Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Progress in Research on Biomarkers of Gestational Diabetes Mellitus and Preeclampsia
Authors Liu Y, Li DY, Bolatai A, Wu N ![]()
Received 24 August 2023
Accepted for publication 31 October 2023
Published 22 November 2023 Volume 2023:16 Pages 3807—3815
DOI https://doi.org/10.2147/DMSO.S433179
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Yang Liu,1 Dan Yang Li,1 Alayi Bolatai,2 Na Wu1,3
1Department of Endocrinology, Shengjing Hospital of China Medical University, Shenyang, Liaoning, People’ s Republic of China; 2Department of Student Affairs, Affiliated Hospital of China Medical University, Shenyang, Liaoning, People’ s Republic of China; 3Medical Department, Shengjing Hospital of China Medical University, Shenyang, Liaoning, People’ s Republic of China
Correspondence: Na Wu, Email [email protected]
Abstract: Gestational diabetes mellitus (GDM) and preeclampsia (PE) are common complications in pregnancy, with incidence rates of 1– 5% and 9.4%, respectively, in China. Both these phenomena can cause adverse pregnancy outcomes and are extremely harmful to the mother and fetus. In this study, we observed that several predictive factors have important value in GDM and PE. Among the GDM group, abnormal levels of adiponectin (APN), C-reactive protein (CRP), and Leptin were observed. The coexistence of PE and GDM in the pregnant population is not uncommon. Ultimately, we discovered abnormal levels of factors such as Visfatin, Advanced oxidative protein product (AOPP), Fibroblast growth factor 21 (FGF21), and resistin in both GDM and PE groups. Particularly, the FGF21 factor holds significant importance in our research. Therefore, we need to complete the analysis and discussion of relevant predictive factors to enable early prediction and disease monitoring of GDM, PE, and other pregnancy-related disorders, ultimately contributing to the long-term health of pregnant women.
Keywords: gestational diabetes mellitus, preeclampsia, predictor of the GDM and PE
Introduction
Hyperglycemia in pregnancy is categorized as diabetes combined with pregnancy (pregestational diabetes mellitus, PGDM), newly discovered overt diabetes, and gestational diabetes mellitus (GDM). GDM refers to a class of diseases in which carbohydrate intolerance is first discovered during second trimester or the third trimester of pregnancy.1
Due to the special clinical status and abnormal function of maternal glucose and lipid metabolism,2 researched showed that during gestation, the effect of progesterone and glucocorticoids on insulin sensitivity have been suggested to be relative for the increase of insulin resistance.3 Meanwhile, on the contrary of normal pregnancy, when β-cell secretion is no longer sufficient to compensate for insulin compensate, it will lead to carbohydrate intolerance.4 Both insulin resistance and insulin insufficiency will lead to the increase of maternal glucose, amino acids and lipids, thus forming GDM (see Figure 1).
 |
Figure 1 Mechanisms of gestational diabetes mellitus. |
For the diagnostic criteria of GDM, though 2-stage oral glucose tolerance test (OGTT) can improve the detection efficiency.5 Nowadays, whether recognizing single or 2-stage OGTT test as golden standard still cannot reach a consensus. When it comes to single stage OGTT, the criteria are abnormal values for all pregnant women whose PGDM or GDM is not diagnosed after 24 to 28 weeks of pregnancy. GDM can be the diagnosis when 5.1mmol/L≤fasting blood glucose<7mmol/L,1hour≥10.0mmol/L, or 8.5mmol/L≤2hours<11.1mmol/L, after ingesting sugar.
Recently, the improvement of living standards has led to increased incidence rates, which are 7.6% in the US and 14.8% in China.6,7 GDM has effects on the fetus, including abortion, premature birth, macrosomia and fetal malformation, growth restriction, distress and death.
Preeclampsia (PE) is a hypertensive disease associated with pregnancy that mainly occurs after 20 weeks of gestation, with symptoms such as hypertension, edema, and proteinuria. It is one of the complications of GDM. At present, the pathogenesis and etiology of PE have not been clarified. It is considered as a multifactorial disease. These include abnormal uterine placental vascular structure, impaired extravillous trophoblast infiltration capacity, and increased vascular resistance, resulting in reduced blood flow to the placenta.8 The excessive activation of inflammatory immunity results in the reduction of maternal immune tolerance to the embryo. At the same time, inflammatory mediators can lead to vascular endothelial injury, decrease the synthesis of vasodilating substances, promote vasospasm, and lead to the rise of blood pressure.9 On the other hand, vascular endothelial cell injury activates platelets and coagulation factors, aggravating the hypercoagulation state of PE. In addition, PE has a familial predisposition, but the mode of inheritance is not clear.10 Elevated blood pressure and proteinuria are the main diagnostic criteria of PE. Furthermore, the occurrence of abnormalities in the liver, kidney, and blood system laboratory indicators or symptoms before eclampsia, such as headache, dizziness, and upper abdominal pain can clarify the diagnosis of PE. The incidence of PE ranges from 2% to 8% worldwide.11 PE is very harmful to the mother, in whom it can lead to cerebral edema, abnormal liver, kidney, and coagulation functions and massive bleeding, which can be life-threatening. The hazard of PE extends to the fetus, with the possibility of placental abruption, leading to fetal growth retardation and even death in the womb.
