Back to Journals » Cancer Management and Research » Volume 15
Pseudoprogression Disease in a Patient with Small Cell Lung Cancer on Immune Checkpoint Inhibitor Therapy
Authors Zhu W, Wu L, Wu J, Lin S, Fang C ![]() , Zhang H
, Zhang H
Received 21 April 2023
Accepted for publication 22 August 2023
Published 1 September 2023 Volume 2023:15 Pages 905—911
DOI https://doi.org/10.2147/CMAR.S418116
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Kenan Onel
Wanshan Zhu, Lexia Wu, Jiaming Wu, Sihong Lin, Cantu Fang, Huatang Zhang
Zhongshan Hospital of Traditional Chinese Medicine Affiliated to Guangzhou University of Traditional Chinese Medicine, Zhongshan, Guangdong Province, People’s Republic of China
Correspondence: Huatang Zhang, Email [email protected]
Abstract: Small cell lung cancer (SCLC) accounts for approximately 15% of all lung cancers and is on the rise annually. It is characterized by low differentiation, high malignancy, and rapid growth. Consequently, treatment options are limited, and the patient’s prognosis is poor. The emergence of immunotherapy has partially improved the survival and prognosis of SCLC patients. However, a unique response known as “pseudoprogression” during immunotherapy has raised concerns. The occurrence of tumor enlargement despite a positive response to immune checkpoint inhibitor therapy undoubtedly affects the assessment of clinical drug efficacy and the selection of subsequent treatment strategies. In this article, we analyze a clinical case of pseudoprogression in a patient with SCLC who received immune therapy (Durvalumab). Currently, there is insufficient evidence-based medicine to guide the diagnosis, differentiation and subsequent treatment strategies for pseudoprogression in SCLC following immunotherapy. Through this case report and literature review, we aim to provide diagnostic and therapeutic insights for the clinical use of immunotherapy in advanced SCLC. Additionally, we hope that fellow readers of this article can engage in further collaborative discussions through more clinical research.
Keywords: small cell lung cancer, immunotherapy, pseudoprogression
Introduction
Small cell lung cancer (SCLC) is an “immunologically cold tumor”, and the efficacy of monotherapy immunotherapy has been less than satisfactory in the past. With continuous in-depth research and exploration, the application of immune checkpoint inhibitors (ICIs) in SCLC patients has gradually matured, and an increasing number of patients are benefiting from immunotherapy. However, among patients receiving immunotherapy, a significant portion experience an atypical response known as “pseudoprogression”. Pseudoprogression is essentially a unique manifestation of effective immunotherapy. Distinguishing between patients with pseudoprogression and true disease progression after immunotherapy is challenging. Currently, there is no standardized definition, uniform diagnostic criteria, or treatment strategy for pseudoprogression, posing a new challenge to clinical practice.
This article aims to report a case of pseudoprogression in a patient with SCLC after immunotherapy and to discuss its underlying mechanisms, diagnostic criteria, and treatment strategies. The goal is to assist clinical physicians in dealing with suspected cases of pseudoprogression in patients with SCLC after immunotherapy by providing relevant reference cases, enhancing awareness of pseudoprogression following immunotherapy in SCLC, and ultimately improving the assessment of disease progression and the safety and efficacy of immunotherapy in the treatment process for SCLC patients.
Case Report
Patient Information
The patient is a female who was admitted on January 8, 2021, due to “repeated cough and expectoration for 3 months, worsening for 3 days”. She had no significant medical history, family history of tumors, or smoking history. Physical examination revealed no visibly enlarged lymph nodes. The cardiopulmonary examination was unremarkable. CT scan on January 13, 2021, showed: 1. Suspected left lower lobe lung cancer (maximal cross-sectional size approximately 70mm × 50mm) with mediastinal lymph node metastasis and obstructive inflammation. 2. A small amount of pleural effusion on the left side. A biopsy of the lesion in the left lower lobe of the lung indicated small-cell lung cancer. (Figure 1) Immunohistochemistry: left lower lung cancer (small cell carcinoma) with mediastinal lymph node metastasis cT4N3M0, stage IIIc. Gene detection: EGFR (-), ALK (-), ROS1 (-). Immunohistochemical results: CK (+), TTF1 (+), P63 (-), CgA (partial+), Syn (+), CD56 (+), Ki-67 (80–90%+).
