")
Back to Journals » Psychology Research and Behavior Management » Volume 16
Psychosocial Challenges of the Coronavirus Disease-2019 Pandemic Among Frontline Health Care Providers and Their Coping Mechanisms at Mbarara Regional Referral Hospital, Southwestern Uganda
Authors Taremwa IM , Ashaba S , Naggayi BRK, Kayongo B, Nimwesiga C, Ayebazibwe C, Tumuhimbse M, Frank J
Received 30 November 2022
Accepted for publication 18 February 2023
Published 24 February 2023 Volume 2023:16 Pages 549—560
DOI https://doi.org/10.2147/PRBM.S399687
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Ivan Mugisha Taremwa,1 Scholastic Ashaba,2,3 Barbara Rita K Naggayi,4 Badru Kayongo,2 Christine Nimwesiga,5 Carlrona Ayebazibwe,1 Manasseh Tumuhimbse,6 John Frank7
1Institute of Allied Health Sciences, Clarke International University, Kampala, Uganda; 2Department of Psychiatry, Mbarara Regional Referral Hospital, Mbarara, Uganda; 3Faculty of Medicine, Mbarara University of Science and Technology, Mbarara, Uganda; 4Faculty of Interdisciplinary Studies, Mbarara University of Science and Technology, Mbarara, Uganda; 5Uganda Nurses and Midwives Council, Ministry of Health, Kampala, Uganda; 6Faculty of Business and Management Sciences, Mbarara University of Science and Technology, Mbarara, Uganda; 7Professorial Fellow, Usher Institute, University of Edinburgh, Edinburgh, UK
Correspondence: Ivan Mugisha Taremwa, Institute of Allied Health Sciences, Clarke International University, P.O Box 7782, Kampala, Uganda, Tel +256 774 346 368, Email [email protected]
Background: As a novel global health pandemic, Coronavirus Disease-2019 (COVID-2019) has posed various challenges to frontline healthcare providers (FHCPs). This study explored the social and psychological challenges of COVID-19 to the FHCPs at Mbarara Regional Referral Hospital, southwestern Uganda.
Methods: This was a cross-sectional study with a qualitative approach. Participants were purposively selected, consented, and interviewed. Interviews were audio-recorded and transcribed. Data were entered into NVivo 10 software and analyzed using a thematic analysis approach.
Results: Fourteen FHCPs with diverse roles, including 8 men, were interviewed. Participants’ median age was 38 years (range: 26– 51 years) and eleven of them were married. The subjects’ experiences were explored in relation to perceived social and psychological challenges of working during the COVID-19 pandemic, and coping mechanisms in the COVID-19 pandemic situation. The social challenges identified were burnout, domestic violence, and a financially constrained environment. A further, psychological challenge was anxiety, as well as fear and distress. FHCPs responded with a variety of coping mechanisms, including situational acceptance, religious coping, coping through emotional support of others, and bulk purchase of supply-constrained basic necessities.
Conclusion: FHCPs experienced numerous social and psychological challenges, which negatively affected their quality of life amidst a wavering pandemic. As the pandemic rages on, creative and low-cost psychosocial interventions for FHCPs are needed, possibly including more formal peer support, and an improved flow of information about ongoing infectious disease control interventions, so FHCPs feel more knowledgeable about what is ahead.
Keywords: psychosocial risks, COVID-19, healthcare providers, coping
Introduction
Over time, humanity has endured a myriad of outbreaks, exerting extreme pressure on health care systems.1,2 In the past two decades, viral epidemics have included: Severe Acute Respiratory Syndrome (SARS), H1N1 influenza, Middle East Respiratory Syndrome (MERS), Ebola Virus Disease (EVD), and the Coronavirus Disease 2019 (COVID-19) pandemic, occurring in 2003, 2009, 2012, 2014 and 2019, respectively.3 The SARS-CoV-2 emerged from Wuhan, Hubei province in China at the end of 2019, and in March 2020, the World Health Organization declared COVID-19 a pandemic.4
As a novel disease, COVID-19 has posed various risks to frontline healthcare providers (FHCPs). For example, there has been a high demand for personal protective equipment (PPE) (5), yet sometimes there are shortages in supply.6,7 Also, the COVID-19 pandemic strained the healthcare workforce amidst the already existing staffing challenges in Uganda, leading to long work hours and burnout.8 Moreover, strict adherence to comprehensive protocols, while caring for those infected with COVID-19,5 and other efforts to limit occupational transmission, necessitated correct and consistent use of PPE, and implementation of strict measures like social distancing interrupted social interactions and personal relationships.5,9 Furthermore, the rapid spread of SARS-CoV-2 instilled fear of contagion, stigma, and subsequent morbidity and mortality.6,10 Also, physical distancing measures to limit the spread of COVID-19 are substantially more difficult to implement in the context of healthcare provision than in many fields.11–13 In addition, compassion fatigue has been reported among frontline healthcare providers who witnessed their patients’ agony and deaths.14,15
In contrast to the previous well-controlled outbreaks, such as viral hemorrhagic fever and EVD, there is a plethora of evidence that the COVID-19 pandemic has been catastrophic in Uganda.8 For example, over-stretched healthcare facilities have been forced into critical but stressful decisions regarding who, among many very sick patients, was to be referred and managed at a tertiary healthcare facility such as Mbarara Regional Referral Hospital (MRRH). Also, transmission from neighboring countries was reported8, requiring additional scarce Ugandan healthcare resources. These consequences have been complicated by the neglect of mental health care in the public health response to the outbreak, which has been in part attributed to the fact that the Ugandan response was more focused on infectious disease control and care responses with limited consideration of psychosocial concerns.16
Whereas the State and non-State actors in Uganda provided support to ensure the safety of FHCPs, this assistance has largely been in terms of PPE, training in case management, and infection control, with few interventions focusing on mitigation of mental health challenges due to COVID-19. To date, there is limited empirical evidence on the precise psychosocial risks of COVID-19 among the FHCPs in Uganda. This study explored the psychosocial challenges of the COVID-19 pandemic among frontline health care providers at Mbarara Regional Referral Hospital, Southwestern Uganda.
