Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
Prognostic Determinants and Treatment Strategies Associated with Long-Term Survival in Early-Stage Hepatocellular Carcinoma: A Retrospective Cohort Study
Authors Pan KC ![]() , Huang HL
, Huang HL ![]() , Lu SN
, Lu SN ![]() , Chang TS
, Chang TS
Received 3 August 2025
Accepted for publication 12 December 2025
Published 23 December 2025 Volume 2025:12 Pages 2893—2905
DOI https://doi.org/10.2147/JHC.S554624
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Mohamed Shaker
Kuan Chen Pan,1 Hui-Ling Huang,1,2 Sheng-Nan Lu,1– 3 Te-Sheng Chang1,4
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, Chang Gung Memorial Hospital, Chiayi, Taiwan; 2Department of Nursing, Chang Gung Memorial Hospital, Chiayi, Taiwan; 3Division of Hepato-Gastroenterology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan; 4College of Medicine, Chang Gung University, Taoyuan, Taiwan
Correspondence: Sheng-Nan Lu, Division of Hepato-Gastroenterology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan, Email [email protected]
Purpose: Hepatocellular carcinoma (HCC) remains a major cause of cancer-related mortality worldwide and is particularly prevalent in Taiwan. While curative treatments offer favorable outcomes for early-stage HCC, prognostic factors change and option medical strategy remain uncertain in long term survival early-stage HCC.
Patients and Methods: This retrospective study analyzed 1144 patients with BCLC stage 0 or A HCC from a cancer registry (2011– 2020) followed through 2023. Prognostic factors were evaluated using Cox regression. Subgroup analyses were performed on patients who survived over five years, and further stratified into 5– 10 years and > 10 years survival groups to assess treatment outcomes and tumor-free status (TFS).
Results: Age > 65, Child-Pugh B, and non-curative treatment were consistent poor prognostic factors; HBV-related HCC was associated with improved survival. Among patients surviving > 10 years, higher TFS rates and lower stage progression were observed compared to those surviving 5– 10 years. Curative treatment significantly increased the likelihood of achieving TFS (p = 0.044).
Conclusion: Long-term survival in early-stage HCC is influenced by age, liver function, viral etiology, and treatment strategy. Curative treatments significantly improve outcomes, and maintaining curative treatment options is crucial for patients who experience recurrence while still in the early stage of HCC.
Keywords: long-term survival, prognostic factors, early-stage HCC, treatment strategy
Introduction
Hepatocellular carcinoma (HCC) is commonly diagnosed cancer and the leading cause of cancer related-death worldwide.1 It is the second cause of cancer-related death and the fourth most common newly diagnosed cancer in Taiwan.2 Despite advances in various treatment modalities, HCC remains a disease that requires close clinical attention. In early-stage HCC, curative treatment is often achievable, and complete tumor eradication can lead to favorable long-term outcomes. Therefore, clinical decision-making and treatment strategies for patients with early-stage HCC must be approached with particular care and precision.
Previous studies have extensively explored the prognostic factors associated with HCC, as well as survival and recurrence outcomes related to initial treatment modalities.3–5 However, most prognostic factor analyses have focused on survival within five years of diagnosis.6 Given the increasing availability and efficacy of therapeutic options, many early-stage HCC patients now survive beyond five years. Nevertheless, limited research has investigated long-term prognostic factors (survival beyond five years) and the evolution of treatment strategies in these long-term survivors. Therefore, this study was designed to investigate the prognostic factors and therapeutic strategies associated with long-term survival in patients with early-stage HCC.
This study aims to focused on the following key questions: (1) Do the prognostic factors for early-stage HCC change in patients who survive more than five years, and which of these factors are associated with long-term survival? (2) What are the curative treatment and stage progression rates among early-stage HCC patients who achieve long-term survival? (3) What clinical characteristics and treatment strategies are associated with higher tumor-free status and favorable long-term outcomes?
Materials and Methods
Population and Data Collection
This retrospective study was conducted using data from the cancer registry of a regional hospital, including patients diagnosed with hepatocellular carcinoma (HCC) between January 2011 and December 2020, with follow-up extending through December 2023. The registry provided comprehensive baseline information, including patient sex, age, tumor stage, viral etiology, liver function reserve (Child-Pugh classification), date and stage at diagnosis, and tumor marker levels. Additional clinical data such as initial treatment type, time to recurrence, subsequent treatments, and date of death or last follow-up were obtained through detailed manual review of individual medical records. Among the 1144 patients included, 22 (1.9%) had missing Child-Pugh scores. These cases were retained in the overall analysis due to completeness of other key variables but were excluded from subgroup analyses where liver function classification was essential.
