Back to Journals » Local and Regional Anesthesia » Volume 18
Prospective Evaluation of the Effectiveness of Brachial Plexus Nerve Block During the Perioperative Period in Long-Term Opioid Users Undergoing Upper Extremity Surgery – A Case Series
Authors Huettner D, Qiu Y, Rosario BL ![]() , Orebaugh S
, Orebaugh S
Received 19 May 2025
Accepted for publication 9 October 2025
Published 15 October 2025 Volume 2025:18 Pages 111—119
DOI https://doi.org/10.2147/LRA.S541354
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Stefan Wirz
Daniel Huettner,1 Yue Qiu,1 Bedda L Rosario,2 Steven Orebaugh1
1Department of Anesthesiology and Perioperative Medicine, University of Pittsburgh Medical Center, Pittsburgh, PA, USA; 2Department of Epidemiology, University of Pittsburgh, Pittsburgh, PA, USA
Correspondence: Steven Orebaugh, Department of Anesthesiology and Perioperative Medicine, University of Pittsburgh Medical Center, Pittsburgh, PA, USA, Email [email protected]
Purpose: This study examined whether chronic opioid use reduces the effectiveness of brachial plexus block in patients undergoing upper extremity surgery.
Patients and Methods: Patients undergoing surgery with brachial plexus blocks were divided into two groups: opioid-dependent (daily opioid use for ≥ 1 month) and control (no opioid use for ≥ 3 months). Pain scores and opioid use were recorded over 72 hours postoperatively.
Results: Forty-six patients were included (23 opioid-dependent and 23 control). The median (IQR) NRS scores upon PACU arrival were 0 (0– 0) in the control group and 0 (0– 5) in the opioid group (p=0.0101). The duration of the nerve block was shorter in opioid-dependent patients (14 versus 22 hours; p=0.0035).
Conclusion: Chronic opioid users experienced shorter brachial plexus block duration and more postoperative pain after being discharged home.
Keywords: anesthesia, opiates, recovery, chronic pain
Introduction
Many patients with orthopedic pathology experience significant pain and may require long-term oral opioids as part of their pain management.1 Recent studies suggest that 6–8% of patients who undergo surgery may develop opioid dependence, although there is evidence that efforts to mitigate this issue are achieving some success.2 Opioid use and abuse remain relatively common in the United States.3,4 Consequently, regional anesthesia providers are likely to encounter patients on long-term opioid therapy with increasing frequency.
The impact of chronic opioid therapy on nerve blockade remains unclear but is clinically relevant. Opioids have the potential to alter pain perception and structurally modify pain pathways.5 Animal studies suggest that long-term opioid exposure reduces the effectiveness of local anesthetics in peripheral nerve blockade.6 Clinical studies, though limited, have reported that chronic opioid use may result in lower sensory levels and reduced duration of block in spinal anesthesia,7–10 as well as decreased effectiveness of field blocks for minor surgical procedures.9,11
To better understand the effects of chronic opioid therapy on peripheral nerve blockade for postoperative analgesia, we conducted a prospective study comparing patients maintained on opioids who underwent upper extremity ambulatory surgery with those who underwent similar surgeries without such exposure. We hypothesized that patients receiving daily opioids for more than one month would have less effective brachial plexus blocks, demonstrated by significantly higher numeric rating scale (NRS) scores upon arrival in the post-anesthesia care unit (PACU). Our primary outcome was the initial NRS score related to surgical site pain recorded on arrival in PACU. Secondary outcomes included block failure rates, block duration, postoperative opioid requirements, and pain scores over three postoperative days.
Material and Methods
Study Design and Patients
This prospective, observational, single-center study was approved by the Institutional Review Board of the University of Pittsburgh (Approval number: STUDY19010112) and was conducted in accordance with the Declaration of Helsinki. All patients provided written informed consent prior to participation.
Adult patients with chronic opioid use undergoing upper extremity surgery were included. The inclusion criteria were age ≥18 years, American Society of Anesthesiologists physical status scores of 1–3, and having undergone elective interscalene or supraclavicular nerve block for upper extremity surgery. The exclusion criteria were as follows: (1) cognitive impairment that impaired autonomy and the ability to provide informed consent; (2) medical conditions for which an interscalene block (ISB) or supraclavicular block (SCB) was contraindicated (for example, pre-existing upper extremity neuropathy or nerve damage to the brachial plexus, ongoing systemic or local infection, recent use of anticoagulation); (3) limb or neck abnormalities, such as amputation, radiation therapy, or infection at the proposed implant site; (4) past or current illicit substance use; (5) intermittent use of opioids (rather than daily); (6) complex regional pain syndrome; and (7) patient refusal. Patients who received daily opioids for more than 1 month preoperatively were assigned to the opioid group, while those who did not receive preoperative opioids for 3 months preoperatively were assigned to the control group.
