Back to Journals » Infection and Drug Resistance » Volume 19
Prolonged Thromboelastography R Time and Thrombocytopenia as Early Warning Indicators of Bleeding in ECMO Patients Who Developed Sepsis During Support: A Retrospective Cohort Study
Authors Xu M, Xu H, Yu YW ![]() , Pan XY, Jin JJ, Li T
, Pan XY, Jin JJ, Li T
Received 24 October 2025
Accepted for publication 19 February 2026
Published 10 March 2026 Volume 2026:19 576614
DOI https://doi.org/10.2147/IDR.S576614
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hazrat Bilal
Mi Xu,1,* Hao Xu,2,* Yong-Wei Yu,1 Xiang-Ying Pan,1,3 Jia-Jia Jin,1,3 Tong Li1
1Intensive Care Unit, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, 310003, People’s Republic of China; 2Intensive Care Unit, Wuxi No.2 People’s Hospital, Wuxi, Jiangsu, 214002, People’s Republic of China; 3Nursing Department, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, 310003, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Tong Li, Email [email protected]
Objective: Bleeding is a major complication in extracorporeal membrane oxygenation (ECMO), particularly when sepsis develops during support. Conventional coagulation tests incompletely reflect haemostatic balance, and reliable early indicators of bleeding risk remain lacking. This study investigated whether dynamic changes in thromboelastography (TEG) parameters and platelet count are associated with subsequent bleeding in this population.
Methods: We conducted a single-center retrospective cohort study including adult patients who developed sepsis during ECMO support between January 2021 and December 2024. Coagulation parameters were recorded at sepsis onset and within 24 hours prior to bleeding events. Major bleeding was defined according to Extracorporeal Life Support Organization criteria. A matched longitudinal analysis was additionally performed in the non-bleeding group using Day 4 after sepsis onset as a comparable observation window. Temporal changes were analyzed using paired statistical tests.
Results: Sixty-four patients were included, of whom 26 (40.6%) developed major bleeding. In the bleeding group, R-time significantly prolonged prior to bleeding compared with sepsis onset (10.1 vs 7.5 min, P = 0.03), while platelet count significantly decreased (93.5 vs 110.0 × 109/L, P = 0.02). In contrast, the non-bleeding group showed no significant longitudinal change in R-time (P = 0.547) or platelet count (P = 0.085) over the matched observation window.
Conclusion: In ECMO patients who develop sepsis, coordinated prolongation of TEG R-time and decline in platelet count precede bleeding events and may represent early warning indicators associated with bleeding risk. These findings are hypothesis-generating and require confirmation in prospective studies.
Keywords: extracorporeal membrane oxygenation, ECMO, sepsis, bleeding complications, thromboelastography, TEG, platelet count
Introduction
Extracorporeal membrane oxygenation (ECMO) serves as a salvage therapy for refractory respiratory or circulatory failure. Infection is a common complication during ECMO support,1,2 which can severely lead to sepsis. Sepsis can not only cause organ dysfunction3 but also lead to complex coagulopathies, even triggering disseminated intravascular coagulation (DIC).4 On the other hand, systemic anticoagulation (eg, with heparin) is required during ECMO to prevent circuit thrombosis. Despite technical improvements, bleeding remains one of the most common and devastating complications in ECMO patients;5,6 an analysis of adverse events in 11,984 venoarterial ECMO (VA-ECMO) patients from the ELSO registry showed that bleeding accounted for up to 62.1%.7 Another retrospective analysis of 7579 venovenous ECMO (VV-ECMO) patients in the ELSO database also indicated that 23.4% of patients experienced bleeding.8
When sepsis complicates ECMO support, patients face a “double hit”: one stemming from ECMO-related coagulation activation and anticoagulation therapy, and the other from sepsis-induced coagulopathy. This complex pathophysiological state makes the management of bleeding risk extremely challenging. Currently, anticoagulation monitoring during ECMO predominantly relies on activated partial thromboplastin time (aPTT) or activated clotting time (ACT),9,10 with doses typically titrated to maintain levels at 1.5–2 times the normal value and between 180–210 seconds, respectively.10 However, in septic patients, aPTT and ACT only reflect parts of the coagulation cascade and fail to provide a comprehensive assessment of the overall balance of the coagulation system.11
Thromboelastography (TEG)12 is a point-of-care viscoelastic coagulation assay that provides a global assessment of the entire haemostatic process, from clot initiation and formation to fibrinolysis, thereby offering a more comprehensive view of coagulation status than conventional tests. A retrospective study of 32 patients with severe respiratory failure receiving ECMO therapy13 observed that despite patients’ aPTT and ACT remaining within the therapeutic anticoagulation range, their TEG tracings already displayed a significant heparin effect. Given this finding and considering that excessive anticoagulation is a persistent risk factor for bleeding during ECMO,14,15 the question of whether a TEG-guided strategy could serve as a safe and feasible alternative to the “conventional” aPTT- or ACT-based monitoring has been an area of active investigation. However, routine anticoagulation titration driven primarily by TEG is not universally recommended in current guidance documents, largely due to limited prospective evidence demonstrating clinical benefit, substantial heterogeneity in viscoelastic testing protocols, and the lack of standardized therapeutic targets across centers.16,17 Nevertheless, TEG may still be clinically valuable as an adjunct tool because it captures the dynamic, whole-blood evolution of coagulation and fibrinolysis that conventional assays (aPTT/ACT) may not reflect, especially in ECMO patients complicated by sepsis where the hemostatic balance is highly unstable This gap between guideline-level evidence and bedside need provides a strong rationale to explore whether specific TEG patterns, together with platelet dynamics, can serve as early warning indicators of bleeding risk in this high-risk population.
