")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Psychological Resilience and Stress Coping Styles in Migraine Patients
Authors Kurtses Gürsoy B , Köseoğlu Toksoy C
Received 23 November 2022
Accepted for publication 24 December 2022
Published 5 January 2023 Volume 2023:19 Pages 63—72
DOI https://doi.org/10.2147/NDT.S398838
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Betül Kurtses Gürsoy,1 Cansu Köseoğlu Toksoy2
1Afyonkarahisar Health Science University, Faculty of Medicine, Department of Psychiatry, Afyonkarahisar, Turkey; 2Afyonkarahisar Health Science University, Faculty of Medicine, Department of Neurology, Afyonkarahisar, Turkey
Correspondence: Betül Kurtses Gürsoy, Afyonkarahisar Health Science University, Faculty of Medicine, Department of Psychiatry, Afyonkarahisar, 03030, Turkey, Tel +90 544 595 1985, Email [email protected]
Purpose: It was aimed to determine the level of psychological resilience and to investigate the psychological and clinical parameters that affect the resilience level in migraine patients.
Patients and Methods: A total of 100 migraine patients and 100 healthy controls who agreed to participate in the study filled in the sociodemographic data form and also Beck Anxiety Scale, Beck Depression Scale, Psychological Resilience Scale for Adults, Perceived Stress Scale, Stress Coping Styles Scale, and Psychological Well-Being Scale. Also, the results of Migraine Disability Assessment Scale (MIDAS) were recorded in order to determine the clinical parameters of migraine patients.
Results: When the migraine patients were examined in terms of the number of painful days in the last 3 months, duration of illness, and correlations between clinical scales, there were statistically significant correlations between the psychological resilience scale and well-being (r=0.691 p< 0.001), positive coping styles (r=0.676 p< 0.001), Beck depression scale (r=− 0.670 p< 0.001).
Conclusion: Self-confident approach, social support-seeking approach, and level of psychological well-being predict psychological resilience in migraine patients. Interventions aiming to increase the level of psychological resilience, which is negatively correlated with depression, are expected to increase the quality of life of patients with migraine.
Keywords: migraine, psychological resilience, coping skills, depression
Introduction
In the global disease burden research performed in 2016, migraine was on the first line in the 15–49 age group while it was second in the years lost with a disability considering all ages.1 Although there are still issues that have not been enlightened in the etiopathogenesis of migraine, a serious burden on the health system, it is known that the key point is structured by the HPA axis and the trigeminal nerve.2
The fight-or-flight response, a well-known short-term response to acute stress, includes hypothalamic signaling of catecholamine release from the adrenal medulla via the sympathetic nervous system. Corticotropin-releasing hormone (CRH) and vasopressin (AVP) are released from the hypothalamic paraventricular nucleus (PVN) as part of a more persistent stress response, stimulating the anterior pituitary gland to release adrenocorticotropic hormone (ACTH) into the circulation. Chronic stress may result in a loss of negative feedback control, as well as long-term changes in HPA regulation and persistent changes in stress reactivity.3 Limbic structures such as the hippocampus, amygdala, and prefrontal cortex help to reset the HPA axis after a stressful event and to regulate its tone. In the literature, there are studies suggesting increased HPA axis response in migraineurs, as well as studies with conflicting results. Inconsistent results have been attributed to heterogeneity of stress types and etiologies.4
Stress is the most commonly known factor that triggers migraine pain. When the behavioral or physiological stressors are frequent/severe, allostatic loading happens. So, both functional and structural changes occur in the brain network and this condition leads the person to give abnormal reactions to environmental factors and the disease to become chronic.5 In other words, stress may help to initiate migraine in people prone to disease while it may also contribute to the migraine becoming chronic.6,7
Psychological resilience is the ability of the person to positively adapt to the encountered vital problems, the power to bounce back, and the skill to get over problems successfully.8,9 Although resilience was first thought to be a personality trait that reduces the negative effects of stress and increases adaptation, nowadays it is accepted that resilience is a dynamic, learnable process that includes sensory, cognitive, and behavioral components.10 Long-term stress reduces the defense power through allostatic loading and creates a basis for diseases. Resilience is expected to increase as a result of interventions aimed to reduce allostatic load.11 Many studies conducted in recent years draw attention to the relationship between resilience and diseases such as colon cancer, hypertension, and ischemic heart disease.9 In fact, it has been suggested that in individuals receiving treatment for colon cancer, the recovery rates are higher in ones with high resilience levels.12
Resilient individuals have a more flexible thinking structure than vulnerable ones and they receive support from their internal and environmental resources to cope with the problems they face (eg, psychological characteristics, familial support).13 Coping with stress is the cognitive and/or behavioral effort to cope with stressful/difficult conditions that test the individual’s resources. This effort is considered as two kinds, if it consists of adaptive efforts such as planning, and seeking social support as a tool, it is problem-focused. If it consists of maladaptive efforts such as blame and denial, it is emotion-focused.14 Resilient individuals emerge from challenging situations by improving their coping styles. It is thought that a problem-focused coping style predicts resilience and resilience predicts psychological well-being.15 In migraine patients, it has been observed that especially undiagnosed anxiety and depression symptoms increase the way of coping with maladaptive stress.16
To our knowledge, no research has been conducted to date on the relationship between resilience and stress-coping styles in people with migraine. The aim of this study is to explore the association between resilience and stress-coping styles in people with migraine. An additional aim was to explore the level of resilience of patients with migraine in relation to socio-demographic factors, perceived stress level, psychological well-being, and severity of the disease.
