Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Promoting Health Literacy to Prevent Depression Among Workers in Industrial Factories in the Eastern Economic Corridor of Thailand
Authors Thongnopakun S ![]() , Visanuyothin S
, Visanuyothin S ![]() , Manwong M
, Manwong M ![]() , Rodjarkpai Y
, Rodjarkpai Y ![]() , Patipat P
, Patipat P ![]()
Received 17 July 2020
Accepted for publication 9 October 2020
Published 2 November 2020 Volume 2020:13 Pages 1443—1453
DOI https://doi.org/10.2147/JMDH.S272574
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Saowanee Thongnopakun,1 Sawitree Visanuyothin,2 Mereerat Manwong,3 Yuvadee Rodjarkpai,1 Pichitra Patipat1
1Faculty of Public Health, Burapha University, Chon Buri, Thailand; 2Maharat Nakhon Ratchasima Hospital, Nakhon Ratchasima, Thailand; 3College of Medicine and Public Health, Ubon Ratchathani University, Ubon Ratchathani, Thailand
Correspondence: Saowanee Thongnopakun Tel +66 38102-730
Email [email protected]
Purpose: This study aimed to identify the factors associated with depression among workers in industrial factories in the Eastern Economic Corridor (EEC) of Thailand. Additionally, a guidebook was created to evaluate the suitability and appropriateness of the health literacy of the workers to prevent depression.
Methods: This study applied a mixed method from May 2019 to May 2020. Two-stage sampling was used to recruit samples. A total of 416 workers were surveyed using a self-administered questionnaire. Moreover, 20 stakeholders enrolled in two focus group discussions (FGDs) using a semi-structured interview questionnaire to explore situations and develop a guidebook. Descriptive statistical, multivariable logistic regression, and content analysis were applied to analyze the data. Both quantitative and qualitative data were used in the development of the guidebook, which were further tested and evaluated by interviewing the 20 stakeholders.
Results: Depression was found in 17.1% of the workers. Job position (adjusted odds ratio [ORadj] = 7.14), hours of online media use (ORadj = 1.87), moody/anxious (ORadj = 5.35), avoiding people (ORadj = 9.12), and self-behavior modification to prevent depression (ORadj = 2.41) were associated with significant depression. The FGDs revealed that stakeholders had blurred perceptions of stress and depression. The sample of industrial factory workers was subjected to workload time constraints but had low level of screening for depression. Online media was used only for working in industries. The guidebook was very interesting and useful for stakeholders and contained definitions and symptoms of depression, self-screening and self-care strategies, consultation and hotline contacts, and health literacy improvement guidelines for factory and health personnel to prevent depression.
Conclusion: This study confirmed that online media and health literacy were imperative factors to address depression among workers in industrial factories. The guidebook was developed based on health literacy and help prevent depression among workers in industrial settings.
Keywords: health literacy, labor, intervention, factory, industry
Introduction
Depression is a significant health problem with increasing severity in all countries.1 From a 2017 World Health Organization (WHO) survey, depression was evident in 300 million people worldwide. The prevalence of depression increased by 18% from 2005 to 2015.2 The estimated cost of depression caused an economic loss of $800 million in the U.S. in 2010. This loss is expected to double in 2030.3 A survey conducted in Thailand indicated that nearly 1 million people had depression, with nearly 2% suffering from major depressive disorder (MDD).4 The number of suicides in Thailand is approximately 4000 per year, mostly aged 30–39 years old,5 with half of them being caused by MDD.6 The prevalence of depression in Thai workers surveyed in the 15–29, 30–44, and 45–59 age groups was 1.0%, 2.8%, and 3.0%, respectively. The east sections of Thailand had the highest prevalence.7 These portions of the country launched the Eastern Economic Corridor (EEC) project, which affected more than one-sixth of total workers in Thailand8 Working in industrial factories affects lifestyle, family relationships, and community,9 especially migrants to the EEC who adjust to new living and working conditions. The high stress of the workplace environment and new lifestyle can result in the progression of health problems, including depression.10 In turn, depression impacts their work effectiveness and their standard of living.11 Without treatment, depression can worsen over time, leading some workers to more serious symptoms of MDD and even others to consider suicide. Surveillance and prevention systems are imperative for decreasing the occurrences of major depression and suicide;12 however, industrial factory workers are not part of the target group for screening depression in Thailand.12
 |
Figure 1 Cover page of guidebook “Depression Literacy for Industrial Workers”. |
Although Thailand implemented the Thailand 4.0 policy to improve the health literacy of workers, a 2016 auto parts survey revealed that 41.9% of workers had low levels of literacy in the areas of eating, exercise, emotions, stop smoking, and stop drinking (3E2S), along with stress management.13 From the literature review, there were few studies about depression among industrial workers.14 Therefore, this study aimed to explore the factors associated with depression among workers in industrial factories in the EEC and developed a guidebook from surveys and focus group discussions (FGDs) to address health literacy and prevent depression.
