Back to Journals » Journal of Pain Research » Volume 13
Psychiatric Comorbidity and Complex Regional Pain Syndrome Through the Lens of the Biopsychosocial Model: A Comparative Study
Authors Duong HP ![]() , Konzelmann M
, Konzelmann M ![]() , Vuistiner P
, Vuistiner P ![]() , Burrus C
, Burrus C ![]() , Léger B
, Léger B ![]() , Stiefel F
, Stiefel F ![]() , Luthi F
, Luthi F ![]()
Received 31 August 2020
Accepted for publication 31 October 2020
Published 3 December 2020 Volume 2020:13 Pages 3235—3245
DOI https://doi.org/10.2147/JPR.S278614
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Hong Phuoc Duong,1 Michel Konzelmann,1,2 Philippe Vuistiner,1 Cyrille Burrus,1,2 Bertrand Léger,1 Friedrich Stiefel,3 François Luthi1,2,4
1Department of Medical Research, Clinique Romande de Réadaptation, Sion, Switzerland; 2Department of Musculoskeletal Rehabilitation, Clinique Romande de Réadaptation, Sion, Switzerland; 3Psychiatric Liaison Service, Lausanne University and Lausanne University Hospital, Lausanne, Switzerland; 4Department of Rheumatology and Rehabilitation, Hôpital Orthopédique, University and University Hospital of Lausanne, Lausanne, Switzerland
Correspondence: Bertrand Léger Tel +41 27 603 2075
Fax +41 27 603 2072
Email [email protected]
Purpose: To compare the prevalence of psychiatric comorbidity between patients with complex regional pain syndrome (CRPS) of the hand and non-CRPS patients and to assess the association between biopsychosocial (BPS) complexity profiles and psychiatric comorbidity in a comparative study.
Patients and Methods: We included a total of 103 patients with CRPS of the hand and 290 patients with chronic hand impairments but without CRPS. Psychiatric comorbidities were diagnosed by a psychiatrist, and BPS complexity was measured by means of the INTERMED. The odds ratios (OR) of having psychiatric comorbidities according to BPS complexity were calculated with multiple logistic regression (adjusted for age, sex, and pain).
Results: Prevalence of psychiatric comorbidity was 29% in CRPS patients, which was not significantly higher than in non-CRPS patients (21%, relative risk=1.38, 95% CI: 0.95 to 2.01 p=0.10). The median total scores of the INTERMED were the same in both groups (23 points). INTERMED total scores (0– 60 points) were related to an increased risk of having psychiatric comorbidity in CRPS patients (OR=1.46; 95% CI: 1.23– 1.73) and in non-CRPS patients (OR=1.21; 95% CI: 1.13– 1.30). The four INTERMED subscales (biological, psychological, social, and health care) were correlated with a higher risk of having psychiatric comorbidity in both groups. The differences in the OR of having psychiatric comorbidity in relation to INTERMED total and subscale scores were not statistically different between the two groups.
Conclusion: The total scores, as well as all four dimensions of BPS complexity measured by the INTERMED, were associated with psychiatric comorbidity, with comparable magnitudes of association between the CRPS and non-CRPS groups. The INTERMED was useful in screening for psychological vulnerability in the two groups.
Keywords: complex regional pain syndrome, psychiatric comorbidity, biopsychosocial complexity, INTERMED
Introduction
Complex regional pain syndrome (CRPS) is a chronic pain condition that often occurs after trauma or surgery.1 In terms of prevalence, the hand is the most common site.2 For similar injuries, the presence of CRPS is associated with longer disability, lower quality of life, and higher costs.3
While there are many controversies surrounding CRPS, the role of psychological disorders has been subject to debate for decades.4,5 Meanwhile, most authors accept that patients who develop CRPS do not present specific psychological characteristics at the onset.6,7 Moreover, many patients with CRPS do not develop psychiatric comorbidities.7 However, prospective studies have shown that mood disorders (anxiety, depression), particularly if they are associated with inadequate protective-type behavior to a perceived threat (avoidance, catastrophism), may contribute to an unfavorable outcome (increased perception of pain and/or disability).8 So far, psychiatric disorders in CRPS patients were mainly evaluated by means of questionnaires without subsequent validation by a psychiatrist, and determinants favouring the presence of psychiatric comorbidities have rarely been identified and contextualized. In CRPS patients, the range of the prevalence of mood disorders diagnosed by a psychiatrist over the course of illness is wide and is estimated to be between 15% and 65%,9–12 comparable to that of other chronic pain syndromes.13 Speck et al,14 in a study of psychiatric disorders identified through questionnaires, found that post-traumatic stress disorder (PTSD) had a prevalence of 38% in CRPS patients. In a publication by the Swiss Health Observatory, the co-occurrence of psychiatric and somatic illnesses in hospitalized patients leads to increased costs by about 28%, compared to situations where only a somatic disease is present.15 Therefore, investigating psychiatric comorbidity in CRPS patients is important, both from the perspective of the patient and that of the health care system.
The biopsychosocial (BPS) model of disease appears particularly relevant in addressing the psychological issues of CRPS patients. Theorized by George Engel some forty years ago,16 the BPS model is now supported by the World Health Organization in its International Classification of Functioning.17 The holistic approach of the BPS model might be more advantageous than the reductionist dualistic approach of the biomedical disease model, especially with regard to the orientation of interdisciplinary care in chronic pain syndromes.18 The BPS model’s underlying assumptions rely on the complex and non-linear interactions between the biological, psychological, and social determinants that affect disease outcomes. Thus, non-linear interactions raise questions, such as their impacts on psychiatric comorbidity which does or does not reach the diagnostic threshold.18–20 One of the validated tools constructed to operationalize the BPS model and to assess patients with regard to BPS case complexity is the INTERMED.21,22 The instrument synthesizes four dimensions, the biological, psychological, social, and health care dimensions diachronically (past, present, and prognosis), based on a semi-structured interview.23,24 The INTERMED has been demonstrated to identify complex patients, those at risk for adverse health outcomes,25–28 and those with high use of health care services.29–32
To date, only one study used the INTERMED to evaluate BPS complexity in patients with CRPS of the knee10 and found that a high level of BPS complexity is associated with an increased risk of psychiatric comorbidities. However, this study was limited to CRPS of the knee, which is a much rarer condition than CRPS of the upper extremities.33 The clinical presentation of the two is comparable but not identical, and CRPS confined to the knee seems to be associated with more unfavorable outcomes (work and quality of life).34 Therefore, CRPS of the hand, the most prevalent CRPS, appears to be a more suitable condition to be evaluated in a comparative study with the aim to measure the associations between BPS complexity and psychiatric comorbidity. In addition, the previous study10 compared “complex” BPS patients versus “non-complex” patients in a dichotomous perspective. BPS complexity, however, should be viewed as a continuum. Finally, the four dimensions of the INTERMED have never been evaluated with regard to their relationship with psychiatric comorbidity. According to the complexity theory, one would expect all four scales to interact with this outcome.18–20 For these reasons, we aimed to measure the probability of having a psychiatric comorbidity according to BPS complexity as assessed by the INTERMED (total score and scores of the four subscales) through a comparative study. By comparing the prevalence of psychiatric comorbidity between CPRS and non-CRPS patients, we would also like to gain information about the role of psychiatric comorbidity in CRPS.
