Back to Journals » International Journal of General Medicine » Volume 18
Limited Predictive Utility of Inflammatory Indices for Postoperative Complications in Primary Lung Cancer Surgery
Authors Özkaya M ![]() , Yalçın NÇ
, Yalçın NÇ ![]() , Özyurt E
, Özyurt E ![]() , Tercan M
, Tercan M ![]()
Received 25 April 2025
Accepted for publication 29 October 2025
Published 4 November 2025 Volume 2025:18 Pages 6627—6635
DOI https://doi.org/10.2147/IJGM.S536626
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ching-Hsien Chen
Muharrem Özkaya,1 Nilay Çavuşoğlu Yalçın,1 Erhan Özyurt,2 Mehmet Tercan2
1Department of Thoracic Surgery, University of Health Sciences, Antalya Training and Research Hospital, Antalya, Türkiye; 2Department of Anesthesiology and Reanimation, University of Health Sciences, Antalya Training and Research Hospital, Antalya, Türkiye
Correspondence: Muharrem Özkaya, Department of Thoracic Surgery, University of Health Sciences, Antalya Training and Research Hospital, Varlık Mahallesi, Kazım Karabekir Street No: 48, Muratpasa, Antalya, 07100, Türkiye, Tel +905326543438, Fax +902422494662, Email [email protected]
Background: Systemic inflammatory indices such as the Pan-Immune Inflammation Value (PIV), Systemic Immune-Inflammation Index (SII), and Systemic Inflammation Response Index (SIRI) are recognized prognostic markers in oncology. Their potential role in predicting early postoperative complications after lung cancer surgery, however, remains uncertain.
Methods: We retrospectively analyzed 68 patients who underwent pulmonary resection for primary lung cancer between January 2019 and November 2024. PIV, SII, and SIRI were calculated from preoperative and first postoperative day blood counts. Associations with 30-day complications were assessed using comparative statistics and receiver operating characteristic (ROC) analysis.
Results: Complications occurred in 10 patients (14.7%). None of the indices differed significantly between patients with and without complications. ROC analysis demonstrated poor predictive performance across all indices (AUC range: 0.447– 0.612). A significant histology imbalance (p=0.039) suggested that tumor biology may have contributed to complication risk.
Conclusion: Despite their established prognostic relevance in oncology, PIV, SII, and SIRI provided limited discrimination for early postoperative complications in lung cancer surgery. These negative findings underscore the importance of cautious interpretation, particularly given the small number of events and low statistical power. They highlight the limited perioperative utility of such indices, helping to prevent their overestimation in clinical practice, and point to the need for prospective studies exploring alternative predictive markers within multimodal models.
Keywords: lung cancer, postoperative complications, PIV, SII, SIRI, inflammatory biomarkers, ROC analysis
Introduction
Lung cancer remains the leading cause of cancer-related mortality worldwide, accounting for approximately 1.8 million deaths annually according to global cancer statistics.1 Surgical resection remains the cornerstone of curative-intent treatment for early-stage non-small cell lung cancer (NSCLC). Despite advances in surgical techniques, perioperative care, and patient selection, postoperative complications continue to significantly impact morbidity, mortality, and healthcare costs in thoracic surgery.2,3
Postoperative complications such as pneumonia, atelectasis, prolonged air leak, and bronchopleural fistula may lead to prolonged hospitalization, delayed recovery, and poorer oncologic outcomes.4 Therefore, early identification of patients at high risk for such complications is essential for optimizing perioperative management and improving surgical outcomes.
Recently, systemic inflammatory markers derived from routine hematological parameters have been explored as potential predictors of oncologic prognosis and surgical outcomes. Among these, the Pan-Immune Inflammation Value (PIV), Systemic Immune-Inflammation Index (SII), and Systemic Inflammation Response Index (SIRI) have attracted attention due to their ease of calculation and cost-effectiveness.5,6 We focused on PIV, SII, and SIRI because, unlike simpler ratios such as NLR or PLR, these composite indices integrate multiple hematologic cell lines (neutrophils, lymphocytes, monocytes, and platelets), thereby providing a broader reflection of systemic immune–inflammatory balance. These indices are thought to reflect the systemic inflammatory and immune status of the host, which plays a critical role in tumor progression, postoperative healing, and immune response regulation. Tumor-associated inflammation has also been recognized as a fundamental component of the tumor microenvironment, playing a pivotal role in cancer progression, immune modulation, and therapeutic resistance.7–9
Previous studies have demonstrated the prognostic significance of these indices in various malignancies. In particular, a recent meta-analysis by Chen et al, which included 16 studies with 4,682 patients, confirmed that elevated pretreatment SII levels were significantly associated with poorer overall survival (OS) and progression-free survival (PFS) in NSCLC patients, most of whom were treated with curative-intent surgery.10 However, while the prognostic relevance of these biomarkers in terms of long-term survival is well-documented, their potential role in predicting early postoperative complications remains unclear.
