")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Psychometric Evaluation of the Polish Version of the Caregiver Priorities and Child Health Index of Life with Disabilities (CPCHILD)
Authors Nowak P , Narayanan U, Szmurło M, Krzyżańska A, Głowacki M, Misterska E, Jóźwiak M
Received 25 August 2021
Accepted for publication 22 December 2021
Published 7 April 2022 Volume 2022:18 Pages 773—785
DOI https://doi.org/10.2147/NDT.S329070
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Paulina Nowak,1 Unni Narayanan,2 Małgorzata Szmurło,3 Anna Krzyżańska,1 Maciej Głowacki,1 Ewa Misterska,4 Marek Jóźwiak1
1Pediatric Orthopedics and Traumatology Department, K. Marcinkowski Medical University W. Dega Orthopedics and Rehabilitation Hospital, Poznan, Poland; 2Division of Orthopaedic Surgery Department, The Hospital for Sick Children, University of Toronto, Toronto, Canada; 3Rehabilitation Department, St Ludwik’s Hospital, Krakow, Poland; 4Department of Pedagogy and Psychology, University of Security, Poznan, Poland
Correspondence: Paulina Nowak, Orthopedics and Traumatology Department, K. Marcinkowski Medical University W. Dega Orthopedics and Rehabilitation Hospital, Poznan, Poland, Tel +48 697467704, Email [email protected]
Purpose: The assessment of the quality of life is an important element of the clinical examination of the patient. The aim of this study was translation and cross-cultural adaptation of the “Caregiver Priorities and Child Health Index of Life with Disabilities” (CPCHILD) questionnaire into Polish language, and testing of reliability and validity of the CPCHILD-PL for children with cerebral palsy (CP).
Material and Methods: A Polish version of CPCHILD was created according to internationally accepted guidelines. Parents (n=77) of 51 boys/26 girls between 3 and 17 years with CP with Gross Motor Function Classification System I–V (GMFCS I–V) participated. To assess the reliability each domain and the total measure was tested for internal consistency and test-retest reliability. Convergent validity was evaluated by correlating the CPCHILD-PL with the CHAQ (Childhood Health Assessment Questionnaire) questionnaire.
Results: Test-retest reliability assessed by Spearman correlation coefficient for the final result of CPCHILD-PL and for most of domains were above 0.90. The values of Cronbach’s-α coefficient (measuring internal consistency) were high for all domains (except for domain 5: Health) and the entire CPCHILD-PL, with the range 0.88– 0.96. The comparison between CPCHILD-PL and the Disability Index (DI) of the CHAQ showed a negative correlation. The higher the DI, the lower the CPCHILD result. The Spearman’s rank coefficient was − 0.75.
Conclusion: The Polish version for the CPCHILD for children with CP seems to be reliable and valid tool for assessing health-related quality of life from the caregiver perspective. It can be used in research and clinical practice for evaluation and comparison of health-related quality of life in children with CP in different countries.
Keywords: cerebral palsy, health-related quality of life, CPCHILD, validity, reliability
Introduction
Cerebral palsy (CP) describes a group of disorders of the development of movement and posture, causing activity limitation, that are attributed to non-progressive disturbances that occurred in the developing fetal or infant brain. The motor disorders of CP are often accompanied by disturbances of cognition, communication, sensation, perception and/or behavior, and/or by seizure disorder and can lead to secondary musculoskeletal problems such as muscle contractures, joint instability and deformities of the limbs and trunk.1 CP is the most common cause of physical disability in children and adolescents.2 The prevalence of CP is 1.5 to 3.3 per 1000 live-born children.3,4
Children with CP experience difficulties with activity and participation in daily life. The significant change is observed in the practice in childhood disability due to cerebral palsy from treating the body structure to improving the participation. It has a special importance in pediatric neuro-orthopedic clinical approach to the decision making process. Research has highlighted the importance of recognizing the impact of CP or its management on the well-being or health-related quality of life (HRQL) of children with CP5–8 as well as on their parents or caregivers9,10 or teachers.11 There is an imperative to evaluate the effectiveness of interventions for CP in terms of the child’s HRQL. Although it is important to consider the child’s priorities whenever possible, this is often a challenge when the child is too young or cognitively very impaired, as is often the case in children with severe CP. The perspectives of parents or caregivers must also be considered. Parent/s or caregiver/s have the most intimate knowledge of their child, their symptoms and the difficulties associated with their care. Clinicians often rely on parents to understand the child’s problems and to recommend interventions to address their challenges. Furthermore, the impact of CP and its management often extends beyond the child to the family at large. In Poland, there are currently no language or culturally appropriate tools available to capture the perspectives of parents or caregivers of children with severe disabilities or to measure the outcomes of interventions for this population.
The Caregiver Priorities & Child Health Index of Life with Disabilities (CPCHILD) is a condition-specific outcome measure that was developed specifically for children with severe (non-ambulatory) CP and other acquired brain injuries, who are reliant on a wheelchair for their mobility and on a caregiver for most of their activities of daily living (GMFCS levels IV & V).12 The questionnaire assesses the parents’/caregivers’ perspective about the comfort, ease of care, health and well-being of their child. The CPCHILD is used for longitudinal monitoring of these domains, to inform clinical decision-making and to assess treatment outcomes. The CPCHILD has robust psychometric properties and high clinical relevance.13 It has been translated into many other. It is used in many scientific studies as a tool to evaluate the HRQL of children with severe CP14 and as the primary outcome measure of various interventions for this population.5,15–20
In Poland, it does not devote too much attention to the needs of parents /caregiver of disable child. The main reason is the lack of appropriate assessment tools which are adopted to polish language and culture.
The aim of this study is to translate and culturally adapt the CPCHILD questionnaire (parent /caregiver version) into Polish, and to analyze the reliability and validity of CPCHILD-PL for use in children with severe CP.
Materials and Methods
A. Translation, Back Translation & Cultural Adaptation
Linguistic and cultural adaptation of the CPCHILD questionnaire was carried out after obtaining the consent of the developers of the questionnaire (Narayanan et al) and The Hospital for Sick Children, Toronto, Canada.12 The questionnaire was translated in accordance with the rules of Beaton et al.13
The process of language and cultural adaptation.
