")
Back to Journals » Cancer Management and Research » Volume 11
Prospect of immunotherapy combined with anti-angiogenic agents in patients with advanced non-small cell lung cancer
Received 14 April 2019
Accepted for publication 24 July 2019
Published 15 August 2019 Volume 2019:11 Pages 7707—7719
DOI https://doi.org/10.2147/CMAR.S212238
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chien-Feng Li
Hongge Liang, Mengzhao Wang
Lung Cancer Center, Department of Respiratory Medicine, Peking Union Medical College Hospital, Beijing, 100730, People’s Republic of China
Abstract: In the latest years, some drugs have been approved by European Medicines Agency (EMA) and/or the US Food and Drug Administration (FDA) for the treatment of patients with advanced non-small cell lung cancer (NSCLC), particularly for the treatment of those who have no targeted gene mutations or who have progressed on previously targeted therapy or platinum-containing dual-agent chemotherapy. In general, these drugs fall into two categories: anti-angiogenic agents and immune checkpoint inhibitors (ICIs). Anti-angiogenic agents currently approved by the FDA and/or EMA for advanced NSCLC treatment include bevacizumab, nintedanib, and ramucirumab. Anlotinib has been approved in advanced NSCLC by Chinese Food and Drug Administration (CFDA). These anti-angiogenic agents can induce anti-angiogenesis by targeting vascular endothelial growth factor (VEGF)/VEGF2 or inhibiting multiple small molecules involved in angiogenic and proliferative pathways such as platelet-derived growth factor receptors (PDGFRs) and fibroblast growth factor receptors (FGFRs). Although these drugs show significant therapeutic efficacy, most patients inevitably experience disease progression resulting in death. ICIs approved by the FDA and/or EMA for advanced NSCLC treatment include nivolumab, pembrolizumab, and atezolizumab. These ICIs can significantly improve efficacy compared with standard chemotherapy by targeting programmed cell death protein 1 (PD-1) receptor or PD-2 receptor with longer response duration and acceptable toxicity. However, the response rate of ICIs is suboptimal, and only a few patients ultimately benefit from immunotherapy. So current efforts have focused on exploring new potential combinatorial strategies with synergistic antitumor activity. Here, we summarized the theoretical basis, current clinical data, and potential future perspective of immunotherapy combined with anti-angiogenic agents for advanced NSCLC.
Keywords: non-small cell lung cancer, immunotherapy, anti-angiogenic agents
Introduction
Lung cancer is the leading cause of cancer-related deaths worldwide. Non-small cell lung cancer (NSCLC) accounts for approximately 85% of all lung cancers. It is often diagnosed at a late stage and has a poor prognosis.1 The ability to induce angiogenesis is a key point in the development of cancer. The formation of new blood vessels can prevent tumors from being deprived of oxygen and nutrients, which is a typical feature of cancer cells.2–4 Hypoxia-driven vascular endothelial growth factor (VEGF) is a major regulator of angiogenesis, which can stimulate the proangiogenic signaling pathway by binding to the VEGF receptor 2 (VEGFR2).5–7 Various drugs targeting this pathway have been developed for advanced NSCLC. In general, there are two types: monoclonal antibodies (mAbs) targeting VEGF (bevacizumab) or VEGFR (ramucirumab) or small molecule tyrosine kinase inhibitor (TKI) inhibiting multiple angiogenesis and proliferative pathway (nintedanib and erlotinib). Table 1 summarizes the results of landmark phase III trial of antiangiogenic agents in NSCLC. Immunotherapy targeting the T cell immune checkpoint receptor programmed cell death protein (PD-1) or its ligand PD-L1 has been approved by US Food and Drug Administration (FDA)/European Medicines Agency (EMA) for the treatment of patients with advanced NSCLC.8–18 The homeostasis of the immune response was based on the physiologic balance between costimulatory and inhibitory molecules, which are present on antigen-presenting cells and tumor cells and can interact with specific receptors on immune cells.19 The PD-1 pathway is a T cell inhibition pathway induced by PD-1 receptor on the T cell membrane binding on PD-L1 on tumor cells. Tumor cells can control this pathway by up-regulating PD-L1 expression and preventing T cell-mediated tumor destruction. Thus, PD-1/PD-L1 antagonist antibodies can activate antitumor T cells and eventually kill tumor cells. Currently, a variety of PD-1/PD-L1 mAbs are approved for the treatment of advanced NSCLC, including nivolumab, pembrolizumab, and atezolizumab. Table 2 summarizes the results of landmark phase III trial of ICIs in NSCLC. Immunotherapy has an improved efficacy, longer duration of response, and controlled toxicity compared with standard chemotherapy and has become one of the major new treatment options for patients with advanced NSCLC. However, only a few patients can benefit from this treatment; this is related to the restriction of useful biomarkers and the complexity and dynamic nature of the tumor microenvironment (TME).13,20
Recently, the investigators are focused on the use of immunotherapy as a basic therapy in combination with other treatment strategies (such as radiotherapy, chemotherapy, and targeted drugs), which have been thought to increase tumor-related immunogenicity by inducing tumor cell death and new antigen release.21,22 Some evidence suggests that angiogenesis may be associated with immunosuppression in the TME, thereby enhancing the immune escape of tumor cells.23 In this review, we outline the current data, ongoing trials, and challenges of immunotherapy plus antiangiogenic agents for the treatment of patients with advanced NSCLC.
