")
Back to Journals » Cancer Management and Research » Volume 11
Prognostic value of pretreatment neutrophil count in metastatic renal cell carcinoma: a systematic review and meta-analysis
Authors Shen J, Chen Z, Fan M, Lu H, Zhuang Q, He X
Received 29 December 2018
Accepted for publication 9 April 2019
Published 10 June 2019 Volume 2019:11 Pages 5365—5374
DOI https://doi.org/10.2147/CMAR.S199849
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Antonella D'Anneo
Jie Shen,* Zhen Chen,* Min Fan, Hao Lu, Qianfeng Zhuang, Xiaozhou He
Department of Urology, The Third Affiliated Hospital of Soochow University, Changzhou 213003, People’s Republic of China
*These authors contributed equally to this work
Background: In recent years, inflammation has become widely recognized as a crucial component in tumor development and progression. Neutrophils are one of the most common inflammatory markers during hematological examinations. The prognostic value of neutrophils in metastatic renal cell carcinoma (mRCC) remains inconsistent. The aim of this meta-analysis is to evaluate the prognostic value of pretreatment neutrophil count in patients with mRCC.
Methods: PubMed, Web of Science and Embase were searched for data on the association between pretreatment neutrophil count and mRCC prognosis up to October 7, 2017. We sorted out relevant studies and extracted the hazard ratio (HR) and its 95% confidence interval (CI) for overall survival (OS) and progression-free survival (PFS).
Results: A total of 13 studies containing 3,021 patients with mRCC were summarized in the present meta-analysis. An elevated pretreatment neutrophil count yielded a worse OS (HR=2.17, 95% CI=1.68–2.79, P<0.001) and PFS (HR=1.78, 95% CI=0.91–3.49, P<0.001). Furthermore, we performed a subgroup analysis based on cut-off value, ethnicity, treatment method and analysis type. As a result, the association between pretreatment neutrophil count and survival was statistically significant in the subgroups of cut-off value, ethnicity, treatment method and analysis type.
Conclusion: Our results show that the pretreatment neutrophil count is associated with mRCC outcomes and can be used as a valuable inflammatory marker for prognosis monitoring.
Keywords: neutrophils, clear-cell metastatic renal cell carcinoma, prognosis, meta-analysis
Introduction
Renal cell carcinoma (RCC) is a common cancer worldwide. Due to gender differences, it accounts for 5% of the adult tumors in men and 3% of the adult tumors in women.1 Although the widespread use of non-invasive radiological techniques and new therapeutic strategies allows the diagnosis and treatment of RCC at an early stage,2 nearly half of RCC patients still develop metastatic renal cell carcinoma (mRCC).3,4 Once metastasis occurs, the 5-year survival rate is not satisfactory.1 A 5-parameter prognostic score developed at the Memorial Sloan-Kettering Cancer Center (MSKCC)5 is commonly used to estimate the prognosis in patients with mRCC. However, after taking into account the different circumstances of each patient, the 5-parameter panel developed at MSKCC may not be suitable for all mRCC patients. Hence, it is important to find a new biomarker that can assess the prognosis of mRCC quickly and specifically.
Nowadays, more and more studies have shown that inflammation plays a significant role in tumor development and progression.6–8 The increase in the level of pro-inflammatory cytokines in cancer patients may indicate the innate immune response of the host to the tumor and disease activity.9,10 During the inflammatory reaction, neutrophils are stimulated and activated by inflammatory cytokines such as IL-8 and TNF-α to promote their phagocytotic and bactericidal effects.11 Several researches have clarified that neutrophil is a prognostic factor of mRCC.12–14 Neutrophils could represent a useful and cheap biomarker to assess the prognostic value of mRCC patients. However, the precision and magnitude of the prognostic impact of pretreatment neutrophil count in mRCC patients remain inconsistent due to different study-specific factors. Thus, we pooled all related studies in this systematic literature review and meta-analysis to unveil prognostic value of pretreatment neutrophil count in mRCC patients.
Materials and methods
Search strategy
Databases including PubMed, Web of Science and Embase were searched completely up to October 7, 2017. The keywords used on the literature retrieval were “neutrophil”, “kidney cancer or renal cancer or renal carcinoma or renal cell carcinoma” and “prognosis or prognostic or survival or outcome”. Two authors (Jie Shen and Zhen Chen) researched the databases independently and unified disagreement through discussion to ensure the validity of the retrieved reference lists.