Block Procedure
Nerve blocks were provided by staff anesthesiologists or supervised residents of the University of Pittsburgh Department of Anesthesiology. Interscalene blocks (ISB) or supraclavicular blocks (SCB) with 0.5% ropivacaine or 0.5% bupivacaine, respectively, were administered based on the upper extremity surgery performed. No adjuvants or vasoconstrictors were added. Block success was determined by evaluating motor and distal sensory functions. A high-frequency (15–6 MHz) linear probe of Sonosite X-Porte ultrasound scanner (Sonosite, Bothell, WA, USA) was used for each block. The head was tilted 45° to the non-operative side while the patient was in a semi-recumbent position at an angle of 30–45 degrees. Oxygen saturation was routinely monitored. Midazolam (1–2 mg) and fentanyl (25–50 mcg) were used as sedatives to manage anxiety as clinically needed. The needle insertion site was sterilized using 70% isopropyl alcohol and 2% chlorhexidine solution.
Interscalene Block
Before performing ISB, the transducer was positioned above the supraclavicular region to provide a short-axis view of the brachial plexus and subclavian artery. The plexus was traced proximally, and the C5, C6, and C7 roots were identified, as described previously.12 A 22-gauge 8-mm insulated block needle (SonoPlex; Pajunk GmbH, Geisingen, Germany) was placed in-plane with the ultrasonic beam on the lateral side of the transducer after local injection of 1–3 mL of 2% lidocaine. Under ultrasound guidance, the needle was gently advanced through the middle scalene muscle toward the lateral boundary of the brachial plexus sheath. The needle tip was moved forward to rest between C5 and C6. After negative aspiration, incremental injections of 12–15 mL of 0.5% bupivacaine or 0.5% ropivacaine were administered to facilitate spread to the brachial plexus roots.
Supraclavicular Block
Before completing SCB, the transducer was placed in the supraclavicular fossa to provide a short-axis image of the brachial plexus and subclavian artery directly above the first rib. After injection with 1–3 mL of 2% lidocaine, a 22-gauge 8-mm block needle (SonoPlex; Pajunk GmbH, Geisingen, Germany) was advanced under direct visualization using an in-plane approach. The brachial plexus appeared as a compact, hyperechoic cluster of nerves with an oval or circular shape situated superior to the first rib and lateral and superficial to the pulsing subclavian artery. After negative aspiration, incremental injections of 20–24 mL of 0.5% bupivacaine or 0.5% ropivacaine were administered to facilitate spread to the brachial plexus trunk. Three locations were targeted for the small incremental injections of anesthetic: (1) the “corner pocket” (ie, the space where the inferior trunk rested on the first rib), (2) between the middle trunk and the usually distinct superior trunk, and (3) between the inferior and middle trunk.13,14
Follow-up
Upon discharge from the recovery unit, the patients completed a pain diary recording pain scores and opioid use over the following 72 hours. Furthermore, the patients were contacted via telephone on postoperative day 2, as part of the standard of care, for follow-up on the discomfort, pain scores, and efficacy of the regional nerve block. Block duration was defined as the interval from completion of local anesthetic injection to the first patient-reported return of surgical-limb pain or request for rescue analgesia, whichever occurred first. We assessed this in PACU and via standardized follow-ups at POD2 by trained staff using a scripted questionnaire.
Outcome Measures
The primary outcome was a PACU NRS score on arrival. We hypothesized that this score would be more than two units higher in chronic opioid patients than in those not opioid dependents. Secondary outcomes included opioid requirement in the operating room, block duration, postoperative opioid requirement, and pain scores for three postoperative days.
