Back to Journals » Journal of Pain Research » Volume 18
Psycho-Socio-Behavioural Substrates of Non-Cancer Chronic Pain: A Twin Study in Italian Adults
Authors Fagnani C ![]() , Toccaceli V, Tenti M
, Toccaceli V, Tenti M ![]() , Medda E, Ferri M, Raffaeli W
, Medda E, Ferri M, Raffaeli W ![]()
Received 28 March 2025
Accepted for publication 29 July 2025
Published 15 October 2025 Volume 2025:18 Pages 5429—5440
DOI https://doi.org/10.2147/JPR.S530951
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Jonathan Greenberg
Corrado Fagnani,1 Virgilia Toccaceli,1 Michael Tenti,2 Emanuela Medda,1 Maurizio Ferri,1 William Raffaeli2
1Centre for Behavioural Sciences and Mental Health, Istituto Superiore Di Sanità, Rome, Italy; 2ISAL Foundation, Institute for Research on Pain, Rimini, Italy
Correspondence: Corrado Fagnani, Centre for Behavioural Sciences and Mental Health, Istituto Superiore di Sanità, Viale Regina Elena 299, Rome, 00161, Italy, Email [email protected]
Background: Chronic pain (CP) is a debilitating condition characterized by pain lasting longer than three months, significantly impairing physical, emotional, and social functioning. Comorbidities such as depression can exacerbate the severity and persistence of CP, leading to greater functional impairment and diminished quality of life. Characterizing the psycho-socio-behavioural substrates of CP is crucial for improving treatment and prevention strategies based on multidisciplinary approaches.
Methods: The study sample included 750 monozygotic (MZ) and dizygotic (DZ) twin pairs aged 18– 82 years, enrolled in the Italian Twin Registry. Non-cancer CP-related characteristics (ie, CP occurrence, intensity and body location) as well as depressive symptomatology, sleep quality and perceived social support were assessed by validated self-report questionnaires. The twin study methodology was applied to control for genetic and shared environmental confounding while estimating the association of CP with psycho-socio-behavioural variables.
Data Analysis: Individual-level and intrapair-level regression were used to estimate the association of CP with psycho-socio-behavioural variables. Biometrical structural equation modelling and mediation analysis were performed to shed light on the etiological mechanisms underlying this association.
Results: As regards CP and depressive symptomatology, individual-level association in the total sample of twins and intrapair-level associations in MZ and DZ pairs discordant for CP were all significant and of similar magnitudes, possibly consistent with a quasi-causal relationship. Under the best-fitting biometrical structural equation model, unique environmental factors explained 73% (95% CI: 19– 100%) of phenotypic correlation between CP and depressive symptoms. Life satisfaction and sleep quality resulted to mediate the association between CP and depression, with a global indirect effect from CP to depression of 0.32 (0.22– 0.44).
Conclusion: This study provides insights into the relationship of CP with depression, suggesting a quasi-causal connection between them, an important contribution of unique environmental factors in this connection, and a mediating role of sleep quality and subjective wellbeing.
Keywords: chronic pain, psychosocial correlates, twins, causality, mediation
Introduction
Chronic pain (CP) is a pervasive and debilitating condition characterized by pain lasting longer than three months,1 significantly impairing physical, emotional, and social functioning.2,3 It is a major public health concern globally, leading to substantial personal suffering and socioeconomic costs.2,4,5 While the etiology of CP is multifaceted, involving complex interactions between genetic, environmental, and psychological factors, the precise mechanisms remain not completely understood.6
Comorbidities such as depression and sleep disturbances can exacerbate the severity and persistence of CP, leading to greater functional impairment and diminished quality of life, or complicating the management of the condition.
Depression, in particular, is one of the most common CP-associated comorbidities. The 2019 European Health Interview survey conducted in Italy on a representative sample of the general population has estimated a prevalence of around 11% of diagnosed depression in non-cancer CP-affected adult subjects compared to around 2% in CP-free subjects.7 The CP-depression comorbidity arises from several factors, and shared neurobiological mechanisms, including neurotransmitter imbalances, maladaptive neuroplasticity, and inflammatory dysfunction, may play a relevant role.8 Moreover, different studies suggest that it complicates diagnosis, treatment, and prognosis of both the conditions.9–12
In this regard, a particularly important syndrome that may be worth mentioning here is fibromyalgia, a complex and still poorly understood pain disorder mainly characterized by widespread pain, chronic fatigue, and sleep disturbance, occurring in a non-negligible percentage of the general population (2–4%). Fibromyalgia patients are at increased risk for a lifetime history of depression compared to other chronic pain patients, and this comorbidity has shown to be an obstacle in improving pain intensity.13–15
Sleep problems represent another frequently occurring comorbidity alongside CP. Studies found that from 50% up to 88% of people experiencing CP struggle with sleep difficulties.16 Individuals experiencing both CP and sleep disturbances tend to have more severe and longer-lasting symptoms, increased disability, and additional comorbid conditions, such as depression, anxiety, and suicidality.17
Evidence suggests that CP and depression, as well as CP and sleep disturbances, affect each other. In fact, sleep disturbances or depression can predict changes in pain levels, while changes in pain can affect sleep or depression.18–21
CP, depression, and sleep disturbances can frequently co-occur. In patients with chronic musculoskeletal pain, Wilson et al22 found that these conditions co-occur in 26.5% of the sample.
Interrelationships among the three conditions have also been documented, but possible causal orders for these relationships are difficult to elucidate,23–26 considering as well that other factors can mediate the relationships.27,28
A better understanding of the interrelations between CP, depression, and sleep disturbances, in particular the heritable components and environmental factors involved in such interrelationships, might be crucial for developing effective interventions and support systems.
