")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Promoting Meaning and Recovery for Psychosis: Comparison of Metacognitively-Oriented Psychotherapists and Clinicians in Psychiatric Rehabilitation
Authors Faith L, Wiesepape C, Kukla M, Lysaker P
Received 15 March 2023
Accepted for publication 6 October 2023
Published 18 October 2023 Volume 2023:19 Pages 2179—2194
DOI https://doi.org/10.2147/NDT.S386004
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Laura Faith,1 Courtney Wiesepape,2 Marina Kukla,3,4 Paul Lysaker1,2, †
1Department of Psychiatry, Richard L Roudebush VA Medical Center, Indianapolis, IN, USA; 2Department of Psychiatry, Indiana University School of Medicine, Indianapolis, IN, USA; 3HSR&D Center for Health Information and Communication, Richard L Roudebush VA Medical Center, Indianapolis, IN, USA; 4Department of Psychology, Indiana University-Purdue University Indianapolis, Indianapolis, IN, USA
†Dr Paul Lysaker passed away on July 25, 2023
Correspondence: Laura Faith, Department of Psychiatry, Richard L Roudebush VA Medical Center, 1481 West 10th Street, Indianapolis, IN, 46202, USA, Tel +1-317-476-5708, Email [email protected]
Introduction: Recovery from psychosis is an expected and desired outcome in psychiatric rehabilitation that may involve subjective outcomes related to personal recovery. While a considerable amount of qualitative research has examined patients’ experience of recovery oriented approaches, there are less studies examining clinicians’ perspectives. Examining the clinician point of view is important for both supporting clinicians within recovery-oriented practice, as well as for understanding underlying therapeutic processes. The aims of this study were to explore clinician experience of offering different psychiatric rehabilitation treatments for individuals with psychosis, and to understand similarities and differences of clinicians whose work differed in its recovery emphasis.
Methods: Open-ended interviews were conducted with 10 psychotherapists providing Metacognitive Reflection and Insight Therapy (MERIT), a recovery oriented form of integrative psychotherapy focused on subjective aspects of recovery, and 10 clinicians providing standard psychiatric rehabilitation services.
Results: Thematic analysis revealed important similarities and differences between these two groups of providers. There were seven themes found for MERIT therapists: Comfort with uncertainty, Emphasis on collaboration, Being part of therapeutic change, Connecting with clients, Emphasis on patient autonomy, Experiencing growth, and Therapist use of self-awareness. There were four themes found for psychiatric rehabilitation clinicians: Value of a structured approach, Focus on a strengths-based approach, Witnessing behavioral change, and Building rapport to support the work.
Discussion: As expected, both similarities and differences arose between clinician groups. Results indicated that both groups focused on the therapeutic relationship and monitoring progress and outcomes. Unexpectedly, MERIT therapists reported growth as well as comfort with uncertainty. These findings suggest that MERIT is a a psychotherapy that offers unique opportunities for creative and flexible exploration of meaning and agency that is both challenging and rewarding for clinicians. Implications for supporting healthy clinician practice and the development of services are discussed.
Keywords: psychosis, recovery, psychotherapy, therapeutic alliance, qualitative, clinician experience
Introduction
It is now widely believed that people with psychosis can recover substantially, if not fully, over time.1,2 Recovery is understood to involve a range of highly individualized and subjective outcomes3 including symptom remission and skill acquisition, sometimes called functional recovery, as well as changes in persons’ subjective sense of self and their place within their communities, sometimes called personal recovery.4,5 To date, this has led to an increasing number of therapeutic approaches within psychiatric rehabilitation including cognitive behavioral therapy for psychosis (CBTp),6 social skills training,7 vocational rehabilitation,8 and supported housing9 each of which is supported by research documenting changes in patients’ behavior.
While patient perspective and experience of treatment is of tantamount importance to understanding the effects of psychiatric rehabilitation, the experience of clinicians as one half of a dyad is also of crucial importance in understanding the recovery process. In psychiatric rehabilitation, clinicians do not merely do interventions to patients. Instead, interventions are an active engagement between the therapist and patient, and happen within evolving interactions in which the dyad attempt to relate to one another, understand the patient’s psychosocial challenges, and respond to these challenges and opportunities.10 Further, beyond the delivery of any specific intervention, the quality of those clinician-patient interactions has been broadly accepted as a reliable predictor of outcome.11 Thus, to support the evolution of the practice of rehabilitation for persons diagnosed with psychosis, it is essential to know how clinicians perceive and respond to their experiences of those interactions.
Clinician Experience of the Process of Rehabilitation
Studies on clinician experience have broadly explored clinicians’ perspective on therapy process, outcomes, and how treatments affect the clinicians. So far, studies have focused on generalist clinicians with few studies that explore perspectives of clinicians who specialize in working with people with SMI or psychosis. To date, research on therapists’ experience of rehabilitation has largely revealed that therapist and patient experiences of process and outcomes are not identical.12 For example, Tzur Bitan and Abayed found that psychotherapists were more likely to experience a positive therapeutic alliance and believe that emotional processing is central to positive outcomes compared the experiences of patients and lay persons.13 Thus, it is important to understand the clinician’s unique perspective of interventions.
Much of the research highlights therapeutic alliance as it relates to outcomes and the process of treatment. Aligning with established quantitative research, qualitative research also shows that therapeutic alliance as an important mechanism of change14 and that meaningful relationships between clinicians, patients, and clinical teams are essential for positive outcomes.10 Other studies highlight clinicians’ report of the complexities of factors that might influence relationships between the therapeutic alliance, the treatment itself, and perception of outcomes. For example, clinicians reported that therapeutic alliance is stronger with a joint focus on patient autonomy and wellness15 and when the clinician has a recovery oriented or strength-based approach.16 Therapeutic alliance itself appears to affect treatment and outcomes, for example, stronger therapeutic alliance is related to higher levels of clinician optimism about patient recovery, a greater sense of personal growth,17 clinician flexibility, and opportunities to observe and respond to changes in patients’ mindsets.18
Other studies explored the clinician’s experience of treatment, for example their preferences or how it affects them personally. One study found that a recovery oriented or strengths-based approach had positive effects on professional and personal satisfaction for providers in community based rehabilitation settings.19 Regarding more specific treatment modalities, structured approaches were valued by mental health providers working with individuals with psychosis as giving them direction on specific therapeutic activities, however left them without direction when confronting more complex and deeply personalized issues recovering persons face.20 Similarly, in a more recent study with a relatively small sample, clinicians described their experience with emerging approaches to recovery as containing structured activities but not a clear conceptual rationale.21 By contrast, art therapy clinicians working valued a less structured approach as it enhanced abilities to relate to and sustain relationships with persons recovering from psychosis.22 Similarly, psychodynamically oriented psychotherapists valued a more unstructured process in which they experienced the idiopathic process of understanding each patient’s unique experience of psychosis and larger meanings in their lives to be essential for the recovery process.23 This is consistent with other work suggesting that less structured aspects of therapy, including play and humor may also deepen the therapeutic alliance and opportunities for personal growth.24 A recent study of therapist experiences of Mentalization-Based Therapy for borderline personality disorder found therapists valued the uncertainties exposed by this approach leading to growth for both themselves and their patients.25 In summary, structured approaches were found to be valued for their guidance, but lacked in discussing complexities or conceptualization, while unstructured approaches seemed to allow for more opportunities for therapeutic connection, growth, and meaning making.
