")
Back to Journals » International Journal of General Medicine » Volume 16
Prognostic Value of PtfV1 in Long-Term Outcomes of Patients with Unstable Angina
Authors Lin H , Lin M, Lin T , Ye M
Received 4 October 2023
Accepted for publication 29 November 2023
Published 22 December 2023 Volume 2023:16 Pages 6065—6072
DOI https://doi.org/10.2147/IJGM.S439105
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Yuriy Sirenko
Huizhong Lin,1,* Maosen Lin,1,* Tao Lin,2 Mingfang Ye1
1Department of Cardiology, Fujian Medical University Union Hospital, Fuzhou City, People’s Republic of China; 2Department of Epidemiology and Health Statistics, Fujian Medical University, Fuzhou City, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Mingfang Ye, Email [email protected]
Background: P-wave terminal force in lead V1 (PtfV1) irregularity has been associated with various cardiovascular conditions, including atrial fibrillation, left ventricular diastolic dysfunction, valvular heart disease, congestive heart failure, stroke, and mortality. However, its prognostic value for unstable angina (UA) has not been extensively studied. To address this knowledge gap, this study aimed to evaluate the long-term predictive significance of PtfV1 at discharge for UA patients.
Methods: A total of 707 patients with newly diagnosed UA were included in this study. PtfV1 measurements were recorded at admission and discharge. PtfV1(+) was defined as an absolute value above 0.04mm·s, while PtfV1(-) was defined as an absolute value below 0.04mm·s. Based on their PtfV1 values at discharge, patients were categorized into two groups: PtfV1(-) and PtfV1(+). Univariate and multivariate regression analyses were conducted to identify variables that could potentially contribute to the risk of UA.
Results: Univariate analysis revealed a higher incidence of total adverse outcomes and major adverse cardiovascular events (MACE) in the PtfV1(+) group compared to the PtfV1(-) group, with a risk ratio (RR) of 2.006 [95% confidence interval (95% CI): 1.389– 2.896] for total outcomes and an RR of 2.759 (95% CI: 1.870– 4.070) for MACE. After adjusting for confounding factors through multivariate analysis, participants with PtfV1(+) had a 46% increased risk [adjusted hazard ratio (HR): 1.458; 95% CI: 1.010– 2.104]for total adverse outcomes and an 86% increased risk (adjusted HR: 1.863; 95% CI: 1.246– 2.786) for MACE compared to those with PtfV1(-).
Conclusion: The presence of PtfV1(+) at discharge is an independent predictor of poor outcomes and provides extended prognostic information for UA patients.
Keywords: P wave terminal force in lead V1, PtfV1, unstable angina, UA, prognosis, electrocardiography, major adverse cardiovascular events, MACE
Introduction
Acute coronary syndrome (ACS), a prevalent and critical form of coronary artery disease,1,2 is characterized by the primary rupture of atherosclerotic plaque and an entirely or partially obstructive thrombus, resulting in unstable angina (UA),3 ST-segment elevation myocardial infarction (STEMI), and non-STEMI (NSTEMI). Unstable angina is a clinical condition in which patients experience severe chest pain without prolonged ST segment deviation on the electrocardiogram, along with elevated cardiac markers. It is now understood that UA is caused by the rupture of atherosclerotic plaque with varying degrees of superficial thrombosis. Patients with UA present heterogeneous clinical manifestations and variable immediate- and long-term risk of death or non-fatal ischemic events.4 Despite advances in its management, the incidence and mortality rates of UA patients remain high.5 Therefore, early identification of diagnostic and prognostic parameters for UA is clinically challenging.