Patients and Methods
In the study, 100 patients who were diagnosed with migraine according to the International Classification of Headache Disorders (ICHD-III) and admitted to the neurology outpatient clinic of Afyonkarahisar Health Sciences University between May 2021 and May 2022, were included. As the control group, 100 healthy controls matched for sociodemographic characteristics were also included. The informed consent form was obtained from all participants for this study. The study was approved by the Ethics Committee of Afyonkarahisar Health Sciences University and the study was conducted in accordance with the Helsinki Declaration (decision date and number: 02.04.2021–2021/208).
The inclusion criteria for the study were: ages between 18 and 65 years, being diagnosed with migraine and giving consent to participate in the study. Exclusion criteria were: having a diagnosis of another type of headache, comorbid psychotic disorders, presence of any cranial organicity in CT or MR imaging methods, severe neurological impairment or chronic systemic diseases, and being pregnant.
SCID-5 (Structured Clinical Interview According to the DSM-5), which is a clinical interview structured according to the DSM-5 (Diagnostic and Statistical Manual for Psychiatric Disorders), published by the American Psychiatric Association in 2013, has been implemented. In addition, sociodemographic data form, Beck Anxiety Scale,17 Beck Depression Scale,18 Psychological Resilience Scale for Adults,13 Perceived Stress Scale,19 Stress Coping Styles Scale,20 Psychological Well-Being Scale,21 and Migraine Disability Assessment Scale (MIDAS)22 were applied by the clinician.
Instruments of Assessment
Sociodemographic Data Form
This form consists of questions including sociodemographic information such as age, gender, marital status, educational level, and job status.
Beck Anxiety Scale
It is a self-report scale developed by Beck et al in 1988.17 The total score of the 21-item scale is used to determine the level of anxiety. Turkish validity and reliability were performed by Ulusoy et al.23
Beck Depression Scale
This scale, whose total score ranges from 0 to 63, is a self-assessment scale consisting of 21 items in a four-Likert structure. Turkish validity and reliability of this scale, developed by Beck et al in 1961,18 was made by Hisli in 1989.24
Psychological Resilience Scale for Adults
This scale, which was developed to measure the psychological resilience of adults, consists of 33 items.13 Two opposite judgments were presented to complete the unfinished sentences, and the participant is expected to mark the judgment to which he/she feels closer. The Turkish validity and reliability of the scale were performed by Basım and Çetin.25 There are six factors consisting of self-perception, future perception, structural style, family harmony, social competence, and social resources in its structure. The cut-off score is not used, and an increase in the total score indicates an increase in mental resilience.
Perceived Stress Scale
The 10-item form of the scale developed by Cohen et al was used in this study.19 Turkish validity and reliability of the 5-point Likert-item scale were performed by Eskin et al.26 The total score of the scale varies between 0–40. The scale does not have a cut-off point. An increase in the scale score indicates a high level of perceived stress.
Stress Coping Styles Scale
The scale was developed by Folkman and Lazarus in 1980,20 and the Turkish validity and reliability of the scale were performed by Şahin et al in 1992.27 Stress Coping Styles Scale is a self-report scale with 4 options, 30 items, and 5 subscales. The subscales include self-confident approach, optimistic approach, helpless approach, submissive approach, and social support-seeking approach. While the self-confident approach, optimistic approach, and social support-seeking approach are called positive coping styles, the helpless approach and the submissive approach are called negative coping styles.
Psychological Well-Being Scale
Psychological Well-Being Scale, that is consisted of eight items, defines important elements of human function, from positive relationships to feelings of adequacy and having a meaningful and purposeful life. Turkish validity and reliability of the scale developed by Diener et al21 were performed by Telef.28
Migraine Disability Assessment Scale (MIDAS)
Migraine Disability Assessment Scale (MIDAS),22 which is developed to measure disability in migraine patients, is one of the commonly used scales and it determines migraine-related disability in the last 3 months. In our country, in the studies conducted on migraine patients, it was stated that MIDAS is a reliable scale for measuring the severity of the disease and determining the treatment strategy.29
Statistical Analysis
The obtained data were evaluated with the SPSS version 25 package program (SPSS Inc., Chicago, IL, USA). Shapiro–Wilks test was used to determine the distribution characteristics of the variables. Normally distributed continuous variables were expressed with mean and standard deviation. Correlations between scales and persistent clinical parameters (duration of diagnosis, number of painful days) were analyzed using the Pearson correlation test. The effects of clinical scales on resilience were evaluated with simple linear regression and mediator-mediated regression analysis. P values less than 0.05 were considered statistically significant.
