Back to Journals » Psychology Research and Behavior Management » Volume 17
Psychometric and Circumplex Properties Evaluation of the International Personality Item Pool-Interpersonal Circumplex (IPIP-IPC) in Chinese People Living with HIV (PLWH)
Authors Wang X ![]() , Han S, Jia C, Yang X, Hu Y
, Han S, Jia C, Yang X, Hu Y ![]() , Zhang Y, Yang Z, Zhang L, Wang Z
, Zhang Y, Yang Z, Zhang L, Wang Z
Received 25 October 2023
Accepted for publication 10 February 2024
Published 22 February 2024 Volume 2024:17 Pages 705—724
DOI https://doi.org/10.2147/PRBM.S446547
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Xiaomeng Wang,1,* Shuyu Han,1,* Changli Jia,2,* Xianxia Yang,3 Yan Hu,4 Yukun Zhang,4 Zhongfang Yang,4 Lili Zhang,5 Zhiwen Wang1
1School of Nursing, Peking University, Beijing, 100191, People’s Republic of China; 2School of Medical and Health Management, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, 430030, People’s Republic of China; 3School of Public Health, Wuhan University, Wuhan, Hubei, 430071, People’s Republic of China; 4School of Nursing, Fudan University, Shanghai, 200032, People’s Republic of China; 5Department of Nursing, Beijing Youan Hospital Affiliated with Capital Medical University, Beijing, 100069, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shuyu Han; Zhiwen Wang, Email [email protected]; [email protected]
Background and Purpose: With the improved life expectancy of people living with HIV (PLWH) due to widespread use of antiretroviral therapy (ART), there is a greater emphasis on enhancing long-term well-being and overall quality of life for PLWH. Understanding interpersonal personalities of PLWH can gain further insight into how to improve the overall quality of life in this population. The International Personality Item Pool-Interpersonal Circumplex (IPIP-IPC) scale has been developed to assess interpersonal personalities of individuals, and this scale has been translated into Chinese. However, the Chinese version of IPIP-IPC has not been tested among PLWH in China. In this study, we aimed to test the psychometric properties and circumplex structure of this scale.
Methods: This study was based on cross-sectional, multi-center, large sample data. We employed the Chinese version of IPIP-IPC scale on 3040 PLWH from April 2022 to April 2023 in China to test its psychometric as well as circumplex properties. The structural summary method (SSM) was employed to analyze the circumplex structure of the scale.
Results: The total scale exhibited a Cronbach’s alpha of 0.85 and McDonald’s omega of 0.91. Out of the 288 possible relationships, 275 relationships satisfy the circular properties hypothesis. The scale demonstrates good reliability and validity, meeting the requirements of psychometrics.
Conclusion: Our findings demonstrate that the Chinese version of the IPIP-IPC scale is a reliable tool for evaluating interpersonal personalities in this population. These results highlight the validity and applicability of the IPIP-IPC scale specifically in the Chinese context, providing valuable insights into the intricacies of interpersonal traits among PLWH.
Keywords: AIDS, interpersonal personality, reliability, validity
Introduction
HIV has transformed from a nearly uniformly fatal infection to a chronic condition due to the development and popularization of antiretroviral therapy (ART).1 As of the end of 2022, 76% (65–89%) of people living with HIV (PLWH) were accessing ART.2 We have witnessed an increase in life expectancy in this population across various regions.3–7 For instance, a cohort study conducted in South Africa reported that PLWH on ART had life expectancies equivalent to approximately 80% of normal life expectancy, as long as they initiated treatment before their CD4 count fell below 200 cells/µL.4 In addition, according to cohort studies in Europe and North America, the life expectancy of PLWH who were on ART with high CD4 counts and survived to 2015, or initiated ART after 2015, was only a few years lower than that of the general population.5 Presently, apart from focusing on viral suppression and increasing survival rates, there is a greater emphasis on enhancing long-term well-being and overall quality of life for PLWH.8 Social function assumes a significant role in determining the comprehensive quality of life of PLWH.9 Within the context of social function, a crucial element is social support.10 Furthermore, social support is associated with many health outcomes, such as ART adherence,11 viral load suppression,12 and anxiety and depression.13 However, due to widely held misconceptions and stereotypes surrounding HIV, PLWH may encounter social discrimination and stigmatization, leading to a loss of social support and feelings of isolation.14 The impact of HIV infection on PLWH extends beyond physical and psychological aspects, significantly impairing interpersonal relationships, further compromising their social function.15
However, previous studies on the social support and social functions of PLWH have predominantly taken a passive perspective, primarily focusing on providing social support to PLWH without considering their personal willingness or preferences.16–18 It is important to recognize that different individuals have distinct ways of interacting and varying perceptions of interpersonal relationships and social support. These differences can be attributed to individuals’ unique interpersonal personalities, which manifest as their tendencies and preferences in interpersonal communication and serve as apparent expressions of their overall personality.19 Furthermore, considering interpersonal personalities becomes crucial when implementing social support programs like peer-support initiatives, understanding interpersonal personality traits can facilitate precise matching for these programs.20,21 The interpersonal circumplex model (IPC) offers a comprehensive framework that provides a detailed description of interpersonal personality traits and their mathematical relationships.22 Extensive research has amply demonstrated the valuable implications of the IPC model in determining interpersonal personalities.23–25 According to the IPC model, interpersonal octants can be positioned along the circumference of a circle, representing the primary dimensions of dominance and warmth (see Figure 1). In this circular arrangement, closely situated octants correlate more positively than those further apart, octants at right angles are unrelated, and octants positioned opposite each other are negatively related. The octants are given alphabetic names in a counterclockwise direction (eg, PA, BC, DE, etc.) and their specific angular location ranges from 0° to 360°.
 |
Figure 1 The interpersonal circumplex model. |
The assessment of the IPC as a measurement of normal variations in interpersonal personality is varied, such as Interpersonal Adjective Scales (IAS),26 The Inventory of Interpersonal Problems (IIP),27 the International Personality Item Pool-Interpersonal Circumplex (IPIP-IPC),28 Revised Interpersonal Adjective Scales (IAS-R),29 and Interpersonal Problems-Short Circumplex (IIP-SC).30 However, scales like IAS, IIP, and IAS-R can be time-consuming in daily practice owing to their extensive items. Wiggins notes that certain adjectives used in the IAS may be unfamiliar (eg, uncharitable, unsparkling) and many of them are negations.31 Furthermore, the Chinese version of the IAS-R and IIP-SC still requires some improvements in terms of its model fit to the circumplex structure.22,32 IPIP-IPC, on the other hand, is a relatively brief and easy to understand measurement of the IPC.28 Therefore, among the available scales, we chose to employ the IPIP-IPC in this study. IPIP-IPC is a scale developed by Patrick M. Markey in 2009 for the rapid, effective, and comprehensive assessment of individuals’ interpersonal traits.28 It is a 32-item alternative measure of the IPC that researchers and clinicians can use at no cost. Previous studies investigating the psychometric properties of the IPIP-IPC have confirmed that eight octant scales exhibit the expected circular pattern and that it exhibits strong convergent validity with the IAS.28 The IPIP-IPC consists of eight dimensions, which are alphabetically arranged as follows: Assured-Dominant (PA), Arrogant-Calculating (BC), Cold-Hearted (DE), Aloof-Introverted (FG), Unassured-Submissive (HI), Unassuming-Ingenuous (JK), Warm-Agreeable (LM), and Gregarious-Extraverted (NO). Each dimension includes four items, resulting in a total of 32 items, with responses scored on a 5-point scale. The internal consistency coefficients of the eight dimensions range from 0.51 to 0.77, and the test–retest reliability is 0.64. In 2016, researcher Hao translated the IPIP-IPC into Chinese, resulting in the official Chinese version of the questionnaire.33 This version maintained the structure of the original scale with 32 items with two items replaced. The Chinese version of the IPIP-IPC demonstrates good reliability, with internal consistency coefficients ranging from 0.621 to 0.796, indicating moderate internal consistency. The relatively limited number of revised items in the scale may contribute to this result. The test–retest reliabilities of the dimensions range from 0.725 to 0.860, suggesting a certain degree of stability. However, a primary limitation of this study is the lack of demographic diversity among different groups, especially for PLWH. The research solely focused on undergraduate students who are from a selective university and have a narrow age range, which limits the generalizability of the findings. Furthermore, owing to pervasive stigma and discrimination in Confucian-dominated Asian culture, the interpersonal relationships of PLWH are more unstable and complicated compared with university students.34 Given the lack of demographic diversity and specific characteristics of PLWH, it is necessary to further test the psychometric properties of the Chinese version of IPIP-IPC among PLWH in China. Moreover, circumplex structure is another property we need to evaluate, as it serves as both the theoretical and statistical foundation of the IPC model. This spatial nature of the IPC model provides a unique perspective in interpreting interpersonal personalities, which goes beyond the traditional approach of simply summing up items to evaluate outcomes. However, this spatial property has not been assessed in Hao’s study. The structural summary method (SSM) is commonly employed to analyze this property.35,36 Therefore, in addition to testing its psychometric properties, it is crucial to analyze the circumplex structure of the Chinese version of IPIP-IPC among PLWH in China using SSM in this study.
In view of the urgent unmet needs of PLWH and the effectiveness of IPIP-IPC in assessing individual interpersonal traits, it is of profound importance to employ IPIP-IPC on PLWH to better facilitate future research into the interpersonal personalities for PLWH. Our study was based on cross-sectional, multi-center, and large sample data. To the best of our knowledge, this study represented the first attempt to utilize IPIP-IPC in Chinese PLWH and further examined the circumplex structure of interpersonal personalities in this population. Moreover, we adopted SSM to test the criterion validity of this scale, taking into account the spatial relationships between external variables and the eight octants. Given validated tool is a prerequisite for the assessment of interpersonal personalities, our primary objective of this study was to test the psychometric properties of the Chinese version of IPIP-IPC for its ability to measure interpersonal personalities within the PLWH community in China, while also investigating the circumplex structure of the scale in this population. By conducting this study, we can provide more evidence in employing this scale among PLWH in China, which will facilitate future researches about interpersonal personalities in this population.
