Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Prognostic Value of the ROX Index for Mortality in Chronic Obstructive Pulmonary Disease: A Retrospective Cohort Study Using the MIMIC-IV Database
Authors Liu K ![]() , Fu Z, Luo D, Xiao H, Wu Q
, Fu Z, Luo D, Xiao H, Wu Q
Received 25 October 2025
Accepted for publication 9 March 2026
Published 14 March 2026 Volume 2026:21 576654
DOI https://doi.org/10.2147/COPD.S576654
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Kai Liu,1,* Zehui Fu,1,* Dahang Luo,1,* Hua Xiao,2 Qiaobin Wu1
1Department of Emergency, the Affiliated Shunde Hospital of Jinan University, Foshan, Guangdong, People’s Republic of China; 2Department of Nephrology, the Affiliated Shunde Hospital of Jinan University, Foshan, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hua Xiao, Department of Nephrology, the Affiliated Shunde Hospital of Jinan University, Foshan, Guangdong, People’s Republic of China, Email [email protected] Qiaobin Wu, Department of Emergency, the Affiliated Shunde Hospital of Jinan University, Foshan, Guangdong, People’s Republic of China, Email [email protected]
Objective: While the ROX index has been extensively studied in acute hypoxemic respiratory failure, its prognostic value in patients with chronic obstructive pulmonary disease (COPD) remains unclear. This study aimed to investigate the association between the ROX index and mortality in critically ill COPD patients.
Methods: We conducted a retrospective cohort study of 2,176 critically ill COPD patients admitted to the intensive care unit (ICU) using the MIMIC-IV database, a publicly available repository of critically ill patients admitted to intensive care units. The ROX index was categorized into quartiles. The association between the ROX index and all-cause mortality was analyzed using restricted cubic splines (RCS) and multivariable Cox proportional hazards models. Subgroup analyses were performed to validate the robustness of the findings.
Results: RCS analysis revealed a nonlinear, L-shaped association between the ROX index and mortality, with an inflection point at 9.72. Below this threshold, each unit increase in the ROX index was associated with a significant 16% reduction in 28-day mortality (HR: 0.84, 95% CI: 0.78– 0.90, P< 0.001). Above 9.72, no significant association was observed (HR: 1.01, 95% CI: 0.96– 1.07, P = 0.628). Compared to the lowest quartile (Q1), patients in Q2 (HR=0.75, 95% CI: 0.59– 0.96, P=0.021), Q3 (HR=0.60, 95% CI: 0.46– 0.77, P< 0.001), and Q4 (HR=0.58, 95% CI: 0.45– 0.75, P< 0.001) had progressively lower 28-day mortality risks; Similar trends were observed for 3-month and 1-year mortality. The association remained statistically significant across all predefined subgroups (all P< 0.05).
Conclusion: The ROX index is a practical bedside tool for risk stratification in critically ill COPD patients. Its predictive value follows a threshold-dependent pattern, with values below approximately 9.72 independently associated with increased mortality. This makes it particularly useful for the early identification of high-risk patients in the ICU.
Keywords: ROX index, chronic obstructive pulmonary disease, MIMIC database, restricted cubic splines
Introduction
Chronic obstructive pulmonary disease (COPD) is a prevalent respiratory condition characterized by persistent and progressive airflow limitation caused by airway and/or alveolar abnormalities, including chronic bronchitis and emphysema.1,2 Its typical clinical presentation includes chronic cough and sputum production, which significantly impair patients’ quality of life. As a leading cause of global morbidity, mortality, and healthcare utilization, COPD poses a substantial and growing public health burden.3 Prevalence increases with age, and World Health Organization projections indicate that COPD is set to become the third leading cause of death worldwide by 2030.4,5 Consequently, the early identification of high-risk patients is critical for improving outcomes. However, existing prognostic tools for COPD, such as the BODE index or DECAF score, often depend on complex composite measures, specialized laboratory tests, or assessments unsuitable for rapid, bedside application during acute exacerbations.6,7 This highlights a need for simple, readily available indices for risk stratification in acute care settings.
The ROX index, defined as the ratio of pulse oximetric saturation (SpO2) to the fraction of inspired oxygen (FiO2) divided by respiratory rate (RR), meets this need by simultaneously quantifying gas exchange efficiency (SpO2/FiO2) and respiratory load (RR). It gained widespread adoption during the COVID-19 pandemic for prognosticating outcomes in acute hypoxemic respiratory failure (AHRF)8,9 and is primarily used to assess the response to high-flow nasal cannula (HFNC) therapy and predict the need for intubation.10–13 Its physiological rationale is particularly relevant to COPD exacerbations, which are frequently driven by worsening ventilation-perfusion mismatch (affecting SpO2/FiO2) and dynamic hyperinflation leading to tachypnea and increased work of breathing (reflected in RR). Due to its ease of use, non-invasive nature, and suitability for repeated assessment, the index represents a practical bedside tool with potential advantages in settings requiring rapid clinical decisions.14,15
The prognostic role of the ROX index in COPD, however, remains less clear. Although it has been used to predict the treatment outcomes of HFNC in patients with acute exacerbation of COPD,16 its relationship with mortality has not been established. To address this, we conducted a retrospective cohort study using the MIMIC-IV database to investigate the association between the ROX index and 28-day all-cause mortality in critically ill COPD patients, identify potential thresholds, and assess the consistency of this association across subgroups.
