Back to Journals » Stem Cells and Cloning: Advances and Applications » Volume 8
Progress toward curing HIV infection with hematopoietic cell transplantation
Authors Petz LD, Burnett J, Li H, Li S, Tonai R, Bakalinskaya M, Shpall E, Armitage S, Kurtzberg J, Regan D, Clark P, Querol S, Gutman J, Spellman S, Gragert L, Rossi J
Received 11 March 2015
Accepted for publication 24 April 2015
Published 28 July 2015 Volume 2015:8 Pages 109—116
DOI https://doi.org/10.2147/SCCAA.S56050
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Bernard Binetruy
Lawrence D Petz,1 John C Burnett,2 Haitang Li,3 Shirley Li,3 Richard Tonai,1 Milena Bakalinskaya,4 Elizabeth J Shpall,5 Sue Armitage,6 Joanne Kurtzberg,7 Donna M Regan,8 Pamela Clark,9 Sergio Querol,10 Jonathan A Gutman,11 Stephen R Spellman,12 Loren Gragert,13 John J Rossi2
1StemCyte International Cord Blood Center, Baldwin Park, CA, USA; 2Department of Molecular and Cellular Biology, Irell and Manella Graduate School of Biological Sciences, 3Department of Molecular and Cellular Biology, Beckman Research Institute, City of Hope, Duarte, CA, USA; 4CCR5-Δ32/Δ32 Research Department, StemCyte International Cord Blood Center, Baldwin Park, CA, USA; 5Department of Stem Cell Transplantation, University of Texas MD Anderson Cancer Center, Houston, TX, USA; 6MD Anderson Cord Blood Bank, Department of Stem Cell Transplantation, University of Texas MD Anderson Cancer Center, Houston, TX, USA; 7Carolinas Cord Blood Bank, Duke University Medical Center, Durham, NC, USA; 8St Louis Cord Blood Bank, SSM Cardinal Glennon Children's Medical Center, St Louis, MO, USA; 9Enhance Quality Consulting Inc., Oviedo, FL, USA; 10Cell Therapy Service and Cord Blood Bank, Banc de Sang i Teixits, Barcelona, Spain; 11BMT/Hematologic Malignancies, University of Colorado, Aurora, CO, USA; 12Immunobiology and Observational Research, CIBMTR, Minneapolis, MN, USA; 13National Marrow Donor Program/Be The Match, Minneapolis, MN, USA
Abstract: HIV-1 infection afflicts more than 35 million people worldwide, according to 2014 estimates from the World Health Organization. For those individuals who have access to antiretroviral therapy, these drugs can effectively suppress, but not cure, HIV-1 infection. Indeed, the only documented case for an HIV/AIDS cure was a patient with HIV-1 and acute myeloid leukemia who received allogeneic hematopoietic cell transplantation (HCT) from a graft that carried the HIV-resistant CCR5-Δ32/Δ32 mutation. Other attempts to establish a cure for HIV/AIDS using HCT in patients with HIV-1 and malignancy have yielded mixed results, as encouraging evidence for virus eradication in a few cases has been offset by poor clinical outcomes due to the underlying cancer or other complications. Such clinical strategies have relied on HIV-resistant hematopoietic stem and progenitor cells that harbor the natural CCR5-Δ32/Δ32 mutation or that have been genetically modified for HIV-resistance. Nevertheless, HCT with HIV-resistant cord blood remains a promising option, particularly with inventories of CCR5-Δ32/Δ32 units or with genetically modified, human leukocyte antigen-matched cord blood.
Keywords: curing HIV infection, hematopoietic cell transplantation, genetic modification of stem cells, CCR5 mutation, CCR5-Δ32/Δ32 cord blood inventory
Introduction and background
Antiretroviral therapy (ART) inhibits various stages in the viral life cycle, reduces the rates of transmission, and improves life expectancy. Unfortunately, ART is non-curative, and nearly all HIV-infected individuals must adhere to daily drug regimens for the entirety of their lives. This requirement indefinitely prolongs issues such as drug resistance, adverse effects, and cost.1 While ART extends and improves the quality of life, it does not fully restore health. Individuals on ART can experience chronic inflammation, immunosenescence, bone density loss, premature aging, and increased non-AIDS morbidity and mortality.2 ART treatment interruptions in aviremic HIV-infected individuals lead to rapid viral recrudescence that reaches pretreatment levels.3 Thus, suppression of viral replication with ART does not eradicate the virus, as long-lived resting memory CD4+ T-cells can harbor latent virus, and while various reservoirs may produce low-levels of virus, such as microglia and astrocytes in the central nervous system, tissue-derived dendritic cells, macrophages, and natural killer cells.4 Further complicating matters, latently infected T-cells may undergo clonal expansion by homeostatic proliferation,5 while infected T-cells and macrophages can persist without undergoing apoptosis or cytotoxic T-lymphocytes (CTL)-induced killing.6,7
Due to persistence of infection during ART, alternative therapeutic strategies are being explored to establish a cure for HIV-1. Current and emerging approaches to eradicate HIV include transplanting virus-resistant hematopoietic stem and progenitor cells (HSPCs) in an effort to generate an HIV-resistant immune system. To achieve HIV resistance, much focus has been placed on natural mutation of or engineered inhibition of the endogenous chemokine receptor CCR5.8 Owing to the role of CCR5 as a co-receptor for HIV entry in CCR5+ CD4+ T-cells, homozygous carriers of a 32-bp deletion in the CCR5 gene (CCR5-Δ32/Δ32) are naturally resistant to HIV.9,10 As an alternative to using allogeneic CCR5-Δ32/Δ32 HSPCs from human leukocyte antigen (HLA)-matched adult or cord blood donors who have this homozygous mutation, genome editing or gene therapy strategies aim to use therapeutic genes that disrupt CCR5 genetically or post-transcriptionally, respectively.