Methods
Setting and Study Participants
The data were collected from April 2022 to April 2023 in China. Before conducting the survey, the researchers distributed survey materials to the data collectors at each research institution and conducted training sessions through online meetings. The data collectors were clinical nurses at designated hospitals and were given the option to choose either paper-based or electronic questionnaires, depending on the preferences of the research site and participants. Clinical nurses were available to assist participants with any questions they had regarding the questionnaires. For electronic questionnaires, participants were not allowed to submit the questionnaire if there were any missing data. For paper-based questionnaires, the collected data were entered into the database with two-person verification to ensure accuracy. As for electronic questionnaires, the data was directly downloaded from the backend system. All survey participants received a compensation of 20 RMB if they completed the questionnaire. Informed consent was obtained from all participants before the study.
We recruited individuals diagnosed with HIV-1 infection from six designated HIV/AIDS hospitals located in Beijing, Shanghai, Kunming, Nanning, Shenzhen, Baoshan, and Jiaxing. The inclusion criteria for the study participants were as follows: (1) diagnosed with HIV-1 infection; (2) age over 18 years; (3) estimated survival time of more than 1 year; (4) voluntary participation in the study.
The exclusion criteria were as follows: (1) Inability to participate in the study due to severe complications, including various opportunistic infections and HIV-associated neurocognitive disorder (HAND); (2) Current engagement in treatment with a mental health professional or counselor; (3) Concurrent participating in other HIV-related research projects.
According to COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) study design checklist,37 it is recommended that sample sizes should be 7 times number of items and ≥100. Considering the IPIP-IPC questionnaire with 32 items, the Patient Health Questionnaire for Depression and Anxiety (PHQ-4) with 4 items, and the Simplified Coping Style Questionnaire (SCSQ) with 20 items, it was estimated that a minimum of 224 participants needed to be recruited for this study.
Demographic, Social, and Disease-Related Characteristics
A questionnaire was used to collect data on demographic, social, and disease-related characteristics of PLWH. Demographic information includes variables such as age, sex, educational level, ethnicity, and religious beliefs. Social variables include occupation, income, marital status, interests, and living conditions. Disease-related variables cover aspects such as transmission route, time of HIV diagnosis, initiation of ART, CD4 count, viral load, presence of comorbidities, and complications.
Survey Instruments
Interpersonal personalities were measured using the IPIP-IPC.28 This scale incorporates 32 items, with each item corresponding to one of the 8 dimensions outlined in the interpersonal circumplex model. Participants rated each item on a 5-point Likert scale. Higher scores within each dimension indicate a greater tendency to exhibit the associated interpersonal personality. The Chinese version of the IPIP-IPC, translated by Hao, exhibited favorable content validity.
PHQ-4 has been utilized to assess negative emotions among PLWH. This scale consists of two dimensions: depression and anxiety, each comprising two items. Essentially, the PHQ-4 combines the PHQ-2 (Patient Health Questionnaire-2) and GAD-2 (Generalized Anxiety Disorder-2).38 The PHQ-2 and GAD-2 are widely recognized screening tools that effectively assess emotional symptoms and demonstrate good sensitivity and specificity in diagnosing psychological abnormalities.39–41 The scale employs a 4-point Likert scale, where higher scores indicate a greater severity of negative emotions. According to prior research, the Cronbach’s alpha of the PHQ-4 in PLWH in China was 0.86.42 The Cronbach’s alpha of the PHQ-4 in the present study was 0.924.
SCSQ43 was employed to assess the coping styles of PLWH. This questionnaire comprises 20 items, encompassing two dimensions: active coping (12 items) and passive coping (8 items). It utilizes a 4-point Likert scale, where higher scores reflect a more characteristic manifestation of the coping style within the respective dimension. In an earlier study conducted in PLWH in China, the Cronbach’s alphas were 0.91 and 0.73 for active and passive coping, respectively.44 The Cronbach’s alpha of the SCSQ was 0.934 in the present study.
Statistical Analysis Methods
Statistical analysis was performed using SPSS 26.0, Amos 25.0, and R 4.3.0 software. Descriptive statistics, including means and standard deviations (S.D.), were used to summarize continuous variables, while frequency and percentages were used for categorical variables.
Internal Consistency
Cronbach’s alpha and McDonald’s omega coefficients were used to assess the internal consistency of the IPIP-IPC questionnaire across its eight dimensions, two factors, and overall scale. While Cronbach’s alpha is widely employed as an indicator of internal consistency, its application assumes certain conditions such as item normality, equal variances, and equal factor loadings within dimensions. However, in realistic research settings, perfect adherence to all these assumptions may not be achievable. Recent studies have questioned the sole reliance on Cronbach’s alpha as an adequate measure of reliability.45 McDonald’s omega, on the other hand, provides a robust estimate of internal consistency even when these assumptions are relaxed.46 Therefore, to better evaluate the internal consistency of the Chinese version of IPIP-IPC questionnaire among PLWH in China, this study reports both McDonald’s omega and Cronbach’s alpha coefficients. Furthermore, since the two factors of the IPIP-IPC (Agreeableness and Dominance) are partially reflected in each dimension owing to the spatial structure of the scale, we cannot simply sum up items within dimensions for internal consistency for these two domains. Drawing from Wiggins’ calculation method,47 the following formula is used to compute the internal consistency of these factors:


In the equations, Zi represents the standardized score of the ith octant, and θi represents the angle of the ith octant.
Circumplex Property
A Pearson correlation matrix was generated to analyze the eight dimensions of the IPIP-IPC scale. If the data adheres to a circumplex structure, dimensions that are closer in the circumplex structure should exhibit higher correlations compared to dimensions that are farther apart. The highest correlation coefficient is observed between two adjacent dimensions at a 45° angle, and the highest negative correlation coefficient is observed between dimensions at a 135° angle. To be more specific, the correlation between dimensions at a 45° angle (eg, PA and BC, BC and DE) should be higher than those at a 90° angle (eg, PA and DE, DE and FG); the correlation between dimensions at a 90° angle should be higher than those at a 135° angle (eg, PA and FG, BC and HI); and the correlation between dimensions at a 135° angle should be higher than those at a 180° angle (eg, PA and HI, BC and JK). If the circumplex structure depicted in Figure 1 is fully adhered to, a total of 288 correlation relationships need to be satisfied. In this study, the circumplex property was evaluated by calculating the proportion of data that satisfied the 288 relationships of correlation using the correspondence index (CI).48 The CI ranges from 1 to −1, where “1” indicates complete adherence to all 288 relationships, “-1” indicates no adherence to any of the 288 relationships, and “0” indicates an equal number of adhered and non-adhered relationships. The circumplex property was analyzed using a randomization test of hypothesized order relations.48,49 This test evaluated the exact probability of obtaining the observed correlation order in the data matrix under the null hypothesis that the eight-circle scale was randomly relabeled. In a correlation matrix with eight dimensions, there are a total of 40,320 possible random matrices that can be used to create a comparative distribution and assess the fit of the original matrix. The RANDALL program was utilized to perform the circumplex property test.
Confirmatory Factor Analysis (CFA)
Given the well-defined theoretical framework presented by the IPIP-IPC, only CFA was employed to assess its construct validity. Firstly, the structural validity of the dimensions was examined as depicted in Figure 2.
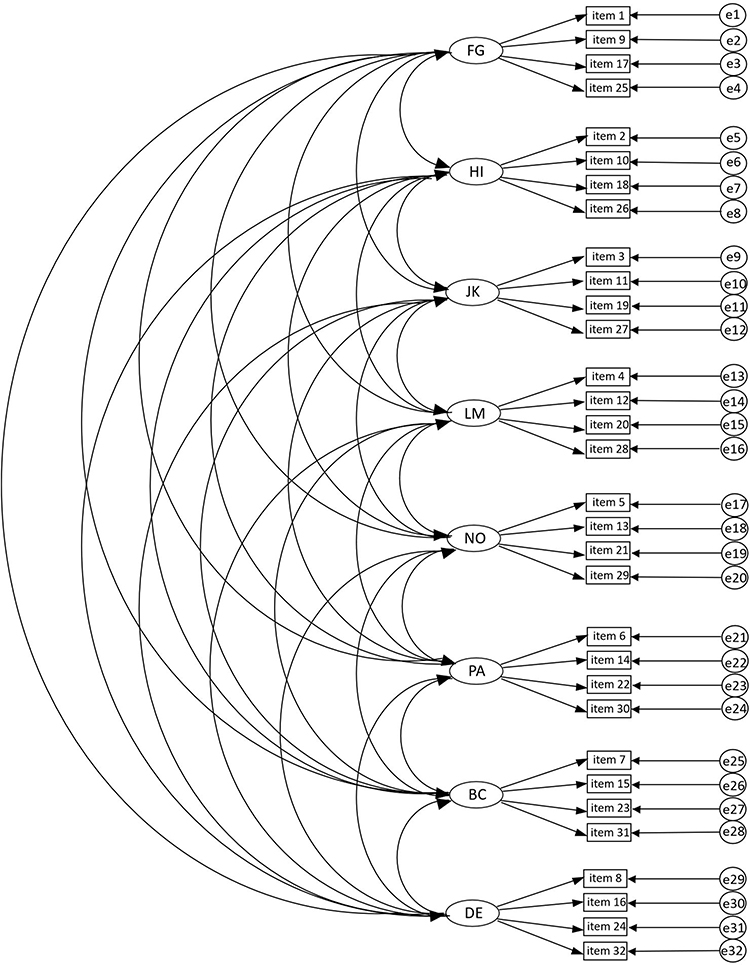 |
Figure 2 CFA model of IPIP-IPC. Abbreviations: PA, Assured-Dominant; BC, Arrogant-Calculating; DE, Cold-Hearted; FG, Aloof-Introverted; HI, Unassured-Submissive; JK, Unassuming-Ingenuous; LM, Warm-Agreeable; NO, Gregarious-Extraverted. |
Subsequently, the two-dimensional angular characteristics of the circumplex structure were incorporated into the CFA analysis based on the quasi-circumplex model proposed by Huang et al,22 as illustrated in Figure 3.