The Concept of Recovery and the Current Study
Considered as a whole, clinicians providing psychiatric rehabilitation services frequently emphasize the therapeutic relationship as important, however other factors can vary substantially. Clinician experience further appears to be influenced by a range of potentially competing factors such as the degree of structure and the potential for flexibility that they perceive is allowed within their practice. However, for rehabilitation services for SMI and psychosis, it remains unclear to what degree differing properties of interventions affect clinician experience and perception of treatment and outcome.
One aspect of a given rehabilitation approach that may affect outcome as well as clinician experience is the emphasis on different aspects of recovery, for example objective vs subjective recovery.2 Multiple recovery oriented psychiatric rehabilitation approaches are anchored in objective measures of outcome and recovery, for example attainment of work, housing, or social skills.26 Other approaches emphasize more subjective outcome and recovery, including the development of a more coherent sense of self, agency, and meaning in one’s life.27 The latter approach may involve a more unstructured approach that allows for emergence of complex indicators of progress, while the former may emphasize a structured approach for targeted, objective outcomes. These differences in focus of recovery may be particularly relevant for clinician experience, as each approach could intuitively provoke different clinician responses.
To explore this issue, the current study sought to assess the experience of clinicians working in differing outpatient psychiatric rehabilitation programs with adults diagnosed with psychosis. We hope to add to the limited research assessing clinician perspective of approaches for individuals with SMI and psychosis. Specifically, the two groups included clinicians offering standard psychiatric rehabilitation programs that were more structured and focused on objective outcomes such as reducing distress or attaining improvements in work, housing, and social functioning and psychotherapists providing Metacognitive Reflection and Insight Therapy (MERIT).28 MERIT is an integrative form of individual psychotherapy that is unstructured and specifically developed to target subjective recovery including the development of a cohesive sense of oneself as an active agent in the world.29 In MERIT, intersubjectivity is emphasized to promote an evolving sense of oneself and one’s challenges and possibilities.30 A more detailed description of MERIT has been provided elsewhere29 and will be summarized further in the methods section. While both approaches aim to promote recovery, research suggests that a relational approach to psychosis may offer unique challenges and possibilities for clinicians and hence may have a different effect on clinician experience.30,31 Thus, the primary aim of this study was to explore the experience of clinicians offering psychiatric rehabilitation for adults diagnosed with psychosis to understand how different approaches emphases of recovery and approaches affect treatment and clinician experience. More specifically, we hope to advance the literature by evaluating similarities and differences as well as important elements of treatments with different recovery emphases.
Materials and Methods
Participants and Procedures
Participants were 20 staff or trainee clinicians providing clinical services to adults with psychosis. The primary inclusion criterion was experience of more than one year of providing mental health care as a frontline clinician. Participants were selected for their expertise working with individuals with psychosis from a range of backgrounds to investigate different approaches to psychiatric rehabilitation. The particular sample was a convenience sample of individuals working in programs serving individuals with serious mental illness (SMI), the majority of which had a primary psychotic disorder, in each of two settings, a Veterans Administration (VA) medical center and a community hospital