GDM and PE have similar risk factors and pathophysiological alterations, whereas GDM may be one of the risk factors for PE.12 The incidence of PE has been shown to be higher in patients with GDM than in those without GDM.13
It is known that obesity is a risk factor of pregnancy complications. The study of Lewandowska showed that excessive pre-pregnancy maternal weight has important influence on the risk of pregnancy complications such as GDM and hypertension, which can cause adverse fetal outcomes.14 Hillier’s research also showed that first trimester GDM screening for pregnant people with obesity may improve GDM-associated outcomes.15 Ke also found that maternal overweight was associated with adverse pregnancy outcomes in GDM.16
GDM with PE can aggravate the disease condition, whereas early detection, diagnosis, treatment can improve the prognosis and reduce treatment cost. The improvement of advances in medical technology has facilitated the discovery of an increasing number of predictors. So far, we have noticed biomarkers like adiponectin (APN), leptin, C-reactive protein (CRP), myokines, γ-glutamyltransferase (GGT), TNF-α, IL-6 and so on have strong relationship with GDM.17,18 In this article, we will discuss the influence of APN, leptin and CRP on GDM (see Table 1).
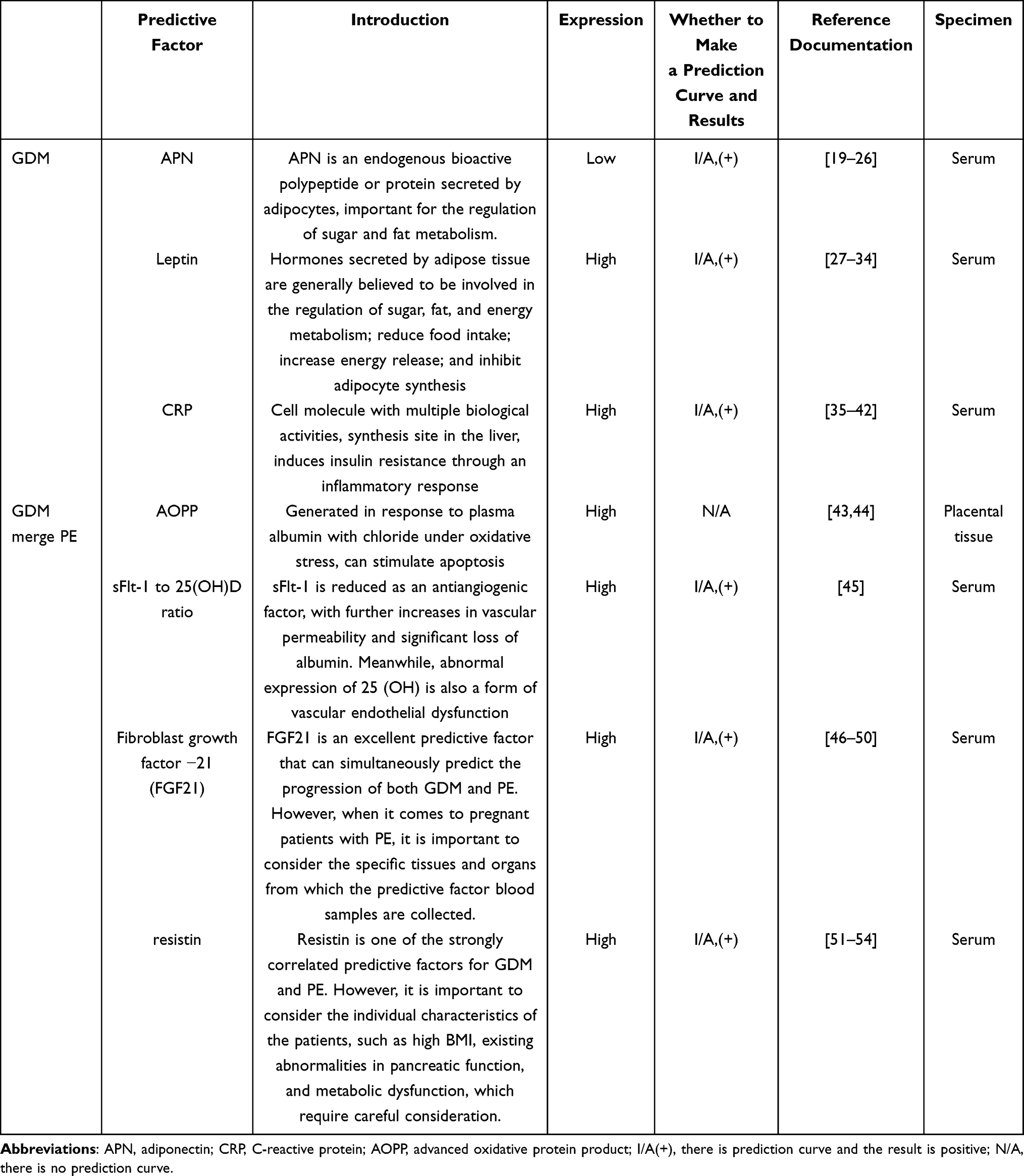 |
Table 1 Predictors of Gestational Diabetes Mellitus (GDM), and Concurrent GDM with PE |
GDM Biomarkers
Adiponectin (APN)
Adiponectin (APN), which is mainly produced and secreted by adipocytes in adipose tissue, has pleiotropic effects on numerous organs, including the liver. The APN structure consists of the following four domains, the N-terminal signal peptide and hypervariable, collagen, and carboxy-terminal globular domains.19 APN plays an important role in regulating glucose and lipid metabolism, which can promote the oxidation of plasma free fatty acids, improve sensitivity to insulin,20 increase glucose uptake by peripheral tissues, and inhibit glucose output and glucose regeneration. APN can improve insulin resistance to a certain extent. As insulin sensitivity changes, blood sugar decreases. The level of APN decreases, the degree of insulin resistance increases, the body’s sensitivity to insulin decreases, and blood glucose increases. Numerous studies have linked serum APN levels to GDM. The result of a study by Xueli and Pei on 84 pregnant women showed that APN levels were significantly lower in the serum of patients with GDM than in those without GDM.21