Materials and Methods
The data utilized in this study were obtained from the Medical Information Mart for Intensive Care IV (MIMIC-IV) database. This database encompasses approximately 190,000 hospital admissions of patients who were admitted to the Beth Israel Deaconess Medical Center (BIDMC) over the period from 2008 to 2019. It serves as a publicly accessible repository containing data on critically ill patients admitted to the intensive care unit (ICU) of a tertiary academic medical center. The database contains comprehensive patient information, including demographic characteristics, vital signs, laboratory results, diagnoses, medication records, in-hospital survival status, and follow-up mortality data obtained from the U.S. Social Security Administration Death Master File. All patient identifiers and private information were anonymized to protect patient rights; This study has obtained ethical approval from the Medical Research Ethics Committee of the Affiliated Shunde Hospital of Jinan University (code JDSY-LL-2026002). Author KL completed the required online course and examination and was granted access to the MIMIC-IV database (Certification ID: 54890087).
The patient selection criteria were as follows: Inclusion criteria consisted of: (1) adult patients (aged ≥18 years); (2) a diagnosis of chronic obstructive pulmonary disease (COPD), confirmed by International Classification of Diseases codes recorded during hospitalization (ICD-9: 491.20, 491.21, 491.22, 496; ICD-10: J44.0, J44.1, J44.9). Exclusion criteria were: (1) no ICU admission during hospitalization; (2) missing records of oxygen saturation (SpO2), respiratory rate (RR), or fraction of inspired oxygen (FiO2) within the first 24 hours of ICU admission, which are required for calculating the ROX index; and (3) multiple ICU or hospital admissions, for whom only the first admission was retained. Data extraction was performed using Navicat Premium software and Structured Query Language (SQL). This being a retrospective cohort study utilizing an existing database, a priori power calculation was not performed. The sample included all eligible patients, and the large cohort size (N=2,176) is considered adequate for robust multivariable modeling and subgroup analyses.
Collected variables comprised demographic information (gender, age, height, weight, race [White, Black, or Other], and admission type [Emergency/Elective]); disease severity scores (APS III, SAPS II, SOFA score, and Charlson Comorbidity Index); comorbidities (including severe liver disease, malignant cancer, renal disease, myocardial infarction, congestive heart failure, cerebrovascular disease, and diabetes); vital signs (calculated as mean values from the first 24 hours after ICU admission, including temperature [°C], heart rate [beats/min], respiratory rate [breaths/min], mean blood pressure [mmHg], oxygen saturation [%], and blood glucose [mg/dL]); and laboratory parameters (also averaged over the first 24 hours in the ICU, including WBC [K/μL], hemoglobin [g/dL], platelets [K/μL], bicarbonate [mEq/L], ALT [U/L], AST [U/L], albumin [g/dL], blood urea nitrogen [mg/dL], sodium [mEq/L], calcium [mEq/L], potassium [mEq/L], chloride [mEq/L], anion gap [mmol/L], INR, PT [seconds], APTT [seconds], PH, PaO2 [mmHg], PaCO2 [mmHg], oxygenation index [mmHg], creatinine [mg/dL], and lactate [mmol/L]). Furthermore, the presence of an acute exacerbation of chronic obstructive pulmonary disease (AECOPD) during hospitalization was documented.
The ROX index was calculated for each patient using data from the first 24 hours after ICU admission. Specifically, all recorded measurements of SpO2, FiO2, and respiratory rate (RR) within this 24-hour window were extracted. In the MIMIC-IV database, these vital signs are typically charted at variable intervals, often hourly or more frequently during active clinical care. For each patient and for each of the three parameters (SpO2, FiO2, RR), a mean value was calculated from all available data points within the first 24 hours. The final ROX index was then computed according to the formula: ROX = (SpO2 / FiO2) / RR. Table S1 presents baseline characteristics and outcomes of patients with and without complete ROX data, allowing assessment of selection bias.
Patients were divided into four equal groups based on their ROX values: Q1 (ROX≤7.79), Q2 (7.79<ROX≤9.72), Q3 (9.72<ROX≤12.26), and Q4 (ROX>12.26). The primary outcome was 28-day all-cause mortality, and secondary outcomes included 3-month mortality, 1-year mortality, in-ICU mortality, and in-hospital mortality.
Categorical variables are presented as frequencies and percentages, with group comparisons performed using the χ2-test or Fisher’s exact test, as appropriate. Continuous variables were first assessed for normality using the Shapiro–Wilk test. Variables following a normal distribution are reported as mean ± standard deviation (SD) and were compared using the one-way ANOVA or Student’s t-test; non-normally distributed variables are presented as median with interquartile range (IQR) and were compared using the Kruskal–Wallis test or Mann–Whitney U-test.
The nonlinear relationship between ROX and 28-day mortality risk was assessed using restricted cubic splines to identify potential inflection points. Survival curves were plotted using Kaplan–Meier curves, and the Log rank test was applied for comparison. Hazard ratios (HR) and 95% confidence intervals (CI) were calculated using Cox proportional hazards regression, with the proportional hazards assumption verified using Schoenfeld residuals (global test P>0.05). Variables with a P-value < 0.1 in univariate Cox regression analysis were initially considered for inclusion in the multivariate model (Table S2). Based on clinical relevance and prior literature, the final multivariate Cox model was further adjusted for age, race, gender, BMI, admission type, MBP, glucose, SAPSII, Charlson Comorbidity Index, severe liver disease, renal disease, congestive heart failure, sepsis, AECOPD, WBC, hemoglobin, creatinine, sodium, potassium, PT, lactate, PH, PaO2, and PaCO2.