Translation of the CPCHILD questionnaire has been comprised several stages. In the first stage, 2 translators working independently translated the original version of the questionnaire into Polish; and one of them, who had a medical background, the other translator with no medical background. Polish was the native language of these translators. In the second stage, the team of 2 translators and project authors compared both translations, then pinpointed the differences and produced a version, which was a consensus between both translators. In the third stage, 2 native English speakers translated the final translated Polish version into English. None of these translators had knowledge of the original version of the Questionnaire in English. The purpose of back translation process was to ensure that the Polish version accurately conveys the contents of the original version and to detect the potential inconsistencies. In the final stage, a committee of 2 orthopedic surgeons, translators, psychologist and two physiotherapists reviewed all the translations to create a prefinal version of the Questionnaire. The aim of the committee was to reach a consensus with regard to all the inconsistencies found in the translations.
B. Psychometric Evaluation of the Polish Version of the CPCHILD
Participants were the parents or primary (legal) caregivers of children with CP who were recruited in two institutions of the authors in Poland. Children were classified according to their GMFCS level.21 Inclusion criteria were: 1) children with cerebral palsy, 2) age between 3 and 18 years old, and the exclusion criteria were: 1) questionnaires with empty fields, 2) questionnaire were filled up only one time.
Measurements
The CPCHILD questionnaire consists of 36 items over 6 domains or subscales. Domains (1) Personal care and Activities of daily livings (9 items) and (2) Positioning, Transferring and Mobility (8 items)) are both rated both in terms of the degree of difficulty associated with each activity or task (7-point scale, from 0 - impossible, to 6 - no difficulty) and the level of assistance required to accomplish these activities/tasks (4-point scale, from 0 - total assistance, to 3 - independent). Items in domain (3) Comfort and Emotions (9 items) are rated both by the frequency of the symptom (6 point scale from 0 - daily to 5 - never) and the intensity of the symptom (4 point scale from 0 - severe to 3 - does not occur). Domain (4) Communication and Social interaction (7 items) assesses the degree of difficulty on a 7-point scale (0 - impossible to 6 - no problem). Domain (5) Health is comprised of 3 items and Domain (6) Overall quality of life has a single item. There is a seventh section on the importance of the contribution of individual items (from all the domains) on the quality of life of the child, rated on a 7-point scale (0 - least important to 6 - most important). Demographic information is collected in sections (8) Information about your child (3 items); and (9) Information about you (the parent or caregiver respondent) (6 items).
Additionally, in the first 4 domains the respondent may add two additional tasks/activities of daily living/symptoms/social activities important to child or the parent /caregiver that may not have been included in the questionnaire. The CPCHILD generates standardized scores from 0 (worst) to 100 (best) for the total and each of the domains.
The Childhood Health Assessment Questionnaire (CHAQ)22 was used to assess convergent validity of the CPCHILD-PL questionnaire, by comparing the scores of the two instruments. CHAQ is a generic measure of health status of children with chronic conditions like juvenile arthritis or other inflammatory diseases (juvenile dermatomyositis, juvenile systemic lupus erythematodus, etc.). It evaluates functional abilities across 8 domains (dressing and self-care, getting up, eating, walking, hygiene, skills, grasping, classes). Each question contains a 5-point scale of difficulty (without difficulty, with some difficulty, with great difficulty, cannot do, it does not apply). The result is referred to as the Disability Index (DI), the higher the greater the child’s disability. It also includes two visual analog scales (VAS) referring to the pain and quality of life of the child.22–24 The CHAQ questionnaire has been used in studies of children with CP.8
Parents or caregivers completed the self-administered CPCHILD questionnaire twice two days apart. Items in the CPCHILD refer to the child’s condition in the previous 2 weeks. During the first test, the parent /caregiver received the CPCHILD and Childhood Health Assessment Questionnaire (CHAQ) questionnaires; and only the CPCHILD questionnaire at the second round. The protocol required that the second administration was completed by the same caregiver. The written consent for study participation from each primary caregiver was obtained. Responses were analyzed if the CPCHILD questionnaire was completed in full. Thirteen respondents were excluded due to the lack of response to at least 1 question on the CPCHILD.
Statistical Analysis
Data were analyzed using the Statistical program.
The CPCHILD questionnaires from the 1st round were analyzed for Internal Consistency of each of the subscales using Crohnbach-α. The results are interpreted as follows: ≥ 0.8 - very good; 0.7–0.79 – good; < 0.7 - poor internal consistency. The sample size was 112.
Test-retest reliability to evaluate the stability of the CPCHILD-PL was tested in those who completed both administrations of the CPCHILD (n=77). The scores of the two administrations were compared using the Spearman’s rank correlation coefficient (rs) to describe the correlation strength between the scores because data didn't have a normal distribution. Wilcoxon signed-rank test was used to compare the difference between the paired groups and scores in each administration.
Convergent validity was evaluated by correlating the responses of CPCHILD-PL questionnaire with the CHAQ which measures some similar clinical constructs. The sample size was 77. Specifically, correlation was evaluated between: (1) the total score of the CPCHILD-PL questionnaire and CHAQ Disability Index (DI); (2) Section 3: Comfort and emotions in the CPCHILD-PL questionnaire and the VAS of pain in the CHAQ questionnaire, (3) Section 6: Child’s overall quality of life in the CPCHILD-PL questionnaire and values of the VAS for overall well-being in the CHAQ questionnaire. The Spearman’s rank correlation coefficient was calculated to determine the correlation strength of variables that did not have a normal distribution. The compliance factor of Kendall (W) was also used to check the association between the total scores of the CPCHILD-PL and the Disability Index of the CHAQ. Its values are in the range 0 to 1 and are interpreted as follows: W ~ 1 - means strong compatibility; W ~ 0 - means no match. In order to calculate the above index, both variables were transformed to the interval (0 to 1), and the CHAQ variable was additionally reversed to maintain the same direction of the variable of the CHAQ as in CPCHILD-PL. The significance level was set at p<0.05 at two-tailed level.
Finally, content validity was assessed using the seventh section of the CPCHILD-PL which recorded the parents’ perception of the importance of each item’s contribution to their child’s quality of life. A mean rating of importance of ≥ 2 or “slightly important” would confirm the importance of the item and justification for its retention.
Results
There were 112 participants who completed the first round and 77 in the second. Due to lower number of responders in the second study, data for the same 77 responders from the first study was take into account in statistical calculations (Tables 1 and 2). The average age of children for the study group (n=77) was 10.97 (SD 4.30; 3–17 years). The ratio of boys and girls was 51:26. Parents/caregivers were predominantly women (70 respondents). The number of children in each GMFCS level in first and second study are shown at Figure 1. The mean (SD; range) of the Total CPCHILD scores across all GMFCS levels was 60.33 (18.2; 28.8 to 95.7). The CPCHILD scores for the population for which it is intended, (GMFCS IV & V), showed mean total scores of 55.59 (SD 10.44; range 36.69–71.75) and 41.62 (SD 8.9; range 28.77–63.11) for GMFCS IV & V respectively, and mean total score 47.15 (SD 12.98; range 26.72–75.96) for GMFCS IV and V together. This shows a wide range of values with no evidence of floor or ceiling effects.
