Back to Journals » Therapeutics and Clinical Risk Management » Volume 22
Prospective Evaluation of Postoperative SIRS and Serum Inflammatory Indices in Percutaneous Nephrolithotomy Patients
Authors Arslantas YB, Sonmez G ![]() , Baydilli N, Bas U
, Baydilli N, Bas U ![]() , Tosun H
, Tosun H ![]() , Demirci D, Akinsal EC
, Demirci D, Akinsal EC
Received 18 September 2025
Accepted for publication 25 December 2025
Published 15 January 2026 Volume 2026:22 568497
DOI https://doi.org/10.2147/TCRM.S568497
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Yusuf Bugra Arslantas,1 Gokhan Sonmez,2 Numan Baydilli,2 Unsal Bas,3 Halil Tosun,2 Deniz Demirci,2 Emre Can Akinsal2
1Urology Clinic, Viransehir State Hospital, Sanliurfa, Türkiye; 2Department of Urology, Erciyes University Faculty of Medicine, Kayseri, Türkiye; 3Urology Clinic, Ekrem Karakaya State Hospital, Develi, Kayseri, Türkiye
Correspondence: Unsal Bas, Develi Ekrem Karakaya State Hospital, Urology Clinic, Kayseri, Türkiye, Tel +90 545 665 97 05, Email [email protected]
Introduction: This study aimed to evaluate the relationship between postoperative systemic inflammatory response syndrome (SIRS) and a broad set of 30 commonly used clinical parameters, along with novel acute inflammation predictive indices such as the systemic immune-inflammation index (SII), the aggregate index of systemic inflammation (AISI), and the systemic inflammation response index (SIRI), in patients undergoing percutaneous nephrolithotomy (PCNL).
Methods: A total of 233 patients aged 18– 75 years who underwent PCNL were prospectively included. All clinical variables and serum-based inflammatory indices, including SII, SIRI, and AISI, were prospectively pre-defined in the study protocol prior to patient enrollment. All patients had sterile preoperative urine cultures and no known disease that could cause fever. Clinical characteristics, operative findings, laboratory parameters, and serum-based inflammatory indices (SII, SIRI, AISI) were recorded. The median preoperative stone size was 270.0 mm2 (IQR: 180.0– 447.0). Stone-free rates and postoperative SIRS development were assessed. Multivariate logistic regression analysis was used to determine independent predictors of SIRS. ROC analyses were conducted to evaluate the predictive performance of inflammatory indices.
Results: The clinically significant stone-free rate was 89.3% (208/233), while the complete stone-free rate was 79.1% (182/233). Postoperative SIRS occurred in 75 patients (32.1%). According to multivariate logistic regression analysis, operation position, residual stone, white blood cell count (103/μL), serum hemoglobin drop (g/dl), amount of physiological serum used (L), and positive renal pelvis urine culture were independently associated with SIRS. Inflammatory indices calculated from serum values, including SII, SIRI, and AISI, were directly associated with SIRS. ROC analysis demonstrated a moderate correlation between these indices and SIRS.
Discussion: The findings of this prospective study indicate that postoperative SIRS risk can be predicted preoperatively and intraoperatively using a combination of commonly utilized clinical parameters and serum-based inflammatory indices. Higher values of SII, SIRI, and AISI were moderately predictive of SIRS development. Identifying high-risk patients prior to or during PCNL may help clinicians implement early preventive strategies and optimize postoperative management.
Keywords: percutaneous nephrolithotomy, postoperative infection, postoperative fever, kidney stone
Introduction
One of the most effective surgical treatments for kidney stones is percutaneous nephrolithotomy (PCNL).1 First performed by Fernström and Johansson in 1976, this procedure is commonly used for stones larger than 2 cm and/or located in the lower calyx.2
Although serious complications can occasionally occur after PCNL, one of the most common complications is infectious complications.3,4 The most frequent of these include postoperative urinary tract infections, fever, systemic inflammatory response syndrome (SIRS), and sepsis, which can have a highly fatal course.5,6
Despite confirming the absence of urinary tract infections preoperatively through urine culture and administering the most up-to-date antibiotic prophylaxis to minimize these infectious complications, surgeons occasionally encounter these significant conditions in some patients during the postoperative period.7
In order to predict the occurrence of SIRS and similar inflammatory processes, certain indices and calculations are utilized. Among these, the most popular indices today include the Systemic Immune-Inflammation Index (SII), the Aggregate Index of Systemic Inflammation (AISI), and the Systemic Inflammation Response Index (SIRI), which are calculated using platelet, neutrophil, monocyte, and lymphocyte counts.8
Postoperative SIRS after PCNL has been extensively studied in the literature. However, existing studies have mostly focused on surgical time, residual stones, urine culture, comorbidities, or classical hematologic markers. However, the predictive value of newer serum-based inflammatory indices such as SII, SIRI, and AISI in SIRS after PCNL has been limitedly investigated.
This study aims to evaluate the relationship between postoperative SIRS and 30 different clinical parameters commonly used in daily clinical practice, as well as novel acute inflammation predictive indices such as SII, AISI, and SIRI in patients undergoing PCNL.
Materials and Methods
Study Design and Patient Selection
This prospective single-center cross-sectional study included patients aged 18 to 75 years who underwent percutaneous nephrolithotomy (PCNL) for kidney stones at the Urology Clinic of Erciyes University between December 2022 and July 2024. All clinical and laboratory variables, including inflammatory indices, were pre-defined in the study protocol prior to patient enrollment.
