")
Back to Journals » Advances in Medical Education and Practice » Volume 13
Psychological Status of College Students During COVID-19 Pandemic: A Cross-Sectional Study in Saudi Arabia
Authors Alanazi M
Received 11 July 2022
Accepted for publication 23 November 2022
Published 2 December 2022 Volume 2022:13 Pages 1443—1451
DOI https://doi.org/10.2147/AMEP.S381916
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Mona Alanazi1– 3
1College of Nursing, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 2King Abdullah International Medical Research Center, Riyadh, Saudi Arabia; 3Ministry of the National Guard – Health Affairs, Riyadh, Saudi Arabia
Correspondence: Mona Alanazi, Kingdom of Saudi Arabia 765, Unit 153, Riyadh, 4575-14813, Saudi Arabia, Tel +966 568100755, Email [email protected]
Purpose: This study aimed to assess the prevalence and associated factors of depression, anxiety, and stress among college students in Saudi Arabia during the COVID-19 outbreak.
Methods: This cross-sectional study was conducted between February 10th to April 10th, 2021. An online self-administered questionnaire was emailed to college students at a large institution in Saudi Arabia. The questionnaire consisted of sociodemographic, educational backgrounds, and the Depression Anxiety Stress Scale-21 (DASS-21).
Results: The study included 311 university students (62.7% female and 39.3% male). The prevalence of higher than moderate level in each of the depression, anxiety, and stress were (n= 164, 52.7%), (n= 222, 71.4%), and (n= 112, 36%), respectively. Further analysis revealed that females, younger age, history of depression, history of being quarantined by a health authority, and having contact with a confirmed case of COVID-19 were associated with a greater level of depression, anxiety, and stress.
Conclusion: Depression, anxiety, and stress were highly prevalent among college students during the outbreak. There was a significant association between demographic characteristics and the DASS 21 score. Researchers are recommended to concentrate their future studies on establishing strategies to enhance students’ flexibility and adaptability in the face of future catastrophes.
Keywords: COVID-19, DASS-21, psychological effect, depression, anxiety, stress, students
Introduction
The COVID-19 pandemic increased not only the risk of physical harm from the virus but also caused undesirable mental effects on the population. Several studies were conducted to report the psychological impact of this epidemic on the general population, healthcare providers, and patients.1–4 To stop the disease from spreading, China and all other countries followed the strategy of lockdowns, either nationwide or in specific areas which are at risk. Educational institutions, financial institutions, economic activity centers, and recreation centers have closed indefinitely. As of April 2020, more than 300 million students were affected by COVID-19 globally.5 Consequently, many schools and colleges have decided to close or resort to distance learning worldwide. Celebrations and public gatherings were prohibited. Patients with severe infections were treated in hospitals, while those with less severe conditions were placed in quarantine centers. These measures successfully limited the spread of the COVID-19 disease, and they were like those that were successful during the H1N1 pandemic and the SARS outbreak.6
However, aside from the risk of infection and physical complications, the pandemic places enormous psychological strain on the population worldwide. Several research has examined the epidemics’ short- and long-term consequences on the population’s social and psychological health. Even after they have recovered, those who have tested positive for COVID-19 were stigmatized, discriminated, and isolated in their community.7 Long quarantine duration, fears of infection, frustration, restricted supplies, poor communication, financial loss, and discrimination were among the psychological stressors experienced by those quarantined.8
Furthermore, anxiety among college students is already a public health issue. Many previous studies have examined students’ anxiety, depression, stress, and factors that may affect students’ mental health globally. In a systematic review study concerning the mental disorders of the students during COVID-19 in Bangladesh, mild to severe symptoms of depression, anxiety, and stress were highly prevalent among the studied cohort.9 Furthermore, systematic review and meta-analysis results revealed that COVID-19 poses mental health risks to young people and college students.10,11 According to Li et al, depression and anxiety significantly increased during the COVID-19 pandemic among college students.
