Back to Journals » Psychology Research and Behavior Management » Volume 16
Psychometric Properties of the Chinese Version of the Comprehensive Autistic Trait Inventory
Received 8 March 2023
Accepted for publication 1 June 2023
Published 15 June 2023 Volume 2023:16 Pages 2213—2223
DOI https://doi.org/10.2147/PRBM.S411599
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Fan Meng,1 Bin Xuan1,2
1School of Educational Science, Anhui Normal University, Wuhu, Anhui Province, People’s Republic of China; 2Institute of Artificial Intelligence, Hefei Comprehensive National Science Center, Hefei, People’s Republic of China
Correspondence: Bin Xuan, Email [email protected]
Background: The Comprehensive Autistic Trait Inventory (CATI) was an appropriate assessment tool that included all the principal dimensions related to autism defined in DSM-5 for the general population. However, its validity and reliability in the general Chinese population still need to be examined.
Purpose: We revised the inventory and estimated the validity and reliability of the Chinese version of the CATI among 2232 general undergraduates.
Methods: The Chinese version of the CATI (CATI-C) was administered to 2259 undergraduates using the online Questionnaires Star electronic system. Internal consistency, convergent validity, discriminant validity, test-retest reliability, and measurement invariance across gender were calculated. In order to determine the diagnostic accuracy and optimal cut-off score of the CATI-C, an analysis using the Receiver Operating Characteristic (ROC) was performed.
Results: The CATI-C includes 35 items of two factors and six dimensions. CFA demonstrated that the fit index of the structure of the scale was good (Satorra-Bentler chi-square/degrees of freedom [S-Bχ2 /df] = 2.406, Standardized Root Mean Square Residual [SRMR] = 0.038, Root Mean Square Error of Approximation [RMSEA] = 0.037, Comparative Fit Index [CFI] = 0.929, Tucker-Lewis Index [TLI] = 0.917). The convergent validity examined based on the Autism Spectrum Quotient total score was satisfactory (r = 0.54). The internal consistency reliability of social factor, non-social factor, and total scores were 0.87, 0.85, and 0.90. The test-retest reliability was 0.80. A cut-off score of 115 provided optimal sensitivity and specificity for the CATI-C (sensitivity = 0.926, specificity = 0.781, and Youden’s index = 0.707).
Conclusion: The CATI-C has satisfactory reliability and validity in measuring autistic traits. It showed a good model fit for social and non-social second-order bifactors and measurement invariance across gender.
Keywords: comprehensive autistic trait inventory, psychometrics, measurement invariance
Introduction
A systematic review reveals an increase in the global prevalence of autism.1 Autism spectrum disorder (ASD) affects approximately 1% of children worldwide, with the prevalence of autism in China close to that in the West.2 ASD is a neurodevelopmental disorder that is defined by deficits in social communication and restricted, repetitive patterns of interests and behaviors. The severity and scope of these core behavioral traits can vary based on where an individual falls on the autism continuum.3 Autistic traits refer to personality traits, social interaction characteristics, and behaviors similar to autism, first observed among parents and relatives of autistic children,4 continuously distributed in individuals on the autism spectrum5,6 and the general population.7–9 Autistic traits can be considered a sixth factor of personality in addition to the Big Five.10,11 Increasing numbers of studies have found that autistic traits are prevalent in the general population,12–14 indicating that the construct of autism might form a continuum in the general population based on trait-like characteristics.15 More and more studies have demonstrated the continuum model. According to the twin concordance study, autistic traits and ASD may share a genetic etiology,16,17 and it is estimated that the heritability of autistic traits is 0.61–0.73.18 Substantial and replicable etiological overlap between ASD and typical variations in social and communication abilities among the general population was found using large ASD consortiums and population-based resources through linkage disequilibrium score regression and de novo variant analysis.19 Using a dual Weibull mixture model, researchers provide perspectives on how autism traits are distributed along a continuum.20 The meta-analysis of four population-based genome-wide association studies investigating autistic-like traits in the general population has shown the role of immune-related genes in specific autistic-like traits.21 More and more refined evidence demonstrates that the continuum view of autistic traits in the general population merits further research.22,23
To understand the prevalence and impact of autistic traits in the general population, researchers designed several psychometric scales. The Autism-Spectrum Quotient (AQ)24 has been widely used to investigate autism-related traits. Additionally, the Social Responsiveness Scale (SRS-2)25 and the Broad Autism Phenotype Questionnaire (BAPQ)26 are often applied to assess autistic traits. Furthermore, the above instruments are supplied qualitatively, primarily focusing on the core ASD features. The diagnostic understanding of autism has changed over the years, and ASD is conceptualized as a “spectrum” in DSM-5.27 Due to the recent development of the subthreshold autism spectrum model,28 subthreshold autistic trait (SAT) measures for the general population have been constructed, such as Subthreshold Autism Trait Questionnaire (SATQ)29 and Adult Autism Subthreshold Spectrum (AdAS Spectrum).30 However, SATQ does not include the modifications in DSM-5 in the criteria for ASD. Although AdAS Spectrum has subscales on sensory sensitivity and elucidates the extent of gender-related camouflage in DSM-5,31 it is a complex (160 items) forced-choice test that does not refer to childhood and adolescence groups. As a result, an adequate assessment tool for the general population taking all the core indicators of autistic traits in DSM-5 into account is required, and it is of significant theoretical and practical value.