Cure of HIV infection with hematopoietic cell transplantation (HCT)
The only known cure of HIV infection has resulted from HCT. This has been accomplished by Hütter et al11 with HCT using peripheral blood stem cells from an HLA-matched adult donor who had the CCR5-Δ32/Δ32 mutation. The patient has remained without any evidence of HIV infection for more than 8 years after discontinuation of antiretroviral drug therapy, and the consensus is that he has been cured.
However, identifying a HLA-matched adult CCR5-Δ32/Δ32 donor for a given patient is not readily feasible in part because the prevalence of the homozygous variant allele is only about 0.8%–1% of individuals of northern European descent12,13 and much less in other ethnic groups.14 Further, when an adult donor is used for a HCT, a very close HLA match between donor and patient is required. Accordingly, finding an adult donor who has a very close HLA match to a patient in need of a transplant and who is also homozygous for the CCR5-Δ32 allele is extremely difficult and will only rarely be possible. In contrast, cord blood CCR5-Δ32/Δ32 units provide a major advantage in that much less stringent HLA matching is required between donor and patient.15
Since donor–recipient HLA matching for a cord blood transplant is much less stringent,15 it is evident that cure of HIV infections by HCT can be much more easily accomplished by using stem cells obtained from a modestly sized inventory of cryopreserved CCR5-Δ32/Δ32 cord blood units. Such an inventory has been developed at StemCyte International Cord Blood Center and is available for use for appropriate patients.
HCT using CCR5-Δ32/Δ32 cord blood units
Units from StemCyte’s inventory of CCR5-Δ32/Δ32 cord blood units have been used for allogeneic HCT in patients with HIV infection. One of the transplants was performed by Dr Rafael F Duarte in Barcelona, Spain using dual haploidentical/cord blood transplantation in a patient with diffuse large B-cell lymphoma and HIV infection.16 Neutrophil engraftment, derived from the haploidentical donor, occurred on day +11. The cord blood was found to have a poor clonogenic capacity, and donor switch to cord blood origin failed, with a persistently low cord blood chimera of <5% for up to 7 weeks. A second CCR5-δ32/δ32 cord blood was infused on day +52, leading to a very rapid increase in chimerism which was from the first cord blood unit and which reached 100% by day +73. At this point, the patient’s hematopoiesis, including CD4+ T-lymphocytes, became CCR5-Δ32/Δ32. Ultrasensitive plasma viral load analysis decreased soon after HCT, reaching minimal levels at the time of full cord blood chimerism. No HIV-1 DNA was detected using droplet digital polymerase chain reaction quantification or semiquantitative tests of amplification. Importantly, although recipient CD4+ T-cells responded to proliferation and activation stimuli, they were resistant to infection by the patient’s isolate as well as by laboratory-adapted HIV-1 strains. Unfortunately, the patient developed an aggressive diffuse large B-cell lymphoma progression, and following very rapid clinical deterioration, died from disease progression 3 months after HCT.16
In addition, as testing of cord blood units for the CCR5 mutation was being carried out, a HCT using a unit that was subsequently determined to be CCR5-Δ32/Δ32 was provided to an adult patient with acute myelogenous leukemia who was not infected with HIV. This unit was transplanted as part of a double cord blood transplant. This unexpected event provided the opportunity to collect post-transplant data, which indicated engraftment of the CCR5-Δ32/Δ32 unit as the “winning unit”. At a time when evaluation of chimerism indicated 100% engraftment by the CCR5-Δ32/Δ32 unit, the patient’s peripheral blood mononuclear cells showed no significant HIV replication with in vitro infection with either of the laboratory strains of HIV-1, BAL (CCR5 tropic), or NL4-3 (CXCR tropic) compared with a normal control.17
Thus, in the only two instances in which we have had an opportunity to test the post-transplant blood specimens of patients who were engrafted with CCR5-Δ32/Δ32 cord blood cells, the patients’ cells in vitro were found to be resistant to infection by HIV.16,17 It is possible that the HIV-infected patient was cured of HIV; unfortunately, his death three months following the transplant prevented definitive evaluation of a possible cure. Nevertheless, these data strongly support the use of cord blood as a platform for broader application of this curative technology to other HIV-1 infected individuals.