Patients with active urinary tract infections confirmed by urine culture, immunodeficiency, bleeding diathesis, or infections originating from other organ systems in the perioperative period were excluded. Individuals with additional diseases that could cause fever (eg, malignancies, familial Mediterranean fever), those with indwelling urinary catheters, and patients who presented with fever or SIRS due to other postoperative causes (such as atelectasis or intra-abdominal/perirenal hematoma) were also excluded. Furthermore, patients with obstructing contralateral stones and those undergoing simultaneous combined procedures (eg, ureterorenoscopy + PCNL) were not included.
Preoperative Evaluation and Antibiotic Prophylaxis
In this study, preoperative evaluation of urinary system stones was performed using non-contrast computed tomography (CT), and postoperative assessments for residual stones or stone-free status were also conducted with CT. Urine culture samples were obtained from all included patients via spontaneous voiding within a maximum of seven days before surgery.
Patients with negative urine cultures received standard antibiotic prophylaxis, consisting of 1 g of ceftriaxone administered 30 minutes before surgery. For patients with positive urine cultures, antibiotic treatment was given based on antibiogram results, and a follow-up urine culture was performed. Surgery was only performed after obtaining a sterile urine culture.
Percutaneous Nephrolithotomy (PCNL) Procedure
All procedures were performed under general anesthesia in either the supine or prone position based on stone location. Fluoroscopy-guided access was achieved using contrast administered through a preoperatively placed ureteral catheter, followed by insertion of a guidewire and tract dilation.
Depending on stone size and location, either mini-PCNL (12–20 Fr sheath) or standard PCNL (30 Fr dilation) was performed. A 14 Fr Malecot catheter was placed at the end of the procedure. Patients whose nephrostomy output remained clear for 48–72 hours had their tubes removed and were subsequently discharged.
Lithotripsy was performed using a standardized Holmium: YAG laser (Quanta Systems, Cyber-Ho, 150 watt, Milan, Italy). Laser settings were adjusted based on stone characteristics using one of the following options: (i) 2 J × 10 Hz = 20 W, (ii) 1 J × 20 Hz = 20 W, (iii) 1.5 J × 12 Hz = 18 W, (iv) 3 J × 7 Hz = 21 W.
Residual fragments >2 mm were extracted using baskets, stone forceps, or the water-cleaning effect; smaller fragments were left for spontaneous passage. Urethral catheters placed during surgery were removed at 12 hours postoperatively.
Inflammatory Indices
The following composite inflammatory indices were calculated from preoperative serum values:
- Systemic Immune-Inflammation Index (SII): (Platelets × Neutrophils)/Lymphocytes
- Systemic Inflammation Response Index (SIRI): (Neutrophils × Monocytes)/Lymphocytes
- Aggregate Index of Systemic Inflammation (AISI): (Platelets × Neutrophils × Monocytes)/Lymphocytes
Data Collection and Parameter Definitions
The relationship between postoperative SIRS was investigated using a total of 33 parameters from the included patients. These parameters included age, gender, body mass index (BMI), diabetes, history of urinary tract infection (UTI) within the past six months, history of previous urinary stone surgery, history of extracorporeal shock wave lithotripsy (ESWL), presence of diabetes mellitus, presence of a perioperative double-J stent or nephrostomy, presence of hydronephrosis, and preoperative serum values (preoperative white blood cell [WBC] and C-reactive protein [CRP] levels, perioperative hemoglobin decrease, SII, SIRI, and AISI).
Additionally, stone size (mm3), stone location, operative side, surgical position (supine or prone), operative time (from percutaneous access needle insertion to Malecot tube placement), presence of residual stones, fluoroscopy duration (minutes), amount of irrigation fluid (normal saline, mL) used perioperatively, number of access points, access sheath size (Fr), perioperative and postoperative blood transfusion volume (mL), and sterile perioperative urine and stone cultures were analyzed. Furthermore, stone metabolic analysis results were evaluated.
Perioperative and Postoperative Evaluations
Serum biochemistry levels and complete blood counts were measured for all patients one day preoperatively and postoperatively. During the first 24 hours after surgery, fever, pulse, and blood pressure were monitored hourly. Patients without signs of infection did not receive additional antibiotic prophylaxis or treatment. Postoperative analgesia was administered upon patient request, with paracetamol or dexketoprofen given at intervals of no less than six hours. Patients were assessed for postoperative fever, SIRS, and sepsis, and their clinical conditions were recorded. Postoperative complications were classified and documented according to the Modified Clavien-Dindo classification.9
Diagnostic Criteria for SIRS and Sepsis
SIRS was defined by the presence of at least two of the following criteria: a white blood cell count lower than 4000 or higher than 12,000 cells/µL, a body temperature above 38°C or below 36°C, a heart rate exceeding 90 beats per minute, or a respiratory rate greater than 20 breaths per minute with a PaCO2 level below 32 mmHg.
Urosepsis was diagnosed based on a qSOFA (Quick Sepsis-Associated Organ Failure Assessment) score of ≥2, which included respiratory rate equal to or greater than 22 breaths per minute, altered mental status with a Glasgow Coma Scale (GCS) score below 13, or systolic blood pressure of 100 mmHg or lower.10,11
Study Endpoints
The primary endpoint of this study was to identify which preoperative and perioperative parameters contribute to the development of postoperative SIRS in PCNL and to determine the cut-off values for SIRS indicator parameters, including SII, AISI, and SIRI. The secondary endpoints included assessing postoperative stone-free rates, infection rates, and complication rates in patients undergoing PCNL.
Statistical Analyses
The distribution of the data was determined using the Kolmogorov–Smirnov test and histogram graphs. Categorical variables were presented as frequency and percentage, while numerical variables with a normal distribution were expressed as mean ± standard deviation (SD). Non-normally distributed numerical variables were reported as median (1st–3rd quartile).
