Back to Journals » Advances in Medical Education and Practice » Volume 10
Provision of feedback to medical teachers on their educational performance: perspectives of internal medicine teachers
Authors Jamshidian S, Haghani F ![]() , Yamani N
, Yamani N ![]() , Sabri MR
, Sabri MR
Received 31 August 2018
Accepted for publication 9 January 2019
Published 26 February 2019 Volume 2019:10 Pages 85—94
DOI https://doi.org/10.2147/AMEP.S184178
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Md Anwarul Azim Majumder
Sepideh Jamshidian,1 Fariba Haghani,1 Nikoo Yamani,1 Mohammad Reza Sabri2
1Department of Medical Education, Medical Education Research Center, Isfahan University of Medical Sciences, Isfahan, Iran; 2Department of Pediatrics, Pediatric Cardiovascular Research Center, Isfahan Cardiovascular Research Institute, Isfahan University of Medical Sciences, Isfahan, Iran
Purpose: Teachers’ evaluation and giving feedback on their educational performance has been a great concern of all medical universities, especially in clinical settings. The opinion of teachers (as feedback recipients) about the feedback process and its usefulness is very critical for the feedback to be effective. This study aimed to identify the perspectives of internal medicine teachers on receiving feedback about their educational performance.
Materials and methods: In a qualitative content analysis study, from October 2016 to July 2017, 16 semi-structured interviews were conducted with the internal medicine teachers selected purposefully. Recorded and transcribed interviews were analyzed using an inductive content analysis approach.
Results: Three themes emerged: “Feedback elements”, “Feedback outcomes”, and “Effective feedback strategies”. The first includes two categories: human and background elements. “Human elements” consists of three subcategories including “Sources of feedback”, “Feedback provider”, and “Feedback recipient”. “Background elements” includes three subcategories which are the underlying conditions in the feedback process: “Performing performance”, “Data collection”, and “Giving feedback”. The third theme contains three categories: “Developing a systemic approach to feedback”, “Appropriate educational policies for teacher recruitment and promotion”, and “Using others’ experiences”.
Conclusion: The current study represents clinical teachers’ opinions about the feedback elements, issues affecting the feedback process, and their recommendations for effective feedback. All these helped the researchers to develop a feedback cycle, which starts with “performing the performance” and continues with “performance data collection”, “data analysis and interpretation”, “feedback presentation”, and “feedback follow-up”. The researchers recommend the feedback officials to study teachers’ opinions obtained in the current study and use the feedback cycle to provide more effective feedback.
Keywords: feedback, clinical teacher, educational performance, feedback cycle, feedback elements
A Letter to the Editor has been published for this article.
Introduction
Feedback is a familiar concept in our daily life1 that first came from engineering.2 Currently, it is applied in many disciplines with a wide range of definitions, most of which imply feedback as information about the gap between the current and the expected function of a system, whereby feedback is used to reduce the gap.3
In education, feedback is defined as an interactive process with the aim of informing learners about their performance,4 provided by a person such as the teacher, classmate, parent, and so on to improve performance.5,6
There is much evidence to confirm the efficacy of feedback for faculty development. Many educational centers across the world have systems that provide feedback to teachers with the aim of improving their performance.7 In a study at the University of Wisconsin, frequent written feedback given to teachers over a period of 12 months resulted in a significant increase in teacher evaluation scores, especially for those who had lower scores before intervention.8
In Skeff’s study, >75% of those who received intensive feedback reported a remarkable increase in their awareness about positive and negative points of their teaching. They also stated that their willingness toward evaluation and improvement of their teaching skills has increased and their passion for being a teacher has enhanced.9
Although substantial evidence indicates the positive effect of feedback on teachers’ performance, feedback provision is comparable to a double-edged sword.10 Success depends on several factors such as cultural background and characteristics of feedback recipients, feedback provider, feedback presentation method, and feedback’s content; neglecting them has negative effects on teachers and their performance.11 Merely informing teachers about their evaluation scores does not help them to improve their performance; this unfacilitated feedback might also lead to negative emotional reactions such as denial and defense, preventing them to think about feedback content.12
Teacher evaluation and feedback provision on their educational performance have been a great concern of medical universities.13 The Education Development Center (EDC) of Isfahan University of Medical Sciences (IUMS), like other medical universities in Iran, has been in charge of teacher evaluation since 1992. Data sources in clinical teacher evaluation are learners and university officials. Data collection is done through Likert scale questionnaires completed by residents and sometimes by interns and university officials. The only feedback provided to teachers is a written report about the results of teacher evaluation, which contain students’ and officials’ scores about teacher performance.