To examine the heterogeneity and robustness of the association between the ROX index and outcomes in patients with COPD, subgroup analyses were conducted based on gender, age (≤65 />65 years), race (White/non-White), BMI (≤30 />30), SAPS II score (≤35 />35), sepsis (yes /no) and AECOPD (yes /no).
Missing data were handled by multiple imputation (5 imputations) using the “mice” package in R. Variables with a missing rate exceeding 20% were excluded. Multicollinearity was assessed using the variance inflation factor (VIF), with VIF<5 indicating no significant collinearity (Table S3). All analyses were two-sided, and a P<0.05 was considered statistically significant. Analyses were performed using R version 4.2.3.
Results
The MIMIC-IV database (version 2.0) included 14,279 adult patients diagnosed with COPD. After applying the exclusion criteria, the final study cohort comprised 2,176 patients, who were stratified into four groups based on ROX index quartiles. The detailed patient selection process is presented in Figure 1.
 |
Figure 1 Flowchart of patient selection. Quartile 1: ROX index≤7.79; Quartile 2: 7.79<ROX index≤9.72; Quartile 3: 9.72<ROX index≤12.26; Quartile 4: ROX index>12.26. |
The study ultimately included 2,176 patients with a median age of 71.55 (63.58, 78.91) years, including 1,250 males (57.44%). As the ROX index progressively increased, patients exhibited gradual decreases in BMI, SAPS II score, APS III score, heart rate, respiratory rate, white blood cell count, and lactate levels, while oxygen saturation and the oxygenation index showed a corresponding upward trend. Detailed baseline characteristics are presented in Table 1.
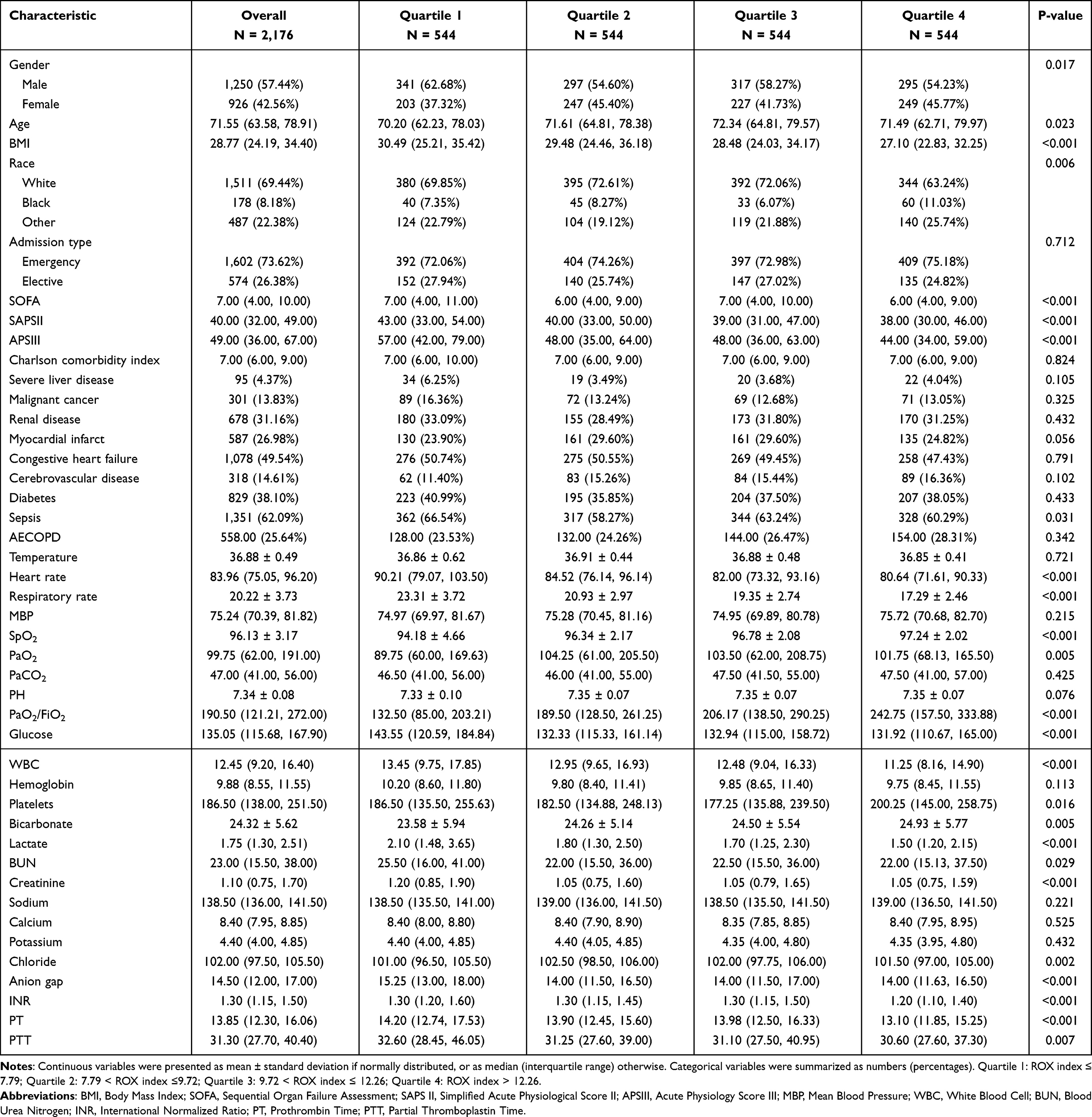 |
Table 1 Baseline Characteristics of Patients with Chronic Obstructive Pulmonary Disease According to the ROX Index |
Figure 2 shows the restricted cubic spline curve depicting the association between the ROX index and all-cause mortality in COPD patients. An L-shaped relationship was observed between the ROX index and mortality, both during hospitalization and throughout the follow-up period. To quantify this association, a simple piecewise linear model was fitted. When the ROX index was below 9.72, each unit increase in the ROX index was associated with a significant reduction in 28-day mortality risk (HR per SD, 0.84 [95% CI 0.78–0.90], P<0.001). Above a ROX index of 9.72, the risk curve plateaued, and no significant association was found between the ROX index and 28-day mortality (HR per SD, 1.01 [95% CI 0.96–1.07], P =0.628). To assess the robustness of the identified inflection point, we performed a bootstrap sensitivity analysis with 1,000 resamples, which yielded a 95% confidence interval of 8.74 to 10.35 for the threshold value (Figure S1 and Figure S2), confirming the stability of the 9.72 cutoff. Furthermore, similar associations were observed in Cox proportional hazards analyses for 3-month mortality, 1-year mortality, in-ICU mortality, and in-hospital mortality.