Materials and Methods
Definition of Operation Terms
Frontline healthcare providers (FHCPs): this study considered FHCPs as the individuals who were both healthcare professionals (such as a physician, nurse, midwife, laboratory personnel, among others) and non-healthcare professionals (such as driver, security personnel, hygienist, among others) who supported the response to the COVID-19 pandemic within the COVID-19 isolation unit at Mbarara Regional Referral Hospital.
Compassion fatigue: the term was used to refer to physical, mental exhaustion and emotional withdrawal as a result of intimate long-term care for sick or traumatized patients over a long time.
Study Design, Site and Duration
This was a cross-sectional study with a qualitative approach. The study was conducted at Mbarara Regional Referral Hospital (MRRH), located in Mbarara City in southwestern Uganda. MRRH is 266 Km from Kampala, the capital city, and has a bed capacity of 350. Mbarara city has a total population of 472,62517 and is interlinked with about 9 border districts in western and southwestern Uganda. The city serves as a major conurbation of the western region, and a gateway to Rwanda, Burundi, Tanzania, and the Democratic Republic of Congo. The study was conducted from November 2020 to March 2021.
COVID-19 Management at MRRH
When the COVID-19 pandemic broke out in Uganda, MRRH established the only isolation, treatment, and intensive care unit (ICU) facilities for the management of patients requiring in-hospital care in the southwestern region. MRRH was also involved in contact tracing and provision of home-based care, in liaison with the district health teams and the health facilities within the region. All the patients who accessed medical care or were screened at the hospital gates and were found positive for COVID-19 were admitted to the MRRH isolation unit or the ICU, depending on the level of care required. Patient care and management were carried out by a team of physicians, nurses, laboratory staff, psychotherapists, cleaners, and guards stationed in the two admission centers. The quality improvement team at the hospital supported the infection prevention and control interventions for COVID-19 in the whole hospital.
Study Participants and Selection
The study enrolled both men and women employed as FHCPs at MRRH, based on their involvement at work in routine care and support of COVID-19 patients, or their community engagement in the control of COVID-19. As the main isolation center, MRRH had dedicated staff for the isolation unit comprising physicians, anesthesiologists, pediatricians, and family physicians. In addition, there were medical officers, critical care nurses, enrolled nurses, midwives, nursing assistants, physiotherapists, psychosocial teams, drivers, cleaners, and security guards. The study enrolled participants who were interfacing with the COVID-19 pandemic in the following occupational roles:
- Screening: the study enrolled one staff involved in the screening at the general out-patients department (OPD).
- Assessment and testing staff: We took into account one person who assessed the suspected contacts as well as one person involved in the collection of their samples and one laboratory testing staff.
- Isolation staff: In the isolation unit, the research team enrolled one nurse, one midwife, one medical officer, and two support staff (specifically, one cleaner and one security guard). In addition, three members of the contact tracing team (one doctor, two drivers, and a nurse) were considered eligible and interviewed. The medical officer and nurse who were enrolled for contact tracing were not the same participants considered eligible for treatment support and monitoring.
- Intensive care unit (ICU) staff: For this study, a nurse and a physician from this unit were considered eligible and interviewed.
Key informant interviews (KIIs) were conducted with one nurse and one medical officer who were both involved in contact tracing, as well as one medical officer and one nurse who were involved in treatment and support, and laboratory personnel. The medical officer and the nurse considered for KII were not the same individuals as in (c) above. The remaining personnel was considered eligible for in-depth interviews (IDIs).
Sampling Strategy and Enrolment Criteria
The study used a purposive sampling strategy to approach the potential participants. The research team contacted the lead physician (head of the case management team) at MRRH to help the team to identify the FHCPs. For purposes of participant mobilization and scheduling of appointments before face-to-face interviews, the research team cross-checked with respective unit in-charges to obtain their mobile telephone and email contacts. This was done to limit face-to-face interaction with the potential participant before the actual interview. This aimed to limit the chance of infection transmission. Participants were contacted by a member of the research team (IMT, CN, and CA) to coordinate the mobilization. Participants were contacted by a telephone call, with three unanswered or unreturned calls considered as “out-of-reach”. In such a circumstance, an initial email invitation was sent out to individuals who potentially and regularly communicated officially by email. A reminder was followed, after 72 hours of no reply, up to three times, and if the team did not receive a reply at all, this was considered a refusal to participate. When a participant was unable to attend due to work obligations, the interview was rescheduled for a different day. If deemed necessary and appropriate, a participant was asked to nominate another staff member with comparable knowledge and expertise, who then was contacted to schedule an interview.
Sample Size Estimation
Guided by the previous recommendation that a minimum sample size of 12 in qualitative studies can achieve data saturation,18–20 a sample size of 14 was deemed adequate for this study based on data saturation during the interviews.