The Comprehensive Autistic Trait Inventory (CATI) consists of 42 items, and each subscale contains seven items that can be assessed using the five-point Likert scale. The autistic traits in the general population were measured according to the diagnostic criteria for ASD in DSM-5. The CATI is composed of social and non-social second-order bifactors. The social factor includes social interactions (SOC), communication (COM), and social camouflage (CAM), while the non-social factor includes repetitive behavior (REP), cognitive rigidity (RIG), and sensory sensitivity (SEN). The CATI maintains psychometric properties superior to the AQ and BAPQ in a study with a large sample of adults.32 Internal consistency for all of the six subscales of the CATI was excellent (0.810–0.940), and total-scale internal consistency was 0.950. The CATI had better convergent validity than the AQ and BAPQ at both the total scale level (r ≥ 0.790) and subscale level (r ≥ 0.680). Additionally, the construct validity of CATI was supported by confirmatory factor analysis (CFA), which showed that the best-fit model had two correlated social and non-social bifactors and measurement equivalence among different gender groups.
Overall, the CATI is an effective measure to assess the autistic traits of the general population, and it is valuable to verify its psychometric properties in different cultural contexts. Though the CATI has been examined in five English-speaking countries, the psychometric properties of its Chinese version have yet to be studied, and there was no evidence supporting the measurement invariance of this factor structure across gender. Exploring the psychometric characteristics of the CATI-C is crucial, as there is currently no Chinese version of an assessment tool for autistic traits based on the DSM-5. In this paper, we explored the psychometric characteristics of the Chinese version of the CATI.
Methods
Participants and Procedure
Based on convenience sampling methods, the participants were recruited from five provinces (Anhui, Henan, Guangdong, Heilongjiang, and Shaanxi) who took part in an online survey and spoke Mandarin Chinese, and the research adhered closely to Internet research ethics.33 The final sample consisted of 2259 undergraduates (see Table 1) from eight general comprehensive universities, aged 18–26 (53.829% females, mean age 20.116 ± 1.491 years), whose responses were uncompleted or less than five minutes were eliminated. The no-clinical sample included 2232 undergraduates who self-reported as non-autistic and 27 undergraduates who self-reported with diagnosed autistic or self-identifying as autistic.
 |
Table 1 Characteristics of Participants (N = 2259) |
After getting the author’s authorization, the English version of CATI began to be translated into Mandarin Chinese. Back-translation was conducted to ensure the faithfulness of the translation. The specific procedures are as follows. First, a native Chinese speaker translated the CATI into Mandarin Chinese. Next, a native English speaker unfamiliar with the CATI translated it back into English. A native English speaker compared the original English version and the back-translated version. According to the author’s advice, discrepancies were revised. There is some inaccurate understanding of items. For example, “I am uncomfortable with unexpected loud noises.” Would be better than “I react poorly to unexpected loud noises”. The Mandarin-Chinese CATI could be considered linguistically equivalent to the original English version.