Results
In the study, 100 migraine patients who met the inclusion criteria, and 100 age and sex-matched healthy controls were included. The mean age of the patient group was 37.8 years and 82 (82%) were female. In the healthy control group, 79% (n=79) were female, the mean age was 35.2 years. No difference was observed between the groups in terms of marital status, employment status and education level.
When the applied scales were evaluated, it was observed that the mean scores of the scales, except for the psychological well-being scale (p=0.055), caused a statistically significant difference between the two groups (Table 1).
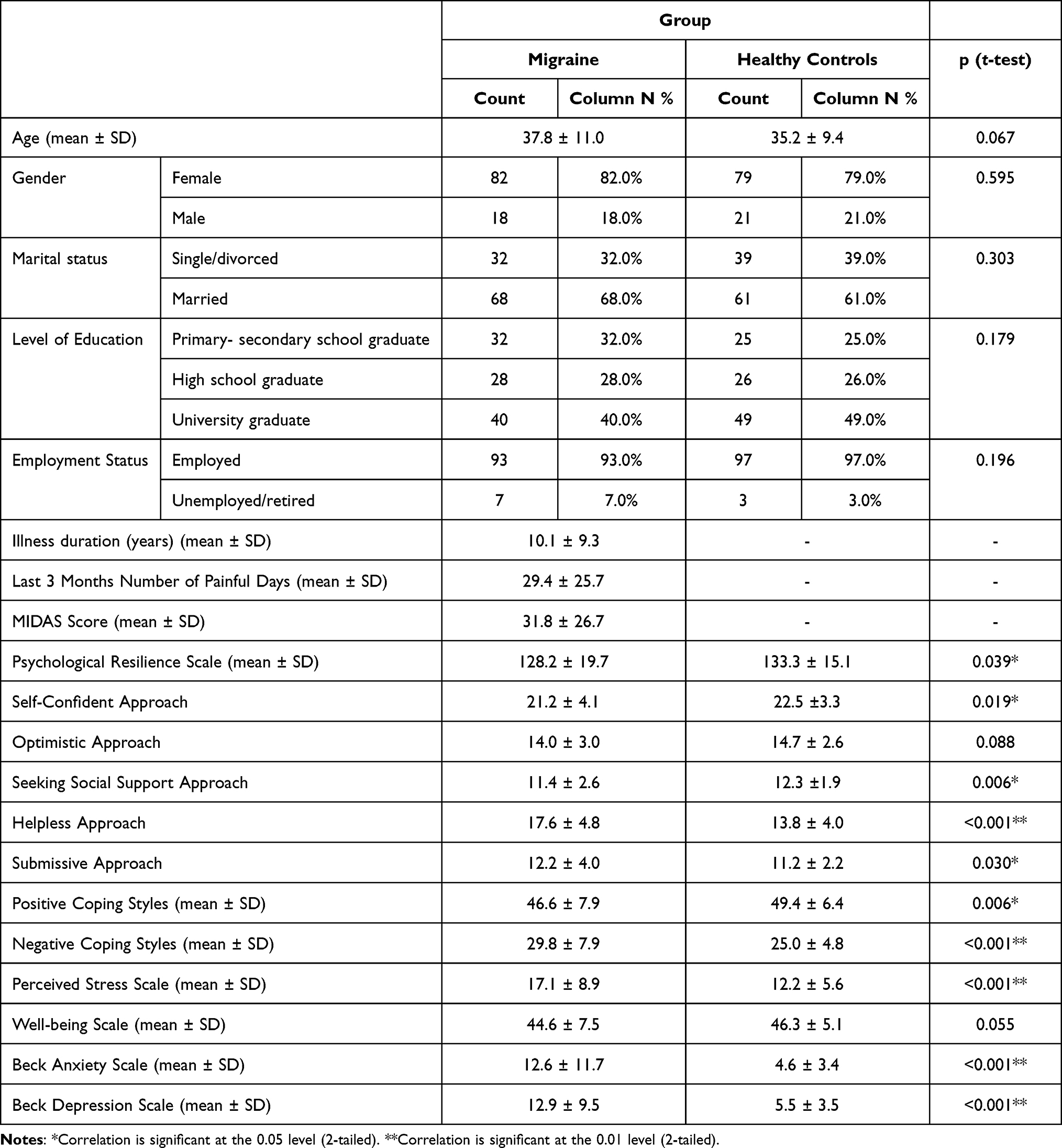 |
Table 1 Sociodemographic and Clinical Scale Scores of the Groups |
When the correlations between the number of painful days in the last 3 months, duration of illness, and clinical scales among migraine patients were examined, a significant direct correlation was present between the psychological resilience scale and well-being (r=0.691 p<0.001), positive coping styles (r=0.676 p<0.001). Additionally it has determined that the psychological resilience scale has significant inverse correlations with negative coping styles (r=−0.471 p<0.001), perceived stress scale (r=−0.623 p<0.001), Beck anxiety scale (r=−0.433 p<0.001) and Beck depression scale (r=−670 p<0.001). Other correlation values are shown in Table 2.