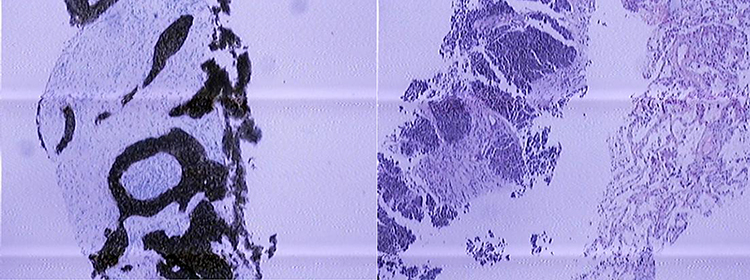 |
Figure 1 January 8, 2021 Pathologic Immunohistochemistry. Pathologic Immunohistochemistry result: Left lower lung cancer (small cell lung carcinoma) with mediastinal lymph node metastasis (cT4N3M0, Stage IIIc). |
Diagnosis and Treatment Process
The patient was diagnosed with left lower lobe lung cancer (small cell carcinoma) with mediastinal lymph node metastasis, cT4N3M0, stage IIIc (limited stage). Considering the large size of the primary lesion, neoadjuvant chemotherapy was planned before further treatment. Following the 2021 NCCN guidelines, the patient received the EP regimen from January 31, 2021, to April 20, 2021: Etoposide injection 110mg on days 1–3, Cisplatin injection 30mg on days 1–3, every 21 days for 4 cycles. After treatment, a partial response (PR) was observed. Subsequently, from May 19, 2021, to June 23, 2021, the patient underwent localized radiation therapy for lung cancer using VMAT (Volumetric Modulated Arc Therapy), GTVnx: imaging left lung mass, GTVnd: imaging enlarged mediastinal lymph nodes. PTVnx:5500cGy/25Fr, 220cGy/Fr; PTVnd: 5500cGy/25Fr, 220cGy/Fr. On July 27, 2021, the EP regimen was continued with adjusted doses of Etoposide 100mg and Oxaliplatin 10mg, but on August 27, 2021, due to chemotherapy intolerance, the patient received monotherapy with Etoposide 100mg.
Durvalumab was approved in December 2019 for the treatment of unresectable stage III non-small cell lung cancer patients who did not experience disease progression after platinum-based chemotherapy and concurrent radiotherapy In China. Therefore, on September 26, 2021, Durvalumab was initiated at a dose of 1000mg every 21 days for immunotherapy. On December 29, 2021, the patient underwent microwave ablation for suspected lung malignant nodules (?). On March 3, 2022, prophylactic radiotherapy was given to the brain. The whole process of IMRT, CTV: the whole brain. PTV:3000cGy/12Fr, 250cGy/Fr. After radiotherapy, he was discharged without any discomfort. From May 11, 2022, the patient continued regular immunotherapy with Durvalumab 1000mg every 21 days. However, subsequent immunotherapy was temporarily halted due to infection with novel coronavirus pneumonia (COVID-19).
Results
Following a comprehensive treatment regimen consisting of four cycles of EP chemotherapy and localized lung cancer radiation therapy, a follow-up chest CT scan on June 21, 2021, revealed that the left lower lobe lung cancer had reduced in size compared to before (maximal cross-sectional size approximately 22mm × 16mm). Multiple metastatic lesions and obstructive inflammation in the left hilum and mediastinum remained largely unchanged. After two additional rounds of chemotherapy and four cycles of Durvalumab immunotherapy, a follow-up chest CT scan on December 27, 2021, showed an enlargement of the left lower lobe nodule (maximal cross-sectional size approximately 24mm × 21mm), as well as persistent enlargement of multiple lymph nodes in the bilateral hilum and mediastinum.
