Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Progression to Abnormal Glucose Tolerance and Its Related Risk Factors Among Women with Prior Gestational Diabetes in Rural Communities of China
Authors Mao P, Jiang S, Guo J ![]() , Jiang Y, Long Q, Tang Y, Luo J, Wiley J
, Jiang Y, Long Q, Tang Y, Luo J, Wiley J ![]() , Vorderstrasse A
, Vorderstrasse A
Received 5 March 2020
Accepted for publication 8 June 2020
Published 29 June 2020 Volume 2020:13 Pages 2259—2268
DOI https://doi.org/10.2147/DMSO.S252542
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Ping Mao,1 Shan Jiang,2 Jia Guo,2 Yuanyuan Jiang,2 Qing Long,2 Yujia Tang,2 Jiaxin Luo,2 James Wiley,3 Allison Vorderstrasse4
1Department of Nursing, Third Xiangya Hospital, Central South University, Changsha, Hunan, People’s Republic of China; 2Xiangya School of Nursing, Central South University, Changsha, Hunan, People’s Republic of China; 3School of Medicine, University of California, San Francisco, San Francisco, CA, USA; 4School of Nursing, New York University, New York, NY, USA
Correspondence: Jia Guo
Xiangya School of Nursing, Central South University, 172 Tongzipo Road, Changsha, Hunan 410013, People’s Republic of China
Tel +86 13875947418
Email [email protected]
Background: The purpose of this study was to describe the status of abnormal glucose tolerance with a longer duration after delivery among women with prior gestational diabetes mellitus (GDM) in a rural community of China, and to explore the influence of socio-demographic factors, GDM-related factors (family history of diabetes, number of children, receipt of treatment for GDM), psychosocial factors (perceived stress, self-efficacy, and social support), lifestyle behaviors (physical activity, sedentary activity, fruit or vegetables intake), and obesity indicators (body mass index and waist circumferences) on abnormal glucose tolerance.
Patients and Methods: A cross-sectional descriptive survey was conducted among women with prior GDM in two county-level hospitals in Western and Eastern Hunan, China from November 2017 to June 2018. Under the guidance of life course theory, data were collected using self-report measures of socio-demographic and GDM-related factors as well as psychosocial factors (perceived stress, self-efficacy, and social support) and postpartum lifestyle behaviors (physical activity, sedentary activity, and fruit and vegetable intake). Additionally, a 75-g oral glucose tolerance test was conducted, and weight, height, and waist circumference were measured on site.
Results: A total of 425 women were included in this study, with an average postpartum duration of 18.04 months. Of these women, 20.9% had abnormal glucose tolerance (AGT). A multivariate analysis indicated that the proportion of abnormal glucose tolerance increased with increased age (OR = 2.13; 1.27– 3.57, p=0.004), ethnic minority (OR: 1.62, 95% CI: 0.96– 2.72, p=0.069), lower educational levels (OR:0.58, 95% CI: 0.33– 1.02, p=0.057), receipt of treatment for GDM during pregnancy (OR =1.93; 1.11– 3.37, p=0.020) and larger waist circumference (OR = 1.08; 1.05– 1.12, p=0.000).
Conclusion: More than one-fifth of the women with GDM in rural China had progression to AGT. More postpartum programs aimed at reducing waist circumference are warranted to delay or prevent progression to type 2 diabetes mellitus for rural Chinese women with prior GDM.
Keywords: gestational diabetes mellitus, abnormal glucose tolerance, postpartum, risk factors, waist circumference
Introduction
The prevalence of diabetes is rising rapidly worldwide. There were 451 million people (aged (18–99 years) with diabetes as of 2017, and this number is projected to increase to increase to 693 million by 2045).1 Additionally, the age of onset of type 2 diabetes mellitus (T2DM) is decreasing across countries; almost 63% of people with diabetes are under 60 years of age.1 Among younger people with diabetes, approximately 18.4 million women were found to have had prior gestational diabetes mellitus (GDM).2 The onset of GDM is defined as the onset or first detection of any degree of glucose intolerance during pregnancy.3 The prevalence of GDM is experiencing an upward trend, with a median estimate between 5.8% and 12.9% worldwide and ranging from 6.8% to 10.4% in China.4,5
Although glucose homoeostasis is most likely to restore to non-pregnancy levels shortly after delivery among women with prior GDM, GDM is strongly associated with progression to abnormal glucose tolerance (AGT) after delivery,6 which has become an emerging health concern worldwide. AGT can appear in the form of impaired fasting glucose (IFG), impaired glucose tolerance (IGT), or T2DM. Both IFG and IGT could be used similarly to predict diabetes.3 The incidence of progression to AGT up to one year after a GDM pregnancy has been reported to be 6.7–54.0%, with up to 70% of women developing T2DM within 20 years.7,8 AGT after GDM-affected pregnancy progresses earlier in Asian countries.9 In China, women with GDM were screened 6–12 weeks postpartum and found to have an incidence of AGT ranging from 21.1% to 57.7%.10 The incidence of progression to AGT is frequent during the early postpartum period and remains stable thereafter,9 and the risk of progression to T2DM is highest during the period 3 to 6 years after the index pregnancy.8 Few studies have explored this time window of postpartum glucose tolerance of women with prior GDM.11
There are various risk factors for progression to AGT among women with histories of GDM. Maternal age and educational background have been identified as socio-demographic factors.12–14 Advanced maternal age has consistently been associated with progression to AGT among women with prior GDM.12 Additionally, women with lower educational levels are more likely to develop persistent AGT in Portuguese and South African populations.13,14 Family history of diabetes and receipt of treatment for GDM during pregnancy have also been identified as strong predictors of the development of AGT in Korea, Germany, and South Africa.14–16
As for lifestyle behaviors, physical activity and dietary patterns have direct and indirect impacts on insulin sensitivity and glucose homeostasis and have been found to be closely associated with the development of AGT after delivery among women with prior GDM.17–19 In the United States, women who increased their total physical activity levels by 7.5 MET-h/wk (equivalent to 150 minutes per week of moderate-intensity physical activity) or more had a 47% lower risk of developing T2DM.17 However, sedentary activities (sitting at work, while driving, otherwise away from home, or at home) were not related to T2DM risk.17 In Canada, increased fruit and vegetable intake was associated with a slightly lower likelihood of developing AGT among women with prior GDM.18 To our knowledge, no studies have explored the influence of physical activity, sedentary activity, and fruit and vegetable intake on the development of AGT among women with prior GDM in China.