Logistic regression analyses (both univariate and multiple) were used to assess relationships between variables. The strength of associations between categorical and numerical variables was evaluated using Receiver Operating Characteristic (ROC) analysis, with the area under the curve (AUC) as the primary measure. AUC values between 0.40 and 0.60 were considered as weak relationship, between 0.60 and 0.80 as moderate relationship, and between 0.80 and 1.0 as strong relationship. The optimal cut-off values for SII, SIRI, and AISI were determined mathematically based on the maximum Youden Index, defined as “sensitivity + specificity – 1”. A p-value of <0.05 was considered statistically significant.
Results
A total of 233 patients were included in the study, of whom 147 (63.1%) were male and 86 (36.9%) were female. The mean age of the patients was 50.4 ± 14.2 years. Mini-PCNL was performed in 205 patients (88%), while conventional PCNL was performed in 28 patients (12%). Among the mini-PCNL procedures, 120 (58.5%) were conducted in the prone position and 85 (41.5%) in the supine position, whereas all conventional PCNL surgeries were performed in the prone position.
The median preoperative stone size was 270.0 mm2 (IQR: 180.0–447.0). The clinically significant stone-free rate was 89.3% (208/233), while the complete stone-free rate was 79.1% (182/233). In the postoperative period, fever occured in 16 patients (6.9%), SIRS in 75 patients (32.1%), and sepsis in 17 patients (7.3%). There were no postoperative mortality in any of the patients who occured fever, SIRS, or sepsis.
No complications occured in 180 patients (77.3%), while complications were observed in 53 (22.7%) patients according to the Modified Clavien-Dindo classification. Grade 1 complications occurred in 18 patients (7.7%), Grade 2 in 28 patients (12.0%), Grade 3 in 1 patient (0.4%), and Grade 4 in 6 patients (2.6%).
Relationship Between Demographic and Clinical Factors with SIRS
Relationship between postoperative SIRS and variables such as age, BMI, gender, and the presence of diabetes, none of these factors were found to have a direct association with postoperative SIRS. Additionally, no significant relationship was identified between SIRS and five clinical factors, including a history of previous ESWL or urinary stone surgery, preoperative DJ stent or nephrostomy, and the presence of preoperative hydronephrosis (p > 0.05 for all).
Relationship Between Urinary Characteristics, Perioperative/Postoperative Factors, and SIRS
Although all patients had a sterile preoperative urine culture, bacterial growth was observed in 65 (27.9%) intraoperatively collected stone cultures. Additionally, bacterial growth was detected in only 13 (5.6%) intraoperatively obtained renal pelvic urine cultures.
The presence of bacterial growth in intraoperatively collected renal pelvic urine cultures, longer hospital stay, prolonged operative time, increased irrigation fluid usage, and clinically significant residual stones were found to increase the risk of SIRS. Furthermore, postoperative SIRS rates for the prone and supine positions were 35.1% and 17.6%, respectively (p < 0.001), indicating that surgical position significantly influenced SIRS (p = 0.005, Nagelkerke R2 = 0.080). However, other urinary and stone characteristics were not found to be significant factors in SIRS (Table 1).
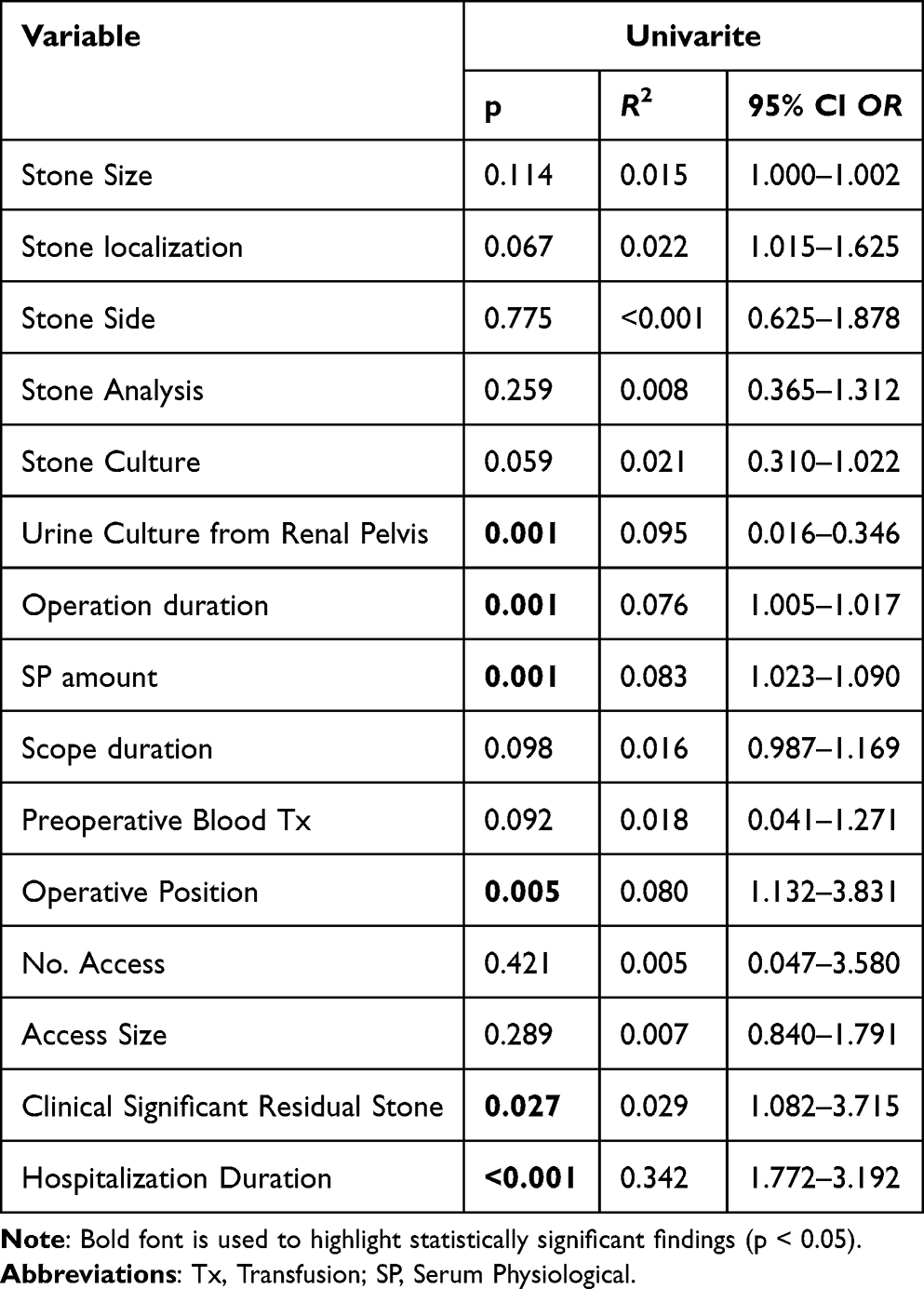 |
Table 1 Relationship of Peroperative, Postoperative and Stone/Urine Characteristics with SIRS |
SII, SIRI, AISI, and Other Serum Markers
Indices calculated based on serum values, such as SII, SIRI, and AISI, were found to be directly associated with SIRS. Additionally, perioperative hemoglobin (Hb) drop and serum white blood cell (WBC) count were also related to SIRS, whereas no significant relationship was observed between CRP levels and SIRS (Table 2).