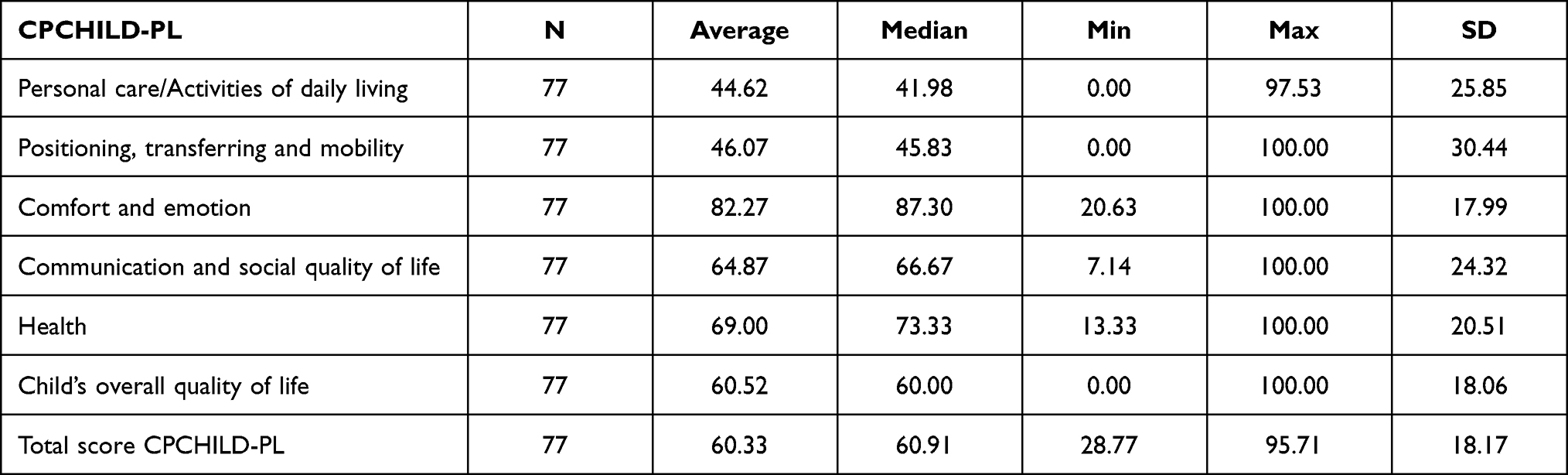 |
Table 1 Descriptive Statistic for Study Group in First Study. Data is Shown for 77 Responders Only Due to the Same Number in the Second Study |
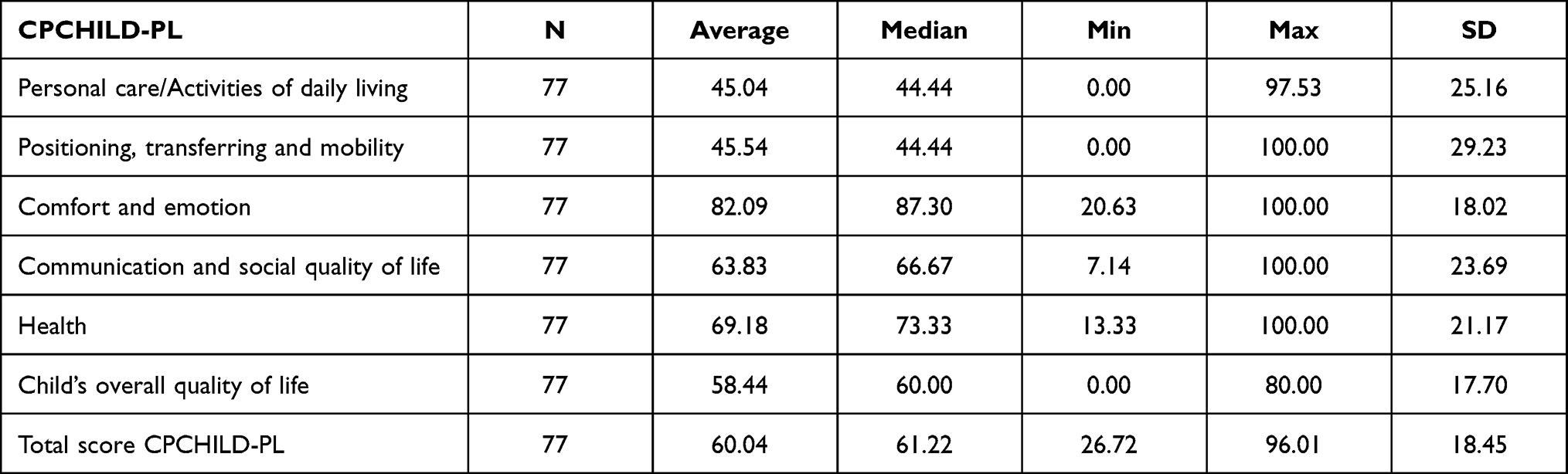 |
Table 2 Descriptive Statistic Study Group in Second Study (n=77) |
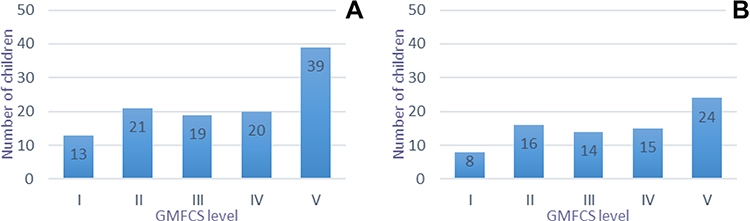 |
Figure 1 The number of children in each GMFCS level in first study (A), and second study (B). |
Internal Consistency (Table 3)
The values of Cronbach- α were very good (> 0.80) in all domains of CPCHILD except domain 5: Health, had Cronbach- α coefficient - 0.50 (Table 3). Cronbach- α coefficient was not calculated for Domain 6 since it contains only one item. The value of Cronbach- α coefficient for the total score was 0.96.