Patients were excluded if they had received any prior HCC-related treatment before the recorded diagnosis, had an uncertain disease stage, were diagnosed with advanced-stage HCC (BCLC stage B, C, or D), or had incomplete treatment records due to referral to other institutions. Following the application of these criteria, only patients with early-stage HCC (BCLC stage 0 or A) and complete treatment and follow-up data were included in the analysis. Curative treatments were defined as surgical resection, liver transplantation, or tumor ablation, while non-curative treatments encompassed all other therapeutic modalities. Tumor-free survival (TFS) was defined as the state in which no viable tumor was detected by dynamic contrast-enhanced imaging (CT or MRI) for at least 6 months following the last treatment session. Patients who remained within the early-stage classification, achieved complete tumor elimination, and experienced no recurrence within up to three treatment sessions were classified as having achieved TFS.
Study Design
The study was conducted in two parts. The first part aimed to identify prognostic factors associated with overall survival, with additional focus on factors specifically predictive of survival beyond five years. Seven key variables were selected based on existing literature: age, sex, viral etiology (hepatitis B or C), tumor burden (tumor number), liver function reserve (Child-Pugh classification), serum tumor marker (AFP level), and initial treatment modality. A subgroup analysis was conducted on patients who survived more than five years, applying the same evaluation framework to further explore characteristics associated with long-term survival.
The second part of the study focused on long-term survivors, comparing patients who survived beyond ten years with those who survived between five and ten years. Patients who were still alive at the last follow-up but had not yet reached ten years of survival were excluded from this comparison. Baseline characteristics and treatment courses were compared between these two subgroups. In addition, treatment outcomes were analyzed by assessing tumor-free status and stage progression rates. Stage progression was defined as advancement to BCLC stage B or C or D. The proportion of curative treatments relative to total treatment sessions was also examined, particularly in patients who achieved tumor-free status, to evaluate whether curative interventions were associated with better long-term outcomes.
Statistical Analysis
Descriptive statistics, including means with standard deviations and percentages, were used to summarize patient demographics and clinical characteristics. Categorical variables were compared using chi-square tests, with or without Yates’ correction, or Fisher’s exact test as appropriate. Survival analyses were performed using the Kaplan–Meier method and Cox proportional hazards regression models. Statistical significance was defined as a two-tailed p-value of less than 0.05. All statistical analyses were conducted using R version 4.2.3 (R Foundation for Statistical Computing). This study was approved by the Institutional Review Board of Chang Gung Memorial Hospital, Chiayi Branch (IRB number: 202500300B0). Informed consent was waived due to the retrospective design. All data were anonymized prior to analysis to ensure patient confidentiality.
Results
Between 2011 and 2020, a total of 3170 patients with hepatocellular carcinoma (HCC) were registered in the cancer registry and followed up until December 2023. Patients were excluded if they had undergone prior treatment, had an unknown disease stage, were classified as BCLC stage B or later, no available treatment records, or were transferred to other institutions. Ultimately, 1144 patients with early-stage HCC (BCLC 0 or A) were included in the analysis. These patients were categorized into three groups based on survival duration: less than 5 years, 5 to 10 years, and more than 10 years (shown in Figure 1). The median survival of the entire cohort was 81.8 months. Specifically, patients with BCLC stage 0 (n = 260) had a median survival of 17.9 months, while those with stage A (n = 884) had a median survival of 76.2 months (p = 0.0012) (shown in Figure 2).
