Back to Journals » Cancer Management and Research » Volume 17

Proton Pump Inhibitor Therapy Reduces Granulation Tissue Duration Following Laryngeal Cancer Surgery: A Retrospective Cohort Study
Authors Wang J, Zhang C, Liu Y
Received 3 June 2025
Accepted for publication 16 September 2025
Published 25 September 2025 Volume 2025:17 Pages 2169—2181
DOI https://doi.org/10.2147/CMAR.S544365
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Yong Teng
Jingjing Wang,1 Chunhe Zhang,2 Yanan Liu3
1Department of Pharmacy, Cangzhou People’s Hospital, Cangzhou, Hebei, People’s Republic of China; 2Department of Laboratory Medicine, Cangzhou People’s Hospital, Cangzhou, Hebei, People’s Republic of China; 3Department of Otorhinolaryngology, Cangzhou People’s Hospital, Cangzhou, Hebei, People’s Republic of China
Correspondence: Yanan Liu, Department of Otorhinolaryngology, Cangzhou People’s Hospital, No. 7 Qingchi North Avenue, Xinhua District, Cangzhou, Hebei, 061000, People’s Republic of China, Email [email protected]
Background: Granulation tissue formation complicates laryngeal cancer surgery recovery and may be exacerbated by laryngopharyngeal reflux. We investigated whether postoperative proton pump inhibitor (PPI) therapy reduces granulation tissue duration through reflux-mediated mechanisms.
Methods: This retrospective cohort study included 89 laryngeal cancer patients undergoing function-preserving surgery (May 2020-December 2024). Patients received either postoperative PPI therapy (n=32) or standard care (n=57). Primary endpoint was granulation tissue duration. Secondary endpoints included Reflux Symptom Index (RSI) and Reflux Finding Score (RFS) changes. Mediation analysis explored whether PPI effects operated through reflux improvement.
Results: Granulation formation rates were comparable between groups (65.6% vs 57.9%, P=0.188). Among patients developing granulation tissue (n=54), the PPI group demonstrated significantly shorter duration (4.0 [4.0, 5.0] vs 8.0 [6.0, 9.0] weeks, P< 0.001). PPI therapy produced superior improvements in RSI (14.0 [13.0, 16.0] vs 4.0 [3.0, 4.0], P< 0.001) and RFS scores (8.0 [6.8, 9.0] vs 2.0 [1.0, 3.0], P< 0.001). Strong negative correlations existed between reflux improvement and granulation duration (RSI: r=− 0.76; RFS: r=− 0.74, both P< 0.001). Mediation analysis revealed RSI improvement accounted for 16.18% of PPI’s therapeutic effect. Benefits were most pronounced in females, early-stage tumors, and patients with lower baseline RSI scores.
Conclusion: Postoperative PPI therapy significantly reduces granulation tissue duration following laryngeal cancer surgery through both reflux-dependent and independent mechanisms, supporting routine perioperative acid suppression in this population.
Keywords: laryngeal cancer, granulation tissue, proton pump inhibitors, laryngopharyngeal reflux
Introduction
Laryngeal squamous cell carcinoma (LSCC) remains a significant global health burden, accounting for approximately 1–2% of all malignancies worldwide, with an estimated 184,000 new cases annually.1 Despite advances in non-surgical approaches, function-preserving surgical techniques—including transoral laser microsurgery, plasma surgery, and partial laryngectomy—remain fundamental in LSCC management, particularly for early-stage disease.2 While these approaches offer favorable oncological outcomes with voice preservation, postoperative complications such as granulation tissue formation remain challenging.3
Granulation tissue, characterized by the proliferation of vascularized connective tissue during wound healing, is a common complication following laryngeal surgery. This condition affects a substantial proportion of patients, with studies reporting incidence rates of 53.8% at one-month post-surgery3 and 44% overall.4 This excessive tissue formation can result in dysphonia, airway obstruction, and prolonged hospitalization, significantly impacting patient recovery and quality of life.5 Although various factors influence granulation tissue formation, emerging evidence suggests that laryngopharyngeal reflux (LPR) may be crucial.6
LPR involves the retrograde flow of gastric contents into the laryngopharynx, causing epithelial damage, ciliary dysfunction, and enhanced inflammatory response in laryngeal tissues.7 The physiological barriers against reflux are often compromised following laryngeal surgery, potentially exacerbating LPR in the immediate postoperative period.8 Pepsin and acid exposure can trigger a cascade of inflammatory events, promoting the upregulation of pro-inflammatory cytokines, growth factors, and matrix metalloproteinases that may facilitate excessive granulation tissue formation.9,10
Proton pump inhibitors (PPIs) represent the gold standard in LPR pharmacological management due to their potent acid-suppressive properties. PPIs effectively reduce acid secretion by irreversibly inhibiting the hydrogen-potassium ATPase enzyme system in gastric parietal cells.11 Recent investigations have revealed that PPIs may possess pleiotropic anti-inflammatory and antioxidant properties, including inhibition of neutrophil activation, reduced pro-inflammatory cytokine production, and attenuation of oxidative stress—all factors implicated in pathological granulation tissue formation.12,13
Despite theoretical rationale and preliminary clinical observations suggesting the potential benefits of PPI therapy after laryngeal surgery, systematic investigations remain limited.14 Previous studies have primarily focused on identifying LPR as a risk factor for surgical complications rather than evaluating the therapeutic potential of acid suppression.15 Furthermore, the mechanisms by which PPIs might influence granulation tissue formation—whether through direct anti-inflammatory effects or indirectly via amelioration of reflux—remain incompletely understood. The relationship between standardized reflux measures (Reflux Symptom Index and Reflux Finding Score) and granulation outcomes has not been thoroughly investigated.