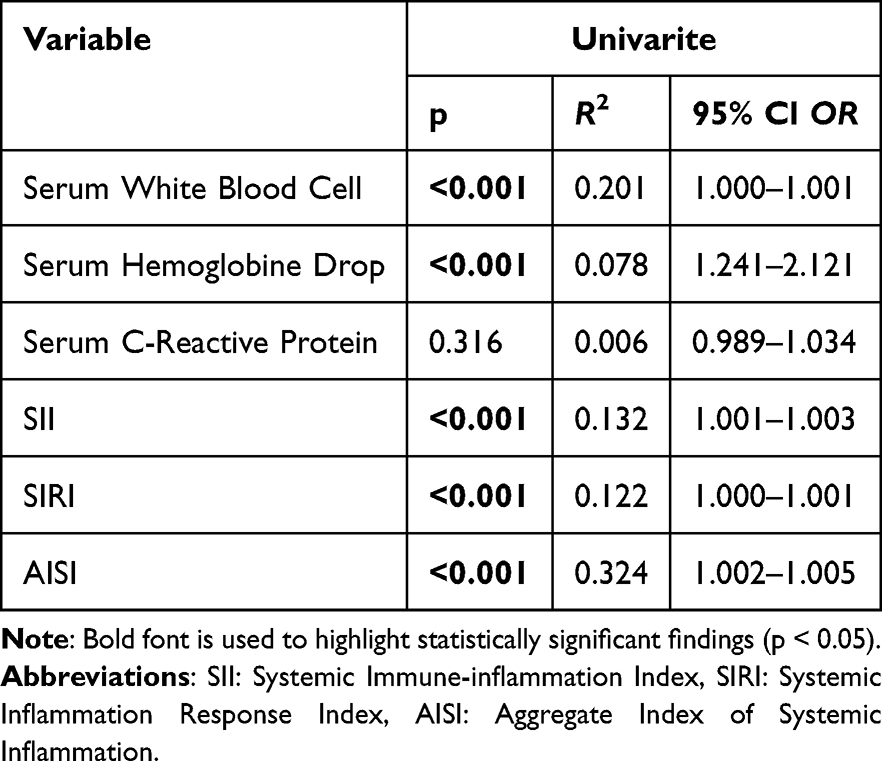 |
Table 2 Relationship of Some Serum Parameters and Their Calculations with Postoperative SIRS |
In the ROC analysis evaluating the relationship of these variables with SIRS, the area under the curve (AUC) values for SII, SIRI, and AISI were 0.607, 0.591, and 0.639, respectively, indicating a moderate correlation between these three parameters and SIRS (Figure 1).
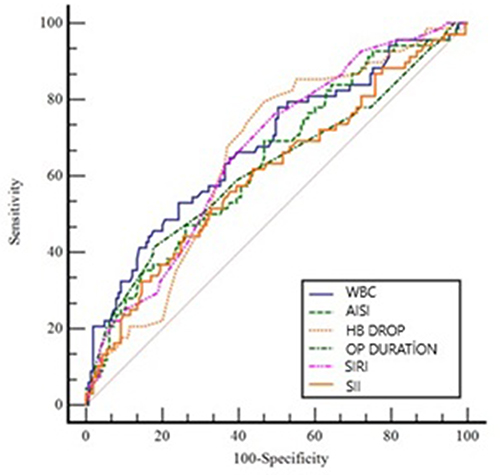 |
Figure 1 ROC curves demonstrating the predictive performance of numerical parameters associated with postoperative SIRS (Systemic Inflammatory Response Syndrome). The figure compares WBC, AISI, Hb drop, operation duration, SIRI, and SII values in terms of sensitivity and specificity. Abbreviations: WBC, White blood cell; SII, Systemic Immune-Inflammation Index; SIRI, Systemic Inflammation Response Index; AISI, Aggregate Index of Systemic Inflammation; Hb,Hemoglobin; OP Duration, Operation duration. |
Furthermore, the cut-off values for the parameters associated with SIRS, calculated based on the Youden Index, are summarized in Table 3.