Selection criteria
All studies included were in accordance with the following criteria: (1) all patients only suffered from mRCC and were confirmed by pathology or imageology; (2) the amount of pretreatment neutrophil and the correlation between pretreatment neutrophils, mRCC patients’ clinical features and prognosis was described; (3) hazard ratio (HR) and its 95% confidence interval (CI) of overall survival (OS) or disease-free survival (DFS) could be found directly or extrapolated from articles. Studies were excluded if they: (1) had localized RCC patients without metastasis; (2) were letters, reviews, case reports, comments and conference abstracts; (3) had studies with duplicate data and (4) had the missing data that precluded further analysis.
Data extraction
In order to ensure the validity, two authors extracted data from the articles independently. The primary information included was author, country, ethnicity, age of patients, patient numbers, follow-up time, cut-off value, HR and relative 95% CI and treatment method. In case of survival data only presented in Kaplan–Meier curves, software designed by Jayne F Tierney and Matthew R Syde15 was chosen to digitize and calculate the HR values and 95% CIs. What’s more, disputed data were resolved by discussion.
Statistical analysis
We divided pretreatment neutrophil counts into two levels (high and low) depending on the cut-off values mentioned in studies. We integrated the pooled HRs and 95% CIs to estimate the effect of pretreatment neutrophil count on the survival of mRCC. We used the Chi-square test and the I2 statistic to test the heterogeneity of combined HRs. If the P-value was less than 0.05 or the I2 was greater than 50%, meaning the existence of heterogeneity, a random-effects model was then used. Otherwise, a fixed-effects model was select. We conducted further analysis to explore the potential cause for the existence of heterogeneity. Begg’s and Egger’s tests were used to find out publication bias. Statistical analyses were performed with STATA 12.0 (Stata Corporation, College Station, TX, USA). A two-tailed P-value less than 0.05 was defined as statistically significant difference.
Results
Search results
Figure 1 displays the articles searching process. Initially, we identified 311 articles were potentially eligible. After examining the titles, abstracts and full text of each article carefully, 287 articles were excluded, and the remaining 24 articles were shortlisted. Among the adopted articles, 11 articles were excluded (3 lacked important data, 1 used continuous or two cut-offs, 4 only reported localized RCC patients, 2 reported both localized and metastatic RCC patients and 1 reported only the relative risk or odds ratios). Finally, a total of 13 articles comprised 3021 mRCC patients were included in our meta-analysis.16–28
 | Figure 1 Flow diagram of the study selection process. |
Study characteristics and quality assessment
Characteristics of the included studies are presented in Table 1. Thirteen studies, which contained 3,021 patients totally, were published from 2002 to 2016. These patients came from eight different countries: Czech Republic, Canada, Germany, Turkey, Denmark, Italy, Korea and Japan. Asian nationals accounted for 11.4% (343 patients), whereas Caucasian patients accounted for the remaining 88.6% (2678 patients). A total of 2,271 patients in 9 articles received multiple therapies, while another 750 patients in the rest 3 articles received targeted therapy or kidney transplantation. Prognostic role of neutrophils in OS was found in 12 articles. Besides, PFS was evaluated in 5 articles. Newcastle–Ottawa Scale (NOS)29 was taken to assess the quality of the included studies. The quality of the studies varied from scores of 5 to 9, with a mean of 6. A higher score was considered to be of better quality.