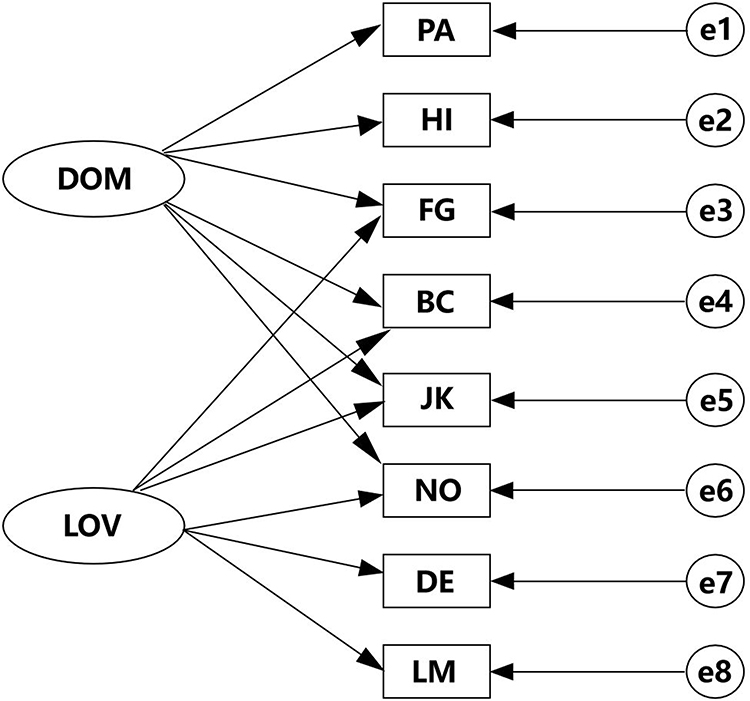 |
Figure 3 CFA model for IPIP-IPC with two-dimensional angular characteristics of the circumplex structure. Abbreviations: DOM, Dominance; LOV, Warmth; PA, Assured-Dominant; BC, Arrogant-Calculating; DE, Cold-Hearted; FG, Aloof-Introverted; HI, Unassured-Submissive; JK, Unassuming-Ingenuous; LM, Warm-Agreeable; NO, Gregarious-Extraverted. |
Both CFA models were considered acceptable if they met the following criteria for model fit:50,51 standardized chi-square (χ2/df) ≤5, goodness-of-fit index (GFI), comparative fit index (CFI), normed fit index (NFI), and Tucker-Lewis index (TLI) all ≥0.90, and the root mean square error of approximation (RMSEA) ≤0.08. Modification indices (MI) greater than 4 were used as indicators to guide model modifications.
Criterion Validity
Prior research consistently indicates a positive link between depression or anxiety and a submissive interpersonal personality.52,53 Additionally, early studies have suggested a positive relationship between higher levels of hostility and the adoption of negative coping strategies.54,55 Therefore, it would be reasonable to examine the correlations between negative emotions and interpersonal personalities, as well as between coping styles and interpersonal personalities to evaluate the criterion validity of the scale. Firstly, Spearman correlations were computed to explore the linear associations between the eight dimensions of the IPIP-IPC scale and negative emotions (anxiety, depression), as well as coping strategies (active coping, passive coping). Subsequently, circumplex correlations were examined using the SSM. Circumplex correlations reflect the spatial relationships between external variables and the eight octants within the circumplex structure. If an external variable represents a prototypical interpersonal personality trait, it is expected to exhibit peak correlations with a particular octant, while its correlations with other octants will progressively decrease as the angular distance from the peak increases. The SSM fits the profile of correlations across circumplex octants to a cosine curve representing a perfect circular structure and quantifies the pattern of correlations in terms of four parameters. The first index is Elevation, in which the average correlation across octants is represented by the distance from the center of the profile to the zero point in the circumplex. The second index is Amplitude, which indicates the differentiation and spread of the variable’s profile within the interpersonal personality, represented by the distance from the center of the profile to the peak. The third index is R2, the coefficient of determination, which represents the degree to which the profile fits the circumplex structure (ie, a cosine curve). A higher R2 indicates a more typical interpersonal personality reflected by the variable (eg, if an external variable reflects agreeableness, it should be primarily associated with LM, followed by NO and JK, with the lowest association with the cold traits). The fourth index is angular displacement, which reflects the peak region of the profile, indicating its primary theme.56 An Elevation and Amplitude greater than 0.15 are considered significantly elevated and differentiated, respectively, while an R2 greater than 0.7 indicates a good fit between the external structure and the circumplex structure.56,57 Angular displacement is only interpretable when both Amplitude and R2 meet the criteria. Furthermore, bootstrap methods will be employed to calculate confidence intervals for the SSM-related indices.58
Before conducting tests on psychometric and circumplex properties, the database was subjected to data cleaning. After calculating the variances of the four items within each dimension and summing up these eight variances, we obtained the total variance of interpersonal personality for each participant and instances with total variances in the top 10% of the distribution were removed. In a study by Locke59 that focused on interpersonal personality, approximately 15% of the data was excluded to minimize the influence of response biases on statistical results.
Result
General Description of Study Participants
In Table 1, a total of 3040 individuals were enrolled in the study across five research centers. The distribution of participants from different locations is as follows: Beijing (517), Shanghai (444), Nanning (505), Shenzhen (469), Kunming (460), Baoshan (604), and Jiaxing (41). The majority of participants were male (78.9%), identified as Han ethnicity (84.3%), and reported no religious beliefs (94.4%). Approximately 58.6% of participants had completed high school education or below. The average age of participants was 40.51 years. Of the participants, 37.3% were married. In terms of occupation, only 32.9% had stable employment, and 36.6% had a monthly income exceeding 5000 yuan. Sexual transmission accounted for the majority (69.0%) of HIV transmissions. The average duration since diagnosis was 77.41 months, with an average ART duration of 71.89 months. The average CD4 lymphocyte count was 492/μL, and 77.2% of participants had an undetectable viral load.
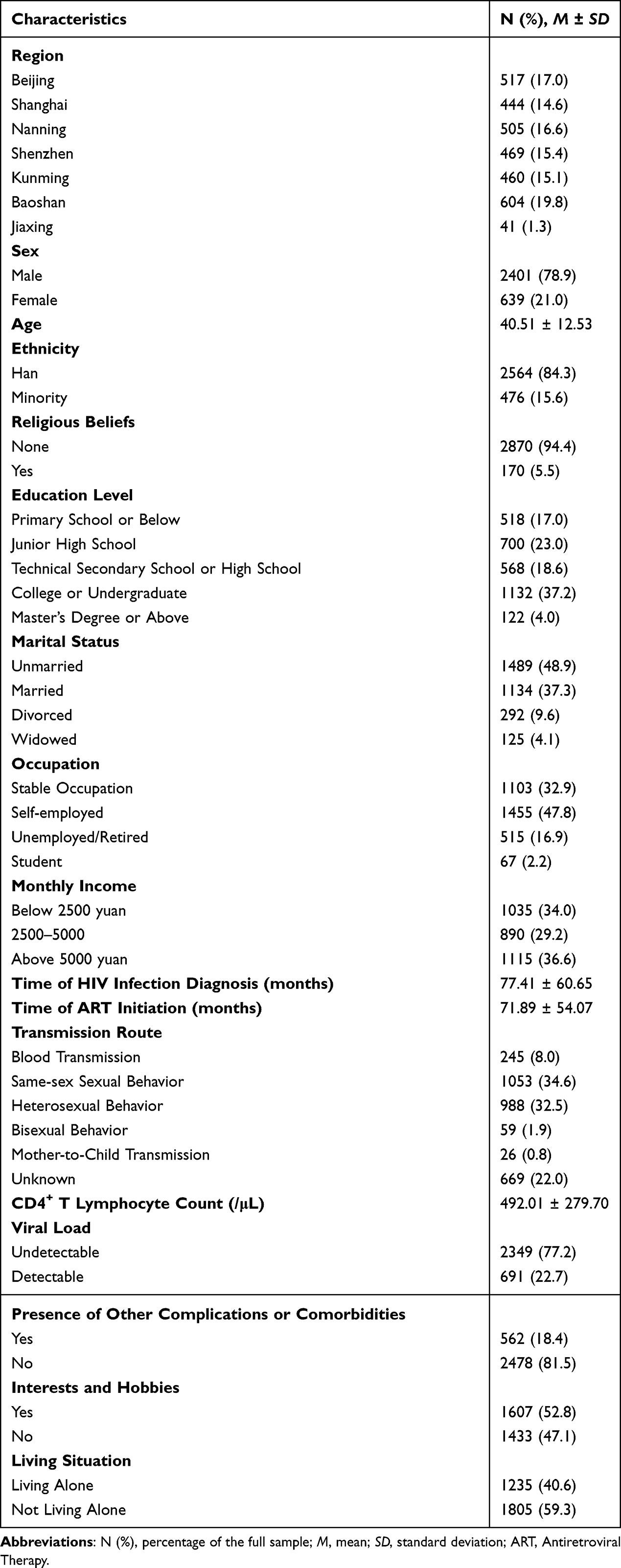 |
Table 1 Participants Characteristics (N = 3040) |
Psychometric Properties and Circumplex Structure
Before examining psychometric properties, the researchers performed data cleaning on the interpersonal personality data. Firstly, one record was removed because of the missing data. Subsequently, the variance within each dimension of interpersonal personality data was calculated, and the distribution of the total variance obtained by summing the variances of the eight dimensions is presented below:
As shown in Table 2, the total variance of interpersonal personality recorded in the database ranges from 0 to 36.00, with a 90% cutoff point at 12.25. Records with a total variance exceeding 12.25 were excluded, resulting in a final sample of 2741 records.