However, the development of such a TEG-guided strategy necessitates a deep understanding of the predictive value and interrelationships of various TEG parameters in complex clinical scenarios. In patients with ECMO complicated by sepsis, accurate prediction of bleeding risk may require integrated assessment of two critical dimensions: coagulation initiation and platelet function. From a pathophysiological perspective, ECMO- and sepsis-related coagulopathy often involves early impairment of clot initiation due to dysregulated coagulation factor activity and anticoagulant exposure, together with platelet consumption and dysfunction driven by systemic inflammation and circuit-related activation. TEG parameters such as R time provide a direct functional readout of the initiation phase of coagulation, whereas platelet count represents a key cellular determinant of effective hemostasis and is frequently one of the earliest components to deteriorate during ECMO support. Although other biomarkers (eg, fibrinogen) are also clinically relevant, their trajectories in sepsis can be highly heterogeneous because fibrinogen may initially increase as an acute-phase reactant before later consumption, making single measurements less informative for early bleeding warning. Therefore, this study aimed to investigate how TEG parameters and platelet count evolve dynamically and work in concert to predict bleeding. We hypothesize that TEG parameters reflecting coagulation initiation and a decreased platelet count may function as complementary early-warning signals. Notably, unlike most prior ECMO studies that evaluated viscoelastic parameters in heterogeneous populations or at isolated time points, our study specifically focuses on the high-risk subgroup of patients who develop sepsis during ECMO support and examines the longitudinal evolution from sepsis onset to the pre-bleeding phase. This dynamic, sepsis-centered perspective provides novel insight into bleeding-specific early warning patterns beyond conventional anticoagulation monitoring. By retrospectively testing this hypothesis, our study seeks to provide a critical theoretical foundation for future development of individualized TEG-based anticoagulation management protocols.
Methods
Ethical
This study was approved by the Ethics Committee of the First Affiliated Hospital, Zhejiang University School of Medicine (Approval No. 2025BIIT0961). As this was a retrospective observational study, the requirement for informed consent was waived by the ethics committee. All patient data were anonymized prior to analysis to ensure confidentiality. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Study Design
Study Participants
This single-center, retrospective study consecutively included patients who received ECMO support in the ICU of the First Affiliated Hospital, Zhejiang University School of Medicine between January 2021 and December 2024, and who developed sepsis during ECMO support. Sepsis was diagnosed according to the Sepsis-3.0 criteria,3 defined as the presence of suspected or confirmed infection, plus an increase in the Sequential Organ Failure Assessment (SOFA) score of ≥2 points from baseline (ΔSOFA≥2).
Inclusion Criteria
- Aged between 18 and 70 years.
- ECMO support duration ≥ 24 hours after initiation.
- For patients who received multiple ECMO runs, only the data from the first ECMO run were analyzed.
Exclusion Criteria
- Absence of any thromboelastography (TEG) testing during ECMO support.
- Use of nafamostat mesylate, bivalirudin, or argatroban for anticoagulation for > 72 hours during ECMO support.
- Presence of severe bleeding prior to ECMO initiation.
- Pregnancy or lactation.
- No diagnosis of sepsis during the ECMO support period.
- Presence of severe bleeding prior to the onset of sepsis.
- Known congenital or acquired hematologic disorders (eg, hemophilia, immune thrombocytopenia), or diagnosis of heparin-induced thrombocytopenia (HIT) during ECMO support.
Major Bleeding Was Defined per ELSO criteria
- Overt bleeding with a ≥2 g/dL drop in hemoglobin over 24 hours or the need for RBC transfusion (≥10 mL/kg) 10;
- Any intracranial or retroperitoneal hemorrhage, or pulmonary hemorrhage with radiologic evidence of infiltration, or any bleeding necessitating surgical repair.