Patients and Methods
Study Design
This was a single-center, retrospective comparative study.
Study Population
Between January 2007 and June 2013, 461 patients (18–65 years old) were admitted to the rehabilitation clinic in Sion, Switzerland after experiencing wrist or hand trauma. The reasons for admission were persistent pain, functional limitations, therapeutic failure of usual outpatient care, and/or inability to return to work. For patients with multiple hospitalizations during the study period, only the first was included. Diagnosis of CRPS was based on the criteria of the “International Association for the Study of Pain” 199435 and the French diagnostic criteria36 from 2007 to 2009 (N=46); since 2010, the Budapest’s criteria for diagnosis of CRPS37 have been used and applied (N=57). Due to the use of different sets of diagnostic criteria, the medical records of all patients were retrospectively reviewed by a senior physician specializing in rheumatology, physical medicine, and rehabilitation with many years of experience in CRPS care (MK) to confirm the diagnosis of CRPS, particularly for patients treated between 2007 and 2009. Other diagnoses, which better explain the clinical condition, were excluded. Analyses were also conducted in the subgroup of CRPS patients using Budapest’s criteria (N=57), comparing these patients with the whole CRPS sample.
Exclusion criteria included: peripheral nervous lesions on the same side of the injury or CRPS type II (N = 22), multiple trauma (N = 19), and hand-shoulder syndrome patients (N = 27).
The comparative group had to fulfill all inclusion criteria, and the existence of CRPS was ruled out by a senior physician. We included a total of 103 patients with CRPS of the hand and 290 patients with chronic hand impairments but without CRPS.
Measurements
The following data were extracted from the database: age, sex, the interval between the trauma and the hospitalization (months), and initial trauma. Initial orthopedic trauma was divided into six categories: 1) forearm/radius fracture, 2) hand fracture, 3) ligament injury of the wrist or the hand, 4) contusion or sprain, 5) simple wound (skin, tendon, or nerve), 6) finger amputation or complex hand injuries (association of multiple lesions).
Pain was measured upon entry using a Visual Analog Scale (VAS) completed by the patient. The VAS was graduated from 0 to 100 mm (0= no pain to 100= extreme pain).
Disability was assessed upon entry using the Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire.38 This self-reported questionnaire contains 30 items, which measure symptoms, impairment, and disabilities in patients with upper limb pathologies. Each item scores from 1 to 5. The total scores are used to calculate a score ranging from 0 (no disability) to 100 (most severe disability). The DASH questionnaire is available in many languages; we used the French version, obtained from http://www.dash.iwh.on.ca/.
The BPS complexity profile was measured through the INTERMED. A detailed description of the INTERMED is presented in Table 1. A trained nurse conducted the semi-structured interview used to obtain the INTERMED score within the three days following admission. For each of the four domains (biologic, psychological, social, and health care), two items regarding the patient’s history and current status and one item regarding the patient’s prognosis were rated with a score ranging from 0 to 3. For each of the domains, the score ranges from 0 to 15. The total score of the four domains ranges from 0 (lowest case complexity) to 60 (highest case complexity). Patients with a score equal to or higher than 21 are considered as “complex”, those with a score less than 21 are considered as “non-complex”.39 For inferential statistical analysis, continuous scores were used. Detailed information about the questionnaire can be found at: http://www.intermedconsortium.com.
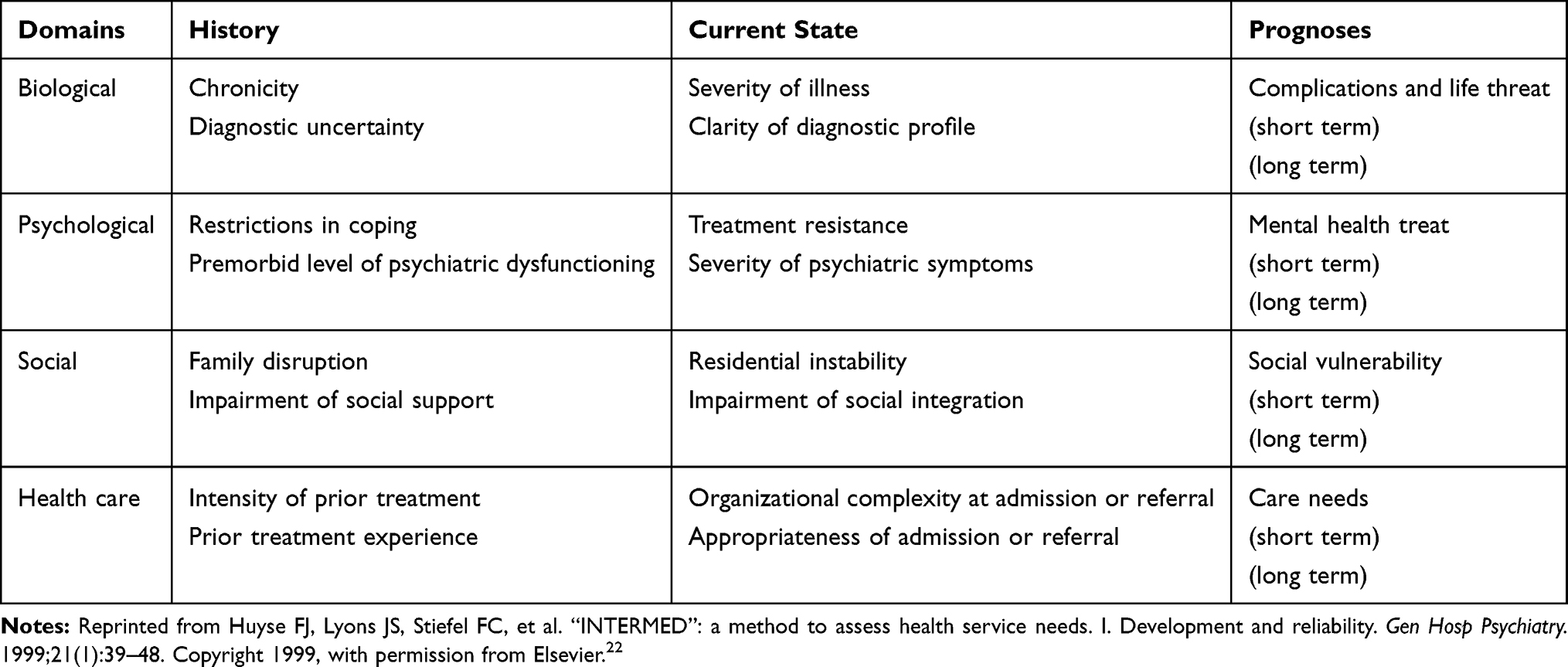 |
Table 1 The INTERMED and Its Items |
Each patient underwent psychiatric evaluation conducted by a senior psychiatrist upon entry after the initial assessment conducted by the treating rehabilitation physician. The diagnosis of psychiatric comorbidities was based on the International Classification of Diseases (ICD-10) criteria;40 the interview lasted about one hour and, if necessary, psychological follow-up was arranged during the stay. The INTERMED score was not communicated to the rehabilitation physician or the psychiatrist.
