Back to Journals » Advances in Medical Education and Practice » Volume 17
Program Director Gender and Female Representation in United States Anesthesiology Residency Programs: A Website Content Analysis
Authors Dankievitch K, Malgieri CJ, Corman BHP, Hayward G, Argo J, Kendall MC
Received 1 May 2026
Accepted for publication 24 June 2026
Published 9 July 2026 Volume 2026:17 617742
DOI https://doi.org/10.2147/AMEP.S617742
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sateesh Arja
Korinne Dankievitch, Christopher James Malgieri, Benjamin HP Corman, Geoffrey Hayward, Jonathan Argo, Mark C Kendall
Department of Anesthesiology, Warren Alpert School of Medicine, Brown University, Providence, RI, USA
Correspondence: Mark C Kendall, Department of Anesthesiology, Warren Alpert School of Medicine, Brown University, Providence, RI, 02903, USA, Tel +414-444-5172, Fax +414-444-5090, Email [email protected]
Purpose: Female program directors (PD) have been suggested to influence gender representation and recruitment; however, their impact within anesthesiology residency programs remains unclear. This study evaluated whether PD gender is associated with differences in female resident and faculty representation and anesthesiology residency program website content.
Methods: Anesthesiology residency programs participating in the 2024– 2025 National Resident Matching Program (NRMP) Match were identified through the American Medical Association’s Fellowship and Residency Electronic Interactive Database (FREIDA). Program websites were evaluated for 13 predefined criteria across three domains: leadership and strategic vision, representation, and resources. Program characteristics, including full-time faculty and residents, were extracted. Scores across domains were compared by program director gender. Data presented as mean (standard deviation) or percentage (%).
Results: A total of 160 programs were included in the analysis; 38% were led by female and 62% by male program directors. Women represented 35% of residents and full-time faculty across all programs. Programs led by female program directors was associated with lower female representation among residents (27.9% vs. 42.8%) and full-time faculty (27.4% vs. 44.4%, p< 0.001) compared to male-led programs. The mean overall website content score was 6.45 ± 3.11, with no difference by program director gender (6.82 ± 3.04 vs. 6.21 ± 3.13, p=0.253). However, representation domain scores were higher in programs with female program directors (2.20 ± 0.95 vs.1.82 ± 1.06; p=0.042).
Conclusion: Women represent more than one-third of anesthesiology program directors, residents, and full-time faculty, reflecting continued progress toward gender equity within the specialty. However, programs led by female program directors had lower female representation among residents and full-time faculty, despite stronger emphasis on visual and descriptive representation within website content. Together, these findings suggest that while leadership equity remains important, recruitment, representation, and workforce equity are shaped by broader structural and institutional factors beyond program director gender alone.
Keywords: anesthesiology residency, gender disparity, representation, women in medicine, diversity
Introduction
The role of a residency program director carries significant responsibility in shaping the academic excellence, culture, and development of residency programs. Female gender representation among program directors has been suggested to influence decision-making, increase representation of women, and attract a broader pool of applicants.1 Although the proportion of women in U.S. academic departments has increased over time, it continues to lag behind in female gender representation, despite women comprising about 50% of medical school matriculants.2 This disparity is particularly evident in departmental leadership where women remain underrepresented.
Prior studies investigating residency programs, including anesthesiology and other specialties, have highlighted the importance of gender equality and representation, with some suggesting that increasing the number of women in leadership roles may help address existing gender imbalances.3–5 Additionally, female and underrepresented minority applicants have been shown to seek programs with strong respective representation during the residency application process, suggesting that programs that emphasize a commitment to inclusive practices on their websites may recruit a broader range of applicants.6
Although female representation has increased across medicine, anesthesiology may differ from other specialties in the distribution of women across residency leadership and faculty roles. Residency program websites often serve as applicants’ first exposure to a program’s culture, values, and visible representation, potentially influencing perceptions and recruitment decisions. Together, these highlight the importance of evaluating both gender representation and website content within anesthesiology residency programs.
It remains unclear whether the gender of a program director is associated with measurable differences in program gender composition, such as the representation of female residents and faculty, or whether the gender of the leadership influences how programs present themselves to applicants. The objective of this study was to determine whether the gender of the program director is associated with the proportion of female residents and faculty in Anesthesiology residency programs. Additionally, we evaluated whether program director gender influences website content of anesthesiology residency programs. We hypothesized that female program directors would be associated with higher proportions of female residents and faculty, based on prior literature suggesting that leadership gender may influence program composition. Additionally, we explored differences in anesthesiology website content between programs led by male versus female program directors.
Materials and Methods
This study received exempt status from the Institutional Review Board of Rhode Island (IRB# 2226049) under 45 CFR 46.101(b). Reporting of this study adheres to the STROBE guidelines for reporting observational studies.7
Identification of Anesthesiology Programs
Anesthesiology residency programs participating in the 2024–2025 National Resident Matching Program (NRMP) Match were identified using the American Medical Association’s Fellowship and Residency Electronic Interactive Database (FREIDA).8 Website hyperlinks were accessed and considered functional if they directed the evaluator to the department website. However, if the hyperlink was nonfunctional, producing an error or inactive webpage, the anesthesiology residency program was identified by google search engine. Military-based residency programs were excluded. Program website content was collected between December 1, 2024, and January 31, 2025.