Twin studies offer a unique and powerful method to disentangle the genetic and environmental influences on complex traits and conditions. By comparing monozygotic (MZ) twins, who share nearly 100% of their genetic material, with dizygotic (DZ) twins, who share approximately 50% of their segregating genes, researchers can estimate the heritability of specific traits and conditions. Moreover, this approach may be particularly suitable to help to understand the interplay between different correlated outcomes.
To the best of our knowledge, no studies so far have explored the relationship between CP, depression, sleep quality and other psychosocial factors that may mediate these relationships within a single twin study. For instance, social support has been found to mediate the relationship between pain and depressive symptoms in osteoarthritis patients,27 and increased social support is found to be associated with lower sleep problems and pain severity in chronic low back pain patients.29 In a longitudinal study on patients with and without chronic pain at baseline, life satisfaction at baseline was associated with lower severe pain at follow-up compared to participants with severe distress and not satisfied with life.30 Moreover, in patients with chronic pain related to spinal cord injury,28 life satisfaction fully mediates the relationship between pain intensity and depression. The association of depression and sleep quality with acute pain has already been explored in a community sample of twins,31 and it has been found that the pattern of genetic and non-shared environmental correlations was compatible with potential causality between sleep quality and pain, and between sleep and depression, but not between pain and depression.
Therefore, the present study applies a twin design to unravel the mechanisms underlying the relationship of CP with depression, sleep quality, satisfaction with life, and social support, using a sample of adult Italian twins drawn from the population-based Italian Twin Registry (ITR).
Specifically, the objective of the present study is twofold: (i) to estimate the association of CP with the specific psycho-socio-behavioural variables listed above, while taking into account confounding effects due to genetic and shared familial environmental factors; (ii) to explore the pathways that might underlie the observed associations between CP and the targeted psycho-socio-behavioural variables, and particularly, possible direct or mediated causal relationships.
The findings of this study have the potential to offer insights into the shared and unique etiological pathways of these complex factors, providing a foundation for more targeted and effective therapeutic approaches.
Material and Methods
Recruitment of Study Sample
In February 2020, a nationwide online survey on CP, based on the LimeSurvey Professional Platform (LimeSurvey GmbH, Hamburg, Germany) was conducted on around 6000 adult twins of Caucasian origin, previously enrolled in the population-based ITR. To date, more than 30,000 twins of all ages and geographical areas joined the ITR and were assessed for socio-demographic and health characteristics, including behavioural and mental health traits.32 Detailed information on the survey procedures and tools can be found elsewhere.33
Study Measures
Zygosity Assessment
Twin pairs were classified as MZ or DZ based on a standard algorithm including questions on physical similarity of the twins during childhood. This method for zygosity assessment is well-established in twin studies and is generally over 95% accurate.
CP Assessment
CP occurrence and intensity were assessed by the Brief Five-Item Chronic Pain Questionnaire, previously validated by our group in a representative sample of the Italian general population.34 More precisely, CP occurrence was identified as a pain status persisting for more than three months, according to the IASP definition,1 and was therefore described by a binary variable (1=yes, 0=no); CP intensity was initially evaluated on a 6-point Likert scale (no pain, very mild, mild, moderate, severe, very severe), but for analytical purposes, the “very mild” and “very severe” categories were subsequently combined with the “mild” and “severe” ones respectively, due to low numbers; indeed, only 13 subjects (3.6%) and 6 subjects (1.7%) reported very mild and very severe pain intensity, respectively (see first report).33 CP body location was assessed by a 70-site map encompassing 35 frontal sites and as many corresponding posterior sites; based on this map, the total number of sites affected by CP was first calculated and then transformed into an ordinal variable (0, 1–2, 3+ sites). This body map allows detailed quantification of pain distribution across multiple anatomical regions, and was previously used by our group in a population-based twin study on chronic pain in Italy.33 Similar approaches have been adopted in previous twin studies investigating the heritability of chronic widespread pain. For instance, Kato et al,35 Burri et al,36 and Markkula et al37 used the American College of Rheumatology (ACR) criteria or similar region-based body maps to define CP phenotypes and reported comparable heritability estimates ranging from 51% to 58%. These findings suggest that the number of painful body regions—regardless of a specific anatomical location—might be a meaningful indicator of pain chronicity and centralization, and supports the validity of using body maps in genetically informed CP research.38
Psycho-Socio-Behavioural Factors’ Assessment
The following psychological, social, and behavioural variables were considered in this study: (i) subjective wellbeing, assessed by the Satisfaction with Life Scale (SWLS)39 (5 items on a 7-point Likert scale from 1 to 7, total score range: 5–35, higher scores indicate higher wellbeing); (ii) depressive symptomatology, assessed by the 2-item Patient Health Questionnaire (PHQ-2)40 (2 items on a 4-point Likert scale from 0 to 3, total score range: 0–6, higher scores indicate worse symptomatology; a score of 3 is sometimes used as a cut-off value for pre-screening of depression); (iii) social support, assessed by the 3-item Oslo Social Support Scale (OSSS-3)41 (1 item on a 4-point Likert scale from 1 to 4 and 2 items on a 5-point Likert scale from 1 to 5, total score range: 3–14, higher scores indicate stronger social support); (iv) sleep quality, assessed by the Pittsburgh Sleep Quality Index (PSQI)42 (19 items grouped into 7 components each ranging from 0 to 3, total score range: 0–21, higher scores indicate worse sleep quality). Cronbach’s alpha values in the current sample were 0.88 for SWLS, 0.52 for OSSS-3, and 0.71 for PSQI. Internal consistency was not calculated for PHQ-2; indeed, Cronbach’s alpha statistic is generally not recommended or considered meaningful with only two items, and it is heavily influenced by the number of items, as also shown by the lower alpha value obtained for the social support scale, based on 3 items.