Measures
Comprehensive Autistic Trait Inventory (CATI)
The Comprehensive Autistic Trait Inventory (CATI) is a self-report questionnaire consisting of 42-item in six subscales (seven items in each subscale). These items are evaluated based on the five-point Likert scale: “Definitely disagree”, “Somewhat disagree”, “Neither agree nor disagree”, “Somewhat agree”, and “Definitely agree”. Reverse-scored items include Items 1, 2, 5, 8, and 10. The English version of CATI calculated the reliability using Cronbach’s alpha of 0.95.
The Autism-Spectrum Quotient (AQ)
The Autism-Spectrum Quotient (AQ)24,34 has been widely used to assess autism-related traits. It is a self-report questionnaire consisting of 50 items in five subscales (Social Skill, Attention Switching, Attention to Detail, Communication, and Imagination), each with a 4-point rating scale, and twenty-four items were reverse-scored. The Chinese version of AQ has demonstrated adequate validity and reliability,35 and the present study calculated the reliability using Cronbach’s alpha of 0.74 and omega coefficient of 0.76.
Chinese Version of Comprehensive Autistic Trait Inventory (CATI-C)
The CATI-C is a self-report questionnaire consisting of 35 items (https://www.cati-autism.com/). Three subscales of SOC, COM, and CAM belong to the social factor; the other three subscales of REP, RIG, and SEN belong to the non-social factor. These items are evaluated based on the five-point Likert scale, ranging from 1(Definitely disagree) to 5 (Definitely agree). Reverse-scored items include Items 1, 2, and 5. The final score can range from 35 to 175, with a higher score indicating a higher level of autistic traits. The present study calculated the reliability using Cronbach’s alpha of 0.90 and omega coefficient of 0.90.
Statistical Methods
Data analysis was performed using SPSS 26.036 for descriptive statistics and ROC analyses, AMOS 24.0 software for discriminant validity analysis, and Mplus 8.0 software for structural equation modeling. One of the subsets was for EFA, and another subset was for CFA showed the best-fit model for the data. To examine the construct validity and across-gender invariance of the CATI-C by applying CFA with Maximum-Likelihood Method (MLM). According to Hu and Bentler’s suggestion, the value of RMSEA below 0.05 can be deemed acceptable, and the CFI and TLI values>0.90 were considered to represent proper model fit.37 The SRMR value smaller than 0.05 was considered good.38 The internal consistency was estimated based on the subscale and overall scale scores. The convergent validity, discriminant validity, and test-retest reliability were tested by correlation analysis.
Results
Construct Validity
Item Analysis and Exploratory Factor Analysis (EFA)
First, the item analysis showed that the correlation index of four items (items 8, 10, 12, 23) with the total score was lower than 0.3, and the correlation coefficients between the score of the other items and the total score ranged from 0.33 and 0.60 (P < 0.001). Second, all subjects were sorted based on the total score and divided into the high total score group and the low total score group according to the criteria of 27%. Significant differences were found in 38 items (P < 0.001) between the high total score and low total score groups. EFA showed that three items (Items 22, 33, 35) tended to load on two factors, with KMO = 0.90 and Bartlett’s test of sphericity χ2 = 12,185.75 (P < 0.001), both considering eigenvalues greater than 1.0 and visually inspecting the scree plot (Figure 1), resulting in 51.75% of cumulative variance explained by six factors—the loading values for each entry range from 0.53 to 0.81 (Table 2).
 |
Table 2 Factor Loadings of the CATI-C Items Resulting from the EFA (n1=1022) |
 |
Figure 1 Scree plot of eigenvalues of CATI-C after principal component analysis. |
Confirmatory Factor Analysis (CFA)
The CFA results for various models are compiled in Table 3. The data fitted well with the model of correlated social and non-social bifactors, with S-Bχ2(df) = 1226.842 (510), SRMR = 0.038, RMSEA = 0.037, CFI = 0.929, TLI = 0.917.
 |
Table 3 The Confirmatory Factor Analysis Results of the CATI-C (n1 = 1022, n2 = 1027) |
Convergent Validity and Discriminant Validity
We used the AQ as the gold standard and correlated it with the CATI in sample 1 (n1=1022). The CATI and AQ correlate at the total score level (r = 0.54, P < 0.010). At the bifactor score level, the AQ also showed a strong correlation with the social factor (r = 0.64, P < 0.010) and non-social factor (r = 0.33, P < 0.010).