Data Collection
Participants were invited by telephone call and email as described above. On the scheduled interview day, the mobilization team confirmed participant presence at least one hour earlier. On the agreed day and time, the members of the research team introduced the study to the participant and sought written informed consent. Data collection was conducted at a place outside the COVID-19 isolation unit, and at all times, national COVID-19 regulations such as hand washing/sanitizing before and after the interview, 2-meter sitting, and correct and consistent use of face masks were ensured. The interview guide found in supplementary material (Appendix 1) was used. The interview guide focused on four sections, namely: the subject’s socio-demographic characteristics; the subject’s specific exposures to risks related to the COVID-19 pandemic; and how the COVID-19 pandemic affected social aspects of the subject’s life, in terms of interactions and relationships. Also, we assessed how preventive measures had affected the interviewee’s ways of living, such as psychological reactions to the threat of the pandemic. The study also specifically inquired about how FHCPs were coping with the COVID-19 pandemic. Each interview lasted approximately 45–60 minutes, and the questions were open-ended with probes, allowing participants to shape the discussion. Additionally, questions were adapted from the initial IDIs and KIIs for use with the next interviewee, allowing an iterative approach to confirm findings and explore emerging themes in greater depth. Interviews were continued until a point of saturation. To ensure the accuracy and reliability of the data collection tool, this was pilot tested with a nurse, a midwife, a clinical officer, a cleaner, and a security guard for content validity, length, and comprehensibility at Kakoba Health Centre III, in Mbarara city, and revised appropriately.
Data Management and Statistical Analysis
Interviews were digitally audio-recorded, then transcribed. Qualitative data were analyzed using thematic content analysis to identify, analyze, and report themes. Two members of the team read the transcripts several times, noted the preliminary ideas, produced initial codes, then generated and refined themes. These were entered into NVivo 10 software for thematic analysis. The data was analyzed to identify all the important themes mentioned by the participants using the Grounded Theory (GT) approach. Representative quotations, as well as statements of particular interest, were extracted to support the themes. Where language was potentially identifying (such as names of towns and organizations), these details were removed. Multiple coding and validity checks were performed to further strengthen the rigor.
Ethical Considerations
Ethical approval was obtained from the Mbarara University of Science and Technology Research Ethics Committee to whom a copy of the proposal and a consent form were presented for approval before the beginning of the study. Written informed consent was obtained from all participants and it was indicated that the interview would be audio recorded, and participated consent to include publication of anonymized responses. Participants who reported psychological issues were referred to the COVID-19 psychosocial team and the psychiatric unit at MRRH. The anonymity of participants was ensured at all stages of data collection and analysis. All the methods were performed in accordance with the Declaration of Helsinki, and other relevant guidelines and regulations.
Results
Fourteen interviews, comprising 9 IDIs and 5 KIIs, were conducted. Participants’ median age was 38 years (range: 26–51 years). Among the study participants, 57% (N=8) were males and most participants (N=11) were married. Twelve (85.7%) had post-secondary education, and the socio-demographics of study participants were summarized as indicated in Table 1.
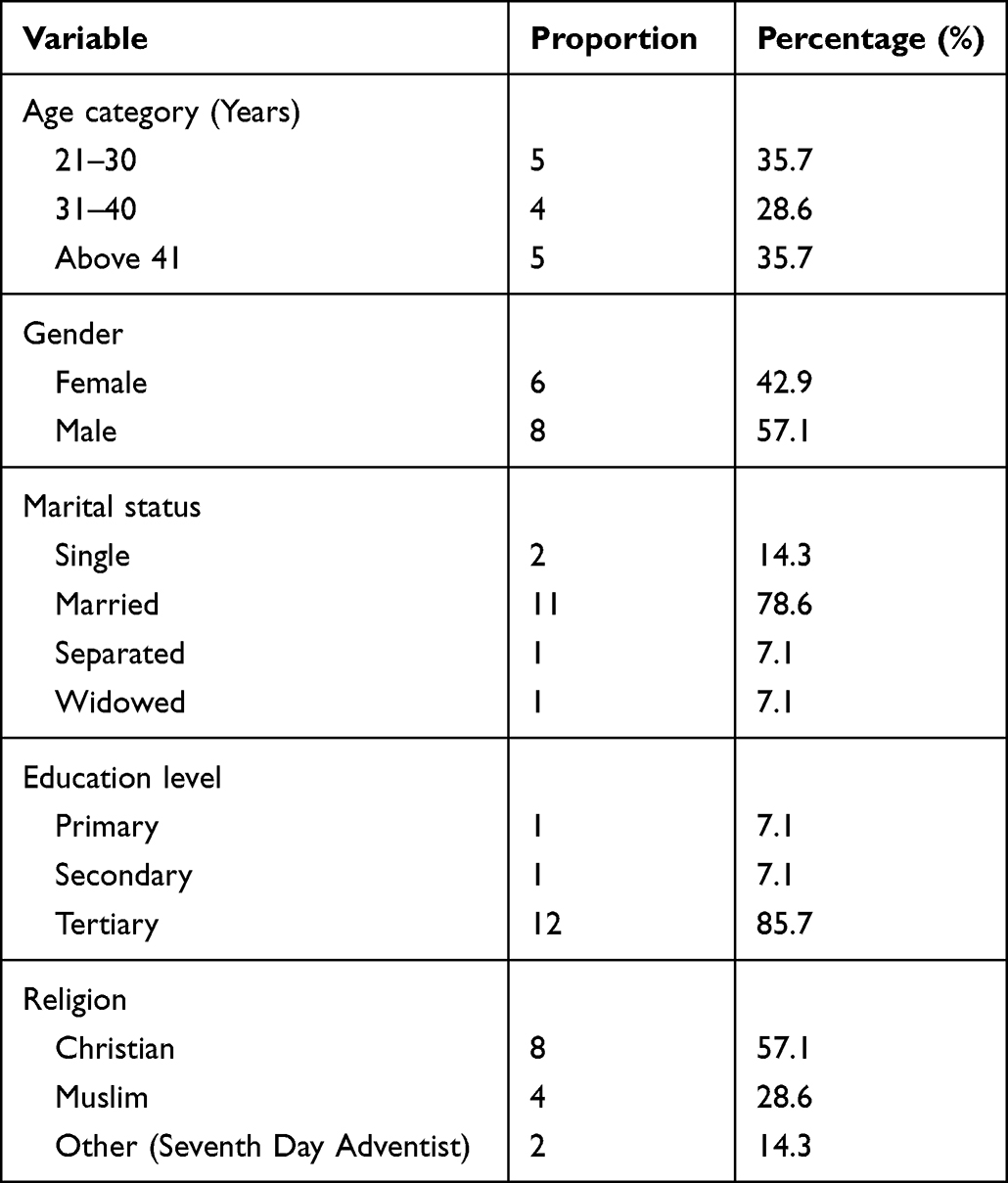 |
Table 1 Demographic Characteristics of the Participants |
The themes were: perceived psychosocial challenges of FHCPs working under the COVID-19 pandemic, and coping mechanisms with the situation of the COVID-19 pandemic. Further, sub-themes were considered under each major them as presented in the results section.