Looking at students in Saudi Arabia, Amr et al found that 20% of college-level Saudi students are anxious.12 Al-Gelban (2009) claimed that 14.3% of secondary school students have anxiety.13 In contrast, Al-Gelban (2007) found significantly higher anxiety levels (48.9% and 66.2%, respectively) among high school students.14 In another study, Alenazi found that the prevalence of depression, anxiety, and stress among 375 respondents was 56.3%, 56%, and 41.9%, respectively.15
Given the widespread of COVID-19 and the transfer to virtual education are extraordinary and new experiences in Saudi Arabia; therefore, significant psychological challenges among the students are anticipated. The distress of having the virus or transmit it to loved ones, combined with the need to adjust to the new education and assessment strategies, would have enormous stress on the students. In addition to the new strategies of teaching, educational institutions must assess the students’ psychological well-being to take appropriate measures to assist students in coping with unprecedented changes.16 Therefore, it is imperative to examine the impacts of COVID-19 pandemic on the mental health of the general population and specifically on high-risk groups, including students who are at a greater risk for psychological disorders compared to others.17 Hence, this study examined the prevalence and associated factors of depression, anxiety, and stress among college students in Saudi Arabia during the COVID-19 pandemic.
Materials and Methods
Research Design, Setting, and Sample
Design
A cross-sectional design with qualitative methods was used in this study.18
Setting
This study was conducted at one of the largest governmental universities in Saudi Arabia. This university is specialized in health sciences and has 14 colleges on three university campuses in three different regions: Riyadh, Jeddah, and Al-Ahsa. The total number of students who are enrolled in this university as of 2021 is approximately 14,000.
Sample
G power software was used to calculate the minimum sample size to produce statistical power of 80%. Based on the criteria of a confidence level of 95%, a margin error of 5%, using a population size of approximately 14,000 university students, and the expected frequency of depression, anxiety, and stress as primary outcomes at 50%, the required sample size is 134 college students. However, the sample size was doubled to 300 college students to be a more representative sample. Students were recruited by a convenience sampling strategy, where the invitations to participate were sent to all students through their university’s emails.
Data Collection Procedure and Timeline of the Survey
Data were collected through e-link using Google forms between February 10th to April 10th, 2021. The author chose to address this date, while the COVID-19 concern is at its peak rather than waiting until the end of summer. By email, the students were invited to participate in the study, informed on the aims of the study, and assured anonymity and confidentiality of their participation. Those who agreed to participate have electronically consented. Our procedures were comparable to those obtained using the standard data collection techniques. This method also promotes self-disclosure among research participants, which is especially important for sensitive topics like depression, anxiety, and stress.19
Research Instruments and Measurements
This study’s instrument included a structured self-reported questionnaire that covered different areas: (1) sociodemographic data, (2) medical history, (3) COVID-19 contact history, and (4) mental health status, including depression, anxiety, and stress.
Sociodemographic variables comprised gender, age, marital status, college and region, year of education, residence, living with parents, and household income. The medical history included personal and family history, such as a history of chronic medical conditions, hospitalization, quarantine by a health authority, COVID-19 testing, and diagnoses of COVID-19 status. Contact history with COVID-19 variables included questions about any direct and indirect communication history with a suspected and positive case of COVID-19.
The mental health status (depression, anxiety, and stress) was assessed using the short version of Lovibond and Lovibond’s (1995) 42-item scale, which is the Depression, Anxiety, and Stress Scales-21 (DASS-21).20,21 DASS-21 was used to measure the negative emotional states of depression, anxiety, and stress. The DASS-21 is a self-report scale with three subscales with 7 Likert scale items ranging from 0 (Did not apply to me at all) to 3 (Applied to me very much or most of the time). Final scores were calculated by adding the items per (sub)scale and multiplying them by 2. Thus, the total scores for the DASS-21-total scale ranged between 0 and 120, and those for each subscale ranged between 0 and 42. Scores for each subscale were classified into five severity ranges: normal, mild, moderate, severe, and extremely severe. The cut-off points for each category were as follows: for depression subscale, normal (0–9), mild (10–13), moderate (14–20), severe (21–27), and extremely severe (28 and more); for anxiety subscale, normal (0–7), mild (8–9), moderate (10–14), severe (15–19), and extremely severe (20 and more); for the Stress subscale, normal (0–14), mild (15–18), moderate (19–25), severe (26–33), and extremely severe (34 and more).20,21
Since this study was conducted in a health-specialized governmental university that has an English exam before enrolling students in the programs, all students are expected to know English very well; therefore, the instrument was administered in its original language, English.