Body mass index (BMI) and waist circumference, two obesity indicators, have been reported to be the strongest risk factors for the progression from GDM to AGT in the United States and Korea.20,21 Excess weight or abnormal fat accumulation increases peripheral insulin resistance and reduces β-cell sensitivity to glucose.22 Compared to women with normal glucose tolerance during pregnancy, women who have developed GDM are more likely to have higher BMIs and waist circumferences after delivery.23 Both BMI and waist circumference were associated with the development of T2DM among women with histories of GDM in urban China.24 Among the general population, the predictive effect of waist circumference on the development of T2DM is stronger than that of BMI.25 It is not clear whether BMI or waist circumference is a better predictor of T2DM in this high-risk population.
Psychosocial factors, such as perceived stress, self-efficacy, and social support, are associated with the development of T2DM and glycemic control.26–29 Perceived stress has been shown to predict abnormal glucose tolerance within the general population of Australia.26,27 Perceived stress have included direct neuroendocrine effects (e.g., the fact that stress hormones such as cortisol and adrenaline are counter-regulatory to insulin), and indirect effects mediated by traditional risk factors (e.g., stress may reduce the likelihood of exercising).27 The protective effects of self-efficacy and social support on glycemic control have been documented among adults with T2DM in the United States and China.28,29 Few studies have explored the effects of psychosocial risk factors on the development of AGT after delivery among women with histories of GDM.
Identifying risk factors for the progression of GDM to AGT is a necessary preliminary step toward designing diabetes prevention programs. However, to our knowledge, no studies have explored the effects of the determinants of AGT and T2DM among women with prior GDM within a theoretical framework. The life course framework has often been used to guide the exploration of factors that influence health outcomes.30 This framework encourages a focus on population disparities, including those categorized by race/ethnicity, socioeconomic status, gender, and age, and emphasizes the collective impact and influence of social environment (e.g., psychosocial factors) and individual behaviors (e.g., physical activity and diet) on health outcomes and conditions.30 The aims of this study were to describe the status of AGT with a longer duration after delivery among women with prior GDM in a rural community of China, and to explore the influence of socio-demographic factors, GDM-related factors (family history of diabetes, number of children, receipt of treatment for GDM), psychosocial factors (perceived stress, self-efficacy and social support), lifestyle behaviors (physical activity, sedentary activity, fruit or vegetables), and obesity indicators (BMI and waist circumferences) on the status of AGT with a guide of the life course framework.
Patients and Methods
Study Design and Sample
A descriptive, cross-sectional design was used in the present study. Data for this study were obtained from women with prior GDM (n = 467). Participants were recruited from two county-level hospitals in Western and Eastern Hunan, China. Participants were eligible for this study if they met the following inclusion criteria: 1) more than 18 years old, 2) history of GDM, and 3) at least six weeks postpartum. The exclusion criteria were as follows: 1) currently pregnant, 2) diabetes diagnosed before pregnancy or after delivery, 3) complication of pregnancy diagnosed during pregnancy (eg, polycystic ovary syndrome, pregnancy-induced hypertension syndrome), 4) currently taking medications that influence glucose metabolism, 5) physical or cognitive disability, 6) current addictive drug abuse, and 7) severe psychiatric disorder.
Measures
The investigator-designed questionnaire consisted of two parts: 1) socio-demographic information (age, ethnicity, educational level, employment, and monthly family income); and 2) GDM-related information (family history of diabetes, number of children, receipt of treatment for GDM, and follow-up after delivery). The age in the study was the age when the questionnaire was filled-in. The receipt of treatment for GDM including diet therapy, physical activity therapy and insulin therapy.
Perceived stress was assessed with the Chinese version of the Perceived Stress Scale (14 items). This scale was translated into Chinese by Yang and colleagues31 based on the version developed by Cohen et al.31 This scale was designed to measure the degree to which one appraises the situations in their own life as stressful. Total scores on this scale may range from 0 to 56. The criterion score for this instrument is 26, indicating increased perceived stress. Higher scores indicate more stress. This scale has been shown to have a Cronbach’s alpha coefficient of 0.78.31 The Cronbach’s alpha of the translated scale was 0.81 in the present study.
The Chinese version of the General Self-Efficacy Scale was used to measure self-efficacy with ten items. The items on the GSES are rated on a 4-point Likert scale, ranging from 1 (“not at all true”) to 4 (“exactly true”). A total score was computed for this scale by taking the mean of the scores on all items. Total scores on this scale could range from 1 to 4. A higher score indicates a higher level of general self-efficacy. The Chinese version of this scale has been shown to have an internal consistency coefficient of 0.87 and a test-retest reliability of 0.83.32 The Cronbach’s alpha of this scale was 0.88 in the present study.
The Social Support Rating Scale (SSRS, Chinese version) was used to assess social support. This scale contains ten items, measuring three dimensions of social support: subjective support (four items), objective support (three items), and support-seeking behavior (three items). Item scores on the SSRS were added together, generating a total support score ranging from 0 to 50, with higher scores indicating stronger social support. The SSRS has been used with a wide range of Chinese populations due to its high reliability and validity, with a Cronbach’s alpha ranging from 0.89 to 0.94.33 The Cronbach’s alpha of this scale was 0.87 in the present study.