Materials and Methods
Study Design
This study used mixed method research with quantitative and qualitative methods of data collection from May 2019 to May 2020.
Population Sample and Sampling Technique
Quantitative
A cross-sectional study was conducted in the EEC of factories that were divided into two groups by the Ministry of Labor: Group 1 had ≥200 industrial workers and Group 2 had <200 industrial workers.15 The study population was comprised of 1,187,300 industrial workers from the EEC.16 The sample size was calculated using Lemeshow et al (1990)17 with α = 0.05, p = 0.58,13 and d = 0.05 (5% precision of estimated). The estimated sample size (n) was 375 industrial workers. With the addition of 5% missing data, 416 industrial workers were recruited from six factories as the representative of car accessories factories, metal products factories, household chemicals factories, auto parts factories, electric factories, and power transformer factories. The Thai participants were 18–60 years old, had worked in the EEC for more than three months, and had access to using online media. None of the participants had a history of depression diagnosed by a physician, and all willingly enrolled in this study. The two-stage simple random sampling provided the two following stages: drawing lots to select 208 workers from each province to be representative of two provinces for industrial factories and then consecutive sampling to complete the sample size.
Qualitative
One province was selected to proceed with the FGDs by drawing lots. A purposeful sampling (Thai nation, working at least three months, and willing to cooperate) was done for 2 groups FGDs; group 1 comprised 10 stakeholders (two employers, one officer of the department of Labor Protection and Welfare, one municipality officer, one health officer of a primary care unit, three related health workers from a community hospital which response for health of workers in industrial Estate, one community leader, and one village health volunteer) and group 2 consisted 10 industrial workers. The FGD was conducted twice of each group: the first assessed the experiences of industrial workers with depression and the second developed the guidebook. FGD was taken 1 hour/time. Both groups were also interviewed to assess the effectiveness of the guidebook.
Materials
Quantitative
An online questionnaire was managed by the researcher and manager of each factory via a QR code. It was specifically designed as a tool for this study based on the Nutbeam concept16 and V-shape from the Ministry of Public Health of Thailand (modified from the Sorensen concept).18 The questionnaire was composed of 88 questions divided into three parts: 1) sociodemographic characteristics (20 questions); 2) health literacy of depression prevention (48 questions) measuring access to health information and health services, overall understanding of mental health, questioning skills to improve one’s knowledge, decision-making skills to choose appropriate practices, self-behavior modification, and knowledge transfer and sharing. A Likert scale was used with a total score of 240 to measure the impact of health literacy on depression prevention. Scores were categorized into four levels: a score <144 was poor, 144–167 was moderate, 168–191 was good, and 192–240 was very good;14 3) the Center of Epidemiologic Studies Depression (CES-D) scale19 had already been translated into the Thai language,20,21 which consisted of a Likert scale of 20 questions measuring emotional and behavioral symptoms of depression over a one-week ago. With a maximum score of 60, scores from 23 to 60 were indicators of depression.