Evaluation of Content
Two independent authors (K.D., B.C.) accessed and evaluated all identified websites. Prior to formal data collection, the reviewers jointly previewed several websites to standardize their interpretation of the assessment criteria; this step focused on clarifying how each criterion should be applied and did not involve discussion of website quality. Each reviewer then assessed each website independently, maintaining individual integrity avoiding any influence from the other reviewer. The sequence of websites was randomized using a computer generated number sequence.
Website content was assessed for the presence of three domains comprising of 13 criteria: Leadership and Strategic Vision (mission statement, initiatives, department message, dedicated section, informational video content, and community engagement), Representation (resident photos, resident biographies, faculty photos, faculty biographies) and Support and Resources (financial, wellness, and mental health). The 13-item website scoring instrument was adapted from previously published literature evaluating similar domains of residency program websites across various medical specialties and was used as a modified tool in this study.6,9 Programs earned a +1 score for each element that was present, and a score of 0 for each element that was absent. After data collection was complete, the total number of criteria met was scored for each residency program (Appendix A). Program scoring was then analyzed by comparing male and female program directors, both for individual criteria, by domain, and by total score.
Program director gender was classified in a binary fashion defined by male or female based on photographs, pronouns (she/her/hers or he/him/his) used in their biographies, and when available, this was supplemented by prior knowledge of the investigators. We did not classify the gender of residents or other faculty members. Information regarding full-time faculty, including the percentage of female faculty for each program, was obtained directly from the FREIDA database. Photo and biography completion rates were scored individually: categories with 50% or more received a score of +1, while those with less than 50% received a score of 0.
Residency programs were categorized by National Institute of Health (NIH) funding, affiliation, geographic location, and program size. Anesthesiology-specific NIH funding dollars were identified using the data released in 2024 by the Blue Ridged Institute for Medical Research.10 Programs were divided into three categories based on affiliation provided by FREIDA; University Based, University and community affiliated, and community-based. Geographic location was divided into four groups based on regions categorized by the US Census Bureau: Northeast, Midwest, South, and West.11 Residency programs were categorized as small (≤19 approved positions), medium (20–49), and large (≥50).12 The number of residents in Postgraduate Year (PGY) 2, PGY-3, and PGY-4 in each program were collected from FREIDA and program website to determine the total program size.
Statistical Analysis
Data are presented as counts (percentages) or as means and standard deviations (SD). Continuous variables were compared between groups using Student’s t-test or the Wilcoxon rank sum test, depending on the distribution of the data. Inter-rater reliability was evaluated using Cohen’s kappa coefficient for binary categorical data. A p-value of <0.05 was considered statistically significant. This descriptive study evaluated all eligible ACGME-accredited Anesthesiology residency programs; therefore, a priori sample size or power calculations were not performed. Subgroup analysis were considered exploratory to describe observed differences within the population. Analysis was performed using IBM SPSS Statistics, version 31 and SigmaPlot 14.5 SystatSoftware, Inc.
Results
A total of 174 anesthesiology residency programs were identified. Fourteen programs were excluded: four lacked functional websites, one was a newly established program projected to begin in 2025, and nine had incomplete or inconclusive information. This resulted in 160 programs included in the analysis. Among the 160 programs, 61 (38%) were led by female program directors and 99 (62%) were led by male program directors (Figure 1). The inter-rater reliability between the two evaluators was excellent, Cohen’s kappa of 0.984 (95% CI 0.98–0.99, p<0.001).
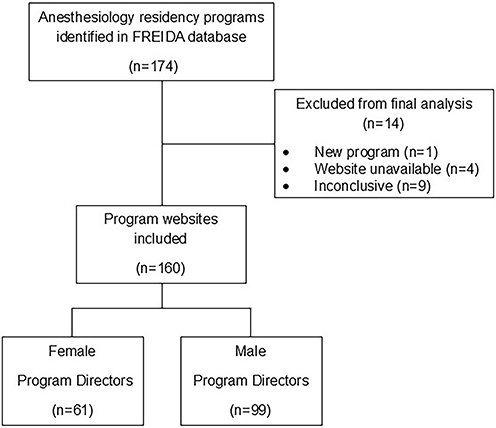 |
Figure 1 Flowchart of website inclusion and exclusion. |
The characteristics of anesthesia residency programs by program director gender are presented in Table 1. Of the four geographic regions, anesthesia residency programs were most concentrated in the Northeast (29%) and least concentrated in the West (23%). The South regions demonstrated significantly higher female program directors (p=0.013) whereas the West region had the fewest female program directors of all four regions, with women accounting for fewer than one-third of program directors (32%, 12/37). Over half of the programs (61%, 98/160), were in cities with populations greater than 250,000 and about two-thirds (62.5%, 100/160) were university-based which showed the largest concentration of female program directors among medial affiliations. Although most programs reported no direct university funding (63.8%, 102/160), programs with female program directors were more likely to receive funding than male led programs (43% vs 32%), although this difference was not significant (p=0.188). Medium sized programs (20–49 residents) were the most common, representing 45% of all programs and had the highest number of female program directors (37.5%, 27/72).
