Back to Journals » Drug Design, Development and Therapy » Volume 19
Protective Effect of Dexmedetomidine Combined with Butorphanol on Perioperative Pulmonary Function in Patients Undergoing Laparoscopic Colorectal Cancer Resection: A Randomized, Double-Blind, 2 * 2 Factorial-Controlled Trial
Authors Li H, Zhou G, Chen H, Liu T ![]() , Xu W, Guo D, Wang S, Gao F
, Xu W, Guo D, Wang S, Gao F ![]()
Received 24 August 2025
Accepted for publication 21 December 2025
Published 30 December 2025 Volume 2025:19 Pages 11911—11923
DOI https://doi.org/10.2147/DDDT.S562937
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Tamer Ibrahim
Huan Li,1,2,* Guangyue Zhou,1,2,* Haoxuan Chen,1,2 Tianya Liu,1,2 Wen Xu,1,2 Dinghui Guo,1,2 Su Wang,1,2 Fang Gao1,2
1Department of Anesthesiology, The Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 2Jiangsu Province Key Laboratory of Anesthesiology, Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fang Gao, Department of Anesthesiology, The Affiliated Hospital of Xuzhou Medical University, No. 99 Huaihai West Road, Xuzhou, Jiangsu, 221002, People’s Republic of China, Tel +86-18052268331, Email [email protected]
Background: Perioperative lung injury significantly affects the outcome of abdominal surgery. Research has shown that both dexmedetomidine and butorphanol can provide some perioperative lung protection. This study evaluated the protective effects of dexmedetomidine or metoprolol on lung function during laparoscopic resection of colorectal cancer and the potential synergistic effects of their combined use.
Methods: A 6-month randomized double-blind placebo-controlled trial with a 2*2 factorial design was conducted at the Affiliated Hospital of Xuzhou Medical University. 176 patients undergoing laparoscopic colorectal cancer resection were randomized into four groups: control (C), dexmedetomidine (D), butorphanol (B), and combination dexmedetomidine + butorphanol (DB). The primary outcome was the arterial-alveolar oxygen partial pressure ratio (a/A ratio) at the end of the administration period (T1). Secondary outcomes included other lung function indices, incidence of postoperative pulmonary complications (PPCs) and other complications, the 15-item Recovery Quality Score (QoR-15) scores, and postoperative inflammatory marker levels.
Results: Factorial analysis revealed significant main effects for Group D on the arterial alveolar oxygen partial pressure ratio (a/A ratio) at T1 (F=18.739, P < 0.001, η2=0.098), and Group B (F=19.048, P < 0.001, η2=0.1), with a significant a significant interaction effect between Group D and Group B (F=6.690, P=0.011, η2=0.037). Administration of dexmedetomidine reduced the alveolar-arterial oxygen pressure difference (A-aDO2), intrapulmonary shunt rate (Qs/Qt), and dead space to tidal volume ratio (Vd/Vt) compared to the control. Butorphanol lowered A-aDO2, decreased pulmonary complications on postoperative day 3, reduced postoperative nausea and vomiting, and improved recovery quality. The combination therapy further reduced Vd/Vt, decreased pulmonary complications on postoperative days 1 and 3, and lowered postoperative IL-6 levels.
Conclusion: Dexmedetomidine combined with butorphanol enhances lung function in laparoscopic surgery patients by improving gas exchange, boosting ventilation efficiency, reducing inflammation, and decreasing postoperative pulmonary complications.
Keywords: dexmedetomidine, butorphanol, perioperative lung protection, ventilator-associated lung injury, postoperative pulmonary complications
Introduction
Perioperative lung injury encompasses a range of conditions, including lung inflammation, impaired gas exchange, radiological abnormalities, and respiratory failure, which serve as alternative endpoints for its characterization.1 Laparoscopic resection of colorectal cancer is a pivotal treatment method for this disease. During surgery, initiating the Trendelenburg position and creating a carbon dioxide (CO2) pneumoperitoneum result in elevated thoracic pressure, collapse of lung-dependent regions, and alveolar damage, leading to the development of atelectasis. This, in turn, causes intrapulmonary shunting, reduced lung compliance, heightened pulmonary vascular resistance, and increased vulnerability to inflammatory lung damage.2–4 In addition, ventilator-induced lung injury (VILI) resulting from mechanical ventilation and systemic inflammatory response due to surgical stimulation increase the susceptibility of patients undergoing laparoscopic colorectal cancer surgery to perioperative lung injury.5–7
Perioperative lung protection involves actively preventing and treating lung injuries from various causes and risk factors to avert pulmonary complications, preserve lung function, and facilitate early recovery. Dexmedetomidine (DEX), a highly selective α2 adrenergic receptor (α2AR) agonist, offers lung protection by modulating pulmonary vasoconstriction, mitigating pulmonary vascular ischemia-reperfusion injury, and suppressing inflammatory factor release.8–11 Butorphanol (BUT), a lipophilic anesthetic, acts as a potent κ-receptor agonist and a weak μ-receptor agonist-antagonist. Animal studies indicate that BUT can inhibit Nuclear Factor kappa B (NF-κB), mitogen-activated protein kinase, and Toll-like receptor signaling pathway (TRIF) via κ receptors, facilitating macrophage phenotypic transformation and reducing inflammatory lung injury.12,13 Furthermore, research shows BUT enhances lung function by improving oxygenation and decreasing dead space ventilation in obese patients undergoing laparoscopic bariatric surgery.14
Most patients undergoing elective surgery exhibit normal preoperative lung function. Perioperative lung injury primarily arises from the stress response and inflammation induced by surgery, along with mechanical ventilation.4 While mechanical ventilation is essential, its adverse effects are somewhat unavoidable, though potentially modifiable through pharmacological intervention. A study has found that DEX and BUT can simultaneously activate µ - opioid receptors (MOR), κ - opioid receptors (KOR), δ - opioid receptors (DOR), and α 2Ars, and exhibit synergistic effects.15 This study hypothesized that DEX and BUT could protect lung function during laparoscopic colorectal cancer resection by mitigating inflammatory lung injury and enhancing oxygenation. We conducted a prospective, 2*2 factorial-controlled trial to assess the impact of DEX combined with BUT on perioperative lung function and to determine whether their combination offers advantages over single-drug use.
Methods
Ethics Statement
This prospective, single-center, double-blind trial followed a 2 * 2 factorial design. The study was registered in the Chinese Clinical Trial Registry (ChiCTR2400081959), approved by the Ethics Committee of the Affiliated Hospital of Xuzhou Medical University (Jiangsu, China; XYFY2024-KL027-02), and adhered to the Declaration of Helsinki. Prior to enrollment, all patients provided written informed consent.