Statistical Methods
All statistical analyses described below were performed with the Stata software version 16 (StataCorp LLC, College Station, TX, USA), with the exception of biometrical modelling that was carried out using the OpenMx package in R.43 As detailed in the appropriate sections, only individual age was considered as a covariate in statistical modelling since it played a significant role in every model, while sex contribution was negligible at all levels of analysis; furthermore, in order to avoid over-adjustment bias in the analysis of the association between CP and psycho-socio-behavioural factors, these factors were not adjusted for in the modelling as they were hypothesized to play a mediating role in the association under study.
Sample Description
Descriptive statistics in terms of means (with standard deviations and ranges) and percentages for socio-demographic and CP characteristics were calculated and are available from a previous report by our group, being the present study sample exactly the same as that considered in our first report.33
Association of CP Characteristics with Psycho-Socio-Behavioural Factors
To investigate if CP characteristics could be associated to psychosocial and behavioural factors, we first considered twins as individual subjects and then exploited the pair-matched nature of twin data.
Individual-Level Association
In the individual-level analysis, linear regression models were fitted to each psycho-socio-behavioural factor as continuous response variable predicted by each CP-related variable, adjusting by age and using robust standard errors estimation to take account of the non-independence of data within twin pairs. For visual inspection of emerging associations, predictive margins of the regression models were estimated and plotted.
Intrapair-Level Association
In the intrapair-level analysis, pairs of twins that were “discordant” for CP occurrence (ie, one pair member reported CP while the other did not) were stratified by zygosity (MZ or DZ) and were analysed as case-control dyads by conditional logistic regression to assess association of CP with each psycho-social/behavioural factor. Intrapair-level associations were then compared to individual-level ones to evaluate genetic/environmental confounding and infer possible causality. Briefly, if individual-level and intrapair-level associations are all significant and of similar magnitudes, then genetic and environmental confounding are unlikely to come into play and a “quasi-causal” relationship can be hypothesized.44
Biometrical Structural Equation Modelling
Biometrical structural equation models in bivariate versions (with CP as a binary variable and psycho-socio-behavioural factors as continuous variables) and including age as a covariate were used to explore genetic and environmental overlap between CP occurrence and those psycho-socio-behavioural factors for which a quasi-causal link with CP was suggested from previous association analyses. These models allow decomposing the variance of each trait and the covariance between them into contributions due to latent additive genetic (A), either non-additive genetic (D) or shared (familial) environmental (C), and unique (individual-specific) environmental (E) sources. The A source represents the additive effects of all gene variants (ie, alleles) that influence the trait, without interactive effects; the D source represents interactions between alleles at the same fixed chromosomal site (ie, locus) (“dominance”) or at different loci (“epistasis”); the C source represents the effects of environmental factors that are shared by the twins within the family (eg, rearing environment, family socio-economic status, parental behaviours, etc.) or in the womb (eg, hormonal exposures); the E source represents the effects of environmental factors that are unique to an individual (eg, lifestyles, relations with peers, infections, etc)., including measurement error. Only three of these four variance/covariance components can be simultaneously estimated because C and D components are confounded when analyzing data from MZ and DZ twins reared together.45 Therefore, a full ACE model was fitted, and it was then compared with the more parsimonious AE model by using the Akaike Information Criterion (AIC). Parameter estimates were reported under the best-fitting model, namely the one with a lower AIC value.
Mediation Analysis
A mediation model further refining the possible quasi-causal link between CP occurrence and specific psycho-socio-behavioural factors was fitted following the regression-based steps recommended by Baron and Kenny46 and including age as a covariate. When significant evidence for mediation emerged, total effect was decomposed into the sum of direct and indirect effect, and confidence intervals for indirect effect was estimated by a bootstrap procedure with 5000 replicates.
Results
Study Participants
Among the 6000 invited twins, 3258 replied to the online survey (response rate 54%); these included 762 intact pairs, plus 1734 unmatched twins. All intact pairs were used for sample description, while subsequent analyses were based on 750 pairs, after excluding twins with unknown zygosity or cancer-related CP.
Sample Description
The main socio-demographic and CP-related characteristics are summarized in our previous report.33 Briefly, the study sample was aged 39 years on average (age range: 18–82 years), and included 34% of males and 57% of MZ twins. CP prevalence was 24.1% (24.4% males, 23.9% females), with 17.8% of CP-affected subjects reporting a severe (16.1%) or very severe (1.7%) pain condition. As regards the causes of pain, “trauma without surgery” and “an illness diagnosed by a doctor” were the most frequently reported origins (39.8% and 35.2%, respectively). As a novel information not reported in our previous work, CP body location was available for 98.9% of CP-affected subjects; for 11.6% of these, pain was localized in only one body site, for 30% in two sites, and for 58.4% in at least three sites. Mean values of the psycho-socio-behavioural factors were 24.8 for SWLS (24.9 males, 24.7 females), 1.2 for PHQ-2 (1.2 males, 1.3 females), 9.8 for OSSS-3 (9.8 males, 9.8 females), and 5.5 for PSQI (5.1 males, 5.7 females).