Study has shown that pregnant women with GDM have significantly lower APN levels than pregnant women without GDM, which is a good indicator for monitoring blood glucose during pregnancy.22 Jinying et al showed that APN level was lower in the serum of patients with GDM than in those without GDM.23 However, the specific values may vary with the pregnancy period, the degree of disease, the weight change in the past history, and even the differences in race.24 The above factors should be taken into account in the early risk assessment.
In addition, APN also has a certain anti-apoptotic and anti-inflammatory mechanism on blood vessels.25 Some studies have proved that the vascular endothelium in GDM patients is continuously damaged, which may also be related to the decline of APN level.26
Leptin
White adipose tissue is the main site of leptin synthesis and secretion regulation. The precursor of leptin consists of 167 amino acid residues with a 21-amino acid residue signal peptide at the N terminal. The precursor signal peptide is cut off in the blood to generate a peptide of 146 amino acids with a molecular weight of 16 KD, forming leptin. Leptin binds to leptin receptors on islet β cells, thereby inhibiting glucose-stimulated insulin secretion, this causes blood glucose to rise.27 Numerous studies have found a clear correlation between leptin levels and GDM, such as that by Yang et al which showed the association between increased leptin concentration and GDM.28 In a study of 120 pregnant women, Fang et al showed that leptin level was increased in the serum of patients with GDM.25 Plowden et al showed pregnant women with high leptin level are more likely to experience adverse pregnancy outcome like GDM.29 Xiao showed that pregnant women with GDM have higher leptin level.30 Peltokorpi also showed that GDM patients have higher leptin level.31 Therefore, leptin may have a predictive value in GDM.
Bawah et al reported that 1 out of 140 pregnant women showed increased leptin levels in the presence of GDM.32 Furthermore, the leptin-predicted GDM area under the curve of the receiver operating characteristic (AUCROC) curve showed that leptin acted as a predictor of GDM. Florian et al reported that the leptin-predicted GDM AUCROC curve had a good predictive effect.33 Thus, elevated levels of leptin may be a predictor of GDM in patients.
In addition, body mass index is also one of the important factors affecting leptin release, so it is necessary to consider that the number of fat cells in overweight or obese people is much greater than that in normal pregnant women, and may be accompanied by abnormal islet function.34 Therefore, the content of leptin released may also interfere with the prediction of GDM.