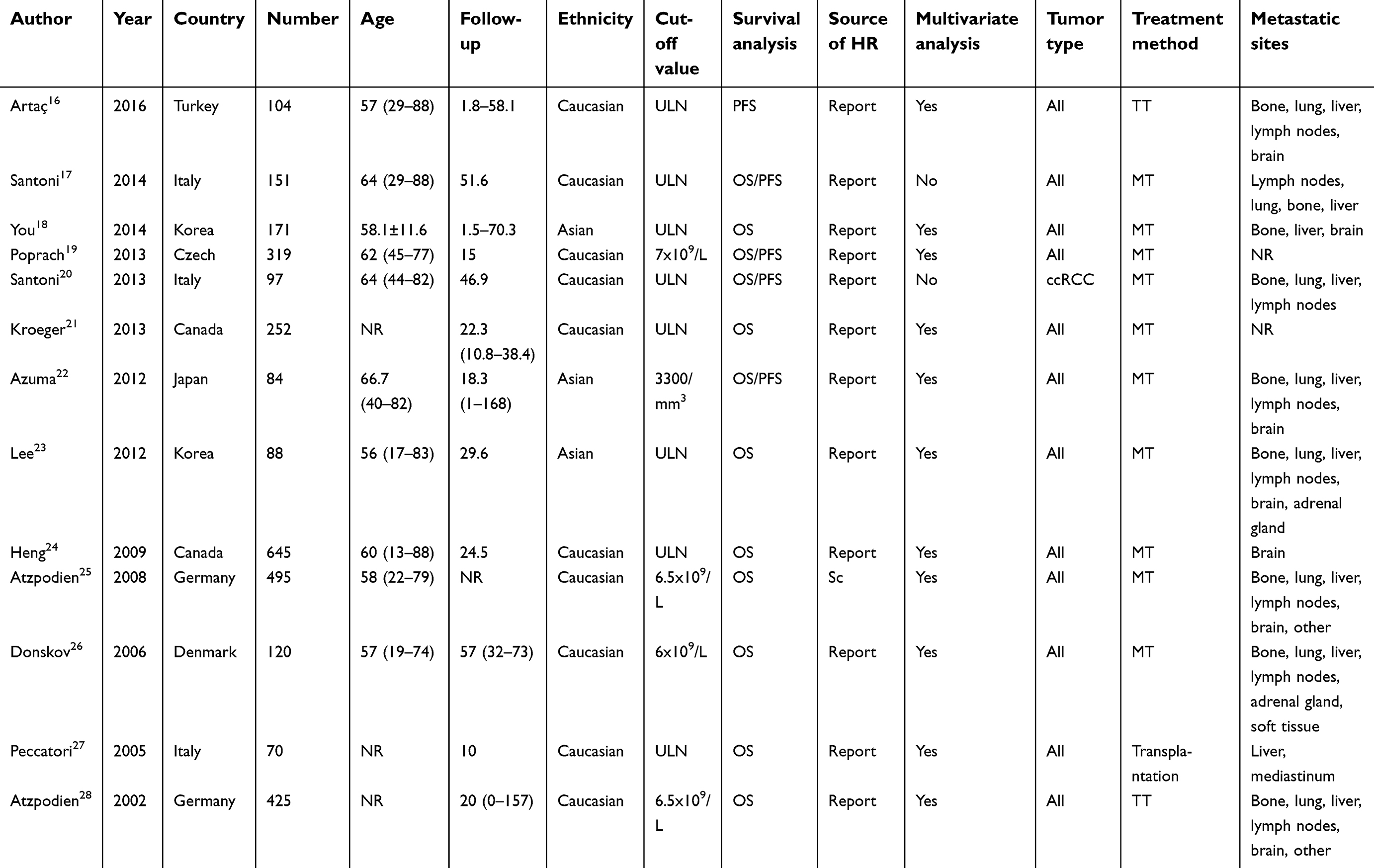 | Table 1 Main characteristics of all studies included in the meta-analysis |
Relationship between pretreatment neutrophil and OS in mRCC patients
Thirteen studies including 3,021 mRCC patients researched the role of elevated pretreatment neutrophil count as a predictor of OS (Figure 2A). A random model was used due to statistical heterogeneity (I2=78.9%, P<0.001) and the pooled data demonstrated that a high pretreatment neutrophil count predicted a worse OS (HR=2.17, 95% CI=1.68–2.79, P<0.001).
 | Figure 2 (A) Forest plots of studies evaluating hazard ratios of pretreatment neutrophil count in metastatic renal cell carcinoma (mRCC) for overall survival. (B) Forest plot of the relationship between pretreatment neutrophil count and overall survival in patients with different ethnicity. |
Relationship between pretreatment neutrophil and PFS in mRCC patients
Figure 3 showed the pooled data for PFS analysis in five studies (755 mRCC patients). The result demonstrated that a high pretreatment neutrophil count predicts a worse PFS (HR=1.78, 95% CI=0.91–3.49, P<0.001) and a random model was adopted in this analysis of PFS because of the statistical heterogeneity (I2=85.8%, P<0.001).