in an urban setting. Participants were invited via verbal announcements in staff meetings or verbal communication. Participants consisted of 10 psychotherapists providing Metacognitive Reflection and Insight Therapy (MERIT)28 and 10 clinicians providing standard psychiatric rehabilitation services (PR-S). MERIT is an integrative, intersubjective therapy that consists of six foundational preconditions and eight elements that can be utilized by therapists to promote metacognition and subjective recovery. MERIT assumptions and elements are described in Table 1. Providers will be referred to as MERIT therapists and PR-S clinicians, respectively. All clinicians and therapists were Master’s level or higher. Trainee clinicians (at a Master’s level) operated under the supervision of a licensed clinician. Participants were asked to provide their self-identified clinician roles via interviews, see Table 2.
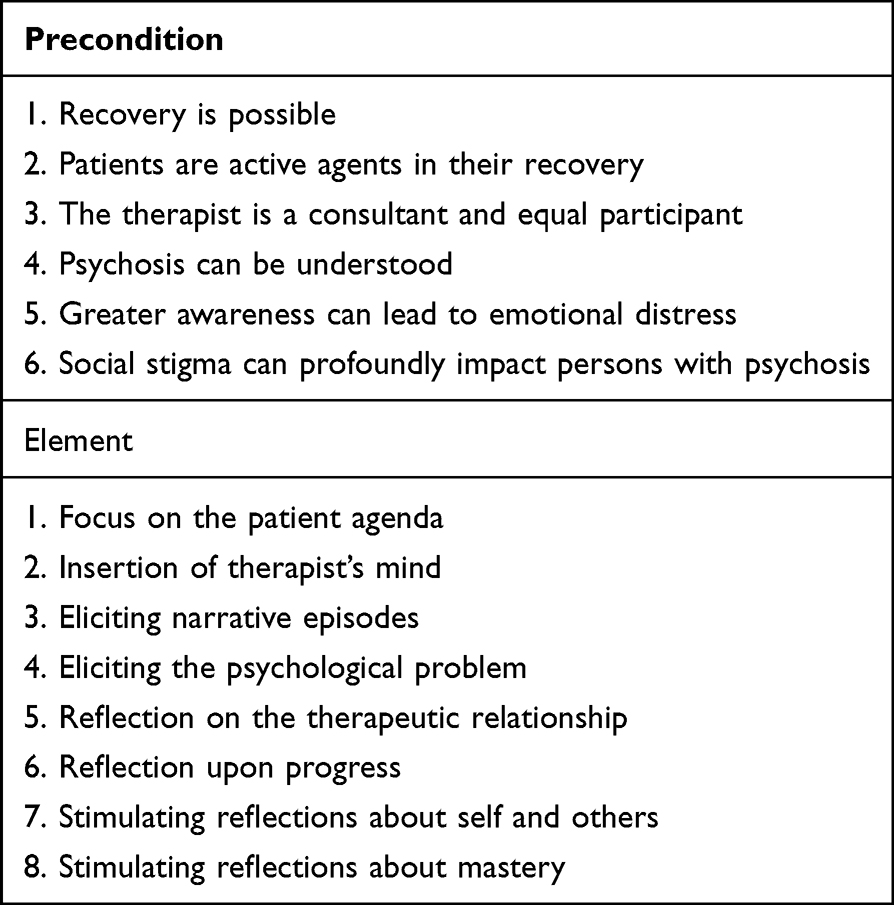 |
Table 1 MERIT Preconditions and Elements |
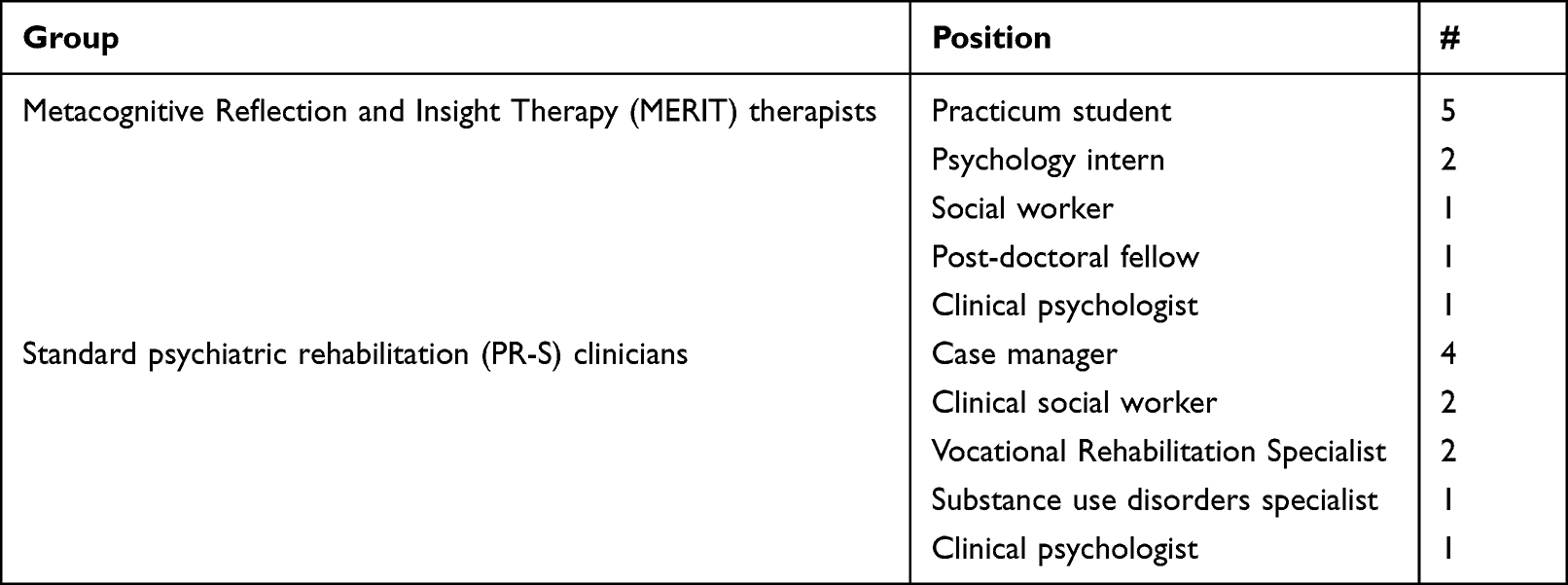 |
Table 2 Self-Identified Clinician Positions |
All participants were informed that this was a voluntary study, and if interested, completed written, informed consent, including publication of anonymized responses. Participants were then invited to engage in a qualitative interview. Interviews were conducted by MK and trained research staff. Participants were not paid. After interviews were completed, audio files were transcribed verbatim and de-identified (eg, all names, locations, and other identifiers were anonymized).
Measures
The current study uses a semi-structured interview that aims to understand therapists’ experiences of their clinical work. Interviews were designed from an empirically based framework32,33 by two of the authors (MK and PL) and purposefully sought to inquire about clincians’ experiences both of the recovery process within rehabilitation, as well as changes in their perspectives and personal experience over the course of rehabilitation. Interview questions are presented in Figure 1.
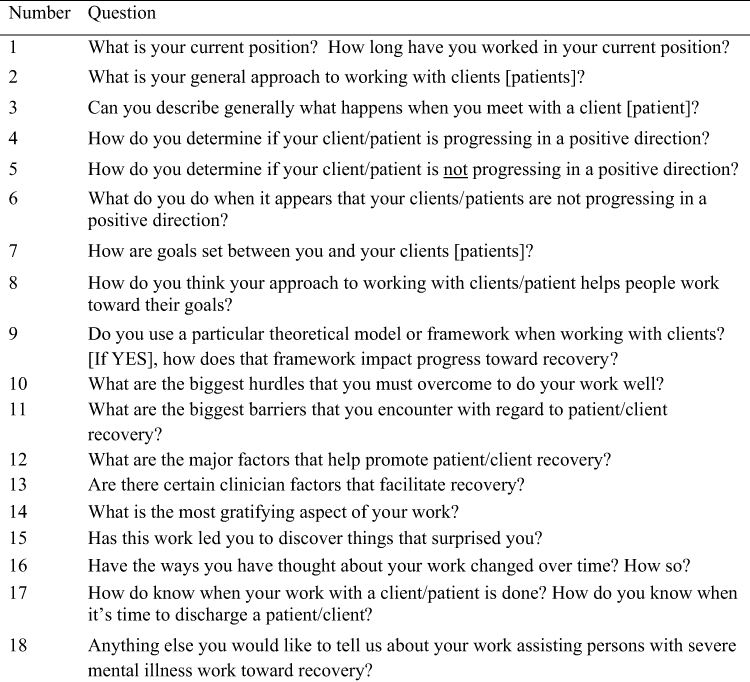 |
Figure 1 Clinician interview questions. |
Thematic Analysis
Qualitative analysis of interviews was conducted using thematic analysis adapted from Braun and Clarke.34 Two independent coders (LF and CW) analyzed the data through multiple phases of coding to find themes across interviews that was derived from the data based on saliency and frequency. This method included multiple iterations and meetings to discuss agreement and discrepancy to decrease bias and maximize validity of the codes and themes. Coding was focused on experiences of the therapist’s own approach to facilitate recovery. Frontline clinicians were coded as two separate groups.
To begin the analysis, coders first familiarized themselves with the data by thoroughly reading transcribed interviews. Initial coding of each interview was completed to summarize information. The coders next read through all completed content codes to generate ideas about possible themes. The coders then met to discuss initial codes and possible themes. Based on this discussion, a codebook was compiled including all possible themes. Next, each coder read through interviews again using the codebook for more focused coding. The coders then independently organized individual codes into themes that appear across interviews. Another group meeting occurred for coders to discuss discrepancies and resolve disagreement among codes and themes. Initial themes were then refined and organized into subthemes. The last phase consisted of reporting the content of each theme using narrative descriptions and participant quotes in the final report.
Results
Thematic analysis was completed for both groups (MERIT therapists and PR-S clinicians). Themes are described in detail below and summarized in Table 3.
MERIT Therapists
Thematic analysis revealed seven themes for MERIT therapists: Comfort with uncertainty, Emphasis on collaboration, Being part of therapeutic change, Connecting with clients, Emphasis on patient autonomy, Experiencing growth, and Therapist use of self-awareness.