C-Reactive Protein (CRP)
C-reactive protein (CRP) is a protein that is released by the liver, whose level rises sharply in the plasma when the body is infected or sustains tissue damage, and that can be produced within several hours following inflammation, while peaking at 8 hours. CRP elevation is common in late pregnancy, infections, inflammation, and burns. CRP opsonizes by activating complement, strengthening phagocytosis, and removing pathogenic microorganisms and damaged, necrotic, and apoptotic tissue cells that invade the body. Elevated serum levels of CRP are indicative of chronic metabolic inflammation and may be associated with cardiovascular disease and insulin resistance (IR) in both men and women.35
Intravascular lipoprotein is an important component of human blood vessels, and the value of lipoprotein in pregnant women with potential for GDM is usually unbalanced. The pathological effect caused by chronic inflammation in the vascular endothelium gradually accumulates, resulting in further increase of CRP value. Meanwhile, the resulting chronic inflammation also further affects blood glucose metabolism. The equilibrium of blood sugar is further broken; Therefore, dysglycolipid metabolism may be one of the main causes of CRP induced GDM.36
Numerous studies have shown that CRP levels are closely related to GDM and that increased serum levels in early pregnancy increase the risk of GDM. Alamolhoda et al showed a statistically significant difference in CRP levels between the GDM and control groups.37 In a study of 120 pregnant women, Liu et al found that serum CRP levels were significantly higher in the GDM group than in the normal group.38 Yu et al showed that CRP may be related to the onset of GDM and that CRP levels were significantly increased in GDM patients.39 The study of Amirian shows that, the CRP level in blood may be a potential predictor of GDM.40 In a study by Durnwald et al, the CRP predicted GDM AUCROC curve results showed CRP to be a good predictor of GDM.41
Vecchie et al reported that women who had experienced adverse pregnancy outcomes were more likely to develop hypertension and get older, and the ROC curve analysis showed that CRP concentrations > 1.86 g/mL could accurately predict adverse outcomes.42 Therefore, elevated serum CRP levels may predict GDM, with higher levels being indicative of a higher risk of GDM.
Biomarkers of PE Occurrence in GDM
The risk factors for GDM and PE are similar and have similar pathophysiological variations. GDM may be one of the risk factors for PE, and patients with GDM have been reported to show a higher probability of developing PE than those without GDM.13 Study shows that GDM combined with PE significantly increases the likelihood of adverse pregnancy outcomes.55 However, the relationship between GDM and PE needs further investigation. Therefore, the study of biomarkers is crucial.
Advanced Oxidative Protein Product (AOPP)
Oxidative stress (OS) refers to the imbalance between oxidant and antioxidant effects in the body, which tends to cause oxidation, leading to inflammatory infiltration of neutrophils. Furthermore, increased secretion of proteases and the production of a large number of oxidative intermediates, which is a negative effect of free radical production in the body, may be observed. Advanced oxidative protein product (AOPP) is mainly formed by the reaction of plasma albumin and chloride under oxidative stress, which can stimulate the respiratory burst of monocytes.43 Furthermore, AOPP promotes the synthesis and release of inflammatory cytokines, causes systemic microinflammation, and participates in the episode of diseases such as chronic kidney disease, diabetes, and heart disease.
Numerous studies have shown that AOPP is associated with the occurrence of GDM combined with PE. A study in 130 pregnant women conducted by Shu et al found that AOPP expression level in placental tissue in pregnant women with GDM and PE was significantly increased and continued gradually increasing further with disease progression.44 Therefore, AOPP correlates with the concurrent onset of GDM and PE, but further studies would be required to determine its usefulness as a biomarker.
Soluble Fms-Like Tyrosine Kinase-1 (sFlt-1) to 25(OH)D Ratio
Vascular endothelial growth factor (VEGF) has a soluble antagonist, sFlt-1, which plays an important role in maintaining vascular growth balance. The expression of sFlt-1 is an important predictor of other diseases associated with pregnancy, and recent studies have shown that this predictor is significantly associated with endothelial cell integrity. Changes in the number of sFlt-1 in poor vascular status and Vitamin D associated with endothelial dysfunction are also related predictors. In particular, significant changes in the value of sFlt-1/25(OH)D, which can further predict the appearance of GDM and PE.45
Fibroblast Growth Factor 21 (FGF21)
Fibroblast growth factor (FGF) is one of the important predictive factors in recent years. Its study on the mechanisms of gestational diabetes mellitus (GDM) and preeclampsia has significant significance. It is a peptide hormone synthesized by various organs. In recent years, the regulatory mechanisms of FGF in the human body have gradually been understood. FGF generally acts in conjunction with its receptor (FGFR).46 FGF also regulates cell differentiation and proliferation. If there are fluctuations in FGF/FGFR values outside the normal range, it is highly likely to indicate pathological changes, with a higher possibility of being associated with cancer and kidney diseases.47 Furthermore, FGF has many subtypes. In this discussion, we found a correlation between FGF-21 and human glucose metabolism, especially significant abnormal expression in studies of diabetic patients.48,49 This substance can be used as one of the predictive factors and holds significant importance in the clinical treatment of GDM patients. However, this factor also undergoes partial changes during pregnancy-related preeclampsia. It is important to timely differentiate diagnostic criteria related to these diseases to avoid unnecessary misdiagnosis. Interestingly, some studies have reported no significant changes in FGF-21 during the pre-eclampsia period in the placenta.50 Further research can verify the specificity of FGF21 expression in GDM, which holds certain significance in clinical exclusionary diagnosis.