 | Figure 3 Forest plots of studies evaluating hazard ratios of pretreatment neutrophil count in metastatic renal cell carcinoma (mRCC) for progression-free survival. |
Subgroup analysis
We performed a subgroup analysis for further exploring the heterogeneity. The results in Table 2 and Figure 2B showed that high pretreatment neutrophil count was linked to a worse OS for Asian mRCC patients (HR=4.04, 95% CI=2.48–6.57, P<0.001) and Caucasian mRCC patients (HR=1.9, 95% CI=1.49–2.43, P<0.001). Neutrophil pretreatment also showed a significant relation to a poor OS in the remaining subgroups: multivariate analysis (HR=2.13, 95% CI=1.62–2.8, P<0.001), univariate analysis (HR=2.4, 95% CI=1.41–4.1, P<0.001), multiple therapy (HR=2.3, 95% CI=1.84–2.87, P<0.001), target therapy or transplantation (HR=1.67, 95% CI=1.04–2.7, P<0.001), upper limits of normal (ULN) (HR=2.5, 95% CI=1.57–3.98, P<0.001) and others (HR=1.82, 95%CI=1.56–2.14, P<0.001).
 | Table 2 Pooled hazard ratios for OS according to subgroup analyses |
Sensitivity analysis
Each selected study was sequentially removed to evaluate whether it could influence the pooled HRs. As shown in Figure 4, the results of the sensitivity analysis showed high robustness in our findings.
 | Figure 4 Sensitivity analysis on the relationships between pretreatment neutrophil count and overall survival in metastatic renal cell carcinoma (mRCC) patients. |
Publication bias
We evaluated the publication bias of OS and PFS using funnel plots, Egger’s and Begg’s tests. Funnel plots of OS and PFS are shown in Figure 5A and B. No publication bias was observed for OS (P<0.001 using Egger’s test). For PFS, asymmetrically distributed plots indicated there was possible publication bias. However, considering that the number of included studies was only five, the funnel plots may not be noteworthy.
 | Figure 5 Funnel plots for the evaluation of potential publication bias. (A) Overall survival for metastatic renal cell carcinoma; (B) Progression-free survival for metastatic renal cell carcinoma. |
Discussion
To our best knowledge, this is the first meta-analysis to synthetically analyze the prognostic value of pretreatment neutrophil count in mRCC patients. We proved that an elevated pretreatment neutrophil count could be a target biomarker for worse OS and PFS in mRCC patients. Results of subgroup analysis also demonstrated that an elevated pretreatment neutrophil count is a reliable biomarker regardless of analysis type, ethnic background and treatment method. Our meta-analysis also provides a theoretical basis for researches based on neutrophil count.
Recently, researches have proved indicators such as neutrophil-to-lymphocyte ratio (NLR) and lymphocyte-to-monocyte ratio (LMR) were a poor prognostic factor in renal cell carcinoma.30–32 The ratio of two inflammation biomarkers works since cancer progression is influenced not only by the tumors’ biologic characteristics but also by the host’s inflammation response. However, depending on these researches, whether neutrophil, lymphocyte or monocyte alone is an independent prognostic factor in renal cell carcinoma is still unknown. Studies have reported lymphocyte could play an anti-tumor effect through inducing cell apoptosis and mediating cytotoxicity.7 Although most articles have demonstrated the poor prognosis of neutrophil in renal cell carcinoma,14,22 there still some articles hold the opposite conclusion.33 Hence, we do this study to elucidate the definite role of neutrophil in renal cell carcinoma.
Neutrophils mainly occur in the blood. They are also called polymorphonuclear leukocytes (PMNs) and account for 50–70% of the total number of peripheral white blood cells.34,35 Generally, neutrophils are well known for their potent phagocytic function. They can swallow bacteria, activate the immune system and induce tissue damage in infections.36 However, in untreated tumors, several studies have reported that neutrophils could produce matrix-degrading enzymes and angiogenic factors to suppress the anti-tumor immune response and promote tumor metastasis.37,38 In the tumor microenvironment, chemokines are generated by tumor tissues, and neutrophils in the blood move through the vascular wall into the tumor tissues following stimulation by chemokines. Those neutrophils that traffic into tumors are referred to as tumor-associated neutrophils (TANs).39,40 TANs can be divided into two different phenotypes: an anti-tumorigenic (N1) phenotype and a pro-tumorigenic (N2) phenotype.41 This plasticity of TANs is regulated by various cytokines in the tumor microenvironment. Fridlender42 has demonstrated that transforming growth factor-β (TGF-β) could induce neutrophil polarization to an N2 neutrophil phenotype. Corresponding to his study, interferon-β (INF-β) was demonstrated by Jablonska41 to induce neutrophil polarization to an N1 phenotype.