To address these knowledge gaps, we conducted a retrospective cohort study examining the effects of postoperative PPI therapy on granulation tissue formation and resolution following laryngeal cancer surgery. We hypothesized that PPI therapy would reduce granulation tissue duration through mechanisms potentially mediated by improvements in reflux indices. Additionally, we sought to identify patient subgroups that might derive differential benefits from PPI therapy, thereby informing more targeted postoperative care protocols for laryngeal cancer patients.
Methods
Study Design and Participants
We conducted a single-center, retrospective cohort study at the Department of Otolaryngology-Head & Neck Surgery, Cangzhou People’s Hospital (Hebei, China). We reviewed medical records of consecutive adults with pathologically confirmed laryngeal squamous cell carcinoma who underwent surgery between May 1, 2020, and December 31, 2024. The Institutional Review Board of Cangzhou People’s Hospital approved the study protocol with a waiver of informed consent for this retrospective review. Patients were eligible if they met all of the following criteria: (1) underwent primary surgical treatment for laryngeal cancer, including function-preserving procedures (CO2-laser transoral resection, plasma surgery, or partial laryngectomy); (2) had documented postoperative endoscopic follow-up of ≥12 weeks; and (3) had reflux assessments (Reflux Symptom Index [RSI] and Reflux Finding Score [RFS]) documented at standard clinical visits. Exclusion criteria included: (1) documented PPI use within 3 months before surgery; (2) previous radiotherapy or chemoradiotherapy followed by salvage surgery; (3) systemic corticosteroid therapy; (4) recurrent disease within 12 weeks after surgery; or (5) insufficient follow-up data. Baseline demographic and oncologic data—including age, sex, body mass index (BMI), smoking and alcohol status, tumor (T) stage, and surgical extent—were extracted from electronic medical records.
Patients underwent one of three function-preserving approaches: CO2 laser resection (n=45, 50.6%), plasma surgery (n=28, 31.5%), or partial laryngectomy (n=16, 18.0%). CO2 laser resection utilized microsurgical techniques for precise tumor excision, primarily for early-stage glottic tumors. Plasma surgery employed controlled plasma energy for enhanced hemostatic control. Partial laryngectomy included various open techniques based on tumor extent. All procedures were performed by the same surgical team using standardized protocols. Tumor staging followed the 8th edition AJCC TNM system. For analysis purposes, early-stage disease was defined as T1-T2 tumors, and advanced-stage as T3-T4 tumors, based on preoperative imaging and histopathological examination.
Treatment Groups and Protocol
In May 2020, our department implemented a new clinical protocol for post-laryngeal cancer surgery care that included systematic use of PPIs. This change in practice created two natural cohorts for comparison. The PPI group comprised patients treated after protocol implementation, while the non-PPI group included those treated before the protocol change who received standard care without acid-suppressive medication. Patients in the PPI group received acid-suppressive medication starting on the seventh postoperative day. Standard therapy consisted of esomeprazole (Nexium®, AstraZeneca, batch numbers varied by supply period) 40mg daily (20mg twice daily) or rabeprazole (Pariet®, Eisai, batch numbers varied by supply period) 20mg daily (10mg twice daily) if esomeprazole was contraindicated. For patients without granulation tissue development, PPI treatment continued for 8 weeks. For patients who developed granulation tissue, PPI treatment continued until complete resolution of granulation was documented. The non-PPI group received identical perioperative care without acid-suppressive medication. Medication adherence was assessed through prescription refill records and documented clinical notes.
Reflux Assessment
The RSI (a 9-item self-administered questionnaire with scores ranging from 0 to 45) was used to evaluate reflux symptoms, with scores >13 considered abnormal. The RFS (an 8-item laryngoscopic assessment with scores ranging from 0 to 26) was used to document laryngeal findings associated with reflux, with scores >7 considered abnormal. These assessments were extracted from medical records at preoperative baseline and during postoperative follow-up visits. While post-operative changes may influence these assessments, they remain standard validated instruments for clinical practice. We acknowledge the limitations of symptom-based assessment in post-operative patients and recognize that future studies would benefit from objective measures such as salivary pepsin assays or 24-hour MII-pH monitoring. All evaluations were conducted by fellowship-trained laryngologists, with analysis focusing on between-group differences to minimize surgical confounding. For analysis purposes, postoperative assessments were categorized into early (4–6 weeks), intermediate (8–12 weeks), and late (16–24 weeks) periods. For patients with persistent granulation, additional assessments were conducted as clinically indicated.
Follow-up and Outcome Definitions
Patients were followed postoperatively with regular laryngoscopic examinations. The standard follow-up protocol included examinations at weeks 2, 3, 4, 6, 8, 10, and 12 during the first three months; at weeks 14, 16, 18, 20, and 24 during months 4–6; and at weeks 30, 36, 48, and 60 during the remainder of the first year. After week 60, patients were examined every six months. The primary endpoint was granulation duration, defined as the interval (weeks) from the first documented evidence of postoperative granulation to the first documentation of complete epithelialization that remained resolved on subsequent examinations. Secondary endpoints included: (i) RSI and RFS scores as documented during clinical visits; (ii) calculated change scores from preoperative to postoperative assessments; (iii) correlations between changes in reflux metrics and granulation duration; (iv) mediation of the treatment effect through changes in RSI and RFS.