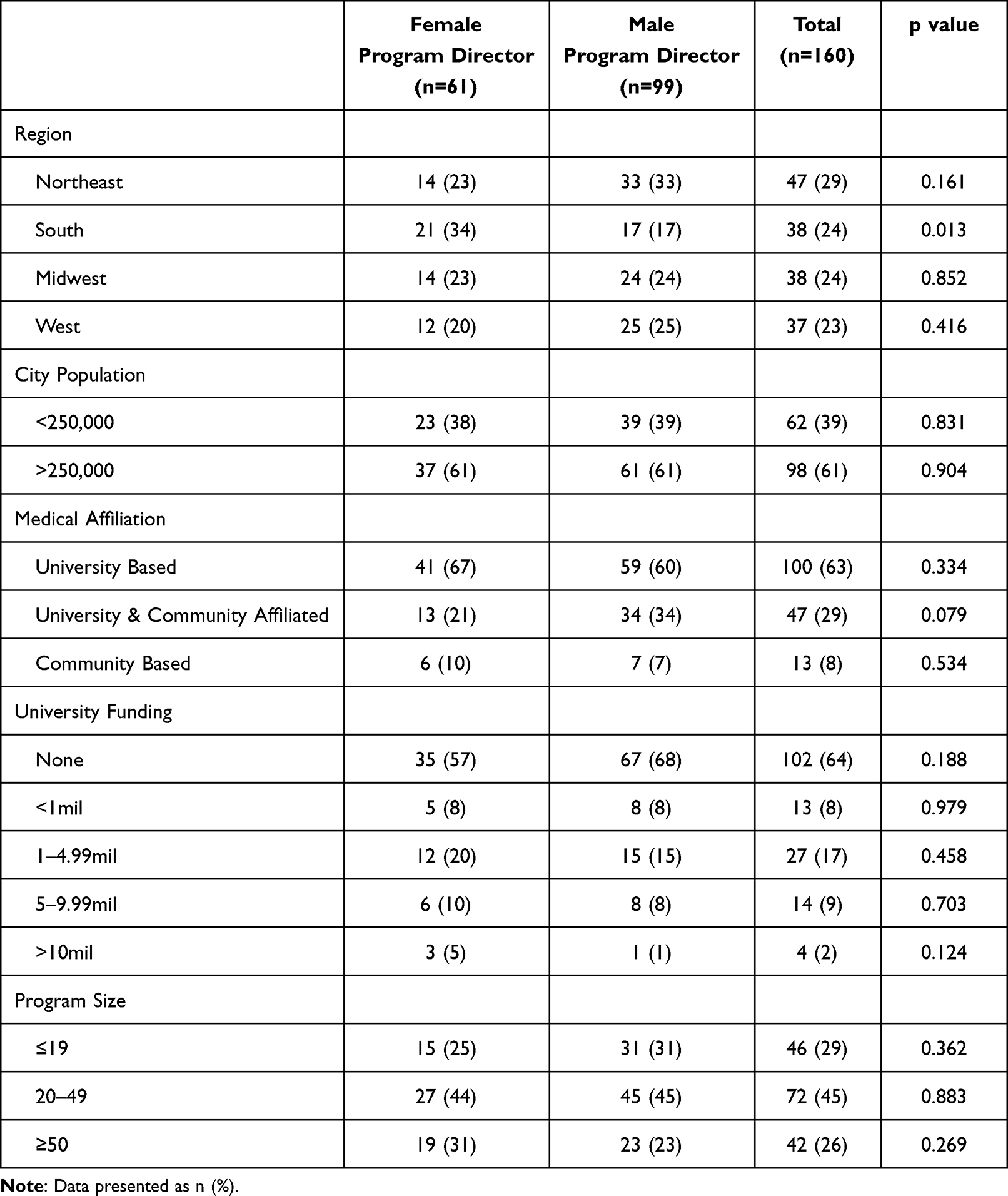 |
Table 1 Characteristics of Evaluated Anesthesiology Residency Programs |
The resident and faculty distribution by program director gender is presented in Table 2. Women represented approximately 35% (2009/5727) of residents and 35% (3463/9774) of full-time faculty across all programs. Programs led by female program directors had lower female representation in both residents (27.9% vs. 42.8%, p<0.001) and full-time faculty (27.4% vs 44.4%, p<0.001).