Resistin
Resistin, also a factor expressed abnormally in the serum of patients with gestational diabetes mellitus (GDM) and preeclampsia (PE), plays a role in the pathogenesis as follows: Essentially, it is a small secreted protein that regulates glucose metabolism. Under normal conditions, it stably modulates the body’s inflammatory response and enhances immune properties in conjunction with insulin. However, once its levels increase, it induces insulin resistance, partially losing the regulatory function of insulin in the body.51 In terms of serum levels in pregnant women, pregnancy itself has a certain probability of altering the serum levels. However, if resistin levels are found to be significantly abnormal, it may indicate the possibility of pregnancy complications, particularly in the occurrence of high resistin expression before the onset of GDM and preeclampsia.52 Resistin detected in GDM patients is closely related to metabolic function, and GDM patients with high resistin expression are often prone to metabolic disorders such as obesity during pregnancy. In investigations of serum levels in PE patients, resistin is one of the best predictive factors, providing a higher level of accuracy in prediction. In relevant experiments, resistin is seen as a significant monitoring factor, but it is necessary to exclude certain interfering factors in correlation tests.32
In addition, the research of Xie also found that, plasma soluble transferrin receptor(sTfR), ceruloplasmin(CP) and apolipoprotein E(ApoE) levels have potential clinical significance in early screening of GDM combined with PE.53 Moreover, Xue promoted that high serum complement factors B concentration during mid-pregnancy is a potential biomarker of the risk of PE in patients with GDM.54
Conclusions
GDM is the most common complication in pregnancy, with a trend towards increased incidence with improving living standards in recent years. PE is also a common complication during pregnancy. GDM and PE are extremely harmful to both mother and fetus. Finding suitable predictors can help improve adverse pregnancy outcomes. APN, leptin, CRP are closely related to the onset of GDM, and in GDM patients, decreased APN levels, and increased leptin and CRP levels may be predictors of GDM. GDM combined with PE is also common in pregnancy, but there are few studies on the predictors of GDM combined with PE. Early in the disease, we can detect it with ultrasound, and we can find the difference on AOPP, sFlt-1/25(OH)D ratio, FGF21 and resistin compared with healthy pregnant women. Whether they can act as biomarkers needs further study.
Expectation
With the improvement of living standards, the incidence of GDM and PE is on the rise. Early diagnosis and early treatment can improve the prognosis, save treatment costs and reduce hospitalization costs. The ideal predictor should be detectable early in the disease, with high sensitivity and specificity. Several factors have been listed in this paper, which are relatively easy to detect. However, the relationship between some factors and the prediction of disease has not been clarified. In the future, we should focus more on whether they have specificity for the detection and the assessment of prognostic effect. Furthermore, studies on these factors can broaden our knowledge about the predictors of GDM combined with PE, in order to carry out rigorous therapeutic regimen for such complications in pregnancy. And there are still many biomarkers waiting to be studied.
Statement
During the preparation of this work the authors used ChatGPT in order to Translate part of the article. After using this tool/service, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the publication.
Statement of Ethics
This article does not contain any studies with human or animals performed by any of the authors.
Consent for Publication
Agreed to publish.
Acknowledgments
In the process of writing this review, we gratefully acknowledge Na Wu for providing intellectual support and technical assistance. She provided a lot of help in the structure and writing standards of the article.
Funding
This research was funded by the National Natural Science Foundation of China, grant number 81700706; the Virtual Simulation Experiment Teaching Project of China Medical University, grant number 2020-47; the 345 Talent Project of Shengjing Hospital; the Natural Science Foundation of Liaoning Province, grant number 2021-MS-182; the Science Foundation of Liaoning Education Department, grant number LK201603; and the Clinical Research Project of Liaoning Diabetes Medical Nutrition Prevention Society, grant number LNSTNBYXYYFZXH-RS01B.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Choudhury AA, Devi Rajeswari V. Gestational diabetes mellitus - A metabolic and reproductive disorder. Biomed Pharmacother. 2021;143:112183. doi:10.1016/j.biopha.2021.112183
2. Yu W, Wu N, Li L, OuYang H, Qian M, Shen H. A review of research progress on glycemic variability and gestational diabetes. Diabetes Metabol Syndr Obes. 2020;13:2729–2741. doi:10.2147/DMSO.S261486
3. Devarshi PA-O, Grant RA-O, Ikonte CJ, Hazels Mitmesser S. Maternal Omega-3 nutrition, placental transfer and fetal brain development in gestational diabetes and preeclampsia. Nutrients. 2019;11(5):1107. doi:10.3390/nu11051107
4. Di Cianni G, Miccoli R, Fau - Volpe L, Lencioni C, Del Prato S. Intermediate metabolism in normal pregnancy and in gestational diabetes. Diabetes Metab Res Rev. 2003;19(4):259–270. doi:10.1002/dmrr.390
5. Chen HT, Deng SQ, Li ZY, et al. 广东地区15家医院孕前糖尿病的调查研究 [Investigation of pregestational diabetes mellitus in 15 hospitals in Guangdong province]. Zhonghua fu Chan ke za zhi. 2017;52(7):436–442. Chinese.