Statistical Analyses
Descriptive statistics for baseline characteristics are summarized by group (control vs opioid-dependent) as counts (percentages) for categorical data or as medians (interquartile ranges [IQR]) for non-normally distributed continuous data. The normal distribution assumption for continuous data was examined using q-q plots and histograms. The Wilcoxon rank-sum test was used to examine between-group differences in non-normally distributed data. The chi-square test (or Fisher’s exact test) was used to compare the frequency distribution of categorical measures between the groups. The Wilcoxon rank-sum test was used to assess between-group differences in the primary (numerical rating scale [NRS] scores on PACU arrival) and secondary (eg, block duration and PACU length of stay) outcomes. To account for multiple hypotheses testing for two group comparison tests (ie, several secondary outcomes), Bonferroni adjusted p-values were also reported. For the secondary outcomes of postoperative pain NRS scores and morphine milligram equivalents (MMEs), linear mixed models were used to test the main effects of group (control vs opioid dependent), time (postoperative days 1, 2, and 3), and group-by-time interactions. For these models, a natural logarithmic transformation was used for the MMEs. For the linear mixed models, Tukey-Kramer adjusted p-values were reported for pairwise comparisons. All statistical analyses were performed using SAS, version 9.4 statistical software (SAS Institute Inc., Cary, NC, USA).
Results
A total of 46 patients were enrolled in the study, with 23 in the long-term opioid group and 23 in the control group. Patient characteristics are summarized in Table 1. Preoperative opioid exposure (type, indication) and individual MMEs values are provided in Table S1. The median (IQR) NRS scores upon PACU arrival were 0 (0–0) in the control group and 0 (0–5) in the opioid group (p=0.0101). Significant differences were observed in block duration between the groups (median block duration: 22 hours for the control group versus 14 hours for the opioid group, p=0.0035, adjusted p=0.2245 with Bonferroni correction). No significant differences were found in PACU morphine milligram equivalents (MMEs), PACU length of stay, or intraoperative opioid/dexmedetomidine/ketamine use (Table 2). Statistically significant differences in mean NRS scores were found between groups (p=0.0070) and across postoperative days (p=0.0021) (Figure 1). Statistically significant differences in mean logarithm postoperative MMEs were found between the groups (p=0.0018) (Figure 2). No complications were reported.