The discriminant validity of the Chinese CATI assessment was assessed through the heterotrait-monotrait (HTMT) ratio of correlations method. HTMT values smaller than 0.85 indicate high discriminant validity;39 the smaller the HTMT value, the higher the discriminant validity.40 All HTMT values were smaller than 0.85 in the current study, as shown in Table 4.
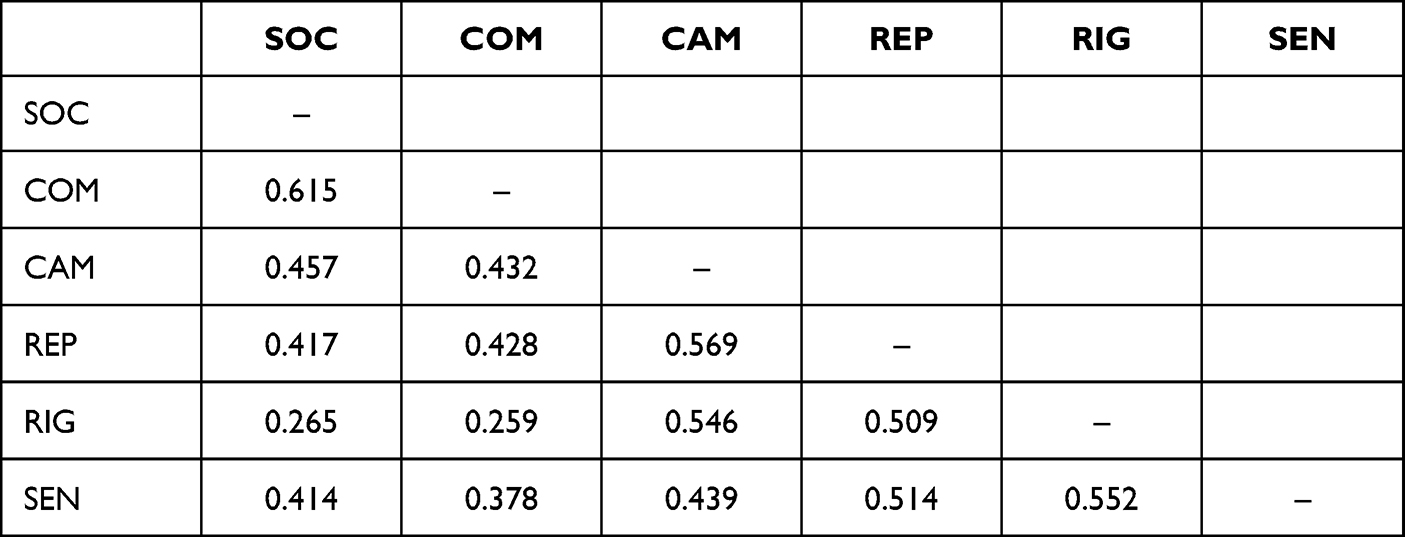 |
Table 4 HTMT of the Subscale of the CATI-C (n2 = 1027) |
Measurement Invariance Across Gender
The correlated bifactor model fitted well with the data for both the male and female participants. Therefore, the results of this study can be directly used for comparing male and female participants, and the differences can be interpreted based on the criteria of ΔCFI < 0.0141 and ΔRMSEA < 0.015,42 as shown in Table 5.
 |
Table 5 Measurement Invariance Across Gender (n2 = 1027) |
Internal Consistency and Test-Retest Reliability
The Chinese version of CATI had high internal consistency, as shown by the analysis of sample 2, with Cronbach’s alpha of 0.90 and an omega coefficient of 0.90. The social factor included 16 items; Cronbach’s alpha was 0.87, and the omega coefficient of 0.87. The non-social factor included 19 items, Cronbach’s alpha was 0.85, and the omega coefficient of 0.86. Cronbach’s alpha for the six subscales was 0.65–0.87, and the omega coefficient was 0.66~0.87.
The test-retest reliability coefficient analyzed with sample 3 was 0.80 on the total score scale, 0.80 for the social factor, and 0.73 for the non-social factor. Regarding subscale scores, test-retest reliability coefficients ranged between 0.48 and 0.76 (all with P < 0.001).