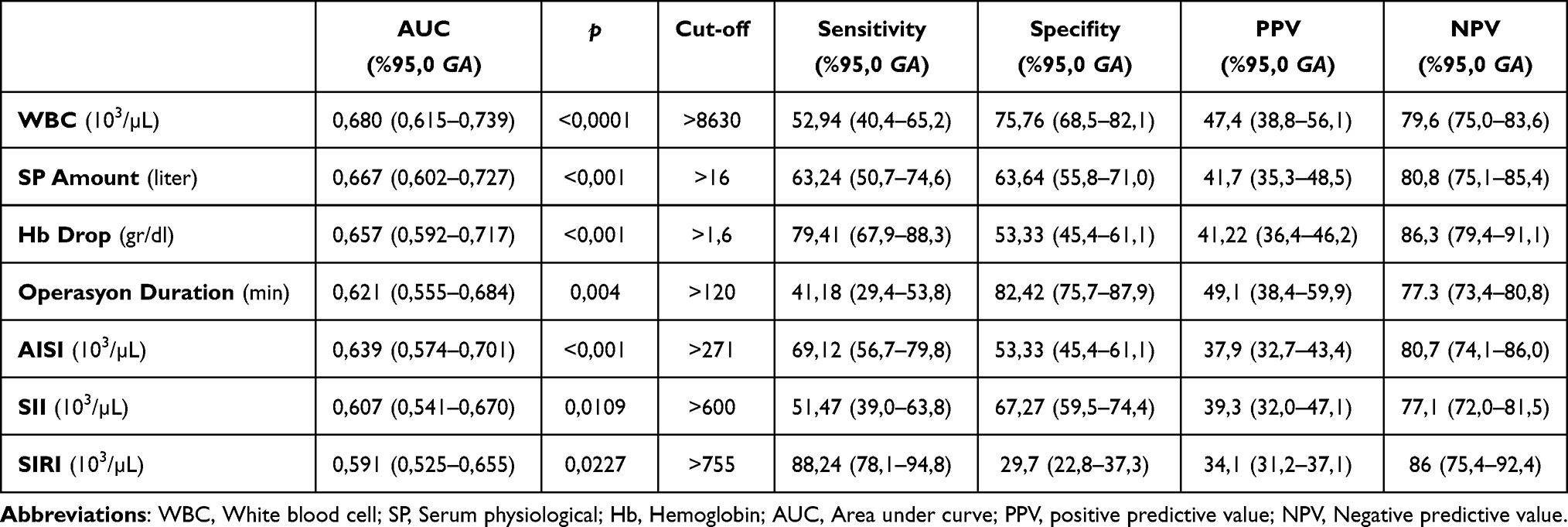 |
Table 3 Sensitivity, Specificity and Cut-off Values of Numerical Parameters Associated with SIRS Calculated According to the Youden Index |
Can After PCNL SIRS Be Predicted?
In our study, some clinical parameters found to be associated with the development of SIRS after PCNL were included in multiple logistic regression analyses. Parameters such as clinically significant residual stone presence, WBC count, operative time, amount of saline used, and hemoglobin decrease were analyzed. However, SII, SIRI, and AISI, which have been previously proven to be associated with SIRS in other studies, were not included in the analysis. Additionally, hospital stay duration was excluded, as it is considered a natural consequence of SIRS.
According to the results, using these parameters, the development of SIRS after PCNL could be predicted with an accuracy of 83.6% (See Table 4).
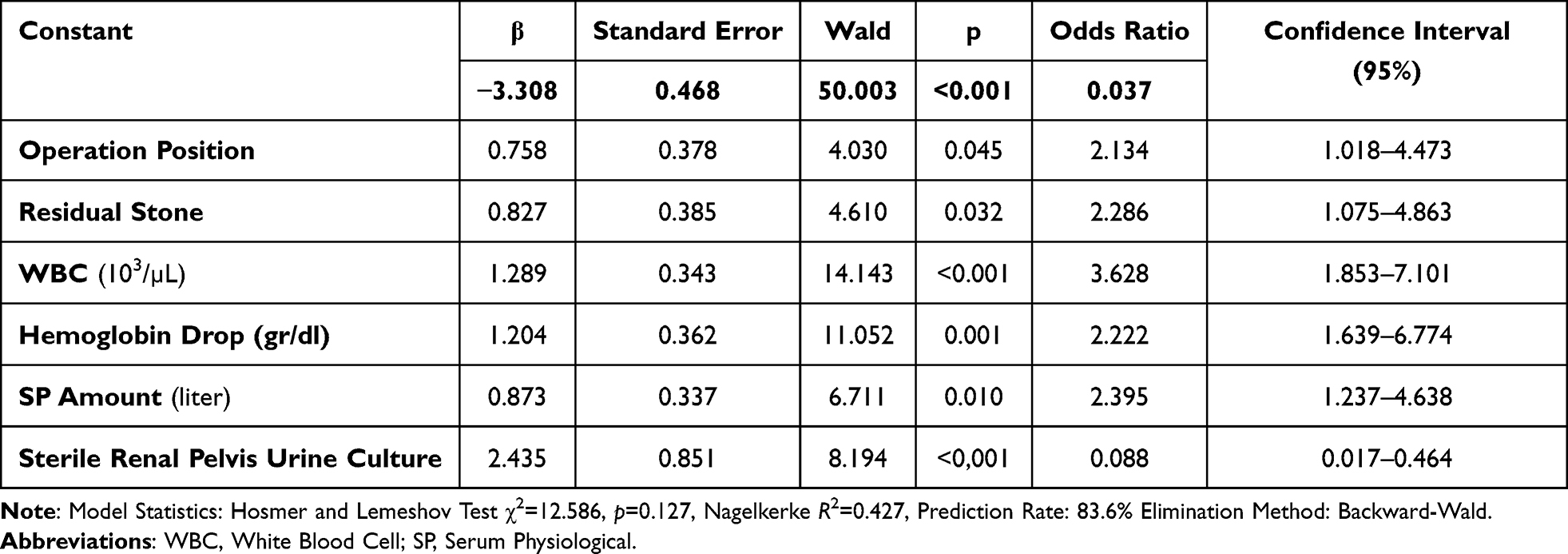 |
Table 4 Evaluation of Some Variables Found to Have a Significant Relationship with Post-PCNL in Univariate Logistic Regression Analyses Using Multiple Logistic Regression Analysis |
Discussion
In our study, the relationship between post-PCNL SIRS and inflammation markers such as SII, AISI, and SIRI was prospectively investigated for the first time in the literature. In an extensive analysis evaluating the effects of 33 different variables on postoperative SIRS, it was determined that prolonged surgery duration, bacterial growth in intraoperative renal pelvis urine cultures, increased amount of intraoperative saline irrigation, performing the surgery in the prone position, and the presence of clinically significant residual stones increased the risk of SIRS. Additionally, a greater decrease in hemoglobin levels, elevated WBC count, and high SII, AISI, and SIRI values were found to be significant factors contributing to postoperative SIRS rates. These findings suggest that certain preoperative, intraoperative, and postoperative parameters play a crucial role in predicting SIRS development after PCNL. Accordingly, the implementation of closer monitoring and preventive strategies in high-risk patients may help reduce postoperative complication rates.