An electrocardiogram (ECG) is a noninvasive diagnostic tool providing valuable information on various cardiac pathologies, particularly myocardial ischemia. Morris et al initially proposed that the P-wave terminal force in lead V1 (PtfV1) is a measure of the amplitude (mm) and timing (s) of a terminal negative P wave when P waves are positive and negative in both directions.6 Various ECG characteristics, such as heart rate, T wave, P wave, ST segment, and QRS wave, have been shown to be indicators of cardiac conditions such as arrhythmia, cardiac hypertrophy, and myocardial infarction. The PtfV1 values, which indicate the extent of deflection of the terminal (negative) section of a biphasic P wave, were first identified in 1964. Studies have indicated that abnormal PtfV1 values are associated with various heart conditions, including left ventricular diastolic dysfunction, congestive heart failure, atrial fibrillation, valvular heart disease, and pericarditis, as well as stroke and death.7–13 Therefore, these values may provide insights into the severity of heart disease.
Despite the essential role of PtfV1 in diagnosing, treating, and predicting outcomes for heart failure, cardiomyopathy, myocardial ischemia, myocardial infarction, and ischemic stroke, there have been limited reports regarding its association with the prognosis of UA. Therefore, this study sought to examine the potential utility of PtfV1 at patient admission and discharge in predicting outcomes for individuals affected by UA.
Materials and Methods
Study Design and Population
Between August 2015 and June 2021, a study was conducted at Fujian Medical University Union Hospital, categorizing patients newly diagnosed with UA into two groups based on their PtfV1 values at discharge. The research project was approved by the Institutional Review Board of the hospital under approval number 2016KY025.
Adults aged 18 to 80 years who were diagnosed with UA following the 2015 American College of Cardiology/American Heart Association guidelines for managing patients with non-ST-segment elevation acute coronary syndrome (NSTE-ACS)14 were eligible for participation.
Exclusion criteria included a history of arrhythmia (atrial fibrillation, atrial tachycardia, ventricular fibrillation, atrial flutter, ventricular flutter, ventricular tachycardia, or borderline ventricular tachycardia), severe underlying illnesses such as heart valve disease, congenital heart disease, or cardiomyopathy, and inability to attend follow-up appointments.
Clinical information, including gender, age, smoking status, medical history, blood pressure, heart rate, radiographic findings, biochemical markers, echocardiograms, and medication treatments, was recorded.
ECG
All patients had their ECG recorded at discharge. PtfV1 values were measured using the electrocardiogram machine (NIHON KOHDEN 1250P) with 12-lead ECG (speed: 25 mm/s, amplitude: 10 mm/mV). PtfV1(-) was defined as an absolute value <0.04 mm·s, and PtfV1(+) was defined as an absolute value ≥0.04mm·s based on previous research.15 Patients with Unstable Angina (UA) were separated into groups based on their PtfV1 values at discharge: those with negative PtfV1 and those with positive PtfV1.
Follow-Up
Patients included in the study were monitored and tracked through regular clinical check-ups and phone calls for a duration ranging from 1 to 91 months, with a mean follow-up duration of 53.1 months. The follow-up process involved collecting information from healthcare professionals, patients themselves, and their family members. The collected information was consistent with the hospital records. The main focus of the follow-up was to assess various endpoints, including major adverse cardiovascular events (such as cardiac death, hospitalization due to heart failure, dangerous heart rhythm abnormalities, nonfatal heart attacks, and repeat angioplasty), stroke resulting from reduced blood flow to the brain, and death from other causes. Follow-up assessments were conducted at six months, one year, two years, and five years after the patients were discharged.
Statistical Analysis
The collected data were analyzed using SPSS 26.0 software. Continuous variables were reported as the mean ± standard deviation (SD) or [median (25th percentile, 75th percentile)] and were compared using the Kruskal–Wallis H-test. Categorical variables were presented as frequencies and percentages and were analyzed using either the chi-square or Kruskal–Wallis H-test. Group comparisons were performed using a one-way analysis of variance (ANOVA) with the least significant difference post hoc test. Multivariable Cox regression analysis was employed to identify the variables associated with an increased risk of unstable angina (UA) as determined by the univariate regression analysis. A p-value less than 0.05 was statistically significant.