The combined effects of immunotherapy and ablation appeared to induce significant anti-tumor activity and promote a transformation of the tumor to a “hot tumor”, enhancing the immune response. A microwave ablation procedure was performed on December 29, 2021, for the left lower lobe lung mass. The patient showed no significant discomfort post-surgery and continued with Durvalumab immunotherapy.
On May 11, 2022, a follow-up chest CT scan after comprehensive treatment for left lower lobe lung cancer showed changes after radiofrequency ablation, with the original lesion slightly larger (maximal cross-sectional size approximately 28mm × 20mm) and some reduction in surrounding inflammation. Multiple new small nodules were observed in both lungs, and a recommendation for further evaluation was given. Post-microwave ablation changes often include necrosis, which can lead to bleeding and increased swelling of surrounding tissues, though no significant enhancement was observed, suggesting no immediate tumor progression. Immunotherapy with Durvalumab was resumed.
On August 5, 2022, a follow-up chest CT scan showed further enlargement of the left lower lobe mass (now approximately 46mm × 37mm) with heterogeneous enhancement. Multiple linear areas of increased density were observed adjacent to the lesion, and the overall findings were consistent with previous scans. A percutaneous lung mass biopsy under CT guidance was performed on August 17, 2022. Pathological examination indicated fibroproliferation in the alveolar septa with minimal infiltrating inflammatory cells and localized necrosis. Immunohistochemistry revealed CD4+ (approximately 50%+) and CD8+ (approximately 70%+) T lymphocytes. (Figure 2) The patient’s CT scan suggested tumor enlargement, and the biopsy findings indicated changes in immune cell infiltration, potentially due to immunotherapy or post-radiation fibrosis. The assessment leaned toward pseudoprogression, prompting the continuation of immunotherapy.
 |
Figure 2 August 17, 2022 Pathological of the puncture biopsy of left lung tumor. Pathological Result: The fibrous tissue of the alveolar septa proliferated, with a few inflammatory cells infiltrating, necrosis visible locally, and no heterotypic cells found. Supplementary immunohistochemistry results: CD4 (about 50%+), CD4 (about 70%+). |
In December 2022, due to a novel coronavirus pneumonia infection, immunotherapy was temporarily suspended. A follow-up chest CT scan on December 29, 2022, compared to August 5, 2022, showed further enlargement of the left lower lobe mass (now approximately 61mm × 45mm) with mixed density. New scattered blurry patches were observed beneath the pleura in both lungs, and a slight increase in pleural effusion was noted on both sides. Pericardial effusion was also observed, and the overall findings were consistent with previous scans. Symptomatic treatment was administered for a week, leading to a subsequent follow-up chest CT scan that showed a reduction in the size of the left lower lobe mass (now approximately 53mm × 40mm), improved inflammation in both lungs and decreased pleural effusion on both sides. As of now, no recurrence, disease progression, or significant adverse reactions have been observed (Figure 3).
 |
Figure 3 Timeline. |
Discussion
In the case of this patient, the re-examination of imaging after immunotherapy indicated a significant increase in tumor lesions, suggesting possible disease progression. However, at this point, whether it is true disease progression, the gold standard for distinguishing true and false progression in pathological diagnosis with immunotherapy, and whether continued immunotherapy is needed after imaging suggests disease progression, and if treatment adjustments are necessary, all raise questions. The diagnosis of inflammatory infiltration through biopsy may not definitively confirm false progression. Additionally, the patient was infected by novel coronavirus pneumonia, and follow-up imaging showed a slight increase in lung cancer tumor lesions. This increase could potentially be attributed to disease progression or worsened inflammation due to viral pneumonia. Determining the efficacy and progression of immunotherapy in this patient presents various possibilities and uncertainties that warrant further exploration.