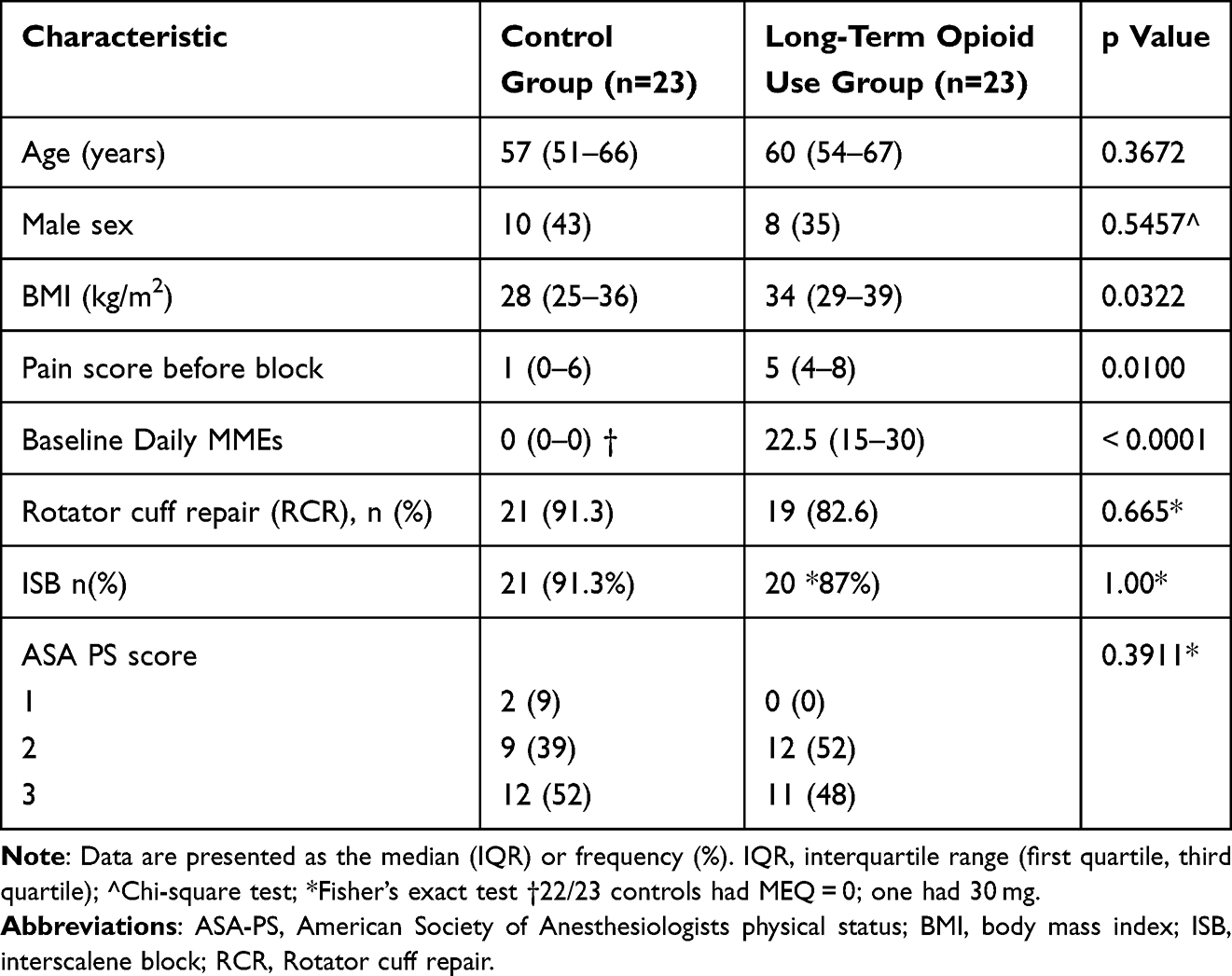 |
Table 1 Comparison of Patient Characteristics |
 |
Table 2 Descriptive Statistics for Secondary Outcomes |
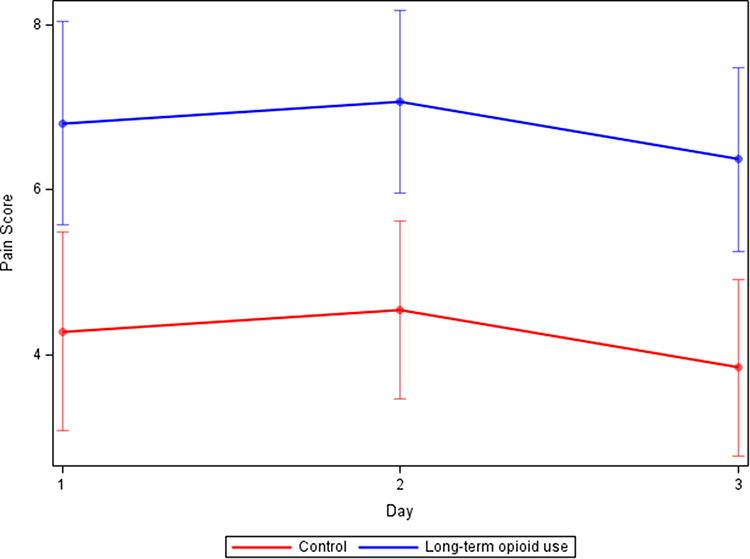 |
Figure 1 Estimated NRS scores. Values are the expected means from the linear mixed model analysis for the control group (red line) and opioid-dependent group (blue line). Error bars indicate 95% confidence intervals. The linear mixed model shows a significant main effect of time (F(2,29)=5.91, p=0.0070) and group (F(1, 29)=11.42, p=0.0021). Further, the NRS scores increase on day 2 and then decrease on day 3 for both groups, with significant differences between days 2 and 3 (Tukey-Kramer adjusted p=0.0264). |
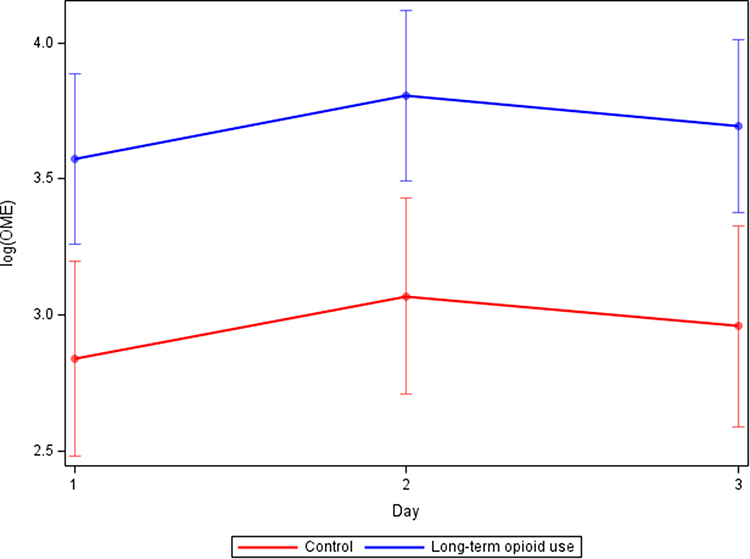 |
Figure 2 Estimated postoperative opioid requirements are shown as expected means from the linear mixed model analysis for the control group (red line) and Long-term opioid use group (blue line). Error bars indicate 95% confidence intervals. The linear mixed model showed statistically significant main effect of group (F(1, 27)=12.02, p=0.0018). |
Discussion
Patients with chronic opioid use exhibited shorter block durations than patients without chronic opioid exposure. Postoperatively, they also experienced greater pain than the general population. To the best of our knowledge, this study represents the first to compare the effectiveness of brachial plexus nerve block in long-term opioid use patients and non-opioid-use patients undergoing upper extremity surgery. In this study, we found no difference in median NRS pain scores in PACU, attesting to the effectiveness of nerve blocks. While the median pain score on arrival in PACU was 0 for each group, statistically significant differences were observed in distribution of scores, with higher scores in the chronic opioid group. Our plan to compare mean scores could not be carried out due to non-normally distributed data, likely suggesting that there is no clinical difference in the primary outcome, or warrant further larger scale study.