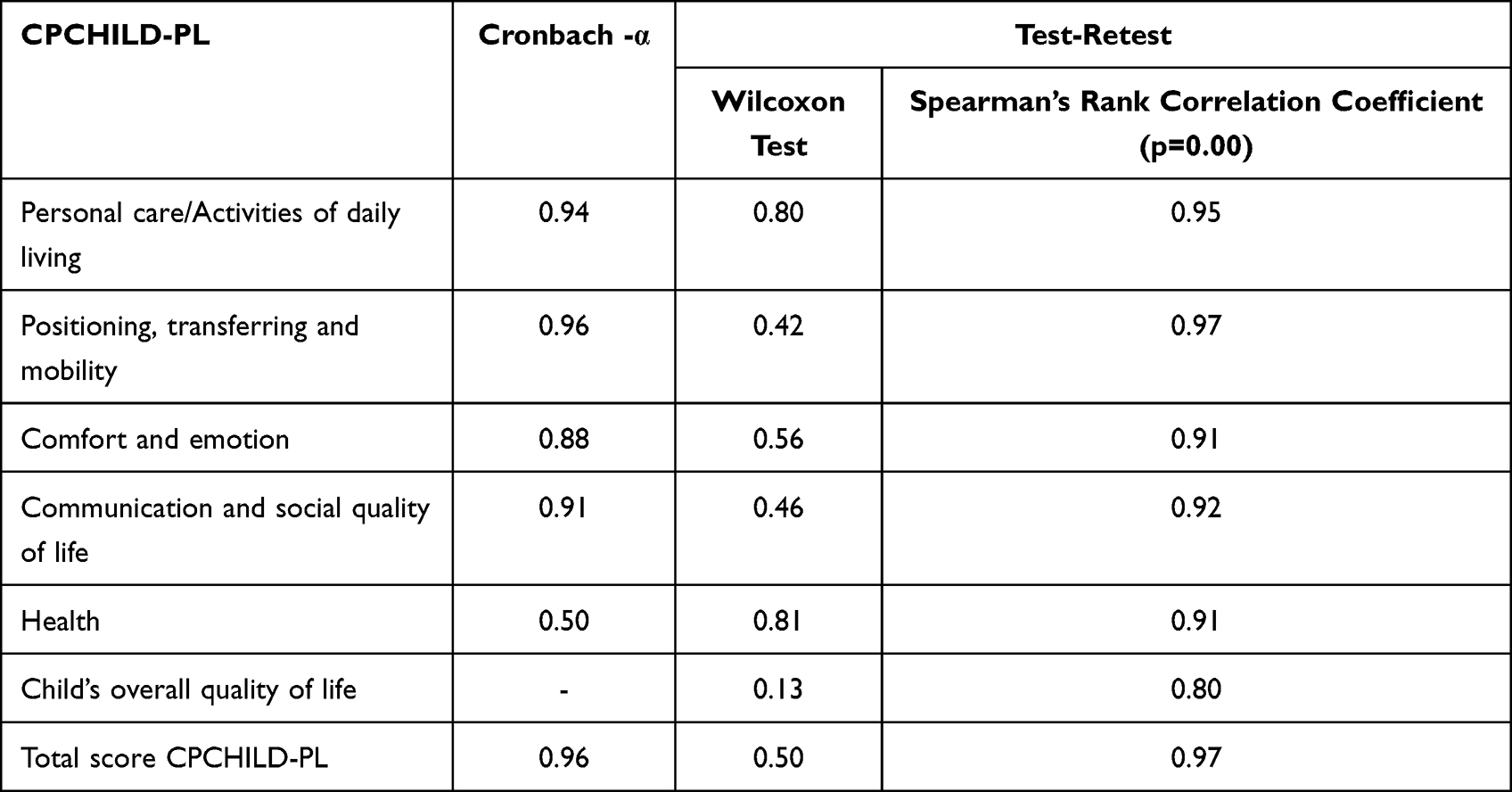 |
Table 3 Values of Cronbach- α Coefficient and Test-Retest for the Final Result and for Individual Domains of CPCHILD-PL |
Test-Retest Reliability
There was a strong positive correlation between the domain and total scores of both administrations with the Spearman correlation coefficient ranging from 0.80 to 0.95 for all the domains; and 0.97 for the total scores of CPCHILD-PL (Table 3).
In the Wilcoxon test, the results of the entire questionnaire and its specific domains had p values of > 0.05, which indicates the concordance of the CPCHILD questionnaire in the first and second tests (details in Table 3).
Known Groups Construct Validity
The CPCHILD-PL mean total scores significantly decreased as hypothesized with increasing GMFCS level (Figure 2). The lower the GMFCS level, the higher the CPCHILD-PL score. Non-ambulatory children (GMFCS IV & V) overall scored significantly less on than the ambulatory children (GMFCS I–III). The differences between each GMFCS level were significant between GMFCS levels III and IV (p <0.05), III and V (p<0.05), and between levels IV and V (p<0.05).
 |
Figure 2 Standardized total score in each GMFCS level in first study (A) and second study (B). |
Convergent Validity
The correlation the total scores of CPCHILD-PL and Disability Index score of the CHAQ questionnaire showed that the higher the DI (worse disability), the lower the CPCHILD score. The Spearman’s rank coefficient was −0.75 (p = 0.00) (Figure 3).
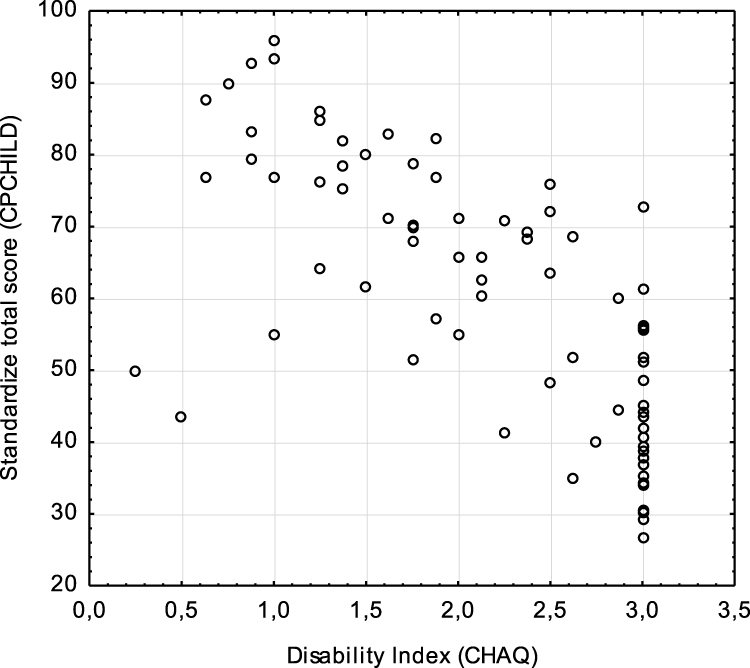 |
Figure 3 Correlation between the standardize total score of CPCHILD-PL and Disability Index (CHAQ). |
Concordance factor W Kendall for the CPCHILD and CHAQ -DI questionnaires was 0.70, suggesting that the strength of this association is high.