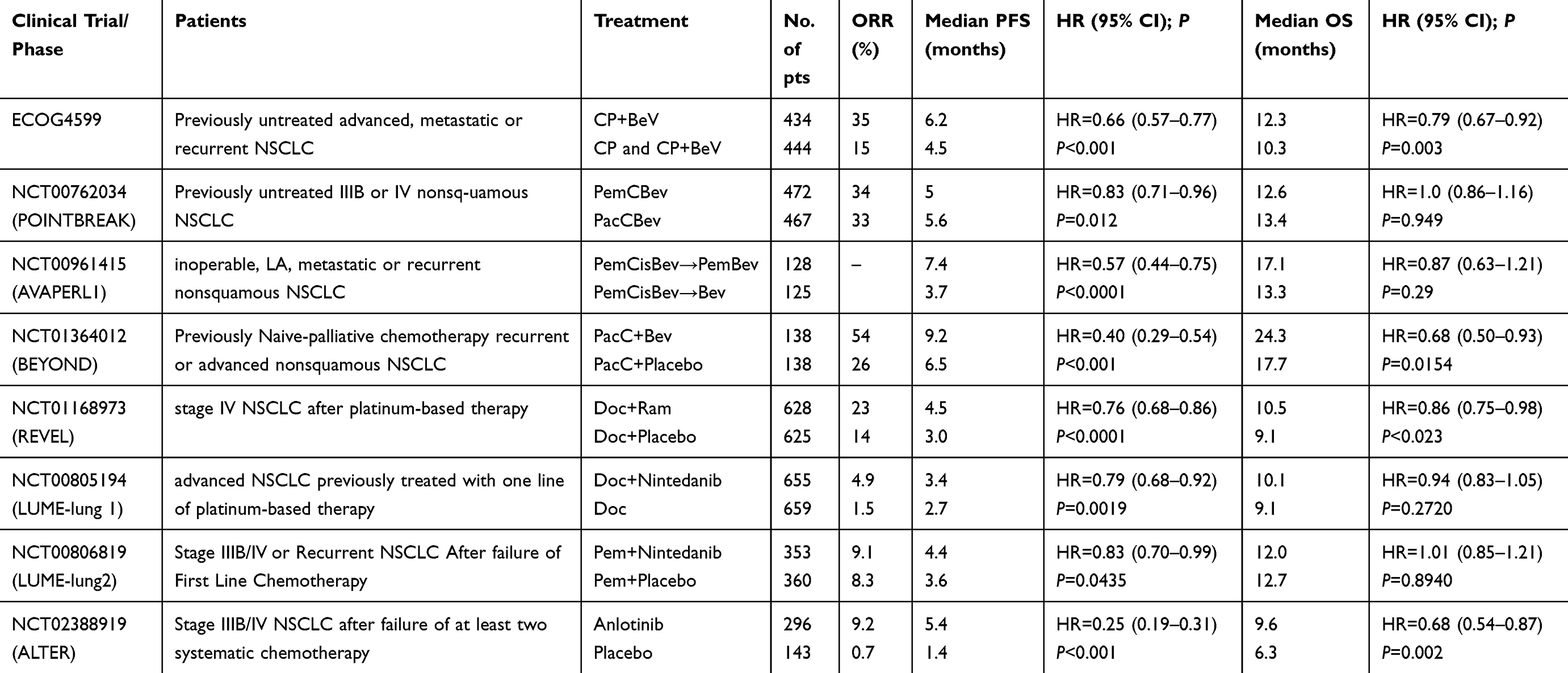 |
Table 1 Results of landmark phase III trials evaluating anti-angogenic agents in metastatic non-small-cell lung cancer |
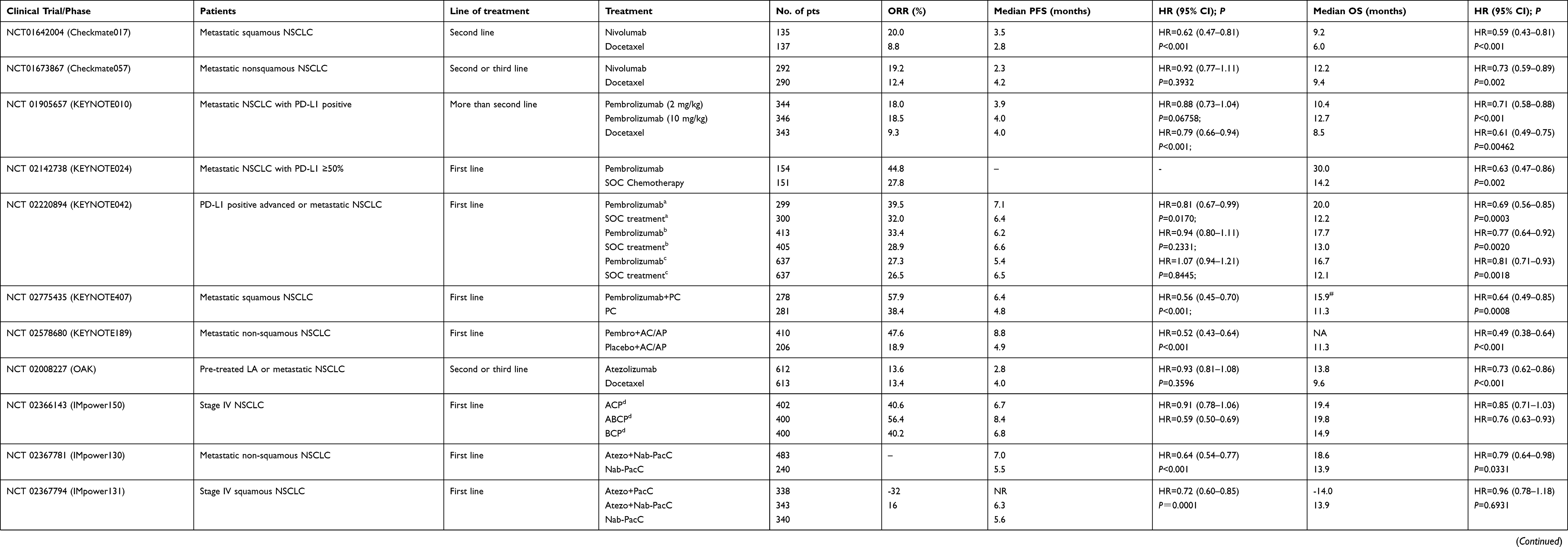 |
Table 2 Results of landmark phase III trials evaluating Immune Checkpoint Inhibitors in metastatic non-small-cell lung cancer |
Antiangiogenic agents
Bevacizumab
Bevacizumab is a fully humanized mAb and can block the interaction of VEGFR1 and VEGFR2, the major receptors involved in endothelial cell proliferation and migration, by binding to VEGF-A and prevents interactions with VEGFR1 and VEGFR2, which are the major receptors involved in endothelial cell proliferation and migration.24–27 Phase III clinical trials (ECOG 4599) evaluated the efficacy of bevacizumab (Bev) in combination with carboplatin (C) and paclitaxel (P) as first-line treatment in patients with metastatic or recurrent NSCLC. The results showed that, in comparison with CP chemotherapy alone, the Bev + CP group significantly prolonged the progression-free survival (PFS) (6.2 months vs 4.5 months; hazards ratio [HR] 0.66; P<0.001) and overall survival (OS) (12.3 months vs 10.3 months; HR 0.79; P=0.003).27,28 In 2006, the US Food and Drug Administration (FDA) approved bevacizumab for patients with unresectable, locally advanced, recurrent, or metastatic nonsquamous NSCLC. The POINTBREAK trial compared the efficacy and safety of pemetrexed (Pem) plus carboplatin (C) plus bevacizumab (Bev) followed by pemetrexed plus bevacizumab (PemCBev) in patients with advanced NSCLC. Results showed that, compared with paclitaxel (Pac) plus carboplatin (C) plus bevacizumab (Bev) followed by bevacizumab (PacBev), PemCBev had superior median PFS (6.0 months vs 5.6 months; P=0.012) but did not prove OS (12.6 months vs 13.4 months; P=0.949) advantage.29 The phase III AVAPERL trial evaluated the safety and efficacy of cisplatin plus pemetrexed plus bevacizumab followed by bevacizumab maintenance with or without pemetrexed in nonsquamous NSCLC. The results showed that patients allocated to BevPem maintenance had significantly improved PFS (7.4 months vs 3.7 months; HR 0.57; 95% confidence interval (CI) 0.44–0.75; P<0.0001), whereas OS did not benefit from double-agent maintenance (17.1 months vs 13.2 months; HR 0.87; 95% CI 0.63–1.21; P=0.29).30 The phaseⅢ BEYOND trial31 confirmed the efficacy of first-line bevacizumab plus carboplatin/paclitaxel (PacC) in Chinese patients with advanced or recurrent non-squamous NSCLC who have not received previous chemotherapy. It is reported that both PFS (9.2 months vs 6.5 months; HR, 0.40; 95% CI, 0.29–0.54; P<0.001) and OS (24.3 months vs 17.7 month; HR, 0.68; 95% CI 0.50–0.93; P=0.0154) was prolonged with PacC + Bev versus PacC + Placebo. In summary, in the advanced non-squamous NSCLC, bevacizuamb combined with CP can improve the therapeutic effect. Compared with paclitaxel, pemetrexed combined with platinum and bevacizumab did not demonstrate superior OS, and the combination with pemetrexed does not appear to improve the efficacy of bevacizumab maintenance therapy.