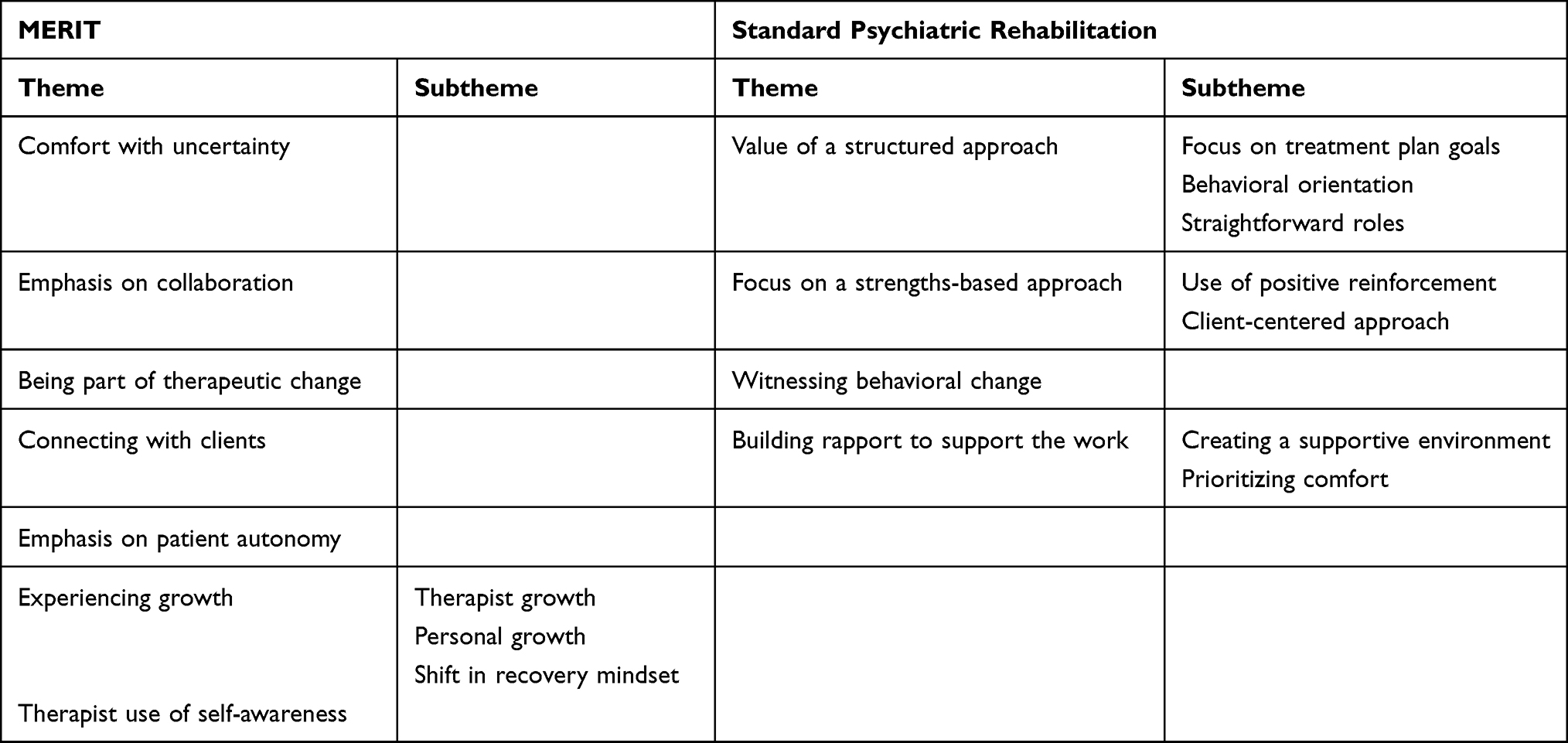 |
Table 3 Themes Generated from Clinician Interviews |
Theme 1. Comfort with Uncertainty
Therapists described the benefits of being comfortable with a certain level of uncertainty arising within sessions. This theme included uncertainty with the content of sessions, therapist’s own reactions, and process elements within sessions. One example from a therapist included a description of their own unexpected discomfort and accepting this as something that is expected and sometimes helpful in therapy to facilitate progress. They said,
I think also something that’s been surprising is kind of the importance of maybe being a little bit uncomfortable with some—when you’re talking about things and even in therapy and how some things can be more awkward but that’s kind of how progress is sometimes made whenever you’re in those uncomfortable situations.
Therapists commented on both content and process elements within sessions. One therapist described the fluid processing of emotions within sessions, and their ability to sit with whatever emotions naturally emerge in session. They said,
I think being able to really sit with someone and allow them to express what’s happening… being able to sit with pain…being able to sit there with them and not try to make it better or take it away or make them feel better about it. Just let them have that experience and sit there with that. The same thing with anger or any of those emotions--just allowing that to exist. I think sometimes we have these reactions where it’s like oh they’re in pain I need to say ‘it’s okay, it’ll be better, there are brighter days’.
A third therapist described the uncertainty of how content will arise and their approach to allowing the unfolding and uncovering of the person’s life in an organic way. They stated,
I think certainly when I start seeing someone I try to get a sense… of what their life history has been; what kind of problems that they’ve had and what things they want to look different in their life and I guess it kind of evolves over time.
Theme 2. Emphasis on Collaboration
Therapists described their active and ongoing collaboration with patients. Collaboration was described as an explicit element throughout therapy that involves thinking together with patients about their life and what they want differently from life. For example, one therapist described how they discuss collaborative therapy with patients:
This is not me deciding like ‘I’m the expert here. I can tell you to do this, this, and this and then you’re going to be better’. Instead ‘let’s talk about it together and let’s think together’ and I think that sets a good frame of therapy that’s again non-hierarchical.
Another therapist described how the emphasis on collaborative therapy is a joint, active process. They said,
I tend to take a non-directive approach and wanting to kind of communicate that it’s a process of us coming together and thinking about their life together rather than me just being completely passive or me giving them advice or that kind of thing.
A third therapist described how “thinking together” involves explicit and implicit messages from patients that are both important to consider. They said,
It’s not as rigid or as structured as ‘what are your goals today?’ but also thinking about not only what the client is telling you but… thinking about what they’re explicitly identifying as things they want different and also thinking about kind of the other messages they might be sending kind of through the way they’re acting or other thoughts that they have about their life.
Theme 3. Being Part of Therapeutic Change
Therapists described their experience being part of patient growth and progress. Therapeutic change differed across patients and involved various subjective outcomes, for example changes in cognitive processes or functional outcomes. One therapist described how a person’s thought processes may change by containing more content as opposed to being more barren. They said,
You need that patience [with this kind of therapy] and when you do see that change happen, it’s so rewarding. Something like having this huge change in thinking and this person has said that his mind feels blank for so long, but now he’s able to think like ‘my mind feels cloudy’ or ‘my mind feels full’ like that is a huge difference right there… a pivotal point in therapy.
Another therapist spoke about one patient who achieved higher levels of metacognition despite others believing they would not get better. They said,
It’s really rewarding seeing people achieve higher levels of metacognition …one of the clients that I’ve been working with for years now. This client has been viewed by other people as a throw away person [as if] there’s really no hope that things can get better but…here we are [in therapy] and this person is making sense of their experiences and piecing things together, so I think seeing that [type of] progress can be really rewarding.
A third therapist described how changes in thinking translated to functioning. Specifically, they noticed how a patient was able to understand themselves and their life better and used this metacognitive knowledge to improve their relationships and quality of life. They said,
I really like seeing people change and seeing them open up, helping them connect different points together, helping them have more of a life and more of those things together. I think that some of the people I started working with…from the first day that I met them to now, it’s amazing how different they are and how much I know about them and what their experiences have been and how they view some of those experiences and upcoming ones, and life, and seeing how much of them has opened [up] and how they start connecting with others…seeing that their life is different and…they enjoy [their life]…where they feel a sense of calm or peace…
Theme 4. Connecting with Clients
An essential element of MERIT therapists’ work was connecting with patients. Therapists described this connection as a very rewarding part of therapy and something that affected them as a person. One therapist described this connection as the most rewarding part of therapy. They said
Getting to truly know people, that’s what I find really rewarding and developing these really rich relationships with the people that I work with.