Identification of a Relevant Threshold
The CATI was originally designed to evaluate autistic traits in non-clinical populations. However, for certain research purposes, a cut-off score is necessary to differentiate between autistic and non-autistic individuals. To this end, ROC analyses were conducted to determine the sensitivity and specificity of the CATI-C total score. The results, depicted in Figure 2, indicate that the CATI-C possesses a high level of discriminatory power, with a maximum area under the curve (AUC) of 0.932 (95% CI: 0.893, 0.971). The optimal cut-off score for identifying individuals with autism is 115, and diagnostic utility was considered acceptable (sensitivity = 0.926, specificity = 0.781, and Youden’s index = 0.707) for the CATI-C.
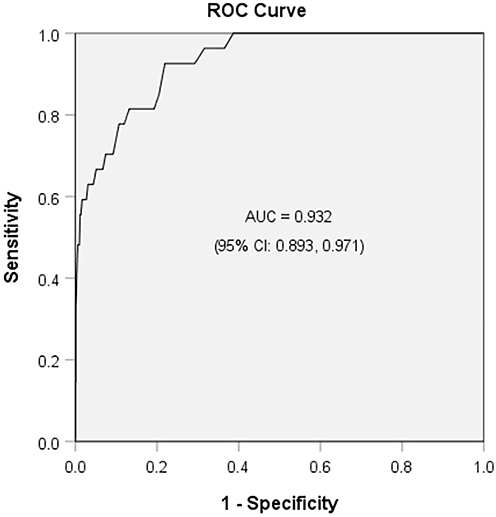 |
Figure 2 ROC curves for CATI-C. |
Discussion
This study presents the psychometric assessment of a novel scale designed to measure autistic traits, which was developed based on the diagnostic criteria for autism spectrum disorder outlined in the DSM-5. The findings indicate that the CATI-C exhibits favorable levels of reliability and validity when applied to the general population. By gaining insight into the behavioral and cognitive patterns of individuals without autism, it becomes possible to more accurately identify those who may require intervention and implement suitable measures to aid them.
This study proved that the psychometric properties of the Chinese version of the CATI are reliable and could be a valuable measurement for assessing autistic traits among Chinese undergraduates. We first revised the original CATI into a Chinese version and rechecked the translation with the original author to confirm the accuracy of the translation. We revised some expressions of the sentences to make them more accurate, easier to understand, and more adaptable to Chinese reading habits. Specifically, item 27, “I expend a lot of mental energy trying to fit in with others”, is revised to “I use a lot of mental energy trying to fit in with others”; item 38, “I react poorly to unexpected loud noises” is revised to “I am uncomfortable with unexpected loud noises”. In addition to the content revisions, some items were removed based on the results of the data analysis. Four items (Items 8, 10, 12, 23) were removed by item analysis because of the poor correlation index with a total score (of <0.3), and three items (Items 22, 33, and 35) were removed by the EFA because they tended to load on two factors. Furthermore, the CFA results showed that the best-fit model was that with social and non-social second-order bifactors (see Figure 3) consistent with the original scale; the social factor included SOC, COM, and CAM, while the non-social factors included REP, RIG, and SEN.
 |
Figure 3 Correlated bifactors model of the Chinese version of the CATI. |
In this study, the strong correlation between the total score of the CATI, social, and non-social bifactors score of the CATI with the total score of the AQ indicated good criterion validity. Currently, all HTMT values were smaller than 0.85, indicating the high discriminant validity of the CATI. Additionally, multi-group factor analysis demonstrated the gender measurement invariance of the CATI. Furthermore, the CATI showed good internal consistency and test-retest reliability. Finally, the CATI-C showed good sensitivity and specificity in discriminating between autistic and non-autistic individuals. The Chinese version of the CATI is a promising instrument for the assessment of the social and non-social autistic traits of undergraduates.
Limitations and Future Research
Limitations of this study include the following. First, all the participants were self-reported undergraduates, which may minimize the results’ generalizability. More population groups, such as clinical groups, enterprise employees, and adolescents, can be included in the future. Second, the criterion validity for the Chinese version of the CATI was only evaluated based on the total score of the AQ. In future research, it is necessary to apply content-matched scales for the criterion validity analysis of each subscale of the Chinese version of the CATI. Furthermore, though the Chinese version of the CATI involved a broad range of autistic trait dimensions,43 it still absent some dimensions such as “hypo-responsiveness of sensory input”,44 “restricted interests”,45 and “rumination”,46 therefore, developing the above absence dimensions would be an area worthy of the future.