Ramucirumab
Ramucirumab is a human IgG1 mAb targeting VEGFR2. Phase III REVEL trial evaluated the efficacy and safety of docetaxel plus ramucirumab combination or docetaxel alone as a second-line treatment for patients with stage IV NSCLC. The results showed that the docetaxel plus ramucirumab combination slightly but statistically prolonged PFS (4.5 months vs 3.0 months; HR 0.76; 95% CI 0.68–0.86; P<0.0001) and OS (10.5 months vs 9.1 months; HR 0.86; 95% CI 0.75–0.98; P=0.023) compared with docetaxel alone. The treatment-related adverse event (AE) rate of the ramucirumab group and the control group was 98% (613/627) and 95% (594/618), respectively. There were no significant increase in thromboembolic events in the ramucirumab group, and hypertension and bleeding was generally mild.32 Based on this result, the FDA approved the use of ramucirumab in combination with docetaxel for patients with metastatic NSCLC with disease progression on or after platinum-based chemotherapy.
Nintedanib
Nintedanib is a triple vascular kinase inhibitor targeting VEGFR, platelet-derived growth factor receptor (PDGFR), and fibroblast growth factor receptor (FGFR). The phase III LUME-Lung 1 trial assessed the efficacy and safety of docetaxel plus nintedanib as a second-line therapy for patients with advanced NSCLC previously treated with one line of platinum-based therapy. Results showed that docetaxel plus nintedanib significantly improved PFS (median 3·4 months vs 2·7 months; HR 0.79; 95% CI 0.68–0.92; P=0·0019) compared with the docetaxel plus placebo group, whereas it did not demonstrate OS advantage (median 10·1 months vs 9·1 months; HR 0.94; 95% CI 0.83–1.05; P=0.2720). However, OS was statistically improved in patients with all adenocarcinoma histology NSCLC (median 12.6 months vs 10.3 months; HR 0·83; 95% CI 0.70–0.99; P=0.0359) and with adenocarcinoma histology that progressed within 9 months after the start of first-line treatment (median 10.9 months vs 7.9 months; HR 0.75; 95% CI 0.60–0.92; P=0.0073) in the docetaxel plus nintedanib group.33,34 Phase III LUME-Lung 2 trial investigated the efficacy and safety of nintedanib plus pemetrexed in patients with pretreated nonsquamous NSCLC. Results suggested that nintedanib plus pemetrexed significantly improved PFS over pemetrexed alone (median 4.4 months vs 3.6 months; HR 0.83; 95% CI 0.70–0.99; P=0.0435), but there was no OS difference between the two groups (median 12.0 months vs 12.7 months; HR 1.01; 95% CI 0.85–1.21; P=0.8940). The nintedanib plus pemetrexed group had a higher incidence of grade ≥3 elevated alanine aminotransferase, elevated aspartate aminotransferase, and diarrhea compared to the control group, but there was no difference in hypertension, bleeding, or thrombosis.35 Based on these results, Europe approved nintedanib for the second-line treatment of NSCLC.
Anlotinib
Anlotinib is a novel multitarget TKI targeting receptor tyrosine kinases VEGF receptors 1 to 3, epidermal growth factor receptor (EGFR), FGFR 1 to 4, PDGFR α and β, and stem cell factor receptor.36–38 Phase III ALTER 0303 trial evaluated the efficacy and safety of anlotinib in patients with advanced NSCLC. Results showed that anlotinib can significantly prolong the OS (9.6 months vs 6.3 months; HR 0.68; 95% CI 0.54–0.87; P=0.002) and PFS (5.4 months vs 1.4 months; HR 0.25; 95% CI 0.19–0.31; P<0.001) over placebo, and it is well tolerated.39 Based on these results, the CFDA approved anlotinib for the third-line treatment of advanced NSCLC.
Immune checkpoint inhibitors
Nivolumab
Nivolumab is a fully human IgG4 PD-1 ICI antibody that may restore antitumor immunity by affecting PD-1–mediated signaling.40–42 Checkmate 017 trial demonstrated that nivolumab statistically improved PFS (3.5 months vs 2.8 months; HR 0.62; 95% CI 0.47–0.81; P<0.001) and OS (9.2 months vs 6.0 months; HR 0.59; 95% CI 0.43–0.81; P<0.001) compared with doctaxel in previously treated advanced or metastatic squamous NSCLC.8 The checkmate 057 trial assessed the efficacy of nivolumab among patients with advanced nonsquamous NSCLC that had progressed during or after platinum-based chemotherapy, and the results suggested that OS was longer with nivolumab than with docetaxel (12.2 months vs 9.4 months; HR 0.73; 95% CI 0.59–0.89; P=0.002) despite its failure to demonstrate PFS advantage (2.3 months vs 4.2 months; HR 0.92; 95% CI 0.77–1.11; P=0.3932).9 Based on the data of these two trials, the FDA and EMA have approved nivolumab as subsequent therapy for patients with metastatic squamous/nonsquamous cell NSCLC. The checkmate 078 trial evaluated the efficacy and safety of nivolumab for treatment in previously treated advanced NSCLC in a predominantly East Asian population and demonstrated superior PFS (2.8 months vs 2.8 months; HR 0.77; 95% CI 0.62–0.95; P=0.0147) and OS (12.0 months vs 9.6 months; HR 0.68; 95% CI 0.52–0.90; P=0.0006) in the nivolumab group over the docetaxel group, which was consistent with checkmate 017 and checkmate 057 trials.11
Pembrolizumab
Pembrolizumab is a human IgG4 mAb against PD-1. Keynote 010 assessed the efficacy of pembrolizumab for patients with previously treated, PD-L1-positive, advanced NSCLC. The results showed that pembrolizumab 2 mg/kg significantly improved OS compared with docetaxel (10.4 months vs 8.5 months; HR 0.71; 95% CI 0.58–0.88; P=0.0008), although it did not demonstrate any PFS difference (3.9 months vs 4.0 months; HR 0.88; 95% CI 0.74–1.05; P=0.07). Pembrolizumab 10 mg/kg statistically improved both OS (12.7 months vs 8.5 months; HR 0.61; 95% CI 0.49–0.75; P<0.0001) and PFS (4.0 months vs 4.0 months; HR 0.79; 95% CI 0.66–0.94; P=0.004). Grades 3–5 treatment-related AEs were less common in the pembrolizumab group than in the control group.12 Keynote 024 found that in patients with advanced NSCLC with PD-L1 expression on at least 50% of tumor cells, pembrolizumab was associated with significantly longer PFS (10.3 months vs 6.0 months; HR 0.50; 95% CI 0.37–0.68; P<0.001) and longer OS (not reached in either group; HR 0.60; 95% CI 0.41–0.89; P=0.005) over platinum-based chemotherapy.13 Keynote 189 demonstrated that the addition of pembrolizumab to standard chemotherapy of pemetrexed and a platinum-based drug significantly prolonged PFS (8.8 months vs 4.9 months; HR 0.52; 95% CI 0.43–0.64; P<0.001) and OS (not reached vs 11.3 months; HR 0.49; 95% CI 0.38–0.64; P<0.001) over chemotherapy alone in patients with first-line treatment metastatic nonsquamous NSCLC without anaplastic lymphoma kinase (ALK) rearrangements or EGFR mutations.14 Keynote 407 assessed the efficacy of pembrolizumab plus chemotherapy with carboplatin plus paclitaxel or nab-paclitaxel in patients with previously untreated metastatic, squamous NSCLC. The results showed that patients in the pembrolizumab combination group had a superior PFS (6.4 months vs 4.8 months; HR 0.56; 95% CI 0.45–0.70; P<0.001) and OS (15.9 months vs 11.3 months; HR 0.64; 95% CI 0.49–0.85; P=0.0008) than chemotherapy alone.15 Keynote 04243 suggested that pembrolizumab monotherapy significantly prolonged OS in previously untreated locally advanced or metastatic patients with a PD-L1 tumor proportion score of 50% or greater (20.0 months vs 12.2 months; HR 0.69; 95% CI 0.56–0.85; P=0.0003), 20% or greater (17.7 months vs 13.0 months; HR 0.77; 95% CI 0.64–0.92; P=0.002), and 1% or greater (16.7 months vs 12.1 months; HR 0.81; 95% CI 0.71–0.93; P=0.0018). Based on the results of all these clinical trials, the FDA and EMA approved single-agent pembrolizumab as the first-line therapy for patients with advanced nonsquamous or squamous NSCLC and PD-L1 expression levels of 50% or more (based on keynote 024), approved pembrolizumab combined with a standard of chemotherapy as first-line therapy for patients with advanced nonsquamous or squamous NSCLC (based on keynote 189 and 407), and approved pembrolizumab as a subsequent therapy for patients with metastatic nonsquamous or squamous NSCLC and PD-L1 expression levels of 1% or more (based on Keynote 010).