Theme I: Perceived Psychosocial Challenges of FHCPs Working Under the COVID-19 Pandemic
Burnout Due to Extended Working Hours
The daily routine was disrupted by extended working hours due to a heavy workload, leaving less time for other activities outside the work environment. This created burnout as narrated by some participants below:
COVID-19 demanded us [FHCPs] more time at work, and shift durations increased to more than 12 hours! You report at 7:00 AM and leave at 10:00 PM! Very tiring… at some point, FHCPs couldn’t even go back home, especially when COVID-19 cases were high! This meant that you have no rest and fatigue was too much! (Male, 51 years)
COVID-19 magnified my work as an ambulance driver. I had to evacuate the suspects [clinically defined as acute onset of symptoms, or contact of a probable or confirmed case or linked to a COVID-19 cluster], and this was tiring …as the lockdown and transport restrictions came into force, I had to pick up the FHCPs from their homes. …even at night, I was always on standby! …. I too drove long routes to Kampala for those critically ill patients and also for contact tracing or burial support. (Male, 39 years)
In addition, the heavy workload created another challenge of compassion fatigue.
Domestic Violence
Another social challenge of COVID-19 faced by the FHCPs was the hostile home environment evidenced by reported spousal domestic violence where a husband physically assaulted a FHCP. This resulted from the changing family environment, as people were now confined to their homes and their daily routines were greatly impacted as narrated:
COVID-19 created a survival challenge. …because of the restrictions, men spent most of their time at home, and this made them overreact to very small mistakes, resulting in domestic violence…. (Female, 37 years)
Additionally, FHCPs were estranged from their families, which negatively affected their relationship as narrated by a participant here:
…I attended to a positive case, and this sent my family members and close relatives in a fear for my life, and even when I got home, they isolated me! (Female, 26 years)
Financial Constraints
Due to the implementation of COVID-19 restrictions, businesses that served as side incomes came to a standstill, and this affected daily income and family welfare. As a result, there were financial constraints as reported here:
Our income reduced drastically, and we could no longer meet necessities. …the men who did not have stable jobs could no longer earn. This resulted in unnecessary quarrels, and often, there was domestic violence. (Female, 37 years)
Fear and Anxiety
The communities’ complacency was critically described by FHCPs when they noted the hesitancy of some people to use masks and their poor adherence to hygiene practices. The unwillingness of communities to adhere to the COVID-19 standard operating procedures (SOPs) contributed to worries among FHCPs as reported:
In the beginning, people did not respond to these measures [COVID-19 control measures]. …as if it was not real! As the political season was at its peak, it looked like a political game! To us the FHCPs, this was worrying, because complacency meant more cases, yet we needed to prevent the COVID-19 transmission. This created stress for the FHCPs. …unfortunately, more people got admitted and some died, this changed their attitude and complacency. (Female, 27 years)
The news reports on the COVID-19 outbreak caused devastating feelings of panic, especially reports that noted COVID-19 is a highly infectious and contagious disease with no cure at the time. This was worsened by news reports about massive deaths recorded in sophisticated healthcare settings in Europe and Asia, as narrated below:
The global media reports and the daily statistical reports were evident that the COVID-19 pandemic would worldly impact us. COVID-19 brought us a lot of fear, anxiety, and panic (like someone who had met a lion!) because it has no cure, and everyone is susceptible. At some point, I experienced stress, mood change, and fear as this was a deadly disease witnessed from what we were watching on the television (TV) globally, and I felt this would worsen for Uganda. (Male, 47 years)
The novelty of COVID-19 increased the levels of anxiety among FHCPs. The FHCPs had limited information and so felt ill-prepared to manage COVID-19 cases compared to previous outbreaks such as Marburg hemorrhagic and Rift valley fevers. The high levels of anxiety affected the willingness of the FHCPs to serve in the COVID-19 unit to the extent that only 2 out of the 23 FHCPs initially assigned to the unit felt comfortable working there, as expressed:
Hearing of the COVID-19 outbreak, as a member of the hospital epidemic response team, I was very worried, and I wondered if I would survive this! (Male, 38 years)
The discomfort and fear of attending to the COVID-19 cases were also highlighted by the FHCPs. This stemmed from the escalating numbers of the reported cases that would expose them to increased risk of contracting COVID-19, as expressed below:
With the first cases being reported from Mbarara Regional Referral Hospital, interaction with the cases was no longer comfortable I think community transmission was at its peak, and serving these patients was the highest risk of my lifetime! We were too scared, we feared for our lives at the peak of a pandemic. (Female, 44 years)
… with more cases being admitted, we perceived it as a serious threat. …I was much worried to get too close to the patient to feed or administer the drug. (Female, 27 years).