Association of CP Characteristics with Psycho-Socio-Behavioural Factors
As regards individual-level association analysis, Figures 1–3, and Supplementary Figures S1–S6 show the predictive margins of the regression models of each psycho-socio-behavioural factor on each CP-related variable. Graphs for social support were not reported due to the lack of clear trends. For the other factors, compared to CP absence: (i) SWLS score significantly decreased with CP occurrence, with a moderate or severe/very severe CP intensity, or with more than three involved body sites; (ii) PHQ-2 score significantly increased with CP occurrence, with any CP intensity level, or with any number of involved body sites; (iii) OSSS-3 score was significantly reduced, only for females, in the presence of CP or in case of more than 3 body sites affected (graphs not reported); (iv) PSQI score was significantly higher in the presence of CP, as well as in case of a moderate or severe/very severe CP intensity, or with more than 3 affected body sites.
 |
Figure 1 Predictive margins of regression models of satisfaction with life on chronic pain occurrence. Abbreviations: CP, chronic pain; SWLS, satisfaction with life scale. Note: *Significant difference compared to base category (ie, no chronic pain). |
 |
Figure 2 Predictive margins of regression models of satisfaction with life on chronic pain intensity. Abbreviations: CP, chronic pain; SWLS, satisfaction with life scale. Note: *Significant difference compared to base category (ie, no chronic pain). |
 |
Figure 3 Predictive margins of regression models of satisfaction with life scale on chronic pain body sites. Abbreviations: CP, chronic pain; SWLS, satisfaction with life scale. Note: *Significant difference compared to base category (ie, no chronic pain). |
As regards intrapair-level association analysis, Table 1 shows the odds ratios estimated by conditional logistic regression of CP occurrence on each psycho-socio-behavioural factor, considering MZ and DZ twin pairs discordant for CP. The odds ratios obtained by standard logistic regression in the total sample of individual twins are also reported in the same table. Among all the psycho-socio-behavioural factors considered, only for PHQ-2, individual-level association (not adjusted for genetic and familial confounding) and intrapair-level association in MZ (totally adjusted for genetic and familial confounding) and DZ discordant pairs (partially adjusted for genetic confounding and totally adjusted for familial confounding) were all significant and of similar magnitudes, possibly consistent with a quasi-causal relationship between CP and depression symptomatology.
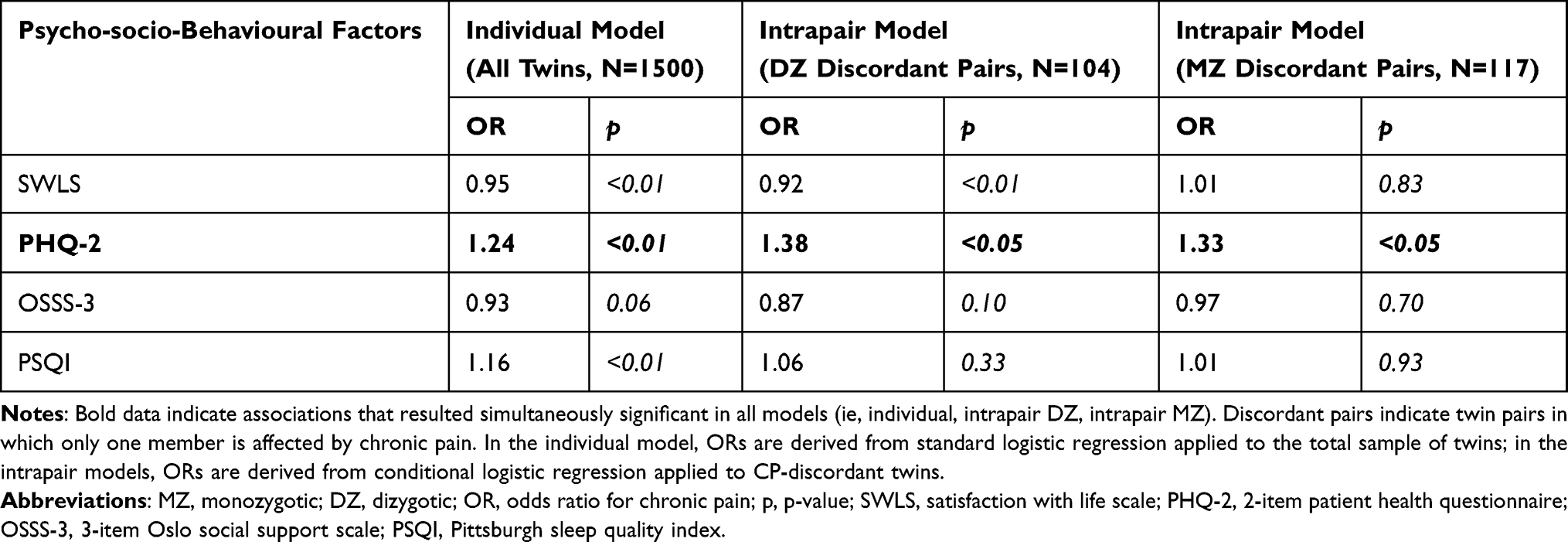 |
Table 1 Individual- and Intrapair-Level Associations of Chronic Pain with Psycho-Socio-Behavioural Factors |
Biometrical Structural Equation Modelling
The comparison between the full ACE and the reduced AE model supported the latter model as the one providing a better balance between goodness of fit and parsimony based on the AIC index (ACE model: AIC=6613.46; AE model: AIC=6611.44); furthermore, the likelihood-ratio test for nested models showed that the C component was not significant (p=0.26). Therefore, the AE parameterization was retained as the best-fitting model. This was in agreement with twin correlations’ estimates in MZ [CP: rMZ=0.38 (95% CI 0.28–0.48), PHQ-2: rMZ=0.28 (0.22–0.34)] and DZ pairs [CP: rDZ=0.00 (−0.11–0.11), PHQ-2: rDZ=0.09 (0.03–0.15)], which did not provide any support for shared environmental effects on the study variables.45 The best-fitting age-adjusted bivariate AE model for CP (as a binary variable) and PHQ-2 (as a continuous variable) provided heritability estimates of 0.33 (95% CI 0.17–0.47) and 0.27 (0.18–0.35) for CP and PHQ-2 respectively, with the remaining proportions of variance explained by unique environmental factors. The phenotypic correlation between CP and PHQ-2 [0.16 (0.12–0.20)] was mainly due to overlapping unique environmental factors [73% (19–100%)], with a lower yet still sizeable genetic contribution [27% (0–81%)].