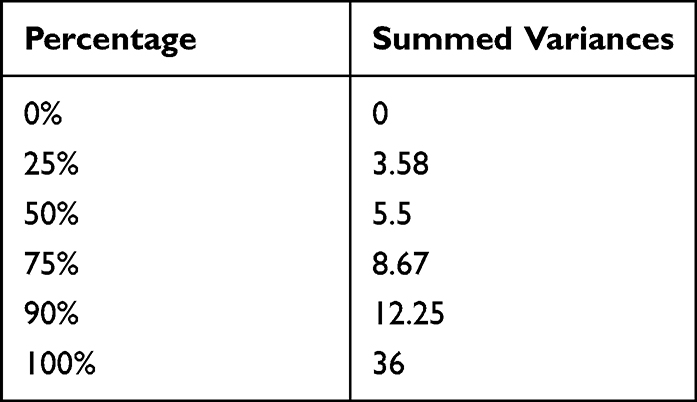 |
Table 2 Distribution of Total Interpersonal Personality Variance |
Internal Consistency
As shown in Table 3, the Cronbach’s alpha values for individual dimensions of interpersonal personality range from 0.53 to 0.81, while McDonald’s omega values range from 0.60 to 0.83. The Cronbach’s alpha for the dominance factor is 0.43 and McDonald’s omega is 0.84. The Cronbach’s alpha for the Warmth factor is 0.72, and McDonald’s omega is 0.89. The total scale demonstrates a Cronbach’s alpha of 0.85 and McDonald’s omega of 0.91.
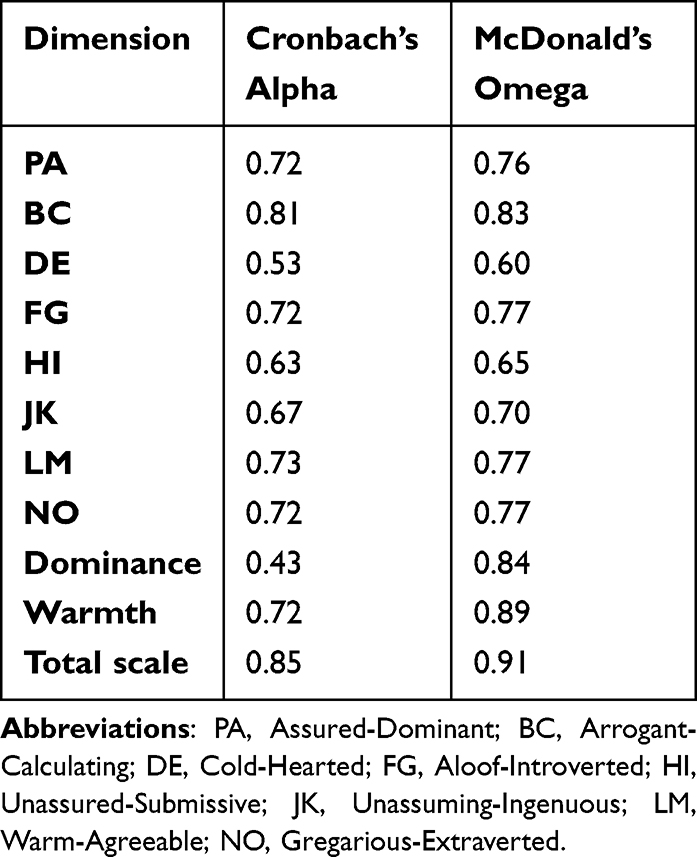 |
Table 3 Internal Consistency Index of the Chinese Version of IPIP-IPC (N = 2741) |
Circumplex Properties
As shown in Table 4 and Figure 4, the correlation matrix of the eight dimensions of interpersonal personalities reveals that the dimension with the largest absolute correlation coefficient is the one that is consistently 45° apart. Furthermore, the results of the circumplex properties test indicate that out of the 288 possible relationships, 275 relationships satisfy the circular properties hypothesis, with a CI of 0.910 (p < 0.01).
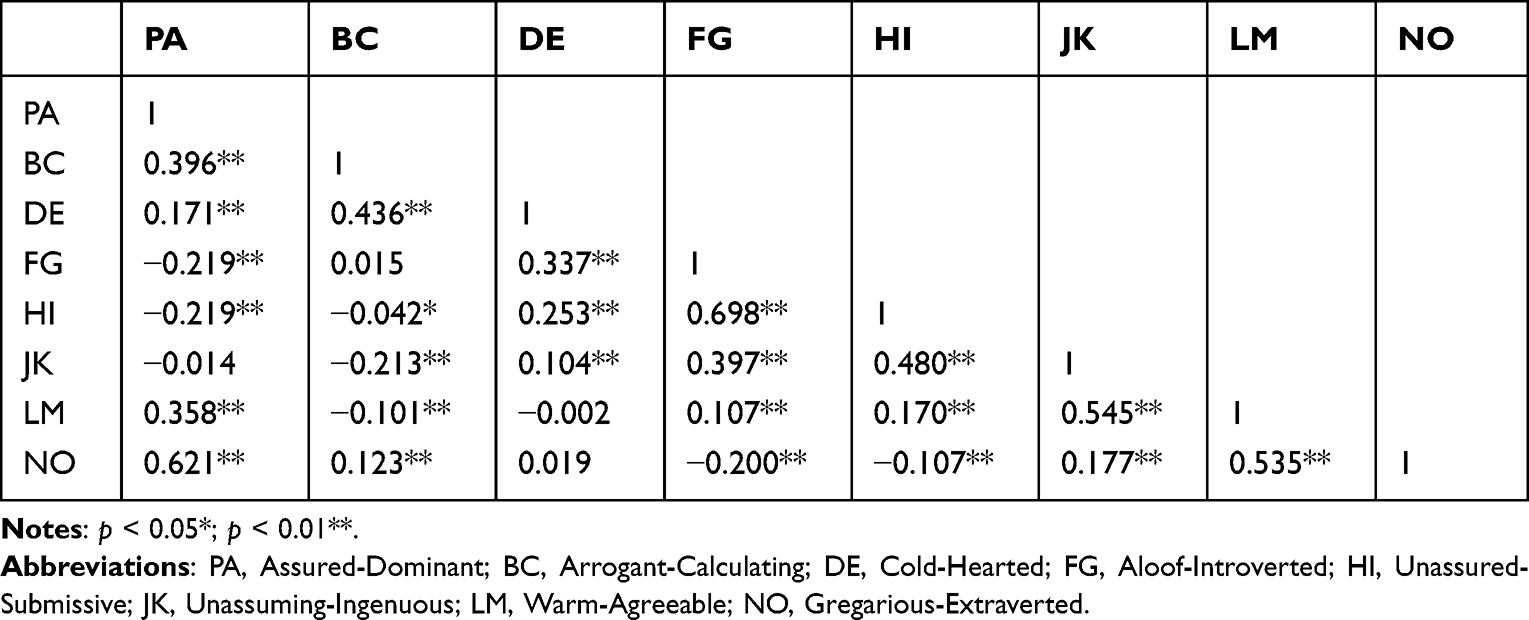 |
Table 4 Spearman Correlation Coefficient Matrix of Interpersonal Personality on Single Dimension (N = 2741) |
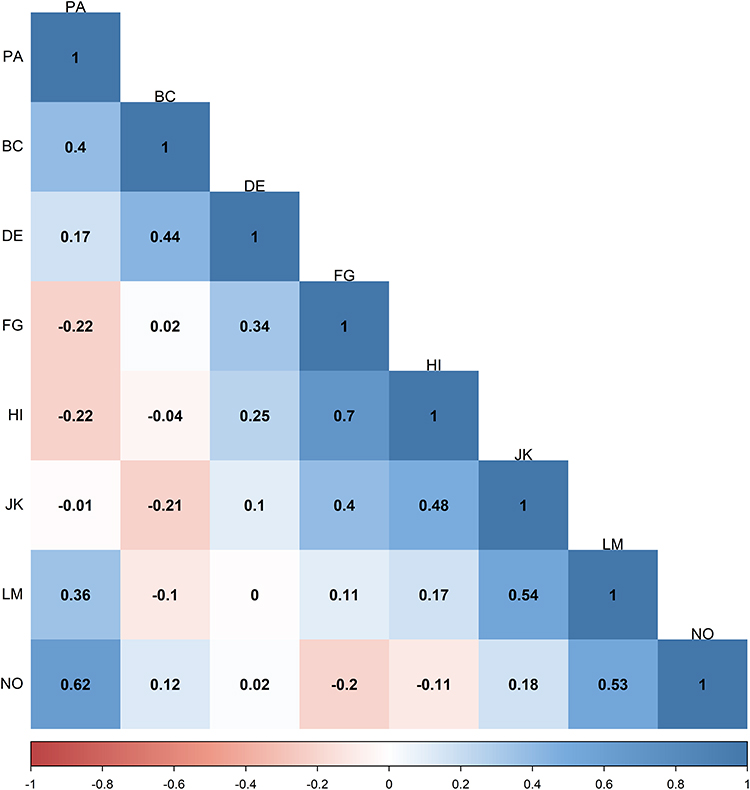 |
Figure 4 Spearman correlation coefficients for interpersonal personality on single dimension (N = 2741). Abbreviations: PA, Assured-Dominant; BC, Arrogant-Calculating; DE, Cold-Hearted; FG, Aloof-Introverted; HI, Unassured-Submissive; JK, Unassuming-Ingenuous; LM, Warm-Agreeable; NO, Gregarious-Extraverted. |
Structural Validity
Figure 5 presents the model diagram of the unstandardized estimated values, which is used to assess the fit between the dimensions of the scale and the actual data and to determine the effectiveness of each item as a measurement indicator for the latent variables. The fit indices of this model are as follows: χ2/df = 4.978, GFI = 0.962, CFI = 0.958, NFI = 0.948, TLI = 0.940, and RMSEA = 0.038.