Atezolizumab
Atezolizumab is a humanized antiprogrammed death-ligand 1 (PD-L1) mAb, reinvigorating anticancer immunity by inhibiting PD-L1 and PD-1 interactions. Phase III OAK trial assessed efficacy and safety of atezolizumab versus docetaxel in previously treated patients with metastatic NSCLC. The trial demonstrated that atezolizumab treatment significantly improved OS in comparison with docetaxel in previously treated NSCLC patients regardless of PD-L1 expression or histology and with acceptable toxicity (13.8 months vs 9.6 months; HR 0.73; 95% CI 0.62–0.87; P=0.0003).16 Based on the OAK trial result, the FDA and EMA approved atezolizumab as a subsequent therapy for patients with metastatic nonsquamous or squamous NSCLC. IMpower13044 showed a significant and clinically meaningful improvement in OS (18.6 months vs 13.9 months; HR 0.79; 95% CI 0.64–0.98; P=0.0331) and a significant improvement in PFS (7.0 months vs 5.5 months; HR 0.64; 95% CI 0.54–0.77; P<0.001) with atezolizumab plus nab-paclitaxel plus carboplatin versus nab-paclitaxel plus carboplatin as first-line treatment of patients with stage IV non-squamous non-small-cell lung cancer and no ALK or EGFR mutations. The interim analysis of the phase III IMpower13145 study showed that the combination of carboplatin plus nab-paclitaxel with atezolizumab improved PFS, compared to carboplatin plus nab-paclitaxel alone in treatment-naïve patients with advanced squamous NSCLC (6.3 months vs 5.6 months; HR 0.72; 95% CI 0.60–0.85; P=0.0001).
Basic theories and preclinical studies of immunotherapy plus antiangiogenic agents in NSCLC
There is increasing evidence that suggests that the TME is closely related to the development and progression of cancer, and the key strategy for targeting TME is to inhibit angiogenesis and stimulate an effective immune response.2,46,47 Tumors are characterized by poorly organized, vascular abnormalities with altered permeability. Angiogenesis is essential for primary tumor growth and has a complex relationship with the immune system.23,48–54 The process of angiogenesis is promoted and influenced by inflammatory mediators such as cytokines and immune cells, which, in turn, can affect the immune microenvironment.55 Antiangiogenic agents can stimulate the immune system, and immunotherapy can also be antiangiogenic.56 When these two types of therapies are combined, they can act synergistically on the tumor. The feasibility and preclinical evidence of immunotherapy combined with antiangiogenic agents are discussed in detail in the following paragraphs.
The immunosuppressive microenvironment enables tumor cells to evade immune surveillance, and VEGF is a key mediator of the immunosuppressive microenvironment.23 VEGF signaling can modulate the immune response by reducing tumor T cell infiltration and influencing systemic effects on immune regulatory cell function, thus reduce the antitumor response. The mechanism involves several key approaches. First, VEGF can induce the clustering defects at the endothelial cell surface by inhibiting the lymphocyte adhesion to activated endothelial cells, thereby inhibiting lymphocyte trafficking across endothelia to the tumor and blocking tumor infiltration of T cells.49,57 Second, VEGF can prevent T cell mobilization and T cell tumor infiltration by upregulating Fas ligand.53 Third, VEGF can effectively induce and proliferate suppressive immune cells, including suppressor immune cell subsets such as regulatory cells (Tregs) and myeloid-derived suppressor cells (MDSCs);50–52,57,58 inhibiting dendritic cell maturation23,51,52 and thymus differentiation, and/or T cell progenitor cells migrate from the thymus and eventually lead to systemic cancer-associated immunosuppressive status.51,54 Judicious dosing and administrative time of antiangiogenic agents can induce normalization of blood vessels by reducing the size and length of these abnormally dilated and tortuous vessels, decreasing hypoxia and vascular permeability, improving pericyte coverage, tumor perfusion, and blood flow, and promoting vessel maturation. This can decrease tumour interstitial fluid pressure, increase drug penetration in tumors,59,60 and synergize with immunotherapy and chemotherapy.61 The normalization of blood vessels is also dose-dependent. Liang J et al62 suggested intermittent application of low-dose anti-angiogenic inhibitor treatment may help improve the effect of chemotherapy by reducing hypoxia-related treatment resistance and improving drug delivery. In addition, the normalization of blood vessels can also improve the perfusion and oxygenation of TME, and then increase tumor infiltration of immune cells.63–65 In NSCLC, antivascular therapy can mediate tumor metabolic changes through the LKB1/AMPK pathway and induce recruitment of macrophages and other specific bone marrow cells, thereby promoting tumor angiogenesis and tumor progression. The effect of this metabolism on the immune microenvironment is one of the potential mechanisms of immunotherapy combined with antiangiogenic therapy.66–70 Some preclinical evidence also suggests that immunotherapy combined with antiangiogenic agents can potentially improve the efficacy of patients with advanced NSCLC.57,71–74 For example, in an in vivo lung adenocarcinoma model, immunotherapy combined with bevacizumab synergistically inhibits tumor growth.74 In the preclinical model of lung cancer, PD-L1 mAb combined with VEGFR2 small molecule inhibitor can significantly downregulate the expression of PD-1 and PD-L1, increase TILs, and inhibit tumor growth by reducing Tregs and MDSCs.75
Clinical trials of immunotherapy plus antiangiogenic agents in NSCLC