Results on “Pain” in the CHAQ questionnaire and domain (3) of CPCHILD-PL: Comfort and Emotions were compared. The higher the score in domain (3) in CPCHILD (better pain scores), the lower the score on the “Pain” scale in CHAQ (lower pain scores) (Figure 4). Comparison between the general quality of life scale of CHAQ and section 6: The overall quality of life of the CPCHILD-PL showed that the higher the results on the CHAQ scale (lower QOL), the lower the results in domain 6 of the CPCHILD (Figure 5).
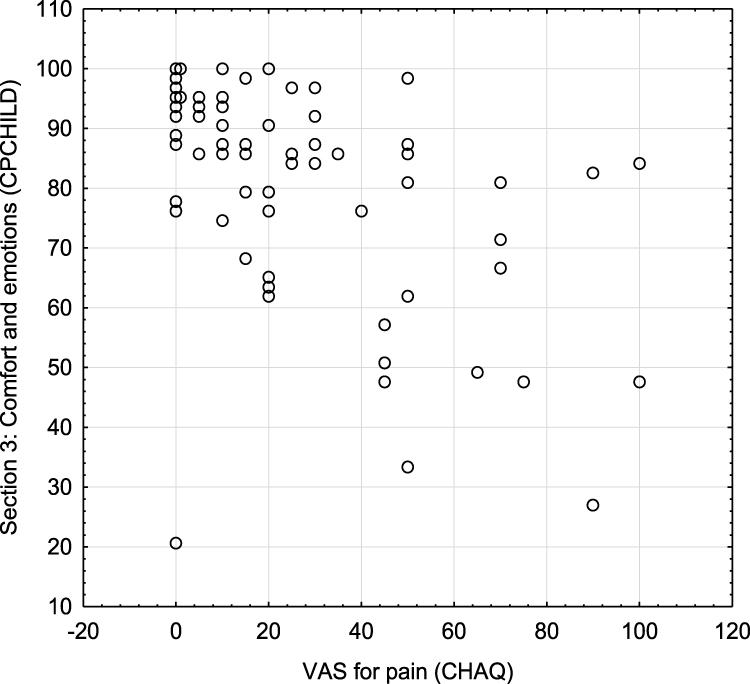 |
Figure 4 Correlation between VAS for pain (CHAQ) and section 3: Comfort and emotions (CPCHILD-PL). |
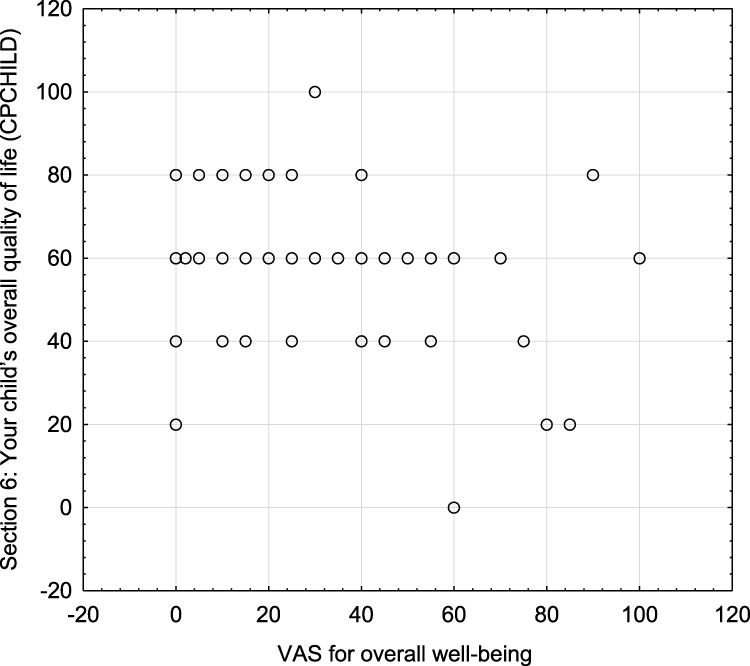 |
Figure 5 Correlation between VAS of overall well-being (CHAQ) and domain 6: Child’s overall child quality (CPCHILD-PL). |
Importance of Items: Content Validity
We also examined the importance ratings that parents/caregivers gave to individual items in domain 7 of the CPCHILD-PL questionnaire as a way to establish the relevance of content validity of the items. The mean importance ratings for all the items was 3.41 (SD 1.23), with the mean importance not falling below the threshold of 2.0 or at least “slightly important” for any item. Items related to Comfort (Section 3), Communication & Social Interaction (Section 4) and Health (Section 5) were rated slightly more important contributors to children’s QOL than items related to Personal Care (Section 1) and Mobility (Section 2) (Figure 6).
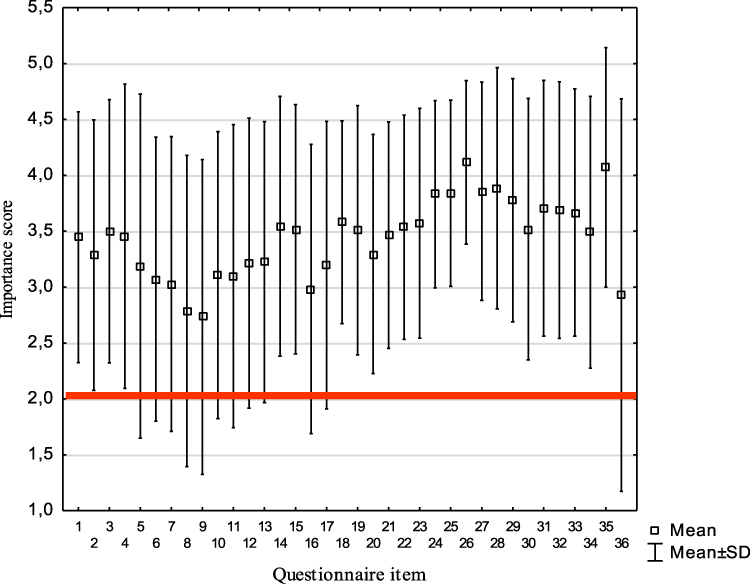 |
Figure 6 Mean importance score with standard deviation in section 7: Importance of items to child’s quality of life. |
Summary
In most of the CPCHILD domains internal consistency is very good. Test -retest reliability showed strong positive correlation between domain and total scores of both administrations. The statistical analysis showed also positive correlation between total score of CPCHILD and Disability Index of the CHAQ, We noticed that in higher GMFCS level the CPCHILD-PL mean total scores were lower.