Moderate to vigorous physical activity and sedentary activity status were assessed with the Chinese version of the International Physical Activity Questionnaire Short Form (IPAQ-S).34 Participants were asked to recall any moderate to vigorous physical activity they had engaged in over the past seven days and to estimate the intensity and duration of these activities (e.g., “How many days did you do vigorous physical activities like heavy lifting, digging, aerobics, or fast bicycling?” “How much time did you usually spend doing vigorous physical activities on one of those days?” and “How much time did you spend sitting on a week day?”). The IPAQ-S had intraclass correlation coefficients above 0.70.34 Moderate to vigorous physical activity was divided into two categories according to the second edition of the Physical Activity Guidelines for Americans: 1) sufficient: 150–300 minutes a week of moderate-intensity physical activity, 75–150 minutes a week of vigorous-intensity aerobic physical activity, or an equivalent combination of moderate to vigorous physical activity, and 2) insufficient: <150 minutes a week of moderate-intensity aerobic physical activity, <75 minutes a week of vigorous-intensity aerobic physical activity, or an equivalent combination of moderate to vigorous physical activity.35
Fruit and vegetable intake was assessed with one item of the Chinese version of the Canadian Diabetes Risk Assessment Questionnaire (“Do you eat vegetables or fruits every day?”). The test-retest reliability of this scale was 0.988.36 Height was measured to the nearest 0.5 cm, and weight (with an empty stomach, light indoor clothing, and no shoes) was measured with a precision of 0.1 kg. BMI was calculated by dividing body mass in kilograms by height in meters squared (kg/m2). Waist circumference was measured on a horizontal plane, midway between the inferior margin of the ribs and the superior border of the iliac crest.
A 2h 75-g oral glucose tolerance test (OGTT) was conducted after a 12-hour fast, followed by a two-hour blood sample. The 2h 75-g OGTT test is a procedure in which a standardized load of glucose is provided and plasma glucose levels are drawn at different times over a 2-h period. Plasma glucose was measured using a hexokinase enzymatic method. AGT was defined according to the following World Health Organization (WHO, 1999) criteria: isolated IFG (I–IFG): 6.1 mmol/L ≤ FPG < 7.0 mmol/L and 2-h PG < 7.8 mmol/L); isolated IGT (I–IGT): FPG < 6.1 mmol/L and 7.8 < mmol/L ≤ 2-h PG < 11.1 mmol/L; compound IFG and IGT: 6.1 mmol/L < FPG < 7.0 mmol/L and 7.8 mmol/L ≤ 2-h PG < 11.1 mmol/L; diabetes: FPG ≥ 7.0 mmol/L or 2-h glucose ≥ 11.1 mmol/L). In the present study, AGT included both prediabetes and diabetes.37
Data Collection
The medical records of women with GDM were reviewed, and the present study included those who delivered their babies at county-level hospitals (the general hospital of Youxian County in Eastern Hunan and the maternal and children’s hospital of Yongding County in Western Hunan) between January 2013 and March 2018. Potential participants who met the inclusion and exclusion criteria received phone calls from the trained local officers (physicians or nurses working at the research sites) to introduce them to the study and invite them to participate.
Data was collected between November 2017 and June 2018 at the research sites. Trained research assistants were available to answer questions and check each questionnaire for unintentionally missing items or pages. Anthropometric measures (height, weight, and waist circumference) and the 2h75-g OGTT were administered by nurses. Written informed consent forms detailing the purposes, benefits, and risks of the present study were completed by participants prior to data collection, and all participant information was kept strictly confidential.The study protocol was approved by the Ethics Committee of Xiangya School of Nursing, Central South University (No. 2016034). The study was in accordance with the Declaration of Helsinki.
Statistical Analysis
All data was double-entered and compared for accuracy using EpiData 3.0 software (The EpiData Association, Odense, Denmark). Data analysis was performed using SPSS (version 22.0; Armonk, NY, United States). For a few missing values for each variable (no more than 5%), mean substitution was used for continuous variables and mode substitution was used for categorical variables. Descriptive analysis results for continuous variables were expressed as means and standard deviations, and categorical variables were described as frequencies and percentages. Correlation analysis was used to explore the association between BMI and waist circumference.
Potential associations between the dependent variable (progression to AGT) and the independent variables (socio-demographic variables, GDM-related characteristics, psychosocial factors, lifestyle behaviors, and obesity-related anthropometric variables) were determined with one-way ANOVAs and chi-square tests. Stepwise multivariate logistic regression analysis (Forward LR) was used to explore the factors that influence progression to AGT and the time since delivery was controlled for (Enter) in the analyses. The inclusion criteria and the exclusion criteria of variables in stepwise multivariate logistic regression analysis were 0.05 and 0.10, respectively. A two-sided p < 0.05 was used to establish statistical significance and the results were expressed as odds ratios (OR) with 95% confidence intervals (CI).
A power analysis of the sample size was conducted. For a logistic regression with N = 425, a two-tailed test of the null hypothesis with an odds ratio of 1.0 for a given predictor against an alternative odds ratio of 1.70 has a power of 0.86, assuming that alpha = 0.05, the base prevalence is 0.20, and the R-squared with other predictors is 0.50 (G*Power 3.1).
Results
A total of 1890 eligible women with prior GDM were contacted by trained local officers. Of these women, 1097 (58.0%) agreed to participate; 477 of these women came to the research sites, and 467 completed the data collection process. Due to family emergencies, 40 women withdrew from the study without completing the 2h 75-g OGTT. These women were also unable to complete the questionnaires. A total of 425 women were included in this study. There was no significant difference in socio-demographic and clinical data (age, ethnicity, parity, and time after delivery) between the 425 included participants and 1645 women who did not participate in this study (ps>0.05).