Based on the potential synergistic antitumor effects and preclinical evidence of immunotherapy combined with antiangiogenic drug therapy, several ongoing clinical trials are evaluating the efficacy and safety of this novel therapeutic combination in patients with NSCLC. Preliminary data suggest that this combination therapy is promising and well tolerated.76,77
Phase III IMpower150 study evaluated the safety and efficacy of atezolizumab plus bevacizumab plus chemotherapy as first-line treatment in patients with metastatic nonsquamous NSCLC. The patients were randomly assigned (1:1:1) to receive atezolizumab plus carboplatin plus paclitaxel (ACPac) (n=402), bevacizumab plus carboplatin plus paclitaxel (BevCPac) (n=400), or atezolizumab plus BCP (ABevCPac) (n=400) every 3 weeks for four or six cycles, followed by maintenance therapy with atezolizumab, bevacizumab, or both until disease progression or unacceptable toxic effects. Atezolizumab was administered at a dose of 1200 mg, bevacizumab at a dose of 15 mg/kg, paclitaxel at a dose of 200 mg/m2 (175 mg/m2 for Asian patients), and carboplatin at an area under the concentration−time curve of 6 mg/mL/min. The two primary end points were PFS and OS. The result showed that the ABevCPac group significantly improved PFS (8.4 months vs 6.8 months; HR 0.59; 95% CI 0.50–0.69) and OS (19.8 months vs 14.9 months; HR 0.76; 95% CI 0.63–0.93) compared with the BevCPac group in intention-to-treat population, regardless of PD-L1 expression status. The safety profile of ABevCPac was consistent with previously reported safety risks of the individual medicines.17,78
Rizvi et al evaluated the safety and efficacy of switching to nivolumab maintenance therapy, as monotherapy or combined with bevacizumab. Patients with advanced NSCLC who did not progress within 42 days of completing more than four cycles first-line platinum-based chemotherapy (± bevacizumab) were assigned to nivolumab 5 mg/kg intravenously every 3 weeks + bevacizumab 15 mg/kg intravenously every 3 weeks (nonsquamous patients; n=12) or nivolumab 3 mg/kg intravenously every 2 weeks (squamous patients [n=8], nonsquamous patients [n=13]) until progression or the occurrence of unmanageable toxicity. The results showed that median PFS of patients treated with nivolumab + bevacizumab was 37.1 weeks and that PFS of patients treated with nivolumab monotherapy was 16 weeks in squamous NSCLC and 21.4 weeks in nonsquamous NSCLC. Median OS was not reached with nivolumab (range 33.3, 86.7+ weeks) or nivolumab monotherapy (range 2.1+, 56.3+ weeks). Objective response rate (ORR) of patients treated with nivolumab + bevacizumab was 8% (1/12, ongoing) and was 10% (2/21) in patients treated with nivolumab only. Any grade treatment-related AE rate in the nivolumab + bevacizumab group and in the nivolumab group were 92% (11/12) and 62% (13/21), respectively. No treatment-related grade 4 AEs were reported; Grade 3 AEs included pneumonitis, cough, and tubulointerstitial nephritis with nivolumab + bevacizumab and pneumonitis and pleural effusion with nivoluamb. The toxicity was well tolerated.77
A phase Ia study evaluated the safety and tolerability of adding ramucirumab to pembrolizumab in patients with various solid tumors including those with previously treated advanced NSCLC (n=27). The results showed that the objective response rate was 30% (1 unconfirmed). Responses occurred in both histologic subtypes and all PD-L1 groups. The disease control rate was 85%. Median PFS was not reached (95% CI 3.98 to NR). Twenty-two patients (81%) experienced a treatment-related AE, and it was well tolerated.76 A single-center phase Ib study evaluated the tolerability, safety, and pharmacokinetics of nivolumab combined with different chemotherapy regimens in patients with advanced NSCLC, cohort C (6 patients) received a combination of nivolumab 10 mg/kg plus carboplatin target area under curve of 6.0 mg/mL/min plus paclitaxel 200 mg/m2 plus bevacizumab 15 mg/kg every 3 weeks up to six cycles, followed by nivolumab 10 mg/kg plus bevacizumab 15 mg/kg every 3 weeks. The results showed that all six patients achieved partial response and that median PFS was not reached. Dose-limiting toxicity, treatment-related deaths, and nonhematologic AEs of grade 3 or worse were not observed. Hematologic AEs of grade 3 or worse were 100%. Select AEs (those with a potential immunologic cause) of any grade were 100%, and AEs leading to discontinuation of chemotherapy were 33.3%.79
In general, the preliminary results showed an acceptable toxicity profile and encouraging antitumor activity of ICIs combined with antiangiogenic agents in patients with advanced NSCLC, but there are still many challenges to overcome in achieving combination therapy. Table 3 summarizes ongoing clinical trials evaluating antiangiogenic drug combination immunotherapy. We are excepting the further follow-up results.
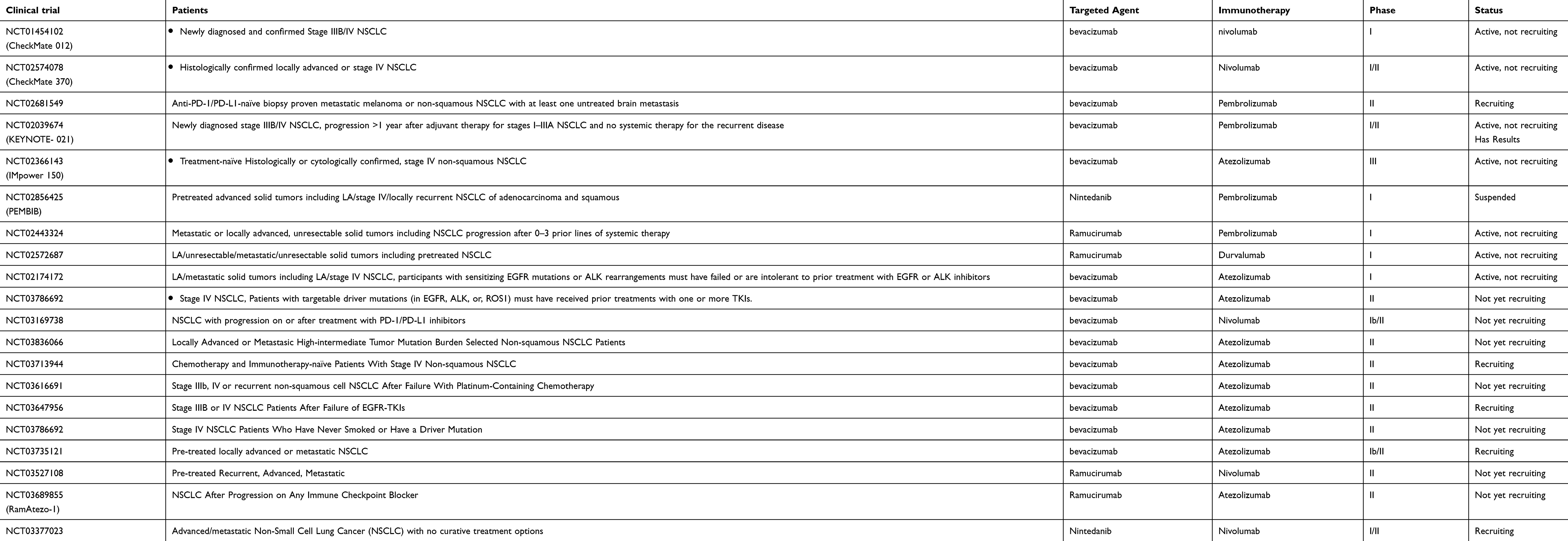 |
Table 3 Clinical trials of immune checkpoint inhibitors in combination with Antiangiogenic agents in advanced NSCLC |
Conclusion and future prospects
In this review, we reviewed the theoretical background and therapeutic potential of immunotherapy combined with antiangiogenic agents for the treatment of patients with advanced NSCLC, paying particular attention to potential treatment-related AEs resulting from combination therapy. However, our understanding of this new combination is just the tip of the iceberg, and many challenges remain to be addressed before it can be extended to clinical practice. More in-depth research is needed to explore which patients can benefit from this new combination, the optimal sequence and timing of immunotherapy in combination with anti-angiogenic agents, and the optimal dose for each drug.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. Ca-Cancer J Clin. 2017;67(1):7–30. doi:10.3322/caac.21387
2. Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144(5):646–674. doi:10.1016/j.cell.2011.02.013
3. Potente M, Gerhardt H, Carmeliet P. Basic and therapeutic aspects of angiogenesis. Cell. 2011;146(6):873–887. doi:10.1016/j.cell.2011.08.039
4. Martino EC, Misso G, Pastina P, et al. Immune-modulating effects of bevacizumab in metastatic non-small-cell lung cancer patients. Cell Death Discov. 2016;2:16025. doi:10.1038/cddiscovery.2016.9
5. Welti J, Loges S, Dimmeler S, Carmeliet P. Recent molecular discoveries in angiogenesis and antiangiogenic therapies in cancer. J Clin Invest. 2013;123(8):3190–3200. doi:10.1172/JCI70212
6. Ferrara N. VEGF-A: a critical regulator of blood vessel growth. Eur Cytokine Netw. 2009;20(4):158–163. doi:10.1684/ecn.2009.0170
7. Nagy JA, Dvorak AM, Dvorak HF. VEGF-A and the induction of pathological angiogenesis. Annu Rev Pathol-Mech. 2007;2:251–275. doi:10.1146/annurev.pathol.2.010506.134925
8. Spigel DR, Reckamp KL, Rizvi NA, et al. A phase III study (CheckMate 017) of nivolumab (NIVO; anti-programmed death-1 [PD-1]) vs docetaxel (DOC) in previously treated advanced or metastatic squamous (SQ) cell non-small cell lung cancer (NSCLC). J Clin Oncol. 2015;33:15. doi:10.1200/jco.2015.33.15_suppl.8009
9. Borghaei H, Paz-Ares L, Horn L, et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. New Engl J Med. 2015;373(17):1627–1639. doi:10.1056/NEJMoa1507643
10. Horn L, Spigel DR, Vokes EE, et al. Nivolumab versus docetaxel in previously treated patients with advanced non-small-cell lung cancer: two-year outcomes from two randomized, open-label, Phase III trials (CheckMate 017 and CheckMate 057). J Clin Oncol. 2017;35(35):3924–3933. doi:10.1200/JCO.2017.74.3062
11. Wu YL, Lu S, Cheng Y, et al. Nivolumab versus docetaxel in a predominantly Chinese patient population with previously treated advanced NSCLC: checkMate 078 randomized Phase III clinical trial. J Thorac Oncol. 2019;14:867–875. doi:10.1016/j.jtho.2019.01.006
12. Herbst RS, Baas P, Kim DW, et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): a randomised controlled trial. Lancet. 2016;387(10027):1540–1550. doi:10.1016/S0140-6736(15)01281-7
13. Reck M, Rodriguez-Abreu D, Robinson AG, et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N Engl J Med. 2016;375(19):1823–1833. doi:10.1056/NEJMoa1606774
14. Gandhi L, Rodriguez-Abreu D, Gadgeel S, et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N Engl J Med. 2018;378(22):2078–2092. doi:10.1056/NEJMoa1801005
15. Paz-Ares L, Luft A, Vicente D, et al. Pembrolizumab plus chemotherapy for squamous non-small-cell lung cancer. N Engl J Med. 2018;379(21):2040–2051. doi:10.1056/NEJMoa1810865
16. Rittmeyer A, Barlesi F, Waterkamp D, et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): a phase 3, open-label, multicentre randomised controlled trial. Lancet. 2017;389(10066):255–265. doi:10.1016/S0140-6736(16)32517-X
17. Socinski MA, Jotte RM, Cappuzzo F, et al. Atezolizumab for first-line treatment of metastatic nonsquamous NSCLC. N Engl J Med. 2018;378(24):2288–2301. doi:10.1056/NEJMoa1716948
18. Antonia SJ, Villegas A, Daniel D, et al. Overall survival with durvalumab after chemoradiotherapy in Stage III NSCLC. N Engl J Med. 2018;379(24):2342–2350. doi:10.1056/NEJMoa1809697
19. Rodriguez-Molinero A, Lopez-Dieguez M, Banegas JR. Tissue homeostasis and cancer. Med Hypotheses. 2007;68(6):1333–1341. doi:10.1016/j.mehy.2006.10.033
20. Brahmer J, Horn L, Jackman D, et al. Five-year follow-up from the CA209-003 study of nivolumab in previously treated advanced non-small cell lung cancer (NSCLC): clinical characteristics of long-term survivors. Cancer Res. 2017;77. doi:10.1158/1538-7445.Am2017-Ct077
21. Pilotto S, Molina-Vila MA, Karachaliou N, et al. Integrating the molecular background of targeted therapy and immunotherapy in lung cancer: a way to explore the impact of mutational landscape on tumor immunogenicity. Transl Lung Cancer Res. 2015;4(6):721–727. doi:10.3978/j.issn.2218-6751.2015.10.11
22. Tan WL, Jain A, Takano A, et al. Novel therapeutic targets on the horizon for lung cancer. Lancet Oncol. 2016;17(8):E347–E362. doi:10.1016/S1470-2045(16)30123-1
23. Ohm JE, Carbone DP. VEGF as a mediator of tumor-associated immunodeficiency. Immunol Res. 2001;23(2–3):263–272. doi:10.1385/IR:23:2-3:263
24. Carmeliet P, Jain RK. Angiogenesis in cancer and other diseases. Nature. 2000;407(6801):249–257. doi:10.1038/35025220
25. Kerbel R, Folkman J. Clinical translation of angiogenesis inhibitors. Nat Rev Cancer. 2002;2(10):727–739. doi:10.1038/nrc905
26. Willett CG, Boucher Y, Di Tomaso E, et al. Direct evidence that the VEGF-specific antibody bevacizumab has antivascular effects in human rectal cancer (vol 10, pg 145, 2004). Nat Med. 2004;10(6):649. doi:10.1038/nm0604-649c
27. Sandler A, Gray R, Perry MC, et al. Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancer. N Engl J Med. 2006;355(24):2542–2550. doi:10.1056/NEJMoa061884
28. Lopez-Chavez A, Young T, Fages S, et al. Bevacizumab maintenance in patients with advanced non-small-cell lung cancer, clinical patterns, and outcomes in the eastern cooperative oncology group 4599 study results of an exploratory analysis. J Thorac Oncol. 2012;7(11):1707–1712. doi:10.1097/JTO.0b013e318265b500
29. Patel JD, Socinski MA, Garon EB, et al. PointBreak: a randomized Phase III study of pemetrexed plus carboplatin and bevacizumab followed by maintenance pemetrexed and bevacizumab versus paclitaxel plus carboplatin and bevacizumab followed by maintenance bevacizumab in patients with Stage IIIB or IV nonsquamous non-small-cell lung cancer. J Clin Oncol. 2013;31(34):4349–U4377. doi:10.1200/JCO.2012.47.9626