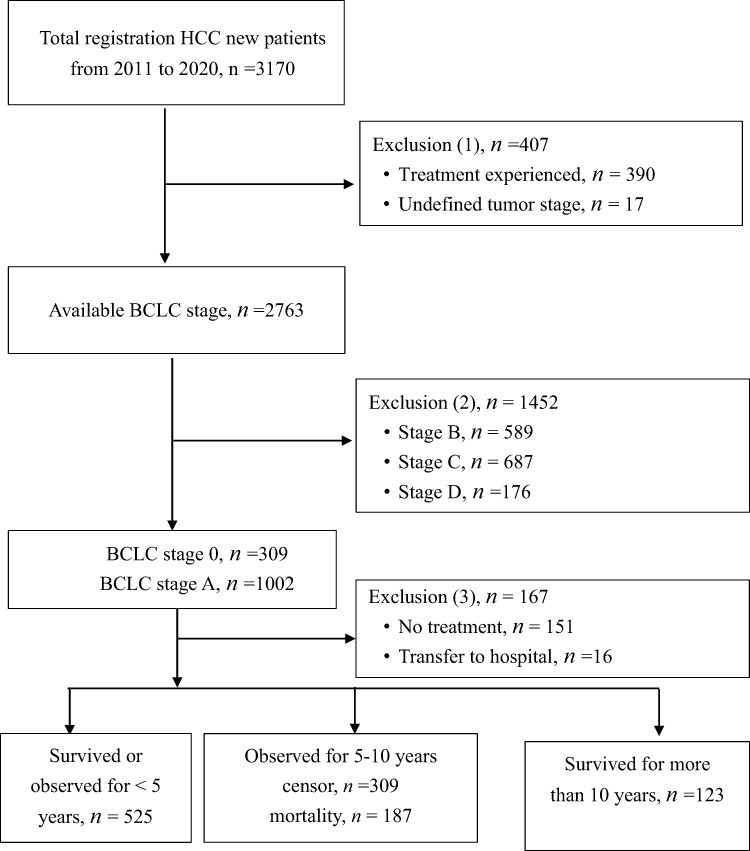 |
Figure 1 Patient selection flowchart. Abbreviations: HCC, hepatocellular carcinoma; BCLC, Barcelona Clinic Liver Cancer. Notes: From 3170 registered hepatocellular carcinoma (HCC) cases (2011–2020), exclusions were made based on prior treatment, undefined staging, and advanced BCLC stages. A total of 1144 early-stage HCC patients (BCLC stage 0 and A) were included for analysis, with subgroup classifications by survival duration. |
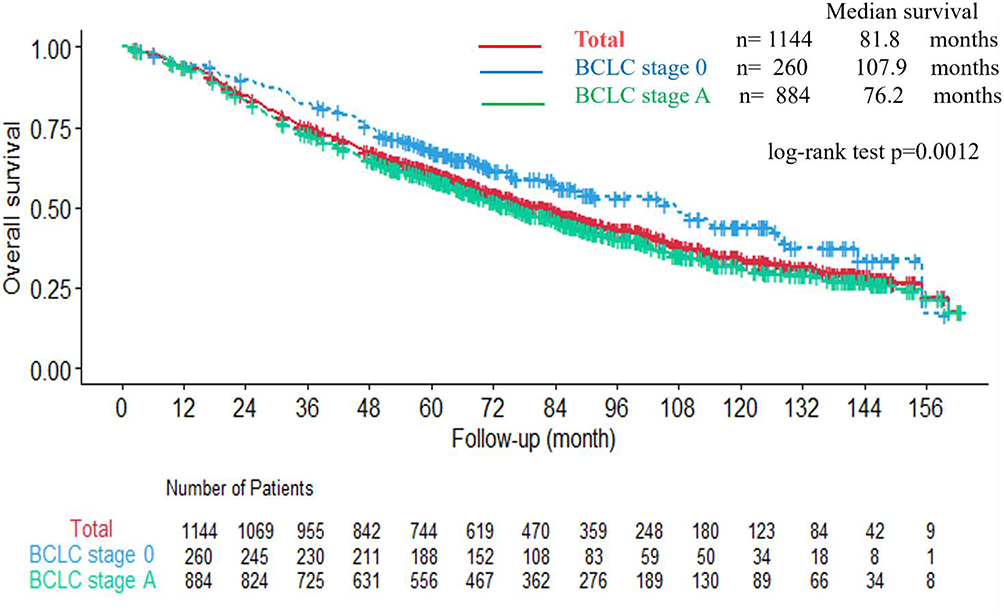 |
Figure 2 Kaplan–Meier survival curves of early-stage HCC patients stratified by BCLC stage 0 (n = 260) and stage A (n = 884), indicating the overall survival differences between the two groups. Abbreviations: HCC, hepatocellular carcinoma; BCLC, Barcelona Clinic Liver Cancer. |
In univariate analysis, the following were identified as poor prognostic factors: age >65 years, presence of multiple tumors, non-viral etiology, Child-Pugh class B, AFP > 20 ng/mL, and non-curative initial treatment, with hazard ratios (HRs) of 1.54, 1.43, 2.48, 1.85, 1.44, and 2.21, respectively. In contrast, patients with HBV-related HCC who received curative treatment had a significantly lower risk of mortality (HR = 0.44). In multivariate analysis, the variable “multiple tumors” was no longer statistically significant (Table 1) Focusing on the subgroup of 619 patients who survived more than 5 years, both univariate and multivariate analyses showed age >65 years, Child-Pugh class B and non-curative treatment were poor prognostic factors, while HBV-related HCC was good prognostic factors (Table 2).