Overall, what is presented to Iranian clinical teachers as feedback does not fall into the definition of feedback as it is not interactive, and also, its main goal is decision-making rather than performance improvement and contains only some scores without any performance description or recommendation. So, one of the main concerns of EDC in IUMS in recent years has been providing effective feedback to clinical teachers about their educational performance. To achieve this, an action research was designed by researchers. Among the clinical departments, internal medicine was chosen as the participant because it is a major discipline for general practitioners, and duration of the rotation is more than others.
In spite of valuable resources available describing how to provide effective feedback, most resources have emphasized on the provision of feedback in line with the background setting of the feedback recipients. So, it was necessary to investigate feedback setting, especially from the viewpoint of their recipients, clinical teachers. Current study, as the first part of the action research, aimed to identify clinical teachers’ perspectives about receiving feedback on their educational performance.
Materials and methods
A qualitative study using semi-structured interviews was conducted in the internal medicine department of IUMS, Iran, from October 2016 to July 2017.
The reason for choosing qualitative rather than quantitative method was to achieve a deep understanding about feedback process from clinical teachers’ point of view without directing them to a particular direction. In addition, qualitative approaches are mostly used for topics that have been less studied before. Although feedback has been addressed in many studies, feedback from clinical teachers’ viewpoint, especially in IUMS, has not been considered yet. Also, considering the diversity of viewpoints – which is necessary in qualitative approaches – was important for researchers. Due to the challenging nature of the feedback, it seemed necessary to have a good communication with the participants, explain about the feedback, and request for their opinions and experiences; again, qualitative approaches are more in line with these features.
Using a purposive sampling strategy, the researcher (SJ) interviewed 16 clinical teachers with different work experiences, age, gender, and educational level. Department of Internal Medicine in IUMS has approximately 65 clinical teachers who work in four educational hospitals. One of the four hospitals, Al-Zahra Hospital, is more challenging for clinical teaching; so, we chose teachers working in this hospital. The researcher enrolled clinical teachers in the study with the help of internal medicine department. The researcher graduated from IUMS in General Medicine and has worked in EDC for several years. So, she is well acquainted with the clinical environment. She was already experienced in interviewing clinical teachers. To get the teachers involved, a formal letter from EDC introducing the researcher and an email containing some explanations about the project were sent to them. Before each interview, the researcher made the time and place arrangement and after that, she sent a letter of appreciation to every interviewee. Data analysis was performed after each interview and, if necessary, trigger questions were modified. Sample triggers for initiating and conducting the interviews were as follows:
- As a clinical teacher, how often do you receive feedback about your educational performance? From whom? How?
- How do you feel when you receive feedback about your highly assessed performance? How about your underperformance? What is your response immediately and sometime after that? Does feedback facilitate your performance improvement? What are the desired and undesired outcomes of receiving feedback for you? Which strategies do you suggest for presenting feedback?
All interviewees except one allowed recording the interviews. The recordings were listened and transcribed verbatim by the researcher (SJ). Data analysis was performed on inductive content analysis method. The purpose of inductive content analysis is to create categories for describing the phenomenon, to increase understanding, and to generate knowledge.14 The transcript was read through several times and then investigated to determine its meaning units, labeling each with a code. The codes were compared based on differences and similarities, and similar codes were grouped into one category. A process of reflecting on and discussing the categories resulted in unifying them into themes or dividing into subcategories. All steps of content analysis were reviewed by two other researchers, and the shortcomings that were raised in the coding method were corrected.
New participants were interviewed until data saturation was achieved, that is, until no additional theme related to study goals emerged.
This study was approved by the University/Regional Research Ethics Committee, Isfahan University of Medical Sciences and Health Services with approval ID 1395.3.719. Verbal informed consent was obtained from all participants under the supervision of Ethics Committee.
To ensure the privacy of the participants, all interviews were coded by the interviewer herself and were presented to other researchers by number. Also, in writing the article and other research reports, the researcher was careful enough not to point someone either explicitly or implicitly.
To ensure trustworthiness, the concepts credibility, dependability, and transferability were considered. Credibility is concerned with the intended focus of the research and represents how well data and processes of analysis address it.15 For credibility, participants with various work experiences and different genders were chosen to reach a wider variety of comments. Also, it was tried to choose the most appropriate method in order to collect sufficient data. Showing representative quotations from the transcribed text represents how well the data were labeled and sorted. Moreover, credibility could be guaranteed via long-term involvement of the researcher with the participants and checking the analysis method and themes emerging from interviews with two other researchers.
To achieve dependability, it is helpful to consider the degree to which data and researcher’s decisions change over time.15 In this study, although some changes occurred during the interviews, their main structure remained unchanged. These little changes were inevitable due to the qualitative nature of the study and the semi-structured interviews. To facilitate transferability, the culture and context of this study were explained, so that the reader can decide to what extent findings could be transferred to other settings. It seems that the findings could be applied for all medical teachers. Representative quotations will also enhance transferability.