Conclusion
Although the current study has limitations, it contributes to the body of evidence supporting the psychometric properties of the CATI in non-Western settings. It is beneficial for a more comprehensive understanding of autism traits in the general population should be assessed. The CATI is one of the most comprehensive self-reported measures currently available, even though it does not reflect every aspect of autism. Examining the psychometric properties of the Chinese version of the CATI will promote autistic trait-related research and cross-cultural studies.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval
All procedures were performed by the ethical standards in the 1964 Declaration of Helsinki and its later amendments. The Ethics Committee of Anhui Normal University (AHNU-ET2019015) approved the study. All the respondents participated voluntarily, and informed consent was obtained before the investigation.
Acknowledgments
The authors would like to thank Dr. Michael C. W. English, the author of the original scale, who has provided helpful advice for the current study’s design and his support and contribution in back-translating the Chinese version of the CATI.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Anhui Topnotch Talents of Disciplines in Universities and Colleges (gxbjZD2020002), the University Synergy Innovation Program of Anhui Province (GXXT-2021-003), the Humanities and Social Science Research Project of the Education Department of Anhui Province (SK2018ZD021), and the Humanities and Social Science Research Project of Henan Province (2020-ZZJH-473) supported this study.
Disclosure
The authors declare there are no competing interests in this work.
References
1. Zeidan J, Fombonne E, Scorah J, et al. Global prevalence of autism: a systematic review update. Autism Res. 2022;15(5):778–790. doi:10.1002/aur.2696
2. Sun X, Allison C, Wei L, et al. Autism prevalence in China is comparable to Western prevalence. Mol Autism. 2019;10(1):1–19. doi:10.1186/s13229-018-0246-0
3. Brosnan M, Lewton M, Ashwin C. Reasoning on the autism spectrum: a dual process theory account. J Autism Dev Disord. 2016;46(6):2115–2125. doi:10.1007/s10803-016-2742-4
4. Kanner L. Autistic disturbances of affective contact. Nerv Child. 1943;2(3):217–250. doi:10.1177/1362361318766571
5. Bralten J, Van Hulzen K, Martens M, et al. Autism spectrum disorders and autistic traits share genetics and biology. Mol Psychiatry. 2018;23(5):1205–1212. doi:10.1038/mp.2017.98
6. Ronald A, Hoekstra RA. Autism spectrum disorders and autistic traits: a decade of new twin studies. Am J Med Genet B. 2011;156(3):255–274. doi:10.1002/ajmg.b.31159
7. Robinson EB, Munir K, Munafò MR, Hughes M, McCormick MC, Koenen KC. Stability of autistic traits in the general population: further evidence for a continuum of impairment. J Am Acad Child Psychiatry. 2011;50(4):376–384. doi:10.1016/j.jaac.2011.01.005
8. Thomas TR, Koomar T, Casten LG, Tener AJ, Bahl E, Michaelson JJ. Clinical autism subscales have common genetic liabilities that are heritable, pleiotropic, and generalizable to the general population. Transl Psychiatry. 2022;12(1):247. doi:10.1038/s41398-022-01982-2
9. Zhang W, Zhuo S, Li X, Peng W. Autistic traits and empathy for others’ pain among the general population: test of the mediating effects of first-hand pain sensitivity. J Autism Dev Disord. 2022;1–15. doi:10.1007/s10803-022-05471-9
10. Wakabayashi A, Baron-Cohen S, Wheelwright S. Are autistic traits an independent personality dimension? A study of the Autism-Spectrum Quotient (AQ) and the NEO-PI-R. Pers Individ Differ. 2006;41(5):873–883. doi:10.1016/j.paid.2006.04.003
11. Lodi-Smith J, Rodgers JD, Cunningham SA, Lopata C, Thomeer ML. Meta-analysis of big five personality traits in autism spectrum disorder. Autism. 2019;23(3):556–565. doi:10.1177/1362361318766571
12. Ruzich E, Allison C, Smith P, et al. Measuring autistic traits in the general population: a systematic review of the Autism-Spectrum Quotient (AQ) in a nonclinical population sample of 6900 typical adult males and females. Mol Autism. 2015;6:2. doi:10.1186/2040-2392-6-2doi:10.1186/2040-2392-6-2
13. Constantino JN, Todd RD. Intergenerational transmission of subthreshold autistic traits in the general population. Biol Psychiatry. 2005;57(6):655–660. doi:10.1016/j.biopsych.2004.12.014
14. Iannuzzo F, Genovese G, Lombardo C, et al. Autistic traits, arousal, and gender features in a nonclinical sample of Italian adolescents. Int J Environ Res Public Health. 2022;20(1):693. doi:10.3390/ijerph20010693
15. Wing L. The continuum of autistic characteristics. In: Schopler E, Mesibov GB, editors. Diagnosis and Assessment in Autism. Boston: Springer Press; 1988:91–110.