Although SII, AISI, and SIRI have been established as effective inflammatory markers, studies investigating their relationship with SIRS following PCNL remain limited. A retrospective study published in 2021, which included 365 patients, reported that postoperative SIRS developed in 108 (29.6%) patients, and SII was found to be strongly associated with postoperative SIRS after PCNL (AUC = 0.782).12 In that study, similar to our findings, prolonged operative time and elevated WBC levels were also identified as factors associated with postoperative SIRS. Another recent retrospective study examining the relationship between SII and post-PCNL SIRS also confirmed a significant association, reporting an AUC value of 0.680, which is comparable to our findings.13 Meanwhile, two recent studies published in 2022 and 2024 demonstrated a link between SIRI and kidney stone formation; however, they did not provide conclusions regarding its impact on postoperative SIRS.14,15 Other studies have explored the associations of AISI and SIRI with conditions such as general SIRS, COVID-19, renal failure, and prostate cancer, but no study has specifically investigated their relationship with post-PCNL SIRS.16–18 From this perspective, our study stands as the first in the literature to prospectively examine the relationship between these inflammatory markers and SIRS following PCNL. Despite the limited existing literature, our results appear to be consistent with those of previous studies, further reinforcing their significance. In addition, the fact that the AUC values of these clinical parameters were not very strong may have been due to the application of strict inclusion and exclusion criteria in our study to ensure patient standardization.
In our study, the cut-off values of markers associated with post-PCNL SIRS were also determined. These values were identified as 8630 for WBC (103/µL), 16 for SP Amount (liter), 1.6 for Hb drop (g/dl), 120 for operation duration (min), 271 for AISI (103/µL), 600 for SII (103/µL), and 755 for SIRI (103/µL), respectively. Although no study in the literature has determined cut-off values for SII, SIRI, and AISI in this context, studies on COVID-19 and certain inflammatory diseases have been conducted, and the cut-off values identified in those studies appear to be similar.19,20 However, due to differences in the diseases investigated, a direct comparison between our study and the literature data could not be made.
According to the results of our study, other factors that increase the risk of post-PCNL SIRS include prolonged operative time, increased Hb drop, and increased amount of perioperative irrigation solution (normal saline). A study published in 2024, conducted on 51 patients with a solitary kidney, reported that prolonged operative time increases the risk of post-PCNL SIRS.21 Similarly, a meta-analysis involving 7507 patients found a direct association between prolonged operative time and SIRS.7 Unlike our study, that meta-analysis also identified an increased number of access tracts and the presence of diabetes mellitus as risk factors for SIRS. In another study published in 2022, prolonged operative time, increased Hb drop, and prolonged hospital stay were found to be associated with SIRS, similar to our findings. However, unlike our study, that research also identified the need for blood transfusion, postoperative complications, and serum CRP levels as factors triggering SIRS.22 Another study also reported that a higher perioperative Hb drop, prolonged operative time, and extended hospital stay were significant risk factors for postoperative SIRS.23 Considering that increased perioperative normal saline usage, prolonged hospitalization, and increased Hb drop are natural consequences of prolonged operative time, our findings appear to be consistent with the literature and represent expected results.
Although serum CRP is known as an important biomarker in inflammatory processes, our study did not find an association between CRP levels and post-PCNL SIRS. Contrary to our findings, Wang et al described CRP as an effective marker for predicting SIRS in their study.24 However, a systematic review reported that while there is a relationship between CRP and post-PCNL SIRS, this association is considered weak. Researchers attribute this to the fact that CRP is not solely an infection marker but also elevates in conditions such as rheumatologic diseases, cancers, and drug reactions.25
The impact of bacterial growth in perioperatively obtained renal pelvic urine cultures and stone cultures on the development of post-PCNL SIRS remains controversial. Singh et al argued that neither of these parameters significantly influences post-PCNL SIRS.26 However, a systematic review reporting a 21% incidence of post-PCNL SIRS found that bacterial growth in stone cultures obtained from the renal pelvis increased the risk of SIRS.27 According to the results of our study, renal pelvic stone cultures were not found to be associated with SIRS, whereas bacterial growth in renal pelvic urine cultures was identified as a risk factor for SIRS. However, it should be noted that in our study, bacterial growth was detected in the renal pelvic urine cultures of only 13 patients and in the stone cultures of 65 patients. The discrepancies between our findings and the literature may be attributed to the small sample size.