TAN promoted tumor progression primarily through the secretion of matrix metalloproteinase-9 (MMP-9), neutrophil elastase (NE) and chemokines.43 MMP-9 is a kind of collagenase. It can promote tumor cell infiltration and metastasis by changing extracellular matrix structure.43 MMP-9 can activate angiogenesis factors, such as vascular endothelial growth factor (VEGF) and fibroblast growth factor-2 (FGF-2), to stimulate tumor angiogenesis and increase tumor blood supply to encourage tumor growth.44
NE is an essential member of the chymotrypsin superfamily of serine proteases, which contains 218 amino acid residues and 4 glycoprotein disulfide bonds. NE primarily promotes the occurrence and development of tumors by stimulating the production of related cell growth factors and inhibiting tumor cell apoptosis.45,46 Recently, Houghton found that NE could enter tumor cells and degrade insulin receptor substrate-1 (IRS1).47 This process strengthened the interaction between phosphatidylinositol 3-kinase (PI3K) and the potent mitogen platelet-derived growth factor receptor (PDGFR), thereby skewing the PI3K axis towards tumor cell proliferation.
IL-8 is a member of the CXC chemokines secreted by TAN. It can bind to CXCR2 expressed on the surface of endothelial cells as well as TANs, which not only promotes tumor angiogenesis but also further recruits neutrophils into the tumor microenvironment, suggesting that TANs secrete interleukin (IL)-8 and may create a positive feedback loop to maintain the number of TANs.48,49
On the other hand, N1 phenotype TANs inhibit tumor growth and metastasis. The major mechanisms are as follows: (1) activating the Fas ligand-related apoptosis pathway and directly promoting tumor cell apoptosis;50 (2) activating dendritic cells and CD4+ T cells to induce IL-12 dependent tumor rejection;51 (3) improving the expression of IgGFc receptors to promote an antibody-dependent cellular cytotoxicity (ADCC) effect52 and (4) releasing reactive oxygen species via the degranulation function, leading to tumor cell reactive oxygen species injury and subsequent tumor cell lysis.53
According to the many mechanisms mentioned earlier, neutrophils have been suggested as a novel therapeutic target for mRCC patients. Narrowing the neutrophil level in the blood and promoting neutrophil polarization to an N1 phenotype could inhibit tumor progression and extend survival time.
This meta-analysis has some limitations. First, all of the included studies in our meta-analysis were retrospective. It is very difficult to avoid selection bias in observational studies. Second, we only paid our attention to articles mentioning the HR and the 95% CI; others were removed because they reported only odds ratios and relative risk for survival. Moreover, the pretreatment neutrophil count could interact with some other cell populations and influenced by diverse conditions, such as hypoxia, acute hemolysis, chronic infection, chronic disease and autoimmune disorders, such as rheumatic disease. Most articles presented in this meta-analysis did not investigate those factors.
In conclusion, this meta-analysis proved that an elevated neutrophil level was linked to a poor prognosis in mRCC patients. The pretreatment neutrophil count was a convenient and cost-effective prognostic indicator that could be used for risk stratification and become an additional component of the MSKCC prognostic score. Furthermore, it can be utilized to formulate individualized treatments for mRCC patients. Finally, we propose that pretreatment neutrophil count may be considered as a completely novel therapeutic target for cancer patients. Our meta-analysis highlighted the probable theoretical foundation for the application of pretreatment neutrophil count in mRCC patients. Considering the limitations of the present analysis, further multicenter studies are required to research the underlying mechanisms and confirm our findings.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (Grant no. 81273267), the National Science Foundation of Jiangsu Province (Grant no. BK20150251), the National Science Foundation of Jiangsu Province (Grant no. BK20151180) and Major Scientific and Technological Projects of Changzhou Health Bureau (Grant no. ZD201405). We thank Professor Jingting Jiang for his excellent technical support.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66(1):7–30. doi:10.3322/caac.21332
2. Escudier B, Porta C, Schmidinger M, et al. Renal cell carcinoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2016;27(suppl 5):v58–v68. doi:10.1093/annonc/mdw328
3. Gupta K, Miller JD, Li JZ, Russell MW, Charbonneau C. Epidemiologic and socioeconomic burden of metastatic renal cell carcinoma (mRCC): a literature review. Cancer Treat Rev. 2008;34(3):193–205. doi:10.1016/j.ctrv.2007.12.001
4. Athar U, Gentile TC. Treatment options for metastatic renal cell carcinoma: a review. Can J Urol. 2008;15(2):3954–3966.