The persistent wearing of PPE resulted in severe discomfort, with scars and excessive sweating (heat stress) with associated mood swings and anxiety. This was largely attributed to the long working hours due to limited staff at the COVID-19 unit. Moreover, the FHCPs reported fear due to the inherent contradiction involved in the use of PPE and the established SOPs. Whereas the use of PPE and adherence to SOPs was initially perceived to protect against contracting COVID-19, some participants expressed fear, especially after some colleagues contracted COVID-19 while using PPE, as narrated here:
…I trusted the PPE. However, some of us contracted COVID-19 when you would do everything as recommended. I wondered whether PPE was efficient. This created a lot of fear as if we were not being protected! (Male, 41 years)
Further, the fear and anxiety of the COVID-19 situation were worsened by the nationwide infection control restrictions, their mode of implementation, and the uncertainty of when the situation would return to normalcy, as narrated by participants here:
…. abrupt measures such as the closure of workplaces, schools, shops, places of worship, curfew, and lockdown caused a lot of fear as this was never heard of. (Female, 53 years)
The President of Uganda timely communicated (through televised and radio broadcasted speech) the instituted nationwide regulations to guide the handling of the pandemic. Although this was novel in the Ugandan context, it created a lot of fear, panic, and anxiety. (Male, 51 years)
Psychological Distress
As more cases of COVID-19 were diagnosed, the psychological distress increased as some of the FHCPs tested positive for COVID-19. This, in addition, widened the human resource gap. The worst situations arose as reports arrived of fellow healthcare workers (from other hospitals) who died of COVID-19 in the line of duty, many describing it as heartbreaking. Furthermore, the psychological distress of the COVID-19 situation was worsened by the implementation of COVID-19 regulations, as narrated by a participant here:
…the streets were empty, all one could see were the army and policemen who were harshly enforcing the COVID-19 preventive measures… a lot of unanswered questions emerged: how long would it take to open again? How long would the food items we had last? Shall we ever get back to our normal lives?. many questions without answers! (Female, 36 years)
Stigma and Discrimination
The FHCPs were discriminated against by fellow staff on other wards, and this led to stigma. This was extended to the hospital transport van as the FHCPs would not board the same van. In the communities, FHCPs were perceived as highly contagious because they were seen as the epitome of COVID-19, as expressed:
…. people would describe the FHCPs as infectious. Communities believed that because of our involvement with the COVID-19 patients, we were asymptomatic and therefore people were on high alert that we might transmit COVID-19 to them. (Female, 44 years)
Theme II: Coping Mechanisms with the Situation of COVID-19 Pandemic
Situational Acceptance
While some FHCPs reportedly struggled to adjust to COVID-19, others coped well. For example, some FHCPs accepted the situation as it is, as narrated here:
…. COVID-19 posed serious challenges I have never met in my over 20 years of practice. …. with the previous outbreaks, one would get some hope that the situation will normalize, but for COVID-19, there was very little hope of anything getting better. I could hardly find any solvable approach, so I had to accept the situation as it is. I had to accept the challenging situation of COVID-19 as it is!. (Male, 51 years)
Religious Coping
Besides, other FHCPs used a prayerful approach, and considered it a routine practice to intercede for divine intervention, as narrated here:
…. I felt that the Almighty God had a big message to humanity through the COVID-19 pandemic. At first, I would pray as I report for work, later, I was joined by two of my colleagues, and we made it compulsory to pray together daily. This relieved my anxiety and I experienced some positive energy to attend to my patients. (Female, 27 years)
Coping Through Emotional Support
Also, the overwhelming COVID-19 situation necessitated self-encouragement, seeking colleague counseling and psychosocial support, as reported here:
….in the beginning, I tried to strengthen myself. However, as more cases showed up, I broke down. One of the recruits was close to me, and we resorted to counseling each other. Also, the psychosocial support unit helped us. These approaches helped us to cope with the difficult COVID-19 situation. (Male, 39 years)
Coping Through Informational Support
Other FHCPs focused on new developments, such as COVID-19 vaccines and this gave assurance to FHCPs, as narrated here:
….as some researchers reported milestones in COVID-19 vaccine discovery, I got relieved. I knew that the vaccine would be a game-changer, and at least it eased on my distress. (Female, 37 years)
Bulk Purchase of Short-Supply Basic Necessities
Due to recurring lockdown measures, FHCPs’ made bulky purchases of food items since people were unsure of how long the situation would last. This assurance of the basic necessitates gave a temporal psychological relief, as reported here:
At the beginning of the lockdown, I had some food. Then there was an extension of the lockdown, and this created a lot of panic. With little food remaining, it was unclear how long this situation would last. With the savings I had, I bought a lot of posho, rice, and beans to last for at least three months. This relieved my subsistence worry and I worked with an assurance that at least my home has food. (Male, 51 years)
Discussion
Socially, the COVID-19 pandemic presented numerous disruptions to the FHCPs’ social interactions and personal relationships. This disruption during the pandemic had an impact on the social relations of the FHCPs caring for COVID patients, both in and outside the workplace, and especially the psychosocial support of family and friends. This creates a social dysfunctionality and imbalance amongst FHCPs. Consistent with previous studies,21,22 taking into account social relations in an outbreak environment is a critical factor in adapting to the uncertainty associated with working under challenging conditions. The long periods away from home experienced by an FHCP who also was a household head implied that family needs would be inadequately met. This inability to provide for the family at home resulted in unstable social relations.23 While family social support and stability contributed to psychosocial well-being during the challenging work conditions of an outbreak, reported occurrences of domestic violence made FHCPs more vulnerable to distress.24,25 Because COVID-19 is highly contagious, FHCPs faced discrimination and stigma. This finding suggests that during an outbreak, discrimination and stigma may be used as a negative protective mechanism for those who are not closely associated with treating suspects/cases, due to fear of contracting the disease. This finding is consistent with previous reports,11,26 in that the discriminatory and stigmatization practices contributed to the FHCPs’ physical exhaustion and compassion fatigue while performing their duties.27 The disrupted routines create minimal opportunities for FHCPs to recover from fatigue.