Results
Characteristics of Patients with UA
After excluding patients with complications, arrhythmias, and incomplete or missing data, a total of 707 patients with newly diagnosed UA were included in the study and categorized into two groups based on their PtfV1 values at discharge (Figure 1). The PtfV1 (-) group consisted of 522 patients with an average age of 67.10 ± 9.6 years, while the PtfV1 (+) group included 185 patients with an average age of 68.57 ± 10.13 years. Table 1 provides an overview of the main characteristics of the patients. Significant differences were observed between the two groups in terms of ejection fraction, left atrium size, serum creatinine levels, and the use of diuretics.
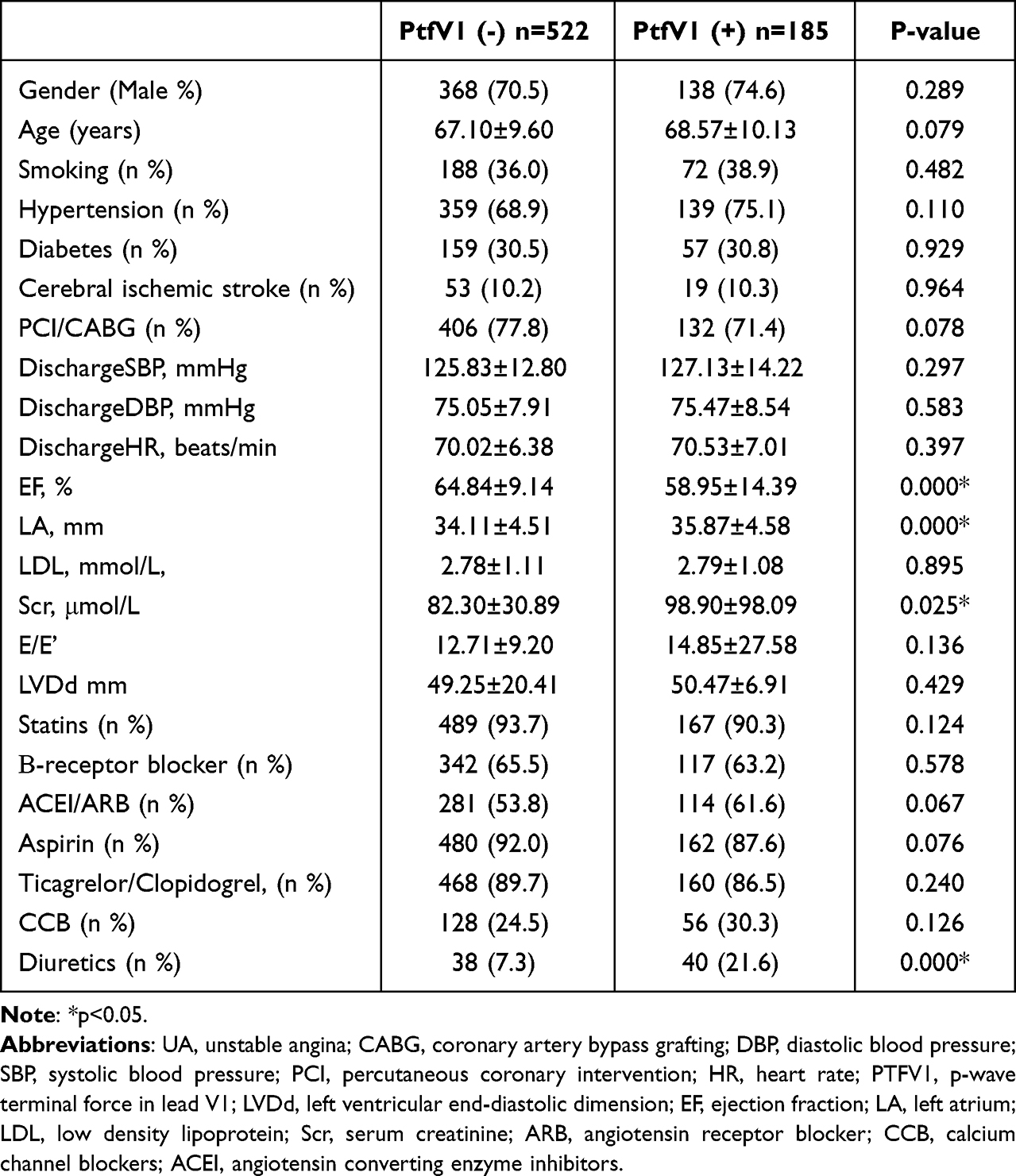 |
Table 1 The Baseline Characteristics of UA Patients in the Two Groups |
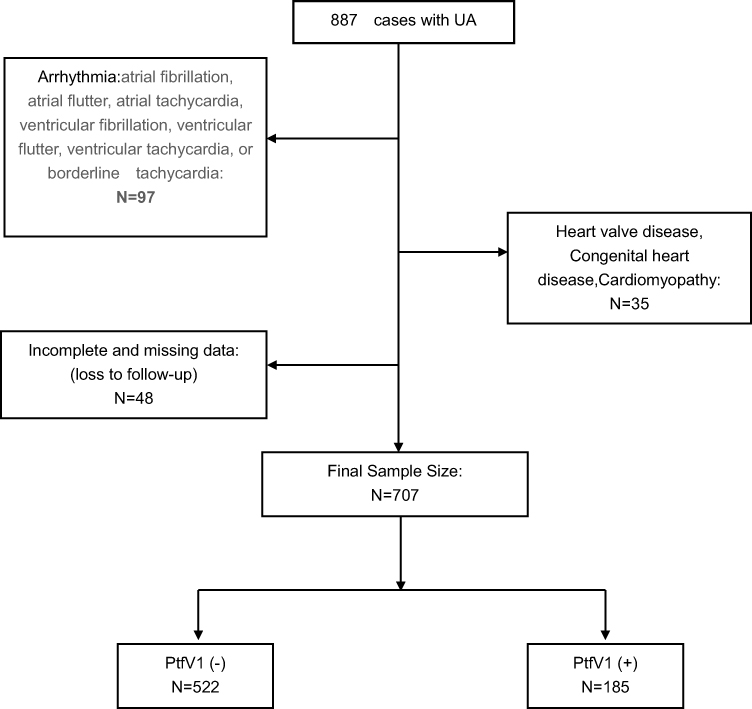 |
Figure 1 Inclusion and exclusion of the study participant. Abbreviations: UA, unstable angina pectoris; PTFV1, p-wave terminal force in lead V1. |
Univariate and Multivariate Regression Analyses for the Overall Poor Survival Outcomes and Major Adverse Cardiac Events (MACEs)