Statistical Analysis
Continuous variables are presented as median (interquartile range) for non-normally distributed data or mean ± standard deviation for normally distributed data, and categorical variables as frequencies and percentages. Normality was assessed using Shapiro–Wilk tests. Between-group comparisons were performed using Mann–Whitney U-tests for non-normally distributed continuous variables or independent t-tests for normally distributed variables and chi-square or Fisher’s exact tests for categorical variables. The effect of PPI use on granulation duration was estimated using logistic regression and linear regression, adjusting for potential confounders, including age, gender, smoking status, alcohol consumption, and T stage. Kaplan-Meier analysis was performed to compare granulation persistence between groups, with the event defined as the complete resolution of granulation tissue. Subgroup analyses were conducted to investigate the consistency of PPI effects across different patient characteristics. Stratified analyses by surgical technique (CO2 laser resection, plasma surgery, partial laryngectomy) and anatomical subsite (glottic, supraglottic, subglottic) were performed to evaluate treatment consistency across different procedures and tumor locations. Interaction terms were included in regression models to test for significant differences in treatment effects between subgroups. The relationships between RSI/RFS change scores and granulation duration were analyzed using Spearman correlation coefficients due to non-normal data distributions and linear regression models. Multivariable models were constructed to adjust for potential confounders. A mediation analysis was performed to investigate whether changes in reflux indices mediated the effect of PPI use on granulation duration. The mediation models included PPI use as the independent variable, granulation duration as the dependent variable, and RSI or RFS change as the mediator, adjusting for age, gender, smoking status, alcohol consumption, and T stage. The significance of mediation effects was tested using bootstrapping with 5,000 resamples, and the proportion of the total effect mediated through each reflux index was calculated.
Statistical analyses were performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA) and R version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria). Two-sided P-values <0.05 were considered statistically significant.
Results
Baseline Characteristics
A total of 89 patients who underwent laryngeal cancer surgery were included in our study, with 32 patients in the PPI group and 57 patients in the non-PPI group. Baseline characteristics are presented in Table 1. No significant differences were observed between the groups regarding age, gender, smoking status, alcohol consumption, or T-stage distribution. However, there was a significant difference in tumor differentiation (P=0.040), with the PPI group having a higher proportion of moderate (37.5% vs 22.8%) and poor differentiation (6.3% vs 0.0%) compared to the non-PPI group.
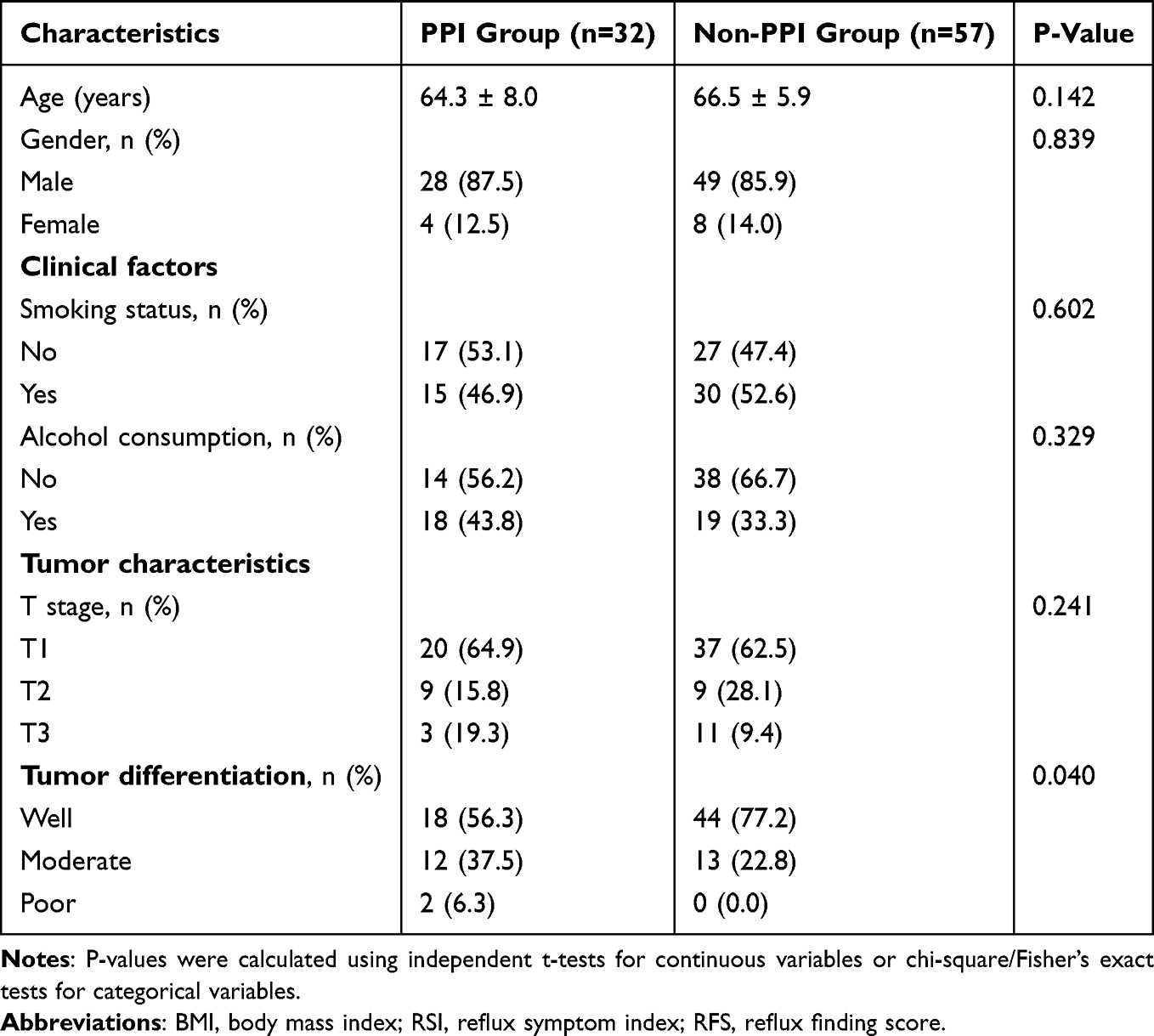 |
Table 1 Baseline Characteristics of Patients in PPI and Non-PPI Groups |
Effect of PPI Use on Granulation Tissue Formation and Duration
As shown in Table 2 and Figure 1A, although the PPI group had a slightly higher rate of granulation tissue formation than the non-PPI group (65.6% vs 57.9%), this difference was not statistically significant (P=0.188; adjusted OR=2.09, 95% CI: 0.70–6.26). However, among patients who developed granulation tissue (n=54), the PPI group demonstrated significantly shorter granulation duration compared to the non-PPI group (4.0 [4.0, 5.0] weeks vs 8.0 [6.0, 9.0] weeks, P<0.001; adjusted β=−3.96, 95% CI: −4.84 to −3.09) (Table 2 and Figure 1B).