Application of Immunotherapy in Small Cell Lung Cancer
Small cell lung cancer’s rapid growth, strong invasiveness, quick progression, and multiple gene mutations without a predominant mutation pose limitations on targeted therapies. While early-stage small cell lung cancer is sensitive to radiotherapy and chemotherapy, recurrence rates are high, with rapid disease progression often leading to relapse or metastasis within a year, resulting in lower survival rates compared to non-small cell lung cancer patients.1 The era of immunotherapy has introduced successful applications of immune checkpoint inhibitors in lung cancer, particularly in small-cell lung cancer patients.
The role of immunotherapy in lung cancer treatment has grown significantly.2 PD-L1 inhibitors like atezolizumab and durvalumab have been approved for small-cell lung cancer treatment. For limited-stage small-cell lung cancer, the advantages of prolonged immune therapy and low toxicity have led to the exploration of immune maintenance therapy following concurrent chemoradiotherapy.3 Recent studies also indicate that immune consolidation therapy after concurrent chemoradiotherapy can improve survival in limited-stage small-cell lung cancer patients. Immunotherapy in combination with chemotherapy has made breakthroughs in first-line treatment and is now a standard option for extensive-stage small-cell lung cancer. Combination therapies, including immunotherapy with chemotherapy, radiation therapy, and anti-angiogenesis agents, are being investigated to enhance immune response effectiveness of “cold tumor” to “hot tumor”. Studies like IMpower133,4 CASPIAN,5 and ASTRUM-0056 highlight the effectiveness of immunotherapy in combination with chemotherapy and targeted therapy. Further exploration is needed for various immunotherapy combination models.
“Pseudoprogression” in Lung Cancer Immunotherapy
Immunotherapy has demonstrated promising anti-tumor activity and manageable adverse reactions in both non-small cell lung cancer and small cell lung cancer, leading to its increasing use. However, atypical clinical responses, such as “pseudoprogression”, can occur during immunotherapy. Pseudoprogression refers to cases where tumor lesions appear larger or new lesions emerge on imaging after immunotherapy, which is later confirmed by biopsy to be necrosis or infiltrating inflammatory cells. Subsequently, the tumor burden decreases. Possible mechanisms for “pseudoprogression” post-immunotherapy include the release of antigens from dying tumor cells, increased infiltration of inflammatory cells, inflammation-induced edema and bleeding, and the accumulation of necrotic byproducts in local lesions.7
Pseudoprogression is rare, occurring in 2–8% of late-stage non-small cell lung cancer patients receiving anti-PD-1/PD-L1 treatment, and it may not be justified to use diagnostic CT scan extensively outside of clinical trials, as recommended by iRECIST. If there is a lack of reliable therapeutic efficacy or biomarkers for disease progression, diagnosis relies on clinical symptom evaluation, physical condition assessment, and close monitoring of imaging. Various forms of Pseudoprogression can occur in lung cancer patients during immunotherapy, making it difficult to distinguish from true disease progression after unsuccessful anti-tumor treatment.
Continuation of Treatment Beyond Disease Progression (TBP) in Immunotherapy
Given the unique features of “Pseudoprogression” during immunotherapy, the potential benefits of continuing treatment beyond disease progression (TBP) require further exploration. The OAK study8 investigated the benefits of continuing immune checkpoint inhibitor therapy with atezolizumab after disease progression and found significant overall survival (OS) benefits compared to changing treatment strategies or no treatment. It also indicated that TBP did not increase toxicity or safety risks. Patients should be re-evaluated with CT scans within 4–8 weeks to exclude confirmed disease progression and monitor toxicity. Clinical improvement or stability, combined with image findings, can guide the decision to continue TBP.9
Factors like inflammation-induced changes due to other causes in lung cancer patients can also affect disease assessment post-immunotherapy. This patient’s increased tumor lesion size after contracting novel coronavirus pneumonia raises questions about whether it’s slow disease progression during ongoing immunotherapy or exacerbated inflammation due to viral pneumonia. Studies suggest that cancer patients undergoing immunotherapy, especially immune checkpoint inhibitors, might experience worsened disease progression and a higher risk of cytokine storms upon contracting COVID-19.10 COVID-19 infection might exacerbate pulmonary inflammation, causing inflammatory lesion development or enlargement, which could subsequently resolve as the inflammation diminishes.