An additional HCT was performed in Utrecht, the Netherlands, using a cord blood unit from StemCyte’s inventory of CCR5-Δ32/Δ32 units. The patient was a 53-year-old male patient with high-risk myelodysplastic syndrome and HIV infection. A dual haploidentical/cord blood HCT using a CCR5-Δ32/Δ32 cord blood unit was performed after myeloablative conditioning.18 The patient achieved neutrophil and platelet engraftment as well as full cord blood chimerism. However, the patient developed a severe lung infection and a relapse of the underlying disorder and died 2 months after the HCT. Analyses of viral and immunological compartments are pending.
A separate CCR5-Δ32/Δ32 cord blood transplantation, which did not involve the StemCyte inventory, was performed at the University of Minnesota with a CCR5-Δ32/Δ32 cord blood unit.19 The patient was a 12-year-old male with HIV and acute lymphoblastic leukemia. Poor HLA-matching may have contributed to the fact that the patient died as a result of graft-versus-host disease 3 months following the transplant.
HCT using CCR5-Δ32/Δ32 units from adults
In addition to the Berlin patient, two other HIV/AIDS patients with malignancy have been transplanted using adult CCR5-Δ32/Δ32 stem cells that were from an HLA-mismatched unrelated donor or an HLA-matched related donor. The patients died of infection within 4 months.19 Also, a patient who carried a detectable fraction of CXCR4-tropic virus was transplanted with a CCR5-Δ32/Δ32 HLA-matched unrelated unit.20 The patient discontinued ART before the initiation of myeloablative treatment but resumed therapy 3 weeks after transplantation because of a rebound of 93,300 copies of HIV RNA per milliliter. The genotypic analysis of HIV-1 variants in this case showed a shift from a dominantly R5-tropic HIV before transplantation toward a CXCR4-tropic HIV after transplantation. It is unclear whether the coreceptor switch took place before the allogeneic transplant or after transplantation in the absence of retroviral drugs.20 Nevertheless, this suggests the possibility that viral escape mechanisms might jeopardize CCR5-knockout strategies to control HIV infection. The patient died 12 months after transplant of relapse of non-Hodgkin’s lymphoma.
Materials and methods
Developing an inventory of CCR5-Δ32/Δ32 cord blood units
Testing of large numbers of samples requires the collaboration of multiple cord blood banks since no single bank has enough units. Specimens for testing were obtained from StemCyte International Cord Blood Center (hereafter referred to as StemCyte) and collaborating cord blood banks: MD Anderson Cancer Center Cord Blood Bank; the Carolinas Cord Blood Bank at Duke University; the St Louis Cord Blood Bank; the Sydney, Australia Cord Blood Bank; the Barcelona, Spain Cord Blood Bank; and the University of Colorado Cord Blood Bank.
Details of the methods used to identify specimens that are CCR5-Δ32/Δ32 have been reported earlier.17
Projections of the probability of finding an appropriately HLA-matched cord blood unit with an adequate cell dose for a patient in need of a HCT
HLA match rates for an inventory of 300 CCR5-Δ32/Δ32 cord blood units were estimated with a population of HLA haplotype frequencies using a population genetic model developed by Gragert et al previously applied to project match rates for the Be the Match Registry® operated by the National Marrow Donor Program.21 The dose requirement for cord blood HCT was incorporated into the model by calculating the percentage of cords with the commonly used minimum adequate total nucleated cells (TNC) dose of 2.5×107/kg for each simulated patient based on his or her weight and considered matched units with inadequate dose as unavailable. More recently, data published by Liu et al,22,23 Van Besien et al,24 and Kwon et al25,26 indicate that a lower minimum cord blood cell dose is adequate when a combined haploidentical and cord blood transplantation is performed. Accordingly, similar projections were also carried out using a minimum cell dose of 1×107/kg. The CCR5-Δ32/Δ32 units in the special inventory are primarily from white donors, and it is true that patients in need of transplantation more commonly find a matched donor from among those in their own ethnic group. To assess match rates for minority populations, we simulated 10,000 African American, Hispanic American, and Chinese American patients searching European origin cord inventory replicates (Table 1).
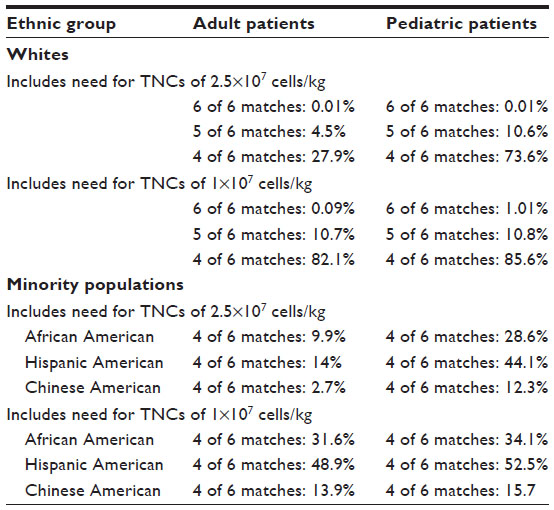 | Table 1 Projected HLA match rates with a 300 unit inventory of CCR5-δ32/δ32 cord blood units |
Genetic modification of stem cells
Due to rarity of the CCR5-Δ32/Δ32 mutation, strategies to engineer HIV resistance in CD34+ HSPCs are being explored using gene therapy and gene-editing. These approaches typically aim to protect cells from viral infection with the expression of anti-HIV genes or with the disruption of host genes required for HIV entry. In such approaches, CD34+ HSPCs undergo ex vivo treatment with genome-editing or gene therapy modalities, followed by transplantation into the HIV/AIDS patient.