 |
Table 2 Association Between PPI Use and Granulation Occurrence and Duration |
 |
Figure 1 PPI effects on granulation tissue formation, duration, and persistence. (A) Granulation occurrence rates in PPI users (65.6%) versus non-PPI users (57.9%) (P=0.624). (B) Box plot of granulation duration in patients with granulation tissue; median duration: PPI group=4.0 weeks, non-PPI group=8.0 weeks (P<0.001). (C) Kaplan-Meier curves of granulation persistence probability over time. Abbreviation: PPI, proton pump inhibitor. |
The Kaplan-Meier analysis (Figure 1C) revealed that granulation persistence probability decreased more rapidly in the PPI group compared to the non-PPI group, with complete resolution occurring by 6 weeks in the PPI group, while some patients in the non-PPI group had persistent granulation tissue beyond 12 weeks.
Effect of PPI Use on Reflux Indices
At baseline, there were no significant differences in pretreatment RSI scores between the PPI and non-PPI groups (27.0 [25.0, 30.0] vs 27.0 [24.0, 28.0], P=0.069). However, after treatment, the PPI group showed significantly lower RSI scores compared to the non-PPI group (13.0 [12.0, 14.0] vs 23.0 [21.0, 25.0], P<0.001) (Table 3 and Figure 2A). The mean RSI change score (pretreatment minus posttreatment) was significantly greater in the PPI group (14.0 [13.0, 16.0] vs 4.0 [3.0, 4.0], P<0.001; adjusted β=10.7, 95% CI: 9.72–11.73), indicating greater improvement in reflux symptoms.
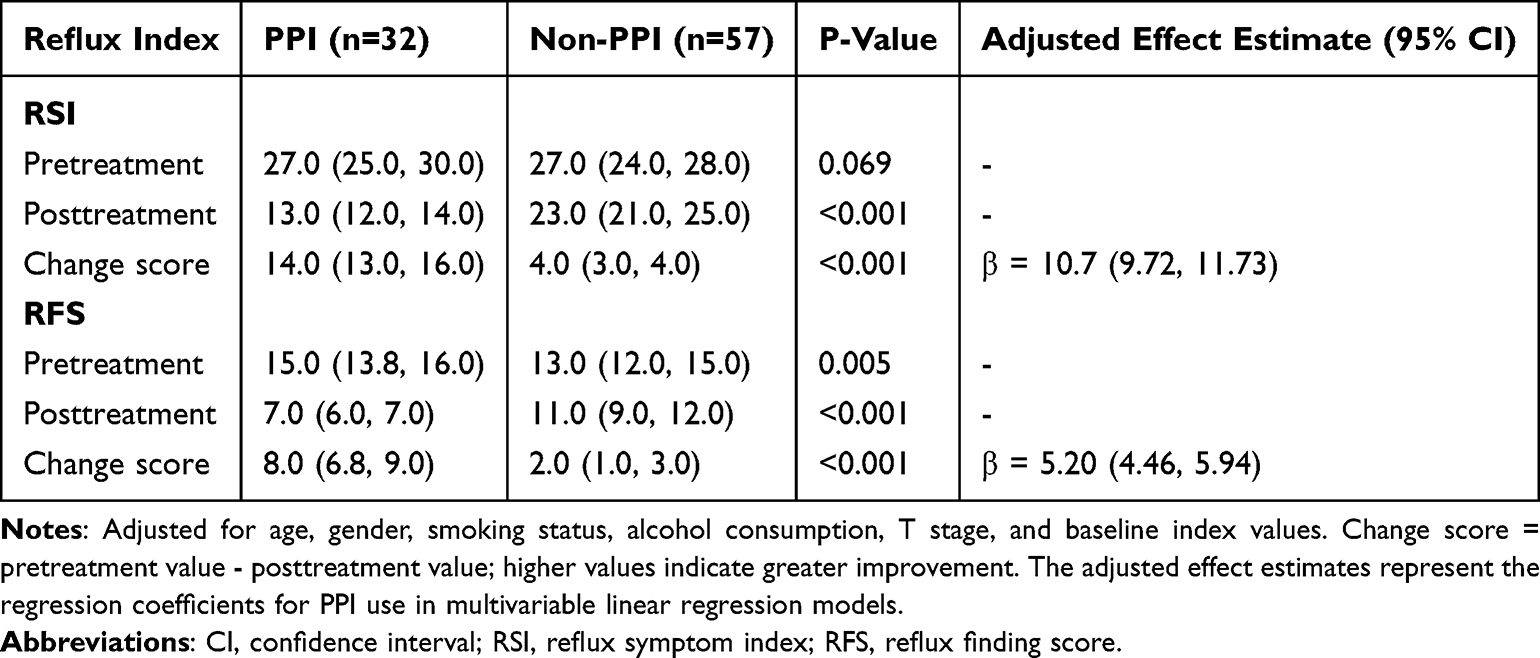 |
Table 3 Association Between PPI Use and Changes in RSI/RFS |
 |
Figure 2 Effect of PPI use on reflux indices and correlation with granulation duration. (A and B) Pre- and post-treatment changes in RSI and RFS scores by PPI status. Both groups showed significant improvement (all P<0.001), with greater improvement in the PPI group. (C and D) Correlation between RSI/RFS change scores and granulation duration. Overall negative correlations were observed (RSI: r=−0.76, P<0.001; RFS: r=−0.74, P<0.001). Abbreviations: PPI, proton pump inhibitor; RSI, reflux symptom index; RFS, reflux finding score. |
Similarly, RFS scores showed a small but statistically significant difference at baseline (15.0 [13.8, 16.0] vs 13.0 [12.0, 15.0], P=0.005). After treatment, the PPI group demonstrated significantly lower RFS scores (7.0 [6.0, 7.0] vs 11.0 [9.0, 12.0], P<0.001) (Table 3 and Figure 2B). The mean RFS change score was significantly greater in the PPI group (8.0 [6.8, 9.0] vs 2.0 [1.0, 3.0], P<0.001; adjusted β=5.20, 95% CI: 4.46–5.94), indicating greater improvement in laryngeal findings.