In this context, our study aimed to evaluate the predictive and prognostic value of preoperative and postoperative PIV, SII, and SIRI specifically for postoperative complications in patients undergoing pulmonary resection for primary lung cancer. By focusing on both preoperative immune status and immediate postoperative inflammatory response, we sought to determine whether these indices could be effectively utilized as risk assessment tools in the perioperative management of lung cancer surgery. Based on prior evidence linking systemic inflammation to adverse outcomes, we hypothesized that higher preoperative and postoperative values of PIV, SII, and SIRI would be associated with an increased risk of early postoperative complications in patients undergoing lung cancer surgery.
Methods
Study Design and Patient Selection
This retrospective cohort study was conducted at the Thoracic Surgery Department of SBU Antalya Research and Education Hospital. Medical records of patients who underwent pulmonary resection between January 2019 and January 2025 were reviewed. A total of 96 patients were initially assessed. Patients whose final pathological diagnosis was not primary lung cancer (n=28) were excluded. The remaining 68 patients with confirmed primary lung cancer were included in the final analysis. The last eligible patient included in the analysis underwent surgery in November 2024.
The study protocol was approved by the Institutional Ethics Committee of SBU Antalya Research and Education Hospital (Approval Number: 2025–010), and the study was conducted in accordance with the Declaration of Helsinki. Due to the retrospective nature of the study, the requirement for informed consent was waived.
Surgical Procedure and Perioperative Management
All patients underwent anatomical pulmonary resections (lobectomy, pneumonectomy, segmentectomy, or wedge resection) performed via open thoracotomy or video-assisted thoracoscopic surgery (VATS), based on tumor location, stage, and patient-specific factors. Standard perioperative care protocols, including prophylactic antibiotics, chest physiotherapy, and postoperative monitoring, were applied uniformly across all patients.
Data Collection
Demographic data (age, sex), clinical characteristics (tumor histology, clinical stage), surgical details (type of resection), hospitalization duration, 30-day mortality, and postoperative complications were recorded. Complications were defined as any adverse event occurring within 30 days postoperatively, including but not limited to atelectasis, prolonged air leak, bronchial leak, pneumothorax, heart failure, cerebrovascular events, and malignant neuroleptic syndrome. Information on smoking status, comorbidities, and nutritional parameters was not consistently available in the retrospective records and therefore was not included in the present analysis.
Inflammatory Biomarker Assessment
Peripheral blood samples were collected within 24 hours preoperatively and on the first postoperative day. All relevant clinical and laboratory data were available for the included patients, and no missing data required imputation or exclusion. The following inflammatory indices were calculated using complete blood count (CBC) parameters:
● Pan-Immune Inflammation Value (PIV): (Neutrophils × Platelets × Monocytes) / Lymphocytes
● Systemic Immune-Inflammation Index (SII): (Neutrophils × Platelets) / Lymphocytes
● Systemic Inflammation Response Index (SIRI): (Neutrophils × Monocytes) / Lymphocytes
Statistical Analysis
Continuous variables were presented as mean ± standard deviation (SD) for normally distributed data or median (interquartile range, IQR) for non-normally distributed data. Categorical variables were expressed as counts and percentages. Comparisons between patients with and without postoperative complications were performed using the Student’s t-test or Mann–Whitney U-test for continuous variables and the Chi-square test or Fisher’s exact test for categorical variables, as appropriate.
The predictive ability of PIV, SII, and SIRI for postoperative complications was assessed using Receiver Operating Characteristic (ROC) curve analysis. Area under the curve (AUC), sensitivity, specificity, and optimal cut-off values (determined by Youden’s index) were calculated.
A p-value of <0.05 was considered statistically significant. All statistical analyses were conducted using SPSS version 21 (IBM Corp., Armonk, NY, USA).
Results
Patient Characteristics
A total of 68 patients who underwent pulmonary resection for primary lung cancer between January 2019 and January 2025 were included in the analysis. The mean age of the patients was 64.8 ± 8.9 years, with a male predominance (83.8% male, 16.2% female). The majority of patients underwent lobectomy (76.5%), followed by wedge resection (10.3%), pneumonectomy (7.4%), and segmentectomy (5.9%). Regarding tumor histology, adenocarcinoma (42.6%) and squamous cell carcinoma (36.8%) were the most common subtypes, while the remaining 20.6% were categorized as others. Most patients were classified as stage 1 disease (51.5%). The median length of hospital stay was 4 days (IQR: 2–6 days). A statistically significant difference in histology was observed between groups: patients who developed complications had a higher proportion of “other” histologies (50%) compared with those without complications (15.5%, p = 0.039). The 30-day mortality rate was observed in 4 patients (5.9%). Detailed patient characteristics are summarized in Table 1.