Discussion
To date, little attention has been paid to evaluation of the priorities and needs of the parents/caregivers of disabled children in Poland. There are currently, in our country, no language or culturally appropriate tools available to capture the perspectives of parents or caregivers of children with severe disabilities or to measure the outcomes of interventions for this population. The Polish version of CPCHILD-PL was developed specifically to address this gap and was then tested for its psychometric properties. The CPCHILD-PL was shown to have a high level of internal consistency, test-retest reliability, and construct validity, to justify its use in children with severe CP. With the exception of domain 5 for Health, Cronbach’s -α coefficient were high for all other domains and the CPCHILD-PL in its entirety. The range of values of 0.88–0.96 were similar to those noted for CPCHILD in other languages, including the original Canadian version 0.74–0.93,25 in the Korean version 0.92–0.96,26 the Norwegian version 0.74–0.93,27 the Dutch version 0.70–0.95.28 The lower Cronbach’s- α for Domain 5: “Health” may be a consequence of the small number of items (3 questions) in that domain and were similar to low values obtained in the Korean version of CPCHILD - 0.63,26 and the Dutch version of CPCHILD-DV - 0.60.28 This was in contrast to the higher values in the Canadian, 0.9025 and Norwegian, 0.8327 versions, respectively.
In order to assess convergent validity of the CPCHILD-PL, the CHAQ questionnaire was used. The CHAQ questionnaire has been used to study children with CP.8 The higher the CHAQ score, the lower the CPCHILD score. In other evaluations of the CPCHILD, the authors have variously compared it to and shown expected convergent validity with other generic measures such as the Pediatric Evaluation of Disability Inventory (PEDI) Caregiver assistance and Child Health Questionnaire (CHQ) in the Canadian study25 and TNO-AZL Preschool Children Quality of Life (TAPQOL) in the Dutch validation.28
The mean importance ratings for each item were all above the threshold of 2 or “slightly important”, confirming that the items of the CPCHILD-PL are believed to be important contributors to the child’s quality of life from the perspective of the parents of children with CP. There was however, not surprisingly, a wide range of the perception of importance of each item by different parents/caregivers. One would not expect all items to be equally important to all parents. As long as the included items in the CPCHILD-PL are deemed to be important by at least some parents and caregivers, and the overall mean rating of importance exceeds the threshold of at least “slightly important”, the items can be considered meaningful. This is an innovative approach of the CPCHILD-PL questionnaire to ensure that the parent’s or caregiver’s priorities are adequately captured.
There are some limitations to our study. The typical family model in Poland has one person (usually the mother) responsible for looking after the child, while the other (usually the father) is employed and is responsible for the financial needs of the family. For this research we focused on obtaining responses only from one parent or primary caregiver, who we defined was the person who spends most of her/his time with the child, knows and understands them best and can accurately determine the child’s problems and difficulties during everyday activities. In other validations of the CPCHILD such as the Canadian,25 Dutch,28 Korean,26 and German29 versions, both parents/caregivers completed the questionnaire.
For the test-re-test reliability, the time interval between the repeat administrations was only 2 days. This was done for convenience as many of the study participants were inpatients in the hospital prior to orthopaedic surgery, and the questionnaires were administered just before surgery and 2 days later (after surgery) while patients were still in the hospital. It is possible that recall bias might increase the reliability as the short interval between responses might make the initial responses easier to recall and replicate. In the other translations, the period between the first and the second questionnaire was: 2 weeks –Dutch,28 Canadian,25 German,29 or 4 weeks – Korean,26 Norwegian.27
We identified some weaknesses of the CPCHILD, related to the clarity of instructions to the respondents. An analysis of parents’ observations, and the results obtained made it necessary to make some modifications in CPCHILD-PL. When assessing the degree of difficulty of particular activities or tasks in domains (1): “Personal care/activities of daily living” and domain (2): “Positioning, transferring and mobility”, parents/caregivers sometimes gave answers based on the child’s abilities to accomplish (or not) the task, rather than the based on how the task was actually performed which might have involved the assistance of the parent/caregiver. We have made the instructions clearer to the respondents that the questions should be answered based on how the task is actually performed (which might be entirely assisted) rather than based on how the child might be able (or not) to do that task.
Another problem that some parents reported was related to items where multiple examples of a task were provided. For example in Domain (1): 1. “eating /drinking or being fed” (in the usual way that is done, ie orally or by tube) “; 4.”toileting activities” (bladder and bowel function, hygiene, etc.)”; 6.”putting on/taking off upper body clothing (shirt, jacket, etc.)”; 8. “Putting on/taking off the lower body clothing (pants, sweats, etc.)”; 9. “hair care (washing, drying, brushing/combing, braiding, etc.)” and in domain (2): items 11.”transferring into /out of a wheelchair/chair”; 16.”getting in and out of a motor vehicle (car, van, bus)”; and 17.”visiting public places (park, theatre, sightseeing, etc.)”. Parents reported that they were unsure about how to respond if the different activities included as examples for a single item had different levels of difficulty. They were unsure whether they were to base their responses on a more difficult or easier example of the task.
Table 4 presents all items requiring culture adaptation and validation to Polish conditions.