Participants
Patients who underwent laparoscopic colorectal cancer resection under general anesthesia at the Affiliated Hospital of Xuzhou Medical University between March 2024 and September 2024 were included in the study. Inclusion criteria comprised: (1) age between 18 and 65 years; (2) body mass index (BMI) of 18.5–30 kg/m2; (3) American Society of Anesthesiologists (ASA) grade I–III; (4) elective laparoscopic colorectal cancer resection under general anesthesia; and (5) provision of informed consent. Exclusion criteria included: (1) severe liver or kidney dysfunction, moderate to severe anemia (Hb < 90g/L); (2) preoperative severe respiratory dysfunction (PaO2 < 60mmHg), FEV1/FVC < 50%, or severe obstructive sleep apnea syndrome (OSAS); (3) known allergy to study drugs or contraindications (such as: severe heart block; severe ventricular dysfunction; or rely on Nocitine) and (4) severe mental disorders or hearing impairment hindering communication. Additional exclusion criteria encompassed: (1) conversion to open surgery or significant hemorrhage (≥800mL or 20% of total blood volume rapidly); (2) withdrawal from the trial or unsuccessful follow-up for various reasons.
Randomization
Patients were randomly assigned to one of four groups: control (Group C), DEX (Group D), BUT (Group B), and DEX + BUT (Group DB) using a random number table The specific steps are as follows: (1) Generate a random sequence: Use a random number generator to generate a random sequence consisting of 184 random numbers from 1 to 184; (2) Allocation sequence: Randomly allocate the trial patients according to the order of surgical arrangement; (3) Grouping: Group C (Control group, n=46) consists of sequences 1–46; The D group (DEX group, n=46) consists of sequences 47–92; Group B (BUT group, n=46) consists of sequences 93–138; The DB group (DEX combined with BUT group, n=46) consists of sequences 139–184. Each patient’s administration method was concealed in an opaque, sealed envelope, which was opened by the researchers only prior to anesthesia induction. Apart from the intraoperative management researchers, the patients, preoperative interview evaluators, and postoperative follow-up personnel remained blinded to the group assignments. The anesthesiologist responsible for intraoperative management does not participate in preoperative visits, grouping, postoperative follow-up evaluations, and data collection.
Optimization of Anesthesia
Patients fasted for 6 to 8 hours before undergoing routine monitoring of peripheral oxygen saturation (SpO2), heart rate (HR), electrocardiogram, bispectral index (BIS), and end-tidal CO2 partial pressure (PET-CO2) upon room entry. Anesthesia induction was achieved via intravenous administration of etomidate (0.05–0.2 mg/kg), sufentanil (0.2–0.4 μg/kg), midazolam (0.1 mg/kg), and rocuronium (0.6 mg/kg). Tracheal intubation was performed using a visual laryngoscope, with an internal diameter of 7.0 mm for males and 6.5 mm for females. The tracheal tube was secured after confirming normal PET-CO2 waveforms and airway pressure on the ventilator. Mechanical ventilation settings included a respiratory rate of 12–20 breaths per minute, an inspiratory-to-expiratory ratio of 1:2, a tidal volume of 6–8 mL/kg, an oxygen flow rate of 2 L/min, an inhaled oxygen concentration (FiO2) of 60%, and the PET-CO2 was maintained between 35–45 mmHg. A Positive End-expiratory Pressure (PEEP) of 5 cmH2O was applied, reduced if peak airway pressure exceeded 30 mmHg. Post-induction, vital signs remained stable Ultrasound-guided transversus abdominis plane block with 0.75% ropivacaine hydrochloride (150 mg) and central venous catheterization via the right internal jugular vein were performed. Anesthesia was maintained using a combination of intravenous and inhalational agents: sevoflurane at 0.6%-1.0%, propofol at 4–6 mg kg−1 h−1, remifentanil at 0.1–0.3 μg kg−1 min−1, and rocuronium at 0.15 mg/kg. Anesthesia depth was adjusted to a BIS of 40–60, with anesthetic doses modified based on BIS, mean arterial pressure (MAP), and heart rate. If the mean arterial pressure decreases by 20% from the baseline value, the following measures are taken based on the presence of bradycardia: In the absence of bradycardia, administer a single intravenous dose of 20–40 μg of epinephrine. If bradycardia is present, administer a single intravenous dose of 1–3 mg of ephedrine, which may be repeated if necessary. In cases where the heart rate falls below 50 beats per minute (HR < 50 bpm), administer 0.25–0.50 mg of atropine intravenously. Sevoflurane was discontinued upon skin suturing, propofol 5–10 minutes before suture completion, and remifentanil immediately after suturing.
The patient was transferred to the Post-Anesthesia Care Unit (PACU) post-surgery. In the PACU, any residual neuromuscular blockade was reversed with neostigmine (0.04 mg/kg) and atropine (0.01 mg/kg) once the tidal volume of spontaneous ventilation surpassed 200 mL Patients were continuously monitored for the return of consciousness, evidenced by appropriate responses to verbal cueing. Tracheal extubation was performed when patients exhibited spontaneous eye opening and a respiratory rate exceeding 10 breaths per minute voluntarily. Pain assessment using the Numeric Rating Scale (NRS) was conducted every 10 minutes post-extubation, with Dezocine 5 mg administered for NRS scores ≥ 4. Patients were reassessed within 10 minutes, with additional doses administered as needed. Upon achieving consciousness, an NRS score ≤ 3 without nausea or vomiting, patients were discharged from the PACU to the ward. In the ward, patients with NRS scores above 4 received Dezocine 5 mg every 6 hours.
Test Grouping and Administration Method
Patients meeting the inclusion criteria were randomly assigned to four groups: Group C, Group D, Group B, and Group DB. Start pumping medication immediately after cutting the skin and stop pumping immediately after suturing the skin for all groups.
Group C received intravenous infusions of two normal saline solutions: one at a rate of 0.05 mL h−1 kg−1 and the other initially at 0.1 mL h−1 kg−1 for 10 minutes before being adjusted to 0.05 mL h−1 kg−1. Group D received an intravenous infusion of DEX (20 ug/mL) at a rate of 0.1 mL h−1 kg−1 for 10 minutes, then adjusted to 0.05 mL h−1 kg−1, along with a simultaneous infusion of normal saline at 0.05 mL h−1 kg−1. Group B received BUT (200ug/mL) at a rate of 0.05 mL h−1 kg−1, along with a simultaneous infusion of normal saline initially at 0.1 mL h−1 kg−1 for 10 minutes before being adjusted to 0.05 mL h−1 kg−1. Group DB received DEX (20ug/mL) at a rate of 0.1 mL h−1 kg−1 for 10 minutes, then adjusted to 0.05 mL h−1 kg−1, along with a simultaneous infusion of BUT (200ug/mL) at 0.05 mL h−1 kg−1.