Results
Sixteen (n=9 female) clinical teachers of internal medicine department (Endocrinology, Nephrology, Cardiology, General, Pulmonary Diseases, and Rheumatology sub-departments) with an average age of 44.1 years and a mean tenure of 7.8 years were interviewed. Fourteen of them were assistant professors, one was an associate professor, and one was a professor. The mean duration of interviews was 42 minutes.
Three themes emerged from 424 codes: “Feedback elements”, “Feedback outcomes”, and “Effective feedback strategies” (Table 1).
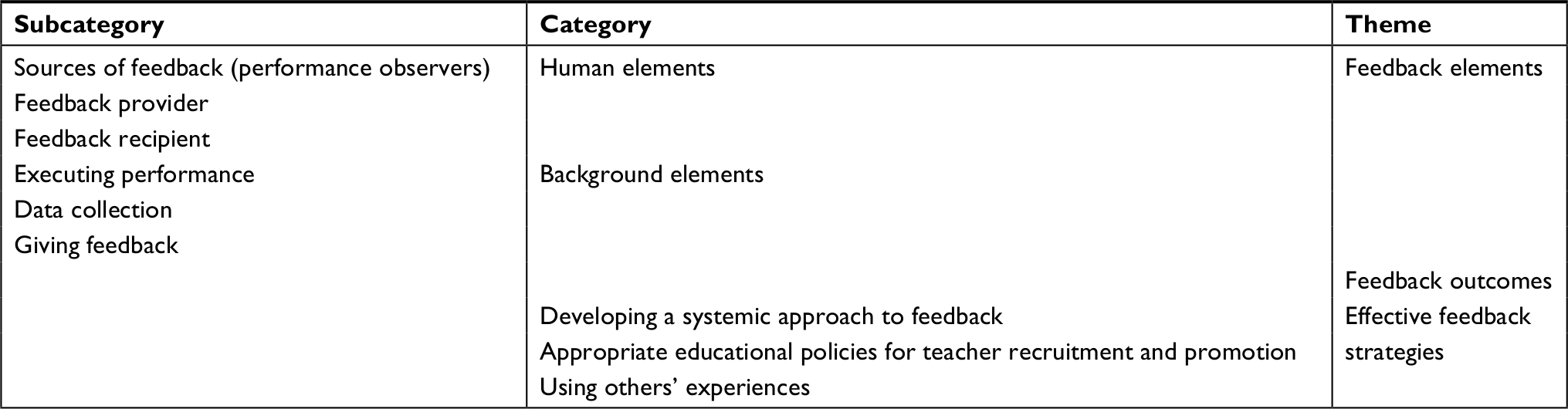 | Table 1 Subcategories, categories, and themes based on analysis of interviews |
Theme 1: Feedback elements
This theme represents essential elements in feedback process and is divided into two categories: “Human elements” and “Background elements”.
Category 1-1: Human elements
This consists of key people in the feedback process.
Subcategory 1-1-1: Sources of feedback (performance observers)
This subcategory describes the suitable sources of performance data based on which the feedback message should be prepared. According to the interviewees, the best people to comment on teaching performance are those who directly observe it, like medical students in all educational levels. As colleagues and nursing staff often do not observe their teaching performance directly, they are not appropriate to evaluate it; but they are suitable to comment on performances such as professional behavior of the teacher. Another data source that was raised involves experts in medical education; they could observe the teaching in a clinical setting or in the classroom and provide feedback to teachers.
A main concern participants pointed was that, although learners directly observe the teaching performance and could be the best evaluators in the field, their opinions are influenced by several factors; for instance, their interest in the subject, abilities, attitude toward education, commitment, and sometimes personal conflict with teachers.
Unfortunately, most residents prefer rotations with easy-going teachers, who never ask them about coming late or leaving soon […]. [P11]
Therefore, they believed for obtaining authentic data, it was necessary to pay attention to the number and variety of learners.
Subcategory 1-1-2: Feedback provider
According to participants, characteristics of the person who presents feedback is very critical in feedback efficacy; s/he should be a competent person in teaching, an expert in the subject matter with years of work experience, familiar with clinical setting, and competent in providing feedback.
Feedback provider should be a competent teacher not just someone who has more years of tenure […] I cannot accept feedback about my teaching from someone who him/herself is not a competent teacher. [P10]
The most important point in this regard was that the feedback recipient and the provider should hold a positive view of each other. If feedback recipient has a negative attitude toward the feedback provider, feedback will still not be effective, because the recipient feels that the purpose of feedback provision is judgment, not performance improvement.