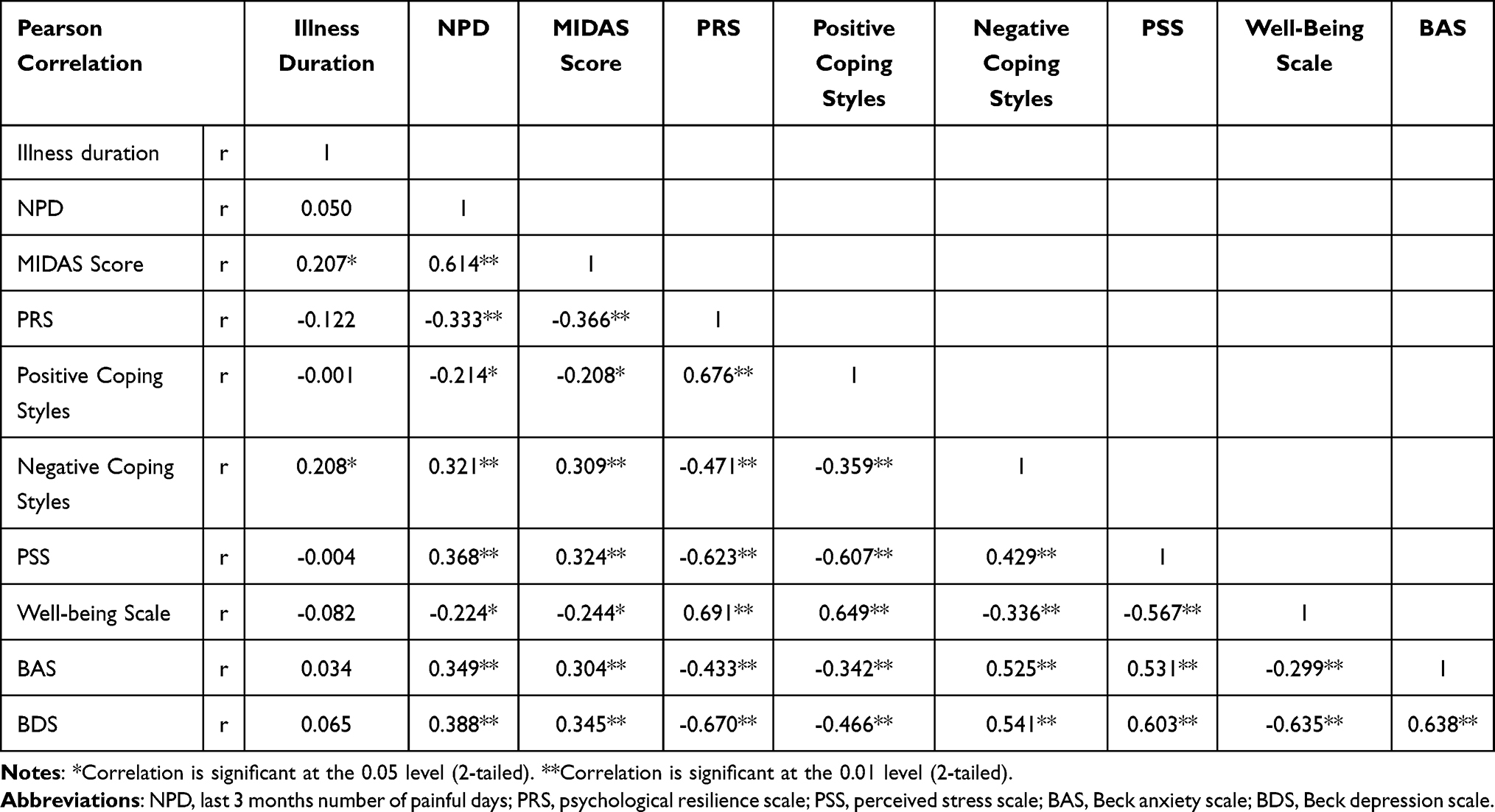 |
Table 2 Correlation Analysis Between Migraine Parameters and Clinical Scale Scores in the Migraine Group |
The variables related to the illness are examined, it is seen that significant positive correlations were present with illness duration and MIDAS score (r=0.207 p=0.039), negative coping styles (r=0.208 p=0.038). On the other hand the number of painful days in the last 3 months showed a significant positive correlation with MIDAS Score (r=0.614 p<0.001), negative coping styles (r=0.321 p=0.001), perceived stress scale (r=0.368 p<0.001), Beck anxiety scale (r=0.349 p<0.001), and Beck depression scale (r=0.388 p<0.001); and the number of painful days in the last 3 months is inversely correlated with psychological resilience scale (r=−0.333 p=0.001), positive coping styles (r=−0.214 p=0.032), and well-being scale (r=−0.224 p=0.025). There were significant positive correlations between the MIDAS score and negative coping styles (r=0.309 p=0.002), perceived stress scale (r=0.324 p=0.001), Beck anxiety scale (r=0.304 p=0.002), and Beck depression scale (r=0.345 p<0.001); and significant inverse correlations between the MIDAS score and psychological resilience scale (r=−0.366 p<0.001), positive coping styles (r=−0.208 p=0.038), well-being scale (r=−0.244 p=0.014).