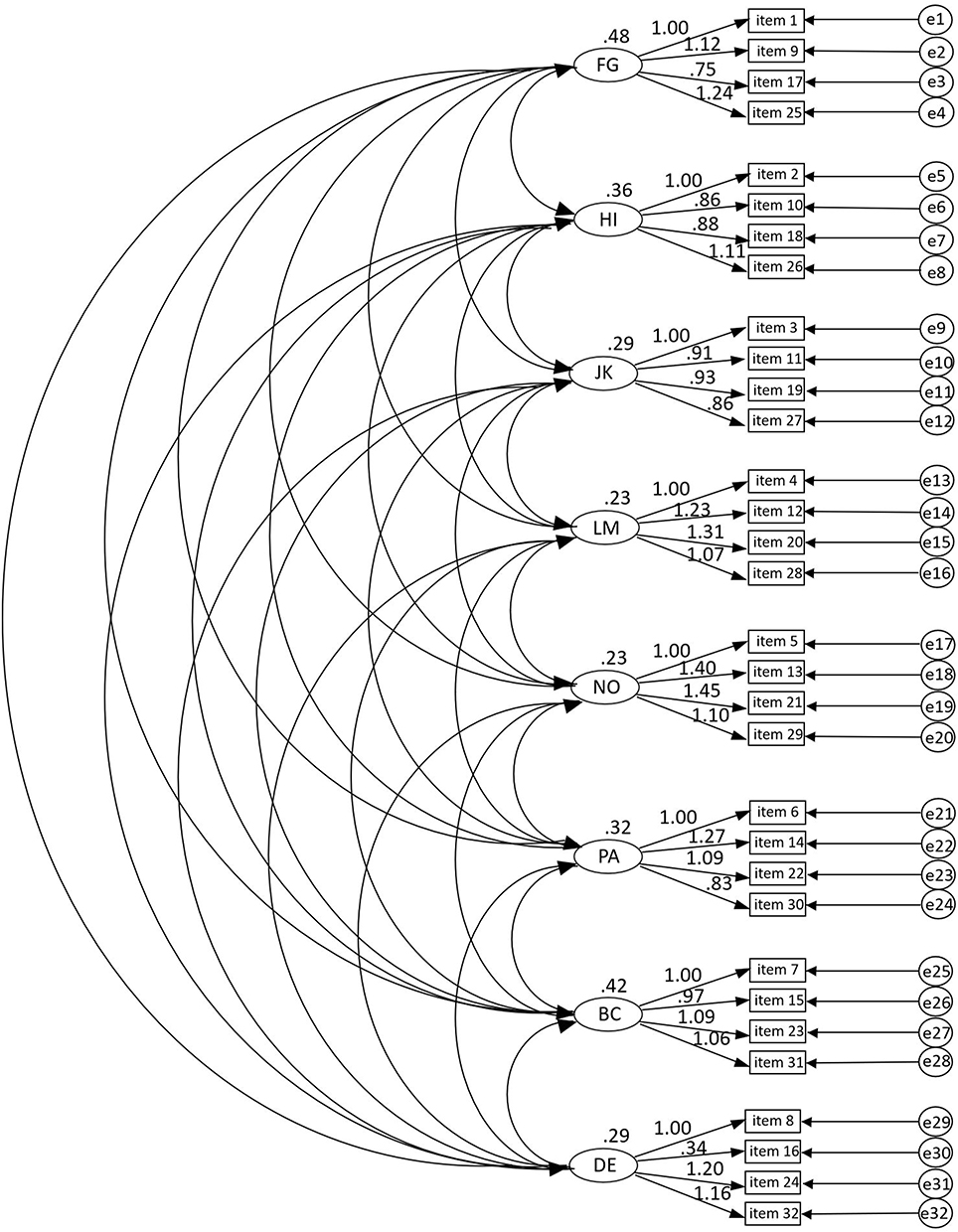 |
Figure 5 CFA model for IPIP-IPC (with unstandardized estimates). Abbreviations: PA, Assured-Dominant; BC, Arrogant-Calculating; DE, Cold-Hearted; FG, Aloof-Introverted; HI, Unassured-Submissive; JK, Unassuming-Ingenuous; LM, Warm-Agreeable; NO, Gregarious-Extraverted. |
Figure 6 displays the model diagram of unstandardized estimated values, which is utilized to examine whether the data factors can reflect the circular properties of the dimensions. The fit indices of this model are as follows: χ2/df = 2.910, GFI = 1.000, CFI = 1.000, NFI = 1.000, TLI = 0.995, and RMSEA = 0.026.
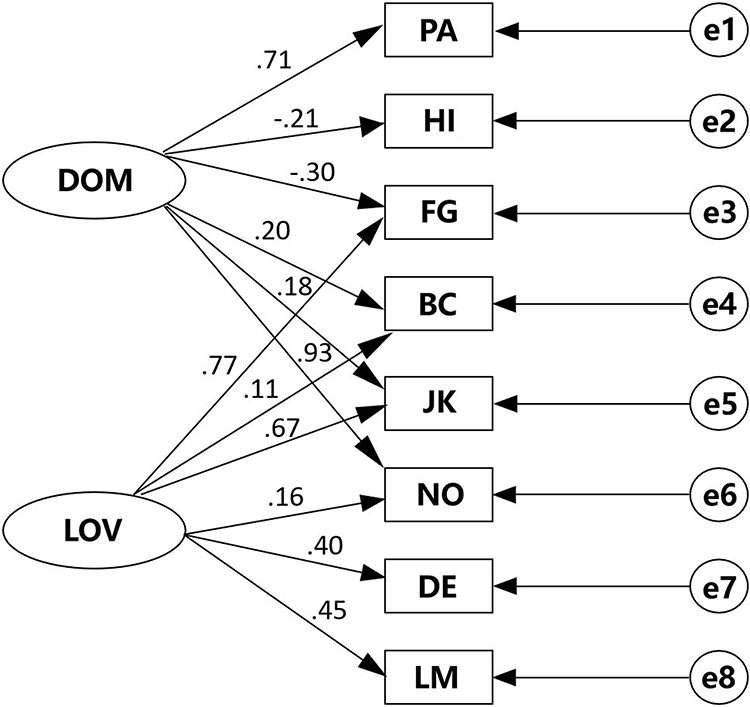 |
Figure 6 CFA model for IPIP-IPC with two-dimensional angular characteristics of the circumplex structure (with unstandardized estimates). Abbreviations: DOM, Dominance; LOV, Warmth; PA, Assured-Dominant; BC, Arrogant-Calculating; DE, Cold-Hearted; FG, Aloof-Introverted; HI, Unassured-Submissive; JK, Unassuming-Ingenuous; LM, Warm-Agreeable; NO, Gregarious-Extraverted. |
Criterion Validity
Spearman Correlation with PHQ-4
Through Spearman correlation analysis, Table 5 demonstrates the correlation between FG, HI, JK, LM, NO, PA, BC, and DE with anxiety, depression, and total scale. The specific results are as follows: PA shows negative correlations with Anxiety, Depression, and Total Scale, with correlation coefficients of −0.046, −0.075, and −0.065, respectively. Conversely, BC does not exhibit significant correlations with Anxiety, Depression, and Total Scale, with p-values greater than 0.05. DE, on the other hand, shows significant positive correlations with Depression and Total Scale, with correlation coefficients of 0.058 and 0.039, respectively. There is no significant correlation between DE and Anxiety, with p-values greater than 0.05. FG shows significant positive correlations with Anxiety, Depression, and Total Scale, with correlation coefficients of 0.115, 0.157, and 0.144, respectively. HI also presents significant positive correlations with Anxiety, Depression, and Total Scale, with correlation coefficients of 0.063, 0.111, and 0.094, respectively. On the other hand, JK and LM do not exhibit significant correlations with Anxiety, Depression, and Total Scale, as the p-values are all greater than 0.05. Finally, NO shows significant negative correlations with Anxiety, Depression, and Total Scale, with correlation coefficients of −0.141, −0.167, and −0.165, respectively.
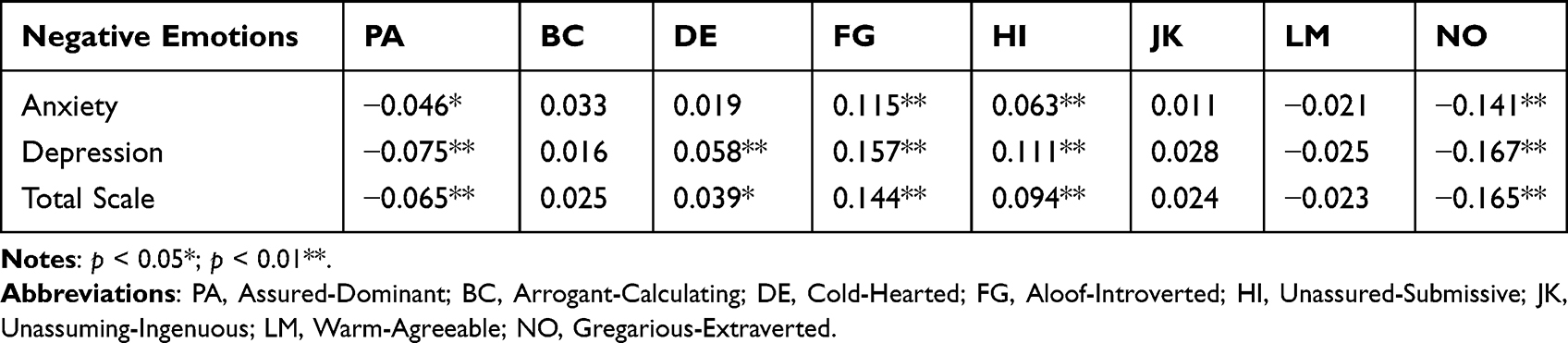 |
Table 5 Spearman Correlation Coefficients Between IPIP-IPC and PHQ-4 |
Spearman Correlation with SCSQ
Through Spearman correlation analysis, Table 6 demonstrates the correlation between FG, HI, JK, LM, NO, PA, BC, and DE with active coping and passive coping. The specific results are as follows: PA, JK, LM, and NO all demonstrate positive correlations with both active coping and passive coping. Secondly, there is a positive correlation between BC and passive coping, while no significant correlation is observed between BC and active coping. DE displays a positive correlation with passive coping, but no significant correlation is found with active coping. DE shows positive correlations with passive coping, with correlation coefficients of 0.026. There is no significant correlation between DE and active coping, with p-values greater than 0.05. FG shows positive correlations with passive coping, but there is no significant correlation between DE and active coping, with p-values greater than 0.05. Similarly, FG shows positive correlations with passive coping, while no significant correlation was found between FG and active coping with p-values greater than 0.05.