In the univariate analysis, there was a significantly higher incidence of overall poor survival outcomes in the PtfV1 (+) group (RR: 2.006; 95% CI: 1.389–2.896; P<0.05) compared to the PtfV1 (-) group, with respect to overall adverse UA findings. Similarly, there was a significant increase in the incidence of MACEs in the PtfV1 (+) group (RR: 2.759; 95% CI: 1.870–4.070; P<0.05) compared to the PtfV1 (-) group, as indicated by the univariate analysis. As shown in Table 2, there was no significant difference in the incidence rate of cerebral ischemic stroke between the two groups.
 |
Table 2 Univariate Analysis of Adverse Outcomes in UA Patients |
To further examine the findings and account for potential confounding factors, a multivariate Cox regression analysis was performed. After adjusting for age, sex, SBP/DBP/HR at discharge, smoking, hypertension, diabetes, history of PCI/CABG, LDL, ejection fraction, left atrium size, serum creatinine levels, drugs for ACEI/ARB, statins, β-receptor blockers, aspirin, ticagrelor/clopidogrel, CCB, and diuretics, patients in the PtfV1 (+) group had a higher incidence rate of MACEs (HR: 1.863, 95% CI: 1.246–2.786) and overall poor survival outcomes (HR: 1.458, 95% CI: 1.010–2.104) compared to patients in the PtfV1 (-) group. Figure 2 demonstrates that there was no significant difference in the incidence rate of cerebral ischemic stroke between the PtfV1 (-) group and the PtfV1 (+) group. Kaplan-Meier survival curves for MACEs and overall adverse outcomes are illustrated in Figure 3.