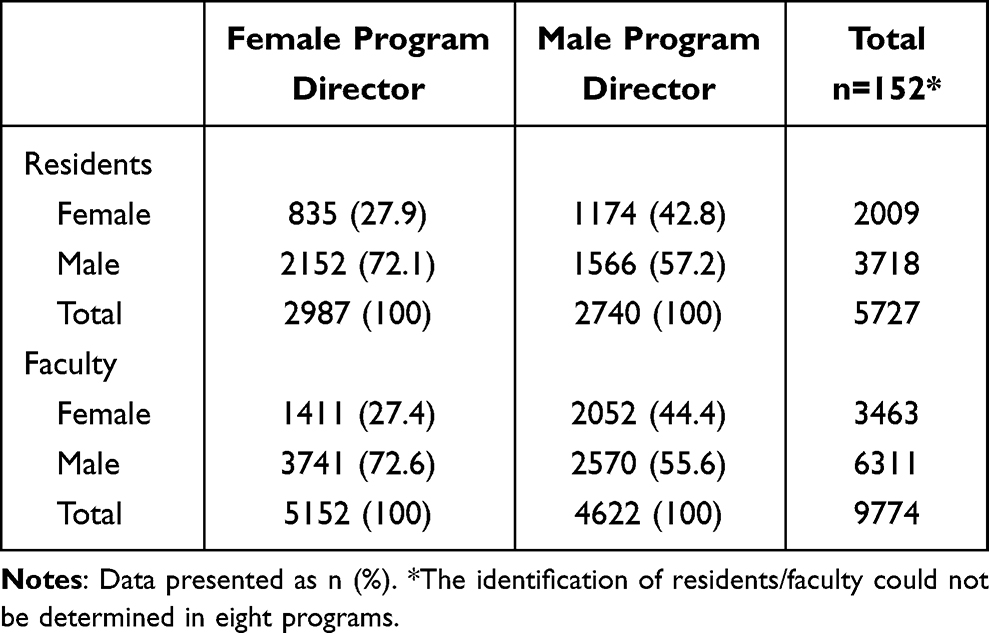 |
Table 2 Residents and Faculty Distribution by Program Director Gender |
Web-based criteria for leadership and strategic vision, representation, and resources among anesthesia residency programs according to program director gender are presented in Table 3. Seven programs (4.4%) did not meet any of the 13 criteria. No programs met all 13 criteria, however 15.0% (24/160) of programs scored greater than 10pts. Of those programs that scored greater than 10pts, only 4 programs scored 12pts. Eleven program websites (6.9%) did not provide names, photographs, or biographies for current residents and faculty. Within the leadership and strategic vision domain, the equal opportunity mission statement was the most frequently met criterion (67.6%, 108/160), followed by resident photos in the recruitment domain (85%, 136/160) and wellness resources in the support and resources domain (74%, 119/160). The least commonly met criteria across all domains were informational video content (23%, 36/160), faculty biographies (12%, 19/160), and financial resources (12%, 19/160).
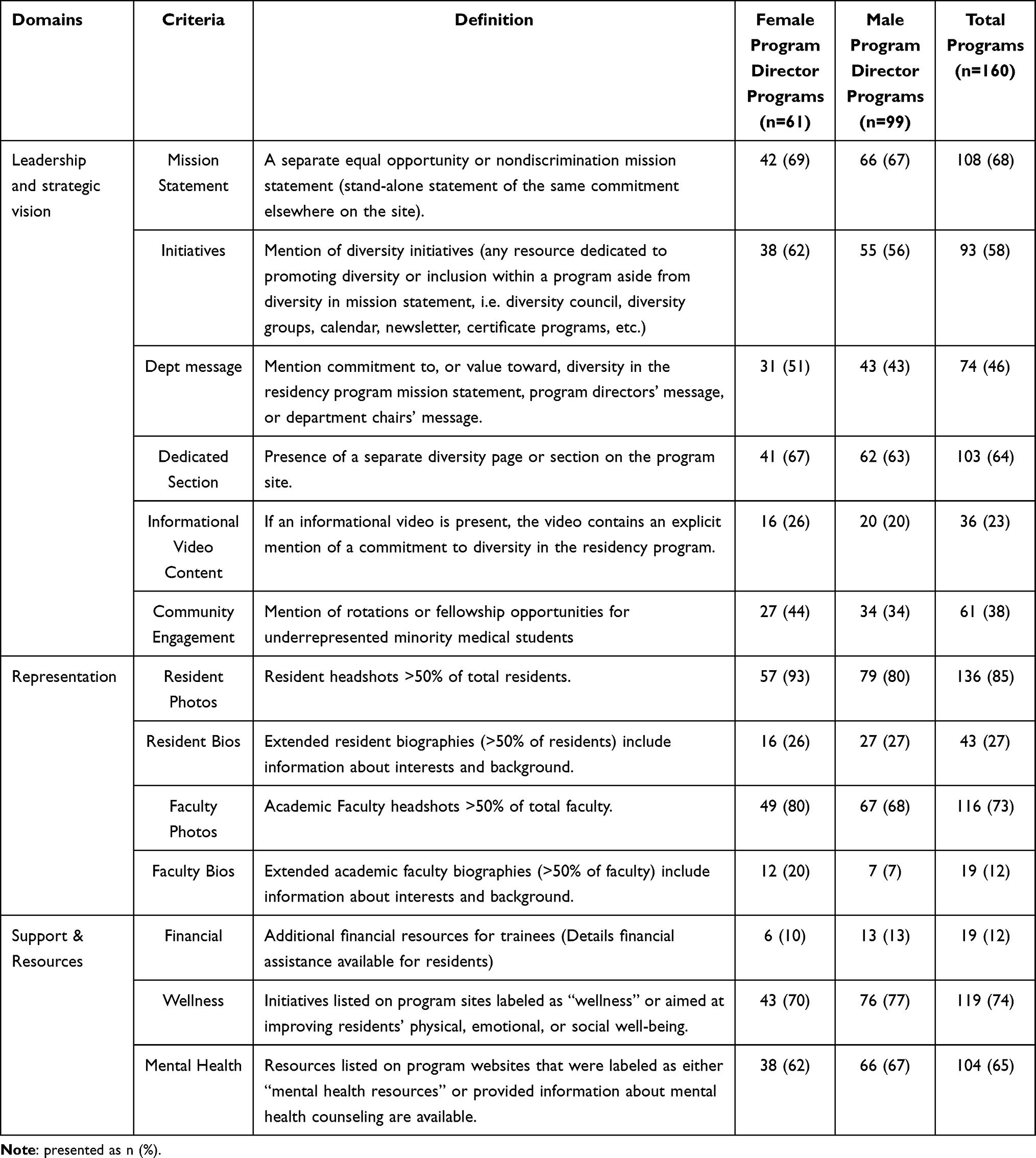 |
Table 3 Evaluation of Leadership, Representation, and Resources of Anesthesiology Residency Programs Websites by Program Director Gender |
The comparison of domain scores between female and male program directors in anesthesia residency programs are presented in Table 4. The median overall score was 6.45±3.11 across all programs with no significant difference in overall scores between female and male program directors (6.82±3.04 vs. 6.21±3.13; median difference 0.61 (−0.39, 1.60), p=0.253). In the representation domain, programs led by female program directors scored higher than those led by male program directors (2.20±0.95 vs. 1.82±1.06 p=0.042). The leadership and strategic vision and support, and resources scores were similar between groups.