16. Lundström S, Chang Z, Råstam M, et al. Autism spectrum disorders and autisticlike traits. Arch Gen Psychiatry. 2012;69(1):46–52. doi:10.1001/archgenpsychiatry.2011.144
17. More RP, Warrier V, Brunel H, et al. Identifying rare genetic variants in 21 highly multiplex autism families: the role of diagnosis and autistic traits. Mol Psychiatry. 2023:1–10. doi:10.1038/s41380-022-01938-4
18. Taylor MJ, Rosenqvist MA, Larsson H, et al. Etiology of autism spectrum disorders and autistic traits over time. JAMA Psychiatry. 2020;77(9):936–943. doi:10.1001/jamapsychiatry.2020.0680
19. Robinson EB, St Pourcain B, Anttila V, et al. Genetic risk for autism spectrum disorders and neuropsychiatric variation in the general population. Nat Genet. 2016;48(5):552–555. doi:10.1038/ng.3529
20. Abu-Akel A, Allison C, Baron-Cohen S, Heinke D. The distribution of autistic traits across the autism spectrum: evidence for discontinuous dimensional subpopulations underlying the autism continuum. Mol Autism. 2019;10(1):1–13. doi:10.1186/s13229-019-0275-3
21. Arenella M, Cadby G, De Witte W, et al. Potential role for immune-related genes in autism spectrum disorders: evidence from genome-wide association meta-analysis of autistic traits. Autism. 2022;26(2):361–372. doi:10.1177/13623613211019547
22. Ten Hoopen LW, de Nijs PF, Slappendel G, et al. Associations between autism traits and family functioning over time in autistic and non-autistic children. Autism. 2023:136236132311517. doi:10.1177/13623613231151784
23. Loukusa S, Gabbatore I, Kotila AR, et al. Non‐linguistic comprehension, social inference, and empathizing skills in autistic young adults, young adults with autistic traits and control young adults: group differences and interrelatedness of skills. Int J Lang Commun Disord. 2023. doi:10.1111/1460-6984.12848
24. Skuse DH, Mandy WP, Scourfield J. Measuring autistic traits: heritability, reliability, and validity of the social and communication disorders checklist. Br J Psychiatry. 2005;187(6):568–572. doi:10.1192/bjp.187.6.568
25. Constantino JN, Davis SA, Todd RD, et al. Validation of a brief quantitative measure of autistic traits: comparison of the social responsiveness scale with the autism diagnostic interview-revised. J Autism Dev Disord. 2003;33(4):427–433. doi:10.1023/A:1025014929212
26. Hurley RS, Losh M, Parlier M, Reznick JS, Piven J. The broad autism phenotype questionnaire. J Autism Dev Disord. 2007;37(9):1679–1690. doi:10.1007/s10803-006-0299-3
27. Maenner MJ, Rice CE, Arneson CL, et al. Potential impact of DSM-5 criteria on autism spectrum disorder prevalence estimates. JAMA Psychiatry. 2014;71(3):292–300. doi:10.1001/jamapsychiatry.2013.3893
28. Dell’Osso L, Dalle Luche R, Gesi C, Moroni I, Carmassi C, Maj M. From asperger’s autistischen psychopathen to DSM-5 autism spectrum disorder and beyond: a subthreshold autism spectrum model. Clin Pract Epidemiol Ment Health. 2016;12:120. doi:10.2174/1745017901612010120
29. Kanne SM, Mazurek MO. Aggression in children and adolescents with ASD: prevalence and risk factors. J Autism Dev Disord. 2011;41(7):926–937. doi:10.1007/s10803-010-1118-4
30. Dell’Osso L, Gesi C, Massimetti E, et al. Adult Autism Subthreshold Spectrum (AdAS spectrum): validation of a questionnaire investigating subthreshold autism spectrum. Compr Psychiatry. 2017;73:61–83. doi:10.1016/j.comppsych.2016.11.001
31. Grzadzinski R, Huerta M, Lord C. DSM-5 and autism spectrum disorders (ASDs): an opportunity for identifying ASD subtypes. Mol Autism. 2013;4(1):1–6. doi:10.1186/2040-2392-4-12
32. English MC, Gignac GE, Visser TA, Whitehouse AJ, Enns JT, Maybery MT. The Comprehensive Autistic Trait Inventory (CATI): development and validation of a new measure of autistic traits in the general population. Mol Autism. 2021;12(1):1–23. doi:10.1186/s13229-021-00445-7