5. Motzer RJ, Mazumdar M, Bacik J, Berg W, Amsterdam A, Ferrara J. Survival and prognostic stratification of 670 patients with advanced renal cell carcinoma. J Clin Oncol. 1999;17(8):2530–2540. doi:10.1200/JCO.1999.17.8.2530
6. Coussens LM, Werb Z. Inflammation and cancer. Nature. 2002;420(6917):860–867. doi:10.1038/nature01322
7. Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflammation. Nature. 2008;454(7203):436–444. doi:10.1038/nature07205
8. Kowalewska M, Nowak R, Chechlinska M. Implications of cancer-associated systemic inflammation for biomarker studies. Biochim Biophys Acta. 2010;1806(2):163–171. doi:10.1016/j.bbcan.2010.06.002
9. Minardi D, Scartozzi M, Montesi L, et al. Neutrophil-to-lymphocyte ratio may be associated with the outcome in patients with prostate cancer. Springerplus. 2015;4:255. doi:10.1186/s40064-015-1036-1
10. Steffens S, Kohler A, Rudolph R, et al. Validation of CRP as prognostic marker for renal cell carcinoma in a large series of patients. BMC Cancer. 2012;12:399. doi:10.1186/1471-2407-12-399
11. Balkwill F, Mantovani A. Inflammation and cancer: back to Virchow? Lancet. 2001;357(9255):539–545. doi:10.1016/S0140-6736(00)04046-0
12. Koo KC, Lee KS, Cho KS, Rha KH, Hong SJ, Chung BH. Comprehensive analysis and validation of contemporary survival prognosticators in Korean patients with metastatic renal cell carcinoma treated with targeted therapy: prognostic impact of pretreatment neutrophil-to-lymphocyte ratio. Int Urol Nephrol. 2016;48(6):985–992. doi:10.1007/s11255-016-1252-9
13. Okada F. Inflammation-related carcinogenesis: current findings in epidemiological trends, causes and mechanisms. Yonago Acta Med. 2014;57(2):65–72.
14. Fox P, Hudson M, Brown C, et al. Markers of systemic inflammation predict survival in patients with advanced renal cell cancer. Br J Cancer. 2013;109(1):147–153. doi:10.1038/bjc.2013.300
15. Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials. 2007;8:16. doi:10.1186/1745-6215-8-16
16. Artac M, Coskun HS, Korkmaz L, et al. Using interferon alfa before tyrosine kinase inhibitors may increase survival in patients with metastatic renal cell carcinoma: a Turkish oncology group (TOG) study. Clin Genitourin Cancer. 2016;14(4):e347–e353. doi:10.1016/j.clgc.2016.04.021
17. Santoni M, Buti S, Conti A, et al. Prognostic significance of host immune status in patients with late relapsing renal cell carcinoma treated with targeted therapy. Target Oncol. 2015;10(4):517–522. doi:10.1007/s11523-014-0356-3
18. You D, Jeong IG, Song C, et al. Analysis of pre-operative variables for identifying patients who might benefit from upfront cytoreductive nephrectomy for metastatic renal cell carcinoma in the targeted therapy era. Jpn J Clin Oncol. 2015;45(1):96–102. doi:10.1093/jjco/hyu171
19. Poprach A, Pavlik T, Melichar B, et al. Clinical and laboratory prognostic factors in patients with metastatic renal cell carcinoma treated with sunitinib and sorafenib after progression on cytokines. Urol Oncol. 2014;32(4):488–495. doi:10.1016/j.urolonc.2013.09.011
20. Santoni M, De Giorgi U, Iacovelli R, et al. Pre-treatment neutrophil-to-lymphocyte ratio may be associated with the outcome in patients treated with everolimus for metastatic renal cell carcinoma. Br J Cancer. 2013;109(7):1755–1759. doi:10.1038/bjc.2013.522