PCNL positioning remains one of the most debated topics in kidney stone surgery. While early studies reported no difference in complication rates between PCNL positions, a meta-analysis published by Li et al in 2024 found that PCNL procedures performed in the prone position had a higher rate of infectious complications compared to the supine and flank positions.28,29 Similarly, our study demonstrated that post-PCNL SIRS occurred significantly more frequently in patients undergoing PCNL in the prone position compared to other positions (35.1% vs 17.6%, p<0.001).
This study has several important limitations. The most significant limitation is the small sample size. Additionally, postoperative SIRS and infection development can be influenced by numerous patient-related and clinical factors. To ensure proper homogenization, patients with clinical characteristics that could increase the risk of infection and SIRS were excluded from the study. Therefore, our findings may not fully reflect the overall population data but rather represent the outcomes of an ideal patient group. Furthermore, other limitations of our study include: (i) The presence of multiple factors that may influence the development of postoperative SIRS, making it challenging to clearly differentiate their effects, (ii) The low number of patients who underwent PCNL with a 30F standard sheath, (iii) The lack of similar studies in the literature regarding cut-off values of inflammatory markers, (iv) the single-center design of the study and lack of long-term follow-up limiting the ability to make adequate comparisons.
Conclusions
This study identified several risk factors for the development of post-PCNL SIRS. These risk factors include bacterial growth in perioperatively obtained renal pelvic urine cultures, prolonged operative time, increased perioperative normal saline usage, prone surgical position, clinically significant residual stones, perioperative hemoglobin (Hb) drop, and preoperative white blood cell (WBC) count. In addition, it was observed that the indices calculated using blood parameters (SII, AISI, SIRI) could be useful in identifying high-risk patients, even if they did not have very high AUC values. Although cut-off values for these risk factors were determined in our study, larger-scale studies with broader sample sizes are needed in the future to establish more precise cut-off values. By paying attention to these parameters, clinicians can recommend more careful antibiotic prophylaxis and closer postoperative follow-up for patients with risk factors.
Ethical Approval
This research has been approved by the research committee of Erciyes University of Medical Sciences (08/06/2022, 2022/438) and the study has been conducted in accordance with the principles of the Helsinki Declaration for medical research. Informed consent was taken from the patients for obtaining their information and publication of their data if remained anonymous.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no competing interests in this work.
References
1. Calvillo-Ramirez A, Angulo-Lozano JC, Acevedo-Rodriguez JE, et al. Comparative outcomes of day-case percutaneous nephrolithotomy versus conventional inpatient surgery: a systematic review and meta-analysis. Urology. 2025;195:214–10. doi:10.1016/j.urology.2024.09.036
2. Liu Y, Zhang H, Wen Z, et al. Efficacy and safety of minimally invasive percutaneous nephrolithotomy versus retrograde intrarenal surgery in the treatment of upper urinary tract stones (> 1 cm): a systematic review and meta-analysis of 18 randomized controlled trials. BMC Urol. 2023;23(1):171. doi:10.1186/s12894-023-01341-3
3. Awedew AF, Alemu CT, Yalew DZ. Efficacy and safety of various endosurgical procedures for management of large renal stone: a systematic review and network meta-analysis of randomised control trials. Urolithiasis. 2023;51(1):87. doi:10.1007/s00240-023-01459-x
4. Jiang K, Zhang P, Xu B, et al. Percutaneous nephrolithotomy vs. retrograde intrarenal surgery for renal stones larger than 2cm in patients with a solitary kidney: a systematic review and a meta-analysis. Urol J. 2020;17(5):442–448. doi:10.22037/uj.v16i7.5609
5. Castellani D, Teoh JY, Pavia MP, et al. Assessing the optimal urine culture for predicting systemic inflammatory response syndrome after percutaneous nephrolithotomy and retrograde intrarenal surgery: results from a systematic review and meta-analysis. J Endourol. 2022;36(2):158–168. doi:10.1089/end.2021.0386
6. Wang L, Li D, He W, et al. Development and validation of a predictive model for post-percutaneous nephrolithotomy urinary sepsis: a multicenter retrospective study. Minerva Urol Nephrol. 2024;76(3):357–366. doi:10.23736/S2724-6051.23.05396-X
7. Puia D, Gheorghincă Ş, Radavoi GD, et al. Can we identify the risk factors for SIRS/sepsis after percutaneous nephrolithotomy? A meta‑analysis and literature review. Exp Ther Med. 2023;25(3):110. doi:10.3892/etm.2023.11809
8. Tuzimek A, Dziedzic EA, Beck J, et al. Correlations between acute coronary syndrome and novel inflammatory markers (Systemic Immune-Inflammation Index, Systemic Inflammation Response Index, and Aggregate Index of Systemic Inflammation) in patients with and without diabetes or prediabetes. J Inflamm Res. 2024;17:2623–2632. doi:10.2147/JIR.S454117
9. Singh AK, Shukla PK, Khan SW, et al. Using the modified clavien grading system to classify complications of percutaneous nephrolithotomy. Curr Urol. 2018;11(2):79–84. doi:10.1159/000447198
10. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
11. Li P, Tang Y, Zeng Q, et al. Diagnostic performance of machine learning in systemic infection following percutaneous nephrolithotomy and identification of associated risk factors. Heliyon. 2024;10(10):e30956. doi:10.1016/j.heliyon.2024.e30956
12. Peng C, Li J, Xu G, et al. Significance of preoperative systemic immune-inflammation (SII) in predicting postoperative systemic inflammatory response syndrome after percutaneous nephrolithotomy. Urolithiasis. 2021;49(6):513–519. doi:10.1007/s00240-021-01266-2
13. Wei Q, Liu A, Sun Z, et al. The predictive value of systemic inflammatory biomarkers in predicting postoperative systemic inflammatory response syndrome after percutaneous nephrolithotomy. Int J Gen Med. 2024;17:6513–6521. doi:10.2147/IJGM.S497322
14. Zhang Z, Wang G, Dai X, et al. Association between the systemic inflammation response index and kidney stones in US adults: a cross-sectional study based on NHANES 2007--2018. Urolithiasis. 2024;52(1):165. doi:10.1007/s00240-024-01668-y
15. Liu CJ, Jan HC, Huang HS. Risks of carotid artery stenosis and atherosclerotic cardiovascular disease in patients with calcium kidney stone: assessment of systemic inflammatory biomarkers. J Pers Med. 2022;12(10):1697. doi:10.3390/jpm12101697
16. Tarle M, Raguž M, Lukšić I. A comparative study of the Aggregate Index of Systemic Inflammation (AISI) and C-Reactive Protein (CRP) in predicting odontogenic abscesses severity: a novel approach to assessing immunoinflammatory response. Diagnostics. 2024;14(19):2163. doi:10.3390/diagnostics14192163
17. Xie W, Xu Z, Qiu Y, et al. A novel nomogram combined the aggregate index of systemic inflammation and PIRADS score to predict the risk of clinically significant prostate cancer. Biomed Res Int. 2023;2023:9936087. doi:10.1155/2023/9936087
18. Ercan Z, Evren Öztop K, Pınar M, et al. The aggregate index of systemic inflammation may predict mortality in COVID-19 patients with chronic renal failure. Eur Rev Med Pharmacol Sci. 2023;27(8):3747–3752. doi:10.26355/eurrev_202304_32173
19. Hamad DA, Aly MM, Abdelhameid MA, et al. Combined blood indexes of systemic inflammation as a mirror to admission to intensive care unit in COVID-19 patients: a multicentric study. J Epidemiol Glob Health. 2022;12(1):64–73. doi:10.1007/s44197-021-00021-5
20. He P, Yang H, Lai Q, et al. The diagnostic value of blood cell-derived indexes in subacute thyroiditis patients with thyrotoxicosis: a retrospective study. Ann Transl Med. 2022;10(6):322. doi:10.21037/atm-22-719
21. Fang Y, Liu Y, Huang H, et al. Analysis of risk factors for SIRS after PCNL in patients with solitary kidney. Urolithiasis. 2024;53(1):10. doi:10.1007/s00240-024-01681-1
22. Akdeniz E, Ozturk K, Ulu MB, et al. Risk factors for systemic inflammatory response syndrome in patients with negative preoperative urine culture after percutaneous nephrolithotomy. J Coll Physicians Surg Pak. 2021;31(4):410–416. doi:10.29271/jcpsp.2021.04.410
23. Chan JY, Wong VK, Wong J, et al. Predictors of urosepsis in struvite stone patients after percutaneous nephrolithotomy. Investig Clin Urol. 2021;62(2):201–209. PMID: 33660448; PMCID: PMC7940850. doi:10.4111/icu.20200319
24. Wang C, Xu R, Zhang Y, et al. Nomograms for predicting the risk of SIRS and urosepsis after uroscopic minimally invasive lithotripsy. Biomed Res Int. 2022;2022:6808239. doi:10.1155/2022/6808239
25. Wu W, Zhang D, Jin T, et al. Progress in the study of biomarkers for early prediction of systemic inflammatory response syndrome after percutaneous nephrolithotomy. Front Immunol. 2023;14:1142346. doi:10.3389/fimmu.2023.1142346
26. Singh I, Shah S, Gupta S, et al. Efficacy of intraoperative renal stone culture in predicting postpercutaneous nephrolithotomy urosepsis/systemic inflammatory response syndrome: a prospective analytical study with review of literature. J Endourol. 2019;33(2):84–92. doi:10.1089/end.2018.0842
27. Li Y, Xie L, Liu C. Prediction of systemic inflammatory response syndrome and urosepsis after percutaneous nephrolithotomy by urine culture, stone culture, and renal pelvis urine culture: systematic review and meta-analysis. Heliyon. 2024;10(13):e33155. doi:10.1016/j.heliyon.2024.e33155
28. Li P, Ma Y, Liao B, et al. Comparison of safety and efficacy of different positions in percutaneous nephrolithotomy: a network meta-analysis. Int J Surg. 2024;110(4):2411–2420. doi:10.1097/JS9.0000000000001130
29. Zhang X, Xia L, Xu T, et al. Is the supine position superior to the prone position for percutaneous nephrolithotomy (PCNL)? Urolithiasis. 2014;42(1):87–93. doi:10.1007/s00240-013-0614-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparative Study of Prone Position Variations for Percutaneous Nephrolithotomy
Yilmaz M, Sahin Y
Research and Reports in Urology 2023, 15:233-241
Published Date: 23 June 2023
Predictive Significance of Admission-Day Blood Routine-Derived Indices for 30-Day Mortality Risk in Elderly Patients with Bacterial Pneumonia
Huang X, Huang L, Zhao S, Yuan L, Wang X, Tang G, Yuan K, Xiao M
International Journal of General Medicine 2025, 18:1295-1309
Published Date: 5 March 2025
Limited Predictive Utility of Inflammatory Indices for Postoperative Complications in Primary Lung Cancer Surgery
Özkaya M, Yalçın NÇ, Özyurt E, Tercan M
International Journal of General Medicine 2025, 18:6627-6635
Published Date: 4 November 2025