In the linear regression analysis, it was found that the predictors of the psychological resilience scale were the self-confidence approach (B=1.085 p=0.016), seeking social support (B=1.668 p= 0.001), and well-being scale (B=0.762 p=0.002) in the migraine group, self-confidence approach (B=1.449 p=0.004), seeking social support (B=1.796 p= 0.003) and perceived stress scale (B= −1.002 p=0.001) in the healthy control group (Table 3).
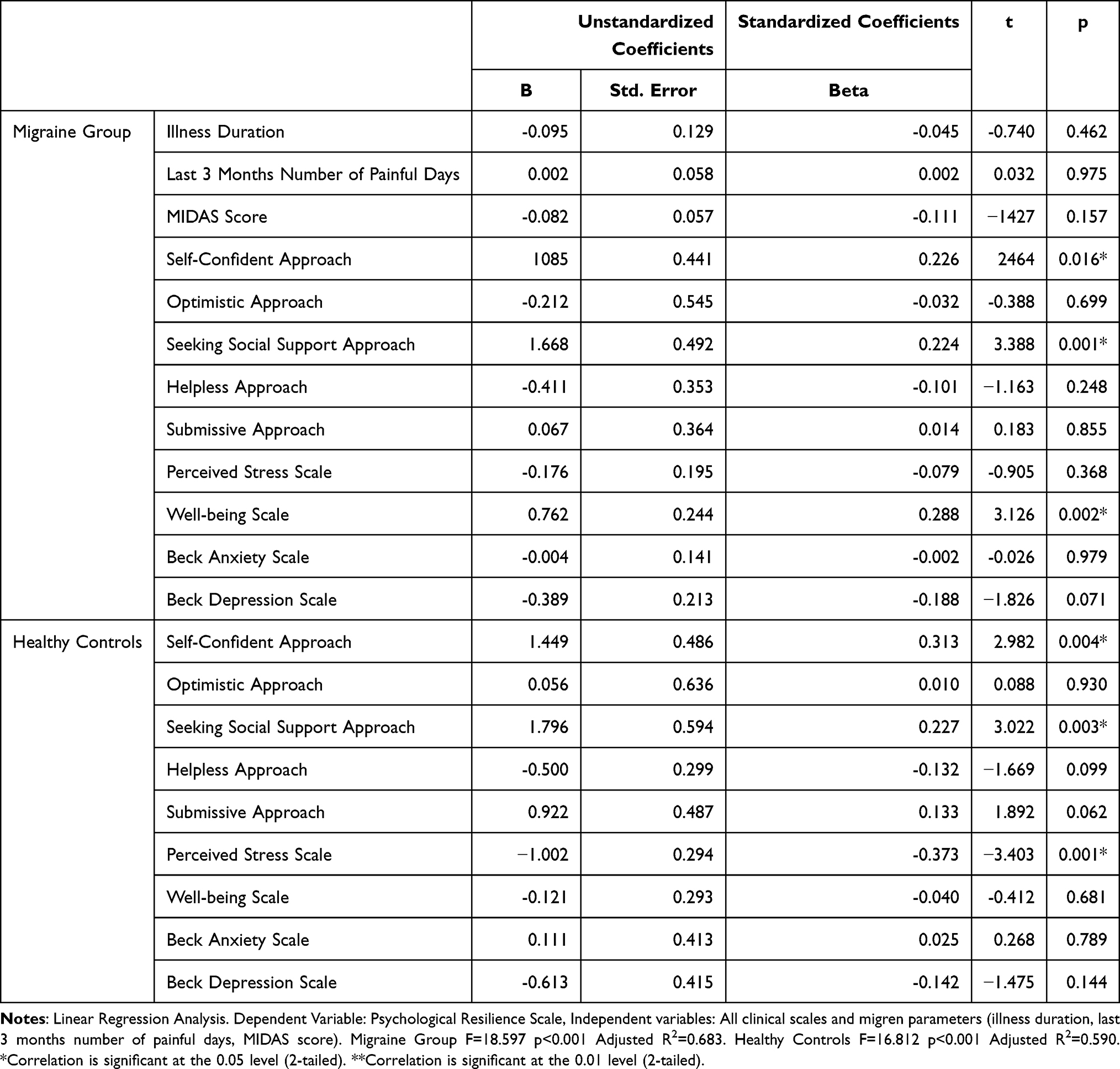 |
Table 3 Evaluation of Psychological Resilience in Groups with Regression Analysis |
Variable-mediated regression analysis was performed in the migraine group. As a result of the variable-mediated regression analysis shown in Figure 1, based on the calculation of β total=(βa x βb)+ βc, it was determined that 48.4% of the effect of the self-confident approach on resilience is an indirect effect through well-being, while 42.2% of the effect of the seeking social support approach on resilience was an indirect effect through well-being.