Methods of Blood Sample Collection and Lung Function Evaluation
One milliliter each of radial artery blood and central venous blood was collected at two time points: within 2 minutes before the start of administration (T0) and within 2 minutes after the end of administration (T1). Blood gas analysis was conducted using a ABL90 Flex blood gas analyzer. Additionally, peripheral venous blood was obtained on the second postoperative day and analyzed at our hospital’s laboratory to assess the levels of Interleukin-6 (IL-6), IL-8, IL-10, Tumor necrosis factor-α (TNF-α), and procalcitonin (PCT).
Prior to the trial, all patients were assessed for the risk of Postoperative pulmonary complications (PPCs) using a simple risk prediction index, with scores recorded and compared between groups as a baseline.16 Pulmonary function was assessed through the arterial alveolar oxygen partial pressure ratio (a/A ratio), intrapulmonary shunt rate (Qs/Qt), oxygenation index (OI), alveolar-arterial oxygen pressure difference (A-aDO2), and dead space to tidal volume ratio (Vd/Vt), calculated using relevant formulas.17 The central venous catheter was placed to collect blood samples instead of mixed venous blood samples.18 Postoperative Pulmonary Complications (PPCs) are determined according to the definition in the Assess Respiratory Risk in Surgical Patients in Catalonia (ARISCAT) index.19 Blood gas analysis measured the partial pressures of oxygen and CO2, as well as hemoglobin concentration. FiO2 and PET-CO2 were directly recorded from the anesthesia machine during mechanical ventilation.
Outcomes
This study’s primary outcome was the a/A ratio at T1. Secondary outcomes included: (1) additional lung function indicators (OI, A-aDO2, Vd/Vt, Qs/Qt); (2) incidence of PPCs on the 1st, 3rd, and 7th days post-operation.; (3) inflammatory markers: IL-6, IL-8, IL-10, TNF-α, and PCT; (4) incidence of emergence agitation (EA) within 30 minutes post-extubation (EA, assessed every 10 minutes in the PACU, is defined as a Richmond Agitation-Sedation Scale (RASS) ≥ 2 at any point);20 postoperative shivering, subcutaneous emphysema, postoperative nausea and vomiting (PONV), and need for postoperative salvage analgesia; (5) The 15-item Recovery Quality (QoR-15) Score on the 1st, 3rd, and 7th days post-operation.
Statistical Analysis
The sample size was determined based on the primary outcome measure (a/A ratio at T1), assuming no interaction between the DEX and BUT. Pre-test results indicated the mean ± standard deviation of the a/A ratio at T1 for groups C, D, B, and DB (10 patients per group) were 81.04 ± 3.85, 92.83 ± 7.55, 96.74 ± 7.13, and 96.69 ± 12.01, respectively. Using PASS v21.0.3 software (NCSS, LLC, Caseville, Utah, USA), the sample size was calculated with a 1:1:1:1 distribution ratio, a significance level of 0.05, and a power of 0.80, resulting in 39 participants per group, totaling 156. Accounting for a 15% dropout rate, 46 patients were included in each group.
Statistical analyses were conducted using SPSS 26.0. All tests were two-sided with a significance level of α=0.05, considering P<0.05 as statistically significant. The Kolmogorov–Smirnov test assessed the normality of variable distributions. Normally distributed quantitative data were reported as mean ± standard deviation ( ± S), with variance homogeneity evaluated via Levene’s or Bartlett’s test. Non-normally distributed data were presented as median (M) and interquartile range (IQR), while categorical variables were expressed as numbers and percentages. The chi-square or Fisher’s exact test was applied for categorical analysis. For normally distributed data with homogeneous variance, ANOVA was employed; the Kruskal-Walli’s test was used for non-normally distributed data. Factorial ANOVA assessed individual and main effects, as well as interaction effects. If interactions were significant, simple effect analysis followed; if not, and a main effect was present, Bonferroni correction facilitated intergroup comparisons. Controlling for confounding factors using hierarchical regression analysis.
± S), with variance homogeneity evaluated via Levene’s or Bartlett’s test. Non-normally distributed data were presented as median (M) and interquartile range (IQR), while categorical variables were expressed as numbers and percentages. The chi-square or Fisher’s exact test was applied for categorical analysis. For normally distributed data with homogeneous variance, ANOVA was employed; the Kruskal-Walli’s test was used for non-normally distributed data. Factorial ANOVA assessed individual and main effects, as well as interaction effects. If interactions were significant, simple effect analysis followed; if not, and a main effect was present, Bonferroni correction facilitated intergroup comparisons. Controlling for confounding factors using hierarchical regression analysis.
Results
Out of 216 patients initially screened, 32 were excluded: 17 for not meeting inclusion criteria, 11 for meeting exclusion criteria, and 4 for refusal to participate. The remaining 184 patients were randomly allocated into 4 groups with 46 patients in each. Throughout the study, four patients required conversion to open surgery, three patients underwent subsequent surgical procedures, and one patient was transferred to the intensive care unit following a sudden heart attack occurring 2 hours post-extubation. Ultimately, 176 patients successfully completed the trial and were included in the analysis. Please refer to Figure 1 for the patient selection flowchart.
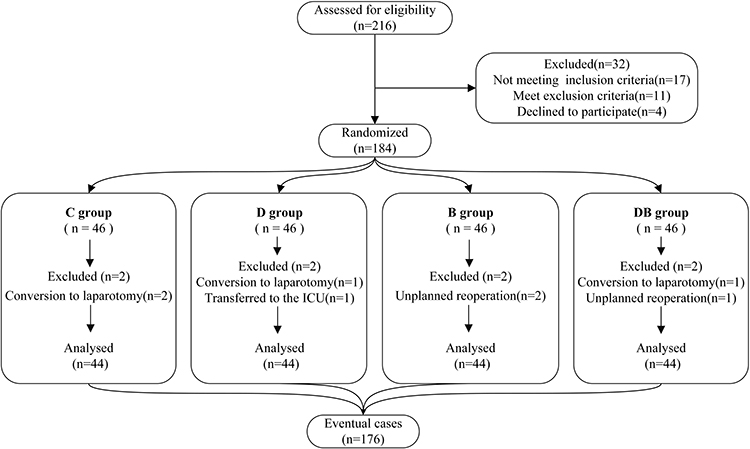 |
Figure 1 Flow diagram of the study. C, control group; D, dexmedetomidine group; B, butorphanol group; DB, dexmedetomidine + butorphanol group. |
Table 1 demonstrates that there were no significant variations among the four groups in baseline characteristics, preoperative complications, simple risk prediction index, intraoperative parameters (such as operation time, anesthesia time, anesthetic drug usage, fluid intake and output, and extubation time), and hospitalization duration (P > 0.05).