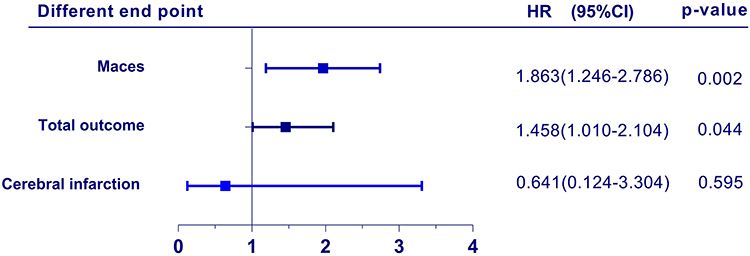 |
Figure 2 Cox regression for the association betweenPtfV1 and different endpoint. Abbreviations: HR, hazard ratio; MACEs, major adverse cardiovascular events. |
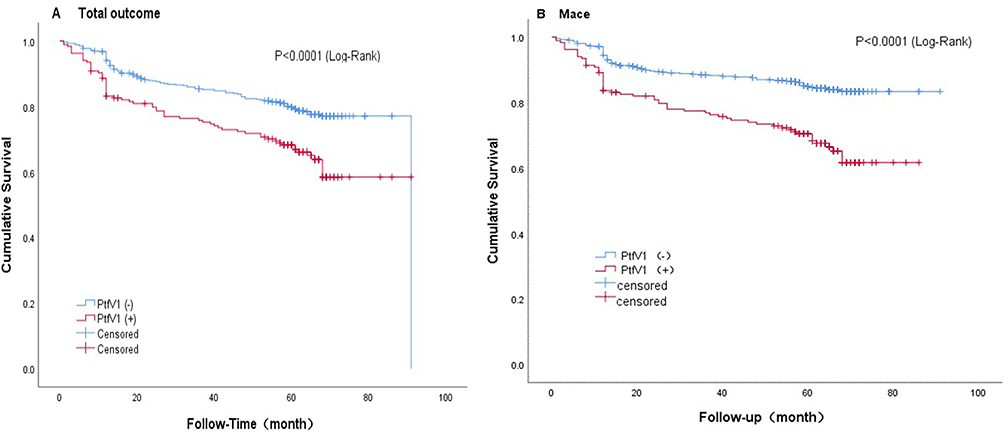 |
Figure 3 Kaplan–Meier survival curves by Total outcome (A) and Mace (B). Abbreviations: MACEs, major adverse cardiovascular events; PTFV1, p-wave terminal force in lead V1. |
Discussion
Herein, we investigated the relationship between PtfV1 values at discharge and long-term adverse outcomes in patients experiencing symptoms of UA. Our findings demonstrated that PtfV1(+) at discharge was an independent risk factor for MACEs in UA patients. Therefore, we advocate that PtfV1 could serve as a widely accessible clinical marker for identifying an increased long-term risk of MACEs in UA patients.
During hospitalization, the PtfV1 values of patients who initially tested positive upon admission may undergo dynamic changes, potentially influenced by clinical treatments such as medication and vascular reconstruction. In some cases, the PtfV1 value becomes negative upon discharge, indicating that this change may be associated with vascular reconstruction or medication that alters atrial volume and pressure load, suggesting an improvement in the patient’s condition.
Earlier studies have indicated a strong correlation between the deep terminal negativity of PtfV1 in electrocardiographic reports and the risk of mortality from cardiovascular disease,10 consistent with the findings of our study.