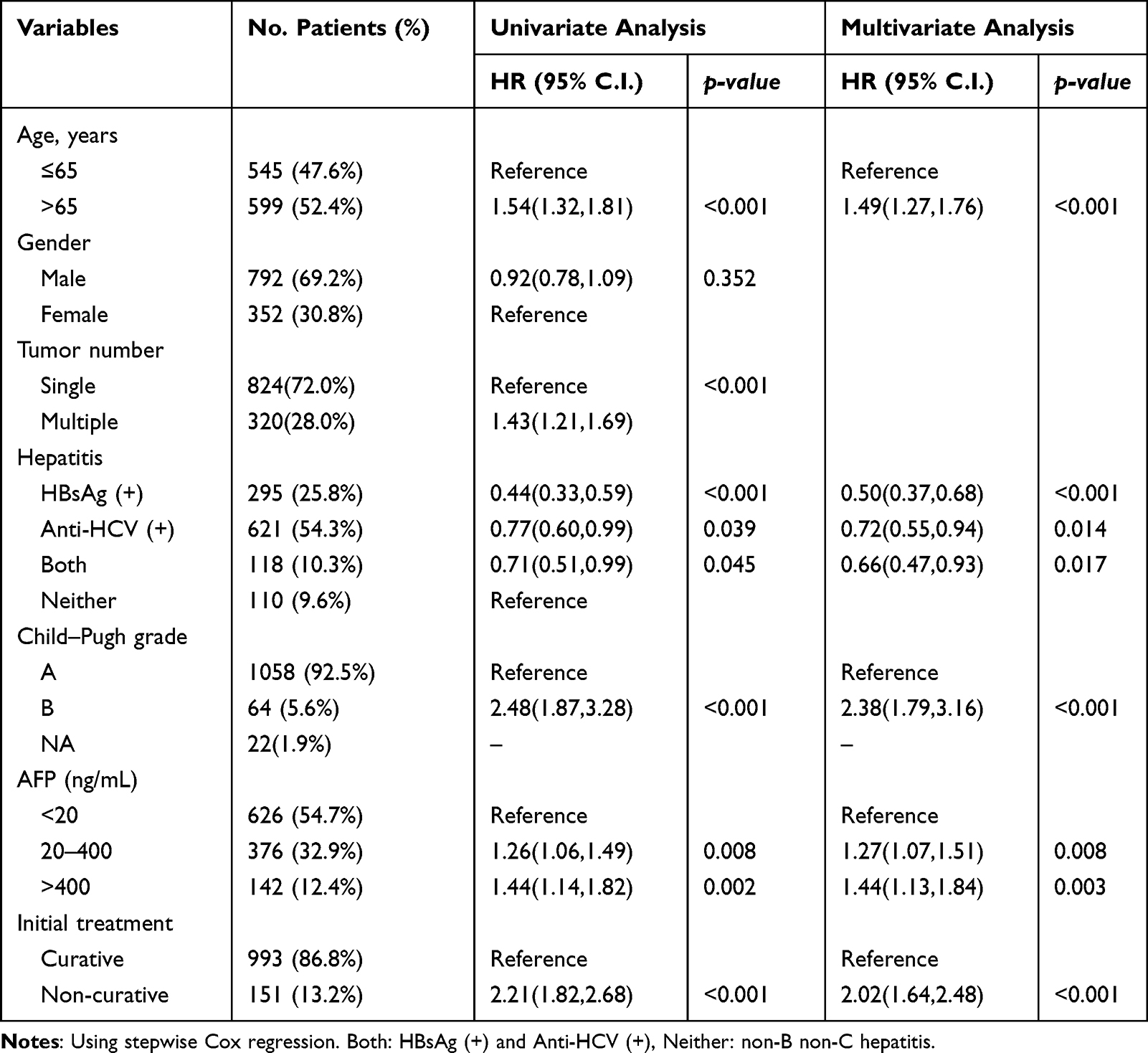 |
Table 1 Characters and Biomarkers on Patients Initially Diagnosed with Early-Stage Hepatocellular Carcinoma in Cancer Registry at Regional Hospital from 2011–2020. Total 1144 Patients |
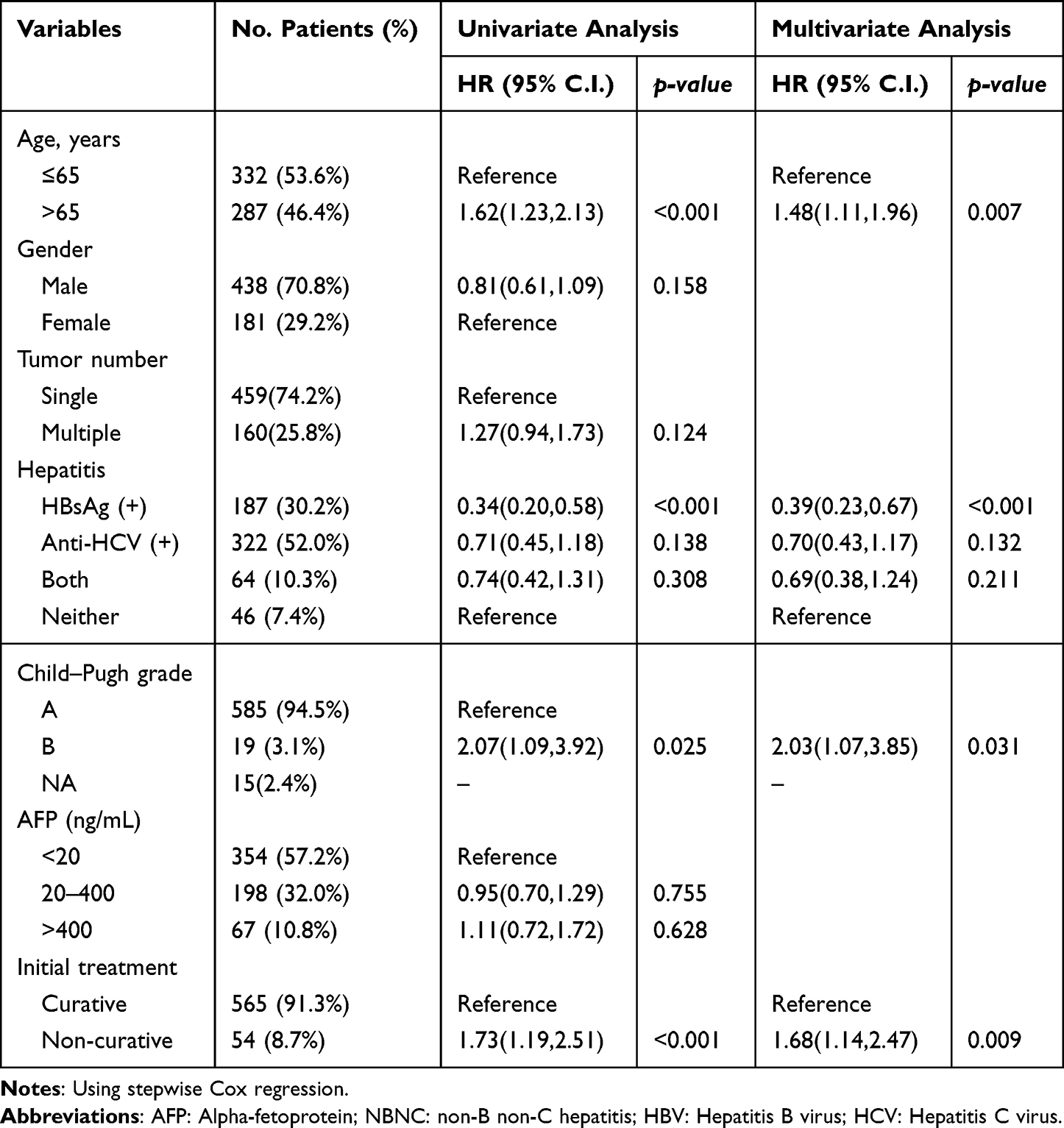 |
Table 2 Characters and Biomarkers on Patients Initially Diagnosed with Early-Stage Hepatocellular Carcinoma in Cancer Registry at Regional Hospital from 2011–2020 with Survival Over 5 Years. Total 619 Patients |
Summarizing findings in Tables 1 and 2, findings were as follows. 1. After multiple adjustment, “multiple tumors” was no more significant. 2. Limited patients with longer survival, effect of “AFP >400” disappeared. 3. Comparing to Table 1, proportions of poor prognostic factors decreased in Table 2, ie “Age > 65 years” from 52.4% to 46.4% (11.5% decrease), “non-hepatitis B” from 74.2% to 69.8% (5.9% decrease), “Child-Pugh Class B” from 5.6% to 3.1% (44.6% decrease) and “non-curative treatment” from 13.2% to 8.7% (34.1% decrease). 4. “Child-Pugh B” affected small proportion of patients, but with highest HR, highest proportion decrease. 5. “Age > 65 years” and “hepatitis B-related” involved large proportion and with stationary effects. 6. The only modifiable factor “initial treatment” plays significant role of both analyses.
During this study period, a total of 123 patients with early HCC lived for more than 10 years and 187 patients died within 5 to 10 years. Patient characteristics about age, gender, hepatitis, AFP, child score, and BCLC stage were demonstrated in Table 3. In survival more than 10 years group, the patient had younger ages, and more hepatitis B carriers compared with survival 5–10 years group.