Statistical Analysis
According to a two-sided test at the α = 5% level, the study had 90% power to detect the smallest odds ratio (OR) greater than one.
Continuous variables with non-normal distributions on the histogram (age, the time between the accident and the hospitalization, INTERMED total and subscales) are presented using median and interquartile ranges. Continuous variables with a normal distribution (VAS, DASH scores) are presented using means and standard deviations. Differences between CPRS and non-CPRS patients, such as clinical characteristics, BPS profile, psychiatric comorbidities, intensity of pain, and level of disability upon entry, were evaluated using binary logistic regression analysis (OR with 95% confidence interval).
The OR of having psychiatric comorbidity according to BPS complexity, assessed using the INTERMED (total score) in both groups and were calculated by means of univariate and multiple logistic regression (adjusted for age, sex, and pain). The OR of having psychiatric comorbidity according to INTERMED total or subscale scores were also analyzed in the multiple logistic regression (adjusted for age, sex, and pain) in the subgroup of CRPS patients diagnosed by the Budapest Criteria. The difference in the OR of having psychiatric comorbidity in relation to INTERMED total score between the CRPS and non-CRPS groups was assessed using multiple logistic regression (adjusted for age, sex, pain, presence of CRPS, and the interaction between CRPS and INTERMED) for the whole cohort. The same method was applied to the four subscales.
All analyses were performed using the Stata program version 16.0 (StataCorp LP 4905 Lakeway Drive College Station, Texas, 77845 USA).
Ethics Approval and Informed Consent
This retrospective comparative study was approved by the ethics committee of the local medical association (Commission Cantonale Valaisanne d’Ethique Médicale (CCVEM 043/07)). Informed written consent was obtained from each patient involved in this study.
Results
Comparisons of Sociodemographic and Clinical Characteristics Between CRPS and Non-CRPS Patients
Figure 1 presents the flow chart of the study. The median age did not differ between CRPS and non-CRPS patients (42 years versus 41 years, respectively, p=0.06). The proportion of women was significantly higher in the CRPS group (35% versus 11%, p<0.001). The median interval between the trauma and the hospitalization was not statistically different between CRPS and non-CRPS patients (8.4 versus 11.6 months, p=0.12). The category of initial injury was similar between the two groups. The frequency of surgery was significantly lower in CRPS patients (64% versus 82%, p <0.001) (see Table 2).
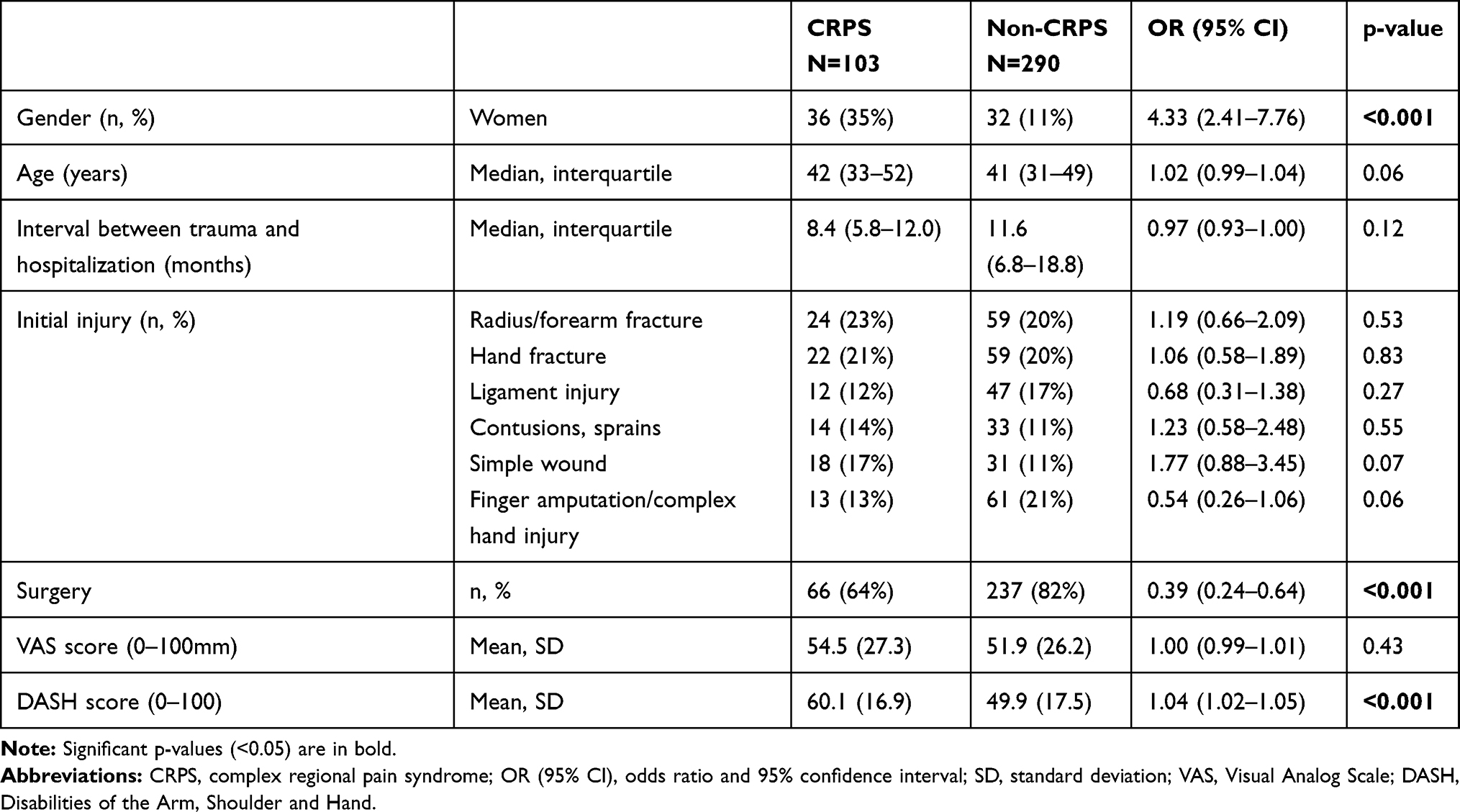 |
Table 2 Comparisons of Sociodemographic and Clinical Characteristics Between CRPS and Non-CRPS Patients |
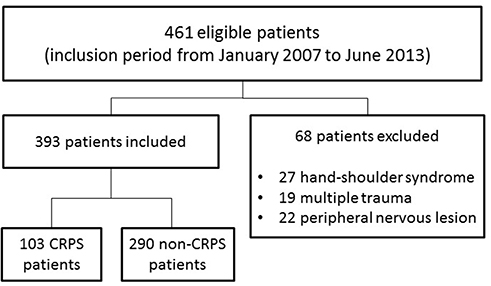 |
Figure 1 Flow chart of the study. |
The mean DASH score at entry was significantly higher in the CRPS population (60.1±16.9 versus 49.9±17.5 points, p<0.001). The severity of pain at entry was not statistically different between the two groups (VAS mean score of 54.5± 27.3 for CRPS patients and 51.9±26.2 for non-CRPS patients, p=0.43) (see Table 2).