Data were collected in a two-step process: 1) the questionnaire was validated by five experts, the content validity was tested, and then the questionnaire corrected; and 2) the items-objective congruence (IOC) index, which was 0.85, was used to obtain validity from five experts. A pilot study was conducted to test the reliability of the questionnaire with a sample of 30 industrial workers in the EEC. The Cronbach’s alpha for health literacy to prevent depression was 0.84.
Qualitative
Semi-structured interviews were used in the FGDs to gather information about the industrial workers’ experiences with depression situation and for the development of the guidebook. Individual interviews were conducted for the guidebook evaluation. The content validity was tested and the questionnaire was corrected by using the items-objective congruence (IOC) index, which was 0.96, to obtain validity from five experts. The IOC of the semi-structured interview to evaluate the guidebook was 0.96.
Data Analysis
Quantitative
Data analysis was conducted using SPSS version 22 (university license). Descriptive statistics were used to describe the sociodemographic characteristics, levels of health literacy to prevent depression, and the Center for Epidemiologic Studies-Depression Scale (CES-D). Univariate analysis categorical data were performed by Fisher’s exact test and chi-square, continuous data were analyzed by Mann–Whitney test, which were used to determine the association between sociodemographic characteristics and health literacy to prevent depression. Multivariable logistic regression was employed to evaluate dependent variables associated with health literacy to prevent depression, which was a dichotomous variable in this study; depression was coded as 1, and no depression was coded as 0. A p-value© < 0.05 was considered to represent statistical significance.
Qualitative
A descriptive content analysis procedure was applied for analysis of qualitative data. The data were recorded in a transcript, validated into categories according to similarity, and analyzed by two co-researchers.
Ethical Considerations
The Ethics Review Committee for Human Research Subjects, Burapha University (certified code: Sci 053/2562) approved this research. This study was conducted in accordance with the principles of the Declaration of Helsinki. The research was explained to the participants who signed informed consent. Their privacy was protected and their data will be kept confidential.
Results
1. Findings from both quantitative and qualitative data regarding industrial workers and depression.
The response rate to the online questionnaire was 100% by 416 participants. The sex ratio of industrial workers was 1:1 and 40.1% were single. Two-fifth of participants did not have enough income to cover their expenses and had a history of alcoholic drinking. The average time for using online media was three hours a day. The FGDs presented many problems that caused stress and depression. Some of the problems identified were that 9.1% of the participants had sleep problems, 10.8% had anxiety or mood issues, and 7.2% avoided people. Only one-fifth had good or very good levels of health literacy to prevent depression. The prevalence of depression was 17.1% of 416 industrial workers.
Blurred Perceptions of Stress and Depression
If we are in the working age, there will be many causes of the problems such as expenditure couple and family matter. If your age is more than 50, the problem will be health problem and underlying disease. Someone may have family’s problem like the worry about their kids or nephews. (Public health officer)
The industrial workers had suffered from working more than be happy 10.5%.
Workload Time Constraints
The FDGs revealed that industrial workers operate under pressure. “… if it is the issues about work, we will mostly speed up work to be finish before deadline. These led us to be stress …” (Industrial worker).
The univariate analysis revealed that job position (p = 0.023), hours of online media use per day (p = 0.001), happiness at work (p = 0.001), sleep problems (p <0.001), moody/anxious (p <0.001), avoiding people (p <0.001), access to health information and health 230 services to prevent depression (p <0.001), questioning skills to enhance knowledge about depression prevention (p <0.001), decision-making skills in choosing appropriate practices to prevent depression (p = 0.005), self-behavior modification (p = 0.008), and knowledge transfer and sharing (p = 0.002) were statistically significant in relation to depression among industrial workers. The results are shown in Table 1.