The secondary endpoints revealed that the average block duration was clinically significantly shorter in opioid-dependent patients. However, PACU MMEs, PACU length of stay, and intraoperative analgesic medication use did not differ significantly, likely because the nerve block was still in effect during this early period. Statistically significant differences in mean NRS scores and mean MMEs were found between groups postoperatively. This suggests that patients chronically exposed to opioids were likely in more pain. However, the opioid group experienced more pain preoperatively (NRS 5 vs 1, p=0.01), and there was a wide range of baseline opioid dosing within and between the two groups. These differences in postoperative NRS and MME are likely a reflection of their baseline status as higher preoperative pain levels are expected to lead to high postoperative pain levels and opioid use. Although higher postoperative pain in long-term opioid use patients is expected, prior work has not characterized early analgesia while the block is at peak effect or the functional duration of block in this population. By quantifying PACU pain and functional block duration, our case series provides practice-relevant data to guide perioperative multimodal strategies.
Managing patients exposed to long-term opioids poses a complex challenge for anesthesiologists. The prevalence of this patient population is on the rise. Anesthesiologists, surgeons, and other healthcare professionals in perioperative care are likely to increasingly encounter opioid users requiring surgical procedures and effective pain management during their clinical practice.15 These patients are highly susceptible to experiencing intense postoperative pain. The limited implementation of guidelines in practical clinical settings could be a contributing factor to the elevated occurrence of poorly managed postoperative pain.16 In the present day, there is a scarcity of evidence regarding the perioperative management of individuals who use opioids. Consequently, much of the available information is derived more from expert opinions than from the clinical trials field.15
Opiates are effective analgesics; however, prolonged exposure to opioids has been associated with the development of opioid-induced hyperalgesia (OIH).17 The primary mechanism of the change in regional anesthesia effectiveness is still unclear. Extensive research has identified multiple molecular pathways and receptors that could potentially be linked to OIH. The cellular and molecular mechanisms responsible for OIH encompass genetic variations, mu opioid receptor (MOR) variants, factors related to neurons and glia, long-term potentiation, heightened neuronal sensitivity, and neuroinflammatory processes. For instance, the periaqueductal gray (PAG) has been identified to house Toll-like receptor4 (TLR4) and glutamate receptors that play a crucial role in the onset and persistence of OIH.18 Activation of MORs has also been shown to crosstalk with L-type voltage-gated Ca2+ channels,19 TRP channels—especially TRPV1.20 K+ channels,21 and Na channels.22,23 This crosstalk may contribute to the desensitization of the nervous system to local analgesics, or by itself lead to the underlying antinociceptive tolerance. Sustained opioid administration may lead to the plasticity of the receptors and neuroadaptive changes in the nervous system.24,25 These alterations in the nervous system may impact the effectiveness of peripheral nerve blocks, as evidenced by patients’ symptoms, block failure or insufficiency, increase opioid requirements in the presence of nerve block, and shorten block duration.