6. Casagrande SS, Linder B, Cowie CC. Prevalence of gestational diabetes and subsequent Type 2 diabetes among U.S. women. Diabetes Res Clin Pract. 2018;141:200–208. doi:10.1016/j.diabres.2018.05.010
7. Gao C, Sun XA-O, Lu L, Liu F, Yuan J. Prevalence of gestational diabetes mellitus in mainland China: a systematic review and meta-analysis. J Diabetes Investig. 2019;10(1):154–162. doi:10.1111/jdi.12854
8. Nakashima A, Shima T, Tsuda S, et al. Disruption of Placental Homeostasis Leads to Preeclampsia. Int J Mol Sci. 2020;21(9):3298. doi:10.3390/ijms21093298
9. Guney G, Taskin MI, Tokmak A. Increase of circulating inflammatory molecules in preeclampsia, an update. Eur Cytokine Netw. 2020;31(1):18–31. doi:10.1684/ecn.2020.0443
10. Valenzuela FJ, Pérez-Sepúlveda A, Torres MJ, Correa P, Repetto GM, Illanes SE. Pathogenesis of preeclampsia: the genetic component. J Pregnancy. 2012;2012:1–8. doi:10.1155/2012/632732
11. Ives CW, Sinkey R, Rajapreyar I, Tita ATN, Oparil S. Preeclampsia-pathophysiology and clinical presentations: JACC State-of-the-Art Review. J Am Coll Cardiol. 2020;76(14):1690–1702.
12. Yang Y, Wu N. Gestational diabetes mellitus and preeclampsia: correlation and influencing factors. Front Cardiovasc Med. 2022;9. doi:10.3389/fcvm.2022.831297
13. Ostlund I, Haglund B, Hanson U. Gestational diabetes and preeclampsia. Eur J Obstet Gynecol Reprod Biol. 2004;113(1):12–16. doi:10.1016/j.ejogrb.2003.07.001
14. Lewandowska MA-O, Więckowska B, Sajdak S. Pre-pregnancy obesity, excessive gestational weight gain, and the risk of pregnancy-induced hypertension and gestational diabetes mellitus. J Clin Med. 2020;9(6):1980. doi:10.3390/jcm9061980
15. Hillier TA, Pedula KL, Ogasawara KK, Vesco KK, Oshiro C, Van Marter JL. Impact of earlier gestational diabetes screening for pregnant people with obesity on maternal and perinatal outcomes. J Perinat Med. 2022;50(8):1036–1044. doi:10.1515/jpm-2021-0581
16. Ke JF, Liu S, Ge RL, Ma L, Li MF. Associations of maternal pre-pregnancy BMI and gestational weight gain with the risks of adverse pregnancy outcomes in Chinese women with gestational diabetes mellitus. BMC Pregnancy Childbirth. 2023;23(1). doi:10.1186/s12884-023-05657-8
17. Ferrari NA-O, Joisten C. Impact of physical activity on course and outcome of pregnancy from pre- to postnatal. Eur J Clin Nutr. 2021;75(12):1698–1709. doi:10.1038/s41430-021-00904-7
18. Chen P, Wang S, Fau - Ji J, et al. Risk factors and management of gestational diabetes. Cell Biochem Biophys. 2015;71(2):689–694. doi:10.1007/s12013-014-0248-2
19. Han WA-O, Yang SA-O, Xiao H, et al. Role of adiponectin in cardiovascular diseases related to glucose and lipid metabolism disorders. Int J Mol Sci. 2022;23(24):15627.
20. Moyce Gruber BL, Dolinsky VA-O. The role of adiponectin during pregnancy and gestational diabetes. Life. 2023;13(2):301. doi:10.3390/life13020301
21. Boyadzhieva M, Atanasova I, Fau - Zacharieva S, Zacharieva S, Fau - Kedikova S, Kedikova S. Adipocytokines during pregnancy and postpartum in women with gestational diabetes and healthy controls. J Endocrinol Investigat. 2013;36:944–949.