 |  | 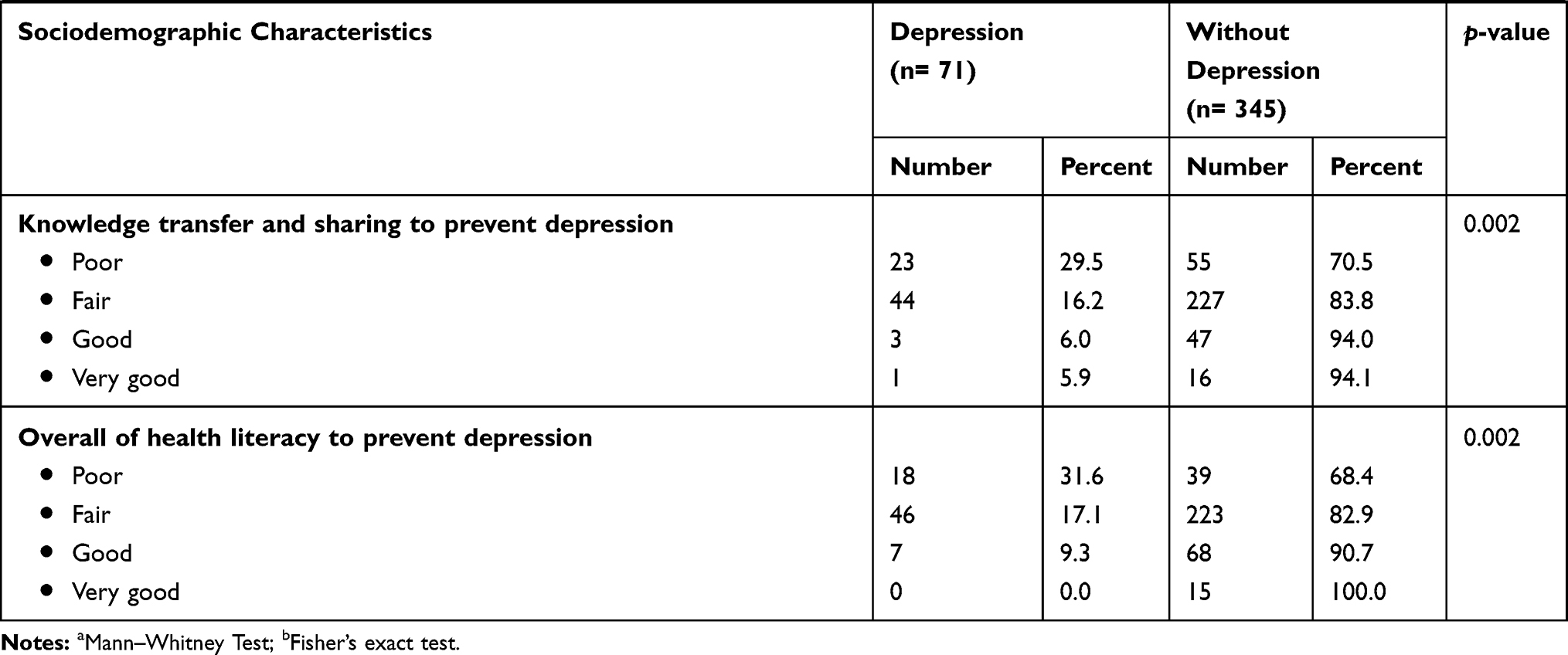 |
Table 1 Associations Between Sociodemographic Characteristics and Health Literacy Toward Depression Among Industrial Workers (Chi-Square Tests) |
Multivariable logistic regression revealed that job positions (Adjusted odds ratio [ORadj] = 0.14, 95% CI: 0.03–0.59); being as chief can prevent depression 86% when compared to managers position, hours of online media use per day (ORadj = 1.87, 95% CI: 1.04–3.35); a person who used online media >3 hours/day was more likely to have depression 1.87 times than who used ≤3 hours/day, moody/anxious (ORadj = 5.35, 95% CI: 1.62–17.70); a person who often/usually was moody/anxious was more likely to have depression 5.35 times than who rarely was moody/anxious, avoiding people (ORadj = 9.12, 95% CI: 3.15–26.42); a person who often/usually avoided people was more likely to have depression 9.12 times than who rarely avoided people, and self-behavior modification to prevent depression (ORadj = 2.41, 95% CI: 1.17–4.95); a poor-fair health literacy behavior change person was more likely to have depression 2.41 times than who had good-very good level of health literacy; these were significant factors with depression. The results are shown in Table 2. The results from the FGDs revealed the use of many activities to address anxiety and depression problems, such as clinic overtime, fast track health services, one-stop services, the promotion of depression knowledge on the boards in some factories, networking, collaboration of caring, consulting, and referring, morning meetings, health education, yearly health checkups, hotlines, consultation units in the factories, job rotation, and offering special debt management for some industrial workers. It was observed that stakeholders put more emphasis on physical health than mental health. Moreover, they perceived that depression was a minor problem among industrial workers. However, half of the stakeholders acknowledged that the improvements in the system could reduce stress and symptoms of depression.