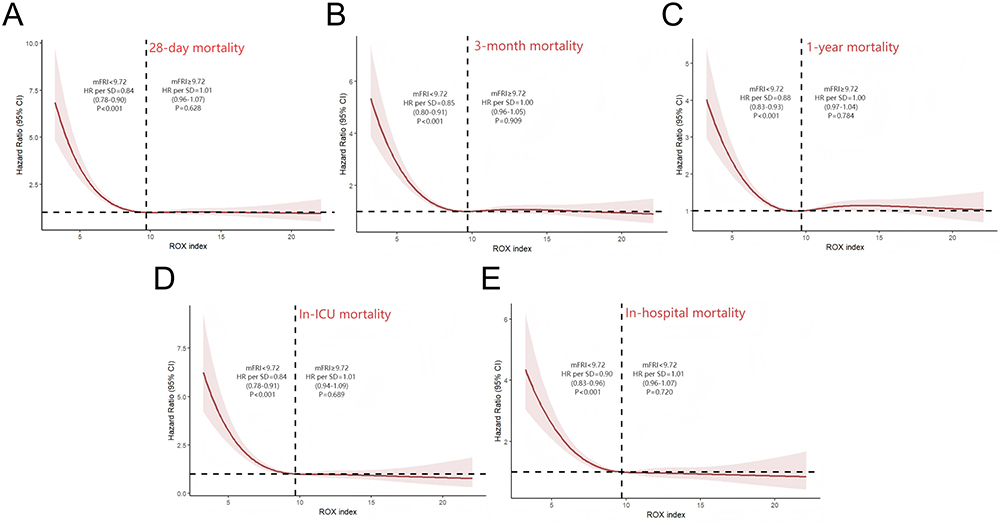 |
Figure 2 Restricted cubic splines showing the association between the ROX index and all-cause mortality risk in patients with chronic obstructive pulmonary disease. (A) 28-day mortality. (B) 3-month mortality. (C) 1-year mortality. (D) In-ICU mortality. (E) In-hospital mortality. |
As shown in Figure 3, patients were categorized into four groups according to ROX index quartiles. Kaplan-Meier survival analysis revealed a progressive decrease in 28-day mortality with increasing ROX index (35.29% vs. 21.88% vs. 18.93% vs. 17.46%, log-rank P<0.001), although the difference between Quartile 3 and Quartile 4 did not reach statistical significance. Similar trends were observed for 3-month and 1-year mortality.
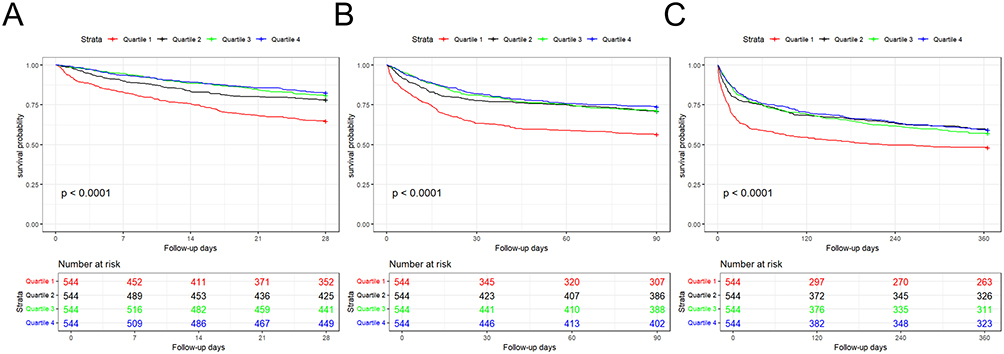 |
Figure 3 Kaplan–Meier curves for all-cause mortality stratified by the ROX index levels. (A) 28-day mortality. (B) 3-month mortality. (C) 1-year mortality. Quartile 1: ROX index≤7.79; Quartile 2: 7.79<ROX index≤9.72; Quartile 3: 9.72<ROX index≤12.26; Quartile 4: ROX index>12.26. |
As shown in Table 2, multivariable regression analysis of outcomes across the four patient groups revealed that, using Quartile 1 as the reference, Quartile 2 (HR=0.75, 95% CI 0.59–0.96, P=0.021), Quartile 3 (HR=0.60, 95% CI 0.46–0.77, P<0.001), and Quartile 4 (HR=0.58, 95% CI 0.45–0.75, P<0.001) all showed significantly lower 28-day mortality. Similar trends were observed for 3-month and 1-year mortality. Regarding in-ICU and in-hospital mortality, while the difference between Quartile 2 and Quartile 1 was not statistically significant (P>0.05), both Quartile 3 and Quartile 4 demonstrated significantly reduced all-cause mortality compared to Quartile 1. Pairwise comparisons among quartiles were further examined using multivariable Cox regression (Tables S4 and S5).