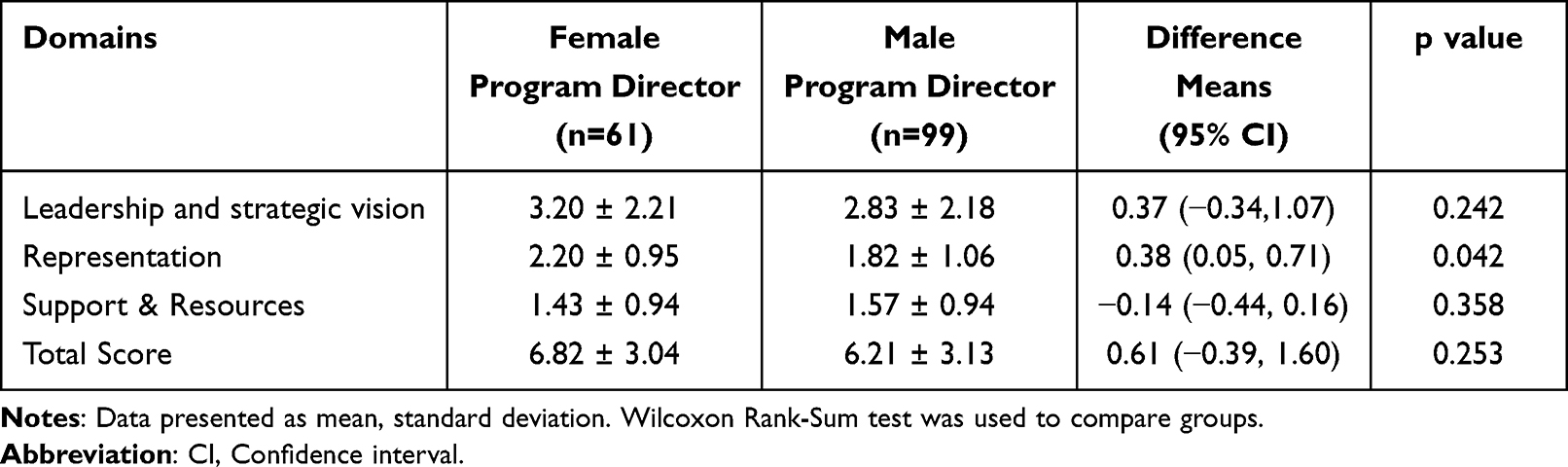 |
Table 4 Total and Domain Specific Website Content Scores by Program Director Gender |
Domain scores by program size and program director gender are shown in Table 5. Overall, there were no significant differences between program size and program director gender. However, among large programs, female program directors had higher representation scores than male program directors (2.53±0.84 vs. 1.87±0.97), mean difference of 0.66 (95% CI, 0.08–1.23), although this difference did not reach statistical difference, p=0.051).