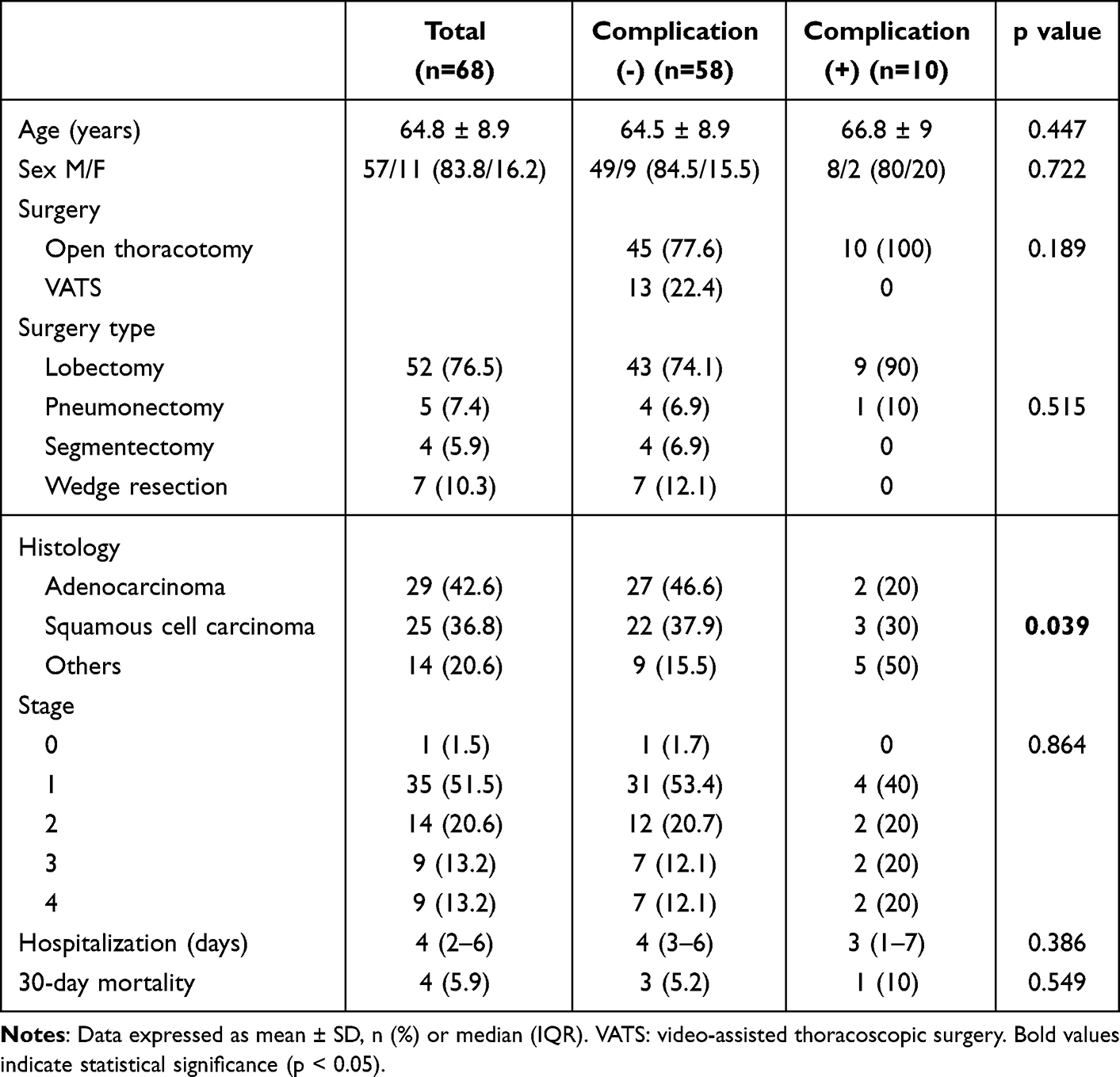 |
Table 1 Characteristic Data of the Study Patients |
Postoperative Complications
Postoperative complications occurred in 10 patients (14.7%), with atelectasis (n=3) being the most frequently observed complication, followed by prolonged air leak (n=2), bronchial leak (n=1), pneumothorax (n=1), heart failure (n=1), cerebrovascular event (n=1), and malignant neuroleptic syndrome (n=1). The distribution of postoperative complications is presented in Table 2.