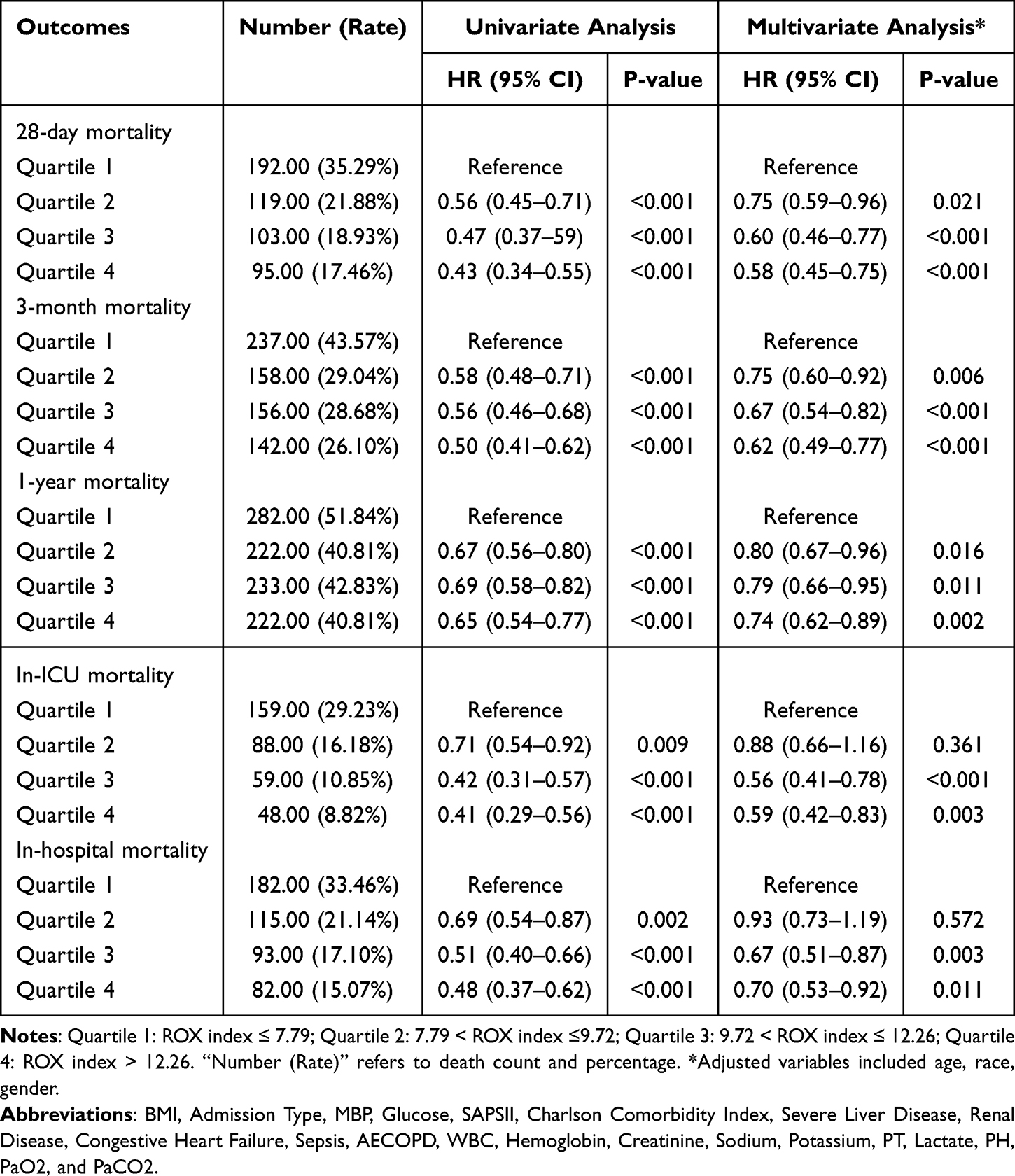 |
Table 2 Associations Between ROX Index Quartiles and All-Cause Mortality at Different Time Points |
As shown in Figure 4, subgroup analyses of COPD patients with ROX index below 9.72 demonstrated significant associations between ROX index and 28-day mortality across all subgroups: male (HR=0.81, 95% CI 0.74–0.89, P<0.001), female (HR=0.89, 95% CI 0.80–0.99, P=0.045), age ≤65 years (HR=0.74, 95% CI 0.63–0.88, P<0.001), age >65 years (HR=0.88, 95% CI 0.81–0.96, P<0.001), White race (HR=0.81, 95% CI 0.75–0.88, P<0.001), non-White race (HR=0.88, 95% CI 0.78–0.99, P=0.044), BMI ≤30 (HR=0.83, 95% CI 0.75–0.92, P<0.001), BMI >30 (HR=0.85, 95% CI 0.77–0.94, P=0.002), SAPS II score ≤35 (HR=0.74, 95% CI 0.58–0.93, P=0.011), SAPS II score >35 (HR=0.84, 95% CI 0.78–0.91, P<0.001), with sepsis (HR=0.84, 95% CI 0.77–0.91, P<0.001), without sepsis (HR=0.87, 95% CI 0.76–0.99, P=0.046), with AECOPD (HR=0.77, 95% CI 0.65–0.92, P=0.003), and without AECOPD (HR=0.85, 95% CI 0.79–0.92, P<0.001). Except for age, no significant interactions were detected between the ROX index and most other variables (all P for interaction > 0.05).