Prevalence of Psychiatric Comorbidity and BPS Profile in the Two Groups
The prevalence of psychiatric comorbidity was not significantly different between CRPS patients and non-CRPS patients (29% versus 21%, p=0.10). The relative risk of having psychiatric comorbidity was 1.38 in CRPS group compared to the non-CRPS group (95% CI: 0.95 to 2.01). The type of psychiatric diagnosis according to the ICD-10 classification did also not differ between the two groups. In CRPS patients, mood disorders (adjustment disorders with mixed depression and anxiety, and depressive disorders) were diagnosed in 24 out of 30 patients (80%), followed by PTSD (N = 3) and personality disorders (N = 3). The distribution of psychiatric diagnoses was similar in non-CRPS patients, with mood disorders accounting for 50 out of 61 patients (82%), followed by PTSD (N = 4), personality disorders (N = 4), and mental disorders related to alcohol (N = 3) (see Table 3).
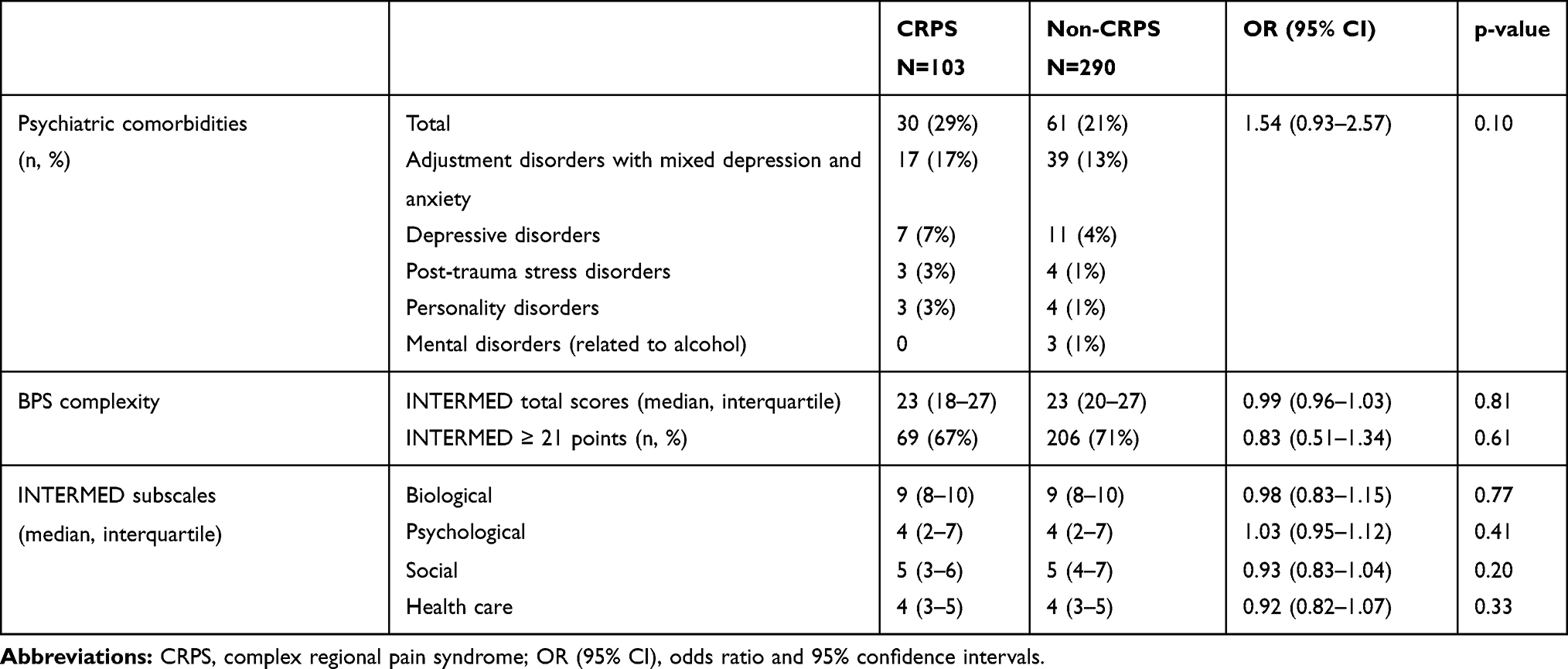 |
Table 3 Psychiatric Comorbidity and BPS Profile Between CRPS and Non-CRPS Patients |
The median scores for BPS complexity, as measured by the INTERMED, were comparable (median 23 points) for the two groups. The percentage of patients with high BPS complexity (INTERMED scores of ≥21 points) was also similar in both groups (Table 3), as were the scores of the four domains (biological, psychological, social, and health care).
Association Between the BPS Complexity and Psychiatric Comorbidity in CRPS Patients and Non-CRPS Patients
In the univariate logistic regression analysis, the INTERMED total as well as all four subscale scores were found to be related to an increased risk of psychiatric comorbidities in both the CRPS and non-CRPS groups (see Supplementary Table 1).
After adjusting for confounding variables (age, sex, and pain) in the multiple logistic regression analysis, INTERMED total scores or subscale scores remained as the significant predictors for the psychiatric comorbidities in both groups (Table 4). In other words, for every one-unit increase in the INTERMED total score, a 46% increase in the odds of having a psychiatric comorbidity in CRPS patients was expected, while a 21% increase was expected in non-CRPS patients. Among the four domains of the INTERMED, the psychological subscale (0–15 points) had the highest OR with psychiatric comorbidity in the CRPS group (OR=2.37, 95% CI: 1.62–3.48) and in the non-CRPS group: OR= 1.65 (95% CI: 1.39–1.97). The OR of having psychiatric comorbidity in relation to the INTERMED total and subscale scores were not statistically different between the two groups.