Assessment and Discrimination of Immunotherapy Efficacy and Progression in SCLC
With ongoing research, the application of immune checkpoint inhibitors in SCLC is maturing, benefiting an increasing number of patients. Although immune combination therapies improve survival and prognosis to a certain extent, effective biomarkers for immunotherapy are lacking. Identifying patients who will benefit from immunotherapy is crucial, affecting treatment decisions and avoiding ineffective therapies. In the exploration of biomarkers, KEYNOTE-604,11 CASPIAN,5 IMPower133,4 and other combined immunotherapy studies found that patients with either high or low levels of PD-L1 expression can benefit from it. Biomarkers like tumor mutation burden (TMB), tumor-infiltrating lymphocytes, and circulating tumor cells have also been explored for predicting the efficacy of ICI response.12
As the role of immune checkpoint inhibitors grows in lung cancer treatment, accurate identification and evaluation of Pseudoprogression becomes more important. While pathological examination is the gold standard for diagnosing Pseudoprogression, its accuracy can be affected by tumor heterogeneity. Puncture biopsy is only a part of the tissue, which cannot represent the overall picture of the tumor, and will affect the accuracy of pathological diagnosis. Additionally, post-ablation changes can obscure residual tumor enhancement and affect imaging interpretation. Combined with the fact that the patient had undergone microwave ablation of lung cancer, the lesions after the operation were enlarged, and the inflammatory exudation of the tissue led to the appearance of a frosted glass-like reaction zone around, delaying the tumor shrinking. The congestion and inflammatory exudation of the ablation area may mask the enhancement of the residual tumor, which may affect the judgment of imaging diagnosis and the selection of puncture sample. A biopsy also carries certain limitations and may cause patient discomfort. Blood-based biomarkers such as plasma CXCL2, MMP2,13 and genomic instability number (GIN)14 have shown potential for distinguishing Pseudoprogression from true progression. In clinical practice, combining blood-based markers with clinical evaluation and imaging monitoring can guide continued immune therapy when tumor lesions increase or new lesions appear on follow-up imaging after immunotherapy.
Therefore, confirming Pseudoprogression requires comprehensive consideration of clinical presentation, blood markers, imaging, and pathological biopsy. Integrating multiple standards can accurately evaluate immune therapy efficacy and disease progression.
Conclusion
This case report highlights the limitations in diagnosing the true and false progression of diseases after immunotherapy, showcasing the diverse clinical manifestations of pseudoprogression. Therefore, further prospective research is needed to advance the evaluation, diagnosis, and discrimination of pseudoprogression in lung cancer or other solid tumors. With the widespread application of immunotherapy in small-cell lung cancer, efforts should be made to address pseudoprogression events during immunotherapy. This includes actively exploring more effective methods for distinguishing, diagnosing, clinically evaluating, managing, and strategizing treatments. These efforts aim to aid in prognosis assessment, treatment monitoring, reduction of non-beneficial cases, and cessation of ineffective ongoing immune therapies for small cell lung cancer patients.
Abbreviations
SCLC, small cell lung cancer; ICI, the immune checkpoint inhibitor; CT, computed tomography; COVID-19, coronavirus pneumonia; TBP, treatment beyond disease progression; OS, overall survival; TMB, tumor mutation burden; GIN, genomic instability number.
Data Sharing Statement
This case report contains clinical data from the electronic medical records from Zhongshan Hospital of Traditional Chinese Medicine Affiliated to Guangzhou University of Traditional Chinese Medicine, China. Additional information is available from the corresponding author upon reasonable request.
Consent for Publication
Written informed consent was obtained from patient for publication of this case report and any accompanying images.