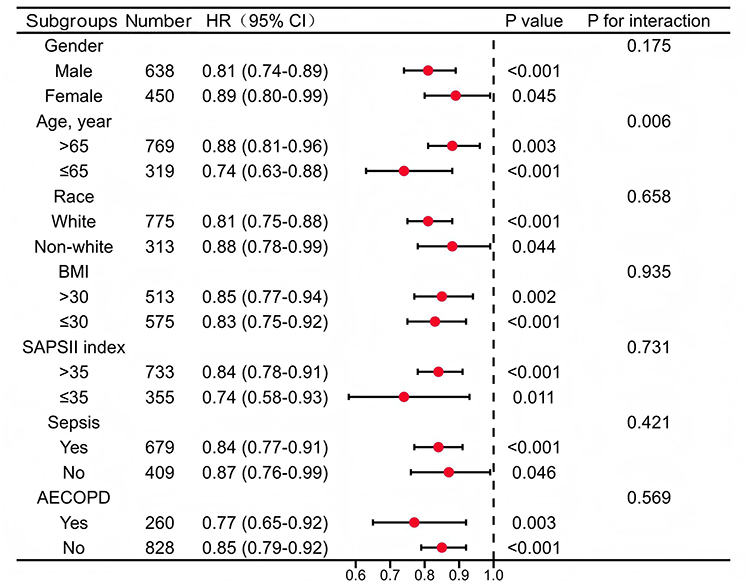 |
Figure 4 Forest plot showing subgroup analyses of the association between the ROX index and 28-day mortality in patients with a ROX index<9.72. |
Discussion
This study revealed a significant nonlinear association between the ROX index and mortality in COPD patients, demonstrating its utility as an effective tool for assessing mortality risk in this population.
This study revealed a significant L-shaped association between the ROX index and mortality in patients with COPD. This relationship may stem from the index’s formula, which integrates two core pathophysiological processes during acute exacerbations of COPD: impaired gas exchange (reflected by SpO2/FiO2) and increased respiratory load (reflected by respiratory rate).3,17 Specifically, when the ROX index falls below the critical threshold of 9.72, a decrease in its value suggests that the patient’s pulmonary function may be in a state of acute decompensation. This state is characterized by a vicious cycle of hypoxemia and tachypnea triggered by worsened ventilation/perfusion mismatch and dynamic pulmonary hyperinflation,18 indicating rapidly escalating respiratory muscle fatigue and a sharply elevated risk of mortality. Conversely, when the index exceeds this threshold, the respiratory system stabilizes, and mortality risk plateaus. At this stage, patient prognosis is likely influenced more by non-respiratory factors, such as underlying comorbidities and organ functional reserve.
This study is the first to validate a significant L-shaped nonlinear association between the ROX index and 28-day mortality in critically ill COPD patients, establishing a specific prognostic threshold of 9.72. This finding extends and refines our previous work in acute hypoxemic respiratory failure (AHRF) cohort, suggesting that the L-shaped association may represent a general prognostic pattern across diseases.19,20 The critical distinction, however, lies in the disease-specific threshold. While reported values are 8.28 for AHRF and approximately 10 for sepsis, the threshold for COPD is 9.72. This difference likely originates from the unique pathophysiology of COPD, including chronic airflow limitation, dynamic hyperinflation, and a tendency toward hypercapnia.
The ROX index is an established bedside tool for assessing HFNC outcomes in AHRF, with a value >6.88 also shown to predict treatment success in COPD-related respiratory failure.16 Additionally, the SpO2/FiO2 ratio has been demonstrated to exhibit a certain correlation with the PaO2/FiO2 ratio,21,22 and may serve as a valid substitute in specific clinical scenarios where arterial blood gas monitoring is unavailable.23 Compared to the PaO2/FiO2 ratio, our findings suggest a distinct role for the ROX index in COPD. Given the high median SpO2 in our cohort, the PaO2/FiO2 ratio may have limited sensitivity. The ROX index adds crucial value by incorporating respiratory rate, thereby capturing the increased respiratory drive typical of COPD exacerbations. It is thus more suitable for early risk stratification in this population, while PaO2/FiO2 remains key for managing severe hypoxemia.
The integration of respiratory rate gives the ROX index a particular advantage in COPD, where dynamic hyperinflation leads to increased work of breathing. This allows it to signal deterioration even before oxygenation significantly declines.3,17 It identifies patients at high risk of mortality, facilitating repeated bedside assessment. A key interpretation from our data is that in patients with preserved SpO2, the predictive power of the ROX index likely stems predominantly from the respiratory rate component. This highlights respiratory effort as a primary risk driver in such exacerbations. The index is most useful in critically ill COPD patients and has limited utility in stable outpatients or those on palliative care. Additionally, we observed differences in the association between the ROX index and mortality at different time points. One possible explanation is that ICU mortality and in-hospital mortality are more directly influenced by the severity of the patient’s acute illness and the therapeutic interventions administered during the ICU stay. In contrast, follow-up mortality rates are more closely correlated with the underlying severity and natural progression of COPD.