30. Barlesi F, Scherpereel A, Gorbunova V, et al. Maintenance bevacizumab-pemetrexed after first-line cisplatin-pemetrexed-bevacizumab for advanced nonsquamous nonsmall-cell lung cancer: updated survival analysis of the AVAPERL (MO22089) randomized phase III trial. Ann Oncol. 2014;25(5):1044–1052. doi:10.1093/annonc/mdu098
31. Zhou C, Wu YL, Chen G, et al. BEYOND: a randomized, double-blind, placebo-controlled, multicenter, Phase III study of first-line carboplatin/paclitaxel plus bevacizumab or placebo in chinese patients with advanced or recurrent nonsquamous non-small-cell lung cancer. J Clin Oncol. 2015;33(19):2197–2204. doi:10.1200/JCO.2014.59.4424
32. Garon EB, Ciuleanu TE, Arrieta O, et al. Ramucirumab plus docetaxel versus placebo plus docetaxel for second-line treatment of stage IV non-small-cell lung cancer after disease progression on platinum-based therapy (REVEL): a multicentre, double-blind, randomised phase 3 trial. Lancet. 2014;384(9944):665–673. doi:10.1016/S0140-6736(14)60845-X
33. Gottfried M, Bennouna J, Bondarenko I, et al. Efficacy and safety of nintedanib plus docetaxel in patients with advanced lung adenocarcinoma: complementary and exploratory analyses of the Phase III LUME-Lung 1 study. Target Oncol. 2017;12(4):475–485. doi:10.1007/s11523-017-0517-2
34. Reck M, Kaiser R, Mellemgaard A, et al. Docetaxel plus nintedanib versus docetaxel plus placebo in patients with previously treated non-small-cell lung cancer (LUME-Lung 1): a phase 3, double-blind, randomised controlled trial. Lancet Oncol. 2014;15(2):143–155. doi:10.1016/S1470-2045(13)70586-2
35. Hanna NH, Kaiser R, Sullivan RN, et al. Nintedanib plus pemetrexed versus placebo plus pemetrexed in patients with relapsed or refractory, advanced non-small cell lung cancer (LUME-Lung 2): a randomized, double-blind, phase III trial. Lung Cancer. 2016;102:65–73. doi:10.1016/j.lungcan.2016.10.011
36. Sun YK, Niu W, Du F, et al. Safety, pharmacokinetics, and antitumor properties of anlotinib, an oral multi-target tyrosine kinase inhibitor, in patients with advanced refractory solid tumors. J Hematol Oncol. 2016;9. doi:10.1186/s13045-016-0332-8
37. Lin B, Song X, Yang D, Bai D, Yao Y, Lu N. Anlotinib inhibits angiogenesis via suppressing the activation of VEGFR2, PDGFRbeta and FGFR1. Gene. 2018;654:77–86. doi:10.1016/j.gene.2018.02.026
38. Taurin S, Yang CH, Reyes M, et al. Endometrial cancers harboring mutated fibroblast growth factor receptor 2 protein are successfully treated with a new small tyrosine kinase inhibitor in an orthotopic mouse model. Int J Gynecol Cancer. 2018;28(1):152–160. doi:10.1097/IGC.0000000000001129
39. Han B, Li K, Wang Q, et al. Effect of anlotinib as a third-line or further treatment on overall survival of patients with advanced non-small cell lung cancer: the ALTER 0303 Phase 3 randomized clinical trial. JAMA Oncol. 2018;4(11):1569–1575. doi:10.1001/jamaoncol.2018.3039
40. Brahmer JR, Drake CG, Wollner I, et al. Phase I study of single-agent anti-programmed death-1 (MDX-1106) in refractory solid tumors: safety, clinical activity, pharmacodynamics, and immunologic correlates. J Clin Oncol. 2010;28(19):3167–3175. doi:10.1200/JCO.2009.26.7609
41. Wang CY, Thudium KB, Han MH, et al. In vitro characterization of the Anti-PD-1 antibody nivolumab, BMS-936558, and in vivo toxicology in non-human primates. Cancer Immunol Res. 2014;2(9):846–856. doi:10.1158/2326-6066.CIR-14-0040
42. Topalian SL, Hodi FS, Brahmer JR, et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N Engl J Med. 2012;366(26):2443–2454. doi:10.1056/NEJMoa1200690
43. Mok TSK, Wu YL, Kudaba I, et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): a randomised, open-label, controlled, phase 3 trial. Lancet. 2019;393(10183):1819–1830. doi:10.1016/S0140-6736(18)32409-7
44. West H, McCleod M, Hussein M, et al. Atezolizumab in combination with carboplatin plus nab-paclitaxel chemotherapy compared with chemotherapy alone as first-line treatment for metastatic non-squamous non-small-cell lung cancer (IMpower130): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019. doi:10.1016/S1470-2045(19)30167-6
45. Jotte RM, Cappuzzo F, Vynnychenko I, et al. IMpower131: primary PFS and safety analysis of a randomized phase III study of atezolizumab plus carboplatin plus paclitaxel or nab-paclitaxel vs carboplatin plus nab-paclitaxel as 1L therapy in advanced squamous NSCLC. J Clin Oncol. 2018;36(18):2. doi:10.1200/JCO.2018.36.18_suppl.LBA9000
46. Hendry SA, Farnsworth RH, Solomon B, Achen MG, Stacker SA, Fox SB. The role of the tumor vasculature in the host immune response: implications for therapeutic strategies targeting the tumor microenvironment. Front Immunol. 2016;7. doi:10.3389/fimmu.2016.00621
47. de Palma M, Biziato D, Petrova TV. Microenvironmental regulation of tumour angiogenesis. Nat Rev Cancer. 2017;17(8):457–474. doi:10.1038/nrc.2017.51
48. Hall RD, Le TM, Haggstrom DE, Gentzler RD. Angiogenesis inhibition as a therapeutic strategy in non-small cell lung cancer (NSCLC). Transl Lung Cancer Res. 2015;4(5):515–523. doi:10.3978/j.issn.2218-6751.2015.06.09
49. Bouzin C, Brouet A, De Vriese J, DeWever J, Feron O. Effects of vascular endothelial growth factor on the lymphocyte-endothelium interactions: identification of caveolin-1 and nitric oxide as control points of endothelial cell anergy. J Immunol. 2007;178(3):1505–1511. doi:10.4049/jimmunol.178.3.1505
50. Finke JH, Rini B, Ireland J, et al. Sunitinib reverses Type-1 immune suppression and decreases T-regulatory cells in renal cell carcinoma patients. Clin Cancer Res. 2008;14(20):6674–6682. doi:10.1158/1078-0432.CCR-07-5212
51. Gabrilovich D, Ishida T, Oyama T, et al. Vascular endothelial growth factor inhibits the development of dendritic cells and dramatically affects the differentiation of multiple hematopoietic lineages in vivo. Blood. 1998;92(11):4150–4166.