For gene therapy applications, CD34+ HSPCs are transduced with an integrative vector that encodes one or more anti-HIV genes. From the late 1990s, several clinical trials were conducted to test the safety, feasibility, and effectiveness of CD34+ HSPCs transduced with gammaretroviral vectors that encoded anti-HIV ribozymes,27–29 antisense transcripts,30 and RNA decoys.31 Due to the tendency of gammaretroviral vectors to integrate near and activate oncogenes,32 more recent approaches have utilized lentiviral vectors,33–37 foamy virus vectors,38–40 or transposons41 for transgene expression.
The first clinical study (NCT00569985) to evaluate a combinatorial lentiviral vector for HIV was performed at the City of Hope (Duarte, CA, USA) for patients with AIDS-related non-Hodgkin’s lymphoma. HIV-infected individuals received CD34+ HSCs that were engineered to express a variety of anti-HIV small RNAs, including a small interfering RNA against HIV tat/rev, an anti-CCR5 ribozyme, and trans-activation response element decoy.33 A related study (NCT01961063) will further evaluate this approach after pre-conditioning with busulfan, which may improve engraftment of transplanted cells. A different combinatorial lentiviral vector, which co-expresses a short hairpin RNA against CCR5 and HIV-1 entry inhibitor peptide C46, is being evaluated in a Phase I/II clinical trial (NCT01734850) in HIV/AIDS patients, who have been exposed to ART. In this trial, conducted by Calimmune, Inc. (Los Angeles, CA, USA) and the University of California, Los Angeles, autologous CD34+ HSPCs and CD4+ T-cells are transduced with the vector and transplanted after preconditioning with busulfan.42 A pending study (NCT01769911) at Fred Hutchinson Cancer Research Center (Seattle, WA, USA) will use autologous CD34+ HSPCs carrying a lentiviral vector with the C46 peptide for patients with HIV-associated non-Hodgkin or Hodgkin lymphoma. The strategy has shown promise in preclinical studies in a pigtail macaque model for HIV.43,44
Genome-editing aims to disrupt host genes required for HIV entry using site-directed DNA nucleases. Site-specific zinc finger nucleases (ZFNs) have been designed to introduce destructive mutations in the CCR5 gene in an effort to eliminate the host co-receptors that are required for HIV infection.45–49 The ZFN against CCR5 appears particularly promising, as it is currently being evaluated in autologous CD4+ T-cells in multiple clinical studies (NCT00842634, NCT01252641, NCT01044654, NCT01543152, and NCT02225665) and in a pending study with autologous CD34+ HSPCs.49 Transcription activator-like effector nucleases 50–52 and the clustered regularly interspaced short palindromic sequence repeats (CRISPR)/Cas9 system50,53–55 represent different classes of gene-editing enzymes that may be used to target host factors to create HIV-resistant cells.
For the genome-editing approaches, an important consideration is that genetic modification of heterozygous CCR5Δ32 cells is likely more efficient than genetic modification of CCR5 wildtype cells, due to the need to achieve biallelic and not monoallelic mutation. Thus, using heterozygous CCR5Δ32 units for genetic modification would be expected to make HCT much more effective for a cure of HIV infection, due to the higher percentage of modified cells with biallelic CCR5 disruption. This concept is consistent with observations from a clinical study of the CCR5 ZFN in autologous CD4+ T-cells, in which a single patient who was heterozygous for CCR5Δ32 had the lowest viral load peak and the longest delay in viral recrudescence.56
While it is impractical to restrict CCR5 genome-editing of autologous cells to patients who carry the heterozygous CCR5Δ32 mutation, heterozygous CCR5Δ32 HSPCs could be obtained from an HLA-matched donor or cord blood. Because heterozygous CCR5Δ32 units are much more readily available than homozygous CCR5-Δ32/Δ32 units, developing a file of HLA typed heterozygous units is eminently feasible. Therefore, using genetically modified heterozygous CCR5Δ32 cord blood units offers a practical means of providing HIV resistant cells to an HIV-infected patient. This is critical for members of minority populations for whom finding an HLA-matched unit from our inventory of ~200 CCR5-Δ32/Δ32 cord blood units is unlikely.
Thus, we are developing a file of HLA typed CCR5 heterozygous cord blood units which will be available for genetic modification prior to HCT of appropriate patients. The major factor in our approach to curing HIV infection is our use of heterozygous CCR5 cord blood units, which allows for significantly greater efficiency of genetic modification, and also allows for far easier HLA matching of available units than does relying on the availability of the quite unusual homozygous CCR5-Δ32/Δ32 units.