 |
Figure 1 Variable-mediated regression analysis in migraine group. (A) The mediation model for self-confident approach and resilience through well-being. (B) The mediation model for seeking social support and resilience through well-being. |
Discussion
In the current study, which aimed to evaluate psychological resilience and the factors affecting psychological resilience in migraine patients, it was determined that the level of psychological resilience in the migraine patients group was at lower levels compared to the healthy controls. In addition to this finding, it was observed that the level of perceived stress, depression, and anxiety levels were higher in migraine patients, and they preferred negative methods more commonly in their way of coping with stress. Interestingly, it was found that there was no difference in terms of psychological well-being levels between the migraine patients group and the healthy control group. While the predictors of resilience in migraine patients were self-confident approach, seeking social support approach, and psychological well-being, the predictors of resilience in healthy controls were self-confident approach, seeking social support approach and perceived stress level.
Resilience comes to the fore in the relationships between the psychological state as a result of stress, illness, and/or trauma and the desired/positive state. In other words, resilience is the ability to return back to the state before stress/illness/trauma or cope with difficulties. It is known that even the most resilient people experience bad mood, fatigue, insomnia, headache, and somatic symptoms not of organic origin when the limits of resilience to problems are exceeded.9 In addition, it is also known that many physical diseases are associated with resilience and that resilience is affected by genetics, environmental factors, past experiences, and coping mechanisms.30 Only a few studies have been found in the literature that investigates the relationship between headache and resilience. The common consensus of these studies is that in headaches, the analysis of the factors affecting resilience will contribute positively to the treatment.31,32 While the study by Kalapurakel et al suggested that acceptance of pain and pain self-adequacy would increase resilience, the study by Esmaeili et al found that acceptance and commitment therapy (ACT) performed on migraine patients increased the level of resilience.33 It is concluded that, in the studies with ACT, one of the factors affecting acceptance behavior is positive coping styles.32,34 Therefore, we think that our study results are supported by the results of these two studies. As a result of the study, it was observed that besides the positive stress coping styles, well-being also increased resilience in migraine group. In the healthy control group, however, psychological well-being did not predict resilience. This outcome leads us to think that psychological well-being is more crucial in the presence of illness. The level of resilience in healthy individuals is affected by the level of perceived stress. It is concluded that migraine is already a serious stress factor for the individual, therefore, the level of well-being of the individual affects resilience in the state of stress rather than stress itself. In other words, for resilience, it is important for an individual with migraine to stay well in the state of migraine rather than the stress caused by migraine. Another indicator of this condition is that the clinical parameters (duration of diagnosis, number of painful days in the last 3 months, MIDAS score scale) related to migraine as a stress factor, did not have any effect on resilience in the performed regression analysis. While there was no statistical difference between the groups in terms of well-being, when it was considered in terms of resilience, the well-being level of the migraine patients group was important. It was observed that the perceived stress level was one of the predictors of resilience in healthy controls who were not under any disease stress.
To summarize the findings of the study, the self-confident approach and the social support-seeking approach in patients with migraine have both direct effects and indirect effects on well-being that increase resilience. Behaviors of a migraine patient with a self-confident approach are acceptance of pain, “making room for pain” and active attempts to control pain. The idea that social support has critical importance in maintaining health and improving function is supported by many studies.35 Knowing that in individuals with headaches, the functionality that decreases in painful days will be compensated by other family members or the social environment will lead them to relax. For this reason, it is often recommended by studies that interventions aiming to improve social relations should be added to the treatment of headache.36 In our study, it was found that psychological resilience was inversely correlated with MIDAS score and the number of painful days in the last 3 months. This suggests that patients with high levels of resilience may be less affected by migraine. Supporting our findings, a recent two-year observational study suggested that social support, self-esteem (which is a concept intertwined with self-confidence), and resilience together are protective forces against diseases.37
Although it is thought that resilient individuals tend to be optimistic, in the current study, it was observed that the optimistic approach, which is one of the positive coping styles, was not among the factors affecting resilience. Also, although depression and anxiety levels were inversely correlated with resilience levels, the absence of regression analysis gave the impression that depression and anxiety were not included in the etiology of resilience, especially in migraine patients, and that depression and anxiety were observed as a result of frailty.