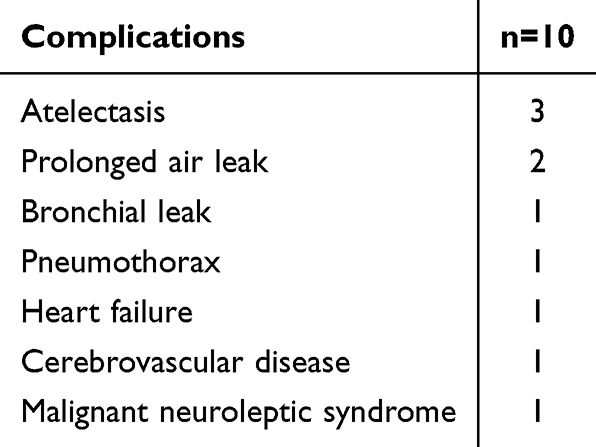 |
Table 2 Postoperative Complications in Study Patients |
Comparison of Inflammatory Biomarkers Between Groups
When comparing patients who developed postoperative complications (complication [+] group) with those who did not (complication [−] group), no statistically significant differences were observed regarding preoperative or postoperative PIV, SII, or SIRI values.
● Preoperative PIV: 578.1 (307.6–773.4) vs 602.4 (366.7–929.2); p = 0.665
● Postoperative PIV: 2352.8 (1432.4–3864.3) vs 2031.9 (819.1–4540.2); p = 0.499
● Preoperative SII: 845.7 (473.2–1069.6) vs 867.7 (498.6–1196.6); p = 0.591
● Postoperative SII: 2205.8 (1715.6–3463.7) vs 2321.5 (1538.1–4447.6); p = 0.795
● Preoperative SIRI: 2.1 (1.2–2.8) vs 1.9 (1.3–2.9); p = 0.931
● Postoperative SIRI: 8.2 (6.3–12.4) vs 6.9 (3.2–12.4); p = 0.260
These results indicate that neither preoperative nor postoperative inflammatory indices were significantly associated with the development of postoperative complications. The comparative analysis of these biomarkers is detailed in Table 3.
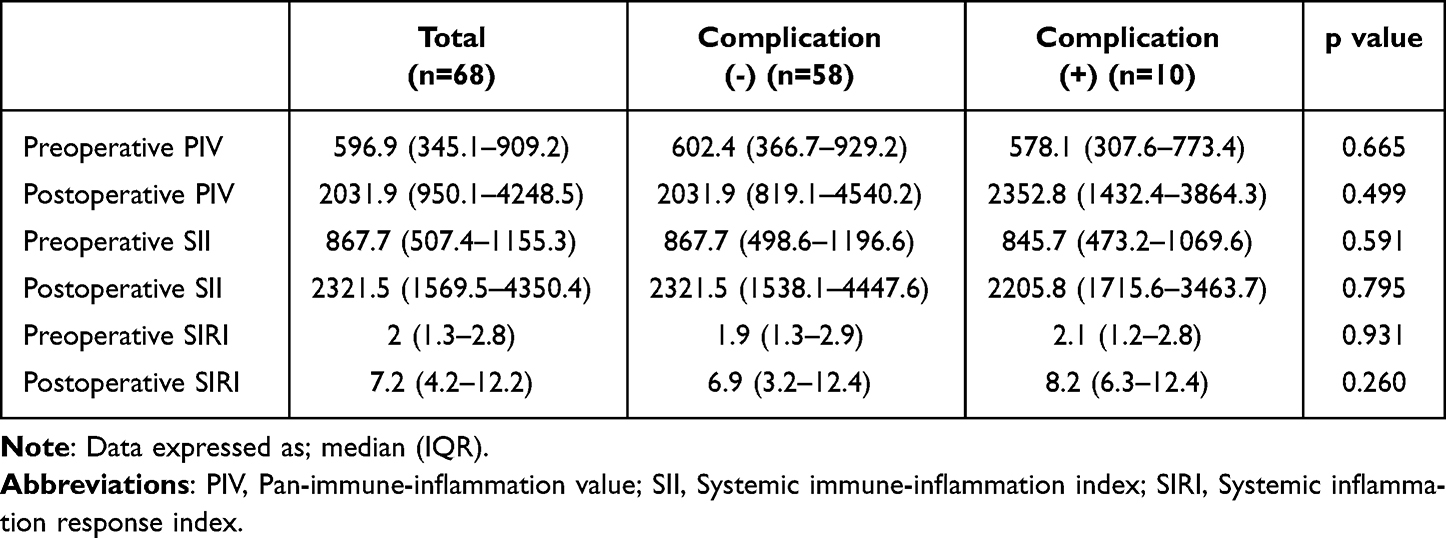 |
Table 3 Comparison of Biomarkers for Development of Complications |
Predictive Performance of Biomarkers for Postoperative Complications
Receiver operating characteristic (ROC) curve analysis was performed to evaluate the predictive performance of the inflammatory indices. All biomarkers demonstrated low predictive value with AUC values ranging from 0.447 to 0.612. The postoperative SIRI yielded the highest AUC (0.612), but this level of performance was still considered poor for clinical prediction.