The DASS-21 scale has been used in the literature to measure our variables of interest (depression, anxiety, and stress), and it has been shown to have high internal consistency among various populations before and during the COVID-19 epidemic.22–25 The DASS-21 scale is a reliable and valid tool with reliability coefficients of 0.91, 0.85, and 0.89, respectively.26 Moreover, the DASS-21 was validated for use among the population in Saudi Arabia and college students.27,28
Ethical Considerations
The ethics committee approved this study of the KSAU-HS and the King Abdullah International Medical Research Center (KAIMRC) with approval number [RYD-21-419812-21674]. The participants provided electronic informed consent. All methods were performed per the KAIMRC and the international guidelines and regulations.
Data Management and Analysis Plan
The data were coded and entered into a data entry file using the Statistical Package for the Social Sciences, version 27 (SPSS). Descriptive statistics and frequency distributions were utilized to describe the sociodemographic data. Depression, anxiety, and stress were described as mild to extremely severe based on the scoring system described above. Spearman correlation was used to detect the correlations between the dependent variables of interest and the continuous independent variable (age). A t-test and ANOVA compare mean tests were implemented to examine depression, anxiety, and stress concerning sociodemographic and health characteristics for categorical variables. The variables with a p-value of less than 0.25 were entered into three separate linear regression models after the assessment of collinearity prior to adding variables in the final model. The critical value of the significance in all the analyses was set at p < 0.05 and a 95% confidence interval. For assumptions of normality, Shapiro–Wilk tests were used for each numeric variable. Second, based on Levene’s test results, we identified that the variance of the groups was not statistically different.
Results
Levels and Prevalence of Depression, Anxiety, and Stress
A total of 311 students participated in the questionnaire. As results showed in Figure 1, the prevalence of depression, anxiety, and stress were, respectively, 15.8%, 5.8%, and 12.2% for at least mild symptoms, 23.5%, 13.2%, and 19.6% for at least moderate symptoms, 19.6%, 16.4%, and 12.5% for at least severe symptoms and 9.6%, 41.8% and 3.9% for at least extremely severe symptoms.
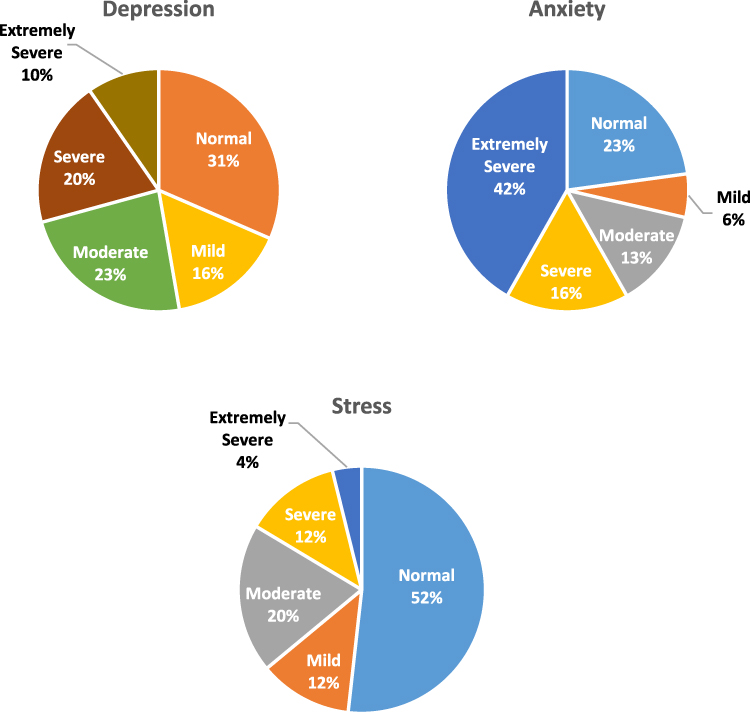 |
Figure 1 Stress, anxiety, and depression levels among the participants (N = 311). Notes: Scores for each subscale were classified into five levels: normal, mild, moderate, severe, and extremely severe. For depression subscale, normal, 0–9; mild, 10–13; moderate, 14–20; severe, 21–27; and extremely severe, 28 and more. For anxiety subscale, normal, 0–7; mild, 8–9; moderate, 10–14; severe, 15–19; and extremely severe, 20 and more. For the Stress subscale, normal, 0–14; mild, 15–18; moderate, 19–25; severe, 26–33; and extremely severe, 34 and more. |
Sociodemographic Characteristics
Of the total participants, 195 (62.7%) were female with a mean age of 21.32 (SD = 1.97), ranging between 18–34 years old. Most of the participants were living with their parents (n = 298, 95.8%), single (n = 294, 94.5%), and never quarantined by health authority (n = 270, 86.8%) or diagnosed with COVID-19 (n = 282, 90.7%). Other characteristics of the participants are reported in Table 1.