Grouping
Enrolled patients were divided into two groups based on the occurrence of major bleeding during ECMO support: the bleeding group (patients with major bleeding) and the Non-bleeding group (patients without major bleeding).
Thromboelastography (TEG) Assay
TEG analysis was performed using a TEG 5000 or TEG 6s analyzer (Haemonetics Corporation, USA) according to the manufacturer’s instructions. Fresh whole blood samples were activated with kaolin and analyzed within 4 minutes after blood collection. The following six TEG parameters were recorded:
R-value (Reaction time): representing the latency of initial fibrin formation (clotting factor activity). Reference range: 5–10 min.
K-value (Kinetics time): representing the speed of clot formation. Reference range: 1–3 min.
α-angle (Alpha angle): representing the rapidity of fibrin cross-linking and clot strengthening. Reference range: 53–72°.
MA (Maximum Amplitude): representing the ultimate strength of the clot. Reference range: 50–70 mm.
LY30 (Lysis at 30 minutes): representing the percentage of clot amplitude reduction 30 minutes after MA, indicating fibrinolysis. Reference range: 0–7.5%.
EPL (Estimated Percent Lysis): an estimated percentage of fibrinolysis. Reference range: 0–15%.
Anticoagulation Management During ECMO
In our institution, unfractionated heparin is the standard anticoagulant used during ECMO support unless contraindicated. Heparin was administered as a continuous intravenous infusion and titrated to maintain the activated partial thromboplastin time (aPTT) at approximately 1.5–2.0 times the normal value (target range: 60–80 s).
Anticoagulation intensity was primarily guided by conventional coagulation assays, while thromboelastography (TEG) was performed as an adjunctive tool rather than serving as the sole determinant for heparin dose adjustments. In the event of clinically significant bleeding or suspected over-anticoagulation, temporary dose reduction or discontinuation of heparin was considered at the treating physician’s discretion.
Data Collection
The following data were extracted from the electronic medical records:
Baseline Characteristics
Including demographic information, medical history, and admission details: age, sex, body mass index (BMI), comorbidities (eg, hypertension, diabetes), time of hospital admission, time of ICU admission, time of ECMO initiation, ECMO mode (eg, VA-ECMO, VV-ECMO), time of sepsis diagnosis, use of intra-aortic balloon pump (IABP), and use of antiplatelet medications.
Laboratory Parameters
Time point A (Pre-sepsis): During ECMO support but before the diagnosis of sepsis. Parameters included: thromboelastography (TEG) parameters (R-time, K-time, α-angle, MA, CI, EPL, LY30), hemoglobin (Hb) level, platelet count (PLT), and coagulation profile (prothrombin time [PT], activated partial thromboplastin time [aPTT], thrombin time [TT], international normalized ratio [INR], fibrinogen [Fib], and D-dimer).
Time point B (Post-sepsis): Within 24 hours after the diagnosis of sepsis. The same parameters as Time point A were collected.
Time point C (Pre-bleeding, Bleeding group only): For patients in the bleeding group, the latest available parameters before the bleeding event were collected. In our ICU, coagulation profiles and thromboelastography are routinely monitored on a daily basis in ECMO patients complicated by sepsis, with blood samples consistently collected each morning between 05:00 and 05:30. Accordingly, Time point C was defined as the most recent routinely obtained measurement within 24 hours prior to the onset of major bleeding.
Outcome Measures
The primary outcome was the occurrence of major bleeding during ECMO support. For patients who experienced bleeding, the time and anatomical site of the bleeding event were recorded.
Statistical Analysis
All statistical analyses were performed using SPSS software (Version 22.0; IBM Corp., Armonk, NY, USA). All hypothesis tests were two-sided, and a significance level (α) of 0.05 was adopted. Continuous variables were tested for normality using the Shapiro–Wilk test and are presented as median (interquartile range, IQR) since all were non-normally distributed. Comparisons between groups (Bleeding vs Non-bleeding) were made using the Mann–Whitney U-test. Comparisons of repeated measures within the same group (eg, pre- vs post-sepsis) were analyzed using the Friedman test; if the overall comparison was significant, post hoc pairwise comparisons were conducted. For paired comparisons between two time points (eg, sepsis onset vs pre-bleeding), the Wilcoxon signed-rank test was applied. Categorical variables are presented as number (percentage, %). Group differences in categorical variables were assessed using the Chi-square test or Fisher’s exact test (when more than 20% of expected cell counts were <5). A P-value of < 0.05 was considered statistically significant.