22. Salem MM, Sokary AAE, Hazzaa SM, Gharib MNE. Predictive value of first trimester measurement of adiponectin and 1,5 anhydroglucitol in diagnosis of gestational diabetes mellitus. J Adv Med Med Res. 2020;111–118. doi:10.9734/jammr/2020/v32i2430758
23. Xu J, Zhao YH, Chen YP, et al. Maternal circulating concentrations of tumor necrosis factor-alpha, leptin, and adiponectin in gestational diabetes mellitus: a systematic review and meta-analysis. Sci World J. 2014;2014:1–12. doi:10.1155/2014/926932
24. Sweeting AN, Wong J, Appelblom H, et al. A novel early pregnancy risk prediction model for gestational diabetes mellitus. Fetal Diagn Ther. 2019;45(2):76–84. doi:10.1159/000486853
25. Fang H, Judd RL. Adiponectin regulation and function. Comprehens Physiol. 2011;8(3):1031–1063.
26. Yun-Hui D, Ma XL. 脂联素减轻糖尿病血管内皮损伤的保护机制 [Mechanisms of adiponectin protection against diabetes-induced vascular endothelial injury]. Sheng Li Xue Bao. 2019;71(3):485–490. Chinese.
27. Yadav A, Kataria V, Saini V, Yadav A. Role of leptin and adiponectin in insulin resistance. Clin Chim Acta. 2013;417:80–84. doi:10.1016/j.cca.2012.12.007
28. Yang M, Peng S, Li W, Wan Z, Fan L, Du Y. Relationships between plasma leptin levels, leptin G2548A, leptin receptor Gln223Arg polymorphisms and gestational diabetes mellitus in Chinese population. Sci Rep. 2016;6(1). doi:10.1038/srep23948
29. Plowden TC, Zarek SM, Rafique S, et al. Preconception leptin levels and pregnancy outcomes: a prospective cohort study. Obes Sci Pract. 2020;6(2):181–188. doi:10.1002/osp4.399
30. Xiao W-Q, He J-R, Shen S-Y, et al. Maternal circulating leptin profile during pregnancy and gestational diabetes mellitus. Diabetes Res Clin Pract. 2020;161:108041. doi:10.1016/j.diabres.2020.108041
31. Peltokorpi A, Irina L, Liisa V, Risto K. Preconceptual leptin levels in gestational diabetes and hypertensive pregnancy. Hypertens Pregnancy. 2022;41(1):70–77. doi:10.1080/10641955.2022.2033763
32. Bawah AT, Seini MM, Abaka-Yawason A, Alidu H, Nanga S. Leptin, resistin and visfatin as useful predictors of gestational diabetes mellitus. Lipids Health Dis. 2019;18(1). doi:10.1186/s12944-019-1169-2
33. Florian AR, Cruciat G, Pop RM, Staicu A, Daniel M, Florin S. Predictive role of altered leptin, adiponectin and 3-carboxy-4-methyl-5-propyl-2-furanpropanoic acid secretion in gestational diabetes mellitus. Exp Ther Med. 2021;21(5). doi:10.3892/etm.2021.9951
34. Lappas M, Yee K, Fau - Permezel M, Rice GE. Release and regulation of leptin, resistin and adiponectin from human placenta, fetal membranes, and maternal adipose tissue and skeletal muscle from normal and gestational diabetes mellitus-complicated pregnancies. J Endocrinol. 2005;186(3):457–465. doi:10.1677/joe.1.06227
35. Yao Z, Zhang Y, Wu H. Regulation of C-reactive protein conformation in inflammation. Inflammat Res. 2019;68(10):815–823. doi:10.1007/s00011-019-01269-1
36. Jiang XC, Liang ZD, Chen DL, Jia JP, Hu JR, Hu L. Correlation of homocysteine, AHSG, CRP with insulin resistance, 25-(OH)2-VitD, blood lipids in gestational diabetes patients. Clin Lab. 2021. doi:10.7754/Clin.Lab.2020.200609
37. Alamolhoda SH, Yazdkhasti M, Namdari M, Zakariayi SJ, Mirabi P. Association between C-reactive protein and gestational diabetes: a prospective study. J Obstet Gynaecol. 2020;40(3):349–353. doi:10.1080/01443615.2019.1631767
38. Liu W, Huang Z, Tang S, Zhang Z, Yu Q, He J. Changes of serum sex hormone-binding globulin, homocysteine, and hypersensitive CRP levels during pregnancy and their relationship with gestational diabetes mellitus. Gynecol Obstet Invest. 2021;86(1–2):193–199. doi:10.1159/000515085
39. Yu N, Cui HA-O, Chen X, Chang Y. Changes of serum pentraxin-3 and hypersensitive CRP levels during pregnancy and their relationship with gestational diabetes mellitus. PLoS One. 2019;14(11):e0224739.