Descriptions of Progression to AGT, Socio-Demographic Factors, Psychosocial Factors, GDM-Related Characteristics, Lifestyle Behaviors, and Obesity-Related Anthropometric Characteristics of Rural Women with Prior GDM
The mean age of the participants was 30.3 years (SD = 5.2). The average amount of time that had passed since delivery upon recruitment for this study were 18.04 months (SD = 12.86, median 18.31), with a range of 2 to 48 months. The average duration of time to the development of AGT for the 89 women was 17.89 months (SD = 12.87). Of all the women that participated in this study, 79.1% (n = 336) had blood glucose levels that had returned to normal and 20.9% (n = 89) had developed AGT, of which 2.6% (n = 11) had I–IFG, 9.2% (n = 39) had I–IGT, 2.8% (n = 12) had both IFG and IGT, and 6.3% (n = 27) had T2DM. Of the women whose postpartum OGTTs revealed AGT, 43.8% (39 out of 89) showed abnormalities through the 2-hour value alone and 30.3% (27 out of 89) had glucose levels indicative of T2DM. Regarding socio-demographic characteristics, more than half of the participants (n = 231, 54.4%) were of Han nationality. Approximately 25% (n = 104, 24.5%) of the participants had no more than nine years of education. Nearly 61.3% (n = 268) of the participants were employed, and 27.5% (n = 117) had monthly family incomes of ≤ 3000 yuan, below the extreme poverty level (Table 1). Regarding GDM-related characteristics, 18.6% (n = 79) of the participants had family histories of diabetes. More than three-fifths (n = 268, 63.1%) of the participants had two or more children. More than one-third (n = 270, 36.5%) of the participants did not take GDM medications during pregnancy (Table 1). Regarding psychosocial characteristics and lifestyle behaviors, the participants’ mean scores for perceived stress, self-efficacy, and social support were 24.71 (SD = 6.06), 2.56 (SD= 0.61), and 44.22 (SD = 5.70), respectively. Approximately 20% (n = 87, 20.5%) of the participants had engaged in sufficient moderate to vigorous physical activity, and approximately 70% (n = 297, 69.9%) had been sitting for no more than six hours per day. Few