Subcategory 1-1-3: Feedback recipient
Some characteristics of feedback recipients, such as personality, age, work experience, and attitude toward feedback, are influential in the feedback process. Also, teacher’s perception of change necessity is a critical factor. As they have many concerns about their patients and their career, sometimes their educational performance is neglected. The participants believed that most people hate to receive negative feedback and like their good performance to be pointed out by others, especially the teachers with some years of tenure, who think they are experienced enough for not requiring any feedback.
Almost all participants believed, despite the unhappy associations of negative feedback, that feedback is still essential, especially for less-experienced teachers, and that it improves clinical teaching, because sometimes people are unconsciously inattentive of their own performance.
I do not see my fault. I think I’m doing the best; if you do not tell me anything about my mistakes, I may continue them for years. [P8]
When someone strongly informs you about your mistake, it will remain in your mind forever and you’ll never do that again. [P13]
Although most participants believed in the usefulness of feedback, they did not appreciate to be under severe supervision.
It infuses bad feelings when you are under strict supervision […] I do not like they think that they can scare me. [P10]
Category 1-2: Background elements
This category contains three underlying conditions in the feedback process.
Subcategory 1-2-1: Executing performance
This shows the setting where the performance is observed while it is being carried out. This situation is affected by factors such as management problems and number and variety of patients and learners; therefore, a teacher’s performance might vary in two different educational institutions with the same students.
The clinical environment is an effective factor […]. Here, I’m very involved in patient care […]. I’m really sure that teaching in the previous center was more relaxed and students were much more satisfied. [P2]
In Khorshid hospital, a clinical round can be done easily, because all patients are in two or three room close together; in Alzahra, for a round, we should walk several kilometers in the hospital […]. The long distance between wards are really exhausting. [P12]
Subcategory 1-2-2: Data collection
This subcategory consists of participants’ opinions about time, place, situation, and methods of data collection and other factors influencing this process. According to them, it is necessary to explain the purpose of data collection to students or other sources of feedback data and reassure them about confidentiality of data. This is even more important when there is a relatively long interval between observing the teacher’s performance and collecting data. Although the usual method of data collection is completing the questionnaire, participants believed that interview or asking the students verbally is significantly a better approach to data collection, because the questionnaires are often completed carelessly. In oral questioning, students need to reflect on the questions and the probability of obtaining honest answers is greater. Most participants suggested using combination of qualitative and quantitative methods.
This is a complex process […]. Thus, it is overly simplistic to use only one method for data collection on teacher performance. [P2]
Using direct observation by an expert and videotaping are other suggestions for collecting reliable data. However, they might interfere with teaching and affect the teacher’s behavior.
They also emphasized precise data analysis and interpretation, especially when the results are not expected.
Subcategory 1-2-3: Giving feedback
Time, place, situation, privacy, content, and manner of presentation are essential elements in feedback presentation. For instance, participants wanted their feedback content show the comparison between their performance and predetermined criteria or their previous performance and not that of others. According to most participants, in spite of being time consuming, verbal feedback is better than written one because of the opportunity the teacher gets to express his/her own comments. They thought receiving only a feedback letter about underperformance leads to resistance against it and prevents the feedback from being accepted, especially for the first time one is receiving feedback. Conversely, a few participants thought that the written format is more effective because one has adequate time to consider the feedback letter. Meanwhile, some believed in a combination of verbal and written feedback.
About feedback content, most participants considered it frustrating when only the negative points of the performance are mentioned, leaving out the positive ones.
If they focus only on a few days that, for any reason, I couldn’t be very active, it would be disappointing to me […] because they do not see my efforts […]. We need to be seen by others. [P11]
In addition, it is not sufficient to merely mention what was wrong if the aim is to improve the performance; teachers desire to know how they could do better. Also, they emphasized on prioritizing the performance problems and focusing on top priorities in feedback content.
Theme 2: Feedback outcomes
This contains participants’ experiences about the outcomes of receiving feedback, including their immediate feelings and reactions or final decisions –which is related to feedback acceptance.
Feedback can lead to a wide range of positive or negative feelings and reactions from happiness, sense of worthiness, and high self-confidence to sadness, disappointment, and so on.
I am not happy because I think my efforts are ineffective. [P12]
Most participants reported despite bad feeling of negative feedback, they would accept it if presented respectfully. Some declared they feel unhappy and would not accept their shortcomings at first; however, after these immediate emotional reactions, they try to think rationally and realize whether the feedback source is authentic or not. If they develop trust on feedback data, they accept the feedback and try to improve their teaching performance.