Abnormal PtfV1 values can typically be explained by two mechanisms. Firstly, the left atrium experiences depolarization and an augmented depolarized vector when there is an increase in left atrial load due to fibrosis, hypertrophy, or ischemia. Additionally, an increased P wave deflection amplitude and prolonged duration at the negative terminal may result from elevated right atrial load, hypertrophy, or prolonged conduction of the interatrial bundle. As such, numerous studies have proposed that PtfV1 signifies an increase in volume or pressure in the left atrium, decreased inter-atrial conduction, and fibrosis of the left ventricle.6,8,16,17 These indications may predict the potential risk of MACEs.15,18
Research indicates that an abnormal PtfV1 value may be linked to left ventricular diastolic dysfunction resulting from infarcted myocardium, even prior to the onset of heart failure symptoms and left ventricular systolic dysfunction.19 This diastolic dysfunction in the left ventricle within a UA context may lead to elevated LV filling pressure and subsequently increased LA pressure,16,20 resulting in an escalation in LA wall tension. When there is an overload in the left atrium, the P wave vector shifts left and backward on the horizontal plane, leading to a significant negative component in the P wave within V1. This suggests that PtfV1, associated with left ventricular diastolic pressure, may serve as an indicator of the severity of unstable angina to a certain extent and is linked to the risk of major adverse cardiac events in UA patients. Previous studies21,22 have shown that risk models utilizing ECG parameters alone have demonstrated good predictive power for diastolic dysfunction and stroke. Our study confirmed the long-term prognostic value of PtfV1 in patients with UA, suggesting that incorporating PtfV1 into a risk model could enable risk stratification for long-term survival in UA patients and allow for early intervention. The use of artificial intelligence in medicine can provide physicians with a comprehensive understanding of PtfV1, particularly in chronic conditions like coronary artery disease and atrial fibrillation.23
On the other hand, Lebek et al24,25 demonstrated a link between abnormal PtfV1 and increased atrial pro-arrhythmic activity and dysfunction in atrial contractility, which is influenced by the activation of CaMKII. CaMKII plays a crucial role in regulating the coupling of cardiac excitation and contraction and is known to induce electrical remodeling in the atrium, potentially leading to arrhythmias and an elevated risk of major adverse cardiac events.24 Furthermore, current evidence suggests that higher levels of reactive oxygen species can trigger the activation of CaMKII.26 Several studies have shown that an increased production of ROS during the development of unstable angina27–29 could activate atrial CaMKII and result in CaMKII-dependent electrical remodeling, leading to the manifestation of abnormal PtfV1. Therefore, abnormal PtfV1 could potentially be used to identify patients who may benefit from specific pharmacological treatments, such as inhibiting CaMKII.
In summary, our investigation revealed that an elevated PtfV1 value at discharge is associated with a higher incidence of major adverse cardiac events in patients with unstable angina. We identified PtfV1 positivity at discharge as an independent risk factor for MACEs and overall outcomes, providing valuable prognostic information for UA patients.
Limitations
Several limitations found in this study should be acknowledged. Firstly, being a single-center study, the sample size was limited. Nonetheless, it should be borne in mind that the clinical characteristics of study subjects at baseline were similar across the groups, which enhanced the robustness of our findings. Secondly, the study population consisted of a specific subset of acute coronary syndrome patients, which may limit the generalizability of the conclusions. Furthermore, due to the relatively short duration of our follow-up, further large-scale clinical studies are warranted to validate our findings.
Data Sharing Statement
The datasets used in this study are not publicly available due to ethical restrictions on data sharing. However, interested researchers can request access to the datasets from the corresponding author.