The anticipated increase in cases exacerbated the psychological distress. The inadequate number of FHCPs assigned to the COVID-19 isolation unit aggravated the situation. Furthermore, capacity gaps in COVID-19 management at lower-level healthcare facilities increased referral cases in an already constrained working environment, marked by inadequate funding and an insufficient health workforce.28,29 However, the efforts of the government and implementing partners to hire more FHCPs were critical in the management of the associated burnout and fatigue. The complacent attitude toward adherence to SOPs at the community level contributed to the eventual cumulative risk of infection and, as a result, increases the number of cases at healthcare facilities. This, in turn, had a direct impact on the psychological well-being of FHCPs during an outbreak.30
While the media helped to raise epidemiological awareness through global statistical reports, it was also a source of psychological distress in a healthcare setting, where FHCPs believed they were unprepared to manage the surge of cases in an outbreak with limited resources. This compares well with previous reports among FHCPs with increased exposure to COVID diagnosis, treatment, and care.12,13,31 Psychological distress negatively impacts professionalism, efficiency, and overall quality of life, which in turn impacts on quality of patient care.32,33 Strict adherence to SOPs, as well as the proper and consistent use of PPE, were used to ensure FHCPs’ safety. The use of PPE was initially thought to be a protective measure but later had the opposite effect. The negative outcomes were due in part to the fact that increased demand for PPE may have caused a break in the global supply chain, compromising product quality.5,9,34 The health risks associated with PPE have been widely reported, with one study,35 concluding that PPE has a negative impact on FHCPs’ physical and mental health.
Whereas FHCPs were recognized as “essential workers” with unrestricted permission to move and deliver a service, COVID-19 enforcement officers sometimes treated them inconsiderately. This situation exacerbated the FHCPs’ pre-existing distress and resulted in psychological frustration in the line of duty. Political speeches can also amplify FHCPs’ fears, frustrations, helplessness, and anxiety during disease outbreaks.36–38 While the presidential directives sought to reduce infection rates through established SOPs, FHCPs were psychologically adversely impacted by experiences outside of the workplace related to COVID-19 infection control, which in turn affected the quality of patient care.
In light of these challenges, various coping strategies for the COVID-19 pandemic situation have been reported. Coping approaches have previously been reported and are critical during an outbreak.39–42 Aside from the dire situation caused by the COVID-19 pandemic, a lack of psychological first-aid and counseling in our healthcare system has exacerbated the pandemic’s psychological effects.1 The coping mechanisms were largely informal, similar to previous reports.21,27,41,42 The absence of institutionalized psychosocial support mechanisms increased distress among FHCPs and this affected the quality of healthcare provision. The findings of this study ought to be interpreted in light of the following; Firstly, as the study was conducted during the first wave of Coronavirus Disease in 2019; it is possible that a number of factors have changed since then. Secondly, as the frontline healthcare providers were recruited from a single tertiary healthcare facility (Mbarara Regional Referral Hospital), the findings may not be generalizable to the entire country. Also, the findings of this study are based on the participants reporting true information.
Conclusions
This study offers a unique perspective on FHCPs during the COVID-19 pandemic in Uganda. The study depicts FHCPs’ negative experiences while doing their best in the face of a new pandemic, under severe resource constraints. The findings highlight the frontline health workers’ social and psychological distress and uncertainty, as they felt an enormous social responsibility to serve the community adequately and professionally in the face of a novel pandemic yet did not feel supported by the community and their institution did not well address their needs to support excellence in care and safety. With the uncertainty surrounding emerging waves and new variants, FHCPs would have benefited from a psychosocial package to supplement workplace safety mechanisms. This is in recognition of the interaction that exists between social and psychological challenges. As we progress through the COVID-19 pandemic and post-recovery, this would be best implemented through an established psychosocial unit at a healthcare facility as a health-systems strengthening intervention. This establishment was critical and is a positive step toward the mental well-being of FHCPs.
Based on this study’s findings, the following actions are recommended: the government must recognize and appreciate the pride and efforts of FHCPs through positive communication between central disease control authorities and peripherally stationed FHCPs. Furthermore, the perception of a low risk of contracting COVID-19, as well as the likelihood of survival, aids in reducing psychological stress. As a result, identifying and mitigating these work-related challenges is critical to protecting FHCPs’ mental health and well-being. Future response plans should also include adequate psychosocial support, counseling, stress management programs, and informal peer support groups for FHCPs, as these are critical coping strategies for the difficulties that arise in a risky environment such as the COVID-19 pandemic.