Mediation Analysis
Figure 4 shows the mediation model for the possible quasi-causal link between CP and depression symptomatology. Results are presented assuming a cascade mechanism from CP to depression, but the inverse model could also be hypothesized. Both life satisfaction and sleep quality resulted to mediate the association between CP and depressive symptoms, with an estimated global indirect effect of 0.32 (0.22–0.44) comprising indirect effects of 0.12 (0.06–0.19) via life satisfaction and of 0.20 (0.12–0.26) via sleep quality. Under the inverse model, the global indirect effect of depressive symptoms on CP was 0.15 (0.09–0.22), with a life satisfaction-mediated component of 0.04 (0.00–0.09) and a sleep quality-mediated component of 0.11 (0.06–0.16).
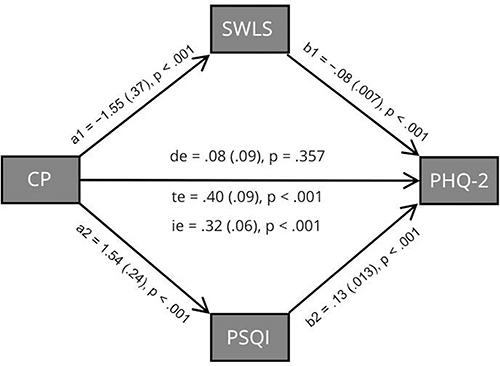 |
Figure 4 Mediation model for the link between chronic pain and depression symptomatology. Abbreviations: CP, chronic pain; SWLS, satisfaction with life scale; PHQ-2, 2-item patient health questionnaire; PSQI, Pittsburgh sleep quality index; a1, a2, b1, b2 unstandardized age-adjusted regression coefficients; p, p-value; te, total effect; de, direct effect; ie, indirect effect. Note: Standard errors of estimates are reported in parentheses. |
Discussion
The main finding of our study is the support for the hypothesis that a quasi-causal relationship may exist between CP and depressive symptoms. Causal inference on this relationship was made possible by the twin study design we used. This unique observational design mimics the well-known advantage of experimental strategies to allow control over unobserved genetic and shared familial confounding while estimating the association between traits. In particular, we found that the association between CP and depressive symptoms remained significant and of similar magnitude both in twins as individual subjects and within MZ and DZ discordant pairs; therefore, the association resulted robust to adjustment for the latent effect of innate and acquired factors that might simultaneously impact on CP and depressive symptoms, being consistent with at least partial causality. Moreover, results argue in favor of unique environmental factors mainly contributing to the CP-depression relationship, with a weaker role of shared genetic effects. Our results are only partially in line with two previous twin studies on different pain phenotypes,31,47 that found a somewhat higher correlation between pain and depression, as well as a substantially larger role of genetic factors in explaining this correlation.
Though very powerful, the discordant-twin design in its cross-sectional version still suffers from the limitation of not being able to conclusively unravel the directionality question, thus leaving doubt on which comes first between CP and depressive symptomatology. In this respect, longitudinal data on discordant twin pairs would represent a maximally informative resource.
Nevertheless, not only a bidirectional association between CP and depression is well-recognized in the literature,20,21,48 but also a “differential causality” was suggested,49 where CP might be a primary causal factor in some individuals, while depression may precede and amplify pain in others.
Given these premises, it is important to understand which mechanisms or factors contribute to the development of one condition when the other is already present, and vice versa.
Our mediation analyses suggested that the effect of CP on depressive symptoms might be fully and indirectly expressed through an impairment of sleep quality and a reduced level of subjective wellbeing as measured by life satisfaction, confirming various literature findings. Several studies have already found that sleep quality mediates the relationship between pain intensity and symptoms of depression.25,26,50,51 A recent meta-analysis of cohort and case-control studies found that sleep disturbance partially mediates the association between depression and pain intensity.52 For what concerns life satisfaction, in a longitudinal study on patients with and without CP at baseline, life satisfaction at baseline was associated with lower severe pain at follow-up, compared to participants with severe distress and not satisfied with life.30 Moreover, life satisfaction fully mediated the relationship between pain intensity and depression in patients with CP related to spinal cord injury.28
It is important to underline, in this framework, that several psychosocial variables, other than sleep and wellbeing, such as catastrophizing53,54 or self-efficacy,55,56 might affect the link from CP to depression and vice versa. Therefore, the evidence of a significant contribution of sleep and wellbeing emerging from our findings may help shaping the borders for a role of these additional factors in mediating the CP-depression comorbidity.
As it is now well-known, intervention strategies in this area require an integrated approach where each involved factor has to be addressed taking into account all the others. The findings of this study have important clinical implications, as they highlight the key role of modifiable factors—specifically, sleep quality and life satisfaction—in mediating the relationship between CP and depression. Addressing these factors may enhance treatment outcomes by reducing depressive symptoms associated with CP. Consistent with our results, a recent meta-analysis demonstrated that cognitive behavioral therapy for insomnia (CBT-I) significantly improves both pain and depressive symptoms in patients with CP and comorbid insomnia.57 Additionally, interventions grounded in positive psychology, which aim to foster life satisfaction and emotional well-being, have been shown to significantly alleviate pain intensity and depressive symptoms.58 These findings underscore the potential benefits of incorporating sleep-focused and well-being-enhancing strategies into multidisciplinary pain management programs.