I do not accept negative feedback at first. […]. Yet, when I think it over, I finally accept at least some aspects of it. [P11]
Sometimes, feedback can lead to inappropriate results. For instance, while receiving feedback based on summative evaluation scores, many teachers attribute their low scores to their strict manner and decide to become more easy-going in teaching.
Being a serious teacher is not to your advantage; students give lower scores to a serious teacher […]. So, after a while many clinical teachers decide not to be so strict. [P12]
All the factors that affect the feedback process, such as human and background elements, can also affect the feedback outcomes. For example, the role of feedback provider is very critical in feedback acceptance. Participants also pointed to the congruence between the feedback content and self-evaluation; more discrepancy leads to lower acceptance. Another one is feedback expectedness; the more the feedback is expectable, the more likely it is to be accepted. So, these two could change the feedback outcomes.
For example, you believe that you tried as much as you could to teach effectively, and so you do not expect to receive negative feedback. In this situation, if someone gives you information about your underperformance, it would be very hard to react properly and remain calm. [P4]
Theme 3: Effective feedback strategies
Category 3-1: Developing a systemic approach to feedback
This was a main suggestion on the part of participants. They suggested to develop a feedback system to provide effective feedback for teachers.
It’s necessary to have a system responsible for giving feedback […]. If I know there is a system with some experts whose mission is to help us, I have no problem to accept the feedback. [P4]
Participants want to have a system with predetermined criteria for expected performance which is responsible for the whole process of feedback. It should also focus on performance improvement while focusing on decision making. This system should pay attention to provide both positive and corrective feedback and follow-up, especially when frequent evaluations during several semesters show underperformance.
Category 3-2: Appropriate educational policies for teacher recruitment and promotion
Items included in this category emphasize on the significant role of right policies in performance improvement. According to the participants, if clinical teachers believe in the importance of their teaching quality, they themselves seek feedback to improve it. They stated that unlike research abilities, teaching competencies have received very little attention in faculty recruitment protocols and promotion by-laws, and therefore, all teachers get educational scores easily. They believed that low-quality teachers should not simply receive educational points for promotion; so, it was necessary to be very strict in recruitment examination and the scores of teaching quality in promotion-associated by-laws and regulations should be increased. In their opinion, by strict regulations, teachers will realize that teaching abilities are highly important and they would seek feedback themselves.
Category 3-3: Using others’ experiences
Some participants recommended making benefit from the experiences of successful universities in feedback provision. Additionally, there are some experienced clinical teachers who are eager to receive feedback and one would indeed benefit from them.
We can learn from clinical teachers of successful universities by inviting them to take part in educational activities for a short time. [P9]
Discussion
The purpose of this study was to identify clinical teachers’ perspectives regarding receiving feedback on their educational performance. Interviews expanded our view about the feedback process with three themes: “Feedback elements”, “Feedback outcomes”, and “Effective feedback strategies”. “Feedback elements” consists of human and background elements.
“Human elements” include key people in the feedback process, such as “Sources of feedback”, “Feedback provider”, and “Feedback recipient”. According to the participants, considering the characteristics, emotions, feelings, and attitude of human elements is very critical to reach desirable results. Although the participants introduced students as the best source of feedback, they doubted their honesty and/or accuracy in performance assessment. This is similar to Gugel’s study where the teachers believed in the usefulness of students’ feedback in their professional development, although they were not sure about data authenticity.16 Indeed, assessing teachers’ performance should be a multifaceted approach in which learners’ comments stand as only one dimension.17
The most emphasized point about feedback provider was that s/he should be accepted by the feedback recipient. Teachers prefer to receive feedback from a competent clinical teacher who is an expert in educational performance. In the systematic review by Veloski et al, feedback was effective when it was provided by an authorized and credible person.18 Audia and Locke reported that people prefer to receive negative feedback from trustworthy people. In this context, trust has several aspects: trust to the assessor’s knowledge, honesty, integrity, and goodwill. Moreover, people tend to get feedback from those who have a positive attitude toward the feedback recipient. All of these are in line with the present study.19
Interestingly, all the participants believed in feedback efficacy, but their response to feedback differed in terms of age, work experience, personality, and so on. Hence, feedback should be tailored to the recipients’ traits. This is similar to studies in which factors such as confidence, experience, fear of incompetence,20 and self-esteem21 are effective in feedback acceptance.
“Background elements” include three underlying conditions in the feedback process: “Performing performance”, “Data collection”, and “Giving feedback”. It is very critical to consider the underlying conditions influencing teachers’ performance while interpreting performance data; otherwise, giving feedback would be associated with undesired outcomes. To obtain authentic data, the data collector should be careful with time, place, and mood of the learners. To reduce errors, a sufficient number of different levels of learners and appropriate methods are needed. Also, the learners should be informed that it is very important to comment carefully and honestly.