Relationship Between Reflux Indices and Granulation Duration
Among patients who developed granulation tissue (n=54), significant negative correlations were observed between RSI change scores and granulation duration (r=−0.76, P<0.001) and between RFS change scores and granulation duration (r=−0.74, P<0.001) (Table 4, Figure 2C and D). These negative correlations indicate that greater improvements in reflux indices were associated with shorter granulation duration. In the unadjusted linear regression models, each unit increase in RSI change score was associated with a 0.36-week decrease in granulation duration (95% CI: −0.45 to −0.28, P<0.001). Similarly, each unit increase in RFS change score was associated with a 0.62-week decrease in granulation duration (95% CI: −0.78 to −0.47, P<0.001). The associations were attenuated after adjusting for potential confounders but remained significant for RSI change (adjusted β=−0.29, 95% CI: −0.51 to −0.06).
 |
Table 4 Relationship Between RSI/RFS Changes and Granulation Duration |
Subgroup Analysis
Analysis across patient subgroups defined by baseline characteristics revealed that PPI therapy consistently shortened granulation duration in most populations examined (Figure 3). However, significant interactions were observed for gender (P for interaction=0.047), T stage (P for interaction=0.005), and pretreatment RSI (P for interaction=0.025). The effect of PPI use on granulation duration was more pronounced in females (β=−5.67, 95% CI: −7.03 to −4.30) compared to males (β=−3.60, 95% CI: −4.52 to −2.68) and in patients with early T stage (β=−4.79, 95% CI: −5.82 to −3.75) compared to late T stage (β=−1.90, 95% CI: −3.07 to −0.73). Additionally, patients with below-median pretreatment RSI scores showed a more substantial effect (β=−5.28, 95% CI: −6.56 to −4.00) compared to those with above-median scores (β=−3.39, 95% CI: −4.28 to −2.49). No significant interactions were observed for age, smoking status, alcohol consumption, or pretreatment RFS scores (all P for interaction > 0.05).
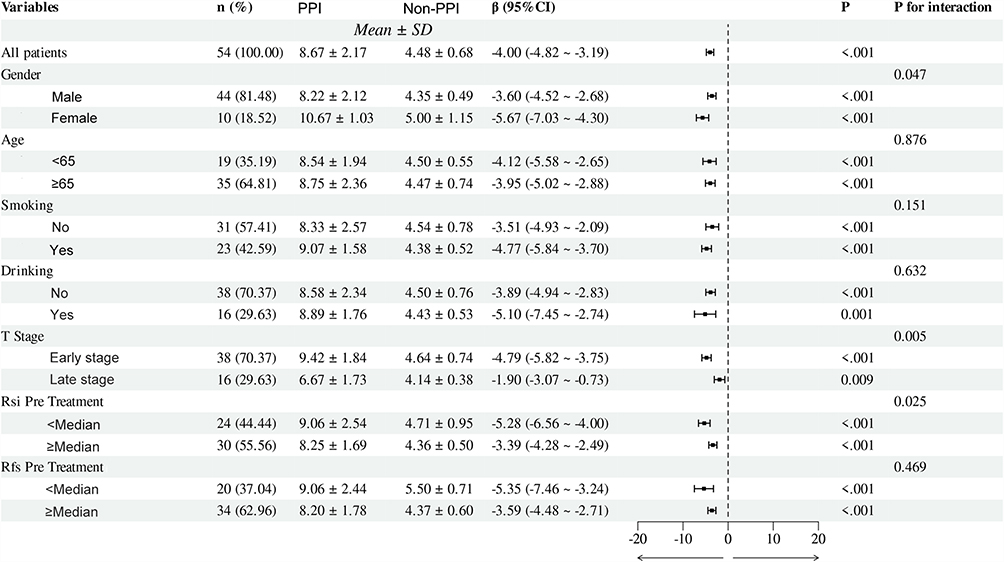 |
Figure 3 Forest plot of PPI effect on granulation duration across patient subgroups. Overall, PPI use was associated with reduced granulation duration (β=−4.00 weeks, 95% CI: −4.82, −3.19). Significant interactions were observed for gender (P=0.047), T stage (P=0.005), and pretreatment RSI (P=0.025). Data are presented as β coefficients (95% CI). Abbreviations: CI, confidence interval; PPI, proton pump inhibitor; RSI, reflux symptom index; RFS, reflux finding score. |
To assess the robustness of these findings across different clinical scenarios, we conducted stratified analyses by surgical approach and tumor location. Surgical techniques were similarly distributed between groups (P=0.183), with CO2 laser resection most common (50.6%), followed by plasma surgery (31.5%) and partial laryngectomy (18.0%). Anatomical distribution comprised glottic (70.8%), supraglottic (24.7%), and subglottic (4.5%) locations.