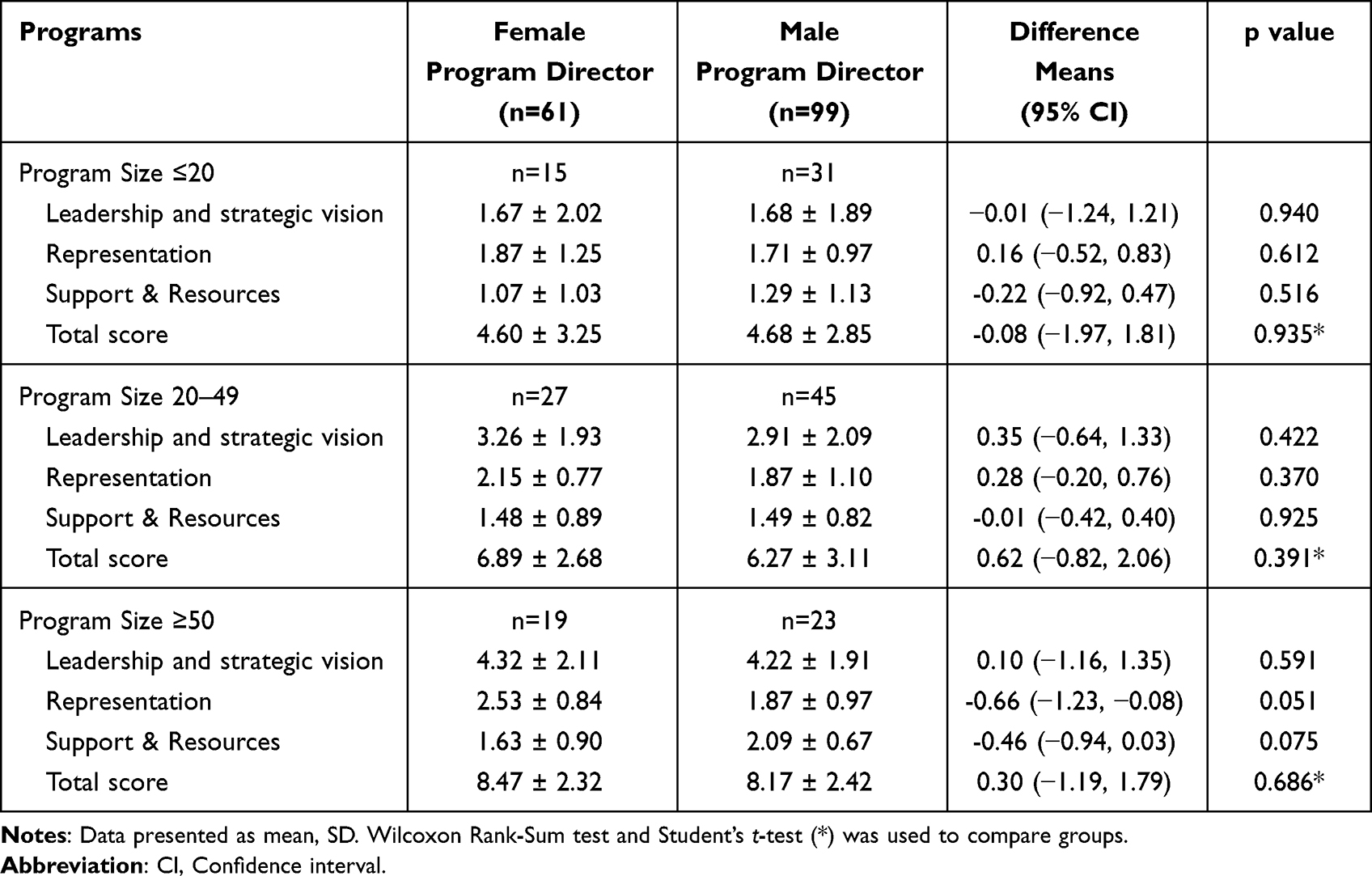 |
Table 5 Website Domain Scores by Program Director Gender and Program Size |
Discussion
Our most important finding was that females comprised 38% of anesthesiology residency program leadership positions, compared to 62% held by men. This represents a meaningful increase from prior literature reporting female representation of 28% in 2009 and 32% in 2019, suggesting a gradual yet sustained trend toward greater gender inclusivity within anesthesiology leadership.13,14 In particular, the current proportion of female program directors in anesthesiology exceeds that observed in other specialties, including orthopedic surgery (12%), gastroenterology (22.7%), and general surgery (23.2%).15–17 Taken together, these findings suggest that anesthesiology has comparatively greater female representation in residency leadership than many peer specialties.
Website content across anesthesiology residency programs varied widely, with 48% of department websites scoring below 50% of the 13 evaluated criteria. These findings corroborate a 2022 evaluation of anesthesiology residency websites, which similarly reported that programs met fewer than half of the analyzed domains, suggesting little improvement in web content comprehensiveness over time.6 Although program director gender was not associated with overall content scores, programs led by female directors scored higher on representation related criteria compared with those led by male directors, while leadership and strategic vision and support/resources scores were similar between groups. Our scoring system was adapted from prior literature and modified for this study; therefore, some subjectivity may remain. Future studies could strengthen this area by developing and validating a more standardized, objective scoring instrument. It is also important to acknowledge that website structure and content may be constrained by institutional policies, departmental website architecture, or administrative requirements, which may limit the extent to which programs can independently shape their online presence.
Among all programs, women accounted for 35% of full-time faculty and 35% of residents, which is consistent with prior national and regional estimates, including a 2024 analysis reporting an average female faculty proportion of 34.1%.18 This finding underscores the persistent gender imbalance within anesthesiology training programs. Interestingly, programs led by female program directors had lower female representation among both residents and full-time faculty compared with programs led by male program directors. Although counterintuitive, this finding is consistent with prior studies across general surgery, internal medicine, and orthopedic surgery, demonstrating no significant association between the gender of program leadership and the proportion of female applicants or matriculants.1,15,19,20
Multiple contextual factors likely contribute to this pattern. Workforce composition is shaped by long standing institutional history, baseline faculty demographics, regional workforce characteristics, and historical recruitment practices, all of which may confound the relationship between program director gender and current gender representation.21,22 Program director tenure is also an important consideration; recently appointed female program directors may not yet have had sufficient time to influence resident recruitment patterns or faculty hiring. Because faculty and resident demographics reflect recruitment practices over many years, current workforce composition may not reflect the influence of newer leadership. Accordingly, these findings should not be interpreted as evidence that female leadership directly determines gender representation. Instead, they highlight the multifactorial nature of recruitment, mentorship, and retention, and suggest that improving gender representation in anesthesiology will require broader structural and cultural changes rather than relying on program director gender alone.23,24
Visual representation on anesthesiology program websites may influence how applicants perceive program culture. An ACGME survey conducted after the 2014 anesthesiology match suggested that the presence of female residents attracted more female applicants.20 Prior studies have also shown that medical students value faculty and resident photographs and biographies when evaluating program culture.25,26 In addition, a 2022 survey found that 42% of anesthesiology residents considered the presence of women among diverse faculty to be important in their decision to pursue the specialty.27,28 Images of faculty and residents can provide insight into the workplace environment and shape applicant impressions; however, our study did not assess the impact of such content. Because we did not directly evaluate applicant perceptions, recruitment behavior, or residency match outcomes, any statements regarding the influence of website content on applicant interest or program transparency should be interpreted cautiously. Nonetheless, prior studies suggest that underrepresentation on program websites may be associated with a decreased sense of belonging,25–29 and anesthesiology residency programs may benefit from prioritizing inclusion, representation, and accessible resources on their websites.