Ethics Approval and Consent to Participate
This research was approved by the Institutional Review Board (IRB) of Fujian Medical University Union Hospital (Approval number: 2016KY025). Written informed consent to participate in the study was obtained before the study began. The ethics committee approved this consent process. This research was observed the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Acknowledgment
The authors express their gratitude to the editors-in-chief, the handling Editor, and the anonymous reviewers for their invaluable and constructive feedback. Additionally, the authors extend their appreciation to the follow-up team for their significant contribution to this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Fujian Provincial Health Technology project under grant number 2021TG008 and the JointFunds for the Innovation of Science and Technology, Fujian province (No.2020Y9069, No.2019Y9093).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Puymirat E, Simon T, Cayla G, et al. Acute myocardial infarction: changes in patient characteristics, management, and 6-month outcomes over a period of 20 years in the FAST-MI program (French registry of acute ST-elevation or non-ST-elevation myocardial infarction) 1995 to 2015. Circulation. 2017;136(20):1908–1919. doi:10.1161/CIRCULATIONAHA.117.030798
2. Rodriguez F, Mahaffey KW. Management of patients with NSTE-ACS: a comparison of the recent AHA/ACC and ESC guidelines. J Am Coll Cardiol. 2016;68(3):313–321. doi:10.1016/j.jacc.2016.03.599
3. Hedayati T, Yadav N, Khanagavi J. Non-ST-segment acute coronary syndromes. Cardiol Clin. 2018;36(1):37–52. doi:10.1016/j.ccl.2017.08.003
4. Widera C, Pencina MJ, Meisner A, et al. Adjustment of the GRACE score by growth differentiation factor 15 enables a more accurate appreciation of risk in non-ST-elevation acute coronary syndrome. Eur Heart J. 2012;33(9):1095–1104. doi:10.1093/eurheartj/ehr444
5. Collet JP, Thiele H, Barbato E, et al. 2020 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021;42(14):1289–1367. doi:10.1093/eurheartj/ehaa575
6. Morris JJ, Estes EH, Whalen RE, Thompson HK, Mcintosh HD. P-wave analysis in valvular heart disease. Circulation. 1964;29(2):242–252. doi:10.1161/01.CIR.29.2.242
7. Jin L, Weisse AB, Hernandez F, et al. Significance of electrocardiographic isolated abnormal terminal P-wave force (left atrial abnormality). An echocardiographic and clinical correlation. Arch Intern Med. 1988;148(7):1545–1549. doi:10.1001/archinte.1988.00380070053014
8. Li W. Evaluation of left ventricular diastolic function of patients with coronary heart disease by ultrasound images on bilateral filtering image noise reduction algorithm combined with electrocardiogram. Pak J Med Sci. 2021;37(6):1699–1704. doi:10.12669/pjms.37.6-WIT.4886
9. Ren Y, Qiu J, Li Z, et al. P-wave terminal force in lead V1 is a predictive indicator for the diagnosis of tuberculous constrictive pericarditis. Heart Lung. 2019;48(2):155–158.
10. Tereshchenko LG, Henrikson CA, Sotoodehnia N, et al. Electrocardiographic deep terminal negativity of the P wave in V(1) and risk of sudden cardiac death: the Atherosclerosis Risk in Communities (ARIC) study. J Am Heart Assoc. 2014;3(6):e001387. doi:10.1161/JAHA.114.001387
11. Huang Z, Zheng Z, Wu B, et al. Predictive value of P wave terminal force in lead V1 for atrial fibrillation: a meta-analysis. Ann Noninvas Electrocardiol. 2020;25(4):e12739. doi:10.1111/anec.12739
12. Kohsaka S, Sciacca RR, Sugioka K, et al. Electrocardiographic left atrial abnormalities and risk of ischemic stroke. Stroke. 2005;36(11):2481–2483. doi:10.1161/01.STR.0000185682.09981.26
13. Sumita Y, Nakatani S, Murakami I, et al. Significance of left atrial overload by electrocardiogram in the assessment of left ventricular diastolic dysfunction. J Echocardiogr. 2020;18(2):105–112. doi:10.1007/s12574-019-00458-5