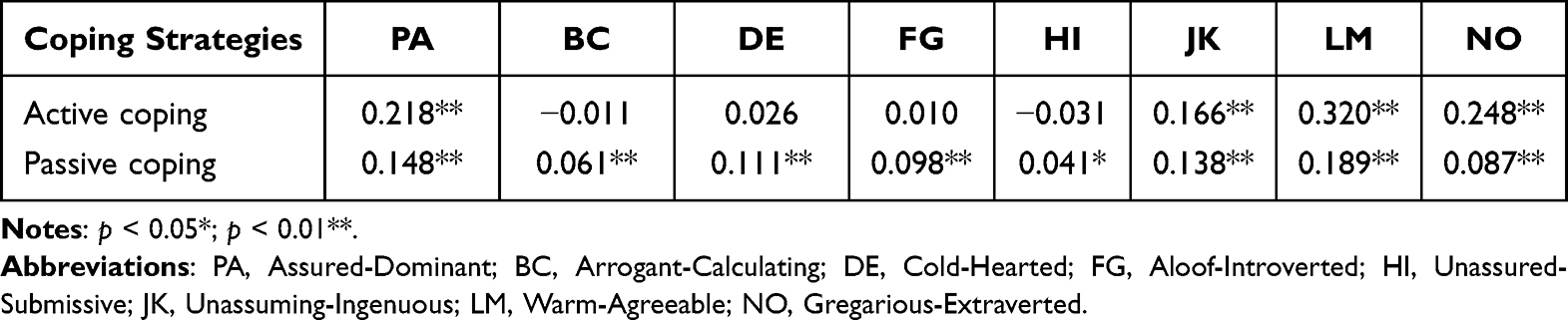 |
Table 6 Spearman Correlation Coefficients Between IPIP-IPC and SCSQ |
Convergence and Divergence with PHQ-4
The circumplex structural summary parameters for PHQ-4 scale are provided in Table 7 and Figure 7. For anxiety, it peaked in the FG octants (218.5, 246.3), with elevations (−0.01, 0.03) but low to negligible amplitudes (−0.01, 0.03). R2 values indicated prototypical profiles. For depression, it peaked at the border of the FG and HI octants (227.9, 247.2), with elevations (−0.00, 0.04) and small to moderate amplitudes (0.11, 0.16). R2 values indicated prototypical profiles. On the whole, anxiety and depression peaked in the FG octants (224.7, 246.4), with elevations (−0.01, 0.04) and small to moderate amplitudes (0.09, 0.15). R2 values indicated prototypical profiles.
 |
Table 7 IPIP–IPC Structural Summary for PHQ-4 Scales |
 |
Figure 7 Amplitude and angular displacement confidence intervals (circumplex plots) for interpersonal personalities profiles of PHQ-4 scales. |
Convergence and Divergence with SCSQ
The circumplex structural summary parameters for SCSQ scale are provided in Table 8 and Figure 8. For active coping, it peaked at the border of the NO and LM octants (11.0, 30.2), with elevations (0.10, 0.15) and small to moderate amplitudes (0.13, 0.18). R2 values indicated prototypical profiles. For passive coping, it has low elevations (0.09, 0.14). R2 values below 0.70 suggested profile complexity, and therefore the amplitude and angular displacement parameters were not interpretable.
 |
Table 8 IPIP–IPC Structural Summary for SCSQ Scales |
 |
Figure 8 Amplitude and angular displacement confidence intervals (circumplex plots) for interpersonal personalities profiles of SCSQ scales. Note: The dotted lines indicate low prototypicality (R2 < 0.70). |
Discussion
This study utilized a large sample size from a multi-center cross-sectional study to test the psychometric properties and circumplex structure of the Chinese version of IPIP-IPC among PLWH in China. Notably, this research represents the first investigation to test the psychometric properties of the Chinese version of the IPIP-IPC on a nationally representative sample of PLWH in China and analyze its circumplex structure. Our study demonstrated that the Chinese version of IPIP-IPC was a reliable tool for assessing interpersonal personalities among PLWH in China. Compared to other scales used for assessing interpersonal personalities, the Chinese IPIP-IPC is a concise instrument consisting of only 32 items, making it practical for researchers to utilize in clinical settings. Our findings not only contribute to the existing body of knowledge but also offer valuable evidence to researchers in selecting appropriate assessment tools for evaluating interpersonal personalities within this specific population. Accurate and reproducible assessment tools are crucial for obtaining robust and reliable results. We anticipate that our study will facilitate further investigations into elucidating the underlying mechanisms linking interpersonal personalities to health-related outcomes, such as medication adherence, social engagement, and disease prognosis.
The results of the study indicate that the Chinese version of the IPIP-IPC scale is a simple, dependable, and consistent tool for assessing interpersonal personalities among PLWH in China. To evaluate the internal consistency, we employed Cronbach’s alpha and McDonald’s omega coefficients. The total scale exhibited a Cronbach’s alpha of 0.85, with individual dimensions ranging from 0.53 to 0.81, and McDonald’s omega of 0.91, with individual dimensions ranging from 0.60 to 0.83. While the Cronbach’s alpha result is not entirely satisfactory, it is important to note that only one dimension falls below the threshold of 0.6. In contrast, in the research conducted by Markey et al, despite conducting four studies, each yielded modest reliability.28 The average composite reliability across these four studies was 0.64 (ranging from 0.51 to 0.75), 0.63 (ranging from 0.50 to 0.77), 0.60 (ranging from 0.46 to 0.70), and 0.64 (ranging from 0.48 to 0.76), respectively. Additionally, the reliability of the Japanese version of the IPIP-IPC scale across its eight dimensions ranged from 0.42 to 0.79, which is even lower than the result of this study.60 This phenomenon may be attributed to Cronbach’s alpha relying on assumptions such as item normality, equal variances, and equal factor loadings within dimensions. These assumptions are idealistic when dealing with a large sample size from a multicenter cross-sectional study, as was the case in this study. Thus, we utilized McDonald’s omega coefficients, which are more flexible with these assumptions, to assess the scale’s internal consistency. For circumplex property, the obtained CI indicates a good fit between the correlation matrix and the circular model with 275 out of 288 order predictions meeting with the current data. These two indicators indicate good consistency and stability of the scale.
The CFAs tested two models to examine two aspects of the IPIP-IPC instrument: (a) the eight factors structure and (b) the circumplex structure of the IPIP-IPC. All the factor loadings were significant and higher than 0.70. These results indicate that the eight dimensions effectively measure the circumplex structure, and provide a solid foundation for further advanced analyses.
For the criterion validity, strong correlations were observed between the Chinese version of IPIP-IPC and PHQ-4 or SCSQ scales. Furthermore, in terms of convergence with the PHQ-4 scales, it was found that individuals with lower dominance scores and slightly negative warmth scores were more likely to experience negative emotions such as depression or anxiety, which aligns with previous research52 where individuals displaying higher levels of submissiveness reported elevated levels of depression or anxiety. In terms of convergence with the SCSQ scales, it was found that individuals who scored high in warmth and positive in dominance tended to adopt active coping styles, which is consistent with previous findings, which indicated that individuals with lower levels of hostility were more prone to using active coping strategies.54 However, the model fit of negative coping was below the threshold, suggesting that PLWH in China were prone to adopt passive coping strategies regardless of their interpersonal personalities. According to studies conducted in Liuzhou, China, PLWH reported experiencing discrimination due to a fear of casual transmission and that even some medical workers treated them badly due to such fear. The social stigma and discrimination may be one possible explanation as to why PLWH adopt negative coping strategies.61,62
In the Chinese version of IPIP-IPC, two items have been modified.33 Specifically, the phrase “Speak softly” has been replaced with “Be considerate and thoughtful towards others”, while “Get along well with others” has been replaced with “Be humble and courteous towards others”. This modification takes into account the nuanced cultural differences in social interactions within Chinese culture, which places emphasis on friendly and peaceful coexistence within groups. Different interpersonal personalities can explain different interpersonal behaviors and predict interpersonal outcomes. This underscores the importance of a person-centered approach in social support interventions. Individuals exhibiting higher levels of hostility may have a dislike for social contact and may also derive less benefit from it.63 Therefore, it might be more conducive and humanistic for social support practitioners to take interpersonal personalities of the recipient into consideration before implementing social support interventions. According to the complementarity theory, individuals are often attracted to those who demonstrate similar levels of affiliation but opposite levels of dominance. Considering this perspective, evaluating interpersonal personalities based on the Chinese version of IPIP-IPC could be essential for partner matching in social support programs in China. Also, studies have shown that interpersonal personalities can be associated with health outcomes,63 parenting styles,64 and the perception of therapy benefit.65 This versatile tool may be promising not only in the field of recovering social function of PLWH but also for many other unexplored domains in China. With the findings from our research, the Chinese version of IPIP-IPC could be employed for assessing interpersonal personalities among PLWH in China with evidence. In clinical settings, health care providers could utilize this scale to assess interpersonal personalities of the PLWH and apply more precise interventions based on the results. Also, this scale can lay the foundations for future researchers to examine the underlying mechanisms between health outcomes and interpersonal personalities. By understanding the distinct interpersonal traits exhibited by PLWH in China and the potential mechanisms underlying them, public health initiatives can be designed to promote effective communication, social support, and overall well-being within this group.