Anesthesiology programs in the Southern region were more often led by female program directors than those in other regions. In contrast, national physician workforce data demonstrate higher proportions of female physicians in the Northeast and West.30 Together, these findings suggest that regional patterns in program director leadership representation do not necessarily mirror broader national workforce trends. Given the limited scope of our data, regional differences should be interpreted cautiously and should not be assumed to reflect broader structural or cultural priorities without further evidence. Further investigation is needed to understand the institutional, historical, and regional factors that shape gender representation in anesthesiology leadership.
Limitations
Our study should be interpreted in the context of several limitations. First, we relied on publicly available information and as a result, our findings may not have captured all internal or updated program information. Website content may not be a completely reliable metric for assessing gender representation because it reflects what programs choose to display rather than direct verification of program composition. Furthermore, website structure and content may be constrained by institutional policies, departmental website architecture, or administrative requirements, which can limit how much program specific information is included. Nonetheless, website content remains relevant because it reflects the information publicly available to applicants and thus provides insight into how residency programs present gender representation. Second, our analysis focused on the gender of the current program directors without directly confirming their gender identity. We acknowledge that external appearance does not necessarily reflect gender identity. Similarly, the gender of faculty and residents was determined from characteristics visible in photographs and the pronouns used in biographical descriptions, which may have introduced misclassification bias. Third, although our scoring system was adapted from previously published criteria, the subjective weighting of certain variables may have influenced our results. Fourth, this was a cross-sectional study based on content available at the time of data collection. Subsequent updates to the FREIDA database or anesthesiology programs websites may not be reflected in our analysis. Finally, we did not evaluate program directors’ academic rank, clinical experience, or tenure. Programs with newly appointed female program directors may not yet have undergone enough recruitment cycles for leadership influence to be reflected in resident or faculty gender composition, which may partially explain the lower proportion of female residents and full-time faculty observed in these residency programs.
Conclusion
Women account for more than one-third of anesthesiology program directors, signaling meaningful progress toward gender balance in residency program leadership. Programs led by women demonstrated a greater emphasis on representation through more extensive biographies and photographs, which may enhance transparency and applicant interest. While program director gender representation remains important, our findings suggest that recruitment, representation, and workforce equity are influenced by factors beyond the gender of program directors alone. As this was an observational, cross-sectional study, future studies should explore the influence of leadership development initiatives and equitable evaluation practices in supporting the recruitment, retention, and advancement of women in anesthesiology.
Abbreviations
ACGME, Accreditation Council for Graduate Medical Education; CI, Confidence Interval; FREIDA, Fellowship and Residency Electronic Interactive Database; IRB, Institutional Review Board; NIH, National Institute of Health; NRMP, National Resident Matching Program; PGY, Postgraduate Year; PD, Program Director; SD, Standard Deviation.
AI Disclosure
Grammarly (basic version) software was used for spelling and proper syntax in the presented manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Medepalli K, Purdon S, Bade RM, Glassberg MK, Burnham EL, Gershengorn HB. Association of women leaders with women program director and trainee representation across US academic internal medicine. J Gen Intern Med. 2023;38(1):57–10. doi:10.1007/s11606-022-07635-w
2. Lautenberger DM, Dandar VM. The State of Women in Academic Medicine 2023-2024: Progressing Toward Equity. Washington, DC: AAMC; November 2024.
3. Marroquin BM. Wake up to the gender gap in academic anesthesiology and address the pipeline. Proc. 2022;36(1):135–137. doi:10.1080/08998280.2022.2128624
4. Gonzalez LS, Fahy BG, Lien CA. Gender distribution in United States anaesthesiology residency programme directors: trends and implications. Br J Anaesth. 2020;124(3):e63–e69. doi:10.1016/j.bja.2019.12.010
5. Sethi S, Edwards J, Webb A, Mendoza S, Kumar A, Chae S. Addressing gender disparity: increase in female leadership increases gender equality in program director and fellow ranks. Dig Dis Sci. 2022;67(2):357–363. doi:10.1007/s10620-020-06686-5
6. Cohen SA, Cohen LE, Perez FD, Macario A, Xie J. Content evaluation of residency websites for all 159 anesthesiology ACGME programs in the USA. J Educ Perioper Med. 2022;24(1):E683. doi: 10.46374/volxxiv_issue1_xie.