women (n = 84, 19.8%) ate fruits or vegetables every day (Table 2). Regarding obesity-related anthropometric characteristics, the participants’ mean postpartum BMI was 24.10 kg/m2 (SD = 3.74) and their mean waist circumference was 80.92 cm (SD = 8.75; Table 2). BMI and waist circumference were highly correlated (r = 0.832, p < 0.001); this is not shown in Table 2.
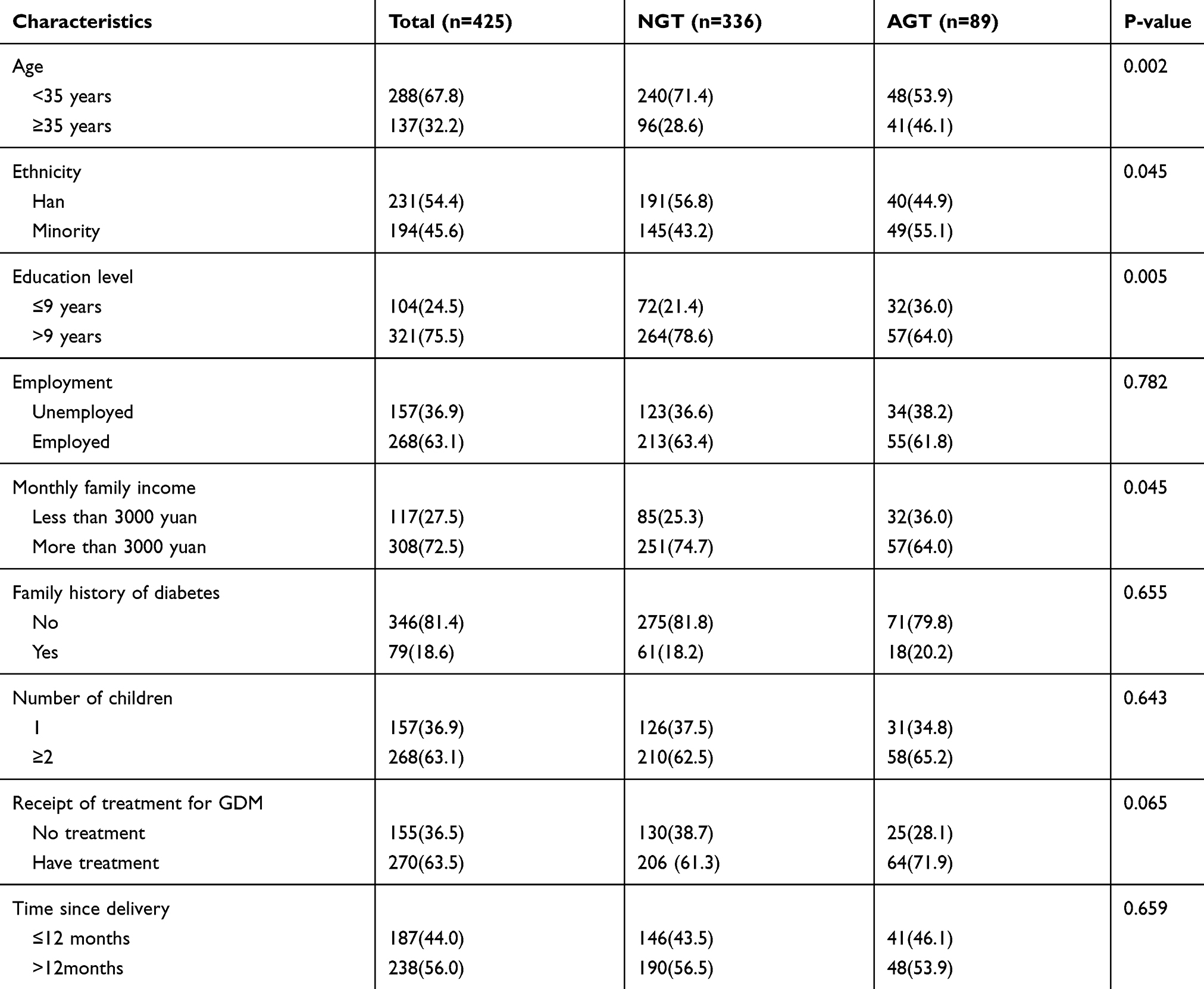 |
Table 1 Postpartum Blood Glucose Category According to Socio-Demographics and GDM-Related Characteristics of Rural Women with Prior GDM |
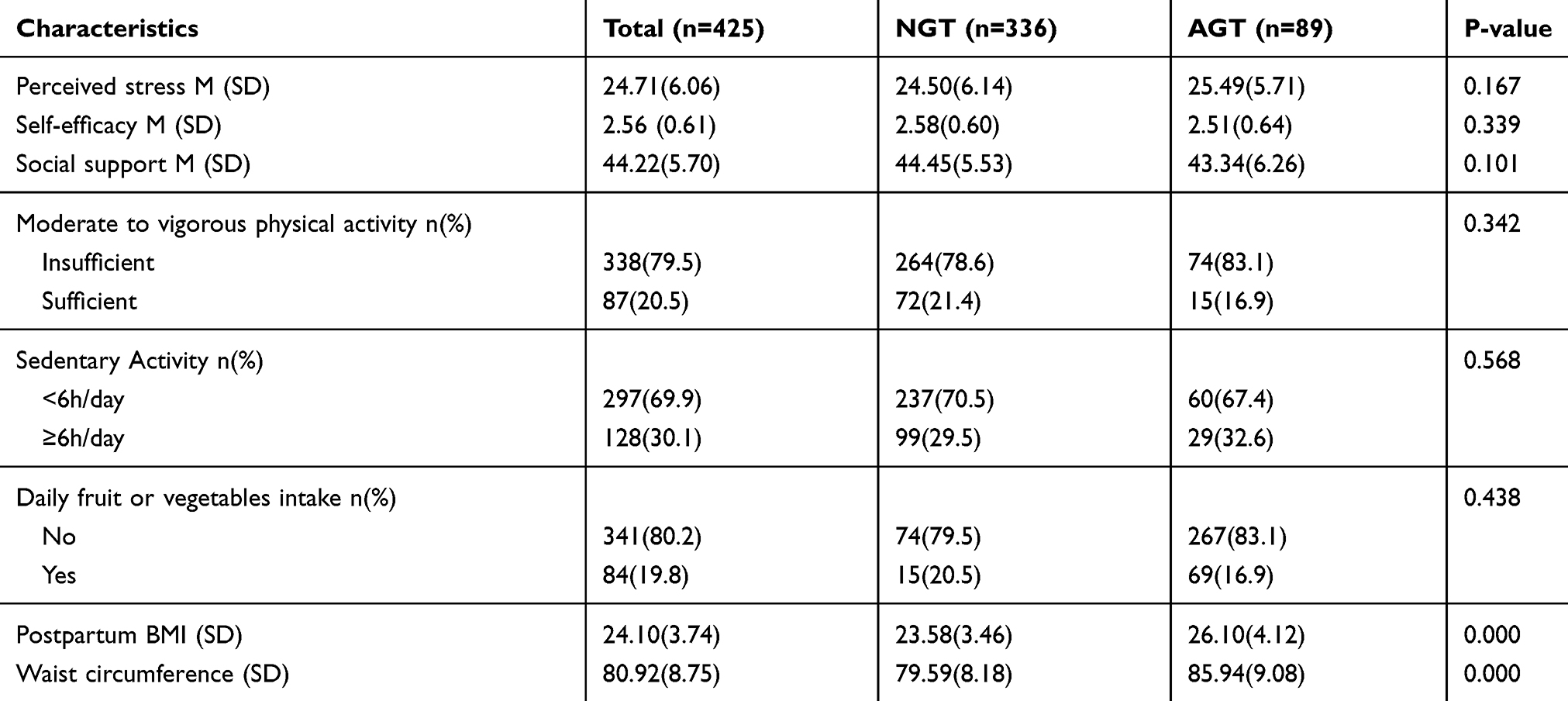 |
Table 2 Postpartum Blood Glucose Category According to Psychosocial Variables, Lifestyle Factors, and Obesity Indicators |
Bivariate Analysis for Progression to AGT Among Rural Women with Prior GDM
A comparison of the women who proceeded to AGT after GDM to those who had GDM but maintained normal glucose tolerance showed that the women with AGT tended to be significantly older (p = 0.002), to be ethnic minorities (p = 0.045), and to have lower education levels (less than 9 years of education; p =0.005). The women with AGT were more likely to report family incomes of less than 3000 yuan per month (p = 0.045). There was no statistically significant difference between the AGT group and the NGT group in terms of employment (p > 0.05).
As for GDM-related characteristics, there were no significant differences between the AGT group and the NGT group in terms of family history of diabetes, number of children, or time since delivery and receipt of treatment for GDM during pregnancy (ps > 0.05).
As for psychosocial characteristics, there were no significant differences between the two groups in terms of perceived stress, self-efficacy, or social support (ps > 0.05). As for lifestyle behaviors, there were no statistically significant differences between the two groups in terms of moderate to vigorous physical activity, sedentary activity, or daily fruit and vegetable intake (ps > 0.05). As for obesity-related anthropometric characteristics, BMI and waist circumference were significantly higher in the AGT group than in the NGT group (ps=0.000).