PPI therapy significantly reduced granulation duration across all surgical techniques and anatomical subsites. Multivariable analysis demonstrated consistent benefits across CO2 laser resection (adjusted β=−4.02 weeks, P<0.001), plasma surgery (adjusted β=−5.85 weeks, P<0.001), and partial laryngectomy (adjusted β=−6.00 weeks, P=0.014). Similarly, both glottic (adjusted β=−3.77 weeks, P<0.001) and supraglottic tumors (adjusted β=−7.58 weeks, P<0.001) showed significant improvements. No significant interactions were observed (P>0.05), indicating universal PPI benefit regardless of surgical approach or tumor location (Supplementary Tables S1–S7).
Mediation Analysis
A mediation analysis was performed to investigate whether the effects of PPI use on granulation duration were mediated by changes in reflux indices (Table 5 and Figure 4). For RSI change, the indirect effect of PPI use on granulation duration was −0.63 weeks (95% CI: −4.17 to 2.13, P=0.760), accounting for 16.18% of the total effect. The direct effect remained substantial at −3.36 weeks (95% CI: −6.24 to 0.16, P=0.080), accounting for 83.82% of the total effect. The total effect was −3.98 weeks (95% CI: −4.90 to −3.12, P<0.001). For RFS change, the indirect effect was 0.33 weeks (95% CI: −2.44 to 2.47, P=0.760), accounting for −4.83% of the total effect. The direct effect was −4.32 weeks (95% CI: −6.66 to −1.78, P<0.001), accounting for 104.83% of the total effect. The total effect was −3.99 weeks (95% CI: −4.82 to −3.16, P<0.001).
 |
Table 5 Mediation Analysis of RSI and RFS on the Association Between PPI Use and Granulation Duration |
 |
Figure 4 Mediation analysis of PPI use on granulation duration. Mediation models with (A) RSI change and (B) RFS change as mediators. Numbers represent effect estimates (95% CI). The total effect of PPI on granulation duration was primarily direct rather than mediated through reflux indices. Percentages indicate proportion of effect mediated. Abbreviations: CI, confidence interval; PPI, proton pump inhibitor; RSI, reflux symptom index; RFS, reflux finding score. |
Discussion
This retrospective cohort study demonstrates that postoperative PPI therapy significantly shortens granulation tissue duration following laryngeal cancer surgery without affecting its incidence. Patients receiving PPIs experienced approximately 4 weeks reduction in granulation persistence compared to non-PPI patients, with complete resolution by 6 weeks in the PPI group versus persistence beyond 12 weeks in some non-PPI cases. These findings have important clinical implications for postoperative care in laryngeal cancer patients.
Our results align with recent evidence on acid suppression in wound healing. Jin et al16 demonstrated that preventive PPI use after cordectomy shortened traumatic granuloma recovery duration, though it did not prevent its occurrence. Stephenson et al17 investigated PPI effects on the incidence of pharynx cutaneous fistulae after total laryngectomy. Bang et al14 observed that postoperative PPI administration in patients with vocal fold mucosal disease and reflux symptoms might improve subjective and objective voice outcomes after laryngeal microsurgery, particularly regarding noise-to-harmonics ratio and strain factor. The observation that PPI therapy did not significantly affect granulation tissue occurrence rates suggests that initial inflammatory triggers for granulation formation may differ from factors influencing subsequent resolution. This distinction has significant implications for targeted perioperative interventions.
Our mediation analysis revealed complex relationships between PPI therapy, reflux indices, and healing outcomes. RSI improvement mediated 16.18% of PPI’s total effect on granulation duration. While not reaching statistical significance with our sample size, this represents a clinically relevant pathway warranting further investigation. Sim et al18 demonstrated that mediation analyses typically require substantially larger sample sizes than direct effect analyses, often necessitating 100–200 participants to detect mediation effects of this magnitude reliably. The direction and proportion of the RSI mediation effect align with the current understanding of the relationship between reflux symptoms and laryngeal healing, as documented by Lechien et al.13
Intriguingly, we observed a suppression effect with RFS (negative mediation percentage of −4.83%), indicating that when accounting for RFS changes, the direct impact of PPI on granulation duration was stronger (−4.32 weeks) than the total effect (−3.99 weeks). This counterintuitive finding reflects the well-documented phenomenon that RFS items are not as responsive to treatment as the overall clinical picture and tend to lag behind RSI,19,20 consistent with the delay in recovery of physical examination changes compared to symptom resolution.21 While RSI and RFS are complementary when assessing treatment response, improvement in RSI does not correlate with that in RFS, creating a temporal discordance where the slower resolution of endoscopic findings captured by RFS masks the actual direct beneficial effect of PPI therapy on granulation tissue healing.22
The biological mechanisms underlying PPI’s beneficial effects likely involve multiple pathways. LPR-induced inflammation is characterized by neutrophilic infiltration, epithelial damage, and upregulation of pro-inflammatory cytokines in laryngeal tissues.10,23 PPIs may mitigate this inflammatory cascade by reducing acid and pepsin exposure, creating a microenvironment more conducive to coordinated wound healing. Beyond acid suppression, growing evidence indicates that PPIs possess direct anti-inflammatory properties. In vitro and animal studies have demonstrated that PPIs inhibit neutrophil activation, reduce pro-inflammatory cytokine production, and downregulate matrix metalloproteinases involved in tissue remodeling.24,25 Importantly, PPIs have been shown to inhibit neutrophil-mediated inflammation (predominant in granulation tissue) more effectively than lymphocyte-mediated processes (reflected in some RFS components,12,24 potentially explaining the divergent mediation patterns observed in our analysis.