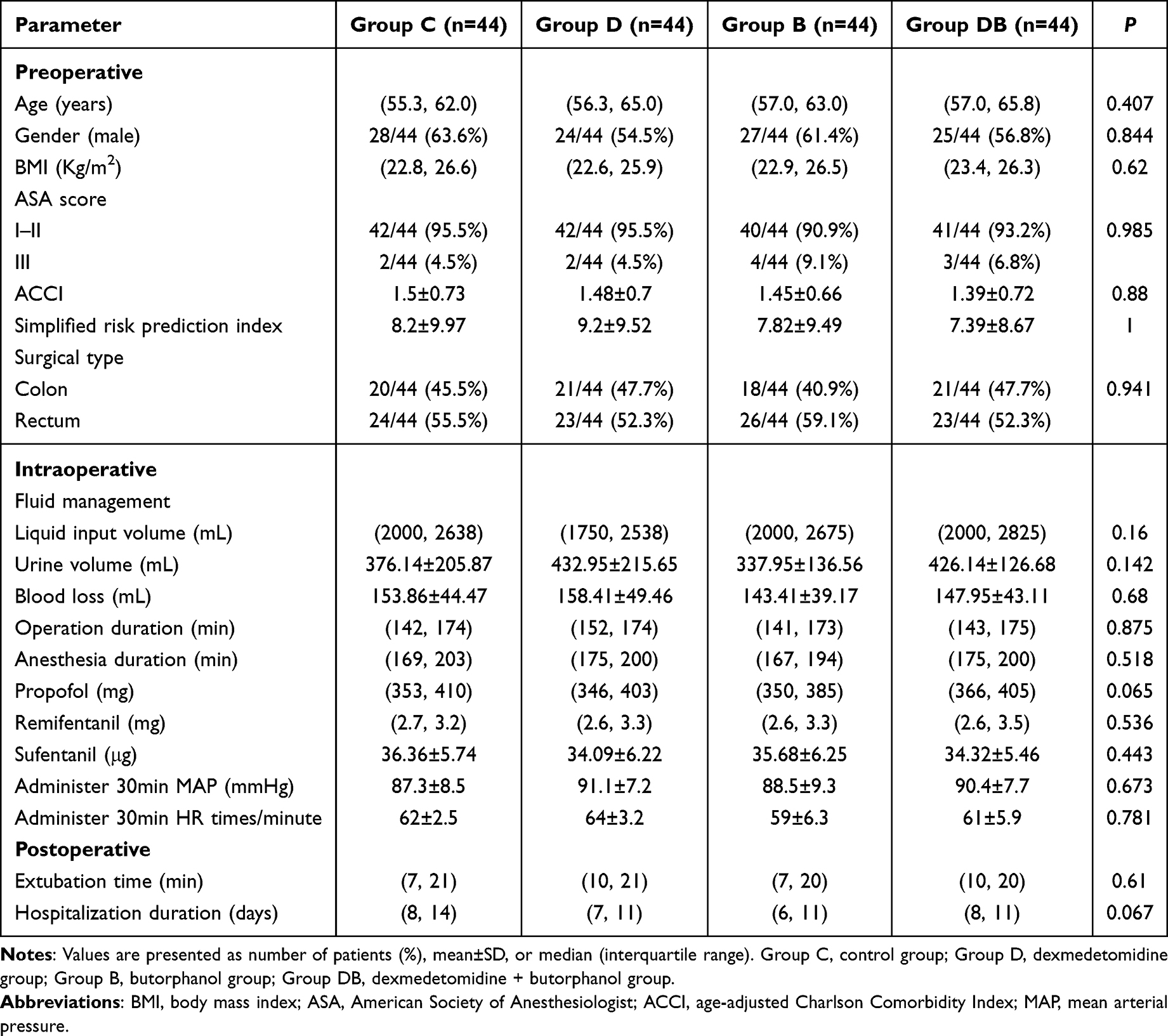 |
Table 1 Baseline Patient Characteristics and Anesthetic Management Parameters |
Primary Outcome
As depicted in Figure 2, the a/A ratio serves as a metric for assessing lung gas exchange efficiency, with lower values indicating reduced efficiency and a potential mismatch in ventilation/blood flow ratio. At baseline (T0), there were no notable discrepancies in the a/A ratio across the four groups (P >0.05). Group C exhibited no significant alteration in the a/A ratio between T0 and T1 (P >0.05). Conversely, at T1, the a/A ratio significantly rose in groups D, B, and DB compared to T0, with a statistically significant difference (P <0.05).
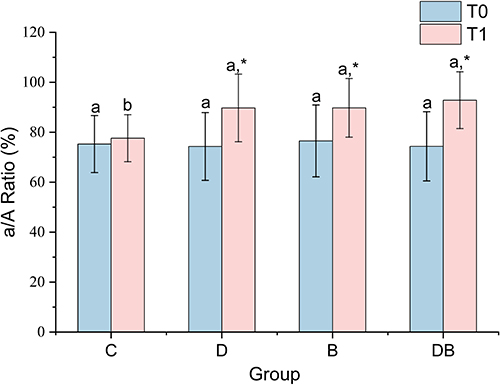 |
Figure 2 Bar chart of a/A ratio for four groups of T0 and T1.C, control group; D, dexmedetomidine group; B, butorphanol group; DB, dexmedetomidine + butorphanol group. a, the group with the highest mean among the four groups or compared to it, with no statistically significant difference (P>0.05, pairwise comparison); b, compared with a, the difference is statistically significant (P<0.05, pairwise comparison); *Compared with T0, the difference is statistically significant. (P<0.05). Abbreviations: a/A ratio, arterial alveolar oxygen partial pressure ratio. |
The analysis revealed a significant main effect for Group D (F=18.739, P < 0.001, η2=0.098), indicating that DEX exerts a significant influence on the a/A ratio at T1. Similarly, a significant main effect was observed for Group B (F = 19.048, P < 0.001, η2=0.1), demonstrating that Group B also significantly impacts the a/A ratio at T1, with an effect size comparable to that of Group D. Furthermore, a significant interaction effect between Group D and Group B was identified (F = 6.690, P=0.011, η2 = 0.037), suggesting that the effects of these groups on the a/A ratio at T1 are not independent but rather interdependent. Hierarchical regression analysis was employed to adjust for age, gender, body mass index (BMI), and risk prediction indices ASA and Age-adjusted Charlson comorbidity index (ACCI).Following the inclusion of variables such as surgical type and duration, the findings indicated that DEX and BUT continued to exert a notable influence on the a/A ratio at T1 (ΔR2=0.086, P<0.001). Moreover, a significant interaction effect was observed between Group D and Group B (F=6.141, P <0.001).
Further analysis of simple effects revealed that, in the absence of DEX, the simple effects of Group B were statistically significant (F=24.16, P< 0.001, η2 = 0.123). This suggests that BUT exerts a significant influence on the a/A ratio at T1 when DEX is not administered. Conversely, when DEX was used, the simple effect of Group B was not significant (F=1.58, P=0.21, η2=0.009), indicating that BUT has a negligible impact on the a/A ratio at T1 in the presence of DEX.