Our findings should be interpreted with caution, due to some study weaknesses. One limitation is the sample size, that did not allow us to test for sex or age differences not only in genetic and environmental contributions to CP-depression comorbidity, but also in mediating effects. In particular, as some pain conditions and psychological vulnerabilities may vary significantly across the lifespan, future studies could explore age-specific patterns more thoroughly. In addition, other variables as occupational impairment, economic burden, or perceived treatments effectiveness could be considered in future studies as potentially important confounding or moderating variables in structural equation modelling and mediation analysis, examining the interplay between chronic pain, depression, and other psychosocial outcomes. Another limitation is the cross-sectional design with simultaneous assessment of exposure and outcome variables; this left open questions about the link between CP and depression, especially with respect to directionality and to whether the estimated effects reflect a long-term or a transient association. As an additional issue, study variables may have been affected by the self-report nature of collected data. Although the present study focused on the psycho-socio-behavioural substrates of CP as a general and heterogeneous condition in the adult population, future investigations may benefit from targeting specific CP conditions such as fibromyalgia or chronic fatigue syndrome that have shown complex psychological and genetic correlates in previous research,37,59 to better elucidate their unique psycho-socio-behavioural profiles. Furthermore, given the wide age range of the twin sample, spanning from young adulthood to elderly, shared environmental influences could not be reliably tested, and gene–environment interactions likely affected our results.
Conclusion
This study provides valuable insights into the relationship between CP and depression, suggesting a potential quasi-causal connection between the two conditions, an important role of modifiable individual-specific factors (including but not limited to lifestyle-related factors) in this connection, and possible mediating effects of sleep quality and subjective wellbeing. These results should be interpreted with caution and need to be replicated in subsequent studies using alternative designs and statistical approaches, and taking pain intensity into account, preferably based on a numerical rating scale assessment. Understanding the CP-depression link is crucial for improving both treatment and prevention strategies, as addressing one condition may help mitigate the other. A multidisciplinary approach integrating pain management, psychological interventions, and other therapeutic modalities can significantly enhance the quality of life for individuals suffering from both CP and depression. This comprehensive approach is critical for providing more effective and holistic care to patients dealing with these interconnected and severe conditions.
Data Sharing Statement
The original data are electronically stored at the Istituto Superiore di Sanità and they will be made available upon reasonable request to the corresponding author.
Ethic Statement
Informed consent was obtained from all subjects involved in the study. The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Board of the Istituto Superiore di Sanità (protocol code: AOOISS 14/04/2020 0013349; date of approval: 14 April 2020).
Acknowledgments
The authors would like to thank all the twins who participated in the online survey. Furthermore, they would like to acknowledge Cristina D’Ippolito for her skillful assistance in data management and Miriam Salemi for her valuable contribution to the engagement of the twins through social media.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funds, grants, or other supports were received for conducting the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Treede RD, Rief W, Barke A, et al. A classification of chronic pain for ICD-11. Pain. 2015;156(6):1003–1007. doi:10.1097/j.pain.0000000000000160
2. Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. Lancet. 2021;397(10289):2082–2097. doi:10.1016/S0140-6736(21)00393-7
3. Dueñas M, Ojeda B, Salazar A, Mico JA, Failde I. A review of chronic pain impact on patients, their social environment and the health care system. J Pain Res. 2016;9:457–467. doi:10.2147/JPR.S105892
4. Breivik H, Eisenberg E, T O. OPENMinds. The individual and societal burden of chronic pain in Europe: the case for strategic prioritisation and action to improve knowledge and availability of appropriate care. BMC Public Health. 2013;13:1229. doi:10.1186/1471-2458-13-12290
5. Smith TJ, Hillner BE. The cost of pain. JAMA Network Open. 2019;2(4):e191532. doi:10.1001/jamanetworkopen.2019.1532
6. Gatchel RJ, Haggard R, Thomas C, Howard KJ. Biopsychosocial approaches to understanding chronic pain and disability. In: Moore RJ, editor. Handbook of Pain and Palliative Care: Biopsychosocial and Environmental Approaches for the Life Course. New York: Springer; 2018:3–22.
7. Maraschini A, Tenti M, Raffaeli W, et al. Chronic pain in Italy: prevalence and psychosocial burden in the adult population. Results from the European health interview survey, 2019. BMC Public Health. 2025; 25. in publication. doi:10.1186/s12889-025-22997-6
8. Sheng J, Liu S, Wang Y, Cui R, Zhang X. The link between depression and chronic pain: neural mechanisms in the brain. Neural Plast. 2017;2017:9724371. doi:10.1155/2017/9724371
9. Worz R. Pain in depression, depression in pain. Pain. 2003;11:5.
10. Ohayon MM.Specific characteristics of the pain/depression association in the general population. J Clin Psychiatry. 2004;65(Suppl 12):5–9.