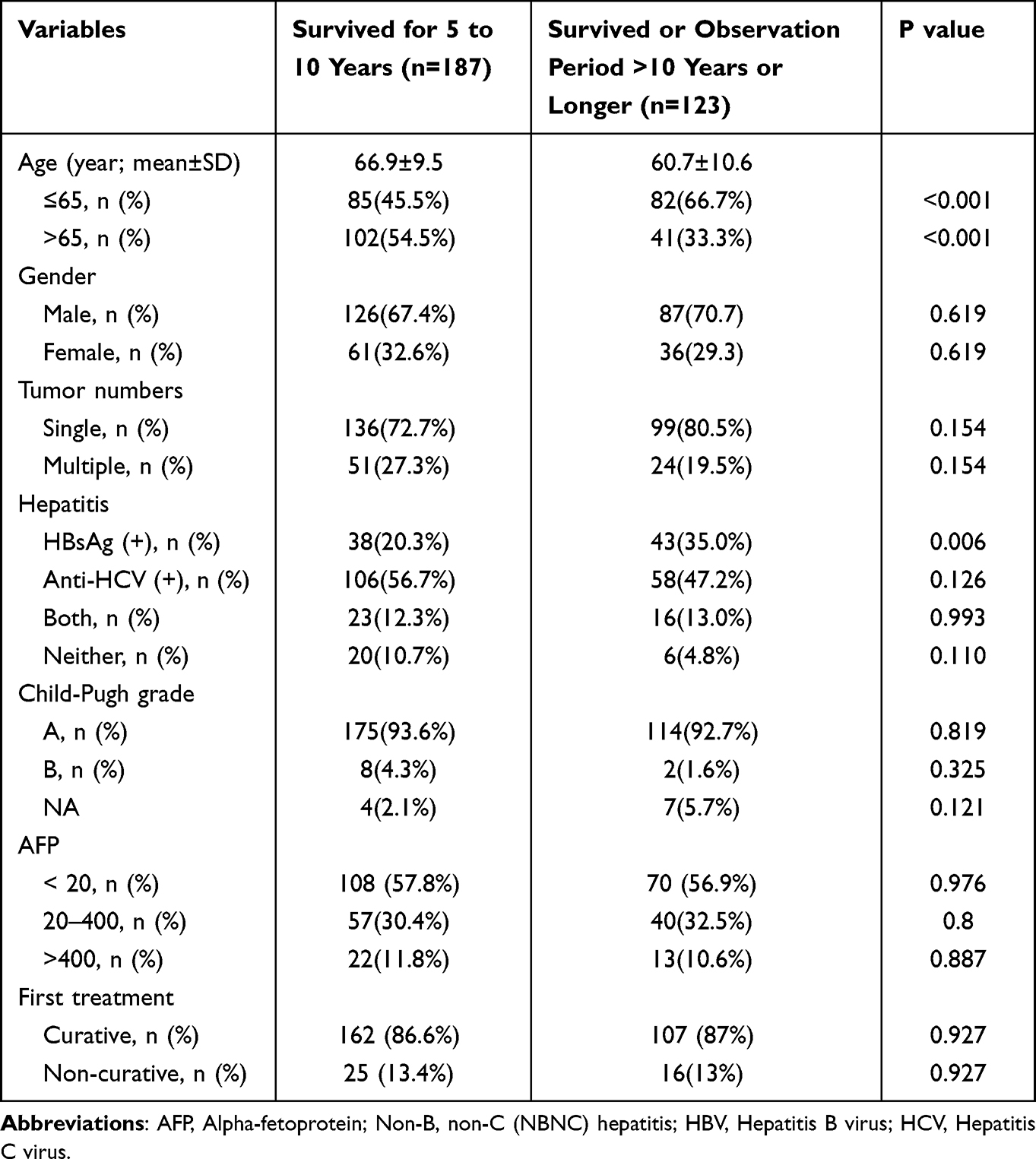 |
Table 3 Characters and Biomarkers on Patients Initially Diagnosed with Early-Stage Hepatocellular Carcinoma in Survival Over 10 Years Group and Survival 5–10 Years Group |
Comparing to Table 2, proportions of poor prognostic factors decreased in patients survived for than 10 years, “Age > 65 years” from 46.4% to 33.3% (28.2% decrease), “non-hepatitis B” from 69.8% to 65.0% (6.9% decrease), and “Child-Pugh Class B” from 3.1% to 1.6% (48.4% decrease) while “non-curative treatment” increased from 8.7% to 13.0% (49.4% increase).