Result
A total of 418 patients received ECMO support during the study period (2021–2024). After initial screening, 127 patients were excluded for not meeting the inclusion criteria, leaving 291 patients who initially met the eligibility requirements. After applying the predefined exclusion criteria, 64 patients were finally enrolled in the study (Figure 1). Baseline characteristics at sepsis onset are presented first, followed by longitudinal changes in coagulation parameters preceding major bleeding. The reasons for exclusion were as follows: 61 patients due to the absence of TEG testing during ECMO support, 25 due to anticoagulation with nafamostat or bivalirudin for >72 hours, 12 due to pre-existing major bleeding before ECMO initiation, 123 due to no diagnosis of sepsis during ECMO, and 6 due to major bleeding occurring prior to the onset of sepsis.
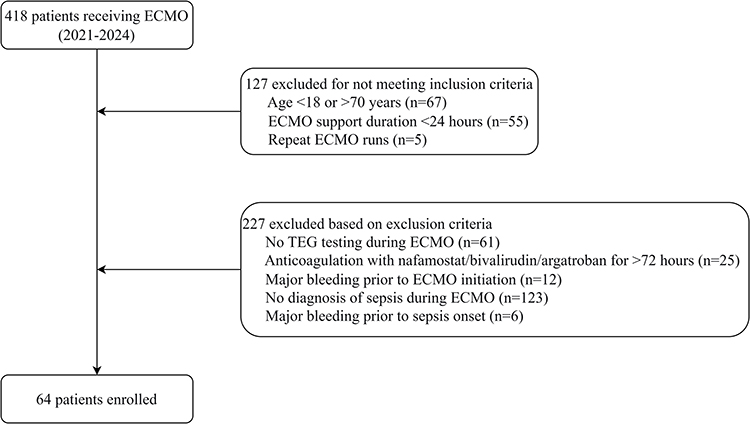 |
Figure 1 Flowchart. |
Table 1 summarizes the baseline characteristics of the 64 enrolled patients at the time of sepsis onset during ECMO support. The median age was 54 (44–60) years, and 81.3% (52/64) were male. VA-ECMO was the predominant mode (62.5%, 40/64). Twenty-three patients (35.9%) were on antiplatelet therapy. Major bleeding occurred in 26 patients (40.6%), with gastrointestinal bleeding (9.4%, 6/64) and intracranial bleeding (7.8%, 5/64) being the most common types. All patients exhibited coagulopathy at sepsis onset, as detailed by TEG and coagulation parameters in Table 1.
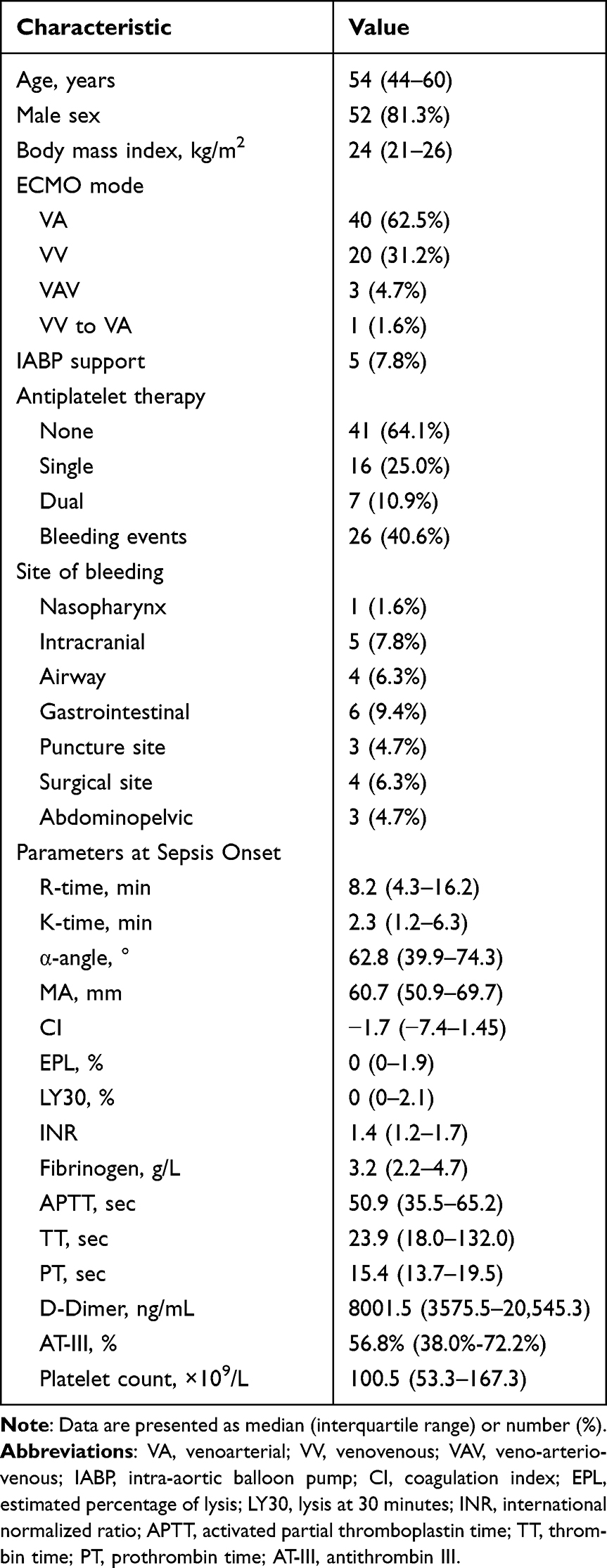 |
Table 1 Baseline and Clinical Characteristics of the Study Cohort (N=64) |
As shown in Table 2, no statistically significant differences were found between the Bleeding group (n=26) and the Non-bleeding group (n=38) in baseline parameters at sepsis onset, including demographic data, ECMO mode, use of IABP support, antiplatelet therapy, TEG parameters, coagulation profiles, and platelet counts.