14. Roffi M, Patrono C, Collet JP, et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: task force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2016;37(3):267–315. doi:10.1093/eurheartj/ehv320
15. Eranti A, Aro AL, Kerola T, et al. Prevalence and prognostic significance of abnormal P terminal force in lead V 1 of the ECG in the general population. Circ Arrhythm Electrophysiol. 2014;7(6):1116–1121. doi:10.1161/CIRCEP.114.001557
16. Tiffany Win T, Ambale Venkatesh B, Volpe GJ, et al. Associations of electrocardiographic P-wave characteristics with left atrial function, and diffuse left ventricular fibrosis defined by cardiac magnetic resonance: the PRIMERI Study. Heart Rhythm. 2015;12(1):155–162. doi:10.1016/j.hrthm.2014.09.044
17. Josephson ME, Kastor JA, Morganroth J. Electrocardiographic left atrial enlargement. Electrophysiologic, echocardiographic and hemodynamic correlates. Am J Cardiol. 1977;39(7):967–971. doi:10.1016/S0002-9149(77)80209-9
18. Li G, Li Q, Huang B, et al. Variations of electrocardiographic parameters during hospitalization predict long-term outcomes in patients with non-ST-segment elevation myocardial infarction. Ann Noninvas Electrocardiol. 2019;24(2):e12613. doi:10.1111/anec.12613
19. Liu G, Tamura A, Torigoe K, et al. Abnormal P-wave terminal force in lead V1 is associated with cardiac death or hospitalization for heart failure in prior myocardial infarction. Heart Vessels. 2013;28(6):690–695. doi:10.1007/s00380-012-0307-9
20. Okin PM, Kamel H, Kjeldsen SE, et al. Electrocardiographic left atrial abnormalities and risk of incident stroke in hypertensive patients with electrocardiographic left ventricular hypertrophy. J Hypertens. 2016;34(9):1831–1837. doi:10.1097/HJH.0000000000000989
21. Hayıroğlu Mİ, Çınar T, Selçuk M, et al. The significance of the morphology-voltage-P-wave duration (MVP) ECG score for prediction of in-hospital and long-term atrial fibrillation in ischemic stroke. J Electrocardiol. 2021;69:44–50. doi:10.1016/j.jelectrocard.2021.09.006
22. Hayıroğlu Mİ, Çınar T, Çiçek V, et al. A simple formula to predict echocardiographic diastolic dysfunction—electrocardiographic diastolic index. Herz. 2021;46(S2):159–165.
23. Hayıroğlu Mİ, Altay S. The role of artificial intelligence in coronary artery disease and atrial fibrillation. Balkan Med J. 2023;40(3):151–152. doi:10.4274/balkanmedj.galenos.2023.06042023
24. Lebek S, Pichler K, Reuthner K, et al. Enhanced CaMKII-dependent late INa induces atrial proarrhythmic activity in patients with sleep-disordered breathing. Circ Res. 2020;126(5):603–615. doi:10.1161/CIRCRESAHA.119.315755
25. Lebek S, Wester M, Pec J, et al. Abnormal P-wave terminal force in lead V1 is a marker for atrial electrical dysfunction but not structural remodelling. ESC Heart Fail. 2021;8(5):4055–4066. doi:10.1002/ehf2.13488
26. Erickson JR, Joiner M-LA, Guan X, et al. A dynamic pathway for calcium-independent activation of CaMKII by methionine oxidation. Cell. 2008;133(3):462–474. doi:10.1016/j.cell.2008.02.048
27. El-Mahdy RI, Mostafa MM, EL-Deen HS, et al. Serum zinc measurement, total antioxidant capacity, and lipid peroxide among acute coronary syndrome patients with and without ST elevation. Appl Biochem Biotechnol. 2019;188(1):208–224. doi:10.1007/s12010-018-2917-x
28. Mohammadi A, Balizadeh Karami AR, Dehghan Mashtani V, et al. Evaluation of oxidative stress, apoptosis, and expression of MicroRNA-208a and MicroRNA-1 in cardiovascular patients. Rep Biochem Mol Biol. 2021;10(2):183–196. doi:10.52547/rbmb.10.2.183
29. Serdar Z, Serdar A, Altin A, et al. The relation between oxidant and antioxidant parameters and severity of acute coronary syndromes. Acta Cardiol. 2007;62(4):373–380. doi:10.2143/AC.62.4.2022281
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.