 |
Table 1 Sociodemographic and Health Characteristics and Their Associations with Depression, Anxiety, and Stress (N = 311) |
Associations Between Depression, Anxiety, and Stress with Sociodemographic Characteristics
Spearman correlation was computed to assess the relationship between age and each of the depression, anxiety, and stress. The results revealed that there was a negative correlation between age and anxiety, r (309) = −0.121, p = 0.034, and stress, r (309) = −0.119, p = 0.037. There was no correlation between age and depression, r (309) = −0.086, p = 0.129.
Further analysis revealed that the average total score for depression, anxiety, and stress was significantly higher among female students than male students, for depression (M = 15.96, SD = 8.87) vs (M = 12.74, SD = 9.36), t = −3.033, p = 0.003, anxiety (M = 17.98, SD = 9.84) vs (M = 14.77, SD = 10.75), t = −2.689, p = 0.008, and stress (M = 16.09, SD = 9.60) vs (M = 12.78, SD = 9.99), t = −2.689, p = 0.004. Moreover, the average total score for depression, anxiety, and stress was significantly higher among students who had history of depression, for depression (M = 21.01, SD = 8.57) vs (M = 12.98, SD = 8.56), t = 6.876, p < 0.001, anxiety (M = 24.17, SD = 8.40) vs (M = 14.68, SD = 9.82), t = 7.299, p < 0.001, and stress (M = 22.72, SD = 8.67) vs (M = 12.61, SD = 9.01), t = 8.287, p < 0.001. Students who are quarantined by a health authority have significantly higher depression than who did not (M = 17.80, SD = 10.37) vs (M = 14.30, SD = 8.92), t = 2.294, p = 0.022. Also, the average total score for depression was significantly higher among students who had contact with a confirmed case of COVID-19 compared to who did not contact any positive case (M = 15.82, SD = 9.13) vs (M = 13.63, SD = 9.12), t = 2.114, p = 0.035. Levels of depression, anxiety, and stress did not vary significantly based on the rest of the sociodemographic characteristics (refer to Table 1).
Predictors of Depression, Anxiety, and Stress
Further analysis was conducted to find out the predictor variables of depression, anxiety, and stress (Table 2). The variables with a p-value of less than 0.25 were entered into three separate linear regression models after the assessment of collinearity prior to adding the variables to the final model to find their effect on each of the depression, anxiety, and stress. All entered independent variables have a variance inflation factor (VIF) of less than 2, indicating no multicollinearity among the independent variables.
 |
Table 2 Linear Regression Model on Predictors of Depression, Anxiety, and Stress |
As shown in Table 2, the linear regression model accounted for a significant portion of the variance in depression [R2 = 0.172 (Adj R2 = 0.156), F-change = 10.55, P ≤ 0.001], anxiety [R2 = 0.179 (Adj R2 = 0.163), F-change = 11.05, P ≤ 0.001], and stress [R2 = 0.211 (Adj R2 = 0.195), F-change = 13.54, P ≤ 0.001].
Discussion
University students generally have poor psychological quality and bearing capacity. The major factors affecting university students’ mental health are the public health emergency caused by COVID-19, the sudden and public uncertainty it has caused, and the potential for serious harm. According to one study, unexpected public health events challenge psychological adaptability, particularly in college students.29–31 Therefore, the purpose of this study was to assess the prevalence and associated factors of depression, anxiety, and stress among college students in Saudi Arabia. Our survey of 311 students in a large university located on three campuses in three different regions of Saudi Arabia revealed that depression, anxiety, and stress were highly prevalent among the participants. More than half of the participants experienced higher than moderate levels of depression and anxiety, while the least was stress reported among 36% of the students for more than moderate level. Therefore, anxiety was the highest, followed by depression and stress.