Results
Identifying CCR5-Δ32/Δ32 units in inventories of cryopreserved cord blood units
We have identified >200 CCR5-Δ32/Δ32 units after having tested samples from approximately 25,000 cryopreserved cord blood units obtained primarily from Caucasians for an incidence of about 0.8%. Testing an additional 15,000 samples from Caucasians is expected to increase the special inventory to approximately 300 units. Further development of the special inventory is eminently feasible, since, according to the estimates of Gonzalez et al,14 there are approximately 400,000 cord blood units cryopreserved around the globe, including 2,000–4,000 homozygous CCR5-Δ32/Δ32 units.
Probabilities of finding adequately matched cord blood units with an adequate cell dose in an inventory of 300 CCR5-Δ32/Δ32 cord blood units
Table 1 indicates the projected probabilities of finding an adequately HLA-matched unit with a TNC count of 2.5×107/kg or with a TNC count of ≥1×107/kg in an inventory of 300 CCR5-Δ32/Δ32 units for pediatric and adult white patients and for patients of other ethnic groups. Projected match rates for white patients using a minimum necessary TNC count of ≥2.5×107/kg were 27.9% for adults and 73.6% for pediatric patients. Using a minimum necessary TNC count of ≥1.0×107/kg, the projected match rates were 82.1% for adults and 85.6% for pediatric patients. Probable match rates were significantly lower for patients of minority ethnic groups.
The HLA match rates when using heterozygous CCR5 units will obviously be much greater, although we have not calculated detailed estimates.
Discussion
Long-term control of HIV infection has been accomplished by Hütter et al11 with HCT using peripheral blood stem cells from an HLA-matched adult donor who had the CCR5-Δ32/Δ32 mutation. The patient has remained without any evidence of HIV infection for more than 8 years after discontinuation of antiretroviral drug therapy, and the consensus is that he has been cured. However, identifying a HLA-matched adult CCR5-Δ32/Δ32 donor for a given patient is not readily feasible because of the infrequency of the CCR5-Δ32/Δ32 allele and the requirement for a very close HLA match between adult donors and patients. Since donor–recipient HLA matching for a cord blood transplant is much less stringent,15 it is evident that cure of HIV infections by HCT can be much more easily accomplished by using stem cells obtained from a modestly sized inventory of cryopreserved CCR5-Δ32/Δ32 cord blood units. Furthermore, experience in two cord blood transplants using CCR5-Δ32/Δ32 cord blood units obtained from our inventory has indicated that after establishing full cord blood chimerism, the patient’s grafted cells were resistant to in vitro infection of HIV.16–18 Such data strongly support the use of cord blood as a platform for broader application of this curative technology to HIV-1 infected patients.
There are several perceived problems with cord blood HCT: these include insufficient cell dose, a prolonged time to engraftment and, in double cord blood transplantation, the inability to predict the dominant, or “winning unit”. Double cord blood transplants using CCR5-Δ32/Δ32 cord blood units can be made available for some adult patients, although finding two adequately HLA matched units for a patient from our modestly sized inventory would be unusual.
The co-infusion of adult progenitor cells, usually adult haploidentical cells, with cord blood stem cells, addresses these problems in a technically, minimally demanding fashion. Dual haploidentical/cord blood transplantation provides adequate cell dose for essentially all patients. Haploidentical/cord blood transplantation has been shown to reduce the post-transplantation period of neutropenia, mostly using units with relatively low cell dose. Liu et al23 reported that the infused post-thaw TNC counts ranged from 1.24 to 2.09×107/kg (median 1.55) of the patient’s body weight. The cord blood cell dose had no measurable impact on outcomes, thus making it possible to select cord blood units with lower cell doses than those that have generally been considered necessary.
Regardless of the patient and donor selection or procedural differences, all groups reporting experience with dual haploidentical/cord blood HCT observed rapid neutrophil recovery with a median time of 10–11 days.18,23–25 The median time to platelet recovery varied among reporting groups from 19 days to 32 days. The incidence and severity of graft-versus-host disease were generally low but, in spite of this, the cumulative incidence of disease recurrence for those with malignant disease was moderate, ie, 17%–28% at 1 year.24 Immune reconstitution after dual haploidentical/cord blood HCT was similar to that seen after cord blood transplantation, in spite of much lower cord blood cell doses.24,57
In dual haploidentical/cord blood HCT, the cord blood almost always predominates (median percentage of cord blood cells is 95% by day 180).23 When providing a HCT attempting to cure HIV, one may use a haploidentical unit and a single CCR5-Δ32/Δ32 cord blood, and have a very high probability that the “winning unit” will be the cord blood. Thus, the use of combined haploidentical and cord blood transplants provides important and, for some patients, essential advantages when considering use of HCT to cure HIV in adults.
The economic viability of HCT for a cure of HIV has been called into question and HCT has been shunned by many as not a plausible alternative to drug therapy. However, realistic estimates of the potential economic impact of HCT for HIV suggest that this type of treatment would be cost-effective.58 For example, the cost of an autologous bone marrow transplant ranges from $40,000 to upwards of $90,000, additional costs, eg, for and required product release testing, it is reasonable to assume a final cost of $250,000–$300,000 per patient. By comparison the cost of lifelong ART therapy has been estimated to be as high as $420,000–$755,000. Thus, it appears that a one-time intervention with stem cell gene therapy is not outside of economic reality in developed countries.