Abbreviations
COVID-19, Coronavirus Disease-2019; FHCPs, Frontline healthcare providers.
Data Sharing Statement
All relevant data are within the paper. The interview guide is included as a supplementary material (Appendix 1).
Ethics Approval and Consent to Participate
Ethical approval was obtained from the Mbarara University of Science and Technology Research and Ethics Committee where a copy of the proposal with a consent form was presented for approval before the beginning of the study. Also, written informed consent was obtained from all participants and it was indicated that the interview would be audio recorded. Participants who reported psychological issues were linked to the COVID-19 psychosocial team and the psychiatric unit at MRRH. The anonymity of participants was ensured at all stages of data collection and analysis. All the methods were performed in accordance with the Declaration of Helsinki, and other relevant guidelines and regulations.
Acknowledgments
We are grateful to the study participants. We gratefully acknowledge Professor Rose Clarke Nanyonga for her generous donation. We are grateful to Noni E. MacDonald for critically reviewing this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by a MicroResearch grant MR 20M MUS 01. Dr. Scholastic Ashaba acknowledges salary support from K4 TW 011929-2. The funders had no role in the study design, data collection, analysis, or decision to publish.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Knobler S, Mahmoud A, Lemon S, et al. The impact of globalization on infectious disease emergence and control: exploring the consequences and opportunities. National Academies Press; 2006.
2. Madhav N, Oppenheim B, Gallivan M, Mulembakani P, Rubin E, Wolfe N. Disease Control Priorities: improving Health and Reducing Poverty. Lancet. 2017;391(10125):e11.
3. Grubaugh N, Ladner J, Lemey P, et al. Tracking virus outbreaks in the twenty-first century. Nat Microbiol. 2019;4(1):10–19. doi:10.1038/s41564-018-0296-2
4. European Centre for Disease Prevention and Control. Event background COVID-19; 2020. Available from: https://www.ecdc.europa.eu/en/novel-coronavirus/event-background-2019.
5. Feng S, Shen C, Xia N, Song W, Fan M, Cowling B. Rational use of face masks in the COVID-19 pandemic. Lancet Respir. Med. 2020;8(5):434–436. doi:10.1016/S2213-2600(20)30134-X
6. World Health Organization. Coronavirus Disease 2019 (COVID-19) Situation Report – 70. World Health Organization; 2020b.
7. WHO. Rational Use of Personal Protective Equipment (PPE) for Coronavirus Disease (COVID-19): Interim Guidance, 19 March 2020. World Health Organization; 2020.
8. Ministry of Health, Uganda; 2020. Available from: https://www.health.go.ug/document/press-release.
9. Ebrahim S, Ahmed Q, Gozzer E, Schlagenhauf P, Memish Z. COVID-19 and community mitigation strategies in a pandemic. BMJ. 2020;1:368.
10. Roy D, Tripathy S, Kar S, Sharma N, Verma SK, Kaushal V. Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian J Psychiatr. 2020;51:102083. doi:10.1016/j.ajp.2020.102083
11. Alradhawi M, Shubber N, Sheppard J, Ali Y. Effects of the COVID-19 pandemic on mental well-being amongst individuals in society- A letter to the editor on “The socio-economic implications of the coronavirus and COVID-19 pandemic: a review”. Int J Surg. 2020;78:147–148. doi:10.1016/j.ijsu.2020.04.070
12. Galea S, Merchant R, Lurie N. The mental health consequences of COVID-19 and physical distancing: the need for prevention and early intervention. JAMA Intern Med. 2020;180(6):817. doi:10.1001/jamainternmed.2020.1562
13. Holmes E, O’Connor R. Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. Lancet Psychiatry. 2020;7(6):547–560. doi:10.1016/S2215-0366(20)30168-1
14. Amir K, Okalo P. Frontline nurses’ compassion fatigue and associated predictive factors during the second wave of COVID-19 in Kampala, Uganda. Nursing Open. 2022;9:2390–2396. doi:10.1002/nop2.1253
15. Nishihara T, Ohashi A, Nakashima Y, et al. Compassion fatigue in a health care worker treating COVID-19 patients: a case report. Bio Psycho Social Med. 2022;16:10. doi:10.1186/s13030-022-00239-0
16. Yi Y, Lagniton PNP, Ye S, Li E, Xu RH. COVID-19: what has been learned and to be learned about the novel coronavirus disease. Int J Biol Sci. 2020;16(10):1753–1766. doi:10.7150/ijbs.45134