Several factors have been suggested as contributors to the variability in postoperative pain among patients. Genetic variations, including single nucleotide polymorphisms in mu, kappa, and delta opioid receptors, ion channel genes, cytotoxic T-cells, glutamate receptors, and cytokine genes, have been shown to influence postoperative pain management.26 Long-term opioid exposure has been associated with a poorer response to analgesics postoperatively.27 Additionally, numerous studies have explored the potential influence of chronic opioid exposure on DNA methylation, which alters the patient’s epigenome and may affect pain scores.28,29
Based on our results regarding the efficacy of nerve blocks in long-term opioid use patients, anesthesiologists may consider using nerve blocks that are both safe and of longer duration for this patient population, with the goal of facilitating a more comfortable postoperative recovery. Continuous peripheral nerve block (CPNB) may be preferred, as it can help compensate for reduced block duration and increased postoperative pain levels, as well as reduce opioid requirements. Since its initial report in 1946, a substantial body of data has been accumulated on CPNB30 For ambulatory patients undergoing shoulder surgery, acute postoperative pain can be effectively and consistently managed with a continuous ISB.31 Continuous ISB after shoulder surgery in an ambulatory setting has also been found to be reliable and safe, significantly decreasing postoperative opioid use.32,33 Alternatively, long-acting local anesthetics could be considered for these patients. Liposomal bupivacaine was initially deemed superior in terms of clinical effectiveness;34 however, recent research suggests its clinical advantages may not be significant.35,36 Analgesic adjuvants, such as opioids, α2-agonists, NMDA receptor antagonists, and other agents, are being explored to enhance and extend anesthetic and analgesic effects.37 As our understanding of nociceptive processes in the PNS grows, innovative techniques for advancing pain management are expected to emerge.
Limitations
This study had several limitations. We hypothesized that “it would be >2 units higher in chronic opioid patients than in non-opioid-dependent patients.” However, because of the limited sample size and non-normally distributed PACU VAS scores on arrival, we were not able to analyze the difference in means. As the median PACU pain scores on arrival demonstrated a significant difference but were zero in both groups due to the limitation of sample size, future larger studies are warranted. In this study, both ropivacaine and bupivacaine were used to provide the brachial plexus blocks, though both of these agents have similar, prolonged durations of effect. Additionally, pain measurement is inherently subjective, whether assessed by nurses in PACU or reported by patients at home. The home pain diary relies on patient compliance, and as anticipated, several patients were lost to follow-up. We also acknowledge the limitation that no prior study is available for us as a reference to calculate a sample size, we refer to this as a convenience sample for a pilot study. Although we adjusted for block technique, the study included both interscalene and supraclavicular approaches with very small supraclavicular sample sizes, so residual confounding by technique cannot be excluded. Although block technique distribution was similar between groups (ISB 21/23 [91.3%] vs 20/23 [87.0%]), the very small SCB counts (2 vs 3) prevented meaningful stratified analyses. Finally, this study is a small, single-center prospective observational case series (n = 46), which limits precision and precludes robust multivariable adjustment. Baseline differences (notably BMI and preoperative pain burden and perioperative management of home opioids) may have confounded observed associations.
Conclusion
Patients with chronic opioid exposure, defined as daily opioid use for ≥1 month preoperatively, reported significantly shorter block duration. After the nerve blocks wore off, patients with chronic opioid use experienced substantially greater pain and required higher doses of opioids. These findings underscore the need for longer-lasting regional anesthetic interventions in this patient population.
Data Sharing Statement
The authors confirm that data supporting the findings of this study are included within the article.
Ethics Approval and Informed Consent
This prospective, observational, single-center study was approved by the Institutional Review Board of the University of Pittsburgh Approval number: STUDY19010112) and was conducted according to the tenets of the Declaration of Helsinki. All patients provided written informed consent prior to participation.
Consent for Publication
Details of any images, videos, and recordings can be published, and the individuals who provided consent have reviewed the article’s content prior to publication.
Acknowledgments
This study was performed during YQ’s resident research rotation at UPMC, under the instruction of Dr. Sakai, Tetsuro.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Howard R, Waljee J, Brummett C, Englesbe M, Lee J. Reduction in opioid prescribing through evidence-based prescribing guidelines. JAMA Surg. 2018;153(3):285–287. doi:10.1001/jamasurg.2017.4436
2. Votta-Velis G, Daviglus ML, Borgeat A, et al. Surgical opioid-avoidance protocol: a postoperative pharmacological multimodal analgesic intervention in diverse patient populations. Reg Anesth Pain Med. 2023;48(12):594–600. doi:10.1136/rapm-2022-103864
3. Keyes KM, Rutherford C, Hamilton A, et al. What is the prevalence of and trend in opioid use disorder in the United States from 2010 to 2019? Using multiplier approaches to estimate prevalence for an unknown population size. Drug Alcohol Depend Rep. 2022;3:100052. doi:10.1016/j.dadr.2022.100052
4. Manchikanti L, Sanapati J, Benyamin RM, Atluri S, Kaye AD, Hirsch JA. Reframing the prevention strategies of the opioid crisis: focusing on prescription opioids, fentanyl, and heroin epidemic. Pain Phys. 2018;21(4):309–326.