Several research findings have found that college students in Saudi Arabia exhibit similar anxiety symptoms and stress, with a predominance of depression and anxiety ranging from 14 to 50%.12,14,32 In general, our study results were similar to Radwan et al study, as our results showed that the prevalence of depression, anxiety, and stress at the different levels were 68.5%, 77.2%, and 48.2%, respectively. Moreover, severe or extremely severe symptoms of depression, anxiety, and stress were 29.2%, 58.2%, and 16.4% of the participants, respectively. The findings of Radwan et al (2021) study revealed that most students experienced moderate-to-severe anxiety levels (89.1%) and depression (72.1%).32 In contrast, only 36% experienced moderate-to-severe stress.32
In contrast to the general population in Saudi Arabia during the pandemic, college students have a greater level of depression, anxiety, and stress. For instance, among the general population in Saudi Arabia, only 17% experienced a moderate-to-severe depressive symptoms, 10% experienced moderate-to-severe anxiety symptoms, and 12% experienced moderate-to-severe stress.33 Furthermore, in the general population, a study conducted by Alyami et al, among the population in Saudi Arabia revealed that the prevalence of depression and anxiety was 9.4% and 7.3%, respectively.34
On the other hand, studies before the pandemic reported moderate levels of depression, anxiety, and stress among college students.35 According to a systematic review study, the prevalence of anxiety among students ranged between 34.9% and 65%.36 Therefore, there has been a noticeable increase in the prevalence of these mental health conditions during the pandemic, mainly due to the fear of the unknown virus (COVID-19) and the fear of the future, especially for the young generation.37
Furthermore, our study investigated the associated factors of depression, anxiety, and stress during the COVID-19 epidemic. Our findings revealed that being female, younger age, having a history of depression, being quarantined by a health authority, and having contact with a confirmed case of COVID-19 were associated with a greater level of depression, anxiety, and stress. Our results were similar to the results of the study conducted by Alamri et al, Qiu et al, and Shigemura et al, as the findings highlighted that being female was associated with greater level of depression, anxiety, and stress, which is consistent with another study by Radwan et al who found that depression, anxiety, and stress scores were significantly different across gender, and age groups.32,33,38,39 At the same time, our results echoed other evidence in international literature indicating that females are more susceptible to stress and post-traumatic symptoms.32,33,38,39
The present study found an association between college-age students with stress and anxiety. Our results were quite similar to the study by Alkhamees et al that showed age was associated with depression, anxiety, and stress. Indeed, according to Alkhamees et al study, 28.3%, 24%, and 22.3% of the population in Saudi Arabia had moderate-to-severe depression, anxiety, and stress related to age, respectively.1 These differences might be because college students are young adults, and they are at higher risk for depression, anxiety, and stress. Therefore, these findings align with previous findings that revealed younger age is associated with higher stress, anxiety, and depression.33 Given these results, it can be concluded that depression, anxiety, and stress might be increased among college students in Saudi Arabia during the COVID-19 epidemic.
Moreover, the present study found that a history of depression positively relates to depression, anxiety, and stress. This finding echoes previous research demonstrating that a history of depression is associated with greater psychological distress during pandemic situations. This finding aligns with earlier studies by Wang et al and Cuthbertson et al, showing that depression or a self-report of poor health status is associated with increased psychological distress.40,41 A possible clarification for this result is that individuals with a history of depression or other psychological distress who perceive their health as poor might feel more vulnerable to fighting a new disease.
Finally, this study showed that participants who were quarantined by a health authority or who were exposed to a positive case of COVID-19 experienced a higher level of depression. This result is also consistent with the literature. For instance, Alkhamees et al and Hossain et al reported that psychological distress, including depression, has been associated with quarantine by a health authority1,42–44 This might be due to the feeling of loneliness and self-isolation. Moreover, our findings regarding the exposure to positive cases are similar to other studies’ results that were conducted earlier in Saudi Arabia. According to Alamri et al, individuals who reported direct contact with COVID-19 patients had experienced a higher level of depression.33 Moreover, according to Zhao et al, individuals who were exposed to positive cases of COVID-19 experienced high levels of depression and fatigue.45 A possible explanation is that students who are exposed to positive cases were forced to self-isolation and repeated virus testing. In addition, they might be afraid of transmitting the virus to their family members or close relatives. Moreover, discriminations and stigma linked to COVID-19, plus social isolation, are already risk factors for an increased level of depression.46,47 This requests more emphasis on students’ mental health, especially as the pandemic progresses or future pandemics occur.