The sensitivity and specificity values were suboptimal across all biomarkers, with the highest sensitivity of 70% observed in several indices but paired with low specificity (43%–52%). The ROC analysis results, including AUC, sensitivity, specificity, and cut-off values, are presented in Table 4, and the corresponding ROC curves are illustrated in Figure 1.
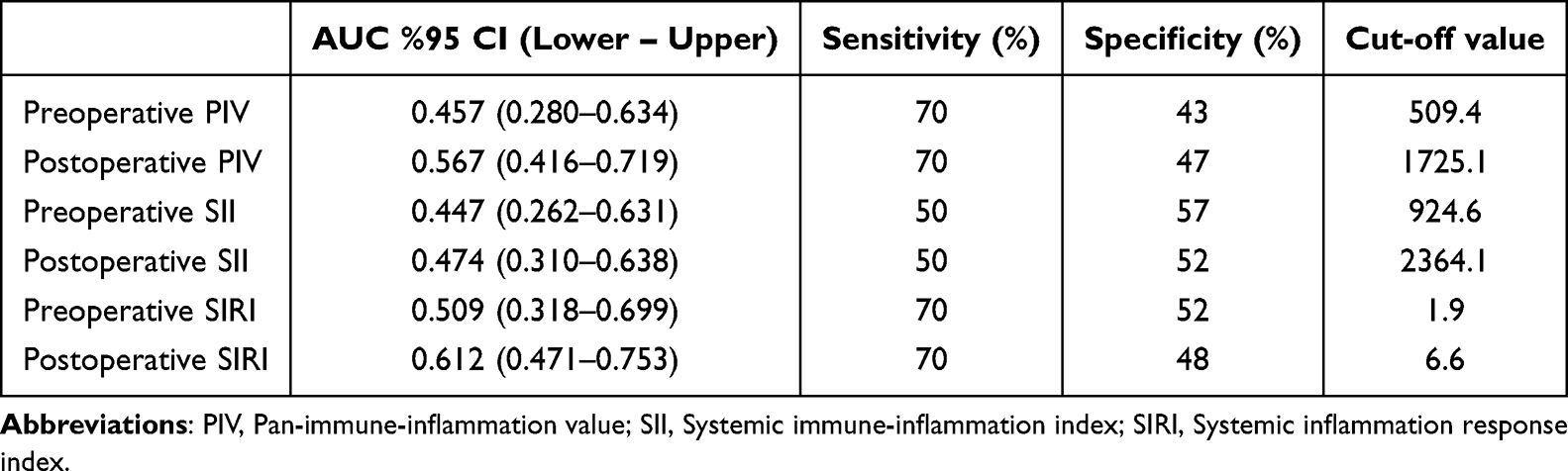 |
Table 4 Biomarkers for Complication Prediction |
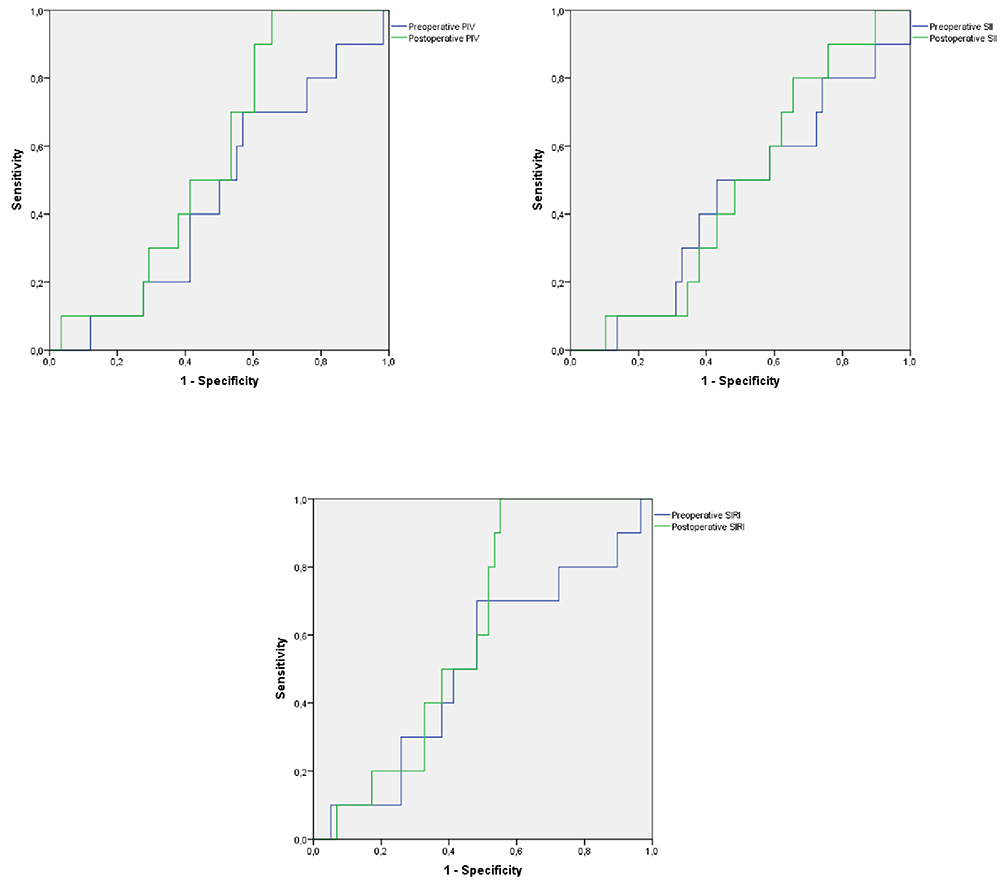 |
Figure 1 Receiver operating characteristic (ROC) curves for preoperative and postoperative PIV, SII, and SIRI in predicting postoperative complications. |
Discussion
Summary of Key Findings
In this retrospective cohort study, we investigated the predictive and prognostic value of three systemic inflammatory indices—Pan-Immune Inflammation Value (PIV), Systemic Immune-Inflammation Index (SII), and Systemic Inflammation Response Index (SIRI)—for postoperative complications in patients undergoing pulmonary resection for primary lung cancer. Our findings demonstrated no statistically significant association between these inflammatory markers and the development of postoperative complications. Additionally, ROC curve analysis revealed low AUC values across all biomarkers, indicating limited predictive capacity for postoperative morbidity. Among the biomarkers evaluated, postoperative SIRI yielded the highest AUC (0.612); however, this level of performance remains insufficient for clinical use.
Comparison with Previous Studies
Numerous studies have explored the prognostic role of systemic inflammatory indices in cancer patients, especially in the context of overall and progression-free survival. Notably, Chen et al recently conducted a meta-analysis that confirmed the prognostic significance of the SII in non-small cell lung cancer (NSCLC), showing its strong association with poor overall survival (OS) and progression-free survival (PFS) outcomes.10 This meta-analysis, which included 16 studies with a total of 4,682 patients, highlighted that most of the included cohorts consisted of resectable NSCLC cases, where pretreatment SII measurements were utilized as prognostic indicators. These findings suggest that systemic immune-inflammation status, reflected by SII levels, may play a critical role in shaping tumor behavior and long-term oncological outcomes in surgically treated lung cancer patients. However, while such findings support the role of systemic inflammation in cancer biology and long-term prognosis, the utility of these indices for predicting early postoperative complications remains largely underexplored.