5. Sheng WS, Hu S, Gekker G, Zhu S, Peterson PK, Chao CC. Immunomodulatory role of opioids in the central nervous system. Arch Immunol Ther Exp. 1997;45(5–6):359–366.
6. Liu Q, Gold MS. Opioid-induced loss of local anesthetic potency in the rat sciatic nerve. Anesthesiology. 2016;125(4):755–764. doi:10.1097/ALN.0000000000001239
7. Vosoughian M, Dabbagh A, Rajaei S, Maftuh H. The duration of spinal anesthesia with 5% lidocaine in chronic opium abusers compared with nonabusers. Anesth Analg. 2007;105(2):531–533. doi:10.1213/01.ane.0000268496.46141.4f
8. Karbasy SH, Derakhshan P. Effects of opium addiction on level of sensory block in spinal anesthesia with bupivacaine for lower abdomen and limb surgery: a case-control study. Anesth Pain Med. 2014;4(5):e21571. doi:10.5812/aapm.21571
9. Hashemian AM, Omraninava A, Kakhki AD, et al. Effectiveness of local anesthesia with lidocaine in chronic opium abusers. J Emerg Trauma Shock. 2014;7(4):301–304. doi:10.4103/0974-2700.142765
10. Dabbagh A, Dahi-Taleghani M, Elyasi H, et al. Duration of spinal anesthesia with bupivacaine in chronic opium abusers undergoing lower extremity orthopedic surgery. Arch Iran Med. 2007;10(3):316–320.
11. Thapa D, Ahuja V, Kosaraju CC, Gill K, Meena A. Incomplete supraclavicular brachial plexus block in an opioid-dependent patient: a case report. J Anaesthesiol Clin Pharmacol. 2022;38(3):487–488. doi:10.4103/joacp.JOACP_212_20
12. Franco CD, Williams JM. Ultrasound-guided interscalene block: reevaluation of the “stoplight” sign and clinical implications. Reg Anesth Pain Med. 2016;41(4):452–459. doi:10.1097/AAP.0000000000000407
13. Hanumanthaiah D, Vaidiyanathan S, Garstka M, Szucs S, Iohom G. Ultrasound guided supraclavicular block. Med Ultrason. 2013;15(3):224–229. doi:10.11152/mu.2013.2066.153.dh1mg2
14. Siddiqui U, Perlas A, Chin K, et al. Intertruncal approach to the supraclavicular brachial plexus, current controversies and technical update: a daring discourse. Reg Anesth Pain Med. 2020;45(5):377–380. doi:10.1136/rapm-2019-101260
15. Coluzzi F, Bifulco F, Cuomo A, et al. The challenge of perioperative pain management in opioid-tolerant patients. Ther Clin Risk Manag. 2017;13:1163–1173. doi:10.2147/TCRM.S141332
16. Alford DP, Compton P, Samet JH. Acute pain management for patients receiving maintenance methadone or buprenorphine therapy. Ann Intern Med. 2006;144(2):127–134. doi:10.7326/0003-4819-144-2-200601170-00010
17. Roeckel L-A, Le Coz G-M, Gavériaux-Ruff C, Simonin F. Opioid-induced hyperalgesia: cellular and molecular mechanisms. Neuroscience. 2016;338:160–182. doi:10.1016/j.neuroscience.2016.06.029
18. Mo J, Lu Z, Peng J, et al. PAG neuronal NMDARs activation mediated morphine-induced hyperalgesia by HMGB1-TLR4 dependent microglial inflammation. J Psychiatr Res. 2023;164:150–161. doi:10.1016/j.jpsychires.2023.05.082
19. Heinke B, Gingl E, Sandkühler J. Multiple targets of μ-opioid receptor-mediated presynaptic inhibition at primary afferent Aδ- and C-fibers. J Neurosci. 2011;31(4):1313–1322. doi:10.1523/JNEUROSCI.4060-10.2011
20. Bao Y, Gao Y, Yang L, et al. The mechanism of μ-opioid receptor (MOR)-TRPV1 crosstalk in TRPV1 activation involves morphine anti-nociception, tolerance and dependence. Channels (Austin). 2015;9(5):235–243. doi:10.1080/19336950.2015.1069450
21. Marker CL, Luján R, Loh HH, Wickman K. Spinal G-protein-gated potassium channels contribute in a dose-dependent manner to the analgesic effect of mu- and delta- but not kappa-opioids. J Neurosci. 2005;25(14):3551–3559. doi:10.1523/JNEUROSCI.4899-04.2005
22. Minett MS, Pereira V, Sikandar S, et al. Endogenous opioids contribute to insensitivity to pain in humans and mice lacking sodium channel Nav1.7. Nat Commun. 2015;6:8967. doi:10.1038/ncomms9967
23. Chattopadhyay M, Mata M, Fink DJ. Continuous delta-opioid receptor activation reduces neuronal voltage-gated sodium channel (NaV1.7) levels through activation of protein kinase C in painful diabetic neuropathy. J Neurosci. 2008;28(26):6652–6658. doi:10.1523/JNEUROSCI.5530-07.2008
24. Gardell LR, King T, Ossipov MH, et al. Opioid receptor-mediated hyperalgesia and antinociceptive tolerance induced by sustained opiate delivery. Neurosci Lett. 2006;396(1):44–49. doi:10.1016/j.neulet.2005.11.009
25. Thompson BL, Oscar-Berman M, Kaplan GB. Opioid-induced structural and functional plasticity of medium-spiny neurons in the nucleus accumbens. Neurosci Biobehav Rev. 2021;120:417–430. doi:10.1016/j.neubiorev.2020.10.015
26. Ren Z-Y, Xu X-Q, Bao Y-P, et al. The impact of genetic variation on sensitivity to opioid analgesics in patients with postoperative pain: a systematic review and meta-analysis. Pain Phys. 2015;18(2):131–152.