 |
Table 2 Comparison of Baseline Parameters at Sepsis Onset Between Bleeding and Non-Bleeding Groups |
Dynamic assessment of the Bleeding group revealed significant changes in TEG parameters and platelet counts from sepsis onset to the pre-bleeding phase (Figure 2 and Table 3). Specifically, the R-time was significantly prolonged in the pre-bleeding phase compared with sepsis onset [10.1 (5.9–29.4) min vs 7.5 (4.0–12.5) min; P=0.03]; in parallel, platelet count was significantly decreased before bleeding events [93.5 (41.5–144.3) ×109/L vs 110.0 (56.5–224.0) ×109/L; P=0.02], highlighting a progressive temporal worsening in coagulation initiation and platelet availability prior to bleeding events. In the non-bleeding group, using a matched observation window (Day 4 after sepsis onset, based on the median 4.3-day interval from sepsis onset to the pre-bleeding sample in the bleeding group), neither R-time (P = 0.547) nor platelet count (P = 0.085) showed a statistically significant longitudinal change. These parallel analyses are provided in Supplementary Table S1.
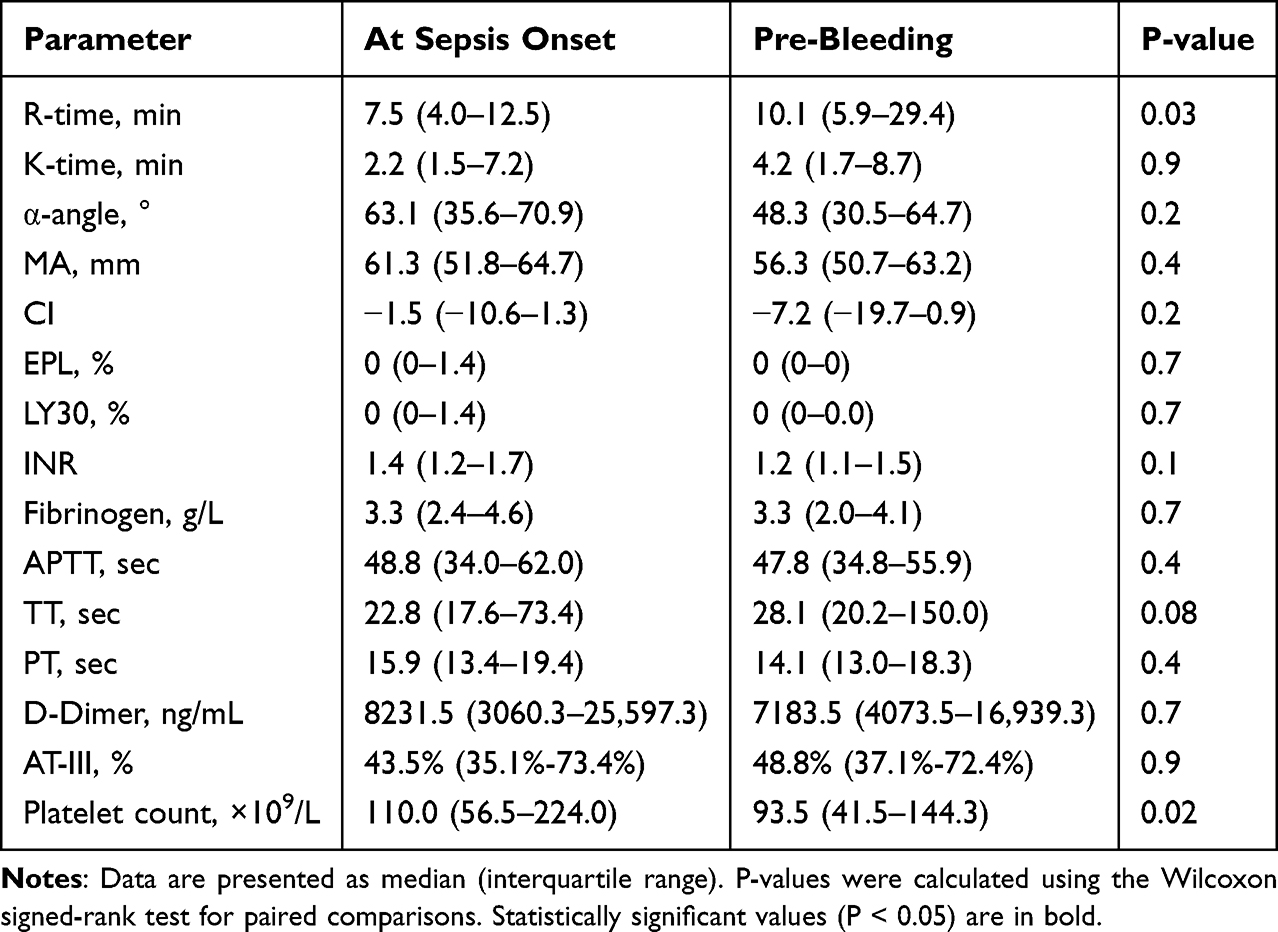 |
Table 3 Dynamic Changes in Parameters from Sepsis Onset to Pre-Bleeding Event in the Bleeding Group (n=26) |
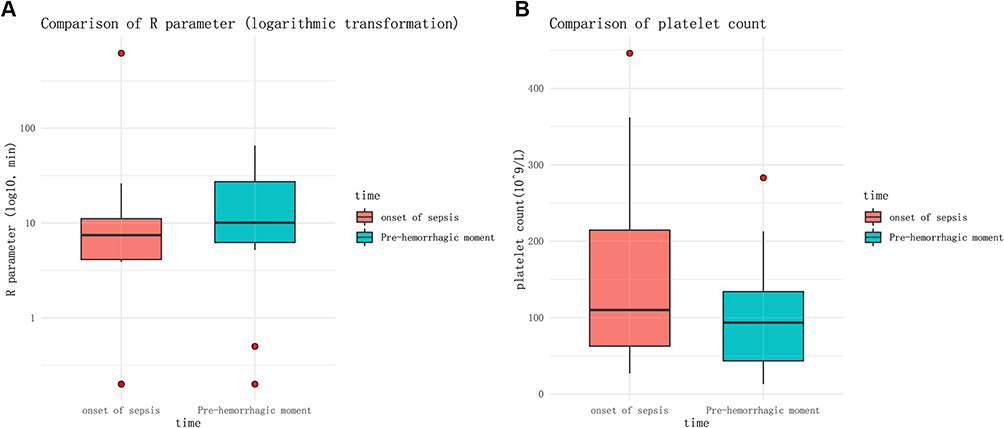 |
Figure 2 Dynamic changes in thromboelastography (TEG) R-time and platelet count in patients with bleeding. (A) R-time at sepsis onset and within 24 h prior to the bleeding event. (B) Platelet count at sepsis onset and within 24 h prior to the bleeding event. Data are presented as median (IQR). P<0.05 indicates a significant difference between time points. |
Discussion
This study aimed to investigate the factors associated with bleeding in patients who developed sepsis during extracorporeal membrane oxygenation (ECMO) support. Our results showed a bleeding incidence of 40.6%. Notably, patients in the bleeding group exhibited a significant progressive prolongation of the thromboelastography (TEG) R-time and a significant decline in platelet count from sepsis onset to the pre-bleeding phase, compared to their levels at sepsis onset. Although the absolute magnitude of these changes was modest, in the context of ECMO complicated by sepsis, where hemostasis is highly fragile and rapidly evolving, even subtle longitudinal shifts in coagulation initiation and platelet availability may reflect clinically relevant deterioration toward bleeding. Importantly, dynamic trends may provide greater warning value than isolated measurements relative to reference ranges. This combined pattern is mechanistically plausible because R-time primarily reflects the initiation phase of coagulation, driven by clotting factor activity and anticoagulant exposure, whereas platelet count represents a distinct cellular determinant of clot propagation and mechanical stability. In ECMO patients complicated by sepsis, bleeding risk is rarely attributable to a single abnormality but rather to the convergence of delayed clot initiation and impaired platelet-mediated clot strengthening. Therefore, concurrent longitudinal deterioration in these two dimensions may function as complementary early warning indicators of impending major bleeding.