52. Gabrilovich DI, Chen HL, Girgis KR, et al. Production of vascular endothelial growth factor by human tumors inhibits the functional maturation of dendritic cells (vol 2, pg 1096, 1996). Nat Med. 1996;2(11):1267. doi:10.1038/nm1096-1096
53. Motz GT, Santoro SP, Wang LP, et al. Tumor endothelium FasL establishes a selective immune barrier promoting tolerance in tumors. Nat Med. 2014;20(6):607–615. doi:10.1038/nm.3541
54. Ohm JE, Gabrilovich DI, Sempowski GD, et al. VEGF inhibits T-cell development and may contribute to tumor-induced immune suppression. Blood. 2003;101(12):4878–4886. doi:10.1182/blood-2002-07-1956
55. Nakamura K, Smyth MJ. Targeting cancer-related inflammation in the era of immunotherapy. Immunol Cell Biol. 2017;95(4):325–332. doi:10.1038/icb.2016.126
56. Garber K. Promising early results for immunotherapy-antiangiogenesis combination. J Natl Cancer Inst. 2014;106:11. doi:10.1093/jnci/dju061
57. Manegold C, Dingemans AMC, Gray JE, et al. The potential of combined immunotherapy and antiangiogenesis for the synergistic treatment of advanced NSCLC. J Thorac Oncol. 2017;12(2):194–207. doi:10.1016/j.jtho.2016.10.003
58. Terme M, Pernot S, Marcheteau E, et al. VEGFA-VEGFR pathway blockade inhibits tumor-induced regulatory T-cell proliferation in colorectal cancer. Cancer Res. 2013;73(2):539–549. doi:10.1158/0008-5472.CAN-12-2325
59. Tong RT, Boucher Y, Kozin SV, Winkler F, Hicklin DJ, Jain RK. Vascular normalization by vascular endothelial growth factor receptor 2 blockade induces a pressure gradient across the vasculature and improves drug penetration in tumors. Cancer Res. 2004;64(11):3731–3736. doi:10.1158/0008-5472.CAN-04-0074
60. Fukumura D, Jain RK. Tumor microvasculature and microenvironment: targets for anti-angiogenesis and normalization. Microvasc Res. 2007;74(2–3):72–84. doi:10.1016/j.mvr.2007.05.003
61. Wu JB, Tang YL, Liang XH. Targeting VEGF pathway to normalize the vasculature: an emerging insight in cancer therapy. Oncotargets Ther. 2018;11:6901–6909. doi:10.2147/OTT.S172042
62. Liang J, Cheng Q, Huang J, et al. Monitoring tumour microenvironment changes during anti-angiogenesis therapy using functional MRI. Angiogenesis. 2019;22:457–470. doi:10.1007/s10456-019-09670-4
63. Farsaci B, Higgins JP, Hodge JW. Consequence of dose scheduling of sunitinib on host immune response elements and vaccine combination therapy. Int J Cancer. 2012;130(8):1948–1959. doi:10.1002/ijc.26219
64. Farsaci B, Donahue RN, Coplin MA, et al. Immune consequences of decreasing tumor vasculature with antiangiogenic tyrosine kinase inhibitors in combination with therapeutic vaccines. Cancer Immunol Res. 2014;2(11):1090–1102. doi:10.1158/2326-6066.CIR-14-0076
65. Huang YH, Yuan JP, Righi E, et al. Vascular normalizing doses of antiangiogenic treatment reprogram the immunosuppressive tumor microenvironment and enhance immunotherapy. P Natl Acad Sci USA. 2012;109(43):17561–17566. doi:10.1073/pnas.1215397109
66. Bonanno L, De Paoli A, Zulato E, et al. LKB1 expression correlates with increased survival in patients with advanced non-small cell lung cancer treated with chemotherapy and bevacizumab. Clin Cancer Res. 2017;23(13):3316–3324. doi:10.1158/1078-0432.CCR-16-2410
67. Curtarello M, Zulato E, Nardo G, et al. VEGF-targeted therapy stably modulates the glycolytic phenotype of tumor cells. Cancer Res. 2015;75(1):120–133. doi:10.1158/0008-5472.CAN-13-2037
68. Nardo G, Favaro E, Curtarello M, et al. Glycolytic phenotype and AMP kinase modify the pathologic response of tumor xenografts to VEGF neutralization. Cancer Res. 2011;71(12):4214–4225. doi:10.1158/0008-5472.CAN-11-0242
69. Noy R, Pollard JW. Tumor-associated macrophages: from mechanisms to therapy (vol 41, pg 49, 2014). Immunity. 2014;41(5):866. doi:10.1016/j.immuni.2014.09.021
70. Zulato E, Curtarello M, Nardo G, Indraccolo S. Metabolic effects of anti-angiogenic therapy in tumors. Biochimie. 2012;94(4):925–931. doi:10.1016/j.biochi.2012.01.001
71. Kwilas AR, Ardiani A, Donahue RN, Aftab DT, Hodge JW. Dual effects of a targeted small-molecule inhibitor (cabozantinib) on immune-mediated killing of tumor cells and immune tumor microenvironment permissiveness when combined with a cancer vaccine. J Transl Med. 2014;12. doi:10.1186/s12967-014-0294-y
72. Li B, Lalani AS, Harding TC, et al. Vascular endothelial growth factor blockade reduces intratumoral regulatory T cells and enhances the efficacy of a GM-CSF - Secreting cancer immunotherapy. Clin Cancer Res. 2006;12(22):6808–6816. doi:10.1158/1078-0432.CCR-06-1558
73. Shi S, Wang R, Chen Y, Song H, Chen L, Huang G. Combining antiangiogenic therapy with adoptive cell immunotherapy exerts better antitumor effects in non-small cell lung cancer models. PLoS One. 2013;8(6):e65757. doi:10.1371/journal.pone.0065757
74. Tao LL, Huang GC, Shi SJ, Chen LB. Bevacizumab improves the antitumor efficacy of adoptive cytokine-induced killer cells therapy in non-small cell lung cancer models. Med Oncol. 2014;31:1. doi:10.1007/s12032-014-0374-0
75. Zhao S, Jiang T, Li X, Zhou C. Combining anti-angiogenesis and immunotherapy enhances antitumor effect in lung cancer. Ann Oncol. 2016;27:S288–S288.
76. Herbst RS, Bendell JC, Isambert N, et al. A phase 1 study of ramucirumab (R) plus pembrolizumab (P) in patients (pts) with advanced gastric or gastroesophageal junction (G/GEJ) adenocarcinoma, non-small cell lung cancer (NSCLC), or urothelial carcinoma (UC): Phase 1a results. J Clin Oncol. 2016;34:15. doi:10.1200/JCO.2016.34.15_suppl.3056
77. Rizvi NA, Antonia SJ, Shepherd FA, et al. Nivolumab (Anti-PD-1; BMS-936558, ONO-4538) maintenance as monotherapy or in combination with bevacizumab (BEV) for non-small cell lung cancer (NSCLC) previously treated with chemotherapy. Int J Radiat Oncol. 2014;90:S32–S32. doi:10.1016/j.ijrobp.2014.08.206
78. Reck M, Mok TSK, Nishio M, et al. Atezolizumab plus bevacizumab and chemotherapy in non-small-cell lung cancer (IMpower150): key subgroup analyses of patients with EGFR mutations or baseline liver metastases in a randomised, open-label phase 3 trial. Lancet Respir Med. 2019;7(5):387–401. doi:10.1016/S2213-2600(19)30084-0
79. Kanda S, Goto K, Shiraishi H, et al. Safety and efficacy of nivolumab and standard chemotherapy drug combination in patients with advanced non-small-cell lung cancer: a four arms Phase Ib study. Ann Oncol. 2016;27(12):2242–2250. doi:10.1093/annonc/mdw416
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.