Limitations
However, it is important to acknowledge several limitations in this study. First, convenience sampling was employed in this study, which may affect the representativeness of the sample. In addition, we only test a few indicators in this study, with other indicators untested, such as test–retest reliability. Lastly, although our study was conducted at multiple centers, it is important to note that our sample only included participants from the eastern, southern, and southwestern regions of China. Therefore, the findings may not fully represent the characteristics of PLWH in the entire country, as the epidemiological characteristics of PLWH can vary across different regions in China.66 These limitations present opportunities for future research endeavors aimed at refining our understanding of personality traits in individuals living with HIV. Future studies could conduct further studies to assess other indicators, such as test–retest reliability and include participants from other regions of China to obtain a more comprehensive understanding of the characteristics of PLWH across the country. In addition, it is worth considering the potential impact of China’s one-child policy on the development of interpersonal skills among the Chinese population. Since the policy was lifted in 2015, a transition period may have ensued, which could have implications for interpersonal personalities, particularly among PLWH who may have smaller social circles. It is recommended that future studies explore generational differences in interpersonal personalities within Chinese culture.
Conclusions
This study conducted a comprehensive evaluation of the psychometric and circumplex properties of the Chinese version of the IPIP-IPC scale among PLWH in China. The findings demonstrate that the IPIP-IPC scale is a reliable tool for assessing interpersonal personalities within this population. These results highlight the validity and applicability of the IPIP-IPC scale specifically in the Chinese context, providing valuable insights into the intricacies of interpersonal traits among PLWH. The nuanced understanding of personality traits obtained from this analysis can serve as a crucial resource for healthcare professionals, enabling the development of tailored interventions and support strategies that take into account the diverse interpersonal needs of individuals within this community. Based on our findings, future researchers could choose this scale to assess interpersonal personalities in this population with evidence. Future research could delve deeper into exploring the relationships between specific areas such as psychological resilience, social engagement, and disease prognosis, and interpersonal personalities among PLWH. By conducting further investigations in these areas, we can enhance our understanding of the psychometric properties in this populations, ultimately improving the effectiveness of interventions and support systems for individuals living with HIV.
Data Sharing Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical Approval
This study was conducted according to the World Medical Association Declaration of Helsinki and approved both by the Peking University Biomedical Ethics Committee (IRB00001052-22178) and the Fudan University Biomedical Ethics Committee (IRB#2021-07-09).
Funding
This study was funded by the National Natural Science Foundation of China (72204006), and the China Postdoctoral Science Foundation (2022M710258).
Disclosure
Xiaomeng Wang, Shuyu Han and Changli Jia are co-first authors for this study. The authors declare no actual or potential competing interests that relate to this article that could be construed as a conflict of interest.
References
1. Teeraananchai S, Kerr SJ, Amin J, Ruxrungtham K, Law MG. Life expectancy of HIV -positive people after starting combination antiretroviral therapy: a meta-analysis. HIV Med. 2017;18(4):256–266. doi:10.1111/hiv.12421
2. Data on the HIV response. Available from: https://www.who.int/data/gho/data/themes/hiv-aids/data-on-The-hiv-aids-response.
3. Zhao Y, Wei L, Dou Z, et al. Changing mortality and patterns of death causes in HIV infected patients — China, 2013–2022. China CDC Wkly. 2023;5(48):1073–1078. doi:10.46234/ccdcw2023.201
4. Johnson LF, Mossong J, Dorrington RE, et al. Life expectancies of South African adults starting antiretroviral treatment: collaborative analysis of cohort studies. PLoS Med. 2013;10(4):e1001418. doi:10.1371/journal.pmed.1001418
5. Trickey A, Sabin CA, Burkholder G, et al. Life expectancy after 2015 of adults with HIV on long-term antiretroviral therapy in Europe and North America: a collaborative analysis of cohort studies. Lancet HIV. 2023;10(5):e295–e307. doi:10.1016/S2352-3018(23)00028-0
6. Bhatta DN, Adhikari R, Karki S, Koirala AK, Wasti SP. Life expectancy and disparities in survival among HIV-infected people receiving antiretroviral therapy: an observational cohort study in Kathmandu, Nepal. BMJ Glob Health. 2019;4(3):e001319. doi:10.1136/bmjgh-2018-001319
7. Coelho LE, Luz PM. Life-expectancy with HIV in Latin America and the Caribbean. Lancet HIV. 2021;8(5):e247–e248. doi:10.1016/S2352-3018(21)00050-3
8. Lazarus JV, Safreed-Harmon K, Barton SE, et al. Beyond viral suppression of HIV - The new quality of life frontier. BMC Med. 2016;14(1):94. doi:10.1186/s12916-016-0640-4
9. Aaronson NK. Quality of life: what is it? How should it be measured? Oncology. 1988;2(5):69–76, 64.
10. Kotwal A, Kim J, Waite L, Dale W. Social function and cognitive status: results from a US nationally representative survey of older adults. J Gen Intern Med. 2016;31. doi:10.1007/s11606-016-3696-0
11. Nutor JJ, Gyamerah AO, Alhassan RK, et al. Influence of depression and interpersonal support on adherence to antiretroviral therapy among people living with HIV. AIDS Res Ther. 2023;20:42. doi:10.1186/s12981-023-00538-8
12. Nakandi RM, Kiconco P, Musiimenta A, et al. Understanding patterns of family support and its role on viral load suppression among youth living with HIV aged 15 to 24 years in southwestern Uganda. Health Sci Rep. 2022;5(1):e467. doi:10.1002/hsr2.467
13. Weldesenbet A, Kebede S, Tusa B. The effect of poor social support on depression among HIV/AIDS patients in Ethiopia: a systematic review and meta-analysis. Depress Res Treat. 2020;2020. doi:10.1155/2020/6633686
14. Garrido-Hernansaiz H, Alonso-Tapia J. Social support in newly diagnosed people living with HIV: expectations and satisfaction along time, predictors, and mental health correlates. J Assoc Nurses AIDS Care JANAC. 2017;28(6):849–861. doi:10.1016/j.jana.2017.06.007
15. Cardona-Arias JA, Higuita-Gutiérrez LF. IMPACTO DEL VIH/SIDA SOBRE LA CALIDAD DE VIDA: METAANÁLISIS 2002-2012 [Impact of HIV/AIDS on quality of life: meta-analysis 2002–2012]. Rev Esp Salud Publica. 2014;88(1):87–101. Spanish. doi:10.4321/S1135-57272014000100006
16. Campbell JI, Musiimenta A, Natukunda S, Eyal N, Haberer JE. “The research assistants kept coming to follow me up; I counted myself as a lucky person”: social support arising from a longitudinal HIV cohort study in Uganda. PLoS One. 2022;17(1):e0262989. doi:10.1371/journal.pone.0262989
17. Saleh A, Perumal N, Muhihi A, et al. Associations between social support and symptoms of antenatal depression with infant growth and development among mothers living with HIV in Tanzania. AIDS Behav. 2023. doi:10.1007/s10461-023-04073-5
18. Yang Y, Liang S, Fan S, et al. Experiences of visiting female sex workers, social interaction, support and HIV infection among elderly men from rural China. BMC Infect Dis. 2023;23(1):356. doi:10.1186/s12879-023-08178-z
19. Carson RC. Interaction Concepts of Personality. Routledge; 2019; doi:10.4324/9780429025136
20. Han S, Zhang Y, Yang X, et al. The effectiveness and sustainability of peer support interventions for persons living with HIV: a realist synthesis. BMJ Glob Health. 2023;8(2):e010966. doi:10.1136/bmjgh-2022-010966
21. Smith R, Drennan V, Mackenzie A, Greenwood N. Volunteer peer support and befriending for carers of people living with dementia: an exploration of volunteers’ experiences. Health Soc Care Community. 2018;26(2):158–166. doi:10.1111/hsc.12477
22. Huang F, Li YH, Zhang JX, Zhu HL. Circumplex model: an approach to integrate personality research. Adv Psychol Sci. 2010;18(01):132.
23. Gurtman MB. Construct validity of interpersonal personality measures: the interpersonal circumplex as a nomological net. J Pers Soc Psychol. 1992;63:105–118. doi:10.1037/0022-3514.63.1.105
24. Ojanen T, Grönroos M, Salmivalli C. An interpersonal circumplex model of children’s social goals: links with peer-reported behavior and sociometric status. Dev Psychol. 2005;41(5):699–710. doi:10.1037/0012-1649.41.5.699
25. Stone LE, Segal DL. Social impairment and personality disorder features among older adults: an application of the circumplex model. Personal Ment Health. 2022;16(1):19–29. doi:10.1002/pmh.1523
26. Wiggins JS. A psychological taxonomy of trait-descriptive terms: the interpersonal domain. J Pers Soc Psychol. 1979;37:395–412. doi:10.1037/0022-3514.37.3.395
27. Horowitz LM, Rosenberg SE, Baer BA, Ureño G, Villaseñor VS. Inventory of interpersonal problems: psychometric properties and clinical applications. J Consult Clin Psychol. 1988;56(6):885–892. doi:10.1037/0022-006X.56.6.885
28. Markey PM, Markey CN. A brief assessment of the interpersonal circumplex: the IPIP-IPC. Assessment. 2009;16(4):352–361. doi:10.1177/1073191109340382
29. Wiggins JS, Trapnell P, Phillips N. Psychometric and geometric characteristics of the Revised Interpersonal Adjective Scales (IAS-R). Multivar Behav Res. 1988;23(4):517–530. doi:10.1207/s15327906mbr2304_8
30. Soldz S, Budman S, Demby A, Merry J. A short form of the inventory of Interpersonal Problems Circumplex Scales. Assessment. 1995;2(1):53–63. doi:10.1177/1073191195002001006
31. Wiggins JS, Behrends RS, Ben-Porath YS, et al. Paradigms of Personality Assessment. Guilford Press; 2003:xii, 386.
32. Qian S, Jin Y. Validation of the circumplex structure of the inventory of interpersonal problems-short circumplex in Chinese College Students. Chin J Appl Psychol. 2022;29(6):538.