Other studies focusing on perioperative morbidity have reported mixed results. For example, Ruan et al demonstrated a correlation between elevated preoperative SII and the incidence of postoperative pneumonia in NSCLC patients,11 while Ginesu et al found that postoperative NLR and MLR were significantly associated with surgical complications in thoracic surgery.12 However, it is noteworthy that in the same study, preoperative SIRI, along with other systemic inflammatory indices, did not show a significant association with the development of postoperative complications, which aligns with the findings of our analysis. These studies, however, did not consistently evaluate PIV, SII, and SIRI together, nor did they focus specifically on the broader spectrum of early postoperative complications as assessed in our analysis.
An additional noteworthy finding in our analysis was the significant difference in tumor histology between patients with and without postoperative complications. Patients in the complication group exhibited a higher proportion of “other” histological subtypes (50% vs 15.5%, p = 0.039). Prior evidence indicates that squamous cell carcinoma and uncommon NSCLC variants such as adenosquamous and sarcomatoid carcinoma are associated with heightened systemic inflammatory responses and worse prognosis. This histology-dependent systemic inflammatory profile may at least partially explain the higher complication rate observed in our cohort.13 In line with this, Mariean et al14 demonstrated that NSCLC subtypes differ in their complete blood count-derived inflammatory marker profiles, with NSCLC-NOS and adenosquamous tumors more frequently showing abnormal values. Similarly, Hao et al15 highlighted the prognostic significance of histologic heterogeneity in NSCLC, underscoring that distinct tumor biology influences both oncologic outcomes and perioperative risks. Taken together, these data suggest that our negative findings regarding inflammatory indices should be interpreted with caution, as they may in part reflect the underlying impact of tumor biology rather than the absence of an inflammatory association. This discrepancy likely reflects biological differences: while systemic inflammation contributes to tumor progression and long-term oncological outcomes, early postoperative morbidity is more directly influenced by acute surgical stress, approach-related tissue trauma, and perioperative clinical factors.