The situation of feedback presentation has been addressed by many studies. Feedback content, presentation method, time, place, and privacy are important issues in this situation. If the feedback content only contains negative points and does not consider the positive aspects of teacher performance, it would be disappointing. According to Mikulincer, frequent negative feedback could result in classic learned helplessness.22 The teachers need to know based on what criteria the performance needs alteration and what steps they should take to have good performance. Similarly, Havelock has pointed out that people are more likely to make some changes when they understand the reason for it and believe that change is to their benefit.23 Unlike Kluger and Denisi’s meta-analysis, most participants preferred verbal, rather than written feedback.22
According to the participants, feedback could lead to different outcomes. Most participants stated that they might get upset at first and fail to accept the feedback, but that they would try to think logically after a while. If they come to the conclusion that the data are authentic, they probably accept feedback and try to act upon it. However, sometimes, presenting feedback leads to unwanted and negative outcomes. This is similar to the results of Kluger and Denisi’s meta-analysis in which in one-third of the situations, feedback was described to alleviate performance.22
The interviewees also suggested useful strategies for effective feedback process, for example, developing a systemic approach to feedback provision. Similar to the approach stated in the feedback guideline,24 it should aim mainly to improve performance. The border between two functions of evaluation (accountability and decision-making) should be clear because combining these two can result in many challenges.25
The next suggestion was to increase the scores of teaching skills in the promotion by-law and faculty employment policies. In that case, teachers are encouraged to seek feedback themselves.
The last suggestion was to use others’ experiences in giving and accepting feedback.
Reflection on feedback elements obtained in this study helped researchers to develop a feedback cycle (Figure 1).
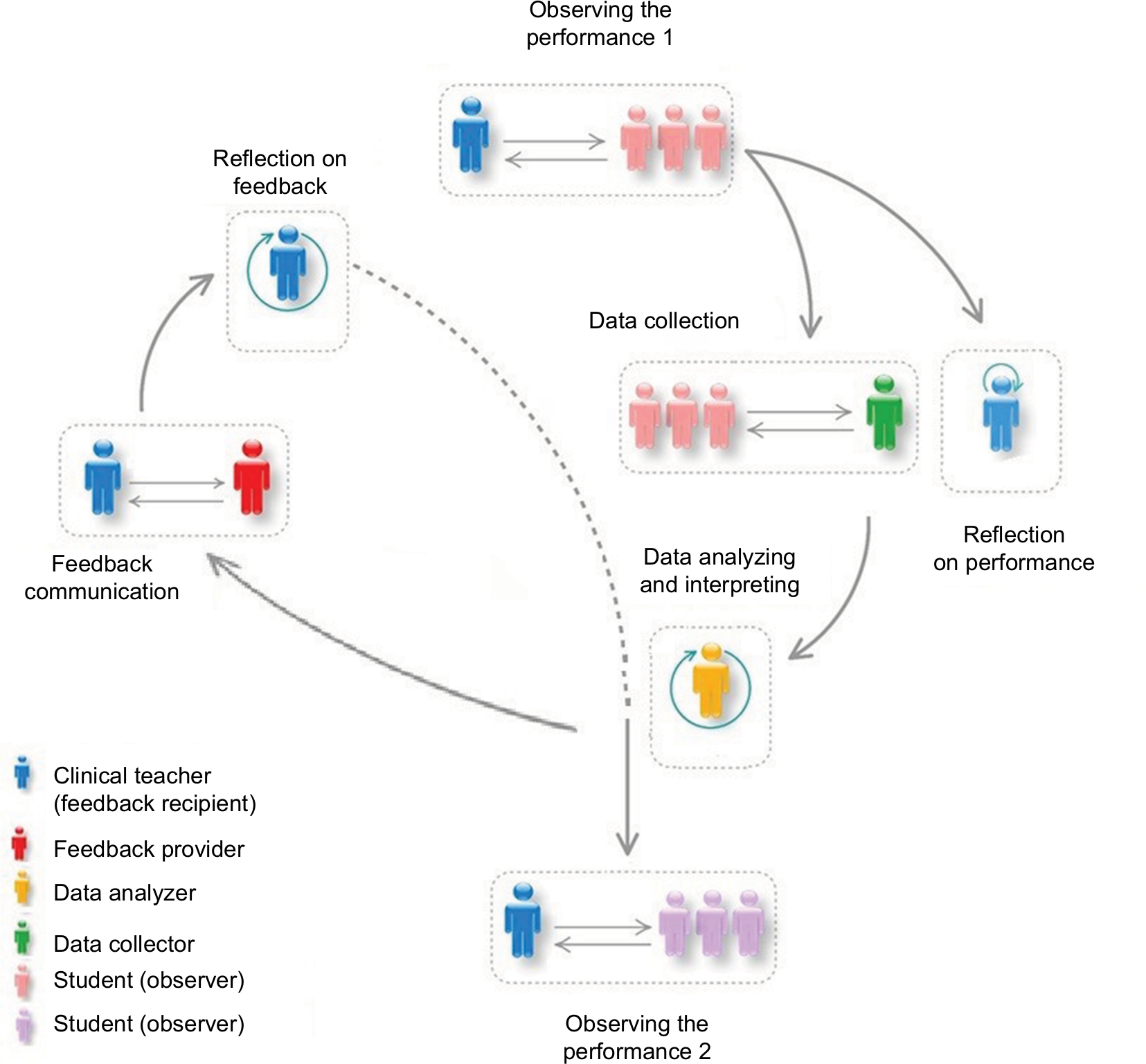 | Figure 1 Feedback cycle. |
The feedback cycle represents the consecutive situations from doing performance to receiving feedback and reflecting on it. Characteristics of each human element and background factor of each situation could affect the related phase. The first is the situation of observing the performance. The clinical teacher and observers (mainly learners) are the key human elements of this situation. The second, collecting data about teachers’ performance, is the situation with two human elements: data sources (observers) and data collector(s). Also, there is a situation where the teacher reflects on his/her performance. The only human element here is the feedback recipient.