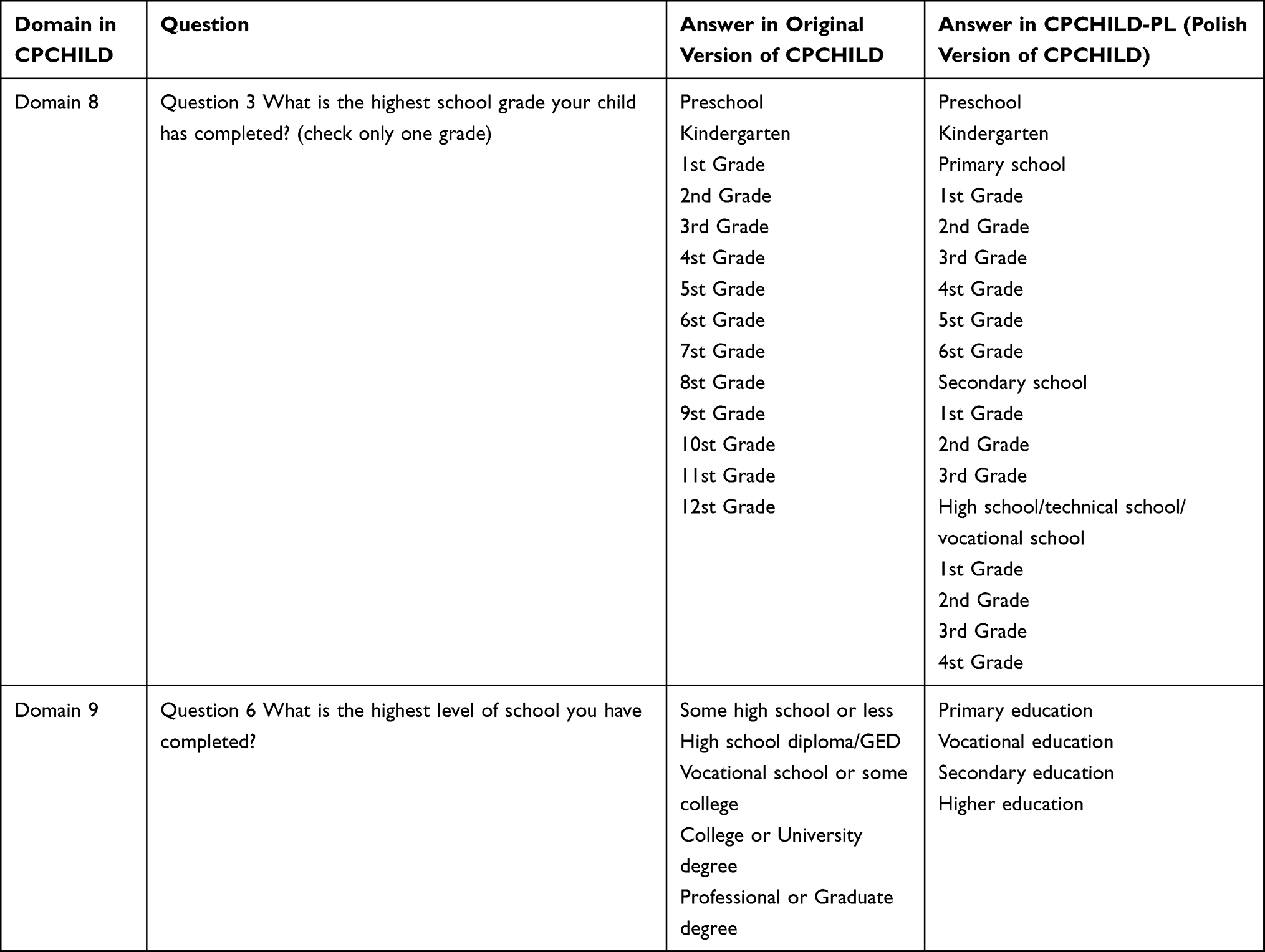 |
Table 4 Items Requiring Modification During the Cultural Adaptation to Polish Conditions |
Some respondents completed the initial part or degree of difficulty of a particular task but did not complete the second part which evaluates the level of assistance required to complete the task, which made their responses unscorable and invalid. Clearer instructions are necessary to bring to the attention of respondents that for each item both parts of questions must be answered: the degree of difficulty of the task (as usually performed) and the level of assistance usually required for the task (for domains 1 and 2), and frequency of symptoms and the intensity of the symptom (for domain 3).
During the translation, there was some difficulty in defining the instructions for domain 7: “The importance of items to child’s quality of life”. Some parents also reported difficulty in understanding this. We chose to simplify the instructions: Evaluate the importance of the following activities for the quality of the child’s life. Item 13. in the original assesses the degree of difficulty of “Standing for exercise /transfers”. This was changed to: “Participate in rehabilitation activities”.
The validation of the CPCHILD-PL revealed to the authors that completion of such a questionnaire was a unique experience for Polish parents. The questionnaire made the parents/caregivers explicitly think about various aspects of caring for their child, and about their child’s health and quality of life which uncovered the extent of their own efforts and sacrifices.
The CPCHILD questionnaire is a reliable and valid outcome measure of value to specialists (physicians, physiotherapists, psychologists, special educators) who care for children with severe CP or acquired brain injury. Its content includes the child’s physical, mental and social domains of functioning, which has been identified by their parents as relevant and important to their quality of life. In addition to its primary function as an outcome measure, the CPCHILD has the ability to identify problems and define goals more precisely to target treatment towards areas that score low and have also been identified as important. The translation and cultural adaptation of the CPCHILD to Polish will allow the wider use of CPCHILD-PL questionnaire for the benefit of children with severe CP in Poland.
Conclusions
The CPCHILD-PL questionnaire is a tool with high reliability and validity that can be used to test the health-related quality of life in children with CP from the perspective of a parent/caregiver.
Abbrevations
CHAQ, Childhood Health Assessment Questionnaire; CP, cerebral palsy; CPCHILD, Caregiver Priorities and Child Health Index of Life with Disabilities; CPCHILD-DV, Dutch version of Caregiver Priorities and Child Health Index of Life with Disabilities; CPCHILD-PL, Polish version of the Caregiver Priorities and Child Health Index of Life with Disabilities; DI, Disability Index; GMFCS, gross motor function classification system; HRQL, health-related quality of life; QOL, quality of life; SD, standard deviation; TAPQOL, TNO-AZL preschool children quality of life.
Declarations
We confirm that this study was conducted in accordance with Declaration of Helsinki.
Data Sharing Statement
The datasets during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Bioethical Commission of the Karol Marcinkowski Poznan University of Medical Science (288/13, 77/14). All parents/caregivers were informed as to the purpose of this study. The written consent for study participation from each primary caregiver was obtained.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Partial financial support was received from Poznan University of Medical Sciences.
Disclosure
Professor Unni Narayanan reports a patent CPCHILD is Copyrighted licensed to Marek Jozwiack; The authors declare that they have no other competing interests in this work.
References
1. Rosenbaum P, Paneth N, Leviton A, et al. A report: the definition and classification of cerebral palsy April 2006. Dev Med Child Neurol. 2007;109:8–14.
2. Odding E, Roebroeck ME, Stam HJ. The epidemiology of cerebral palsy: incidence, impairments and risk factors. Disabil Rehabil. 2006;28(4):183–191. doi:10.1080/09638280500158422
3. (SCPE) SoCPiE. Prevalence and characteristics of children with cerebral palsy in Europe. Dev Med Child Neurol. 2002;44(9):633–640.