Another therapist described the impact patients have had on them, being able to witness resiliency and understand each person’s journey. They said,
I think it’s an absolute privilege to get to know people’s stories. I think too sometimes it’s really hard to see how much people suffer, but I think I’m always reminded of in those moments where I feel kind of overwhelmed by that is the resiliency that people show that a lot of the people that I see have suffered an immense amount and have been through all kinds of things that are just heartbreaking, but they continue to find ways to make a life that matters to them and to see them doing things again and getting back to life—that really is fulfilling. So not just seeing people recover, but also really getting to know them as humans and getting to really see what their journey has been, the ups and the downs.
Another therapist reflected on the relational importance of viewing people with severe mental illnesses as the same as themselves, despite stigma that exists in society. They stated,
I think many people with severe mental illness, because there’s a lot of stigma out there and because of some of the historical perspectives on people with severe mental illness, are treated very poorly but when you get to know them and when you actually take the time to sit with them, they’re normal people. A lot of people don’t take the time to do that, so I think I really find a lot of value in just trying to connect with them and trying to kind of sit with them and talk with them and figure out what they want to do with their life and figure out kind of where they’re coming from.
Theme 5. Emphasis on Patient Autonomy
MERIT therapists discussed their emphasis on patient autonomy or agency as a mechanism for persons to better understand themselves and to improve quality of life. One therapist described how this emphasis allows patients to self-direct their own life and therefore create more meaningful goals than ones that are prescribed. They said,
Well I think…by really focusing on what [the patient’s] true desires are or what they really want from life or treatment it actually sets them up for more success because it’s something that’s meaningful to them and it’s something that’s rooted in the context of their lives and by that alone I think it’s more attainable than something I’m prescribing or something I’m putting on them. I think it’s more like organic and I think it also helps develop the sense of agency too.
Another therapist further described how emphasizing autonomy can encourage individuals to set attainable goals. They said,
I think agency, so the person’s ability to make decisions and choices for themselves, knowing that they are an active agent in their world and that they can do that. The capacity to do it—I think sometimes people understand someone’s capacity so they think ‘okay well this is it, they’re not going to get past this’ but allowing that person to kind of meet or figure that out. I know that everyone can’t be the top…that’s not possible, but someone can be more capable than they thought they were or someone else thought they were, but it’s about going out and trying it.
A third therapist described how patient autonomy fits within the metacognitive model of treatment. They said,
I think [the metacognitive model]…[on] a large scale view that it really helps people to do things like recover a sense of agency, to really reflect on who they are as a person, as a human with a storied past and to figure out what that end means for their future and take understandings of themselves from the past and use that to kind of master current and future situations and then I think on more of a more micro level I guess I think it really helps people to know their own mind better.
Theme 6. Experiencing Growth
MERIT therapists described personal or professional growth throughout their work with patients. Growth fit into one of three subthemes (described below): therapist growth, personal growth, and shift in recovery mindset.
Subthemes
Subtheme 1. Therapist Growth
Several therapists described professional growth that they developed by gaining experience as a MERIT therapist. For example, some described their improved ability to conceptualize their clients, while others discussed improvements in active therapeutic engagement. One therapist reflected on their improved ability to take more therapeutic risks with patients. They said,
I think I gave myself more permission to make mistakes or to not know or to go out on a limb and try something even though I’m not sure it’s the right thing to do and then to be really reflective about that afterwards and try to understand…why it worked or why it didn’t.
Another therapist noticed their ability to challenge their naturally passive communication style to a more direct communication style as it was more beneficial to the patient. They said,
I think one thing for me is just personality wise I’m not a very direct person and I think this type of work demands—not demands but requires you to be somewhat direct and not essentially confrontational, but being able to address hard personal issues that are happening in the room.
A third MERIT therapist described how their view of themselves as a capable therapist has changed over time through consultation with other MERIT therapists. They said,
I think before I constantly felt like everyone is an expert and I’m always learning, but now I see it as, you know, I’m learning and so are [the other MERIT therapists] and so it’s not like everything that I do is wrong, or I’m never going to be this, and this person is so wonderful; there’s never going to be this idea that everyone else is an expert like we’re all learners together… to be able to have those conversations [in consultation] and be able to say ‘okay this is what I’m struggling with’ and hearing that back and forth that they’ve struggled with [therapy] or how they would approach. [therapy]
Subtheme 2. Personal Growth
Therapists described growth as a person outside the therapy room, for example changes in their understanding of themselves, other people, or the world. One person said,
I never expected…to feel transformed myself personally…I think that’s a kind of growth that’s separate from growing as a clinician. I feel like even though my understanding of humanity was very rich before; that it’s grown even more now…that was something that was unexpected for me but in a good way.
Another therapist described their own increased self-reflection as a result of their interactions with patients. They said,
The most surprising thing for me has been when you work with someone … and you think about their lives … some of these things make me reflect and think about some [personal] stuff and that’s really surprised me at certain times where it was like ‘wow how am I even here, why am I even thinking about that or how is that affecting me or touching me … like [it’s] my own’.… before I thought, ‘okay I’m decent on self-reflection’, but apparently there’s always room to grow.
Subtheme 3. Shift in Recovery Mindset
MERIT therapists described growth in their understanding of “recovery” as a result of using the metacognitive model with patients. For example, one therapist described how MERIT supports recovery by promoting sense of self. They said,
I think in general in some ways the metacognitive model is more meaningful [as a therapeutic approach] in terms of promoting recovery because it helps them to really kind of develop a meaningful representation of themselves and kind of integrate these past life narratives into this meaningful sense of self.
Another therapist described how learning MERIT changed their own view of recovery to mean a range of possibilities, for instance living with symptoms rather than expecting them to fully remit. They said,
Before I started to do this kind of work I think recovery looked a lot different to me like I assumed that recovery meant…full remission like you’re never going to see any kind of like psychotic symptoms again or no drinking or alcohol use or anything like that and now I see symptom remission and goal setting a lot differently. I see it as something about okay maybe if it’s you can’t get rid of these things then you can find a way that you can make sense of them and that will bring a certain level of relief as well too.
Theme 7. Therapist Use of Self-Awareness
MERIT therapists described the importance of ongoing self-awareness in the therapy room. For example, one therapist described their ability to use their in-the-moment reactions during therapy as a tool. They said,
[This approach has] an emphasis on really being aware of your reactions to a client or again kind of what you’re being pulled —what a client is pulling you to say or how they’re pulling you to act so I think with me that’s been something that I’ve been working on is being more aware of myself in session and using myself as a tool to measure interpersonal interactions [the patient] has with other people and how other people might see them or feel compelled to act.
Another therapist described their awareness of themselves as an integral part of the intersubjective element of therapy, and any potential changes that can be made, when patients are not progressing. They said,
[When a patient is not progressing] my first instinct …would be thinking about what I’m doing that’s not being helpful because I think with taking an integrative approach, focusing on some metacognitive deficits, it’s an approach where I should be able to meet the person where they’re at and help them scaffold to the next progression in [metacognitive] development…so I think if someone is not progressing to me that would indicate that there’s probably something I could do better.
Standard Psychiatric Rehabilitation Clinicians
There were four themes found for PR-S clinicians: Value of a structured approach, Focus on a strengths-based approach, Witnessing behavioral change, and Building rapport to support the work.
Theme 1. Value of a Structured Approach
PR-S clinicians described their emphasis of structured approaches with their patients. The use of structured approaches fit within three subthemes: focus on treatment plan goals, behavioral orientation, and straightforward roles.