Our subgroup analysis revealed significant variations in PPI efficacy across patient populations. The effect was more pronounced in females compared to males, patients with early T-stage disease compared to late-stage, and those with lower pretreatment RSI scores compared to higher scores. The gender difference aligns with findings by Lechien et al26 who reported greater responsiveness to PPI therapy in female LPR patients, potentially due to gender-specific differences in inflammatory profiles and wound healing mechanisms. The more substantial effect in early T-stage disease likely reflects the smaller wound surface area and less extensive disruption of tissue architecture, allowing for more efficient healing when inflammation is controlled.16 The differential effect based on pretreatment RSI suggests that patients with more severe baseline reflux symptoms may require more intensive or prolonged acid suppression therapy or adjunctive treatments targeting other aspects of the inflammatory cascade.27
From a clinical perspective, our findings suggest that PPI therapy should be continued even when endoscopic improvement lags, as the beneficial effects on granulation resolution may precede visible changes in overall laryngeal inflammation. Furthermore, the divergent mediation patterns between RSI and RFS highlight the value of incorporating subjective and objective assessments when evaluating treatment response in this population. The substantial shortening of granulation duration with PPI therapy may translate to earlier functional recovery, reduced healthcare utilization, and improved patient quality of life.16
Our study has several strengths, including a well-defined patient cohort, standardized PPI protocol, comprehensive reflux assessment, and detailed subgroup analysis. Mediation analysis provides insights into potential mechanistic pathways that extend beyond simple associations. However, several limitations warrant consideration. The retrospective design introduces potential selection bias, although we attempted to mitigate this through multivariable modeling. Post-operative RSI and RFS assessment presents methodological challenges, as patients invariably experience dysphonia and mucosal edema that subside during natural healing, potentially confounding genuine LPR-related changes. Nevertheless, the consistent PPI benefits across different surgical techniques, combined with mediation analysis showing RSI improvement accounted for only 16% of therapeutic effect, suggest that direct anti-inflammatory mechanisms predominate. Our stratified analysis demonstrates PPI efficacy across all surgical approaches, with comparable granulation formation rates (~60%) but consistent therapeutic benefit regardless of surgical invasiveness, indicating effects through common inflammatory pathways. We did not have direct measures of tissue inflammation or objective reflux assessments such as pH monitoring or pepsin detection.28,29 Future studies would benefit from objective measures including salivary pepsin assays, 24-hour MII-pH monitoring, the GERD Questionnaire (GERDQ), or inflammatory biomarkers when technically feasible. The fixed PPI dosing protocol did not allow for dose-response evaluation, and while adequately powered for primary analyses, sample size may have limited detection of mediation effects.
Future research should include prospective randomized trials to establish causality and optimize treatment protocols. Investigating different PPI regimens, adjunctive therapies targeting complementary inflammatory pathways, and direct assessment of tissue inflammatory markers would provide deeper mechanistic insights. Evaluating patient-reported outcomes such as voice quality and swallowing function would further elucidate the clinical benefits of shortened granulation duration.
Conclusion
Our study provides evidence that postoperative PPI therapy significantly reduces granulation tissue duration following laryngeal cancer surgery, with effects that appear to operate through reflux-dependent and reflux-independent pathways. The contribution of symptomatic improvement to this effect, though not reaching statistical significance in our sample, represents a clinically meaningful pathway that warrants further investigation in larger studies. These findings support the consideration of routine postoperative PPI administration in this patient population, particularly for females, those with early-stage disease, and patients with lower baseline reflux symptom severity. The complex relationship between endoscopic findings and healing outcomes underscores the need for comprehensive assessment approaches when evaluating treatment efficacy in this clinical context.
Data Sharing Statement
Some or all of the datasets generated and/or analyzed in the current study are not publicly available, but are available on reasonable request by the relevant authors.
Consent to Participate
Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Ethics
This study was approved by the Ethics Committee of Cangzhou People’s Hospital. The requirement for patient consent was waived due to the retrospective nature of the study, which involved anonymized data from medical records and posed minimal risk to the participants. The use of anonymized data ensured that individual privacy was protected. The study strictly adhered to the principles outlined in the Declaration of Helsinki, ensuring that all patient information was handled with confidentiality and used solely for research purposes.
Funding
No funding was received for this research.
Disclosure
The authors declare no competing interests.
References
1. Bray F, Laversanne M, Sung H. et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Gong H, Huang Q, Shi Y, et al. Oncologic outcomes of transoral laser microsurgery versus open partial laryngectomies in the management of early stage glottic carcinoma. Am J Otolaryngol. 2022;43(6):103551. doi:10.1016/j.amjoto.2022.103551
3. Rioja E, Blanch JL, Bores A, Bernal-Sprekelsen M, Vilaseca I. Clinical significance of granulation tissue after transoral laser microsurgery for glottic cancer. J Laryngol Otol. 2015;129(4):377–382. doi:10.1017/S0022215115000444
4. Jabbour N, Tracy JC, Du E, Tracy LF. Healing after transoral carbon dioxide laser surgery for early glottic cancer. J Laryngol Otol. 2023;137(2):205–212. doi:10.1017/S0022215121004679
5. Hollis AN, Ghodke A, Farquhar D, Buckmire RA, Shah RN. Postoperative Inhaled Steroids Following Glottic Airway Surgery Reduces Granulation Tissue Formation. Ann Otol Rhinol Laryngol. 2022;131(11):1267–1273. doi:10.1177/00034894211065805
6. Wang L, Sun S, Wang S, Liang D, Ji W. Clinical observation of traumatic granuloma after CO(2) laser cordectomy and laryngopharyngeal reflux. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2014;49(5):374–378.
7. Wang C, Zhang J, Li CC, et al. The ambulatory arterial stiffness index and target-organ damage in Chinese patients with chronic kidney disease. BMC Nephrol. 2013:14257. doi:10.1186/1471-2369-14-257.