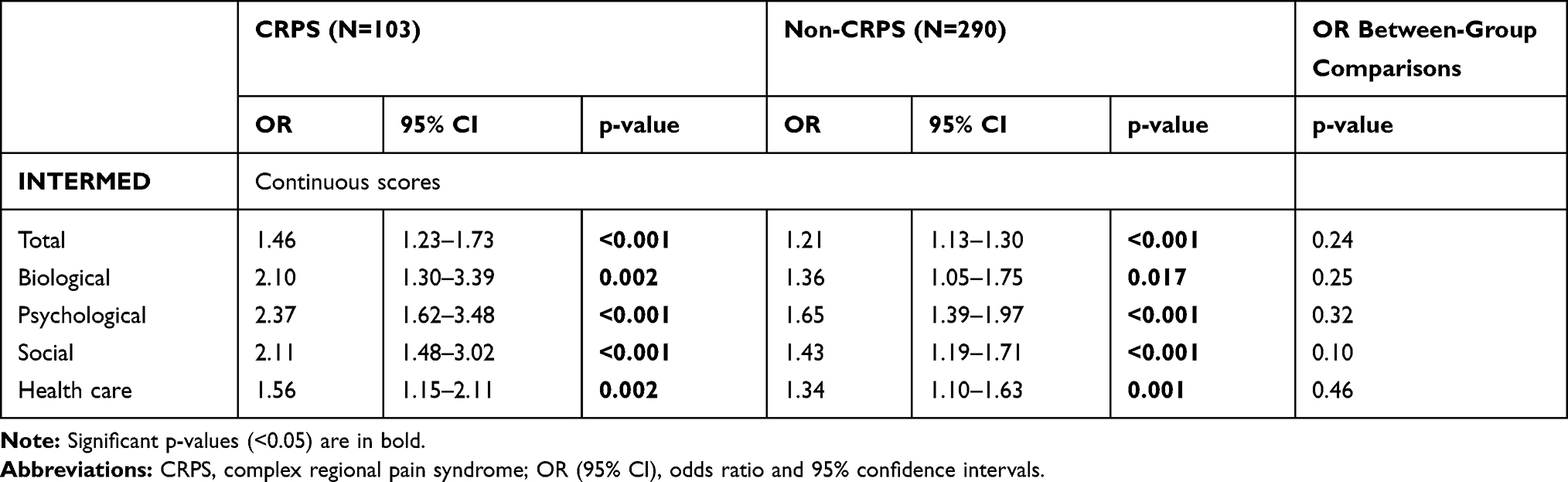 |
Table 4 Results of the Multiple Logistic Regression Analyses (Adjusted for Age, Gender and Pain) Between BPS Complexity Assessed by Means of the INTERMED and Presence of Psychiatric Comorbidity in the Two Groups |
Analyses were conducted in the subgroup of CRPS patients using the Budapest Criteria (N=57) to evaluate the relationship between BPS complexity and psychiatric comorbidity. The prevalence of psychiatric comorbidity was 30% (29% in the whole CRPS sample), and the INTERMED median scores were of 23 points in this subgroup (similar to the whole CRPS sample). Of note, the OR of having a psychiatric comorbidity in relation to INTERMED total scores was 1.29 (95% CI: 1.10 −1.51, p=0.001) in the multiple logistic regression (adjusted for age, sex, and pain). The OR of having a psychiatric comorbidity in relation to INTERMED four subscale scores were also statistically significant in this subgroup (see Supplementary Table 2).
Discussion
Psychiatric comorbidities, mainly mood disorders (anxiety, depression), were found in 29% of CRPS patients, versus in 21% of the non-CRPS patients, though this difference was not statistically significant. BPS complexity was associated with psychiatric comorbidity. The higher the complexity, the greater the risk: there was a 46% increase in the odds for psychiatric comorbidities in the CRPS group, and a 21% increase in the odds for psychiatric comorbidities in the non-CRPS group for each additional point of the INTERMED score (0–60 points), after adjusting for age, sex, and pain intensity. The differences in the OR of having psychiatric comorbidity in relation to INTERMED total and subscale scores were not statistically different between the two groups. Moreover, the scores of all INTERMED subscales were associated with psychiatric comorbidity. This result is consistent with complexity concepts related to the BPS model of disease, which assumes that there is an interrelationship between biological, psychological, and social determinants of health.18–20 Regarding the issue of psychiatric comorbidity in CRPS patients, it seems interesting to take into account not only the biological and psychological but also social and health care-related determinants, such as access to interdisciplinary care. In addition, the results suggest that psychiatric morbidity in itself is not necessarily a problem for medical care, but biopsychosocial complexity does.29–32,41
The BPS profile, level of complexity, and severity of pain were comparable between the CRPS and non-CRPS patients. The main difference between the two groups was limited to severity of disability; with the DASH scores having a significant average difference of 10.2 points.42 These results suggest that patients with CRPS are not fundamentally different from non-CRPS patients in terms of psychiatric comorbidity. This finding is in line with a study conducted by Park et al, who found that patients with chronic CRPS were not more psychologically disturbed than other chronic pain patients.43 Our study confirms the utility of the INTERMED to identify complex patients, including those in this population, and to direct interdisciplinary care.