Secondary Outcome
Table 2 presents the a/A ratio, OI, A-aDO2, Qs/Qt, and Vd/Vt values for the four groups at T0 and T1. The analysis revealed no significant differences in OI, A-aDO2, Qs/Qt, and Vd/Vt among the four groups at T0 (P > 0.05). In Group C, there were no significant differences in OI, A-aDO2, Qs/Qt, and Vd/Vt between T0 and T1 (P >0.05). Conversely, significant differences in OI, A-aDO2, Qs/Qt, and Vd/Vt between T0 and T1 were observed in groups D, B, and DB (P <0.05). At T1, there was no significant difference in OI values among the four groups (P > 0.05). However, significant differences were observed at T1 among the four groups in A-aDO2, Qs/Qt, and Vd/Vt. Pairwise comparisons (following Bonferroni correction) indicated that compared to Group C, Group D exhibited lower A-aDO2, Qs/Qt, and Vd/Vt at T1 (P A-aDO2 = 0.005, P Qs/Qt = 0.001, P Vd/Vt = 0.041). Additionally, in Group B, A-aDO2 was lower at T1.
 |
Table 2 The a/A Ratio, OI, A-aDO2, Qs/Qt, and Vd/Vt Values at T0 and T1 |
PPCs, including respiratory infection, respiratory failure, bronchospasm, atelectasis, pleural effusion, pneumothorax, and aspiration pneumonia, were defined according to the ARISCAT criteria.17 Figure 3 illustrates a significant variance in the occurrence of PPCs among the four groups on the first- and third-days post-surgery (Pday1 = 0.046, Pday3 = 0.016), with no notable difference on the seventh day (Pday7 > 0.05). Pairwise comparisons (adjusted using Bonferroni correction) revealed that compared to Group C, Group DB exhibited lower PPCS rates on the first day post-surgery, while both Group B and Group DB had lower rates on the third day. Notably, there was a significant discrepancy in PONV incidence (P=0.03), with Group B showing lower rates compared to Group C. Conversely, no significant variations were observed among the groups concerning subcutaneous emphysema, postoperative chills, remedial analgesia, and EA (P > 0.05). (For more supplementary content, please refer to Supplementary Tables 1 and 2).
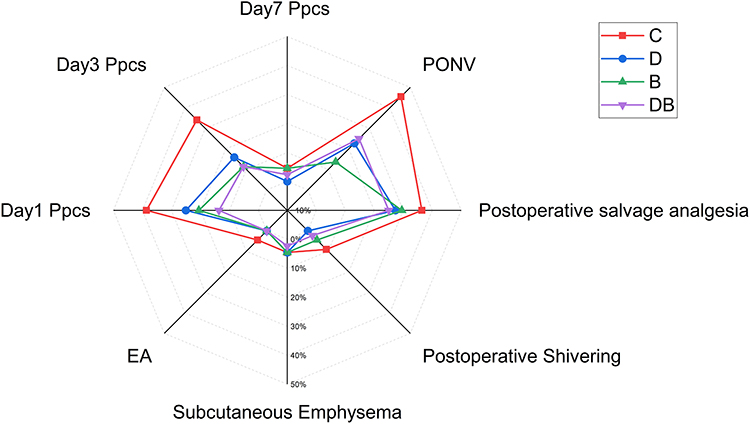 |
Figure 3 Radar chart of the incidence of postoperative complications and salvage analgesia. C, control group; D, dexmedetomidine group; B, butorphanol group; DB, dexmedetomidine + butorphanol group. Abbreviations: PPCs, postoperative pulmonary complications; PONV, postoperative nausea and vomiting; EA, emergence agitation. |
QoR-15 scores effectively assess postoperative recovery across various clinical contexts.19 As depicted in Figure 4, significant differences in QoR-15 scores were observed among the four groups on postoperative days 1, 3, and 7 (P < 0.05). Pairwise comparisons with Bonferroni correction revealed that Group B had higher QoR-15 scores than Group C and Group D on day 1 (Pday1-C < 0.001, Pday1-D = 0.024). On days 3 and 7, Group B outperformed all other groups (Pday3-C = 0.001, Pday3-D = 0.001, Pday3-DB = 0.003; Pday7-C < 0.001, Pday7-D < 0.001, Pday7-DB = 0.001), indicating superior postoperative recovery in Group B (Supplementary Table 3).
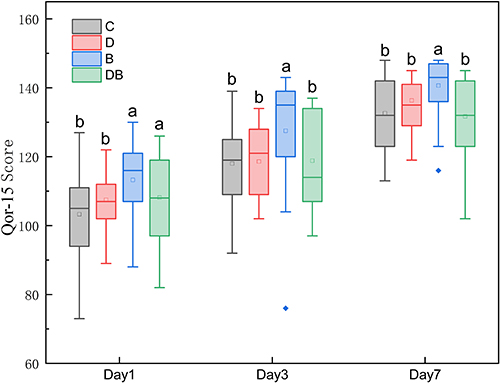 |
Figure 4 Box plot of the QoR-15 scores among the four groups on postoperative days 1, 3, and 7. C, control group; D, dexmedetomidine group; B, butorphanol group; DB, dexmedetomidine + butorphanol group. a, the group with the highest mean among the four groups or compared to it, with no statistically significant difference (P>0.05, pairwise comparison); b, compared with a, the difference is statistically significant (P<0.05, pairwise comparison). Abbreviations: QoR-15, The 15-item Recovery Quality Scale. |
Postoperative IL-6 concentrations were lower in Group DB compared to Group C (P=0.031), whereas no significant differences were observed in postoperative IL-8, IL-10, TNF-α, and PCT levels across the four groups, as illustrated in Figure 5. The combined administration reduced IL-6 release, indicating a potential mechanism for the lung-protective effects of the combination (Supplementary Table 4).
 |
Figure 5 Bar chart of postoperative inflammatory factors. C, control group; D, dexmedetomidine group; B, butorphanol group; DB, dexmedetomidine + butorphanol group. a, the group with the highest mean among the four groups or compared to it, with no statistically significant difference (P>0.05, pairwise comparison); b, compared with a, the difference is statistically significant (P<0.05, pairwise comparison). Abbreviations: IL, Interleukin; PCT, procalcitonin. |
The salvage analgesic Dezocine, acting as a kappa receptor agonist and a mu receptor antagonist, may influence postoperative recovery quality, postoperative pulmonary complication rates, and postoperative inflammatory factor levels. Through stratified regression analysis controlling for the number of salvage analgesics, statistically significant differences persisted in postoperative QOR-15 scores, incidence of pulmonary complications on the first and third postoperative days, and IL-6 concentration across the four groups. Conversely, there was no significant distinction in rescue analgesia frequency among the groups, suggesting a balanced impact of Dezocine on the relevant outcome indicators within the four groups.