Importantly, these hemostatic changes should be interpreted within the infection-specific framework of sepsis-induced coagulopathy, where pathogen-driven inflammation and dysregulated host responses can rapidly destabilize coagulation balance during ECMO support. The R-time prolongation observed in our study is comparable to findings in previous literature. A study in pediatric ECMO patients18 reported a median R-time of 9.8 minutes but did not evaluate its association with bleeding outcomes. The range of R-times (7.9–10.8 min) reported by Panigada et al13 is similar to our findings; however, that study, which had higher platelet counts (119–121 ×109/L), reported a lower incidence of major bleeding (22%). Furthermore, an RCT17 that targeted an R-time of 16–24 minutes for anticoagulation found a very high bleeding complication rate (59.5%). Collectively, these findings, along with our results, suggest that dynamic monitoring of R-time and platelet count may aid in the early identification of bleeding risk in septic patients on ECMO. Clinically, such progressive deterioration may warrant closer surveillance and individualized reassessment of anticoagulation intensity and transfusion support, although prospective validation is required before routine implementation.
Although the activated partial thromboplastin time (aPTT) is the conventional monitoring parameter for anticoagulation management during ECMO, it only reflects part of the coagulation cascade and fails to provide a comprehensive assessment of hemostatic status.17,19–21 We found no significant differences in baseline demographics, ECMO configuration, support devices, medication use, TEG parameters, or conventional coagulation assays between the bleeding and non-bleeding groups. Notably, even within the bleeding group, traditional coagulation parameters before bleeding did not differ significantly from their baseline values at sepsis onset. This indicates that the occurrence of bleeding may be more closely related to the dynamic progression of coagulopathy rather than the initial state. The significant prolongation of R-time prior to bleeding suggests that TEG may be more sensitive than conventional tests in detecting this evolving hemostatic abnormality.
Several considerations are important when interpreting these findings. To clarify whether the observed temporal deterioration in R-time and platelet count represents a bleeding-specific signal rather than a common trajectory during ECMO support, parallel longitudinal analyses were also conducted in the non-bleeding cohort and are provided in the Supplementary Materials (Supplementary Table S1). In brief, no significant longitudinal change was observed in non-bleeding patients for R-time (P = 0.547) or platelet count (P = 0.085) over the matched Day-4 window. Although the absolute magnitude of R-time prolongation and platelet decline was modest, the hemostatic balance in ECMO patients complicated by sepsis is particularly vulnerable, and even borderline dynamic shifts may precede clinically significant bleeding. From a practical perspective, these parameters should not be viewed as definitive treatment thresholds, but rather as early warning indicators that may prompt intensified surveillance, repeat viscoelastic testing, and individualized reassessment of anticoagulation intensity and supportive transfusion strategies. Prospective studies are needed to determine whether incorporating such dynamic monitoring into anticoagulation management protocols can reduce bleeding complications.
Our study has several limitations. First, this was a single-center, retrospective study with a limited sample size, which may introduce selection bias and leaves residual confounding (eg, individual variations in anticoagulant dosage) uncontrolled. Given the retrospective design and the lack of multivariable adjustment, our findings should be interpreted as associative and hypothesis-generating rather than conclusive evidence of independent prediction. Second, the timing of TEG measurements was not standardized, and the observed dynamic changes might be influenced by monitoring frequency. Future large-scale, prospective studies are warranted to validate our findings and to further investigate whether a TEG-guided individualized anticoagulation strategy can effectively reduce bleeding complications. In addition, bleeding events may also occur in ECMO patients without sepsis, and future studies should compare septic versus non-septic bleeding phenotypes to clarify sepsis-specific mechanisms.
Conclusion
In patients developing sepsis during ECMO support, bleeding events are preceded by a dynamic prolongation of TEG R-time and a progressive decrease in platelet count. Dynamic combined monitoring of TEG parameters (especially R-time) and platelet count may provide early warning indicators associated with major bleeding risk. However, these findings should be interpreted as early warning indicators rather than definitive independent predictors, intended to support risk stratification and enhanced surveillance, and should be considered hypothesis-generating, requiring confirmation in larger prospective studies before routine clinical implementation.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Consent for Publication
All listed authors consent to the submission, and all data are used with the consent of the person generating the data.
Acknowledgments
Thanks to Zhejiang University Press for the language revision of our manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Zhejiang Medical Association Clinical Research Fund Project (2016ZYC-A14), the Zhejiang Provincial Natural Science Foundation of China (No. LQ23H020004), the Medical and Health Research Project of Zhejiang province (No. 2024KY983, 2025KY783), and the Traditional Chinese Medicine Science and Technology Plan of Zhejiang province (No. 2025ZR140).
Disclosure
The authors declare that they have no competing interests.
