neurosci Biobehav R. 2004;28(3):343–351. doi:10.1016/j.neubiorev.2004.03.007
75. Rollins AL, Neill SJ O, Davis KE, Devitt TS. Special section on relapse prevention: substance abuse relapse and factors associated with relapse in an inner-city sample of patients with dual diagnoses. Psychiat Serv. 2005;56(10):1274–1281. doi:10.1176/appi.ps.56.10.1274
76. Barrick C, Connors GJ. Relapse prevention and maintaining abstinence in older adults with alcohol-use disorders. Drug Aging. 2002;19(8):583–594. doi:10.2165/00002512-200219080-00004
77. Sheeran P, Harris PR, Epton T. Does heightening risk appraisals change people’s intentions and behavior? A meta-analysis of experimental studies. Psychol Bull. 2014;140(2):511–543. doi:10.1037/a0033065
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.