Discussion
This study assessed the protective effects of DEX and BUT on lung function in patients undergoing laparoscopic colorectal cancer surgery. Our results indicate that: (1) DEX or BUT monotherapy enhances lung protection by ameliorating intraoperative pulmonary ventilation, enhancing gas exchange efficiency, and decreasing intrapulmonary shunt, as evidenced by improvements in parameters such as the a/A ratio, Qs/Qt, A-aDO2, and Vd/Vt. (2) Synergistic effects of DEX and BUT combination: Concurrent administration resulted in a notably superior enhancement in the a/A ratio compared to individual agent use, suggesting a synergistic interplay. (3) Clinical advantages of intraoperative administration: Both medications lowered the occurrence of PPCs and improved recovery quality. The combined treatment notably decreased PPCs and reduced postoperative IL-6 levels.
The combination of DEX and BUT demonstrates a significant synergistic effect in enhancing the a/A ratio, potentially achieved through the interaction with multiple receptors and the simultaneous suppression of inflammatory signaling pathways. Fundamental research has elucidated a multifaceted pharmacological foundation for this synergy: animal studies have confirmed the concurrent activation of µ-opioid receptors (MORs), κ-opioid receptors (KORs), δ-opioid receptors (DORs), and α2Ars.15 This multi-target synergistic mechanism has been supported by clinical evidence. Several randomized controlled trials have indicated that the DEX–BUT combination improves postoperative analgesia, extends its duration, and optimizes the depth of sedation, implying potential benefits for perioperative organ protection.21–23
The opioid receptor system plays a crucial role in the regulation of inflammation. Research indicates that pure kappa opioid receptor (KOR) antagonism can worsen lipopolysaccharide-induced systemic inflammation by increasing the levels of proinflammatory cytokines IL-1β and IL-6 in the peripheral blood of mice.24 Clinical studies have revealed that patients receiving treatment with BUT show reduced levels of TNF-α and IL-1β, as well as elevated IL-10 levels.25 This effect could be attributed to BUT’s partial agonist activity at the KOR. Moreover, DEX is recognized as a potent anti-inflammatory agent with demonstrated efficacy in various species models for suppressing inflammatory responses. Studies have shown that its administration leads to reductions in IL-6 and TNF-α levels in animals experiencing severe inflammation, as well as decreased levels of IL-6, TNF-α, and C-reactive protein in surgical patients.14,26 While this study did not find significant differences in inflammatory markers between Group D or B compared to Group C, the combined use of both agents notably decreased the occurrence of PPCs and levels of postoperative IL-6. This observed effect is likely due to the inhibition of the NF-κB pathway by DEX and BUT, resulting in the suppression of pulmonary inflammation and release of inflammatory cytokines.13,14 This mechanism potentially explains the synergistic lung-protective outcomes of the combined therapy, suggesting the need for further research in this area.
Previous research indicates that DEX, a selective α2-adrenergic receptor agonist, reduces the shunt fraction (Qs/Qt) during one-lung ventilation (OLV) by inhibiting histamine-induced bronchoconstriction and improving pulmonary ventilation efficiency.9,10,27 Our study revealed that the Qs/Qt ratio in the DEX group was significantly lower compared to the other groups (P <0.05), aligning with prior observations and indicating a consistent positive impact of DEX on pulmonary hemodynamics.
The study revealed an increase in the oxygenation index (OI) at T1 compared to T in Group D (406.51 ± 62.81 mmHg vs 445.12 ± 65.17 mmHg), consistent with previous reports of DEX enhancing OI in septic patients.28 However, no statistically significant difference in OI was evident among the four groups at T1. This disparity may be attributed to contextual variations: prior favorable outcomes were predominantly observed in OLV or acute lung injury cohorts, whereas this investigation included patients undergoing two-lung ventilation during laparoscopic procedures. The distinct mechanical stresses associated with these ventilation strategies might have partially obscured the OI-enhancing effects of DEX in the context of laparoscopic two-lung ventilation. Thus, the assessment of lung-protective drug efficacy should account for the specific respiratory mechanical milieu.
Contrary to previous research, a recent meta-analysis has shown inadequate evidence to substantiate the impact of DEX on pneumonia or acute respiratory distress syndrome.29 The occurrence of PPCs in Group D did not exhibit a significant variance compared to Group C in this study. Various mechanisms could elucidate this finding: the anti-inflammatory properties of DEX might necessitate a specific threshold to manifest as enhancements in clinical endpoints; during laparoscopic surgery, the physical lung damage associated with pneumoperitoneum could be the predominant factor in the development of PPCs, overshadowing the influence of pure inflammatory regulation. Further exploration is warranted to elucidate this matter.
Kappa opioid receptor (KOR) has been shown to enhance pulmonary vascular function by reducing inflammation and vascular endothelial cell apoptosis.30 Additionally, KOR agonists have been found to have both preventive and therapeutic benefits in hypoxic pulmonary hypertension and high-altitude pulmonary edema by improving pulmonary vascular function and reducing oxidative stress.31 Previous research has established that buprenorphine (BUT), acting as a KOR agonist, safeguards pulmonary vasculature and enhances lung function.15 The results of this study further corroborate the role of BUT in improving pulmonary ventilation, optimizing gas exchange efficiency, and decreasing the occurrence of PPCs. Group B demonstrated the lowest occurrence of PONV, possibly due to BUT’s antagonistic impact on MOR, thus mitigating or eradicating MOR-related side effects like PONV. Consequently, the superior recovery quality observed in Group B could be linked to its reduced PONV incidence.
Although dezocine, a rescue analgesic acting as a KOR agonist and MOR antagonist, could potentially influence QoR-15 scores, PPC incidence, and postoperative inflammatory cytokine levels, several factors mitigate its impact in this study. First, there was no statistically significant difference in the number of rescue analgesic administrations across the four groups. Second, even after adjusting for the number of rescue doses using stratified regression analysis, the differences in QoR-15 scores, PPC rates on postoperative days 1 and 3, and IL-6 levels remained statistically significant. Therefore, we conclude that the influence of dezocine on the relevant outcome measures was balanced across all groups.