The study being a cross-sectional study, and the evaluation scales being self-reported scales are the limitations of the current study. However, the fact that the included sample group included only migraine patients, not patients with general headaches, that the measured psychological scales were multidimensional, and that many factors that could affect resilience were evaluated together are valuable aspects of the study. It is thought that psychotherapeutic interventions targeting stress-coping mechanisms will contribute to migraine treatment by increasing resilience. Follow-up studies carried out on this subject will shed light on the issue.
Conclusion
As a result, the level of psychological resilience in migraine patients is lower than in healthy controls. The best predictors of this condition in the current study are the stress coping styles used by the individual and the level of well-being. It is expected that with the increase in the resilience level, a decrease in the depression level, anxiety level, perceived stress level, the number of painful days in the last 3 months, and the MIDAS score and an increase in well-being are also expected. It is thought that follow-up studies on resilience will enlighten the subject.
Data Sharing Statement
Please contact the corresponding author for data request.
Acknowledgments
The authors would like to thank all patients and healthy volunteers who supported and participated in this study.
Funding
The authors report there is no funding associated with the work featured in this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Vos T, Abajobir AA, Abbafati C, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet. 2017;390(10100):1211–1259. doi:10.1016/S0140-6736(17)32154-2
2. van Staveren I. Migraine and stress—an exploratory cross-country study of external stress factors. BMC Res Notes. 2021;14:174. doi:10.1186/s13104-021-05587-8
3. Tietjen GE, Buse DC, Collins SA. Childhood maltreatment in the migraine patient. Curr Treat Options Neurol. 2016;18(7):31. doi:10.1007/s11940-016-0415-4
4. Eller-Smith OC, Nicol AL, Christianson JA. Potential mechanisms underlying centralized pain and emerging therapeutic interventions. Front Cell Neurosci. 2018;12:35. doi:10.3389/fncel.2018.00035
5. Pancheri C, Maraone A, Roselli V, et al. The role of stress and psychiatric comorbidities as targets of non-pharmacological therapeutic approaches for migraine. Riv Psichiatr. 2020;55(5):262–268. doi:10.1708/3457.34458
6. Sauro KM, Becker WJ. The stress and migraine interaction. Headache. 2009;49(9):1378–1386. doi:10.1111/j.1526-4610.2009.01486.x
7. Waliszewska-Prosół M, Nowakowska-Kotas M, Chojdak-łukasiewicz J, Budrewicz S. Migraine and sleep—an unexplained association? Int J Mol Sci. 2021;22(11):5539. doi:10.3390/ijms22115539
8. Luthar SS, Cicchetti D, Becker B. The construct of resilience: a critical evaluation and guidelines for future work. Child Dev. 2000;71(3):543–562. doi:10.1111/1467-8624.00164
9. Babic R, Babic M, Rastovi P, et al. Resilience in health and illness. Psychiatr Danub. 2020;32(2):226–232.
10. Sisto A, Vicinanza F, Campanozzi LL, Ricci G, Tartaglini D, Tambone V. Towards a transversal definition of psychological resilience: a literature review. Med. 2019;55(11):745. doi:10.3390/medicina55110745
11. Stacy M, Schulkin J. Suicide: allostatic regulation and resilience. Psychoneuroendocrinology. 2022;139:105691. doi:10.1016/j.psyneuen.2022.105691
12. Franjic D, Babic D, Marijanovic I, Martinac M. Association between resilience and quality of life in patients with colon cancer. Psychiatr Danub. 2021;33(13):297–303.
13. Friborg O, Hjemdal O, Rosenvinge JH, Martinussen M. A new rating scale for adult resilience: what are the central protective resources behind healthy adjustment? Int J Methods Psychiatr Res. 2003;12(2):65–76. doi:10.1002/mpr.143
14. Carver CS, Scheier MF, Weintraub KJ. Assessing coping strategies: a theoretically based approach. J Pers Soc Psychol. 1989;56(2):267–283. doi:10.1037/0022-3514.56.2.267
15. Mayordomo T, Viguer P, Sales A, Satorres E, Meléndez JC. Resilience and coping as predictors of well-being in adults. J Psychol Interdiscip Appl. 2016;150(7):809–821. doi:10.1080/00223980.2016.1203276
16. Petrovics-Balog A, Majláth Z, Lukács M, et al. The effect of psychiatric comorbidities and stress-coping strategies on perceived quality of life in migraine. Ideggyogy Sz. 2019;72(11–12):397–404. doi:10.18071/isz.72.0397
17. Beck AT, Epstein N, Brown G, Steer RA. An inventory for measuring clinical anxiety: psychometric properties. J Consult Clin Psychol. 1988;56:893–897. doi:10.1037//0022-006x.56.6.893
18. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An Inventory for Measuring Depression. Arch Gen Psychiatry. 1961;4:561–571. doi:10.1001/archpsyc.1961.01710120031004
19. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24(4):385–996. doi:10.2307/2136404
20. Folkman S, Lazarus RS. An analysis of coping in a middle-aged community sample. J Health Soc Behav. 1980;21(3):219–239. doi:10.2307/2136617
21. Diener E, Wirtz D, Tov W, et al. New well-being measures: short scales to assess flourishing and positive and negative feelings. Soc Indic Res. 2010;97:143–156. doi:10.1007/s11205-009-9493-y
22. Stewart WF, Lipton RB, Kolodner KB, Sawyer J, Lee C, Liberman JN. Validity of the Migraine Disability Assessment (MIDAS) score in comparison to a diary-based measure in a population sample of migraine sufferers. Pain. 2000;88:41–52. doi:10.1016/S0304-3959(00)00305-5
23. Ulusoy M, Sahin NH, Erkmen H. Turkish version of the Beck Anxiety Inventory: psychometric properties. J Cogn Psychother an Int Q. 1998;12(2):163–172.