Multivariate Logistic Regression Results for Progression to AGT Among Rural Women with Prior GDM
The stepwise multivariate logistic regression model showed that older women (OR: 2.13, 95% CI: 1.27–3.57, p=0.004), ethnic minority women (OR: 1.62, 95% CI: 0.96–2.72, p=0.069), women with lower educational levels (OR:0.58, 95% CI: 0.33–1.02, p=0.057), women who did not receive treatment for GDM during pregnancy (OR:1.93, 95% CI: 1.11–3.37, p=0.020) and women with higher waist circumference (OR:1.08, 95% CI: 1.05–1.12, p=0.000) were at a higher risk of developing progression to AGT when controlled for the time since delivery (Table 3).
 |
Table 3 Logistic Regression of AGT Among Rural Women with Prior GDM |
Discussion
The proportion of women with AGT was 20.9%, and I–IGT was more common than other types of AGT among rural Chinese women with prior GDM during a mean follow-up period of 18 months. This study helped to fill a gap in the literature concerning the determinants of long-term abnormal glucose tolerance using a life course framework. Advanced age, receipt of treatment for GDM during pregnancy, and large waist circumference were associated with increased risk of progression to AGT, while family history of diabetes, insufficient moderate to vigorous physical activity, and high BMI do not associated with progression to AGT.
A relatively high proportion of the women participating in the present study had abnormal glucose tolerance. At a mean time of 18 months after delivery, 6.3% of the participants developed T2DM. This finding is in line with those of a study of Korean women, in which 6.9% of the participants developed T2DM at a median time of 16 months after pregnancy.38 In addition to T2DM, a high percentage of women (14.6%) exhibited pre-diabetes in the present study. This percentage was higher than the rate of pre-diabetes (10.0%) among Iranian women, who developed pre-diabetes at a mean time of 22.8 months after pregnancy.39 However, it should be noted that the cutoff value for IFG used in the present study (6.1 mmol/L) was higher than that used in the Iranian study (5.5 mmol/L).
Our findings suggested that the proportion of women with I–IGT was higher than the proportions of women with other types of AGT. This conclusion is in line with those of previous studies of women with prior GDM in Germany and Belgium.40,41 However, among Finland and Indian women with prior GDM, the majority of AGT was in the form of I–IFG.42,43 This difference could be explained by the fact that I–IFG and I–IGT represent distinct metabolic abnormalities and there might be a difference between these abnormalities across women with a history of GDM.
Similar to previous studies of other ethnic groups, the present study showed that advanced age, ethnic minority status, and low educational level are risk factors for progression to AGT among women with prior GDM.13,14,21 However, women with minority nationalities were also at a higher risk of developing AGT in the present study; this result was inconsistent with the results of a previous study in China.10 Given nearly half of the participants (45.6%) in the present study were ethnic minorities, there likely was adequate power to detect a difference. Women with less than nine years of education were also more likely to develop AGT in the present study; this result was in line with the results of studies of Portuguese women at six-week follow-up and studies of South African women with prior GDM at five-to-six-year follow-up.13,14 Receipt of treatment for GDM during pregnancy was significantly associated with the progress from prior GDM to AGT among women in rural China. This finding was consistent with the findings of previous studies.14,16 Receipt of treatment for GDM during pregnancy, especially insulin treatment, could be a vital indicator of the severity of metabolic abnormalities.13 There was no statistically significant association between family history of diabetes and progression to AGT. This finding is not consistent with a study among women with prior GDM in northern France.44 It might be because the relationship between family history of diabetes and development of diabetes was more likely to be found in the women who have already developed T2DM in advanced age. Psychosocial factors (perceived stress, self-efficacy, and social support) did not influence the progression from GDM to AGT in the participants of the present study. Additionally, there were no statistically significant associations between lifestyle behaviors (moderate to vigorous physical activity, sedentary activity, and fruit and vegetable intake) and progression to AGT. This finding was inconsistent with the findings of studies of the United States and Canada.17,18 Other factors may contribute to AGT development within women with a history of GDM. For example, the severity of hyperglycemia during pregnancy has been shown to be associated with progression to AGT.9 Waist circumference has a stronger association with an increased risk of AGT progression among women with prior GDM, while BMI was not. This result was consistent with the results of studies of women in urban China one to five years after pregnancy and studies of women in Korea six years after pregnancy.21,24 The superiority of waist circumference over BMI could be interpreted to mean that waist circumference mainly measures abdominal fat, reflecting visceral fat, which is the most important fat deposit in terms of its effects on cardiovascular risk and T2DM.45 BMI is indiscriminate in that it includes both fat mass and muscle mass.46 In other words, the development of AGT in women with prior GDM may be more likely to correlate with higher subcutaneous fat mass.
Limitations
This review had some limitations. First, the range of postpartum duration varied, the according variation in obesity indicators might affect their glucose metabolism. Second, all of the participants were recruited from two hospitals of two rural communities of Central South China, this may have limited the generalizability of the results to women in rural China.
Implications
Women with prior GDM should be informed of the future risk of T2DM upon diagnosis of GDM, as it is important for them to monitor their glucose levels regularly after delivery. More attention should be paid to the procession of AGT from GDM to progression to AGT in this high-risk group (e.g., advanced age, and receipt of treatment for GDM during pregnancy). Fortunately, waist circumference is a modifiable risk factor for progression to AGT, and women with higher waist circumferences should be provided with strategies to reduce this factor.
Studies on the influences of prenatal factors (eg, severity of hyperglycemia during pregnancy) on progression to AGT across different areas in China are recommended. Intervention studies of women with histories of GDM with longer follow-up periods are also indicated to further verify the effect of waist circumference reduction on risk of developing progression to AGT. The low response rate of 22.5% in this study indicates that other recruitment strategies needed to be explored among these young mothers with prior GDM.
Conclusion
Progression to AGT occurs frequently in women with GDM in rural communities in Central South of China. Nurses should place more focus on postpartum blood glucose metabolism in treating women who are older, have received treatment for GDM during pregnancy, or have higher waist circumference. More postpartum programs are indicated to identify and reduce modifiable risk factors among women with prior GDM in rural communities of Central South China.