33. Hao Y. The Revision of Interpersonal Circumplex Inventory (IPIP-IPC) [Master]. Yangzhou University; 2016. Available from: https://kns.cnki.net/KCMS/detail/detail.aspx?dbcode=CMFD&dbname=CMFD201701&filename=1016288714.nh&v=.
34. Ho LP, Goh ECL. How HIV patients construct liveable identities in a shame based culture: the case of Singapore. Int J Qual Stud Health Well Being. 2017;12(1):1333899. doi:10.1080/17482631.2017.1333899
35. Gurtman MB. The circumplex as a tool for studying normal and abnormal personality: a methodological primer. In: Differentiating Normal and Abnormal Personality. Springer Publishing Company; 1994:243–263.
36. Wu LZ, Asan AE, Halberstadt AL, Pincus AL. Comparing English-language and Chinese-language assessment of DSM-5 personality disorders and interpersonal problems in Chinese bilingual speakers. J Pers Assess. 2022;104(4):509–521. doi:10.1080/00223891.2021.1960359
37. Mokkink LB, Prinsen CA, Patrick DL, et al. COSMIN study design checklist for patient-reported outcome measurement instruments; 2019.
38. Kroenke K, Spitzer RL, Williams JBW, Löwe B. An ultra-brief screening scale for anxiety and depression: the PHQ-4. Psychosomatics. 2009;50(6):613–621. doi:10.1176/appi.psy.50.6.613
39. Byrd-Bredbenner C, Eck K, Quick V. GAD-7, GAD-2, and GAD-mini: psychometric properties and norms of university students in the United States. Gen Hosp Psychiatry. 2021;69:61–66. doi:10.1016/j.genhosppsych.2021.01.002
40. Maroufizadeh S, Omani-Samani R, Almasi-Hashiani A, Amini P, Sepidarkish M. The reliability and validity of the Patient Health Questionnaire-9 (PHQ-9) and PHQ-2 in patients with infertility. Reprod Health. 2019;16(1):137. doi:10.1186/s12978-019-0802-x
41. Scoppetta O, Cassiani-Miranda CA, Arocha-Díaz KN, Cabanzo-Arenas DF, Campo-Arias A. Validity of the patient health questionnaire-2 (PHQ-2) for the detection of depression in primary care in Colombia. J Affect Disord. 2021;278:576–582. doi:10.1016/j.jad.2020.09.096
42. Tam CC, Sun S, Yang X, Li X, Zhou Y, Shen Z. Psychological distress among HIV healthcare providers during the COVID-19 pandemic in China: mediating roles of institutional support and resilience. AIDS Behav. 2021;25(1):9–17. doi:10.1007/s10461-020-03068-w
43. Xie Y. Reliability and validity of the simplified Coping Style Questionnaire. Chin J Clin Psychol. 1998;6:114–115.
44. Xiao X, Chen C, Gao C, Wang H, Reynolds NR. Ways of coping mediate the relationship between self-efficacy for managing HIV and acceptance of illness among people living with HIV. J Adv Nurs. 2020;76(11):2945–2954. doi:10.1111/jan.14488
45. Agbo AACA. Review of limitations and associated recommendations. J Psychol Afr. 2010;20:233–240.
46. Stensen K, Lydersen S. Internal consistency: from alpha to omega? Tidsskr Den Nor Laegeforening Tidsskr Prakt Med Ny Raekke. 2022;142(12). doi:10.4045/tidsskr.22.0112
47. Wiggins JS. Interpersonal Adjectives Scales Professional Manual. Psychological Assessment Resources; 1997.
48. Rounds J, Tracey TJ, Hubert L. Methods for evaluating vocational interest structural hypotheses. J Vocat Behav. 1992;40(2):239–259. doi:10.1016/0001-8791(92)90073-9
49. Tracey TJG. RANDALL: a Microsoft FORTRAN program for a randomization test of hypothesized order relations. Educ Psychol Meas. 1997;57:164–168. doi:10.1177/0013164497057001012
50. Tze HL, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model. 1999;6:1–55. doi:10.1080/10705519909540118
51. Hubert L, Arabie P. Evaluating order hypotheses within proximity matrices. Psychol Bull. 1987;102:172–178. doi:10.1037/0033-2909.102.1.172
52. Bird T, Tarsia M, Schwannauer M. Interpersonal styles in major and chronic depression: a systematic review and meta-analysis. J Affect Disord. 2018;239:93–101. doi:10.1016/j.jad.2018.05.057
53. Frandsen FW, Simonsen S, Poulsen S, Sørensen P, Lau ME. Social anxiety disorder and avoidant personality disorder from an interpersonal perspective. Psychol Psychother Theory Res Pract. 2020;93(1):88–104. doi:10.1111/papt.12214
54. McCormick RA, Smith M. Aggression and hostility in substance abusers: the relationship to abuse patterns, coping style, and relapse triggers. Addict Behav. 1995;20(5):555–562. doi:10.1016/0306-4603(95)00015-5
55. Piferi RL, Lawler KA. Hostility and the cardiovascular reactivity of women during interpersonal confrontation. Women Health. 2000;30(3):111–129. doi:10.1300/J013v30n03_08
56. Wright AGC, Pincus AL, Hopwood CJ, Thomas KM, Markon KE, Krueger RF. An Interpersonal Analysis of Pathological Personality Traits in DSM-5. Assessment. 2012;19(3):263–275. doi:10.1177/1073191112446657
57. Hopwood CJ, Ansell EB, Pincus AL, Wright AGC, Lukowitsky MR, Roche MJ. The circumplex structure of interpersonal sensitivities. J Pers. 2011;79:707–740. doi:10.1111/j.1467-6494.2011.00696.x
58. Zimmermann J, Wright AGC. Beyond description in interpersonal construct validation: methodological advances in the circumplex structural summary approach. Assessment. 2017;24(1):3–23. doi:10.1177/1073191115621795
59. Locke KD. Development and validation of a circumplex measure of the interpersonal culture in work teams and organizations. Front Psychol. 2019;10:850. doi:10.3389/fpsyg.2019.00850
60. Hashimoto Y, Oshio A. 対人円環モデルに基づいた IPIP-IPC-J の作成 [Development of a Japanese version of the International Personality Item Pool-Interpersonal Circumplex]. Shinrigaku Kenkyu. 2016;87(4):395–404. Japanese. doi:10.4992/jjpsy.87.15215
61. Hua J, Emrick CB, Golin CE, et al. HIV and stigma in Liuzhou, China. AIDS Behav. 2014;18(2):S203–S211. doi:10.1007/s10461-013-0637-3
62. Zhang YX, Golin CE, Bu J, Emrick CB, Nan Z, Li MQ. Coping strategies for HIV-related stigma in Liuzhou, China. AIDS Behav. 2014;18(2):S212–S220. doi:10.1007/s10461-013-0662-2
63. Wiebe DJ, Song A, Ramirez Loyola MD. Chapter 12 - what mechanisms explain the links between personality and health?*. In: Johansen C, editor. Personality and Disease. Academic Press; 2018:223–245. doi:10.1016/B978-0-12-805300-3.00012-8
64. Blanch A, Aluja A. Personality and job stress: a comparison of direct effects on parenting. Span J Psychol. 2011;14(2):667–674. doi:10.5209/rev_sjop.2011.v14.n2.15
65. Hadziahmetović N, Alispahić S, Tuce Đ, Hasanbegović-Anić E. Therapist’s interpersonal style and therapy benefit as the determinants of personality self-reports in clients. Vojnosanit Pregl. 2016;73(2):135–145. doi:10.2298/vsp140911141h
66. Qiao YC, Xu Y, Jiang DX, et al. Epidemiological analyses of regional and age differences of HIV/AIDS prevalence in China, 2004–2016. Int J Infect Dis. 2019;81:215–220. doi:10.1016/j.ijid.2019.02.016
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Validation of the Connor-Davidson Resilience Scale-10 in South Africa: Item Response Theory and Classical Test Theory
Pretorius TB, Padmanabhanunni A
Psychology Research and Behavior Management 2022, 15:1235-1245
Published Date: 16 May 2022
Validity and Reliability of the Thai Version of the 19-Item Compliance-Questionnaire-Rheumatology
Panichaporn S, Chanapai W, Srisomnuek A, Thaweeratthakul P, Katchamart W
Patient Preference and Adherence 2022, 16:2149-2158
Published Date: 17 August 2022
Psychometric Properties of the Montreal Cognitive Assessment (MoCA) to Detect Major Neurocognitive Disorder Among Older People in Ethiopia: A Validation Study
Daniel B, Agenagnew L, Workicho A, Abera M
Neuropsychiatric Disease and Treatment 2022, 18:1789-1798
Published Date: 22 August 2022
Development and Initial Validity of the Patients’ Literacy Scale Among Outpatients in Hangzhou City, China
Jiang D, Sang T, Xiao X, Wu Z, Wang H, Yang Q
Patient Preference and Adherence 2022, 16:2483-2496
Published Date: 7 September 2022
Research and Evaluation of a Cyberchondria Severity Scale in a Chinese Context
Wang D, Sun L, Shao Y, Zhang X, Maguire P, Hu Y
Psychology Research and Behavior Management 2023, 16:4417-4429
Published Date: 1 November 2023