A non-negligible proportion of CRPS patients suffered from mental disorders, which deserve identification and adequate treatment. Considering psychiatric comorbidity from the perspective of the BPS model of disease, our results could also contribute to pacify the never-ending debate – which also surrounds other chronic conditions – between those who perceive the CRPS as a somatic condition and those who view it as psychogenic or functional disorder.4,44,45 The particularly high level of disability in the CRPS population underlines the importance of appropriate interdisciplinary care.46
Our results confirm those of a previous study which assessed patients with CRPS confined to the knee,10 which found a comparable prevalence of psychiatric comorbidity between the cases and controls and that BPS complexity was also correlated with psychiatric comorbidity. The relationship between BPS complexity assessed by the INTERMED and psychiatric comorbidity has been observed in various populations, such as in patients with somatic symptom disorders,25 advanced cancer,26 in need of organ transplantation,27 or suffering from orthopedic trauma41 or multiple sclerosis.28 Although a comparative study could not prove a causal link, these previous studies speak in favor of a probable association. The hypothesis that BPS complexity is a risk factor for psychiatric comorbidity is also strengthened by the results concerning the correlation between INTERMED subscales and psychiatric comorbidity, which indicates that the psychological dimension of the INTERMED is not the only dimension associated with psychiatric comorbidity. This hypothesis is also in line with observations that mental crises are determined by multiple factors47 and that allostatic overload may persistently activate not just different neuroendocrine and cardiovascular responses, but also emotional responses.48 Identifying BPS complexity by means of the INTERMED also provides the opportunity for providing early intervention, which decrease the allostatic load, as demonstrated in a previous study which used the INTERMED to conceive and implement early interventions. In the mentioned study, depressive symptoms and major depressive disorders were decreased in the INTERMED-based intervention group (compared to care as usual).49
Indeed, mood disorders are the most prevalent psychiatric comorbidity in CRPS populations,9,10,12 a finding which was confirmed by our study. Our results with regard to the prevalence of mood disorders are situated between the prevalence of 15.6% in Brinkers’ study9 and of 65% in Rommel’s study,12 in which psychiatric disorders were diagnosed by psychiatrists. The disparity in the prevalence of psychiatric disorders was presumably explained by the differences in the characteristics of the studied population (for example: age, and time of follow-up), as well as the different settings in which these studies were conducted (in or outpatients). The overall prevalence of psychiatric comorbidity of CRPS patients in our study was slightly higher than the prevalence in the previous study, which included patients with CRPS of the knee (29% versus 20%); the mean INTERMED total score was also higher (23 versus 19 points). This difference is most likely due to the higher level of BPS complexity in our study (additional risk for each additional point on the INTERMED scale), rather than by a difference related to the location of the syndrome. This hypothesis is strengthened by the fact that the two samples have similar social conditions (with a majority being men from the secondary sector, with long-term work incapacity due to the CRPS). The BPS complexity as measured by the INTERMED is therefore not only useful in detecting psychiatric comorbidity in clinics but also in identifying confounding BPS variables patients with chronic pain in research and in comparing different populations from a more comprehensive perspective.23
The prevalence of other psychiatric disorders was low, with personality disorders diagnosed in three patients (3%) and PTSD in three patients (3%). Other authors have found different prevalence rates for these disorders in patients with CRPS. For personality disorders (a diagnosis which by definition has to precede the occurrence of the CRPS), Brinkers et al9 reported a 11% prevalence, while Monti et al11 reported a particularly high prevalence of 60% in a sample of only 25 patients, based on a structured clinical interview. The latter result11 should be considered with caution, since only 16% of the patients did not qualify for a psychiatric diagnosis. For PTSD, the prevalence in patients with CRPS also seems variable. It ranges from none at all9 to a prevalence of 38% of patients who meet the criteria for PTSD.14 Interestingly, in the last study,14 maladaptive coping (also one of the items of the INTERMED) was related to the presence of PTSD, which was, however, not based on a clinical diagnosis by a psychiatrist. As mentioned, selection bias or differences in the referral patterns related to medical settings could explain these large differences in PTSD prevalence. In addition, CRPS is a rare condition for which it may be difficult to assemble representative samples. In many studies, the duration of symptoms extends over several years, which may lead, for example, to the exclusion of CRPS with more favorable outcomes.
Two other psychiatric diagnoses were associated with CRPS in the literature, but not found in our sample: somatoform pain disorder and dissociative or conversion disorder, also called functional neurological disorder (FND). Brinkers et al9 found these two diagnoses, respectively, in 3% of patients who consulted in an Anesthesiology Department,9 whereas Bass50 found 84% of patients meeting the criteria for somatoform disorder and 42% for functional neurological symptoms compatible with conversion disorder in a medico-legal context (litigation). The prevalence of these disorders is thus highly variable and seems to depend on the clinical setting. Diagnosing a conversion disorder or FND in the context of a CRPS is very specific, since conversion disorder often manifests itself with neurological signs (dystonia, claw-hand, etc.), which are also part of the Budapest CRPS criteria.37 Some authors will thus consider that the presence of one condition excludes the presence of the other entity, while other authors propose to conceive CRPS and FND as disorders, which share common features and can co-exist.44 These reasons explain why the prevalence of FND can change from one study to another.
The investigation of psychiatric comorbidity in patients who have developed CRPS is still in its infancy. Most studies are based on questionnaires for the reason of convenience, and few have applied the gold standard - the clinical evaluation by a psychiatrist. To date, only two factors have been found to be associated with the risk of developing a psychiatric disorder which reaching the diagnostic threshold in CRPS patients: maladaptive coping strategies for PTSD,14 and BPS complexity in this study for all psychiatric disorders.
The use of the BPS complexity model of disease in CRPS patients could help bridge some gaps in the research about this syndrome, particularly regarding the controversial issue about the influence of various psychosocial factors.7,8,51 It may also be of interest to study whether an investigation based on this model provides a better understanding of the particularly high health care costs produced by CRPS,3 as the co-occurrence of somatic and psychiatric disorders is one of the drivers of increased resource consumption.15 The self-assessment version of the INTERMED (the IM-SA), a more time-efficient method than the semi-structured interview based INTERMED, may be an alternative in time-restrained settings, since it also guides multidisciplinary care.52 However, the INTERMED approach has been also demonstrated to have a therapeutic effect since it allows patients to express emotional distress in front of an empathic witness and caretakers to foster therapeutic alliance,53 effects which may not be achieved with the IM-SA.
Strengths and Limitations
The following strengths characterize this study: the relatively large sample, which is rare for chronic pain condition3 and the interval between the event precipitating the CRPS and the assessment by the psychiatrist was only a few months. In most studies,7 this interval was several years, which may induce selection bias due to the higher prevalence of CRPS patients with less favorable outcomes. The diagnosis by a psychiatrist allows the objectification of psychological disorders as most previous studies were limited to the use of questionnaires.7 Contrary to studies that have chosen chronic low back pain as a control,54 our comparative group is very similar, which allows a more judicious comparison between groups.
Our study has also several limitations. First, our sample is mainly composed of men, whereas women show a higher propensity to develop CRPS.3 The predominance of men is explained by our setting, which mainly admits workers from the secondary economic sector. This may limit the generalizability of our findings. However, it is especially relevant to investigate this population, since these patients are at risk of suffering from hand trauma with consequences that can be particularly severe. Second, our study used different sets of CRPS criteria,35–37 as others have done before.33 We hope that this limitation is at least partially offset by the fact that all diagnoses were confirmed by the same physician, who has many years of clinical experience and expertise in the field of CRPS (MK). Moreover, analyses conducted in the subgroup of CRPS patients using the Budapest Criteria (N=57) showed a comparable relationship between BPS complexity and psychiatric comorbidity compared to the whole cohort of CRPS patients in the multiple logistic regression (adjusted for age, sex, and pain) (See Supplementary Table 2). Third, the data were derived from patients with a CRPS sufficiently resistant to treatment to justify sustained interdisciplinary inpatient care, which represents only a portion of patients with CRPS.
Conclusion
Psychiatric comorbidities were diagnosed in 29% of patients suffering from CRPS of the hand, with mood disorders accounting for the majority of diagnoses. We found no statistical differences between the CRPS and non-CRPS groups in terms of psychiatric comorbidity and BPS complexity, except for the higher disability in CRPS patients. The INTERMED total score, as well as the scores of its four dimensions were associated with the presence of psychiatric comorbidity. The OR of having psychiatric comorbidity in relation to the INTERMED total as well as all four subscales were comparable between the two groups. The use of INTERMED to assess BPS complexity seems to be promising in screening the two groups and identifying those with psychosocial vulnerabilities and in orienting interdisciplinary care.