Limitations and Recommendation
This study had some limitations that should be considered. This study did not have any baseline information about the participants’ psychological status before the COVID-19 outbreak; therefore, no pre- and post-epidemic evaluations were available. Longitudinal studies are recommended to determine whether this information will last for a more extended time. Another limitation of this study is that because the universities were closed due to the COVID-19 pandemic and students were not physically available, data were collected through the e-survey technique. Interview studies are recommended to obtain in-depth information.
Conclusion and Implications for Practice
Depression, anxiety, and stress are prevalent among college students during the COVID-19 outbreak in Saudi Arabia. This study highlighted some subgroups of students who are at higher risk. For instance, younger age, females, and history of depression were significantly related to stress and anxiety scores. The depression level was significantly higher among females, and participants with a history of depression had been quarantined by a health authority, or had contact with a positive case of COVID-19. Future interventions should concentrate on developing strategies that promote the students’ mental health and well-being. Moreover, community health and mental care should be accessible to all students, especially those at higher risk for psychological distress. Furthermore, each educational institution is recommended to start focusing on the student’s mental well-being activities and promote their health-seeking behaviors. Collaboration between Well Students Centers and colleges is urgently needed to create programs targeting students’ mental health. Arranging periodic webinars on mental health promotion might empower the students to face future challenges.
In summary, the psychological status of college students in Saudi Arabia is significantly impacted by a public health outbreak. Therefore, they require immediate attention, assistance, and support. It is recommended that government and colleges collaborate to solve this issue to provide prompt and high-quality psychological support to college students in Saudi Arabia, special consideration must be implemented to the individuals at risk because of their vulnerability towards serious mental disorders.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Alkhamees AA, Alrashed SA, Alzunaydi AA, Almohimeed AS, Aljohani MS. The psychological impact of COVID-19 pandemic on the general population of Saudi Arabia. Compr Psychiatry. 2020;1(102):152192. doi:10.1016/j.comppsych.2020.152192
2. Al Sulais E, Mosli M, AlAmeel T. The psychological impact of COVID-19 pandemic on physicians in Saudi Arabia: a cross-sectional study. Saudi J Gastroenterol. 2020;26(5):249–255. doi:10.4103/sjg.SJG_174_20
3. Al-Hanawi MK, Mwale ML, Alshareef N, et al. Psychological distress amongst health workers and the general public during the COVID-19 pandemic in Saudi Arabia. Risk Manag Healthc Policy. 2020;13:733–742. doi:10.2147/RMHP.S264037
4. Mosli M, Alourfi M, Alamoudi A, et al. A cross-sectional survey on the psychological impact of the COVID-19 pandemic on inflammatory bowel disease patients in Saudi Arabia. Saudi J Gastroenterol. 2020;26(5):263–271. doi:10.4103/sjg.SJG_220_20
5. Struyf T, Deeks JJ, Dinnes J, et al. Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID‐19. Cochrane Database Syst Rev. 2022;5. doi:10.1002/14651858.CD013665.pub3
6. Algaissi AA, Alharbi NK, Hassanain M, Hashem AM. Preparedness and response to COVID-19 in Saudi Arabia: building on MERS experience. J Infect Public Health. 2020;13(6):834–838. doi:10.1016/j.jiph.2020.04.016
7. Hassounah M, Raheel H, Alhefzi M. Digital response during the COVID-19 pandemic in Saudi Arabia. J Med Internet Res. 2020;22(9):e19338. doi:10.2196/19338
8. Khan A, Alsofayan Y, Alahmari A, et al. COVID-19 in Saudi Arabia: the national health response. East Mediterr Health J. 2021;27(11):1114–1124. doi:10.26719/emhj.21.048