21. Kroeger N, Xie W, Lee JL, et al. Metastatic non-clear cell renal cell carcinoma treated with targeted therapy agents: characterization of survival outcome and application of the international mRCC database consortium criteria. Cancer. 2013;119(16):2999–3006. doi:10.1002/cncr.28151
22. Azuma T, Matayoshi Y, Nagase Y, Oshi M. Neutrophil number after interferon-alfa treatment is an independent predictive marker of overall survival in metastatic renal cell carcinoma. Clin Genitourin Cancer. 2012;10(3):180–184. doi:10.1016/j.clgc.2012.03.006
23. Lee JL, Park I, Park K, et al. Efficacy and safety of vascular endothelial growth factor receptor tyrosine kinase inhibitors in patients with metastatic renal cell carcinoma and poor risk features. J Cancer Res Clin Oncol. 2012;138(4):687–693. doi:10.1007/s00432-012-1148-8
24. Heng DY, Xie W, Regan MM, et al. Prognostic factors for overall survival in patients with metastatic renal cell carcinoma treated with vascular endothelial growth factor-targeted agents: results from a large, multicenter study. J Clin Oncol. 2009;27(34):5794–5799. doi:10.1200/JCO.2008.21.4809
25. Atzpodien J, Reitz M. Peripheral blood neutrophils as independent immunologic predictor of response and long-term survival upon immunotherapy in metastatic renal-cell carcinoma. Cancer Biother Radiopharm. 2008;23(1):129–134. doi:10.1089/cbr.2007.0429
26. Donskov F, von der Maase H. Impact of immune parameters on long-term survival in metastatic renal cell carcinoma. J Clin Oncol. 2006;24(13):1997–2005. doi:10.1200/JCO.2005.03.9594
27. Peccatori J, Barkholt L, Demirer T, et al. Prognostic factors for survival in patients with advanced renal cell carcinoma undergoing nonmyeloablative allogeneic stem cell transplantation. Cancer. 2005;104(10):2099–2103. doi:10.1002/cncr.21477
28. Atzpodien J, Royston P, Wandert T, Reitz M. Metastatic renal carcinoma comprehensive prognostic system. Br J Cancer. 2003;88(3):348–353. doi:10.1038/sj.bjc.6600768
29. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603–605. doi:10.1007/s10654-010-9491-z
30. Gu L, Li H, Chen L, et al. Prognostic role of lymphocyte to monocyte ratio for patients with cancer: evidence from a systematic review and meta-analysis. Oncotarget. 2016;7(22):31926–31942. doi:10.18632/oncotarget.7876
31. Na N, Yao J, Cheng C, et al. Meta-analysis of the efficacy of the pretreatment neutrophil-to-lymphocyte ratio as a predictor of prognosis in renal carcinoma patients receiving tyrosine kinase inhibitors. Oncotarget. 2016;7(28):44039–44046. doi:10.18632/oncotarget.9836
32. Hu K, Lou L, Ye J, Zhang S. Prognostic role of the neutrophil-lymphocyte ratio in renal cell carcinoma: a meta-analysis. BMJ Open. 2015;5(4):e006404. doi:10.1136/bmjopen-2014-006404
33. Motzer RJ, Escudier B, Bukowski R, et al. Prognostic factors for survival in 1059 patients treated with sunitinib for metastatic renal cell carcinoma. Br J Cancer. 2013;108(12):2470–2477. doi:10.1038/bjc.2013.236
34. Stegenga ME, van der Crabben SN, Blumer RM, et al. Hyperglycemia enhances coagulation and reduces neutrophil degranulation, whereas hyperinsulinemia inhibits fibrinolysis during human endotoxemia. Blood. 2008;112(1):82–89. doi:10.1182/blood-2007-11-121723
35. Pham CT. Neutrophil serine proteases: specific regulators of inflammation. Nat Rev Immunol. 2006;6(7):541–550. doi:10.1038/nri1841