27. Elmallah RK, Ramkumar PN, Khlopas A, et al. Postoperative pain and analgesia: is there a genetic basis to the opioid crisis? Surg Technol Int. 2018;32:306–314.
28. Doehring A, Oertel BG, Sittl R, Lötsch J. Chronic opioid use is associated with increased DNA methylation correlating with increased clinical pain. Pain. 2013;154(1):15–23. doi:10.1016/j.pain.2012.06.011
29. Gerra MC, Dallabona C, Arendt-Nielsen L. Epigenetic alterations in prescription opioid misuse: new strategies for precision pain management. Genes. 2021;12(8):1226. doi:10.3390/genes12081226
30. Ilfeld BM. Continuous peripheral nerve blocks: an update of the published evidence and comparison with novel, alternative analgesic modalities. Anesth Analg. 2017;124(1):308–335. doi:10.1213/ANE.0000000000001581
31. Boezaart AP. Continuous interscalene block for ambulatory shoulder surgery. Best Pract Res Clin Anaesthesiol. 2002;16(2):295–310. doi:10.1053/bean.2002.0239
32. Fredrickson MJ, Ball CM, Dalgleish AJ. Successful continuous interscalene analgesia for ambulatory shoulder surgery in a private practice setting. Reg Anesth Pain Med. 2008;33(2):122–128. doi:10.1016/j.rapm.2007.09.007
33. Fredrickson MJ, Ball CM, Dalgleish AJ. Analgesic effectiveness of a continuous versus single-injection interscalene block for minor arthroscopic shoulder surgery. Reg Anesth Pain Med. 2010;35(1):28–33. doi:10.1097/AAP.0b013e3181c771bd
34. Bergese SD, Ramamoorthy S, Patou G, Bramlett K, Gorfine SR, Candiotti KA. Efficacy profile of liposome bupivacaine, a novel formulation of bupivacaine for postsurgical analgesia. J Pain Res. 2012;5:107–116. doi:10.2147/JPR.S30861
35. Hussain N, Brull R, Sheehy B, et al. Perineural liposomal bupivacaine is not superior to nonliposomal bupivacaine for peripheral nerve block analgesia. Anesthesiology. 2021;134(2):147–164. doi:10.1097/ALN.0000000000003651
36. Sandhu HK, Miller III CC, Tanaka A, Estrera AL, Charlton-Ouw KM. Effectiveness of standard local anesthetic bupivacaine and liposomal bupivacaine for postoperative pain control in patients undergoing truncal incisions: a randomized clinical trial. JAMA Netw Open. 2021;4(3):e210753. doi:10.1001/jamanetworkopen.2021.0753
37. Jeon YH. The use of adjuvants to local anesthetics: benefit and risk. Korean J Pain. 2018;31(4):233–234. doi:10.3344/kjp.2018.31.4.233
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effects of Esketamine Combined with Ultrasound-Guided Pectoral Nerve Block Type II on the Quality of Early Postoperative Recovery in Patients Undergoing a Modified Radical Mastectomy for Breast Cancer: A Randomized Controlled Trial
Yu L, Zhou Q, Li W, Zhang Q, Cui X, Chang Y, Wang Q
Journal of Pain Research 2022, 15:3157-3169
Published Date: 11 October 2022