Our results suggest that PIV, SII, and SIRI may not be adequate standalone markers for early postoperative complication prediction in lung cancer surgery, especially in the absence of complementary clinical or radiological risk factors.
Evidence from other malignancies suggests that single CBC-derived indices may have only modest standalone discrimination, whereas combining inflammatory with non-inflammatory markers improves performance. In a large gastric-cancer cohort, SII and SIRI alone showed only fair diagnostic ability (male AUCs 0.655 and 0.720; female AUCs 0.593 and 0.654), while the nutritional-inflammatory index PNI outperformed them (AUC ~0.90 in both sexes). Importantly, a composite model that combined CEA with SII, SIRI and PNI achieved substantially higher discrimination (AUC 0.916 in males; 0.893 in females) and a high nomogram C-statistic (0.917 in males; 0.875 in females), underscoring the value of multi-parameter models over single indices. These data support our proposal that future perioperative risk tools should integrate inflammatory indices with clinical variables and additional biomarkers rather than rely on PIV/SII/SIRI alone.16
Importance of Reporting Negative Results
The primary novelty of our study lies in the reporting of negative findings: despite their prognostic relevance in long-term oncologic outcomes, PIV, SII, and SIRI demonstrated limited utility in predicting early postoperative complications. Reporting such results is important to prevent overestimation of these indices in perioperative risk stratification and to guide future research toward more comprehensive predictive approaches. By sharing negative findings, our study contributes to scientific integrity and provides balanced evidence, helping to shape more realistic expectations and guide future study designs.
Study Strengths and Limitations
The main strength of this study lies in its focus on a well-defined cohort of surgically treated primary lung cancer patients, with systematic evaluation of inflammatory biomarkers both preoperatively and postoperatively. The uniform application of perioperative care protocols further reduces variability and enhances data reliability.
However, the retrospective nature of the study and the relatively small sample size limit the generalizability of our findings. Another limitation is that important clinical confounders such as smoking status, comorbidities, and nutritional status were not consistently available in the retrospective records and therefore were not included in the analysis, which may have influenced postoperative outcomes. Inflammatory markers were assessed only at two time points (preoperatively and on the first postoperative day), reflecting standard institutional practice; this restricted our ability to capture the full dynamics of postoperative inflammatory changes. Furthermore, the relatively small number of patients with complications (n=10, 14.7%) severely limits the statistical power of the study and raises the risk of a type II error, meaning that a true association between inflammatory indices and complications may not have been detected. Therefore, our negative findings should be interpreted with caution and confirmed in larger, adequately powered prospective studies. Additionally, surgical approach (thoracotomy vs VATS) may have influenced systemic inflammatory responses because thoracotomy is associated with greater muscle trauma. However, due to the small sample size, stratified analysis or matching by surgical approach could not be performed. This limitation should be considered when interpreting the results, and future larger-scale studies are warranted to clarify the impact of surgical approach on inflammatory indices.
Clinical Implications and Future Directions
Given their simplicity and accessibility, systemic inflammatory indices remain attractive candidates for perioperative risk assessment. Nonetheless, based on our findings, PIV, SII, and SIRI alone cannot be recommended as reliable predictors for early postoperative complications in lung cancer surgery. Future prospective, multicenter studies with larger sample sizes, dynamic serial biomarker measurements, and incorporation of multimodal risk factors are warranted. Integrating these indices into comprehensive models that include clinical variables, imaging findings, and functional assessments may enhance predictive accuracy and clinical utility.
Conclusion
This single-center retrospective study highlights the value of reporting negative findings: despite their established prognostic relevance, PIV, SII, and SIRI showed poor discrimination for early postoperative complications. Given the small number of events and the imbalance in histology, these results should be interpreted with caution. While these indices cannot be recommended as standalone perioperative tools, larger multicenter studies with dynamic biomarker monitoring and integration of clinical, imaging, and functional parameters are warranted to clarify their potential role within comprehensive predictive models.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article. Additional details are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study protocol was approved by the Institutional Ethics Committee of SBU Antalya Research and Education Hospital (Approval Number: 2025-010) and was conducted in accordance with the Declaration of Helsinki. Due to the retrospective nature of the study, the requirement for informed consent was waived. Patient data confidentiality was strictly maintained; all data were anonymized prior to analysis, and no identifiable patient information was used or disclosed.