Limitation
This study has several limitations. Firstly, it is a single-center study with a limited sample size, focusing solely on laparoscopic colorectal cancer resection. To enhance generalizability, large multicenter trials encompassing diverse surgical types are necessary. Secondly, the study evaluated lung function using only the a/A ratio, Qs/Qt, OI, A-aDO2, and Vd/Vt, omitting respiratory mechanics indicators during mechanical ventilation. Additionally, while the incidence of PPCs was observed, their severity was not assessed. Thirdly, this study focused solely on the short-term effects of DEX and BUT on lung function, leaving the long-term impacts unexplored. Finally, the primary pathophysiological alterations in VILI include pulmonary vascular endothelial cell damage and heightened vascular permeability.32 Although changes in Clara cell secretory protein (CC16), endothelin-1 (ET-1), and intercellular adhesion molecule-1 (ICAM-1) concentrations may indicate the extent of lung tissue injury, these biomarkers were not assessed in this study.33–36
Conclusion
In summary, intraoperative intravenous infusion of DEX and BUT can significantly improve lung ventilation efficiency and reduce the incidence of PPCs, which has a certain positive significance in protecting patients’ perioperative lung function. The combination therapy of the two is superior to monotherapy and has high safety, which is worth promoting in clinical practice.
Abbreviations
A-aDO2, Alveoli arterial oxygen pressure difference; a/A ratio, Arterial alveoli oxygen pressure ratio; α2AR, α2 adrenergic receptor; ASA, American society of anesthesiologists; ARISCAT, Assess respiratory risk in surgical patients in catalonia; BMI, Body mass index; BIS, Bispectral index; BUT, Butorphanol; CO2, Carbon dioxide; DEX, Dexmedetomidine; DOR, δ-opioid receptor; EA, Emergence agitation; FiO2, Inhaled oxygen concentration; HR, Heart rate; ICU, intensive care unit; KOR, κ-receptor; LPVS, Lung protective ventilation strategy; MAP, Mean arterial pressure; MAPK, Mitogen-activated protein kinase; MOR, µ-opioid receptor; NF-κB, Nuclear factor κB; NRS, Numerical rating scale; OI, Oxygenation index; OLV, One-lung ventilation; PACU, Post-anesthesia care unit; PCT, Procalcitonin; PETCO2, Partial pressure of end-tidal carbon dioxide; PEEP, Positive end-expiratory pressure; PONV, Postoperative nausea and vomiting; PPCs, Postoperative pulmonary complications; QoR-15, 15-item quality of recovery score; Qs/Qt, Intrapulmonary shunt rate; RASS, Richmond agitation-sedation scale; SpO2, Pulse oxygen saturation; TNF-α, Tumor necrosis factor-α; IFN, Interferon; IL, Interleukin; Vd/Vt, Dead space to tidal volume ratio; VILI, Ventilator-induced lung injury.
Data Sharing Statement
Please contact the corresponding author if you would like access to the datasets used or analyzed in this research.
Ethics Approval and Informed Consent
This trial was approved by the Ethics Committee of the Affiliated Hospital of Xuzhou Medical University (no. XYFY2024-KL027-02). The trial was registered before patient enrollment with the Chinese Clinical Trial Registry (ChiCTR2400081959). Written informed consent was obtained from all patients. This is in accordance with the Declaration of Helsinki.
Acknowledgments
The authors thank the Affiliated Hospital of Xuzhou Medical University for support with this study. The work described has not been submitted elsewhere for publication, in whole or in part, and all the authors listed have approved the enclosed manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Jiangsu Provincial Health Commission Medical Research Key Project (ZD2021015), Paired Assistance Scientific Research Project by The Affiliated Hospital of Xuzhou Medical University (FXJDBF2024216), and Construction Project of High-Level Hospital of Jiangsu Province (GSPJS202513).
Disclosure
The authors report no conflicts of interest in this work.
References
1. O’Gara B, Talmor D. Perioperative lung protective ventilation. Br Med J. 2018;362. doi:10.1136/bmj.k3030
2. Xue S, Wang D, Tu HQ, et al. The effects of robot-assisted laparoscopic surgery with Trendelenburg position on short-term postoperative respiratory diaphragmatic function. Anesthesiology. 2024;24(1):92. doi:10.1186/s12871-024-02463-3
3. Tharp WG, Neilson MR, Breidenstein MW, et al. Effects of obesity, pneumoperitoneum, and body position on mechanical power of intraoperative ventilation: an observational study. J Appl Physiol. 2023;134(6):1390–1402. doi:10.1152/japplphysiol.00551.2022
4. Yue H, Yong T. Progress in the relationship between mechanical ventilation parameters and ventilator-related complications during perioperative anesthesia. Postgrad MED J. 2024;100(1187):619–625. doi:10.1093/postmj/qgae035
5. Marini JJ, Rocco PRM, Gattinoni L. Static and Dynamic Contributors to Ventilator-induced Lung Injury in Clinical Practice. AM J RESP CRIT CARE. 2020;201(7):767–774. doi:10.1164/rccm.201908-1545CI
6. Goligher EC, Dres M, Fan E, et al. Mechanical Ventilation–induced Diaphragm Atrophy Strongly Impacts Clinical Outcomes. AM J RESP CRIT CARE. 2018;197(2):204–213. doi:10.1164/rccm.201703-0536OC
7. Hu S, Wan X, Li X, et al. Aerobic exercise alleviates pyroptosis-related diseases by regulating NLRP3 inflammasome. Front Physiol. 2022;13:965366. doi:10.3389/fphys.2022.965366
8. Xu B, Gao H, Li D, et al. Nebulized dexmedetomidine improves pulmonary shunt and lung mechanics during one-lung ventilation: a randomized clinical controlled trial. Peer J. 2020;8:e9247. doi:10.7717/peerj.9247
9. Lee SH, Kim N, Lee CY, et al. Effects of dexmedetomidine on oxygenation and lung mechanics in patients with moderate chronic obstructive pulmonary disease undergoing lung cancer surgery. EUR J ANAESTH. 2016;33(4):275–282. doi:10.1097/EJA.0000000000000405
10. Cui J, Gao M, Huang H, et al. Dexmedetomidine Improves Lung Function by Promoting Inflammation Resolution in Patients Undergoing Totally Thoracoscopic Cardiac Surgery. Oxid Med Cell Longevity. 2020;2020:8638301. doi:10.1155/2020/8638301
11. Bai Y, Zhang J, Zhao B, et al. Dexmedetomidine attenuates one‐lung ventilation associated lung injury by suppressing inflammatory responses: a systematic review and meta‐analysis. Clin Exp Pharmacol. 2021;48(9):1203–1214. doi:10.1111/1440-1681.13525
12. Zheng Y, Hu R, Hu J, et al. Protective effects of butorphanol in oleic acid-endotoxin “two-hit” induced rat lung injury by suppression of inflammation and apoptosis. Sci Rep. 2024;14(1):14231. doi:10.1038/s41598-024-53483-5
13. Luan G, Pan F, Bu L, et al. Butorphanol Promotes Macrophage Phenotypic Transition to Inhibit Inflammatory Lung Injury via κ Receptors. Front Immunol. 2021;12:692286. doi:10.3389/fimmu.2021.692286
14. Wang X, Zeng S, Li X, et al. The Protective Effects of Butorphanol on Pulmonary Function of Patients with Obesity Undergoing Laparoscopic Bariatric Surgery: a Double-Blind Randomized Controlled Trial. Obes Surg. 2020;30(10):3919–3929. doi:10.1007/s11695-020-04755-2
15. Ahsan MZ, Khan FU, Zhao MJ, et al. Synergistic interaction between butorphanol and dexmedetomidine in antinociception. Eur J Pharm Sci. 2020;149:105322. doi:10.1016/j.ejps.2020.105322
16. Jin Y, Xie G, Wang H, et al. Incidence and Risk Factors of Postoperative Pulmonary Complications in Noncardiac Chinese Patients: a Multicenter Observational Study in University Hospitals. BioMed Res Int. 2015;2015:265165. doi:10.1155/2015/265165
17. Wang Y, Wang H, Wang H, et al. Exploring the intraoperative lung protective ventilation of different positive end-expiratory pressure levels during abdominal laparoscopic surgery with Trendelenburg position. Ann Transl Med. 2019;7(8):171. doi:10.21037/atm.2019.03.45
18. Gupta S, Fernandes RJ, Rao JS, Dhanpal R. Perioperative risk factors for pulmonary complications after non-cardiac surgery. J Anaesthesiol Clin Pharmacol. 2020;36(1):88–93. doi:10.4103/joacp.JOACP_54_19
19. Jiang L, Wang J, Chen W, et al. Effect of clock rhythm on emergence agitation and early postoperative delirium in older adults undergoing thoracoscopic lung cancer surgery: protocol for a prospective, observational, cohort study. BMC Geriatr. 2023;24;1.