Conclusion
HCT using peripheral blood stem cells from an adult donor having the CCR5-Δ32/Δ32 mutation has produced a cure of a HIV-infected person. However, CCR5-Δ32/Δ32 donors are quite unusual, and this coupled with the fact that the use of stem cells from peripheral blood and bone marrow of adults requires a very close HLA match between the donor and the recipient makes it impossible to frequently perform HCT using CCR5-Δ32/Δ32 stem cells from adult donors for patients in need of treatment for HIV. The less stringent HLA matching required using cord blood stem cells that makes the use of cord blood units having the CCR5-Δ32/Δ32 mutation, or that are genetically modified to be resistant to HIV infection, a much more viable approach.
A key facet of our work is providing cord blood units that contain stem cells that are resistant to HIV to patients infected with HIV. One approach has been the development of an inventory of CCR5-Δ32/Δ32 cord blood units. We have >200 such units in our continuously enlarging inventory, and three have been used for HCT. In two instances we were able to test peripheral blood samples post-transplant, and in vitro studies indicated that the patient’s peripheral blood cells were resistant to HIV. This is encouraging and suggests that cure of HIV may be achieved using cord blood CCR5-Δ32/Δ32 cells in HCT.
We are expanding our work to include genetic modification of donor stem cells to make them resistant to infection by HIV. Previous research on genetic modification has relied on modification of wild type cells, whereas our studies will involve modification of the heterozygous CCR5 units that are also in our inventory. This approach has three major advantages which are the following: 1) that the genetic modification of heterozygous units will yield a significantly higher percentage of modified cells which may make HCT of HIV more effective; 2) that an inventory of HLA-typed heterozygous CCR5 units to be used for genetic modification for a given patient can be developed far easier than an inventory of CCR5-Δ32/Δ32 units; and 3) it will be much more feasible to find a HLA matched unit for members of minority populations from the list of heterozygous units than it is for the comparatively small list of homozygous CCR5 cord blood units.
No approach to a cure of HIV has been successful other than HCT with stem cells that are resistant to infection by HIV. We expect to add to the list of HCTs that have been successful in curing HIV.
Disclosure
The authors report no conflicts of interest in this work.
References
Este JA, Cihlar T. Current status and challenges of antiretroviral research and therapy. Antiviral Res. 2010;85(1):25–33. | |
Deeks SG, Autran B, Berkhout B, et al. Towards an HIV cure: a global scientific strategy. Nat Rev Immunol. 2012;12(8):607–614. | |
Davey RT Jr, Bhat N, Yoder C, et al. HIV-1 and T cell dynamics after interruption of highly active antiretroviral therapy (HAART) in patients with a history of sustained viral suppression. Proc Natl Acad Sci U S A. 1999;96(26):15109–15114. | |
Dahabieh MS, Battivelli E, Verdin E. Understanding HIV latency: the road to an HIV cure. Annu Rev Med. 2015;66:407–421. | |
Maldarelli F, Wu X, Su L, et al. HIV latency. Specific HIV integration sites are linked to clonal expansion and persistence of infected cells. Science. 2014;345(6193):179–183. | |
Shan L, Deng K, Shroff NS, et al. Stimulation of HIV-1-specific cytolytic T lymphocytes facilitates elimination of latent viral reservoir after virus reactivation. Immunity. 2012;36(3):491–501. | |
Deng K, Pertea M, Rongvaux A, et al. Broad CTL response is required to clear latent HIV-1 due to dominance of escape mutations. Nature. 2015;517(7534):381–385. | |
Burke BP, Boyd MP, Impey H, et al. CCR5 as a natural and modulated target for inhibition of HIV. Viruses. 2014;6(1):54–68. | |
Liu R, Paxton WA, Choe S, et al. Homozygous defect in HIV-1 coreceptor accounts for resistance of some multiply-exposed individuals to HIV-1 infection. Cell. 1996;86(3):367–377. | |
Paxton WA, Martin SR, Tse D, et al. Relative resistance to HIV-1 infection of CD4 lymphocytes from persons who remain uninfected despite multiple high-risk sexual exposure. Nat Med. 1996;2(4):412–417. | |
Hütter G, Nowak D, Mossner M, et al. Long-term control of HIV by CCR5 Delta32/Delta32 stem-cell transplantation. N Engl J Med. 2009;360(7):692–698. | |
Martinson JJ, Chapman NH, Rees DC, Liu YT, Clegg JB. Global distribution of the CCR5 gene 32-basepair deletion. Nat Genet. 1997;16(1):100–103. | |