40. Amirian A, Rahnemaei FA, Abdi F. Role of C-reactive Protein(CRP) or high-sensitivity CRP in predicting gestational diabetes Mellitus:Systematic review. Diabetes Metabol Syndr Clin Res Rev. 2020;14(3):229–236. doi:10.1016/j.dsx.2020.02.004
41. Durnwald CA-O, Downes K, Leite R, Elovitz M, Parry S. Predicting persistent impaired glucose tolerance in patients with gestational diabetes: the role of high sensitivity CRP and adiponectin. Diabetes Metab Res Rev. 2018;34(2). doi:10.1002/dmrr.2958
42. Vecchié A, Bonaventura AA-O, Carbone FA-O, et al. C-reactive protein levels at the midpregnancy can predict gestational complications. Biomed Res Int. 2018;2018:1–8. doi:10.1155/2018/1070151
43. Mohammedi K, Bellili-Muñoz N, Driss F, et al. Manganese superoxide dismutase (SOD2) polymorphisms, plasma advanced oxidation protein products (AOPP) concentration and risk of kidney complications in subjects with type 1 diabetes. PLoS One. 2014;9(5):e96916. doi:10.1371/journal.pone.0096916
44. Shu JJ, Xiong HL, Yang J. Expression and significance of LCN-2 and AOPP in gestational diabetes mellitus complicated by preeclampsia. J Nanchang Univ. 2018;58(05):59–61. doi:10.13764/j.cnki.ncdm.2018.05.012
45. Walentowicz-Sadlecka MA-O, Domaracki PA-OX, Sadlecki PA-O, et al. Assessment of the SFlt-1 and sFlt-1/25(OH)D Ratio as a Diagnostic Tool in Gestational Hypertension (GH), Preeclampsia (PE), and Gestational Diabetes Mellitus (GDM). Disease Markers2019;2019;1875–8630.
46. Ghedini GC, Ronca R, Presta M, Giacomini A. Future applications of FGF/FGFR inhibitors in cancer. Expert Rev Anticancer Ther. 2018;18(9):861–872. doi:10.1080/14737140.2018.1491795
47. Xie Y, Su N, Yang J, et al. FGF/FGFR signaling in health and disease. Signal Transduct Targeted Ther. 2020;5(1):181.
48. Bonakdaran S, Khorasani ZM, Jafarzadeh F. Increased serum level of fgf21 in gestational diabetes mellitus. Acta Endocrinologica. 2017;13(3):278–281. doi:10.4183/aeb.2017.278
49. Wang Z, Yuan M, Xu C, Zhang Y, Ying C, Xiao X. FGF21 serum levels in the early second trimester are positively correlated with the risk of subsequent gestational diabetes mellitus: a propensity-matched nested case-control study. Front Endocrinol. 2021;12. doi:10.3389/fendo.2021.630287
50. Dekker Nitert M, Scholz-Romero K, Kubala MH, McIntyre HD, Callaway LK, Barrett HL. Placental fibroblast growth factor 21 is not altered in late-onset preeclampsia. Reprod Biol Endocrinol. 2015;13(1). doi:10.1186/s12958-015-0006-3
51. Acquarone E, Monacelli F, Borghi R, Nencioni A, Odetti P. Resistin: a reappraisal. Mech Ageing Dev. 2019;178:46–63.
52. Siddiqui K, George TP. Resistin role in development of gestational diabetes mellitus. Biomark Med. 2017;11(7):579–586. doi:10.2217/bmm-2017-0013
53. Xie Y, Zhou W, Tao XA-OX, Lv H, Cheng ZA-O. Early gestational blood markers to predict preeclampsia complicating gestational diabetes mellitus. Diabetes Metabol Syndr Obes. 2023;Volume 16:1493–1503. doi:10.2147/DMSO.S410912
54. Xue Y, Yang N, Ma L, Gu X, Jia K. Predictive value of the complement factors B and H for women with gestational diabetes mellitus who are at risk of preeclampsia. Pregnancy Hypertens. 2022;30:210–214. doi:10.1016/j.preghy.2022.10.010
55. Yang SY, Fan L, Yin YP. Analysis of high risk and prognostic factors of preeclampsia in pregnant women with gestational diabetes mellitus. Mater Child Health Care China. 2021;36(03):638–640. doi:10.19829/j.zgfybj.issn.1001-4411.2021.03.049
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Impact of Gestational Diabetes Mellitus on the Development of Preeclampsia in Twin Pregnancies: A Retrospective Cohort Study Conducted at a Tertiary Hospital
Wu H, Zhang L, Xie Z, Cai H, Zhang J, Yu L
International Journal of Women's Health 2025, 17:75-86
Published Date: 20 January 2025
Genetic Insights Into Lipid Traits and Lipid-Modifying Drug Targets in Pregnancy Complications: A Two-Sample Mendelian Randomization Study
Shao H, Xu C, Zhang C, Li L, Wu P, Chen Z, Guan R
International Journal of Women's Health 2025, 17:221-234
Published Date: 31 January 2025
A Comparative Cross-Sectional Study Between Gestational Diabetes Mellitus and Preeclampsia: Medication Adherence, Depression and Quality of Life
Noor R, Abbas G, Khurram H, Aslam A, Randhawa FA, Assiri A, Shah S
International Journal of Women's Health 2026, 18:565083
Published Date: 8 January 2026