8. LeBlanc B, Lewis E, Caldito G, Nathan CA. Increased Pharyngeal Reflux in Patients Treated for Laryngeal Cancer: a Pilot Study. Otolaryngol Head Neck Surg. 2015;153(5):791–794. doi:10.1177/0194599815601026
9. Li Y, Xu G, Zhou B, et al. Effects of acids, pepsin, bile acids, and trypsin on laryngopharyngeal reflux diseases: physiopathology and therapeutic targets. Eur Arch Otorhinolaryngol. 2022;279(6):2743–2752. doi:10.1007/s00405-021-07201-w
10. Tan JJ, Dai YF, Wang F, et al. Pepsin-mediated inflammation in laryngopharyngeal reflux via the ROS/NLRP3/IL-1beta signaling pathway. Cytokine. 2024:178156568. doi:10.1016/j.cyto.2024.156568.
11. Chen YY, Wang CC, Lin YC, et al. Validation of Pharyngeal Acid Reflux Episodes Using Hypopharyngeal Multichannel Intraluminal Impedance-pH. J Neurogastroenterol Motil. 2023;29(1):49–57. doi:10.5056/jnm22047
12. Kedika RR, Souza RF, Spechler SJ. Potential anti-inflammatory effects of proton pump inhibitors: a review and discussion of the clinical implications. Dig Dis Sci. 2009;54(11):2312–2317. doi:10.1007/s10620-009-0951-9
13. Lechien JR, Akst LM, Hamdan AL, et al. Evaluation and Management of Laryngopharyngeal Reflux Disease: state of the Art Review. Otolaryngol Head Neck Surg. 2019;160(5):762–782. doi:10.1177/0194599819827488
14. Bang JH, Lee SG, Kwon KJ, et al. Effect of Proton Pump Inhibitor on the Outcome of Laryngeal Microsurgery in Patients With Vocal Fold Mucosal Disease With Reflux Symptoms. J Voice. 2024;38(4):931–935. doi:10.1016/j.jvoice.2022.01.009
15. Gunjawate DR, Ravi R. Scientometric analysis of trends in research in laryngopharyngeal reflux. Eur Arch Otorhinolaryngol. 2025;282(5):2525–2532. doi:10.1007/s00405-025-09381-1
16. Jin X, Niu Y, Gu W, Wang J. Effects of Antiacid Therapy on Granuloma after Transoral Type IV-VI Cordectomy in Patients with Early-Stage Glottic Cancer. Biomed Res Int. 2020;20204178376. doi:10.1155/2020/4178376
17. Stephenson KA, Fagan JJ. Effect of perioperative proton pump inhibitors on the incidence of pharyngocutaneous fistula after total laryngectomy: a prospective randomized controlled trial. Head Neck. 2015;37(2):255–259. doi:10.1002/hed.23591
18. Sim M, Kim SY, Suh Y. Sample Size Requirements for Simple and Complex Mediation Models. Educ Psychol Meas. 2022;82(1):76–106. doi:10.1177/00131644211003261
19. Belafsky PC, Postma GN, Koufman JA. The validity and reliability of the reflux finding score (RFS). Laryngoscope. 2001;111(8):1313–1317. doi:10.1097/00005537-200108000-00001
20. Habermann W, Schmid C, Neumann K, Devaney T, Hammer HF. Reflux symptom index and reflux finding score in otolaryngologic practice. J Voice. 2012;26(3):e123–127. doi:10.1016/j.jvoice.2011.02.004
21. Belafsky PC, Postma GN, Koufman JA. Laryngopharyngeal reflux symptoms improve before changes in physical findings. Laryngoscope. 2001;111(6):979–981. doi:10.1097/00005537-200106000-00009
22. Hutnik R, Zlatopolsky A, Mehraban-Far S, et al. Laryngopharyngeal reflux: comparing improvements in reflux symptom index with reflux finding score. Am J Otolaryngol. 2020;41(6):102730. doi:10.1016/j.amjoto.2020.102730
23. Liu D, Qian T, Sun S, Jiang JJ. Laryngopharyngeal Reflux and Inflammatory Responses in Mucosal Barrier Dysfunction of the Upper Aerodigestive Tract. J Inflamm Res. 2020;131291–131304. doi:10.2147/JIR.S282809
24. Fowler JF, Eubank TA, Garey KW. Proton pump inhibitor effect on macrophage and neutrophil function: a systematic review. Front Immunol. 2024;151477993. doi:10.3389/fimmu.2024.1477993
25. Ghebremariam YT, Cooke JP, Gerhart W, et al. Pleiotropic effect of the proton pump inhibitor esomeprazole leading to suppression of lung inflammation and fibrosis. J Transl Med. 2015:13249. doi:10.1186/s12967-015-0614-x.
26. Lechien JR, Carroll TL, Bobin F, et al. Influence of Age and Sex on Clinical and Therapeutic Features of Laryngopharyngeal Reflux. Otolaryngol Head Neck Surg. 2022;166(3):468–476. doi:10.1177/01945998211020284
27. Boom L, Edens M, Rinia B. Reflux finding score and reflux symptom index as potential predictors for proton pump inhibitor response in globus pharyngeus patients: a prospective study. Auris Nasus Larynx. 2020;47(4):609–615. doi:10.1016/j.anl.2020.02.002
28. Hayat JO, Gabieta-Somnez S, Yazaki E, et al. Pepsin in saliva for the diagnosis of gastro-oesophageal reflux disease. Gut. 2015;64(3):373–380. doi:10.1136/gutjnl-2014-307049
29. Zhang M, Pandolfino JE, Zhou X, et al. Assessing different diagnostic tests for gastroesophageal reflux disease: a systematic review and network meta-analysis. Therap Adv Gastroenterol. 2019:121756284819890537. doi:10.1177/1756284819890537.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.