20. Reilly J, Shulman MA, Reilly J, et al. Measurement of quality of recovery after surgery using the 15-item quality of recovery scale: a systematic review and meta-analysis. BRIT J ANAESTH. 2022;128(6):1029–1039. doi:10.1016/j.bja.2022.03.009
21. Ding X, Cui H, Ma P, et al. Efficacy of dexmedetomidine versus midazolam when combined with butorphanol for sedation and analgesia during burn dressing changes: a randomized clinical trial. Front Pharmacol. 2022;13:965441. doi:10.3389/fphar.2022.965441
22. Ding X, Luo Y, Shi L, et al. Butorphanol in combination with dexmedetomidine provides efficient pain management in adult burn patients. Burns. 2021;47(7):1594–1601. doi:10.1016/j.burns.2020.12.025
23. Xu X, Tao Y, Yang Y, et al. Application of Butorphanol versus Sufentanil in Multimode Analgesia via Patient Controlled Intravenous Analgesia After Hepatobiliary Surgery: a Retrospective Cohort Study. Drug Des Dev Ther. 2023;17:3757–3766. doi:10.2147/DDDT.S433136
24. Wu L, Zhao H, Zhang Z, et al. Combined spinal-epidural anesthesia with acupoint injection for labor anesthesia reduces IL-1β/IL-10 ratio in maternal peripheral blood, umbilical cord blood and improves the labor outcomes: a prospective randomized controlled trial. Clin Immunol. 2022;236:108935. doi:10.1016/j.clim.2022.108935
25. Ohta Y, Miyamoto K, Kawazoe Y, et al. Effect of dexmedetomidine on inflammation in patients with sepsis requiring mechanical ventilation: a sub-analysis of a multicenter randomized clinical trial. Crit Care. 2020;24(1):493. doi:10.1186/s13054-020-03207-8
26. Jiang H, Kang Y, Ge C, et al. One-lung ventilation patients: clinical context of administration of different doses of dexmedetomidine. J Med Biochem. 2022;41(2):230–237. doi:10.5937/jomb0-33870
27. Zorrilla-Vaca A, Grant MC, Law M, et al. Dexmedetomidine improves pulmonary outcomes in thoracic surgery under one-lung ventilation: a meta-analysis. J Clin Anesth. 2024;93:111345. doi:10.1016/j.jclinane.2023.111345
28. Huang SQ, Zhang J, Zhang XX, et al. Can Dexmedetomidine Improve Arterial Oxygenation and Intrapulmonary Shunt during One-lung Ventilation in Adults Undergoing Thoracic Surgery? A Meta-analysis of Randomized, Placebo-controlled Trials. CMJ. 2017;130(14):1707–1714.
29. Wu Q, Wang HY, Li J, et al. κ-Opioid Receptor Stimulation Improves Endothelial Function in Hypoxic Pulmonary Hypertension. PLoS One. 2013;8(5):e60850. doi:10.1371/journal.pone.0060850
30. Xu G, Zhao J, Liu Z, et al. Dexmedetomidine Combined with Butorphanol or Sufentanil for the Prevention of Post-operative Nausea and Vomiting in Patients Undergoing Microvascular Decompression: a Randomized Controlled Trial. Front Med. 2020;7:583031. doi:10.3389/fmed.2020.583031
31. Xie F, Sun DF, Yang L, et al. Effect of anesthesia induction with butorphanol on postoperative nausea and vomiting: a randomized controlled trial. World J Clin Cases. 2023;11(32):7806–7813. doi:10.12998/wjcc.v11.i32.7806
32. Dinges HC, Otto S, Stay DK, et al. Side Effect Rates of Opioids in Equianalgesic Doses via Intravenous Patient-Controlled Analgesia: a Systematic Review and Network Meta-analysis. ANESTH ANALG. 2019;129(4):1153–1162. doi:10.1213/ANE.0000000000003887
33. Liu Y, Cai X, Fang R, et al. Future directions in ventilator-induced lung injury associated cognitive impairment: a new sight. Front Physiol. 2023;14:1308252. doi:10.3389/fphys.2023.1308252
34. Anggrahini DW, Emoto N, Nakayama K, et al. Vascular endothelial cell-derived endothelin-1 mediates vascular inflammation and neointima formation following blood flow cessation. Cardiovasc Res. 2009;82(1):143–151. doi:10.1093/cvr/cvp026
35. Zhong H, Lin H, Pang Q, et al. Macrophage ICAM-1 functions as a regulator of phagocytosis in LPS induced endotoxemia. INFLAMM RES. 2021;70(2):193–203. doi:10.1007/s00011-021-01437-2
36. Johnson MDL, Younis US, Menghani SV, et al. CC16 Binding to α4 β1 Integrin Protects against Mycoplasma pneumoniae Infection. Am J Resp Crit Care. 2021;203(11):1410–1418. doi:10.1164/rccm.202006-2576OC
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Perioperative Butorphanol for the Prevention of Postoperative Pulmonary Complications After Thoracoscopic Lung Resection: A Randomized, Double-Blind, Placebo-Controlled Trial
Wang X, Zhang Y, Wu Y, Yin T, Xia J, Zhao L, Zeng S, Wu K, Sun J, Liu S
Drug Design, Development and Therapy 2026, 20:621698
Published Date: 14 July 2026