33. Convery I, Cox D. A review of research ethics in internet-based research. Pract Res Higher Educ. 2012;6(1):50–57.
34. Baron-Cohen S, Wheelwright S, Skinner R, Martin J, Clubley E. The autism-spectrum quotient (AQ): evidence from asperger syndrome/high-functioning autism, males and females, scientists, and mathematicians. J Autism Dev Disord. 2001;31(1):5–17. doi:10.1023/A:1005653411471
35. Zhang L, Sun Y, Chen F, et al. Psychometric properties of the autism-spectrum quotient in both clinical and non-clinical samples: Chinese version for mainland China. BMC Psychiatry. 2016;16(1):1–10. doi:10.1186/s12888-016-0915-5
36. SPSS I. Corp Ibm SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM Corp, Released; 2018.
37. Lt H, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Modeling. 1999;6(1):1–55. doi:10.1080/10705519909540118
38. Shi D, Maydeu-Olivares A, DiStefano C. The relationship between the standardized root mean square residual and model misspecification in factor analysis models. Multivar Behav Res. 2018;53(5):676–694. doi:10.1080/00273171.2018.1476221
39. Franke G, Sarstedt M. Heuristics versus statistics in discriminant validity testing: a comparison of four procedures. Int Res. 2019;29(3):430–447. doi:10.1108/IntR-12-2017-0515
40. Henseler J, Ringle CM, Sarstedt M. A new criterion for assessing discriminant validity in variance-based structural equation modeling. J Acad Mark Sci. 2015;43(1):115–135. doi:10.1007/s11747-014-0403-8
41. Cheung GW, Rensvold RB. Evaluating goodness-of-fit indexes for testing measurement invariance. Struct Equ Modeling. 2002;9(2):233–255. doi:10.1207/S15328007SEM0902_5
42. Chen FF. Sensitivity of goodness of fit indexes to lack of measurement invariance. Struct Equ Modeling. 2007;14(3):464–504. doi:10.1080/10705510701301834
43. Donati MA, Berrocal C, Primi C, et al. Measuring subthreshold autistic traits in the general population: psychometric properties of the Adult Autism Subthreshold Spectrum (AdAS spectrum) scale. Psychiatry Res. 2019;281:112576. doi:10.1016/j.psychres.2019.112576
44. Wolff JJ, Dimian AF, Botteron KN, et al. A longitudinal study of parent‐reported sensory responsiveness in toddlers at‐risk for autism. J Clin Child Psychol. 2019;60(3):314–324. doi:10.1111/jcpp.12978
45. Volkmar FR, McPartland JC. From kanner to DSM-5: autism as an evolving diagnostic concept. Annu Rev Clin Psychol. 2014;10:193–212. doi:10.1146/annurev-clinpsy-032813-153710
46. Golan O, Haruvi-Lamdan N, Laor N, Horesh D. The comorbidity between autism spectrum disorder and post-traumatic stress disorder is mediated by brooding rumination. Autism. 2022;26(2):538–544. doi:10.1177/13623613211035240
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cultural Adaptation and Psychometric Evaluation of the Chinese Version of the Perceived Stress Reactivity Scale
Qu X, Luo Y, Liu Y, He X, Zhang Y
Psychology Research and Behavior Management 2025, 18:375-385
Published Date: 22 February 2025