Acknowledgments
This study was funded by China Medical Board (Grant Number: 16-256) and Technology Innovation Guidance Plan Project of Hunan Province (Grant Number: 2018ZK4032).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Federation ID. IDF Diabetes Atlas.
2. Cho NH, Shaw JE, Karuranga S, et al. IDF diabetes atlas: global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract. 2018;138:271–281. doi:10.1016/j.diabres.2018.02.023
3. Association AD14. Management of diabetes in pregnancy: standards of medical care in diabetes-2019. Diabetes Care. 2019;42(Suppl 1):S165–S172. doi:10.2337/dc19-S014
4. Zhu Y, Zhang C. Prevalence of gestational diabetes and risk of progression to Type 2 diabetes: a global perspective. Curr Diab Rep. 2016;16(1):7. doi:10.1007/s11892-015-0699-x
5. Wu L, Han L, Zhan Y, et al. Prevalence of gestational diabetes mellitus and associated risk factors in pregnant Chinese women: a cross-sectional study in Huangdao, Qingdao, China. Asia Pac J Clin Nutr. 2018;27(2):383–388. doi:10.6133/apjcn.032017.03
6. Pastore I, Chiefari E, Vero R, Brunetti A. Postpartum glucose intolerance: an updated overview. Endocrine. 2018;59(3):481–494. doi:10.1007/s12020-017-1388-0
7. Nouhjah S, Shahbazian H, Amoori N, et al. Postpartum screening practices, progression to abnormal glucose tolerance and its related risk factors in Asian women with a known history of gestational diabetes: a systematic review and meta-analysis. Diabetes Metab Syndr. 2017;11(Suppl 2):S703–S712. doi:10.1016/j.dsx.2017.05.002
8. Benhalima K, Lens K, Bosteels J, Chantal M. The risk for glucose intolerance after gestational diabetes mellitus since the Introduction of the IADPSG criteria: a systematic review and meta-analysis. J Clin Med. 2019;8:9. doi:10.3390/jcm8091431
9. Moon JH, Kwak SH, Jang HC. Prevention of type 2 diabetes mellitus in women with previous gestational diabetes mellitus. Korean J Intern Med. 2017;32(1):26–41. doi:10.3904/kjim.2016.203
10. Zhang DD, Gao Q, Bai F, Li FB. Influencing factors of postpartum glucose abnormalities among gestational diabetes women. Chin J Fam Plan. 2015;23:376–379.
11. Li W, Zhang S, Liu H, et al. Different associations of diabetes with beta-cell dysfunction and insulin resistance among obese and nonobese Chinese women with prior gestational diabetes mellitus. Diabetes Care. 2014;37(9):2533–2539. doi:10.2337/dc14-0573
12. Rayanagoudar G, Hashi AA, Zamora J, et al. Quantification of the type 2 diabetes risk in women with gestational diabetes: a systematic review and meta-analysis of 95,750 women. Diabetologia. 2016;59(7):1403–1411. doi:10.1007/s00125-016-3927-2
13. Gante I, Ferreira AC, Pestana G, et al. Maternal educational level and the risk of persistent post-partum glucose metabolism disorders in women with gestational diabetes mellitus. Acta Diabetol. 2018;55(3):243–251. doi:10.1007/s00592-017-1090-y
14. Chivese T, Norris SA, Levitt NS. Progression to type 2 diabetes mellitus and associated risk factors after hyperglycemia first detected in pregnancy: a cross-sectional study in Cape Town, South Africa. PLoS Med. 2019;16(9):e1002865. doi:10.1371/journal.pmed.1002865
15. Kim SH, Kim MY, Yang JH, et al. Nutritional risk factors of early development of postpartum prediabetes and diabetes in women with gestational diabetes mellitus. Nutrition. 2011;27(7–8):782–788. doi:10.1016/j.nut.2010.08.019
16. Lobner K, Knopff A, Baumgarten A, et al. Predictors of postpartum diabetes in women with gestational diabetes mellitus. Diabetes. 2006;55(3):792–797. doi:10.2337/diabetes.55.03.06.db05-0746
17. Bao W, Tobias DK, Bowers K, et al. Physical activity and sedentary behaviors associated with risk of progression from gestational diabetes mellitus to type 2 diabetes mellitus: a prospective cohort study. JAMA Intern Med. 2014;174(7):1047–1055. doi:10.1001/jamainternmed.2014.1795
18. Mercier R, Perron J, Weisnagel SJ, Robitaille J. Associations between fruit and vegetables intake and abnormal glucose tolerance among women with prior gestational diabetes mellitus. Eur J Nutr. 2019;58(2):689–696. doi:10.1007/s00394-018-1669-2
19. Imamura F, Micha R, Wu JH, et al. Effects of saturated fat, polyunsaturated fat, monounsaturated fat, and carbohydrate on glucose-insulin homeostasis: a systematic review and meta-analysis of randomised controlled feeding trials. PLoS Med. 2016;13(7):e1002087. doi:10.1371/journal.pmed.1002087
20. Bao W, Yeung E, Tobias DK, et al. Long-term risk of type 2 diabetes mellitus in relation to BMI and weight change among women with a history of gestational diabetes mellitus: a prospective cohort study. Diabetologia. 2015;58(6):1212–1219. doi:10.1007/s00125-015-3537-4
21. Cho NH, Jang HC, Park HK, Cho YW. Waist circumference is the key risk factor for diabetes in Korean women with history of gestational diabetes. Diabetes Res Clin Pract. 2006;71(2):177–183. doi:10.1016/j.diabres.2005.06.003
22. Tzanetakou IP, Katsilambros NL, Benetos A, Mikhailidis DP, Perrea DN. “Is obesity linked to aging?”: adipose tissue and the role of telomeres. Ageing Res Rev. 2012;11(2):220–229. doi:10.1016/j.arr.2011.12.003