11. Arnow BA, Hunkeler EM, Blasey CM, et al. Comorbid depression, chronic pain, and disability in primary care. Psychosom Med. 2006;68(2):262–268. doi:10.1097/01.psy.0000204851.15499.fc
12. Tenti M, Raffaeli W, Gremigni P. A narrative review of the assessment of depression in chronic pain. Pain Manag Nurs. 2022;23(2):158–167. doi:10.1016/j.pmn.2021.03.009
13. Wolfe F, Michaud K, Li T, Katz RS. Chronic conditions and health problems in rheumatic diseases: comparisons with rheumatoid arthritis, noninflammatory rheumatic disorders, systemic lupus erythematosus, and fibromyalgia. J Rheumatol. 2010;37(2):305–315. doi:10.3899/jrheum.090781
14. Kleykamp BA, Ferguson MC, McNicol E, et al. The prevalence of psychiatric and chronic pain comorbidities in fibromyalgia: an ACTTION systematic review. Semin Arthritis Rheum. 2021;51(1):166–174. doi:10.1016/j.semarthrit.2020.10.006
15. Munipalli B, Chauhan M, Morris AM, et al. Recognizing and treating major depression in fibromyalgia: a narrative primer for the non-psychiatrist. J Prim Care Community Health. 2024;15:21501319241281221. doi:10.1177/21501319241281221
16. Smith MT, Haythornthwaite JA. How do sleep disturbance and chronic pain inter-relate? Insights from the longitudinal and cognitive-behavioral clinical trials literature. Sleep Med Rev. 2004;8(2):119–132. doi:10.1016/S1087-0792(03)00044-3
17. Husak AJ, Bair MJ. Chronic pain and sleep disturbances: a pragmatic review of their relationships, comorbidities, and treatments. Pain Med. 2020;21(6):1142–1152. doi:10.1093/pm/pnz343
18. McBeth J, Wilkie R, Bedson J, Chew-Graham C, Lacey RJ. Sleep disturbance and chronic widespread pain. Curr Rheumatol Rep. 2015;17(1):469. doi:10.1007/s11926-014-0469-9
19. Koffel E, Kroenke K, Bair MJ, Leverty D, Polusny MA, Krebs EE. The bidirectional relationship between sleep complaints and pain: analysis of data from a randomized trial. Health Psychol. 2016;35(1):41–49. doi:10.1037/hea0000245
20. Bondesson E, Larrosa Pardo F, Stigmar K, et al. Comorbidity between pain and mental illness - evidence of a bidirectional relationship. Eur J Pain. 2018;22(7):1304–1311. doi:10.1002/ejp.1218
21. Yang H, Hurwitz EL, Li J, et al. Bidirectional comorbid associations between back pain and major depression in US adults. Int J Environ Res Public Health. 2023;20(5):4217. doi:10.3390/ijerph20054217
22. Wilson KG, Eriksson MY, Joyce LD, Mikail SF, Emery PC. Major depression and insomnia in chronic pain. Clin J Pain. 2002;18(2):77–83. doi:10.1097/00002508-200203000-00002
23. O’Brien EM, Waxenberg LB, Atchison JW, et al. Negative mood mediates the effect of poor sleep on pain among chronic pain patients. Clin J Pain. 2010;26(4):310–319. doi:10.1097/AJP.0b013e3181c328e9
24. Generaal E, Vogelzangs N, Penninx BW, Dekker J. Insomnia, sleep duration, depressive symptoms, and the onset of chronic multisite musculoskeletal pain. Sleep. 2017;40(1). doi:10.1093/sleep/zsw030
25. Juan W, Rui L, Wei-Wen Z. Chronic neck pain and depression: the mediating role of sleep quality and exercise. Psychol Health Med. 2020;25(8):1029–1035. doi:10.1080/13548506.2020.1724308
26. Alhalal EA, Alhalal IA, Alaida AM, Alhweity SM, Alshojaa AY, Alfaori AT. Effects of chronic pain on sleep quality and depression: a cross-sectional study. Saudi Med J. 2021;42(3):315–323. doi:10.15537/smj.42.3.20200768
27. Ferreira VM, Sherman AM. The relationship of optimism, pain and social support to well-being in older adults with osteoarthritis. Aging Mental Health. 2007;11(1):89–98. doi:10.1080/13607860600736166
28. Williams TL, Joseph C, Nilsson-Wikmar L, Phillips J. The interrelationship between pain, life satisfaction and mental health in adults with traumatic spinal cord injury, in the context of a developing country. Spinal Cord Ser Cases. 2024;10(1):9. doi:10.1038/s41394-024-00622-9
29. Saravanan A, Bajaj P, Mathews HL, Tell D, Starkweather A, Janusek L. Social support is inversely associated with sleep disturbance, inflammation, and pain severity in chronic low back pain. Nur Res. 2021;70(6):425–432. doi:10.1097/NNR.0000000000000543
30. Larsson B, Dragioti E, Gerdle B, Björk J. Positive psychological well-being predicts lower severe pain in the general population: a 2-year follow-up study of the SwePain cohort. Ann Gen Psychiatry. 2019;18:8. doi:10.1186/s12991-019-0231-9
31. Gasperi M, Herbert M, Schur E, Buchwald D, Afari N. Genetic and environmental influences on sleep, pain, and depression symptoms in a community sample of twins. Psychosom Med. 2017;79(6):646–654. doi:10.1097/PSY.0000000000000456
32. Medda E, Toccaceli V, Fagnani C, et al. The Italian twin registry: an update at 18 years from its inception. Twin Res Hum Genet. 2019;22(6):572–578. doi:10.1017/thg.2019.75
33. Fagnani C, Toccaceli V, Tenti M, et al. An Italian twin study of non-cancer chronic pain as a wide phenotype and its intensity. Medicina. 2022;58(11):1522. doi:10.3390/medicina58111522
34. Toccaceli V, Tenti M, Stazi MA, et al. Development and validation of the italian “brief five-item chronic pain questionnaire” for epidemiological studies. J Pain Res. 2022;15:1897–1913. doi:10.2147/JPR.S362510
35. Kato K, Sullivan PF, Evengård B, Pedersen NL. Chronic widespread pain and its comorbidities: a population-based study. Arch Intern Med. 2006;166(15):1649–1654. doi:10.1001/archinte.166.15.1649