 |
Table 2 Multiple Logistic Regression Analysis of Factors Associated with Sociodemographic Characteristics and Health Literacy Toward Depression Among Industrial Workers |
2. The guidebook promotes mental health and prevents depression among industrial workers in the EEC.
The results of the FGDs with 20 stakeholders led to the development of the guidebook components dealing with definitions and symptoms of depression, self-screening and self-care strategies, consultation and hotline contacts, and health literacy improvement guidelines for factory and health personnel to prevent depression. The results of the guidebook evaluation showed that it was interesting and useful for the stakeholders. The figure 1 shows QR code on the cover page of guidebook “Depression Literacy for Industrial Workers”, which provides the complete guidebook.
Understand Themselves and Surrounding People
This guidebook made me understand myself. I can evaluate myself whether I had depress or not. (Officer of the municipality)
Easy to Understand and to Put into Practice
The content was quite good, clear, and easy to comprehend. When I read it, it made me to understand more. I asked myself whether I had depression or not. (Industrial workers).
Many Format of Guidebook
The guidebook was issued in both e-book and paper book formats for industrial workers to evaluate. It was also recommended that the researcher provides a picture book for industrial workers who may be illiterate or have limited time to read.
Discussion
The results revealed that one in five industrial workers had depression, but qualitative data indicated that there were very few problems about depression perceived in factories. There were five significant factors associated with depression as following; job positions, hours of using online media per day, moody/anxious, avoiding people, self-behavior modification to prevent depression. However, only two the hours of using online media per day and self-behavior modification to prevent depression could be modified in the guidebook as ways for industrial workers to prevent depression.
The percentage of industrial workers with depression surveyed in this study by CES-D19,21 was 17.1%, which was higher than the study in Sweden study among a population of individuals 20–64 years old22 and less than the study in Japan, Korea, and Vietnam.23–25 Based on the FGDs results, stakeholders thought that working in factories resulted in high stress and lower levels of happiness. Moreover, there were low level of screening for depression in industrial workers. They mentioned that stress may lead to depression which is consistent with Takada et al (2009)23 and the WHO (2009).2
This study revealed that managers were 7.14 times more likely to experience depression compared to chief and this agrees with studies by Thangthum (2015) and Cheung and Yip (2015).26,27 Job position is closely associated to depression, anxiety, and stress. Managers have greater responsibilities which require making important decisions which explains why they are more prone to stress and depression.23,28 Alternatively, Lazaeus and Folkman (1976),29 McGrath and Robert (1976), and Motowidlo et al (1986) confirmed that stress can have both positive and negative effects on work effectiveness.30 However, stress experienced over long durations can cause physical and mental health problems in workers.31 There is a need for employers to manage workload appropriately, make roles and responsibilities clear, promote good relationships and communication, and ensure fairness and equity for all to reduce stress and depression.32
The Electronic Transactions Development Agency (ETDA) of Thailand found that the Thai used the internet 6.4 hours/day or 45 hours/week on average.32 These were the results of studies which were concordant to this study. Overuse of social media can have negative effects on physical, mental, and societal health.33 Lin et al (2016) found that using social media more than 2 hours a day more than doubles feelings of loneliness.34 Social media usage on a smart phone can be associated with depression, and people with depression used smartphones for 68 minutes/day on average.35 If a person becomes addicted to using social media, they could experience a decrease in happiness and an increase in depression.36 Even though this study pointed that more online use results in more depression, Pewnil (2015) showed that social media had both positive and negative effects at the same time.37 Depression is an emotional and mental disorder. This study confirmed that the moody/anxious symptoms and avoiding people in industrial workers were consistent with many studies.38–40