Subthemes
Subtheme 1. Focus on Treatment Plan Goals
Clinicians described how their practice and monitoring goals is tied to the treatment plan. For example, one clinician stated,
We continually reference back to that treatment plan and that helps us to see… if there’s any progress towards their goals that they’ve established…
Several clinicians described the time they spend creating treatment plans, referencing back to this plan, and using the plan as a tool in their program.
Subtheme 2. Behavioral Orientation
Clinicians described their focus on behavioral methods and outcomes throughout the treatment process. One clinician described how they track engagement to determine if the patient is interested and progressing. They said,
We have specific tasks to complete which are workshops for them to attend and…follow up appointments and so if they are attending those we feel like they’re showing interest in the program and if they’re attending their appointments we monitor that.
Several clinicians specifically mentioned utilizing established behavioral approaches, for example motivational interviewing or cognitive behavioral therapy. One clinician said,
I draw from a lot of different things. We don’t do therapy necessarily…I’ll do skill training and motivational interviewing. We do CBT [cognitive behavioral therapy]. We do DBT [dialectical behavior therapy] stuff, we do a lot of supportive listening and processing so it depends on the situation…It’s just kind of pulled from everything.
Another clinician reflected on his behavioral preference because it has a clear timeline and concrete, attainable goals. They said,
I think that’s why I’m drawn to case management just because there are more tangible goals to achieve here. Sometimes in therapy it does seem like it’s kind of limitless, at least in my experience…for me obviously when I’ve got somebody who’s living in a shelter and then 3 months later they’ve got their own place that’s really to me quite satisfying to see.
Subtheme 3. Straightforward Roles
Clinicians described clearly defined roles in their programs, which are at times “directive” to assist with behavioral goals. For example, one clinician described the necessity to be directive with clients who are sometimes directionless. They said,
I am kind of directive…sometimes I have to be ‘cause of [the client’s] ability to establish goals has been diminished. They just…want immediate gratification sometimes and it’s real difficult for them to develop planning for the future so sometimes with suggestions we talk about cutting down, stopping using, finding support systems for abstinence, reconnecting with family or leisure time activities or whatever things that they’ve lost in the past; help them reconnect to those.
Another clinician described their clearly defined role to help persons obtain housing. They said,
It’s a lot focused on housing…until we actually get them in the [program sponsored] apartment, we don’t focus on a lot of other things because we’re a housing first program so traditionally we’re not going to do too much outside of getting them housed.
Theme 2. Focus on a Strengths-Based Approach
PR-S clinicians described their approach as “strengths-based”. This often meant creating an encouraging environment focused on what the patient can do rather than what they cannot do. There were two subthemes: use of positive reinforcement and client-centered approach.
Subthemes
Subtheme 1. Use of Positive Reinforcement
PR-S clinicians described creating an environment of positivity and encouragement using positive reinforcement. For example, one clinician said,
Of course [I utilize] the strengths approach and definitely [using] positive reinforcement…I’m very task oriented and making sure that you’re always giving that positive feedback and [telling them] how well they’re doing and how great they’re doing, getting through this part of the program quickly and what they’ve learned and just constantly giving them positive feedback about the successes that they do have.
Another clinician described their emphasis on encouragement. They stated,
I try to…use a variety of encouragements. I try not to use any type of negative reinforcement whatsoever.
Subtheme 2. Client-Centered Approach
Part of a strengths-based approach for PR-S clinicians was the creation of a client-centered environment. One clinician described how this translates to treatment plan development:
[In developing the treatment plan] I ask more specific questions about ‘when do you want to have this done by’ or ‘what do you think the main problem is’…[the treatment plan is] very valuable because you know not [sic] what I would like to have them do, but what they’re wanting to do, so I really want them to be in charge of that and I help support them ‘cause I don’t want to… have a bunch of goals that I would like for them because I don’t think we would get as far with it.
Another clinician described how treatment is primarily led by the patient themselves rather than the clinician dictating their treatment goals. They said,
We actually want the information from the veteran, what their choice might be and ask them [directly].
Theme 3. Witnessing Behavioral Change
PR-S clinicians described witnessing behavioral changes for patients throughout treatment. One clinician described how rewarding it has been to see patients move from being in restrictive environments to living in the community. They said,
[It has been rewarding to see] some of the outstanding progress that’s been made with some of our folks. Some of our veterans have come from being arrested or hospitalized on a biweekly basis and, for instance there’s one that I’m thinking of right now who has not been hospitalized or arrested for 4 years so that’s pretty good.
Another clinician described the investment in their patients reaching goals. They said,
When they let you know that they achieved their end goal of employment or just even overcome any small goal…I’m not just doing my job; I really care about their success.
Another clinician described how the program determines discharge based on behavioral markers of progress. They said,
Basically if they’re at the point where they’re attending all of their appointments, they’re getting all of their paperwork done, they’re paying their rent, they’re paying their bills and they know when to ask for help. They know when to reach out and are able to do that then typically we’ll discharge with the voucher.
Theme 4. Building Rapport to Support the Work
PR-S clinicians described building rapport with their clients throughout treatment. There were two subthemes: Creating a supportive atmosphere and Prioritizing comfort.
Subthemes
Subtheme 1. Creating a Supportive Atmosphere
PR-S clinicians described how a supportive atmosphere contributes to the relationship. One clinician described how their own availability makes an impact on trust. They said,
One of the things I really try to do is be available…A lot of our clients have high needs and so when they reach out to us either with a message or walking in, I try to get back to them within the same day…I feel like that helps them know that I’m here for them so that they feel like they can trust me and that I’ll be there if they need me.
Another clinican described how assistance with housing demonstrated tangible support or evidence that they are “on their side”. They said,
[Patients have] been disconnected in so many ways that they see it as really positive to have somebody who’s quote unquote on their side and giving people housing is pretty straightforward and if you stick with the bureaucracy long enough, you’re going to get them housing.
A third clinician described how their own demeanor contributes to the supportive environment. They said,
I think that having support is very important and knowing that someone cares is important and so…I tend to remain pretty consistent with them. I don’t get angry …I’m just pretty consistent and more direct and very honest and I think that me remaining a consistent factor in their life is helpful a lot of times.
Subtheme 2. Prioritizing Comfort
PR-S clinicians described the value of having a comfortable environment to support the relationship. One clinician described their approach beginning therapy with a patient,
Generally the main goal for me when I first meet with a client is try to establish rapport and get an understanding of why they’re there, why they’ve come, what they need help with and help them get comfortable ‘cause a lot of times they’ve never been in therapy and get comfortable just being in the room, you know, with somebody.
A second clinician described their approach to respond to distress with comfort. They said,
A lot of people have paranoia or they’ve even had bad previous treatment experiences, so I try to be very warm and inviting and then build up a relationship before getting in too deep with detail or emotions.
Discussion
The current study aimed to examine interviews from therapists offering Metacognitive Reflection and Insight Therapy (MERIT) and clinicians offering standard psychiatric rehabilitation services (PR-S) to further understand the experience of clinicians offering a range of psychiatric rehabilitation services to individuals with psychosis that vary in their recovery emphasis. Generally, findings aligned with the goals of each approach, for instance MERIT therapists described an interpersonal therapy that emphasized the therapeutic relationship and subjective goals, while PR-S clinicians described a goal-oriented treatment that emphasized patient strengths. There were some unexpected findings in the MERIT therapist group that will be discussed further below (ie, Comfort with uncertainty and Experiencing growth themes).