Treatment results of not only initial treatment session but also the 2nd and 3rd treatment sessions were shown in Figure 3. In the group of 123 patients who survived for more than 10 years, a treatment flowchart (shown in Figure 3) was created based on the number of treatments and recurrence status. In the initial treatment, 52 (42.3%) out of 123 patients achieved tumor-free status (TFS). The 71 recurrent cases, but 2 with stage progression, underwent 2nd treatment, and 35 (35/69=50.7%) achieved TFS. The 34 patients experienced the 2nd recurrence, but one with stage progression, underwent the 3rd treatment, and 13 (13/33=39.4%) achieved TFS. In the 123 patients, 100 (81.3%) achieved TFS within 3 sessions of treatment. The TFS rate per treatment sessions was 44.4% (100 TFS/ 225 sessions).
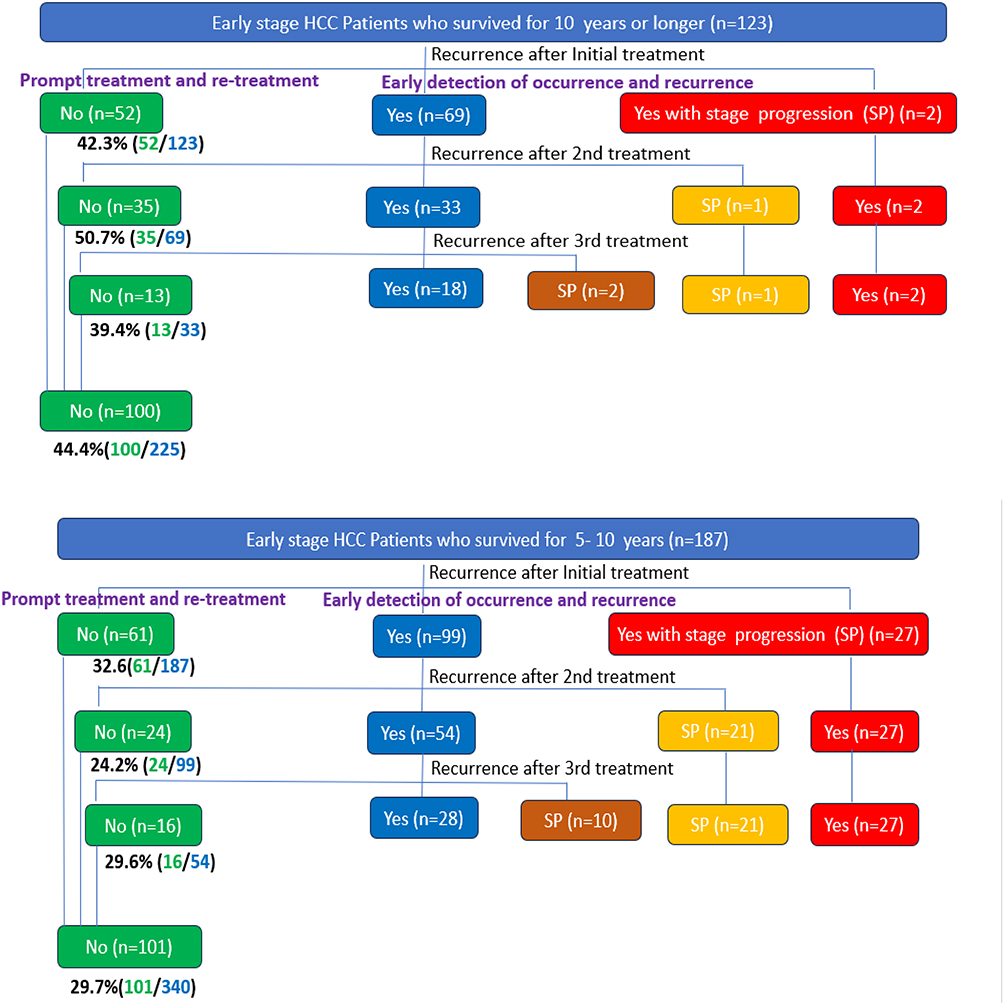 |
Figure 3 Treatment outcomes of patients who survived >10 years and survived 5–10 years across their first three treatments. Abbreviations: HCC, hepatocellular carcinoma; BCLC, Barcelona Clinic Liver Cancer. Note: Outcomes include tumor-free status, recurrence within early-stage HCC (BCLC 0 or A), and progression beyond BCLC stage B. |
In the group of 187 patients who survived for 5–10 years group, a treatment flowchart (shown in Figure 3) was created based on the number of treatments and recurrence status. In the initial treatment, 61 (32.6%) out of 187 patients achieved tumor-free status. The 126 recurrent cases, but 27 with stage progression, underwent 2nd treatment, and 24 (24/99=24.2%) achieved TFS. Seventy-five patients experienced the 2nd recurrence, but 21 with stage progression, underwent the 3rd treatment, and 16 (16/54=29.6%) achieved TFS. In the 187 patients, 101 (54%) achieved TFS within 3 sessions of treatment. The TFS rate per treatment sessions was 29.7% (101 TFS/ 340 sessions).