Self-behavior modification to prevent depression was significantly associated with depression prevention. Levin (1976) mentioned that healthcare is the process of promotion, prevention, detection, and treatment of one’s own health.41 WHO (1987) defined self-care as activities that individuals, families, and communities engage in to promote, prevent, diagnose, treat, and rehabilitate health.42 Orem (1985) defined self-care as individual activities to maintain good health and well-being.43 Self-care requires self-management skills to engage in basic care of oneself.44 One study indicated that self-management of epilepsy in patients was directly linked to depression. Patients with low degrees of self-management have a higher chance of depression.45 Self-perception, self-love, self-esteem, and self-confidence made workers recognize the value of their health and healthy behaviors. In contrast, without these feelings, workers have a more difficult time seeing their value which, in turn, causes more stress, fatigue, desperation, pessimism, and self-harm.46
The results of this study emphasized that two significant factors––the hours of using online media per day and self-behavior modification to prevent depression ––could be modified to improve health literacy to prevent depression among industrial workers. The guidebook was developed with both factors in mind. The key success factor of the guidebook is not its development but rather its ability to be used and acted upon in reality. The process of the guidebook development involved two focus groups: 1) situations and experiences with depression from the stakeholders provided the researcher a deep understanding of the associated factors of depression; 2) participation by stakeholders in the guidebook development was crucial for the creation of a suitable and sustainable guidebook in the EEC. An e-book and paper book were developed and sent to 20 stakeholders for evaluation. They suggested that making a picture book accessible to the industrial workers would increase their comprehension; the main reason being that picture books are large, colorful, easy to read, and simple in their storyline and structure.47 On average, Thai people only read eight lines per day or 3–4 books per year, in comparison to Malaysians who read 40 books per year and Vietnamese who read 60 books per year.48
Conclusion
The purpose of this study was to investigate the factors associated with depression among workers in industrial factories in the EEC in Thailand. The associated significant factors with depression were job position, hours of online media use, moody/anxious symptoms, avoiding people, and self-behavior modification to prevent depression. The stakeholders involved in the FGDs indicated that health literacy mostly focused on physical health and depression was perceived to be a minor problem in the EEC. In our study, a research model was developed based on health literacy to address depression that occurred in 17.1% of the workers and a guidebook was created as a useful resource to help prevent depression in industrial workers in the EEC.
Limitations and Recommendations
To generalize the results of this study to reduce depression, one should consider the context, which is to enhance health literacy of depression prevention and reduce the negative effects of using social media in an industrial setting. The effectiveness of the guidebook, including the addition of a picture book, should be tested by implementing methods to promote health literacy to prevent depression.
Acknowledgments
The authors wish to thank Burapha University for funding this study. The researcher would like to express gratitude to all informants who contributed to the research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Depression 2018. 2018. Available from: http://www.searo.who.int/thailand/news/technical-factsheet-depression-thai.pdf.
2. World Health Organization. Mental Health in the Workplace. Genewa Switzerland: World Health Organization; 2019. Available from: https://www.who.int/mental_health/in_the_workplace/en/.
3. World health organization. Making Mental Health a Global Development Priority. Washington DC: World health organization; 2016. Available from: https://www.who.int/mental_health/WB_WHO_meeting_2016.pdf.