Acknowledgments
The researchers received no grants from funding agencies in either the public, commercial, or not-for-profit sectors, for this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Nesbit EG, Leal TA, Kruser TJ. What is the role of radiotherapy for extensive-stage small cell lung cancer in the immunotherapy era? Transl Lung Cancer Res. 2019;8(Suppl 2):S153–S162. doi:10.21037/tlcr.2019.05.01
2. Chiou VL, Burotto M. Pseudoprogression and immune-related response in solid tumors. J Clin Oncol. 2015;33(31):3541–3543. doi:10.1200/JCO.2015.61.6870
3. El Sayed R, Blais N. Immunotherapy in extensive-stage small cell lung cancer. Curr Oncol. 2021;28(5):4093–4108. doi:10.3390/curroncol28050347
4. Liu SV, Reck M, Mansfield AS, et al. Updated overall survival and PD-L1 subgroup analysis of patients with extensive-stage small-cell lung cancer treated with atezolizumab, carboplatin, and etoposide (IMpower133). J Clin Oncol. 2021;39(6):619–630. doi:10.1200/JCO.20.01055
5. Goldman JW, Dvorkin M, Chen Y, et al. Durvalumab, with or without tremelimumab, plus platinum-etoposide versus platinum-etoposide alone in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): updated results from a randomised, controlled, open-label, Phase 3 trial. Lancet Oncol. 2021;22(1):51–65. doi:10.1016/S1470-2045(20)30539-8
6. Cheng Y, Han L, Wu L, et al. Effect of first-line serplulimab vs placebo added to chemotherapy on survival in patients with extensive-stage small cell lung cancer: the ASTRUM-005 randomized clinical trial. JAMA. 2022;328(12):1223–1232. doi:10.1001/jama.2022.16464
7. West HJ. JAMA oncology patient page. Immune checkpoint inhibitors. JAMA Oncol. 2015;1(1):115. doi:10.1001/jamaoncol.2015.0137
8. Gandara DR, von Pawel J, Mazieres J, et al. Atezolizumab treatment beyond progression in advanced NSCLC: results from the randomized, Phase III OAK study. J Thorac Oncol. 2018;13(12):1906–1918. doi:10.1016/j.jtho.2018.08.2027
9. Wang P, Yin T, Zhao K, Yu J, Teng F. Efficacy of single-site radiotherapy plus PD-1 inhibitors vs PD-1 inhibitors for oligometastatic non-small cell lung cancer [published correction appears in J Cancer Res Clin Oncol. 2021 Dec 8]. J Cancer Res Clin Oncol. 2022;148(5):1253–1261. doi:10.1007/s00432-021-03849-3
10. Khoury E, Nevitt S, Madsen WR, Turtle L, Davies G, Palmieri C. Differences in outcomes and factors associated with mortality among patients with SARS-CoV-2 infection and cancer compared with those without cancer: a systematic review and meta-analysis. JAMA Netw Open. 2022;5(5):e2210880. doi:10.1001/jamanetworkopen.2022.10880
11. Rudin CM, Awad MM, Navarro A, et al. Pembrolizumab or placebo plus etoposide and platinum as first-line therapy for extensive-stage small-cell lung cancer: randomized, double-blind, Phase III KEYNOTE-604 study. J Clin Oncol. 2020;38(21):2369–2379. doi:10.1200/JCO.20.00793
12. Ready N, Farago AF, de Braud F, et al. Third-line nivolumab monotherapy in recurrent SCLC: checkMate 032. J Thorac Oncol. 2019;14(2):237–244. doi:10.1016/j.jtho.2018.10.003
13. Matsuo N, Azuma K, Hattori S, et al. Association between soluble immune mediators and tumor responses in patients with nonsmall cell lung cancer treated with anti-PD-1 inhibitor. Int J Cancer. 2019;144(5):1170–1179. doi:10.1002/ijc.31923
14. Jensen TJ, Goodman AM, Kato S, et al. Genome-wide sequencing of cell-free DNA identifies copy-number alterations that can be used for monitoring response to immunotherapy in cancer patients. Mol Cancer Ther. 2019;18(2):448–458. doi:10.1158/1535-7163.MCT-18-0535
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.