24. Hisli N. Beck Depresyon Envanterinin üniversite öğrencileri için geçerliği, güvenirliği [Depression Inventory for university students-Turkish version]. Psikol Derg. 1989;7(23):3–13.
25. Basim HN, Çetin F. Yetişkinler için psikolojik dayaniklilik ölçeği’nin guvenilirlik ve geçerlilik çalişmasi. = The reliability and validity of the resilience scale for adults-Turkish version. Türk Psikiyatr Derg. 2011;22(2):104–114.
26. Eskin M, Harlak H, Demirkıran F, Dereboy Ç. Algilanan stres ölçeğinin türkçeye uyarlanmasi: güvenirlik ve geçerlik analizi [The adaptation of the Perceived Stress Scale into Turkish: A reliability and validity analysis- Turkish version]. Yeni Symp. 2013;51(3):132–140.
27. Şahin NH, Durak A. Stresle Başa Çıkma Tarzları Ölçeği: Üniversite öğrencileri için uyarlanması [A brief of coping styles inventory for university students-Turkish version]. Psikol Derg. 1995;10(34):56–73.
28. Telef BB. Psikolojik İyi Oluş Ölçeği: Türkçeye Uyarlama, Geçerlik ve Güvenirlik Çalışması [The Adaptation of Psychological Well-Being into Turkish: a Validity and Reliability Study-Turkish version]. J Educ. 2013;28(3):374–384.
29. Ertaş M, Siva A, Dalkara T, et al. Validity and reliability of the Turkish migraine disability assessment (MIDAS) questionnaire. Headache. 2004;44(8):786–793. doi:10.1111/j.1526-4610.2004.04146.x
30. Stewart DE, Yuen T, Systematic A. Review of resilience in the physically Ill. Psychosomatics. 2011;52(3):199–209. doi:10.1016/j.psym.2011.01.036
31. Kalapurakkel S, Carpino EA, Lebel A, Simons LE. “pain can’t stop Me”: examining pain self-efficacy and acceptance as resilience processes among youth with chronic headache. J Pediatr Psychol. 2015;40(9):926–933. doi:10.1093/jpepsy/jsu091
32. Stonnington CM, Kothari DJ, Davis MC. Understanding and promoting resiliency in patients with chronic headache. Curr Neurol Neurosci Rep. 2016;16(1):6. doi:10.1007/s11910-015-0609-2
33. Esmaeili N, Asgari P, Khorami N, Bakhtiarpour S. Effectiveness of acceptance and commitment therapy on perfectionism and resilience in migraine patients. Int Arch Heal Sci. 2021;8(3):138–142. doi:10.4103/iahs.iahs_115_20
34. Shayeghian Z, Hassanabadi H, Aguilar-Vafaie ME, Amiri P, Besharat MA. A randomized controlled trial of acceptance and commitment therapy for type 2 diabetes management: the moderating role of coping styles. PLoS One. 2016;11(12):e0166599. doi:10.1371/journal.pone.0166599
35. Ozbay F, Fitterling H, Charney D, Southwick S. Social support and resilience to stress across the life span: a neurobiologic framework. Curr Psychiatry Rep. 2008;10(4):304–310. doi:10.1007/s11920-008-0049-7
36. Zautra AJ, Infurna FJ, Zautra EK, Gallardo CÉ, Velasco L. The humanization of social relations: nourishment for resilience in midlife. Emotion Aging Health. 2016;207–227. doi:10.1037/14857-011
37. Liu Q, Jiang M, Li S, Yang Y. Social support, resilience, and self-esteem protect against common mental health problems in early adolescence A nonrecursive analysis from a two-year longitudinal study. Med. 2021;100(4):e24334. doi:10.1097/MD.0000000000024334
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.