Regarding similarities between the two groups of clinicians, not surprisingly we found that both groups focused on the therapeutic relationship and monitoring progress. Therapeutic alliance has long been recognized as an important element of recovery-oriented care for persons with psychosis, is associated with recovery outcomes,11,35,36 and is recognized by clinicians from qualitative interviews as an important element of psychiatric rehabilitation.13,14,23 Although the groups both valued the relationship, they were described differently. PR-S clinicians valued a comfortable, supportive relationship with clear roles. MERIT therapists, conversely, described a relationship that was non-hierarchical, evolved with time, and emphasized subjective goals that supported patient autonomy. Progress monitoring was a focus among both groups, however, it was also described differently. PR-S clinicians’ approaches were more structured and focused on behavioral treatment plans. MERIT therapists described an unstructured, flexible approach focused on more subjective outcomes that were related to cognitive processes and resultant functional outcomes.
Unexpected findings emerged from MERIT therapists, including themes of Comfort with uncertainty and Experiencing growth. An important part of MERIT therapists’ work was allowing therapy to be an evolving process of understanding a person’s life, which also meant that this process was sometimes uncomfortable. Accepting and allowing the discomfort of the unexpected seemed to open up a space therapists and patients could enter together to untangle uncharted territory and walk together in uncovering meaning. Regarding growth, not only did MERIT therapists discuss growth as a therapist, but also their growth as a person. These growth areas were often transformative for therapists, for example, gaining a richer understanding of humanity or of themselves as a person. Therapist growth may be an important factor in prevention of burnout, as growth has been negatively associated with burnout.37 In a recent qualitative study, psychologist interviews revealed responses to burnout which included self-care, creativity, and self-discovery.38 In this study, psychologists’ growth outside their career was used to cope with professional demands. However, in the current study, growth occurred inside and adjacent to the therapy room. This is important because it was found that MERIT therapists reported powerful experiences of growth within their work, and may mean that being a MERIT therapist contributes to lower levels of burnout. More research is needed to address this important question.
Not surprisingly, the structure and approach of how clinicians described their approach in each group had several differences. For instance, PR-S clinicians valued a highly structured approach while MERIT therapists described a more unstructured approach. These differences fit with the goals of each approach towards objective versus subjective outcomes, respectively. MERIT themes appear in line with other work suggesting that improvisation may play a central role in psychoanalysis and integrative psychotherapy to facilitate a natural dialogical exchange and open previously unsafe areas towards new discoveries.39,40 Educational theory, has similarly highlighted the value of embracing unpredictability to create a supportive environment to bolster the possibility of a transformative experience.41
Our findings align with previous literature evaluating patient experiences of MERIT. Lysaker et al interviewed patients receiving either MERIT or supportive therapy.42 Unique to MERIT was patients’ reports of the ability to integrate current experiences into the understanding of their lives, increased sense of agency, and the ability to understand and manage pain. Similarly, de Jong et al found that MERIT patients reported that the therapy was beneficial to their recovery, and specifically helped them understand their own thinking.43 They further explained that the main mechanisms of change were their own active role in therapy, ability to vent and self-express, and the therapeutic alliance.
Limitations
The study has limitations worth noting. The overall sample was modest in size. Clinicians in the PR-S group had greater variation in their job titles and the MERIT group included many persons in training. These group differences may have contributed to the observed results. Future research is needed with larger samples, while controlling for the length of clinician careers, previous training, and supervision. Additionally, the study settings were in urban United States outpatient hospitals and may not generalize to other settings. More research is needed to explore therapists in other settings with differing training, policies, and theoretical orientations (eg, inpatient hospitals, community mental health settings, and facilities outside of the United States).
Conclusions
This study explored the experiences of clinicians offering metacognitive psychotherapy and standard psychiatric rehabilitation services. Findings highlight that both groups of clinicians focused on the therapeutic relationship and emphasized recovery outcomes. MERIT therapists uniquely reported comfort with uncertainty in their work that allowed an environment where new discoveries can be made, and was powerful and impactful for therapists. These findings highlight how metacognitive psychotherapy can promote subjective outcomes while being an impactful experience for clinicians.
Data Sharing Statement
The authors have chosen not to make the data available.
Ethics Statement
The study was approved by the Indiana University institutional review board and all participants provided informed consent.
Acknowledgment
This work is in memory of Dr Paul Lysaker, who was an integral part of this study as well as decades of other important work that influenced this project.
Funding
The study was not funded.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Davidson L. Recovering a sense of self in schizophrenia. J Pers. 2020;88(1):122–132. doi:10.1111/jopy.12471
2. Leonhardt BL, Huling K, Hamm JA, et al. Recovery and serious mental illness: a review of current clinical and research paradigms and future directions. Expert Rev Neurother. 2017;17(11):1117–1130. doi:10.1080/14737175.2017.1378099
3. Leendertse JCP, Wierdsma AI, van den Berg D, et al. Personal recovery in people with a psychotic disorder: a systematic review and meta-analysis of associated factors. Front Psychiatry. 2021;12:622628. doi:10.3389/fpsyt.2021.622628
4. Lysaker PH, Kukla M, Leonhardt BL, et al. Meaning, integration, and the self in serious mental illness: implications of research in metacognition for psychiatric rehabilitation. Psychiatr Rehabil J. 2020;43(4):275–283. doi:10.1037/prj0000436
5. Skar-Fröding R, Clausen HK, Šaltytė Benth J, Ruud T, Slade M, Sverdvik Heiervang K. The importance of personal recovery and perceived recovery support among service users with psychosis. Psychiatr Serv. 2021;72(6):661–668. doi:10.1176/appi.ps.202000223
6. Wood L, Burke E, Morrison A. Individual cognitive behavioural therapy for psychosis (CBTp): a systematic review of qualitative literature. Behav Cogn Psychother. 2015;43(3):285–297. doi:10.1017/S1352465813000970
7. Turner DT, McGlanaghy E, Cuijpers P, van der Gaag M, Karyotaki E, MacBeth A. A meta-analysis of social skills training and related interventions for psychosis. Schizophr Bull. 2018;44(3):475–491. doi:10.1093/schbul/sbx146
8. Kukla M, Salyers MP, Strasburger AM, Johnson-Kwochka A, Amador E, Lysaker PH. Work-focused cognitive behavioral therapy to complement vocational services for people with mental illness: pilot study outcomes across a 6-month posttreatment follow-up. Psychiatr Rehabil J. 2019;42(4):366–371. doi:10.1037/prj0000365