Abbreviations
CRPS, Complex regional pain syndrome; PTSD, Post-traumatic stress disorder; BPS, Biopsychosocial; VAS, Visual Analog Scale; DASH, Disabilities of the Arm, Shoulder, and Hand; OR, Odds ratio; ICD, International Classification of Diseases; FND, Functional neurological disorder.
Data Sharing Statement
All datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This retrospective comparative study was approved by the ethics committee of the local medical association (Commission Cantonale Valaisanne d’Ethique Médicale (CCVEM 043/07)). Informed written consent was obtained from each patient involved in this study.
Acknowledgments
The authors wish to thank Dr. Jean Savoy for his careful reading of the draft of this text and his constructive comments. We would like to acknowledge of Dr. Marie Gartmann for her help with providing raw and additional data and the nursing team for conducting the INTERMED interview.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest and have no funding to declare.
References
1. Bruehl S. Complex regional pain syndrome. BMJ. 2015;351:h2730. doi:10.1136/bmj.h2730
2. Veldman PH, Reynen HM, Arntz IE, Goris RJ. Signs and symptoms of reflex sympathetic dystrophy: prospective study of 829 patients. Lancet. 1993;342(8878):1012–1016. doi:10.1016/0140-6736(93)92877-V
3. Scholz-Odermatt SM, Luthi F, Wertli MM, Brunner F. Direct health care cost and work incapacity related to complex regional pain syndrome in switzerland: a retrospective analysis from 2008 to 2015. Pain Med. 2019;20(8):1559–1569. doi:10.1093/pm/pnz030
4. Feliu MH, Edwards CL. Psychologic factors in the development of complex regional pain syndrome: history, myth, and evidence. Clin J Pain. 2010;26(3):258–263. doi:10.1097/AJP.0b013e3181bff815
5. Atkinson L, Vile A. Unravelling the complex regional pain syndrome enigma. Pain Med. 2020;21(2):225–229. doi:10.1093/pm/pnz150
6. de Mos M, Huygen FJ, Dieleman JP, Koopman JS, Stricker BH, Sturkenboom MC. Medical history and the onset of complex regional pain syndrome (CRPS). Pain. 2008;139(2):458–466. doi:10.1016/j.pain.2008.07.002
7. Beerthuizen A, Van‘t Spijker A, Huygen FJ, Klein J, de Wit R. Is there an association between psychological factors and the complex regional pain syndrome type 1 (CRPS1) in adults? A systematic review. Pain. 2009;145(1–2):52–59. doi:10.1016/j.pain.2009.05.003
8. Bean DJ, Johnson MH, Heiss-Dunlop W, Lee AC, Kydd RR. Do psychological factors influence recovery from complex regional pain syndrome type 1? A prospective study. Pain. 2015;156(11):2310–2318.
9. Brinkers M, Rumpelt P, Lux A, Kretzschmar M, Pfau G. Psychiatric disorders in complex regional pain syndrome (CRPS): the role of the Consultation-Liaison psychiatrist. Pain Res Manag. 2018;2018:2894360. doi:10.1155/2018/2894360
10. Vouilloz A, Deriaz O, Rivier G, Gobelet C, Luthi F. Biopsychosocial complexity is correlated with psychiatric comorbidity but not with perceived pain in complex regional pain syndrome type 1 (algodystrophy) of the knee. Joint Bone Spine. 2011;78(2):194–199. doi:10.1016/j.jbspin.2010.07.006
11. Monti DA, Herring CL, Schwartzman RJ, Marchese M. Personality assessment of patients with complex regional pain syndrome type I. Clin J Pain. 1998;14(4):295–302. doi:10.1097/00002508-199812000-00005
12. Rommel O, Willweber-Strumpf A, Wagner P, Surall D, Malin JP, Zenz M. [Psychological abnormalities in patients with complex regional pain syndrome (CRPS)]. Schmerz. 2005;19(4):272–284. [Article in German]
13. Klinger R, Denecke H, Glier B, et al. [Quality control in the therapy of chronic pain. Results obtained by a task force of the German Section of the International Association for the Study of Pain on psychological assessment of chronic pain. XI. Assessment and multiaxial classification of pain]. Schmerz. 1997;11(6):378–385. [Article in German]
14. Speck V, Schlereth T, Birklein F, Maihofner C. Increased prevalence of posttraumatic stress disorder in CRPS. Eur J Pain. 2017;21(3):466–473. doi:10.1002/ejp.940
15. Swiss Health Observatory. Available from: https://www.obsan.admin.ch/fr/publications/comorbidite-somato-psychique-dans-les-hopitaux-suisses-de-soins-aigus.
16. Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196(4286):129–136. doi:10.1126/science.847460
17. World Health Organization. ICF: international classification of functioning, disability and health. Available from: http://www.who.int/classification/icf.
18. Wade D. Complexity, case-mix and rehabilitation: the importance of a holistic model of illness. Clin Rehabil. 2011;25(5):387–395. doi:10.1177/0269215511400282
19. Plsek PE, Greenhalgh T. Complexity science: the challenge of complexity in health care. BMJ. 2001;323(7313):625–628. doi:10.1136/bmj.323.7313.625
20. Wilson T, Holt T, Greenhalgh T. Complexity science: complexity and clinical care. BMJ. 2001;323(7314):685–688. doi:10.1136/bmj.323.7314.685
21. Wade DT, Halligan PW. The biopsychosocial model of illness: a model whose time has come. Clin Rehabil. 2017;31(8):995–1004. doi:10.1177/0269215517709890
22. Huyse FJ, Lyons JS, Stiefel FC, et al. “INTERMED”: a method to assess health service needs. I. Development and reliability. Gen Hosp Psychiatry. 1999;21(1):39–48. doi:10.1016/S0163-8343(98)00057-7
23. Huyse FJ, de Jonge P, Lyons JS, Stiefel FC, Slaets JP. INTERMED: a tool for controlling for confounding variables and designing multimodal treatment. J Psychosom Res. 1999;46(4):401–402.
24. Stiefel FC, de Jonge P, Huyse FJ, et al. “INTERMED”: a method to assess health service needs. II. Results on its validity and clinical use. Gen Hosp Psychiatry. 1999;21(1):49–56. doi:10.1016/S0163-8343(98)00061-9
25. van Eck van der Sluijs JF, de Vroege L, van Manen AS, Rijnders CAT, van der Feltz-cornelis CM. Complexity assessed by the INTERMED in patients with somatic symptom disorder visiting a specialized outpatient mental health care setting: a cross-sectional study. Psychosomatics. 2017;58(4):427–436. doi:10.1016/j.psym.2017.02.008
26. Mazzocato C, Stiefel F, de Jonge P, Levorato A, Ducret S, Huyse FJ. Comprehensive assessment of patients in palliative care: a descriptive study utilizing the INTERMED. J Pain Symptom Manage. 2000;19(2):83–90. doi:10.1016/S0885-3924(99)00156-6
27. Ludwig G, Dobe-Tauchert P, Nonnast-Daniel B, et al. Assessing psychosocial vulnerability and care needs of pretransplant patients by means of the INTERMED. Z Psychosom Med Psychother. 2014;60(2):190–203.