References
1. Vogel AM, Lew DF, Kao LS, Lally KP. Defining risk for infectious complications on extracorporeal life support. J Pediatric Surg. 2011;46(12):2260–10. doi:10.1016/j.jpedsurg.2011.09.013
2. Bizzarro MJ, Conrad SA, Kaufman DA, Rycus P. Infections acquired during extracorporeal membrane oxygenation in neonates, children, and adults. Pediatric Crit Care Med. 2011;12(3):277–281. doi:10.1097/PCC.0b013e3181e28894
3. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
4. Levi M, van der Poll T. Inflammation and coagulation. Crit Care Med. 2010;38:S26–34. doi:10.1097/CCM.0b013e3181c98d21
5. Brodie D, Bacchetta M. Extracorporeal membrane oxygenation for ARDS in adults. New Engl J Med. 2011;365(20):1905–1914. doi:10.1056/NEJMct1103720
6. Paden ML, Conrad SA, Rycus PT, Thiagarajan RR. Extracorporeal life support organization registry report 2012. ASAIO J. 2013;59(3):202–210. doi:10.1097/MAT.0b013e3182904a52
7. Chung M, Cabezas FR, Nunez JI, et al. Hemocompatibility-related adverse events and survival on venoarterial extracorporeal life support: an ELSO registry analysis. JACC Heart Fail. 2020;8(11):892–902. doi:10.1016/j.jchf.2020.09.004
8. Nunez JI, Gosling AF, O’Gara B, et al. Bleeding and thrombotic events in adults supported with venovenous extracorporeal membrane oxygenation: an ELSO registry analysis. Intensive Care Med. 2022;48(2):213–224. doi:10.1007/s00134-021-06593-x
9. Bembea MM, Annich G, Rycus P, Oldenburg G, Berkowitz I, Pronovost P. Variability in anticoagulation management of patients on extracorporeal membrane oxygenation: an international survey. Pediatric Crit Care Med. 2013;14(2):e77–84. doi:10.1097/PCC.0b013e31827127e4
10. McMichael ABV, Ryerson LM, Ratano D, Fan E, Faraoni D, Annich GM. 2021 ELSO adult and pediatric anticoagulation guidelines. ASAIO J. 2022;68(3):303–310. doi:10.1097/MAT.0000000000001652
11. Müller MC, Meijers JC, Vroom MB, Juffermans NP. Utility of thromboelastography and/or thromboelastometry in adults with sepsis: a systematic review. Crit Care. 2014;18(1):R30. doi:10.1186/cc13721
12. Hartert H. Blood clotting studies with thrombus stressography; a new investigation procedure. Klinische Wochenschrift. 1948;26(37–38):577–583. doi:10.1007/BF01697545
13. Panigada M, Iapichino G, L’Acqua C, et al. Prevalence of “flat-line” thromboelastography during extracorporeal membrane oxygenation for respiratory failure in adults. ASAIO J. 2016;62(3):302–309. doi:10.1097/MAT.0000000000000325
14. Aubron C, DePuydt J, Belon F, et al. Predictive factors of bleeding events in adults undergoing extracorporeal membrane oxygenation. Ann Intens Care. 2016;6(1):97. doi:10.1186/s13613-016-0196-7
15. Combes A, Brodie D, Chen YS, et al. The ICM research agenda on extracorporeal life support. Intensive Care Med. 2017;43(9):1306–1318. doi:10.1007/s00134-017-4803-3
16. Vajter J, Volod O. Anticoagulation management during ECMO: narrative review. JHLT Open. 2025;8:100216. doi:10.1016/j.jhlto.2025.100216
17. Panigada M, Iapichino GE, Brioni M, et al. Thromboelastography-based anticoagulation management during extracorporeal membrane oxygenation: a safety and feasibility pilot study. Ann Intens Care. 2018;8(1):7. doi:10.1186/s13613-017-0352-8
18. Alexander DC, Butt WW, Best JD, Donath SM, Monagle PT, Shekerdemian LS. Correlation of thromboelastography with standard tests of anticoagulation in paediatric patients receiving extracorporeal life support. Thrombosis Res. 2010;125(5):387–392. doi:10.1016/j.thromres.2009.07.001
19. Oude Lansink-Hartgring A, de Vries AJ, Droogh JM, van den Bergh WM. Hemorrhagic complications during extracorporeal membrane oxygenation - The role of anticoagulation and platelets. J Crit Care. 2019;54:239–243. doi:10.1016/j.jcrc.2019.09.013
20. Honore PM, Barreto Gutierrez L, Kugener L, et al. Use of multiple laboratory tests including anti-factor Xa to optimally manage anticoagulation during ECMO. Crit Care. 2020;24(1):427. doi:10.1186/s13054-020-03145-5
21. Moussa MD, Soquet J, Lamer A, et al. Evaluation of anti-activated factor X activity and activated partial thromboplastin time relations and their association with bleeding and thrombosis during veno-arterial ECMO support: a retrospective study. J Clin Med. 2021;10(10):2158. doi:10.3390/jcm10102158
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.