7. Chu LF, Young CA, Zamora AK, et al. Self-reported information needs of anesthesia residency applicants and analysis of applicant-related web sites resources at 131 United States training programs. Anesth Analg. 2011;112(2):430–439. doi:10.1213/ANE.0b013e3182027a94
8. Avery L, Rotondi M. More comprehensive reporting of methods in studies using respondent driven sampling is required: a systematic review of the uptake of the STROBE-RDS guidelines. J Clin Epidemiol. 2020;117:68–77. doi:10.1016/j.jclinepi.2019.09.024
9. American Medical Association. FREIDA™. The AMA residency and fellowship programs database. Available from: https://freida.ama-assn.org.
10. Blue Ridge Institute for Medical Research. BRIMR rankings of NIH funding in 2024. Available from: https://brimr.org/brimr-rankings-of-nih-funding-in-2024/U.S.
11. U.S Census Bureau. Census Regions and Divisions of the United States. Available from: https://www2.census.gov/geo/pdfs/maps-data/maps/reference/us_regdiv.pdf.
12. Kenevan MR, Stewart TM, Warner MA, Rose SH, Long TR. The changing characteristics of anesthesiology program directors. J Educ Perioper Med. 2018;20(3):E625.
13. Long TR, Brown MJ, Elliott BA, Rose SH. Characteristics of anesthesiology residency program directors. J Clin Anesth. 2010;22(8):583–586. doi:10.1016/j.jclinane.2010.05.005
14. Esmaeeli S, Seu M, Akin J, Nejatmahmoodalilioo P, Knezevic NN. Program directors research productivity and other factors of anesthesiology residency programs that relate to program doximity ranking. J Educ Perioper Med. 2021;23(2):E662. doi:10.46374/volxxiii_issue2_knezevic
15. Dias R, Herzog I, Alomary S, Beebe KS. Is program director gender associated with gender diversity among orthopaedic surgery residency programs? Clin Orthop Relat Res. 2024;482(8):1351–1357. doi:10.1097/CORR.0000000000003070
16. Jamorabo DS, Chen R, Gurm H, et al. Women remain underrepresented in leadership positions in academic gastroenterology throughout the United States. Ann Gastroenterol. 2021;34(3):316–322. doi:10.20524/aog.2021.0597
17. Hughes A, Im K, Zhu J, Saunders B. A descriptive analysis of general surgery residency program directors in the United States. Am J Surg. 2022;224(5):1247–1251. doi:10.1016/j.amjsurg.2022.06.020
18. Novoa J, Harmon SR, Pandit S, et al. Female faculty representation in anesthesiology: a retrospective cross-sectional analysis. Cureus. 2024;16(12):e75045. doi:10.7759/cureus.75045
19. Pelley E, Carnes M. When a specialty becomes “women’s work”: trends in and implications of specialty gender segregation in medicine. Acad Med. 2020;95(10):1499–1506. doi:10.1097/ACM.0000000000003555
20. Ren AL, Choi J, Wren SM. Female department chairs and diversity among general surgery applicants and entering residents. Surg Open Sci. 2025;28:101–103. doi:10.1016/j.sopen.2025.10.008
21. Kranner PW, Mussehl DA, Hess AS. Gender diversity in anesthesiology programs: the role of current residents and department leadership in the 2014 match results. J Educ Perioper Med. 2016;18(1):E401.
22. Winkel AF, Telzak B, Shaw J, et al. The role of gender in careers in medicine: a systematic review and thematic synthesis of qualitative literature. J Gen Intern Med. 2021;36(8):2392–2399. doi:10.1007/s11606-021-06836-z
23. Knoepfler M, Liu C, Narkhede A, Cao B, Gupta S. Coaching, connection, and the role of gender: a qualitative study of physician mentor perspectives. J Gen Intern Med. 2026. doi:10.1007/s11606-026-10255-3
24. Gisselbaek M, Marsh B, Soriano L, et al. Gender and Race/Ethnicity dynamics in anesthesiology mentorship: results of a European survey. BMC Anesthesiol. 2024;24(1):311. doi:10.1186/s12871-024-02692-6
25. Read CE, Tracz JA, Mhaimeed N, Mainville RN, Elzie CA. Examination of residency program websites for the use of gendered language and imagery. BMC Med Educ. 2023;23(1):697. doi:10.1186/s12909-023-04677-4
26. Ku MC, Li YE, Prober C, Valantine H, Decisions GSC. Decisions: how program diversity influences residency program choice. J Am Coll Surg. 2011;213(2):294–305. doi:10.1016/j.jamcollsurg.2011.04.026
27. Patel S, Lin KK, Milam AJ, et al. Diversity, equity, and inclusion among anesthesiology trainees. Womens Health Rep (New Rochelle). 2022;3(1):414–419. doi:10.1089/whr.2021.0123
28. Hayward G, Kendall MC, Bui D, et al. Characteristics of anesthesia program that graduating medical students find important: a cross-sectional survey. J Clin Anesth. 2025;103:111791. doi:10.1016/j.jclinane.2025.111791
29. Gaeta TJ, Birkhahn RH, Lamont D, Banga N, Bove JJ. Aspects of residency programs’ web sites important to student applicants. Acad Emerg Med. 2005;12(1):89–92. doi:10.1197/j.aem.2004.08.047
30. U.S. Physician Workforce Data Dashboard. https://www.aamc.org/data-reports/report/us-physician-workforce-data-dashboard. Available from:
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.