4. Department of Mental Health. Thai National Mental Health Survey 2013 Nonthaburi. Mimistry of Public Health Thailand; 2013. Available from: https://forums.dmh.go.th/index.php?topic=138165.0.
5. Tantipasawasin S. Suicide in Thai Society. Chonburi Hosp J. 2019;44(1):1.
6. Horsaengchai TB, Hansa Dhammahaso P. Self-awareness reinforcing model for prevention the risky behavior to suicide of adolescents by Buddhist peaceful means. J MCU Peace Stud. 2019;7(sup):154–167.
7. Aekplakorn W. Thai National Health Examination Survey. Nonthaburi Thailand: NHES V; 2014.
8. National statistical office. Labour Force Bangkok Thailand. Ministry of Digital Economy and Society; 2019. Available from: http://statbbi.nso.go.th/staticreport/page/sector/en/02.aspx.
9. Nisaisuk N. The Impact of Eastern Seaboard Industrial Development, Rayong: A Case Study of Mab Yangporn Community, Pluak Daeng District Rayong Province Chon Buri Thailand. Burapha University; 2013.
10. Horesh N, Klomek AB, Apter A. Stressful life events and major depressive disorders. Psychiatry Res. 2008;160(2):192–199. doi:10.1016/j.psychres.2007.06.008
11. Kongsomboon K. Factors affecting depression in workplace: marital status, BMI, stress level, work duration, job pattern, and daytime sleepiness. Chula Med J. 2010.
12. Department of Mental Health. Guidebook of Depressive Disorders Surveillance and Care: Provincial Level. Nonthaburi Thailand: Ministry of Public Health; 2014.
13. Health Education Division. Health Literacy of Health and Behavior Evaluation in Thailand Nonthaburi Thailand Ministry of Public Health; 2017.
14. Health Education Division. Creating and Evaluating the Health Literacy and Health Behavior Among Child and Youth and Over 15 Years Old Nonthaburi Thailand. Ministry of Public Health; 2018.
15. Department of Labour Protection and Welfare. Ministerial Regulations Arrangement of Welfare in Workplace, 2005. Bangkok Thailand: Ministry of Labour; 2005. Available from:: https://www.ieat.go.th/handbook/Program_IEAT/pages/en/Department/MOL.html.
16. Nutbeam D. The evolving concept of health literacy. Soc Sci Med. 2008;67(12):2072–2078. doi:10.1016/j.socscimed.2008.09.050
17. Organization WH; Lemeshow S, Hosmer DW, Klar J, Lwanga SK. Adequacy of Sample Size in Health Studies. Chichester: Wiley; 1990.
18. Department of Health. Conceptual model of health literacy (Thailand). Access to health information access to health information Bangkok Thailand. 2018.
19. Radloff LS. The CES-D scale: A self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1(3):385–401. doi:10.1177/014662167700100306
20. Vorapongsathorn T, Pandii W. The validity of the CES-D. Thai J Clin Psychol. 1990;21:26–45.
21. Trangkasombat U, Larpboonsarp V, Havanond P. CES-D as a screen for depression in adolescents. J Psychiatr Assoc Thailand. 1997;42(1):2–13.
22. Waldenström K, Ahlberg G, Bergman P, et al. Externally assessed psychosocial work characteristics and diagnoses of anxiety and depression. Occup Environ Med. 2008;65(2):90–96. doi:10.1136/oem.2006.031252
23. Takada M, Suzuki A, Shima S, Inoue K, Kazukawa S, Hojoh M. Associations between lifestyle factors, working environment, depressive symptoms and suicidal ideation: a large-scale study in Japan. Ind Health. 2009;47(6):649–655. doi:10.2486/indhealth.47.649
24. Lim S, Chi S, Lee JD, Lee H-J, Choi H. Analyzing psychological conditions of field-workers in the construction industry. Int J Occup Environ Health. 2017;23(4):261–281. doi:10.1080/10773525.2018.1474419
25. Braquehais MD, Valero S, Matalí JL, et al. Promoting voluntary help-seeking among doctors with mental disorders. Int J Occup Med Environ Health. 2014;27(3):435–443. doi:10.2478/s13382-014-0271-y
26. Thangthum J. Working Factors Influencing on Stress and Operational Efficiency of Manufacturing Employees in Electronic Industry. Rajamangala University of Technology Thanyaburi; 2015.