Ruiz-Ferrer M, Barroso N, Antinolo G, Aguilar-Reina J. Analysis of CCR5-Delta 32 and CCR2-V64I polymorphisms in a cohort of Spanish HCV patients using real-time polymerase chain reaction and fluorescence resonance energy transfer technologies. J Viral Hepat. 2004;11(4):319–323. | |
Gonzalez G, Park S, Chen D, Armitage S, Shpall E, Behringer R. Identification and frequency of CCR5Delta32/Delta32 HIV-resistant cord blood units from Houston area hospitals. HIV Med. 2011;12(8):481–486. | |
Smith AR, Wagner JE. Alternative haematopoietic stem cell sources for transplantation: place of umbilical cord blood. Br J Haematol. 2009;147(2):246–261. | |
Duarte RF, Salgado M, Sánchez-Ortega I, et al. CCR5 δ32 homozygous cord blood allogeneic transplantation in a patient with HIV: a case report. Lancet HIV. Epub May 19, 2015. | |
Petz LD, Redei I, Bryson Y, et al. Hematopoietic cell transplantation with cord blood for cure of HIV infections. Biol Blood Marrow Transplant. 2013;19(3):393–397. | |
Kwon M, Kuball JH, Ellerbroek P, et al. Single cord blood transplantation combined with an HLA mismatched third party donor for high-risk hematological patients with HIV infection. Blood. 2013;122(21):3401–3401. | |
Hütter G. More on shift of HIV tropism in stem-cell transplantation with CCR5 delta32/delta32 mutation. N Engl J Med. 2014;371(25):2437–2438. | |
Kordelas L, Verheyen J, Beelen DW, et al. Shift of HIV tropism in stem-cell transplantation with CCR5 Delta32 mutation. N Engl J Med. 2014;371(9):880–882. | |
Gragert L, Eapen M, Williams E, et al. HLA match likelihoods for hematopoietic stem-cell grafts in the US registry. N Engl J Med. 2014;371:339–348. | |
Liu H, Rich ES, Godley L, et al. Reduced-intensity conditioning with combined haploidentical and cord blood transplantation results in rapid engraftment, low GVHD, and durable remissions. Blood. 2011;118(24):6438–6445. | |
Liu H, van Besien K. Alternative donor transplantation--“mixing and matching”: the role of combined cord blood and haplo-identical donor transplantation (haplo-cord SCT) as a treatment strategy for patients lacking standard donors? Curr Hematol Malig Rep. 2015;10(1):1–7. | |
Van Besien K, Liu H, Jain N, et al. Umbilical cord blood transplantation supported by third-party donor cells: rationale, results, and applications. Biol Blood Marrow Transplant. 2013;19(5):682–691. | |
Kwon M, Bautista G, Balsalobre P, et al. Haplo-cord transplantation using CD34+ cells from a third-party donor to speed engraftment in high-risk patients with hematologic disorders. Biol Blood Marrow Transplant. 2014;20(12):2015–2022. | |
Kwon M, Balsalobre P, Serrano D, et al. Single cord blood combined with HLA-mismatched third party donor cells: comparable results to matched unrelated donor transplantation in high-risk patients with hematologic disorders. Biol Blood Marrow Transplant. 2013;19(1):143–149. | |
Amado RG, Mitsuyasu RT, Symonds G, et al. A phase I trial of autologous CD34+ hematopoietic progenitor cells transduced with an anti- HIV ribozyme. Hum Gene Ther. 1999;10(13):2255–2270. | |
Mitsuyasu RT, Merigan TC, Carr A, et al. Phase 2 gene therapy trial of an anti-HIV ribozyme in autologous CD34+ cells. Nat Med. 2009;15(3):285–292. | |
Rossi JJ. Ribozyme therapy for HIV infection. Adv Drug Deliv Rev. 2000;44(1):71–78. | |
Liu D, Donegan J, Nuovo G, Mitra D, Laurence J. Stable human immunodeficiency virus type 1 (HIV-1) resistance in transformed CD4+ monocytic cells treated with multitargeting HIV-1 antisense sequences incorporated into U1 snRNA. J Virol. 1997;71(5):4079–4085. | |
Kohn DB, Bauer G, Rice CR, et al. A clinical trial of retroviral-mediated transfer of a rev-responsive element decoy gene into CD34(+) cells from the bone marrow of human immunodeficiency virus-1-infected children. Blood. 1999;94(1):368–371. | |
Hacein-Bey-Abina S, Garrigue A, Wang GP, et al. Insertional oncogenesis in 4 patients after retrovirus-mediated gene therapy of SCID-X1. J Clin Invest. 2008;118(9):3132–3142. | |
DiGiusto DL, Krishnan A, Li L, et al. RNA-based gene therapy for HIV with lentiviral vector-modified CD34(+) cells in patients undergoing transplantation for AIDS-related lymphoma. Sci Transl Med. 2010;2(36):36ra43. | |
Ledger S, Howe A, Murray J, Symonds G. Lentiviral vector mediated gene therapies provide stable protection against HIV infection: the use of short-hairpin RNA to CCR5 and membrane anchored C peptide entry inhibitors. Mol Ther. 2014;22:S271–S271. | |