Overall, the ROX index offers the advantages of being non-invasive, straightforward, and suitable for continuous dynamic monitoring. It is applicable for early screening, routine monitoring, and treatment response evaluation in critically ill COPD patients. The index’s simplicity and reliance on routinely available parameters (SpO2, RR, and FiO2) give it potential utility in scenarios requiring frequent assessment, though this requires validation in such specific environments. Its primary limitation lies in the reduced sensitivity for detecting worsening oxygenation when SpO2 is near normal,24 although the incorporation of respiratory rate partially mitigates this shortcoming. In contrast, the oxygenation index, as an invasive gold-standard assessment, provides more precise oxygenation data but is limited in routine dynamic evaluation due to operational constraints and the inability for continuous monitoring. Therefore, these two indices hold complementary value in clinical practice: the ROX index is suitable for daily dynamic monitoring and risk stratification, whereas at critical junctures or when the ROX index contradicts the clinical picture, the oxygenation index should be obtained via arterial blood gas analysis for calibration.
This study has several limitations. First, as a single-center retrospective cohort study utilizing the MIMIC-IV database, the findings are derived from the patient population and clinical practices of a specific tertiary academic medical center, which may limit their generalizability to other healthcare settings. Second, although we adjusted for a range of potential confounders, residual confounding may still exist due to unmeasured or incompletely documented variables inherent to retrospective research, such as FEV1, smoking status, long-term oxygen therapy, and details of inhaled maintenance therapy, furthermore, excluding 2312 patients with missing ROX component data may have introduced selection bias. Third, the prognostic value of the ROX index observed in this critically ill ICU cohort may not be applicable to non-ICU COPD populations, including stable outpatients or patients managed in general wards. Fourth, due to challenges in reliably determining the primary reason for hospital or ICU admission from ICD codes in the MIMIC-IV database, we were unable to assess whether the optimal ROX index threshold varies according to different admission etiologies. Finally, regarding measurement, the ROX index was calculated using averaged values of its components over the first 24 hours of ICU admission to obtain a stable estimate. While this approach reduces the influence of transient fluctuations, it may obscure dynamic temporal changes that could carry additional prognostic significance. Moreover, the use of retrospectively extracted discrete measurements may not fully capture the continuous physiological status of patients.14
Conclusion
In conclusion, this study demonstrates that the ROX index is an independent and effective predictor of mortality risk in critically ill COPD patients. Notably, this association is nonlinear and threshold-dependent, with prognostic value most pronounced when the index falls below the identified cutoff of approximately 9.72. The significant association between lower ROX index values and increased mortality persisted after multivariable adjustment for available clinical covariates in this retrospective cohort. Our findings support extending the clinical application of the ROX index as a practical bedside tool, particularly for early risk stratification at ICU admission. As these conclusions are derived from ROX index values averaged over the initial 24 hours of ICU care, future studies are warranted to compare the predictive utility of alternative ROX metrics—such as the initial value, the worst value within 24 hours, or serial trends—to identify the most clinically actionable approach.
Abbreviations
COPD, Chronic obstructive pulmonary disease; SpO2, pulse oximetric saturation; FiO2, fraction of inspired oxygen; HFNC, high-flow nasal cannula; AHRF, acute hypoxemic respiratory failure; MIMIC-IV, Medical Information Mart for Intensive Care IV; ICU, intensive care unit; BIDMC, Beth Israel Deaconess Medical Center; SQL, Structured Query Language; HR, hazard ratio; OR, odds ratio; MD, median difference; CI, Confidence intervals; IQR, interquartile range confidence interval; BMI, Body Mass Index; SOFA, Sequential Organ Failure Assessment; SAPS II, Simplified acute physiological score II; APSIII, Acute Physiology and Chronic Health Evaluation III; AKI, acute kidney injury; MBP, mean blood pressure; BUN, blood urea nitrogen; INR, International normalized ratio; PT, prothrombin time; PTT, partial thromboplastin time. VIF, variance inflation factors; RRT, renal replacement therapy.
Data Sharing Statement
Data were retrospectively collected from the Medical Information Mart for Intensive Care-IV (MIMIC-IV) database (version 2.0; https://physionet.org/content/mimiciv/2.0/).
Ethics Approval and Consent to Participate
This study utilized data from the MIMIC-IV version 2.0 database. The use of this deidentified, publicly available database was granted a waiver of informed consent and approval by the Institutional Review Board of Beth Israel Deaconess Medical Center.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Foshan Self-Funded Scientific and Technological Innovation Projects (2420001003634), Scientific Research and Cultivation Fund of the Affiliated Shunde Hospital of Jinan University (202401009), and Medical Cultivation Specialty Project of the 14th Five-Year Plan in Foshan.
Disclosure
The authors declare no competing interests in this work.