9. Friesinger JG, Topor A, Bøe TD, Larsen IB. Studies regarding supported housing and the built environment for people with mental health problems: a mixed-methods literature review. Health Place. 2019;57:44–53. doi:10.1016/j.healthplace.2019.03.006
10. Kukla M, McGuire AB, Salyers MP. Barriers and facilitators related to work success for veterans in supported employment: a nationwide provider survey. Psychiatr Serv. 2016;67(4):412–417. doi:10.1176/appi.ps.201500108
11. Shattock L, Berry K, Degnan A, Edge D. Therapeutic alliance in psychological therapy for people with schizophrenia and related psychoses: a systematic review. Clin Psychol Psychother. 2018;25(1):e60–e85. doi:10.1002/cpp.2135
12. Hasson-Ohayon I, de Jong S, Igra L, Carter SA, Faith LA, Lysaker P. Longitudinal changes in therapeutic alliance with people with psychosis: relationship between client and therapist assessments. Clin Psychol Psychother. 2021;28(5):1243–1253. doi:10.1002/cpp.2572
13. Tzur Bitan D, Abayed S. Process expectations: differences between therapists, patients, and lay individuals in their views of what works in psychotherapy. J Clin Psychol. 2020;76(1):20–30. doi:10.1002/jclp.22872
14. Tzur Bitan D, Shalev S, Abayed S. Therapists’ views of mechanisms of change in psychotherapy: a mixed-method approach. Front Psychol. 2022;13:565800. doi:10.3389/fpsyg.2022.565800
15. Bressi Nath S, Alexander LB, Solomon PL. Case managers’ perspectives on the therapeutic alliance: a qualitative study. Soc Psychiatry Psychiatr Epidemiol. 2012;47(11):1815–1826. doi:10.1007/s00127-012-0483-z
16. Scheel MJ, Davis CK, Henderson JD. Therapist use of client strengths: a qualitative study of positive processes. Couns Psychol. 2013;41(3):392–427. doi:10.1177/0011000012439427
17. Osborn LA, Stein CH. Mental health care providers’ views of their work with consumers and their reports of recovery-orientation, job satisfaction, and personal growth. Community Ment Health J. 2016;52(7):757–766. doi:10.1007/s10597-015-9927-8
18. Knox M, Esteban EE, Hernandez EA, Fleming MD, Safaeinilli N, Brewster AL. Defining case management success: a qualitative study of case manager perspectives from a large-scale health and social needs support program. BMJ Open Qual. 2022;11(2):e001807. doi:10.1136/bmjoq-2021-001807
19. Kraus SW, Stein CH. Recovery-oriented services for individuals with mental illness and case managers’ experience of professional burnout. Community Ment Health J. 2013;49(1):7–13. doi:10.1007/s10597-012-9505-2
20. Waller H, Garety P, Jolley S, et al. Training frontline mental health staff to deliver “low intensity” psychological therapy for psychosis: a qualitative analysis of therapist and service user views on the therapy and its future implementation. Behav Cogn Psychother. 2015;43(3):298–313. doi:10.1017/S1352465813000908
21. Steele R. Mental health clinicians’ views of summary and systematic review utility in evidence-based practice. Health Info Libr J. 2021;38(4):295–303. doi:10.1111/hir.12359
22. Holttum S, Wright T, Wood C. Art therapy with people diagnosed with psychosis: therapists’ experiences of their work and the journey to their current practice. Int J Art Ther. 2021;26(4):126–136. doi:10.1080/17454832.2021.1893370
23. Adame AL. “Present through it all”: a qualitative exploration of psychotherapy and psychosis. J Humanist Psychol. 2019;59(6):859–876. doi:10.1177/0022167816665524
24. Hussong DK, Micucci JA. The use of humor in psychotherapy: views of practicing psychotherapists. J Creat Ment Health. 2021;16(1):77–94. doi:10.1080/15401383.2020.1760989
25. Gardner KJ, Wright KM, Elliott A, et al. Learning the subtle dance: the experience of therapists who deliver mentalisation-based therapy for borderline personality disorder. J Clin Psychol. 2022;78(2):105–121. doi:10.1002/jclp.23208
26. Morin L, Franck N. Rehabilitation interventions to promote recovery from schizophrenia: a systematic review. Front Psychiatry. 2017;8:100. doi:10.3389/fpsyt.2017.00100
27. van Weeghel J, van Zelst C, Boertien D, Hasson-Ohayon I. Conceptualizations, assessments, and implications of personal recovery in mental illness: a scoping review of systematic reviews and meta-analyses. Psychiatr Rehabil J. 2019;42(2):169–181. doi:10.1037/prj0000356
28. Lysaker PH, Klion RE. Recovery, Meaning-Making, and Severe Mental Illness: A Comprehensive Guide to Metacognitive Reflection and Insight Therapy. New York: Routledge; 2017.
29. Lysaker PH, Gagen E, Klion R, et al. Metacognitive Reflection and Insight Therapy: a recovery-oriented treatment approach for psychosis. Psychol Res Behav Manag. 2020;13:331–341. doi:10.2147/PRBM.S198628
30. Hasson-Ohayon I, Kravetz S, Lysaker PH. The special challenges of psychotherapy with persons with psychosis: intersubjective metacognitive model of agreement and shared meaning. Clin Psychol Psychother. 2017;24(2):428–440. doi:10.1002/cpp.2012
31. Hamm JA, Ridenour JM, Hillis JD, Neal DW, Lysaker PH. Fostering intersubjectivity in the psychotherapy of psychosis: accepting and challenging fragmentation. J Psychother Integr. 2021;32(4):377–389. doi:10.1037/int0000271
32. Farkas M, Gagne C, Anthony W, Chamberlin J. Implementing recovery oriented evidence based programs: identifying the critical dimensions. Community Ment Health J. 2005;41(2):141–158. doi:10.1007/s10597-005-2649-6
33. Dalum HS, Pedersen IK, Cunningham H, Eplov LF. From recovery programs to recovery-oriented practice? A qualitative study of mental health professionals’ experiences when facilitating a recovery-oriented rehabilitation program. Arch Psychiatr Nurs. 2015;29(6):419–425. doi:10.1016/j.apnu.2015.06.013
34. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
35. Bourke E, Barker C, Fornells-Ambrojo M. Systematic review and meta-analysis of therapeutic alliance, engagement, and outcome in psychological therapies for psychosis. Psychol Psychother. 2021;94(3):822–853. doi:10.1111/papt.12330
36. Faith LA, Howie JH, Blanco E, Jarvis SP, Rempfer MV. Therapeutic alliance in a cognitive rehabilitation programme for people with serious mental illness: a qualitative analysis. Psychol Psychother. 2022;95(4):958–969. doi:10.1111/papt.12412
37. Taku K. Relationships among perceived psychological growth, resilience and burnout in physicians. Pers Individ Differ. 2014;59:120–123. doi:10.1016/j.paid.2013.11.003
38. Turnbull MG, Rhodes P. Burnout and growth: narratives of Australian psychologists. Qual Psychol. 2021;8(1):51. doi:10.1037/qup0000146
39. Kindler A. Spontaneity and improvisation in psychoanalysis. Psychoanal Inq. 2010;30(3):222–234. doi:10.1080/07351690903206181
40. Roe D, Lysaker PH. Meaning, recovery, and psychotherapy in light of the art of jazz. Psychiatr Rehabil J. 2023. doi:10.1037/prj0000565
41. O’Donnell A. Unpredictability, transformation, and the pedagogical encounter: reflections on “what is effective” in education. Educ Theory. 2013;63(3):265–282. doi:10.1111/edth.12023
42. Lysaker PH, Kukla M, Belanger E, et al. Individual psychotherapy and changes in self-experience in schizophrenia: a qualitative comparison of patients in metacognitively focused and supportive psychotherapy. Psychiatry. 2015;78(4):305–316. doi:10.1080/00332747.2015.1063916
43. de Jong S, Hasson-Ohayon I, van Donkersgoed R, Aleman A, Pijnenborg GHM. A qualitative evaluation of the effects of Metacognitive Reflection and Insight Therapy: “living more consciously”. Psychol Psychother. 2020;93(2):223–240. doi:10.1111/papt.12212
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.