The situation of analyzing and interpreting data with one or two human elements (data analyzer and/or feedback provider) may appear to be an unimportant situation and is often neglected. However, it could help the feedback provider to plan a successful feedback session; this is a time for the feedback provider to reflect on data, interpret them, and decide about the way to build on them for setting feedback content. Sometimes, s/he realizes that the information is not enough to give feedback and further investigation about teacher performance is required.
The situation of feedback communication is the most noticed part in the literature; the two human elements are feedback provider and recipient. The behavior of feedback provider and the presentation method play critical roles in feedback acceptance. The last situation of each cycle is reflection on the feedback received. The next cycle begins with the situation of doing the performance again. According to the participants, it is necessary to have a situation for feedback follow-up, which could precede the second cycle and address the predicted outcomes and unintended consequences of feedback presentation.
It should be noted that sometimes, only one person has the role of an observer, data collector, analyzer, and feedback provider; for example, when an expert (instead of learners) is the performance observer, s/he observes the performance, collects data, analyzes and interprets data, and gives feedback to the teacher. Another example is when the learners give feedback to the teacher directly. This cycle is somewhat similar to the one raised by van de Ridder et al.21 Ridder’s model has five phases. In phase A1, the feedback recipient receives instructions and performs a task according to certain standards. Phase B relates to the feedback provider’s observation and interpretation of the performance. Phases A1 and B, except for the interpretation part, are approximately equal to the first phase, “Observing the performance 1” in our model. Since, in some cases, the feedback provider and performance observer are not the same person, we consider two different people for these roles in our model and have an additional phase of data collection. Therefore, the interpretation part of Ridders’ phase B is placed after data collection, in “Analyzing and interpreting” phase in our model. Ridder’s phase C is “Feedback communication”. First, we labeled this phase as “Feedback presentation”; since “communication” is more appropriate due to representing the interaction between feedback provider and recipient, we changed it based on Ridder’s model. In phase D of Ridder’s model, feedback is interpreted by the recipient. We showed this phase by “Reflection on feedback”. Phase A2 is comparable with the phase “Observing performance 2”. To represent the importance of reflection on performance in accepting the feedback, we added this phase.
One limitation of the current study was that clinical teachers’ opinions about feedback were affected by their attitude toward summative evaluation system, and it took a long time for the interviewer to explain them about evaluation and feedback. Another limitation was that clinical teachers were very busy, and it was difficult for the interviewer to set an appropriate time for the interview. The main limitation was there were lot of problems and challenges in the clinical setting; so, the subject of feedback seemed to be very trivial against these problems.
Conclusion
The current study brought up clinical teachers’ opinions toward feedback effectiveness, feedback elements, issues affecting the feedback process, and their recommendations for effective feedback. They had positive attitude toward feedback effectiveness, but they had concerns about issues such as the authenticity of data sources and data gathering methods, choosing an appropriate feedback presenter, congruence between the feedback recipient and the provider, the contextual factors, feedback content, and feedback presentation method.
All these helped the researchers to develop a feedback cycle. Researchers recommend feedback officials to study teachers’ opinions about feedback process and use the feedback cycle to provide more effective feedback.
Feedback literature had shown the importance of feedback presentation method and feedback message, but this study emphasized more on other factors such as data source or data gathering. In other words, the most important part of the feedback cycle for clinical teachers was obtaining authentic data and interpreting them accurately.