17. Uganda National Population and Housing Census. Area Specific Profiles, Mbarara District; 2014.
18. Guest G, Bunce A, Johnson L. How many interviews are enough? An experiment with data saturation and variability. Field Methods. 2006;18(1):59–82. doi:10.1177/1525822X05279903
19. Braun V, Clarke V. (Mis) conceptualising themes, thematic analysis, and other problems with Fugard and Potts’. Sample-size tool for thematic analysis. Int J Soc Res Methodol. 2016;19(6):739–743. doi:10.1080/13645579.2016.1195588
20. Fugard AJ, Potts HW. Supporting thinking on sample sizes for thematic analyses: a quantitative tool. Int J Soc Res Methodol. 2015;18(6):669–684. doi:10.1080/13645579.2015.1005453
21. Gamma AE, Slekiene J, von Medeazza G, et al. Contextual and psychosocial factors predicting Ebola prevention behaviours using the RANAS approach to behaviour change in Guinea-Bissau. BMC Public Health. 2017;17:446. doi:10.1186/s12889-017-4360-2
22. Low LL, Tong SF, Ang JY, et al. Social responsibility perspective in public response to the COVID-19 pandemic: a grounded theory approach. BMC Public Health. 2022;22:469. doi:10.1186/s12889-022-12819-4
23. Zhang C, Yang L, Liu S, et al. Survey of insomnia and related social psychological factors among medical staff involved in the 2019 novel coronavirus disease outbreak. Front Psychiatry. 2020;11:306. doi:10.3389/fpsyt.2020.00306
24. Katana E, Amodan BO, Bulage L, et al. Violence and discrimination among Ugandan residents during the COVID-19 lockdown. BMC Public Health. 2021;21:467. doi:10.1186/s12889-021-10532-2
25. Sharma A, Borah SB. Covid-19 and Domestic Violence: an Indirect Path to Social and Economic Crisis. J Fam Violence. 2022;37(5):759–765. doi:10.1007/s10896-020-00188-8
26. Banerjee D, Nair V. Handling the COVID-19 pandemic: proposing a community based Tool kit for psycho-social management and preparedness. Asian J Psychiatr. 2020;7(51):102152. doi:10.1016/j.ajp.2020.102152
27. Kwaghe AV, Ilesanmi OS, Amede PO, et al. Stigmatization, psychological and emotional trauma among frontline health care workers treated for COVID-19 in Lagos State, Nigeria: a qualitative study. BMC Health Serv Res. 2021;21:855. doi:10.1186/s12913-021-06835-0
28. Koutsoumpa M, Odedo R, Banda A, et al. Health workforce financing in Uganda: challenges and opportunities. Eur J Public Health. 2020;30(Supplement_5):ckaa165–525. doi:10.1093/eurpub/ckaa165.525
29. Abuduxike G, Acar Vaizoglu S, Asut O, Cali S. An Assessment of the Knowledge, Attitude, and Practice Toward Standard Precautions Among Health Workers From a Hospital in Northern Cyprus. Saf Health Work. 2021;12(1):66–73. doi:10.1016/j.shaw.2020.09.003
30. Shewasinad Yehualashet S, Asefa KK, Mekonnen AG, et al. Predictors of adherence to COVID-19 prevention measure among communities in North Shoa Zone, Ethiopia based on health belief model: a cross-sectional study. PLoS One. 2021;16(1):e0246006. doi:10.1371/journal.pone.0246006
31. Pappa S, Ntella V, Giannakas T, Giannakoulis VG, Papoutsi E, Katsaounou P. Prevalence of depression, anxiety, and insomnia among HCPs during the COVID-19 pandemic: a systematic review and meta-analysis. Brain Behav Immun. 2020;88:901–907. doi:10.1016/j.bbi.2020.05.026
32. Chatterjee SS, Barikar CM, Mukherjee A. Impact of COVID-19 pandemic on pre-existing mental health problems. Asian J Psychiatr. 2020;51:102071. doi:10.1016/j.ajp.2020.102071
33. Xiong J, Lipsitz O, Nasri F, et al. Impact of COVID-19 pandemic on mental health in the general population: a systematic review. J Affect Disord. 2020;277:55–64. doi:10.1016/j.jad.2020.08.001
34. World Health Organization. Rolling Updates on Coronavirus Disease (COVID-19). World Health Organization; 2020c.
35. Loibner M, Hagauer S, Schwantzer G, Berghold A, Zatloukal K. Limiting factors for wearing personal protective equipment (PPE) in a health care environment evaluated in a randomised study. PLoS One. 2019;14:e0210775. doi:10.1371/journal.pone.0210775
36. Shultz JM, Cooper JL, Baingana F, et al. The role of fear-related behaviors in 2013-2016 West Africa Ebola virus disease outbreak. Curr Psychiatry Rep. 2016;18(11):104. doi:10.1007/s11920-016-0741-y
37. Freckelton QI. COVID-19: fear, quackery, false representations and the law. Int J Law Psychiatry. 2020;72:101611. doi:10.1016/j.ijlp.2020.101611
38. Hyland-Wood B, Gardner J, Leask J, et al. Toward effective government communication strategies in the era of COVID-19. Humanit Soc Sci Commun. 2021;8:30. doi:10.1057/s41599-020-00701-w
39. Chen Y, Zhou H, Zhou Y, Zhou F. Prevalence of self-reported depression and anxiety among pediatric medical staff members during the COVID-19 outbreak in Guiyang, China. Psychiatry Res. 2020;288:113005. doi:10.1016/j.psychres.2020.113005
40. Thai TT, Le PTV, Huynh QHN, Pham PTT, Bui HTH. Perceived Stress and Coping Strategies During the COVID-19 Pandemic Among Public Health and Preventive Medicine Students in Vietnam. Psychol Res Behav Manag. 2021;14:795–804. doi:10.2147/PRBM.S317059
41. Budimir S, Probst T, Pieh C. Coping strategies and mental health during COVID-19 lockdown. J Ment Health. 2021;30(2):156–163. doi:10.1080/09638237.2021.1875412
42. Teferu E, Solomon S, Kumbi K, et al. COVID-19-Related Anxiety and the Coping Strategies in Southeast Ethiopia. Psychol Res Behav Manag. 2021;14:1019–1031. doi:10.2147/PRBM.S309806
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.