Acknowledgments
The authors thank the surgical team and data management staff at the Thoracic Surgery Department of SBU Antalya Research and Education Hospital for their support in data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no conflicts of interest in relation to this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Javed H, Olanrewaju OA, Ansah Owusu F, et al. Challenges and solutions in postoperative complications: a narrative review in general surgery. Cureus. 2023:15. doi:10.7759/cureus.50942
3. Semmelmann A, Baar W, Fellmann N, Moneke I, Loop T. The impact of postoperative pulmonary complications on perioperative outcomes in patients undergoing pneumonectomy: a multicenter retrospective cohort study of the german thorax registry. J Clin Med. 2024;14(1):13. doi:10.3390/jcm13010035
4. Pan H, Chen H, Li W, et al. Early outcomes of radical surgery in non-small-cell lung cancer patients with and without COVID-19 history: a multi-center real-world study. Ther Adv Respir Dis. 2024;18:17534666241298794. doi:10.1177/17534666241298794
5. Basar kilic S, Erdal H. Pan-immune inflammation value and systemic inflammatory index as a measure of systemic inflammation in patients with psoriasis: a retrospective study. Medicine. 2025;104.
6. Midik MM, Gunenc D, Acar PF, Karaca BS. Prognostic value of blood-based inflammatory markers in cancer patients receiving immune checkpoint inhibitors. Cancers. 2025;17. doi:10.3390/cancers17010037
7. Nishida A, Andoh A. The role of inflammation in cancer: mechanisms of tumor initiation, progression, and metastasis. Cells. 2025;14. doi:10.3390/cells14070488
8. Greten FR, Grivennikov SI. Inflammation and cancer: triggers, mechanisms and consequences. Immunity. 2019;51(1):27–41. doi:10.1016/j.immuni.2019.06.025.Inflammation
9. Balkwill F, Mantovani A. Inflammation and cancer: back to virchow? Lancet. 2001;357(9255):539–545. doi:10.1016/S0140-6736(00)04046-0
10. Chen WH, Shao JJ, Yang Y, et al. Prognostic significance of systemic immune inflammatory index in NSCLC: a meta-analysis. Lung Cancer Manag. 2024:13. doi:10.2217/lmt-2023-0010
11. Ruan Y, Cao W, Han J, Yang A, Xu J, Zhang T. Impact of preoperative inflammatory biomarkers on postoperative pneumonia and one-month pulmonary imaging changes after surgery for non-small cell lung cancer. Front Oncol. 2025;15:1–14. doi:10.3389/fonc.2025.1489068
12. Ginesu GC, Paliogiannis P, Feo CF, et al. Inflammatory indexes as predictive biomarkers of postoperative complications in oncological thoracic surgery. Curr Oncol. 2022;29(5):3425–3432. doi:10.3390/curroncol29050276
13. Mazzella A, Maiolino E, Maisonneuve P, Loi M, Alifano M. Systemic inflammation and lung cancer: is it a real paradigm? Prognostic value of inflammatory indexes in patients with resected non-small-cell lung cancer. Cancers. 2023;16(1):15. doi:10.3390/cancers15061854
14. Mariean CR, Tiucă OM, Mariean A, et al. The impact of the histologic types of lung cancer on CBC-derived inflammatory markers—current knowledge and future perspectives. J Clin Med. 2025:14. doi:10.3390/jcm14093038
15. Hao B, Fan T, Xiong J, et al. The prognostic significance of the histological types in patients with nonsmall cell lung cancer ≤2 cm. Front Surg. 2021;8:1–9. doi:10.3389/fsurg.2021.721567
16. Zheng J, Zheng L, Wang X, et al. The clinical value of the combined detection of systemic immune-inflammation index (SII), systemic inflammation response index (SIRI), and prognostic nutritional Index (PNI) in early diagnosis of gastric cancer. J Inflamm Res. 2025;18:813–826. doi:10.2147/JIR.S496703
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Predictive Significance of Admission-Day Blood Routine-Derived Indices for 30-Day Mortality Risk in Elderly Patients with Bacterial Pneumonia
Huang X, Huang L, Zhao S, Yuan L, Wang X, Tang G, Yuan K, Xiao M
International Journal of General Medicine 2025, 18:1295-1309
Published Date: 5 March 2025
Prospective Evaluation of Postoperative SIRS and Serum Inflammatory Indices in Percutaneous Nephrolithotomy Patients
Arslantas YB, Sonmez G, Baydilli N, Bas U, Tosun H, Demirci D, Akinsal EC
Therapeutics and Clinical Risk Management 2026, 22:568497
Published Date: 15 January 2026