Finally, participants’ suggestions about feedback effectiveness, especially the systemic approach, and their description of such a system could be helpful for feedback officials.
Acknowledgments
The researchers would like to appreciate all the clinical teachers who participated in the interviews for their valuable comments. The authors would like also to appreciate Isfahan Medical Education Research Center and The National Agency for Strategic Research in Medical Education for their financial support for this study with the registered project no. 395719 and the grant no. 960217, respectively.
Author contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interests in this work.
References
Bishop S. The Complete Feedback Skills Training Book. Hampshire: Gower; 2000:5–6. | ||
Wiliam D. Feedback: part of a system. Educ Leadersh. 2012;70(1):30–34. | ||
van de Ridder JM, Stokking KM, McGaghie WC, Ten Cate OT. What is feedback in clinical education? Med Educ. 2008;42(2):189–197. | ||
Dinmohammadi MR, Jalali A, Bastani F, parvizi S, Borimnejhad L. bazkhord: onsore asasie amoozeshe balini (vazhehnameh tosifi). Iranian J Med Educ. 2009;9(3):5. Persian. | ||
Hattie J, Timperley H. The power of feedback. Rev Educ Res. 2007;77(1):81–112. | ||
Haghani F, Fakhari M. Feedback in clinical education: concept, barriers, and strategies. Iranian J Med Educ. 2014;13(10):869–885. | ||
Farr Darling L, Erickson G, Clarke A. Collective Improvisation in a Teacher Education Community. Vancouver: Springer; 2007:171–184. | ||
Schum TR, Yindra KJ. Relationship between systematic feedback to faculty and ratings of clinical teaching. Acad Med. 1996;71(10):1100–1102. | ||
Skeff KM. Evaluation of a method for improving the teaching performance of attending physicians. Am J Med. 1983;75(3):465–470. | ||
Kluger AN, Denisi A. Feedback interventions: toward the understanding of a double-edged sword. Curr Dir Psychol Sci. 1998;7(3):67–72. | ||
Rao TV, Rao R. The Power of 360 Degree Feedback: Maximizing Managerial and Leadership Effectiveness. Thousand Oaks, CA, USA: SAGE Publications; 2005:85–95. | ||
Boerboom TB, Jaarsma D, Dolmans DH, Scherpbier AJ, Mastenbroek NJ, van Beukelen P. Peer group reflection helps clinical teachers to critically reflect on their teaching. Med Teach. 2011;33(11):e615–e623. | ||
Collection of evaluation and ranking skills for education development centers; 2011. Available from: http://www.iauardabil.ac.ir/old/web_med/download/edo/bakhshname-edo/meyar.pdf. Accessed January 1, 2018. | ||
Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. | ||
Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112. | ||
Gugel RL. Teacher Perception of Student Feedback at the Secondary Level. Ann Arbor: Chicago Concordia University; 2015:69–70. | ||
Kite ME. Using student feedback as one measure of faculty teaching effectiveness. Effective evaluation of teaching: a guide for faculty and administrators. Soc Teach Psychol. 2012:30–37. | ||
Veloski J, Boex JR, Grasberger MJ, Evans A, Wolfson DB. Systematic review of the literature on assessment, feedback and physicians’ clinical performance: BEME guide No. 7. Med Teach. 2006;28(2):117–128. | ||
Audia PG, Locke EA. Benefiting from negative feedback. Hum Resour Manage Rev. 2003;13(4):631–646. | ||
Eva KW, Armson H, Holmboe E, et al. Factors influencing responsiveness to feedback: on the interplay between fear, confidence, and reasoning processes. Adv Health Sci Educ Theor Pract. 2012;17(1):15–26. | ||
van de Ridder JM, McGaghie WC, Stokking KM, Ten Cate OT, Ridder J, Cate OT. Variables that affect the process and outcome of feedback, relevant for medical training: a meta-review. Med Educ. 2015;49(7):658–673. | ||
Kluger AN, Denisi A. The effects of feedback interventions on performance: a historical review, a meta-analysis, and a preliminary feedback intervention theory. Psychol Bull. 1996;119(2):254–284. | ||
Havelock P. Breaking through the “criticism barrier”: how to make feedback effective. The Foundation Years. 2008;4(4):177–179. | ||
Lefroy J, Watling C, Teunissen PW, Brand P. Guidelines: the do’s, don’ts and don’t knows of feedback for clinical education. Perspect Med Educ. 2015;4(6):284–299. | ||
Santiago P, Benavides F. Teacher evaluation: a conceptual framework and examples of country practices. OECD review on evaluation and assessment frameworks for improving school outcomes. 2009:7–9. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.