23. Ratner RE. Prevention of type 2 diabetes in women with previous gestational diabetes. Diabetes Care. 2007;30(Suppl 2):S242–5. doi:10.2337/dc07-s223
24. Wang L, Liu H, Zhang S, et al. Obesity index and the risk of diabetes among Chinese women with prior gestational diabetes. Diabet Med. 2014;31(11):1368–1377. doi:10.1111/dme.12532
25. Mirzaei M, Khajeh M. Comparison of anthropometric indices (body mass index, waist circumference, waist to hip ratio and waist to height ratio) in predicting risk of type II diabetes in the population of Yazd, Iran. Diabetes Metab Syndr. 2018;12(5):677–682. doi:10.1016/j.dsx.2018.04.026
26. Williams ED, Magliano DJ, Tapp RJ, Oldenburg BF, Shaw JE. Psychosocial stress predicts abnormal glucose metabolism: the Australian Diabetes, Obesity and Lifestyle (AusDiab) study. Ann Behav Med. 2013;46(1):62–72. doi:10.1007/s12160-013-9473-y
27. Harris ML, Oldmeadow C, Hure A, et al. Stress increases the risk of type 2 diabetes onset in women: a 12-year longitudinal study using causal modelling. PLoS One. 2017;12(2):e0172126. doi:10.1371/journal.pone.0172126
28. Chlebowy DO, Garvin BJ. Social support, self-efficacy, and outcome expectations: impact on self-care behaviors and glycemic control in Caucasian and African American adults with type 2 diabetes. Diabetes Educ. 2006;32(5):777–786. doi:10.1177/0145721706291760
29. Shao Y, Liang L, Shi L, Wan C, Yu S. The effect of social support on glycemic control in patients with Type 2 diabetes mellitus: the mediating roles of self-efficacy and adherence. J Diabetes Res. 2017;2017:2804178. doi:10.1155/2017/2804178
30. Office of Disease Prevention and Health Promotion, U.S. Department of Health and Human Services. Healthy People 2020. Washington (DC): DHHS; 2010. Available from http://www.healthypeople.gov/2020/topicsobjectives2020/pdfs/hp2020_brochure.pdf.
31. Yang TZ, Huang HT. An epidemiological study on stress among urban residents in social transition period. Chin J Epidemiol. 2003;11–15.
32. Zhang JX, Schwarzer R. Measuring optimistic self-beliefs: a Chinese adaptation of the General Self-Efficacy Scale. Psychologia Int J Psychol Orient. 1995;38(3):174–181.
33. Xiao SY. Theoretical basis and application in research of social support rating scale. J Clin Psychol. 1994;98–100.
34. Qu NN, Li KJ. Study on the reliability and validity of international physical activity questionnaire (Chinese Vision IPAQ). Chin J Epidemiol. 2004;87–90.
35. Piercy KL, Troiano RP, Ballard RM, et al. The physical activity guidelines for Americans. JAMA. 2018;320(19):2020–2028. doi:10.1001/jama.2018.14854
36. Guo J, Shi Z, Chen JL, et al. Translation and validation of the Canadian diabetes risk assessment questionnaire in China. Public Health Nurs. 2017;(Suppl 1).
37. Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med. 1998;15(7):539–553. doi:10.1002/(SICI)1096-9136(199807)15:7<539::AID-DIA668>3.0.CO;2-S
38. Yang SJ, Hwang SY, Baik SH, et al. Serum magnesium level is associated with type 2 diabetes in women with a history of gestational diabetes mellitus: the Korea National Diabetes Program study. J Korean Med Sci. 2014;29(1):84–89. doi:10.3346/jkms.2014.29.1.84
39. Valizadeh M, Alavi N, Mazloomzadeh S, Piri Z, Amirmoghadami H. The risk factors and incidence of type 2 diabetes mellitus and metabolic syndrome in women with previous gestational diabetes. Int J Endocrinol Metab. 2015;13(2):e21696. doi:10.5812/ijem.21696
40. Schaefer-Graf UM, Klavehn S, Hartmann R, et al. How do we reduce the number of cases of missed postpartum diabetes in women with recent gestational diabetes mellitus? Diabetes Care. 2009;32(11):1960–1964. doi:10.2337/dc09-0627
41. Benhalima K, Van Crombrugge P, Moyson C, et al. Prediction of glucose intolerance in early postpartum in women with gestational diabetes mellitus based on the 2013 WHO criteria. J Clin Med. 2019;8:3. doi:10.3390/jcm8030383
42. Huopio H, Hakkarainen H, Paakkonen M, et al. Long-term changes in glucose metabolism after gestational diabetes: a double cohort study. BMC Pregnancy Childbirth. 2014;14(1):296. doi:10.1186/1471-2393-14-296
43. Goyal A, Gupta Y, Kalaivani M, et al. Long term (>1year) postpartum glucose tolerance status among Indian women with history of Gestational Diabetes Mellitus (GDM) diagnosed by IADPSG criteria. Diabetes Res Clin Pract. 2018;142:154–161. doi:10.1016/j.diabres.2018.05.027
44. Vambergue A, Dognin C, Boulogne A, et al. Increasing incidence of abnormal glucose tolerance in women with prior abnormal glucose tolerance during pregnancy: DIAGEST 2 study. Diabet Med. 2008;25(1):58–64. doi:10.1111/j.1464-5491.2007.02306.x
45. Kramer H, Shoham D, McClure LA, et al. Association of waist circumference and body mass index with all-cause mortality in CKD: the REGARDS (Reasons for Geographic and Racial Differences in Stroke) Study. Am J Kidney Dis. 2011;58(2):177–185. doi:10.1053/j.ajkd.2011.02.390
46. Evans PD, McIntyre NJ, Fluck RJ, McIntyre CW, Taal MW. Anthropomorphic measurements that include central fat distribution are more closely related with key risk factors than BMI in CKD stage 3. PLoS One. 2012;7(4):e34699. doi:10.1371/journal.pone.0034699
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.