27. Cheung T, Yip PS. Depression, anxiety and symptoms of stress among Hong Kong nurses: a cross-sectional study. Int J Environ Res Public Health. 2015;12(9):11072–11100. doi:10.3390/ijerph120911072
28. Sukmaitree J, et al. Stress management in organization. Prae-Wa Kalasin J Kalasin Univ. 2019;6(1):141–156.
29. Lazaeus RS, Folkman S. Stress Appraisal and Coping. New York: Springer; 1976.
30. McGrath. JE, Robert JR. Time and Human Interaction. New York: Guilford; 1976.
31. Motowidlo SJ, Packard JS, Manning MR. Occupational stress: its causes and consequences for job performance. J Appl Psychol. 1986;71(4):618–629. doi:10.1037/0021-9010.71.4.618
32. Electronic Transactions Development Agency (EDTA). Thailand Internet User Profile 2016. Bangkok Thailand; 2016.
33. Poll N Social media with Thai children and youth future 2017. Available from: http://nidapoll.nida.ac.th/index.php?op=polls-detail&id=523.
34. Lin LY, Sidani JE, Shensa A, et al. Association between social media use and depression among US young adults. Depress Anxiety. 2016;33(4):323–331. doi:10.1002/da.22466
35. Saeb S, Zhang M, Karr CJ, et al. Mobile phone sensor correlates of depressive symptom severity in daily-life behavior: an exploratory study. J Med Internet Res. 2015;17(7):e175. doi:10.2196/jmir.4273
36. Van den Eijnden RJ, Meerkerk G-J, Vermulst AA, Spijkerman R, Engels RC. Online communication, compulsive Internet use, and psychosocial well-being among adolescents: a longitudinal study. Dev Psychol. 2008;44(3):655. doi:10.1037/0012-1649.44.3.655
37. Pewnil T, Isarabhakdi P. Family, communication, and mental well-being among high school students in Kanchanaburi province,
38. World Health Organization. Mental disorders: World Health Organization 2019. Available from: https://www.who.int/news-room/fact-sheets/detail/mental-disorders.
39. National institute of mental health. Depression United State of America. The National Institute of Mental Health (NIMH); 2018.
40. Reynolds SM To Disclose or Not to Disclose? Self-Disclosure of Mental Health in the Workplace. 2019.
41. Levin LS. Self-care: an international perspective. Soc Policy. 1976;7(2):70–75.
42. World Health Organization ROfS-EA. Self Care for Health. New Delhi: WHO Regional Office for South-East Asia; 2014.
43. Orem DE. Nursing: Concept of Practice Ed. r, Editor. New York: Mc Graw-Hill; 1985.
44. Tobin DL, Reynolds RV, Holroyd KA, Creer TL. Self-management and social learning theory. Self Manage Chronic Dis. 1986;29–55.
45. DiIorio C, Shafer PO, Letz R, et al. Behavioral, social, and affective factors associated with self-efficacy for self-management among people with epilepsy. Epilepsy Behav. 2006;9(1):158–163. doi:10.1016/j.yebeh.2006.05.001
46. Srichan S, Sueprasertsitth C. Self-Care Behaviors Among Working-Age People in Chachoengsao Municipality. Chon Buri Thailand: Burapha University; 2018.
47. Tan S Picture Books: who Are They For?
48. Wiriyakulopas K, Thanusorn K, Phakatip C, konglumphoon B. The information needs and Thaksin university library community information services guidelines. Thaksin Univ Lib j. 2013;3:1–19.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.