Barclay SL, Yang Y, Zhang S, et al. Safety and efficacy of a tCD25 preselective combination anti-HIV lentiviral vector in human hematopoietic stem and progenitor cells. Stem Cells. 2015;33(3):870–879. | |
Centlivre M, Legrand N, Klamer S, et al. Preclinical in vivo evaluation of the safety of a multi-shRNA-based gene therapy against HIV-1. Mol Ther Nucleic Acids. 2013;e2:e120. | |
Case SS, Price MA, Jordan CT, et al. Stable transduction of quiescent CD34(+)CD38(−) human hematopoietic cells by HIV-1-based lentiviral vectors. Proc Natl Acad Sci U S A. 1999;96(6):2988–2993. | |
Cheng Q, Dong L, Zhang F, et al. Short communication: efficiently inhibiting HIV-1 replication by a prototype foamy virus vector expressing novel H1 promoter-driven short hairpin RNAs. AIDS Res Hum Retroviruses. 2015;31(2):183–188. | |
Olszko ME, Trobridge GD. Foamy virus vectors for HIV gene therapy. Viruses. 2013;5(10):2585–2600. | |
Kiem HP, Wu RA, Sun G, von Laer D, Rossi JJ, Trobridge GD. Foamy combinatorial anti-HIV vectors with MGMTP140K potently inhibit HIV-1 and SHIV replication and mediate selection in vivo. Gene Ther. 2010;17(1):37–49. | |
Tamhane M, Akkina R. Stable gene transfer of CCR5 and CXCR4 siRNAs by sleeping beauty transposon system to confer HIV-1 resistance. AIDS Res Ther. 2008;5:16. | |
Wolstein O, Boyd M, Millington M, et al. Preclinical safety and efficacy of an anti–HIV-1 lentiviral vector containing a short hairpin RNA to CCR5 and the C46 fusion inhibitor. Mol Ther Methods Clin Dev. 2014;1:11. | |
Younan PM, Peterson CW, Polacino P, et al. Lentivirus-mediated gene transfer in hematopoietic stem cells is impaired in SHIV-infected, ART-treated nonhuman primates. Mol Ther. 2015;23(5):943–951. | |
Younan P, Kowalski J, Kiem HP. Genetic modification of hematopoietic stem cells as a therapy for HIV/AIDS. Viruses. 2013;5(12):2946–2962. | |
Kim E, Kim S, Kim DH, Choi BS, Choi IY, Kim JS. Precision genome engineering with programmable DNA-nicking enzymes. Genome Res. 2012;22(7):1327–1333. | |
Holt N, Wang J, Kim K, et al. Human hematopoietic stem/progenitor cells modified by zinc-finger nucleases targeted to CCR5 control HIV-1 in vivo. Nat Biotechnol. 2010;28:839–847. | |
Tebas P, Stein D, Binder-Scholl G, et al. Antiviral effects of autologous CD4 T cells genetically modified with a conditionally replicating lentiviral vector expressing long antisense to HIV. Blood. 2013;121(9):1524–1533. | |
Maier DA, Brennan AL, Jiang S, et al. Efficient clinical scale gene modification via zinc finger nuclease-targeted disruption of the HIV co-receptor CCR5. Hum Gene Ther. 2013;24(3):245–258. | |
Li L, Krymskaya L, Wang J, et al. Genomic editing of the HIV-1 coreceptor CCR5 in adult hematopoietic stem and progenitor cells using zinc finger nucleases. Mol Ther. 2013;21(6):1259–1269. | |
Ye L, Wang J, Beyer AI, et al. Seamless modification of wild-type induced pluripotent stem cells to the natural CCR5Delta32 mutation confers resistance to HIV infection. Proc Natl Acad Sci U S A. 2014; 111(26):9591–9596. | |
Mussolino C, Alzubi J, Fine EJ, et al. TALENs facilitate targeted genome editing in human cells with high specificity and low cytotoxicity. Nucleic Acids Res. 2014;42(10):6762–6773. | |
Mussolino C, Morbitzer R, Lutge F, Dannemann N, Lahaye T, Cathomen T. A novel TALE nuclease scaffold enables high genome editing activity in combination with low toxicity. Nucleic Acids Res. 2011;39(21):9283–9293. | |
Wang W, Ye C, Liu J, Zhang D, Kimata JT, Zhou P. CCR5 Gene disruption via lentiviral vectors expressing Cas9 and single guided RNA renders cells resistant to HIV-1 infection. PLoS One. 2014; 9(12):e115987. | |
Mandal PK, Ferreira LM, Collins R, et al. Efficient ablation of genes in human hematopoietic stem and effector cells using CRISPR/Cas9. Cell Stem Cell. 2014;15(5):643–652. | |
Cho SW, Kim S, Kim JM, Kim JS. Targeted genome engineering in human cells with the Cas9 RNA-guided endonuclease. Nat Biotechnol. 2013;31(3):230–232. | |
Tebas P, Stein D, Tang WW, et al. Gene editing of CCR5 in autologous CD4 T cells of persons infected with HIV. N Engl J Med. 2014; 370(10):901–910. | |
Jain N, Liu H, Artz AS, et al. Immune reconstitution after combined haploidentical and umbilical cord blood transplant. Leuk Lymphoma. 2013;54(6):1242–1249. | |
DiGiusto DL, Stan R, Krishnan A, Li H, Rossi JJ, Zaia JA. Development of hematopoietic stem cell based gene therapy for HIV-1 infection: considerations for proof of concept studies and translation to standard medical practice. Viruses. 2013;5(11):2898–2919. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.