9. Al Mamun F, Hosen I, Misti JM, Kaggwa MM, Mamun MA. Mental disorders of Bangladeshi students during the COVID-19 pandemic: a systematic review. Psychol Res Behav Manag. 2021;14:645. doi:10.2147/PRBM.S315961
10. Kauhanen L, Wan Mohd Yunus WM, Lempinen L, et al. A systematic review of the mental health changes of children and young people before and during the COVID-19 pandemic. Eur Child Adolesc Psychiatry. 2022;12:1–9. doi:10.1007/s00787-022-02060-0
11. Li Y, Wang A, Wu Y, Han N, Huang H. Impact of the COVID-19 pandemic on the mental health of college students: a systematic review and meta-analysis. Front Psychol. 2021;12:669119. doi:10.3389/fpsyg.2021.669119
12. Amr M, Amin TT, Saddichha S, et al. Depression and anxiety among Saudi university students: prevalence and correlates. Arab J Psychiat. 2013;24(1):1–7. doi:10.12816/0000092
13. Al Gelban KS. Prevalence of psychological symptoms in Saudi secondary school girls in Abha, Saudi Arabia. Ann Saudi Med. 2009;29(4):275–279. doi:10.4103/0256-4947.55308
14. Al-Gelban KS. Depression, anxiety and stress among Saudi adolescent school boys. J R Soc Promot Health. 2007;127(1):33–37. doi:10.1177/1466424007070492
15. Alenazi SF, Hammad SM, Mohamed AE. Prevalence of depression, anxiety and stress among male secondary school students in Arar city, Saudi Arabia, during the school year 2018. Electron Physician. 2019;11(2):7522–7528. doi:10.19082/7522
16. Khoshaim HB, Al-Sukayt A, Chinna K, et al. Anxiety level of university students during COVID-19 in Saudi Arabia. Front Psychiatry. 2020;11(11):579750. doi:10.3389/fpsyt.2020.579750
17. Ho CS, Chee CY, Ho RC. Mental health strategies to combat the psychological impact of COVID-19 beyond paranoia and panic. Ann Acad Med Singapore. 2020;49(1):1–3.
18. Polit DF, Beck CT. Nursing Research: Generating and Assessing Evidence for Nursing Practice. Lippincott Williams & Wilkins; 2008.
19. Davis RN. Web-based administration of a personality questionnaire: comparison with traditional methods. Behav Res Methods Instrum Comput. 1999;31(4):572–577. doi:10.3758/BF03200737
20. Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the beck depression and anxiety inventories. Behav Res Ther. 1995;33(3):335–343. doi:10.1016/0005-7967(94)00075-U
21. Brown TA, Chorpita BF, Korotitsch W, Barlow DH. Psychometric properties of the Depression Anxiety Stress Scales (DASS) in clinical samples. Behav Res Ther. 1997;35(1):79–89. doi:10.1016/S0005-7967(96)00068-X
22. Najjuka SM, Checkwech G, Olum R, Ashaba S, Kaggwa MM. Depression, anxiety, and stress among Ugandan university students during the COVID-19 lockdown: an online survey. Afr Health Sci. 2021;21(4):1533–1543. doi:10.4314/ahs.v21i4.6
23. Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
24. Tan W, Hao F, McIntyre RS, et al. Is returning to work during the COVID-19 pandemic stressful? A study on immediate mental health status and psychoneuroimmunity prevention measures of Chinese workforce. Brain Behav Immun. 2020;87(1):84–92. doi:10.1016/j.bbi.2020.04.055
25. Wang C, Pan R, Wan X, et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav Immun. 2020;87(1):40–48. doi:10.1016/j.bbi.2020.04.028
26. Beard C, Björgvinsson T. Beyond generalized anxiety disorder: psychometric properties of the GAD-7 in a heterogeneous psychiatric sample. J Anxiety Disord. 2014;6(28):547–552. doi:10.1016/j.janxdis.2014.06.002
27. Alshloul MN, Bdair IA, Alalyani MM. Severity of depression, anxiety, and stress among undergraduate health science students in Abha, Saudi Arabia. Open J Psychiatry Allied Sci. 2021;12(2):132–139. doi:10.5958/2394-2061.2021.00029.X
28. Mirza AA, Milaat WA, Ramadan IK, et al. Depression, anxiety and stress among medical and non-medical students in Saudi Arabia: an epidemiological comparative cross-sectional study. Neurosci J. 2021;26(2):141–151. doi:10.1016/j.comppsych.2020.152192