36. Ashtekar AR, Saha B. Poly’s plea: membership to the club of APCs. Trends Immunol. 2003;24(9):485–490.
37. Pekarek LA, Starr BA, Toledano AY, Schreiber H. Inhibition of tumor growth by elimination of granulocytes. J Exp Med. 1995;181(1):435–440. doi:10.1084/jem.181.1.435
38. Tazawa H, Okada F, Kobayashi T, et al. Infiltration of neutrophils is required for acquisition of metastatic phenotype of benign murine fibrosarcoma cells: implication of inflammation-associated carcinogenesis and tumor progression. Am J Pathol. 2003;163(6):2221–2232. doi:10.1016/S0002-9440(10)63580-8
39. Galdiero MR, Bonavita E, Barajon I, Garlanda C, Mantovani A, Jaillon S. Tumor associated macrophages and neutrophils in cancer. Immunobiology. 2013;218(11):1402–1410. doi:10.1016/j.imbio.2013.06.003
40. Galdiero MR, Garlanda C, Jaillon S, Marone G, Mantovani A. Tumor associated macrophages and neutrophils in tumor progression. J Cell Physiol. 2013;228(7):1404–1412. doi:10.1002/jcp.24260
41. Jablonska J, Leschner S, Westphal K, Lienenklaus S, Weiss S. Neutrophils responsive to endogenous IFN-beta regulate tumor angiogenesis and growth in a mouse tumor model. J Clin Invest. 2010;120(4):1151–1164. doi:10.1172/JCI37223
42. Fridlender ZG, Sun J, Kim S, et al. Polarization of tumor-associated neutrophil phenotype by TGF-beta: “N1” versus “N2” TAN. Cancer Cell. 2009;16(3):183–194. doi:10.1016/j.ccr.2009.06.017
43. Dumitru CA, Lang S, Brandau S. Modulation of neutrophil granulocytes in the tumor microenvironment: mechanisms and consequences for tumor progression. Semin Cancer Biol. 2013;23(3):141–148. doi:10.1016/j.semcancer.2013.02.005
44. Ebrahem Q, Chaurasia SS, Vasanji A, et al. Cross-talk between vascular endothelial growth factor and matrix metalloproteinases in the induction of neovascularization in vivo. Am J Pathol. 2010;176(1):496–503. doi:10.2353/ajpath.2010.080642
45. Gasparini C, Menegazzi R, Patriarca P, Dri P. Evidence that elastase is the TNF-R75 shedding enzyme in resting human polymorphonuclear leukocytes. FEBS Lett. 2003;553(3):360–364.
46. Wada Y, Yoshida K, Tsutani Y, et al. Neutrophil elastase induces cell proliferation and migration by the release of TGF-alpha, PDGF and VEGF in esophageal cell lines. Oncol Rep. 2007;17(1):161–167.
47. Houghton AM, Rzymkiewicz DM, Ji H, et al. Neutrophil elastase-mediated degradation of IRS-1 accelerates lung tumor growth. Nat Med. 2010;16(2):219–223. doi:10.1038/nm.2084
48. Lopez-Lago MA, Posner S, Thodima VJ, Molina AM, Motzer RJ, Chaganti RS. Neutrophil chemokines secreted by tumor cells mount a lung antimetastatic response during renal cell carcinoma progression. Oncogene. 2013;32(14):1752–1760. doi:10.1038/onc.2012.201
49. Shang K, Bai YP, Wang C, et al. Crucial involvement of tumor-associated neutrophils in the regulation of chronic colitis-associated carcinogenesis in mice. PLoS One. 2012;7(12):e51848. doi:10.1371/journal.pone.0051848
50. Chen YL, Chen SH, Wang JY, Yang BC. Fas ligand on tumor cells mediates inactivation of neutrophils. J Immunol. 2003;171(3):1183–1191.
51. Medina-Echeverz J, Fioravanti J, Zabala M, Ardaiz N, Prieto J, Berraondo P. Successful colon cancer eradication after chemoimmunotherapy is associated with profound phenotypic change of intratumoral myeloid cells. J Immunol. 2011;186(2):807–815. doi:10.4049/jimmunol.1001483
52. Hubert P, Heitzmann A, Viel S, et al. Antibody-dependent cell cytotoxicity synapses form in mice during tumor-specific antibody immunotherapy. Cancer Res. 2011;71(15):5134–5143. doi:10.1158/0008-5472.CAN-10-4222
53. Granot Z, Henke E, Comen EA, King TA, Norton L, Benezra R. Tumor entrained neutrophils inhibit seeding in the premetastatic lung. Cancer Cell. 2011;20(3):300–314. doi:10.1016/j.ccr.2011.08.012
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.