4. Sellier E, Platt MJ, Andersen GL, Krägeloh-Mann I, De La Cruz J, Cans C. Decreasing prevalence in cerebral palsy: a multi-site European population-based study, 1980 to 2003. Dev Med Child Neurol. 2016;58(1):85–92. doi:10.1111/dmcn.12865
5. Hwang JH, Varte L, Kim HW, Lee DH, Park H. Salvage procedures for the painful chronically dislocated hip in cerebral palsy. Bone Joint J. 2016;98(1):137–143. doi:10.1302/0301-620X.98B1.35202
6. Lai C-J, Chen C-Y, Chen C-L, Chan P-YS, Shen IH, Wu C-Y. Longitudinal changes in health-related quality of life in preschool children with cerebral palsy of different levels of motor severity. Res Dev Disabil. 2017;61:11–18. doi:10.1016/j.ridd.2016.11.013
7. McCullough N, Parkes J. Use of the child health questionnaire in children with cerebral palsy: a systematic review and evaluation of the psychometric properties. J Pediatr Psychol. 2008;33(1):80–90. doi:10.1093/jpepsy/jsm070
8. Morales NMO, Funayama CAR, Rangel VO, et al. Psychometric properties of the Child Health Assessment Questionnaire (CHAQ) applied to children and adolescents with cerebral palsy. Health Qual Life Outcomes. 2008;6(1):109. doi:10.1186/1477-7525-6-109
9. Palisano RJ, Almarsi N, Chiarello LA, Orlin MN, Bagley A, Maggs J. Family needs of parents of children and youth with cerebral palsy. Child Care Health Dev. 2010;36(1):85–92. doi:10.1111/j.1365-2214.2009.01030.x
10. Raina P, Donnell M, Rosenbaum P, et al. The health and well-being of caregivers of children with cerebral palsy. Pediatrics. 2005;115(6):e626. doi:10.1542/peds.2004-1689
11. Crowe M, Maciver D, Rush R, Forsyth K. Psychometric evaluation of the ACHIEVE assessment. Front Pediatr. 2020;8:245. doi:10.3389/fped.2020.00245
12. Narayanan UG, Fehlings D, Weir S, Knights S, Kiran S, Campbell K. Initial development and validation of the Caregiver Priorities and Child Health Index of Life with Disabilities (CPCHILD). Dev Med Child Neurol. 2006;48(10):804–812. doi:10.1017/S0012162206001745
13. Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. 2000;25(24):3186–3191. doi:10.1097/00007632-200012150-00014
14. Jo BSM, Chung C, Kim K, et al. Validation of common questionnaires assessing physical activity using accelerometer in children and adolescents with cerebral palsy. Dev Med Child Neurol. 2015;57(S5):92–93.
15. DiFazio R, Shore B, Vessey JA, Miller PE, Snyder BD. Effect of hip reconstructive surgery on health-related quality of life of non-ambulatory children with cerebral palsy. J Bone Joint Surg Am. 2016;98(14):1190–1198. doi:10.2106/JBJS.15.01063
16. DiFazio RL, Miller PE, Vessey JA, Snyder BD. Health-related quality of life and care giver burden following spinal fusion in children with cerebral palsy. Spine. 2017;42(12):E733–E739. doi:10.1097/BRS.0000000000001940
17. Difazio RL, Vessey JA, Zurakowski D, Snyder BD. Differences in health-related quality of life and caregiver burden after hip and spine surgery in non-ambulatory children with severe cerebral palsy. Dev Med Child Neurol. 2016;58(3):298–305. doi:10.1111/dmcn.12872
18. Elema A, Zalmstra TAL, Boonstra AM, Narayanan UG, Reinders-Messelink HA, Putten AAJ. Pain and hospital admissions are important factors associated with quality of life in nonambulatory children. Acta Paediatrica. 2016;105(9):e419–e425. doi:10.1111/apa.13493
19. Narayanan U, Cahill P, Sponseller P, et al. Impact of corrective spinal fusion surgery on health related quality of life of children with cerebral palsy. Dev Med Child Neurol. 2016;58(S5):67–68.
20. Narayanan UG, Sponseller P, Newton PO, Marks MC. The CPCHILD questionnaire is sensitive to change following scoliosis surgery in children with cerebral palsy: PAPER #62. Spine J Meet Abstracts. 2011;2011:86–87.
21. Palisano R, Rosenbaum P, Walter S, Russell D, Wood E, Galuppi B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol. 1997;39(4):214–223. doi:10.1111/j.1469-8749.1997.tb07414.x
22. Romicka AM, Ruperto N, Gutowska-Grzegorczyk G, Musiej-Nowakowska E, Wyszynska E. (PRINTO) ftPRITO. The Polish version of the Childhood Health Assessment Questionnaire (CHAQ) and the Child Health Questionnaire (CHQ). Clin Exp Rheumatol. 2001;19(4Suppl.23):121–125.
23. Ruperto N, Ravelli A, Pistorio A, et al. Cross-cultural adaptation and psychometric evaluation of the Childhood Health Assessment Questionnaire (CHAQ) and the Child Health Questionnaire (CHQ) in 32 countries. Review of the general methodology. Clin Exp Rheumatol. 2001;19(4 Suppl 23):S1–9.
24. Singh G, Athreya BH, Fries JF, Goldsmith DP. Measurement of health status in children with juvenile rheumatoid arthritis. Arthritis Rheum. 1994;37(12):1761–1769. doi:10.1002/art.1780371209
25. Narayanan UG, Weir S, Fehlings DL. The Caregiver Priorities and Child Health Index of Life with Disabilities (CPCHILD) questionnaire. Manual and interpretation guide; 2007.
26. Sung KH, Kwon -S-S, Narayanan UG, et al. Transcultural adaptation and validation of the Korean version of caregiver priorities & Child Health Index of Life with Disabilities (CPCHILD). Disabil Rehabil. 2015;37(7):620–624. doi:10.3109/09638288.2014.932449
27. Pettersson K, Bjerke KM, Jahnsen R, Öhrvik J, Rodby-Bousquet E. Psychometric evaluation of the Scandinavian version of the caregiver priorities and child health index of life with disabilities. Disabil Rehabil. 2017;41:1–7. doi:10.1080/09638288.2017.1370498
28. Zalmstra TAL, Elema A, Boonstra AM, et al. Validation of the Caregiver Priorities and Child Health Index of Life with Disabilities (CPCHILD) in a sample of Dutch non-ambulatory children with cerebral palsy. Disabil Rehabil. 2015;37(5):411–416. doi:10.3109/09638288.2014.923524
29. Jung NH, Brix O, Bernius P, et al. German translation of the caregiver priorities and child health index of life with disabilities questionnaire: test–retest reliability and correlation with gross motor function in children with cerebral palsy. Neuropediatrics. 2014;45(5):289–293. doi:10.1055/s-0034-1372304
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.