29. Debowska A, Horeczy B, Boduszek D, Dolinski D. A repeated cross-sectional survey assessing university students’ stress, depression, anxiety, and suicidality in the early stages of the COVID-19 pandemic in Poland. Psychol Med. 2020;2:1–4. doi:10.1017/S003329172000392X
30. Fawaz M, Samaha A. E‐learning: depression, anxiety, and stress symptomatology among Lebanese University students during COVID‐19 quarantine. Nurs Forum. 2021;56(1):52–57. doi:10.1111/nuf.12521
31. Rith-Najarian LR, Boustani MM, Chorpita BF. A systematic review of prevention programs targeting depression, anxiety, and stress in university students. J Affect Disord. 2019;257:568–584. doi:10.1016/j.jad.2019.06.035
32. Radwan E, Radwan A, Radwan W, Pandey D. Prevalence of depression, anxiety and stress during the COVID-19 pandemic: a cross-sectional study among Palestinian students (10–18 years). BMC Psychol. 2021;9(1):1–2. doi:10.1186/s40359-021-00688-2
33. Alamri HS, Algarni A, Shehata SF, et al. Prevalence of depression, anxiety, and stress among the general population in Saudi Arabia during covid-19 pandemic. Int J Environ Res Public Health. 2020;17(24):9183. doi:10.3390/ijerph17249183
34. Alyami HS, Naser AY, Dahmash EZ, Alyami MH, Alyami MS. Depression and anxiety during the COVID‐19 pandemic in Saudi Arabia: a cross‐sectional study. Int J Clin Pract. 2021;75(7):e14244. doi:10.1111/ijcp.14244
35. Al Bahhawi T, Albasheer OB, Makeen AM, et al. Depression, anxiety, and stress and their association with khat use: a cross-sectional study among Jazan University students, Saudi Arabia. Neuropsychiatr Dis Treat. 2018;14:2755. doi:10.2147/NDT.S182744
36. Alahmadi AM. Prevalence of anxiety among college and school students in Saudi Arabia: a systematic review. J Health Inform Dev Ctries. 2019;13(1):1.
37. Sallam M, Dababseh D, Yaseen A, et al. Conspiracy beliefs are associated with lower knowledge and higher anxiety levels regarding COVID-19 among students at the University of Jordan. Int J Environ Res Public Health. 2020;17(14):4915. doi:10.3390/ijerph17144915
38. Qiu J, Shen B, Zhao M, Wang Z, Xie B, Xu Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: implications and policy recommendations. Gen Psychiatry. 2020;33(2):e100213. doi:10.1136/gpsych-2020-100213
39. Shigemura J, Ursano RJ, Morganstein JC, Kurosawa M, Benedek DM. Public responses to the novel 2019 coronavirus (2019‐nCoV) in Japan: mental health consequences and target populations. Psychiatry Clin Neurosci. 2020;74(4):281. doi:10.1111/pcn.12988
40. Wang C, Pan R, Wan X, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. 2020;17(5):1729. doi:10.3390/ijerph17051729
41. Cuthbertson BH, Hull A, Strachan M, Scott J. Post-traumatic stress disorder after critical illness requiring general intensive care. Intensive Care Med. 2004;30(3):450–455. doi:10.1007/s00134-003-2004-8
42. Hossain MM, Sultana A, Purohit N. Mental health outcomes of quarantine and isolation for infection prevention: a systematic umbrella review of the global evidence. Epidemiol Health. 2020;42. doi:10.4178/epih.e2020038
43. Mazza C, Ricci E, Biondi S, et al. A nationwide survey of psychological distress among Italian people during the COVID-19 pandemic: immediate psychological responses and associated factors. Int J Environ Res Public Health. 2020;17(9):3165. doi:10.3390/ijerph17093165
44. Montano RL, Acebes KM. Covid stress predicts depression, anxiety and stress symptoms of Filipino respondents. Int J Acad Res Bus Soc Sci. 2020;9(4):78–103. doi:10.20525/ijrbs.v11i6
45. Zhao YJ, Zhang SF, Li W, et al. Mental health status and quality of life in close contacts of COVID-19 patients in the post-COVID-19 era: a comparative study. Transl Psychiatry. 2021;11(1):1–7. doi:10.1038/s41398-021-01623-0
46. Corfield EC, Martin NG, Nyholt DR. Co-occurrence and symptomatology of fatigue and depression. Compr Psychiatry. 2016;71:1–10. doi:10.1016/j.comppsych.2016.08.004
47. Weinstein A, Maayan G, Weinstein Y. A study on the relationship between compulsive exercise, depression and anxiety. J Behav Addict. 2015;4(4):315–318. doi:10.1556/2006.4.2015.034
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.