28. Hoogervorst EL, de Jonge P, Jelles B, et al. The INTERMED: a screening instrument to identify multiple sclerosis patients in need of multidisciplinary treatment. J Neurol Neurosurg Psychiatry. 2003;74(1):20–24. doi:10.1136/jnnp.74.1.20
29. Stiefel FC, de Jonge P, Huyse FJ, et al. INTERMED–an assessment and classification system for case complexity. Results in patients with low back pain. Spine. 1999;24(4):
30. Scerri M, de Goumoens P, Fritsch C, Van Melle G, Stiefel F, So A. The INTERMED questionnaire for predicting return to work after a multidisciplinary rehabilitation program for chronic low back pain. Joint Bone Spine. 2006;73(6):736–741. doi:10.1016/j.jbspin.2005.12.012
31. Koch N, Stiefel F, de Jonge P, et al. Identification of case complexity and increased health care utilization in patients with rheumatoid arthritis. Arthritis Rheum. 2001;45(3):216–221. doi:10.1002/1529-0131(200106)45:3<216::AID-ART251>3.0.CO;2-F
32. de Jonge P, Hoogervorst EL, Huyse FJ, Polman CH. INTERMED: a measure of biopsychosocial case complexity: one year stability in multiple sclerosis patients. Gen Hosp Psychiatry. 2004;26(2):147–152. doi:10.1016/j.genhosppsych.2003.09.001
33. van Bussel CM, Stronks DL, Huygen FJ. Complex regional pain syndrome type I of the knee: a systematic literature review. Eur J Pain. 2014;18(6):766–773. doi:10.1002/j.1532-2149.2013.00434.x
34. van Bussel CM, Stronks DL, Huygen F. Clinical course and impact of complex regional pain syndrome confined to the knee. Pain Med. 2019;20(6):1178–1184. doi:10.1093/pm/pnz002
35. Merksey H, Bogduk N. Classification of Chronic Pain: Description of Chronic Pain Syndromes and Definitions of Pain Term.
36. Doury PC. Algodystrophy: a spectrum of disease, historical perspectives, criteria of diagnosis, and principles of treatment. Hand Clin. 1997;13(3):327–337.
37. Harden RN, Bruehl S, Perez RS, et al. Validation of proposed diagnostic criteria (the “Budapest Criteria”) for complex regional pain syndrome. Pain. 2010;150(2):268–274. doi:10.1016/j.pain.2010.04.030
38. Hudak PL, Amadio PC, Bombardier C. Development of an upper extremity outcome measure: the DASH (disabilities of the arm, shoulder and hand) [corrected]. The Upper Extremity Collaborative Group (UECG). Am J Ind Med. 1996;29(6):602–608. doi:10.1002/(SICI)1097-0274(199606)29:6<602::AID-AJIM4>3.0.CO;2-L
39. de Jonge P, Bauer I, Huyse FJ, Latour CH. Medical inpatients at risk of extended hospital stay and poor discharge health status: detection with COMPRI and INTERMED. Psychosom Med. 2003;65(4):534–541. doi:10.1097/01.PSY.0000077504.01963.1B
40. World Health Organization. The ICD-10 classification of mental and behavioural disorders. Available from: https://www.who.int/classifications/icd/en/bluebook.pdf.
41. Luthi F, Stiefel F, Gobelet C, Rivier G, Deriaz O. Rehabilitation outcomes for orthopaedic trauma individuals as measured by the INTERMED. Disabil Rehabil. 2011;33(25–26):2544–2552. doi:10.3109/09638288.2011.579223
42. Sorensen AA, Howard D, Tan WH, Ketchersid J, Calfee RP. Minimal clinically important differences of 3 patient-rated outcomes instruments. J Hand Surg Am. 2013;38(4):641–649. doi:10.1016/j.jhsa.2012.12.032
43. Park HY, Jang YE, Oh S, Lee PB. Psychological characteristics in patients with chronic complex regional pain syndrome: comparisons with patients with major depressive disorder and other types of chronic pain. J Pain Res. 2020;13:389–398. doi:10.2147/JPR.S230394
44. Popkirov S, Hoeritzauer I, Colvin L, Carson AJ, Stone J. Complex regional pain syndrome and functional neurological disorders - time for reconciliation. J Neurol Neurosurg Psychiatry. 2019;90(5):608–614. doi:10.1136/jnnp-2018-318298
45. Hill RJ, Chopra P, Richardi T. Rethinking the psychogenic model of complex regional pain syndrome: somatoform disorders and complex regional pain syndrome. Anesth Pain Med. 2012;2(2):54–59. doi:10.5812/aapm.7282
46. Harden RN, Oaklander AL, Burton AW, et al. Complex regional pain syndrome: practical diagnostic and treatment guidelines, 4th edition. Pain Med. 2013;14(2):180–229. doi:10.1111/pme.12033
47. Suzuki SI, Takei Y. Psychosocial factors and traumatic events. In: Gellman MD, Turner JR, editors. Encyclopedia of Behavioral Medicine. New York, NY: Springer; 2013.
48. McEwen BS. Stressed or stressed out: what is the difference? J Psychiatry Neurosci. 2005;30(5):315–318.
49. de Jonge P, Hadj FB, Boffa D, et al. Prevention of major depression in complex medically ill patients: preliminary results from a randomized, controlled trial. Psychosomatics. 2009;50(3):227–233. doi:10.1176/appi.psy.50.3.227
50. Bass C, Yates G. Complex regional pain syndrome type 1 in the medico-legal setting: high rates of somatoform disorders, opiate use and diagnostic uncertainty. Med Sci Law. 2018;58(3):147–155. doi:10.1177/0025802418779934
51. Beerthuizen A, Stronks DL, Huygen FJ, Passchier J, Klein J, Spijker AV. The association between psychological factors and the development of complex regional pain syndrome type 1 (CRPS1)–a prospective multicenter study. Eur J Pain. 2011;15(9):971–975. doi:10.1016/j.ejpain.2011.02.008
52. van Reedt Dortland AKB, Peters LL, Boenink AD, et al. Assessment of biopsychosocial complexity and health care needs: measurement properties of the INTERMED self-assessment version. Psychosom Med. 2017;79(4):485–492. doi:10.1097/PSY.0000000000000446
53. Stiefel F, Zdrojewski C, Bel Hadj F, et al. Effects of a multifaceted psychiatric intervention targeted for the complex medically ill: a randomized controlled trial. Psychother Psychosom. 2008;77(4):247–256. doi:10.1159/000129658
54. Bean DJ, Johnson MH, Kydd RR. Relationships between psychological factors, pain, and disability in complex regional pain syndrome and low back pain. Clin J Pain. 2014;30(8):647–653. doi:10.1097/AJP.0000000000000007
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.