36. Burri A, Ogata S, Livshits G, Williams F. The association between chronic widespread musculoskeletal pain, depression and fatigue is genetically mediated. PLoS One. 2015;10(11):e0140289. doi:10.1371/journal.pone.0140289
37. Markkula R, Järvinen P, Leino-Arjas P, Koskenvuo M, Kalso E, Kaprio J. Clustering of symptoms associated with fibromyalgia in a Finnish twin cohort. Eur J Pain. 2009;13(7):744–750. doi:10.1016/j.ejpain.2008.09.007
38. Burri A, Ogata S, Rice D, Williams FMK. Twelve-year follow-up of chronic pain in twins: changes in environmental and genetic influence over time. Eur J Pain. 2018;22(8):1439–1447. doi:10.1002/ejp.1233
39. Diener E, Emmons RA, Larsen RJ, Griffin S. The Satisfaction with Life Scale. J Pers Assess. 1985;49(1):71–75. doi:10.1207/s15327752jpa4901_13
40. Kroenke K, Spitzer RL, Williams JB. The patient health questionnaire-2: validity of a two-item depression screener. Med Care. 2003;41(11):1284–1292. doi:10.1097/01.MLR.0000093487.78664.3C
41. Kocalevent RD, Berg L, Beutel ME, et al. Social support in the general population: standardization of the Oslo social support scale (OSSS-3). BMC psychol. 2018;6(1):31. doi:10.1186/s40359-018-0249-9
42. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index (PSQI): a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
43. Neale MC, Hunter MD, Pritikin JN, et al. OpenMx 2.0: extended structural equation and statistical modeling. Psychometrika. 2016;81(2):535–549. doi:10.1007/s11336-014-9435-8
44. McGue M, Osler M, Christensen K. Causal inference and observational research: the utility of twins. Perspect Psychol Sci. 2010;5(5):546–556. doi:10.1177/1745691610383511
45. Neale MC, Cardon LR. Methodology for Genetic Studies of Twins and Families. Dordrecht: Kluwer Academic Publishers; 1992.
46. Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51(6):1173–1182. doi:10.1037//0022-3514.51.6.1173
47. Pinheiro MB, Morosoli JJ, Colodro-Conde L, Ferreira PH, Ordoñana JR. Genetic and environmental influences to low back pain and symptoms of depression and anxiety: a population-based twin study. J Psychosom Res. 2018;105:92–98. doi:10.1016/j.jpsychores.2017.12.007
48. Chang MH, Hsu JW, Huang KL, et al. Bidirectional association between depression and fibromyalgia syndrome: a nationwide longitudinal study. J Pain. 2015;16(9):895–902. doi:10.1016/j.jpain.2015.06.004
49. Fishbain DA, Cutler R, Rosomoff HL, Rosomoff RS. Chronic pain-associated depression: antecedent or consequence of chronic pain? A review. Clin J Pain. 1997;13(2):116–137. doi:10.1097/00002508-199706000-00006
50. Miró E, Martínez MP, Sánchez AI, Prados G, Medina A. When is pain related to emotional distress and daily functioning in fibromyalgia syndrome? The mediating roles of self-efficacy and sleep quality. Br J Health Psychol. 2011;16(4):799–814. doi:10.1111/j.2044-8287.2011.02016.x
51. Diaz-Piedra C, Catena A, Miro E, Martinez MP, Sanchez AI, Buela-Casal G. The impact of pain on anxiety and depression is mediated by objective and subjective sleep characteristics in fibromyalgia patients. Clin J Pain. 2014;30(10):852–859. doi:10.1097/AJP.0000000000000040
52. Karimi R, Mallah N, Scherer R, Rodríguez-Cano R, Takkouche B. Sleep quality as a mediator of the relation between depression and chronic pain: a systematic review and meta-analysis. Br J Anaesth. 2023;130(6):747–762. doi:10.1016/j.bja.2023.02.036
53. Kim HJ, Park H, Juon HS. The mediating role of pain catastrophizing on the association between depression and pain severity and interference among elderly Asian immigrants with chronic pain. J Pain Res. 2021;14:737–745. doi:10.2147/JPR.S304440
54. Kardash L, Wall CL, Flack M, Searle A. The role of pain self-efficacy and pain catastrophizing in the relationship between chronic pain and depression: a moderated mediation model. PLoS One. 2024;19(5):e0303775. doi:10.1371/journal.pone.0303775
55. Peñacoba Puente C, Velasco Furlong L, Écija Gallardo C, Cigarán Méndez M, Bedmar Cruz D, Fernández-de-Las-Peñas C. Self-efficacy and affect as mediators between pain dimensions and emotional symptoms and functional limitation in women with fibromyalgia. Pain Manag Nurs. 2015;16(1):60–68. doi:10.1016/j.pmn.2014.04.005
56. Skidmore JR, Koenig AL, Dyson SJ, Kupper AE, Garner MJ, Keller CJ. Pain self-efficacy mediates the relationship between depressive symptoms and pain severity. Clin J Pain. 2015;31(2):137–144. doi:10.1097/AJP.0000000000000094
57. Selvanathan J, Pham C, Nagappa M, et al. Cognitive behavioral therapy for insomnia in patients with chronic pain–a systematic review and meta-analysis of randomized controlled trials. Sleep Med Rev. 2021;60:101460. doi:10.1016/j.smrv.2021.101460
58. Müller R, Gertz KJ, Molton IR, et al. Effects of a tailored positive psychology intervention on well-being and pain in individuals with chronic pain and a physical disability: a feasibility trial. Clin J Pain. 2016;32(1):32–44. doi:10.1097/AJP.0000000000000225
59. Sullivan PF, Evengård B, Jacks A, Pedersen NL. Twin analyses of chronic fatigue in a Swedish national sample. Psychol Med. 2005;35(9):1327–1336. doi:10.1017/S0033291705005222
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.