References
1. Agustí A, Celli BR, Criner GJ, et al. Global initiative for chronic obstructive lung disease 2023 report: GOLD executive summary. Eur Respir J. 2023;61(4):2300239. doi:10.1183/13993003.00239-2023
2. Brightling C, Greening N. Airway inflammation in COPD: progress to precision medicine. Eur Respir J. 2019;54(2):1900651. doi:10.1183/13993003.00651-2019
3. Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. Lancet. 2022;399(10342):2227–12. doi:10.1016/S0140-6736(22)00470-6
4. Kahnert K, Jörres RA, Behr J, Welte T. The diagnosis and treatment of COPD and its comorbidities. Dtsch Arztebl Int. 2023;120(25):434–444. doi:10.3238/arztebl.m2023.027
5. Ko FW, Chan KP, Hui DS, et al. Acute exacerbation of COPD. Respirology. 2016;21(7):1152–1165. doi:10.1111/resp.12780
6. Celli BR, Cote CG, Marin JM, et al. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med. 2004;350(10):1005–1012. doi:10.1056/NEJMoa021322
7. Steer J, Gibson J, Bourke SC. The DECAF Score: predicting hospital mortality in exacerbations of chronic obstructive pulmonary disease. Thorax. 2012;67(11):970–976. doi:10.1136/thoraxjnl-2012-202103
8. Zhou X, Liu J, Pan J, Xu Z, Xu J. The ROX index as a predictor of high-flow nasal cannula outcome in pneumonia patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis. BMC Pulm Med. 2022;22(1):121. doi:10.1186/s12890-022-01914-2
9. Hu M, Zhou Q, Zheng R, et al. Application of high-flow nasal cannula in hypoxemic patients with COVID-19: a retrospective cohort study. BMC Pulm Med. 2020;20(1):324. doi:10.1186/s12890-020-01354-w
10. Roca O, Messika J, Caralt B, et al. Predicting success of high-flow nasal cannula in pneumonia patients with hypoxemic respiratory failure: the utility of the ROX index. J Crit Care. 2016;35:200–205. doi:10.1016/j.jcrc.2016.05.022
11. Tatkov S. Nasal High-Flow Therapy: role of F i O2 in the ROX Index. Am J Respir Crit Care Med. 2019;200(1):115–116. doi:10.1164/rccm.201902-0376LE
12. Blez D, Soulier A, Bonnet F, Gayat E, Garnier M. Monitoring of high-flow nasal cannula for SARS-CoV-2 severe pneumonia: less is more, better look at respiratory rate. Intensive Care Med. 2020;46(11):2094–2095. doi:10.1007/s00134-020-06199-9
13. Roca O, Caralt B, Messika J, et al. An index combining respiratory rate and oxygenation to predict outcome of nasal high-flow therapy. Am J Respir Crit Care Med. 2019;199(11):1368–1376. doi:10.1164/rccm.201803-0589OC
14. Vega ML, Dongilli R, Olaizola G, et al. COVID-19 Pneumonia and ROX index: time to set a new threshold for patients admitted outside the ICU. Pulmonology. 2022;28(1):13–17. doi:10.1016/j.pulmoe.2021.04.003
15. Biccard BM, Gopalan PD, Miller M. Patient care and clinical outcomes for patients with COVID-19 infection admitted to African high-care or intensive care units (ACCCOS): a multicentre, prospective, observational cohort study. Lancet. 2021;397(10288):1885–1894. doi:10.1016/S0140-6736(21)00441-4
16. Schaeffer BZ, Fazio SA, Stocking JC, et al. Using the ROX index to predict treatment outcome for high-flow nasal cannula and/or noninvasive ventilation in patients with COPD exacerbations. Respir Care. 2024;69(9):1100–1107. doi:10.4187/respcare.11544
17. Lareau SC, Fahy B, Meek P, Wang A. Chronic obstructive pulmonary disease (COPD). Am J Respir Crit Care Med. 2019;199(1):P1–p2. doi:10.1164/rccm.1991P1
18. Ritchie AI, Wedzicha JA. Definition, causes, pathogenesis, and consequences of chronic obstructive pulmonary disease exacerbations. Clin Chest Med. 2020;41(3):421–438. doi:10.1016/j.ccm.2020.06.007
19. Wu J, Zhao J, Ji X, Kang X, Li B, Zhu J. Association of the ROX index with mortality in sepsis patients: a retrospective study. Front Med. 2025;12:1709669. doi:10.3389/fmed.2025.1709669
20. Liu K, Ma X-Y, Xiao H, Gu W-J, Lyu J, Yin H-Y. Association between the ROX index and mortality in patients with acute hypoxemic respiratory failure: a retrospective cohort study. Respir Res. 2024;25(1):143. doi:10.1186/s12931-024-02771-9
21. Rice TW, Wheeler AP, Bernard GR, Hayden DL, Schoenfeld DA, Ware LB. Comparison of the Sp o 2 /F io 2 ratio and the Pa o 2 /F io 2 ratio in patients with acute lung injury or ARDS. Chest. 2007;132(2):410–417. doi:10.1378/chest.07-0617
22. Reddy M, Kulkarni M, Kanakalakshmi ST, Shenoy L, KrishnaBhat RR. Non-invasive SpO2/FiO2 ratio (SFR) as surrogate for PaO2/FiO2 ratio (PFR): a scoping review. J Critical Care Med. 2025;11(3):221–232. doi:10.2478/jccm-2025-0024
23. Batchinsky AI, Wendorff D, Jones J, et al. Noninvasive SpO2/FiO2 ratio as surrogate for PaO2/FiO2 ratio during simulated prolonged field care and ground and high-altitude evacuation. J Trauma Acute Care Surg. 2020;89(Suppl 2S):S126–s131. doi:10.1097/TA.0000000000002744
24. Tusman G, Bohm SH, Suarez-Sipmann F. Advanced uses of pulse oximetry for monitoring mechanically ventilated patients. Anesth Analg. 2017;124(1):62–71. doi:10.1213/ANE.0000000000001283
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.