Compared survival over 10 years group with survival 5–10 years group related to their first 3 sessions of treatment (Table 4). After 1st treatment, 52 patients (42.3%) achieved TFS in survival over 10 years group, and 61 patients (32.6%) achieved TFS in survival 5–10 years group. There was no statistical significance (P=0.084). After the 2nd treatment, 70.7% of patients in survival over 10 years compared with 45.5% of patients in survival 5–10 years achieved TFS with statistical significance (P<0.001). One hundred patients (81.3%) in survival over 10 years group achieved, and 101 patients (54%) in survival 5–10 years had TFS. There was statistical significance (P<0.001).
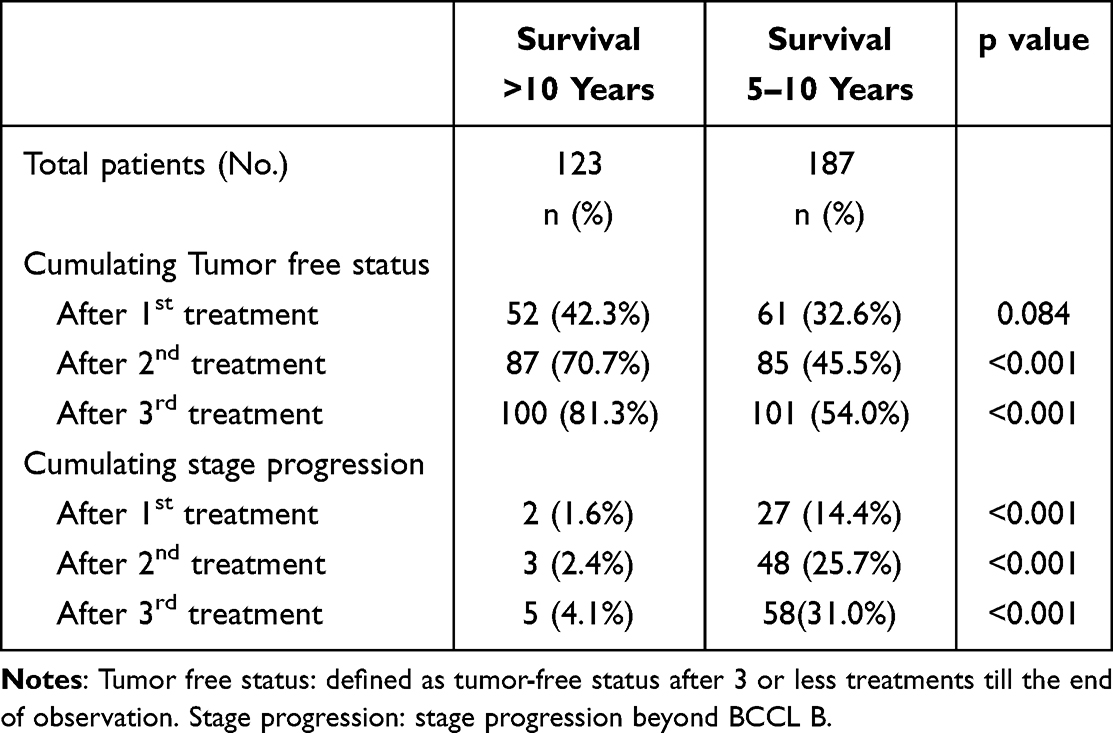 |
Table 4 Patients with Early-Stage Liver Cancer Who Received the First Three Treatments and Stage Progression Status During Follow-Up Period Were Divided into Two Groups: Over 10 Years and Survival 5–10 Years |
In cumulating stage progression, after the first three sessions treatment, only 5 patients (4.1%) in the >10-year group experienced stage progression compared to 58 patients (31%) in the 5–10-year group (p < 0.001). Similar significant differences were observed after the first and second treatment sessions.
In total, there were 225 treatment sessions in the >10-year survival group and 340 sessions in the 5–10-year group, all within early-stage disease. (Table 5). In initial treatment, 107 curative treatment sessions (87%) in survival over 10 years compared to 156 curative treatment sessions (83.4%) in survival 5–10 years were no statistical significance (P=0.391). In 2nd treatment, curative treatment ratios were 71% (49/69) compared to 61.6% (61/99) with no statistical significance. (P=0.207) There was statistical significance (P=0.092) in 3rd treatment and total first sessions treatment. (P=0.041). Compared curative treatment ratios in the first three treatments, gradually decreased curative treatment ratio was found in two groups (P of trends 0.002 and <0.001).
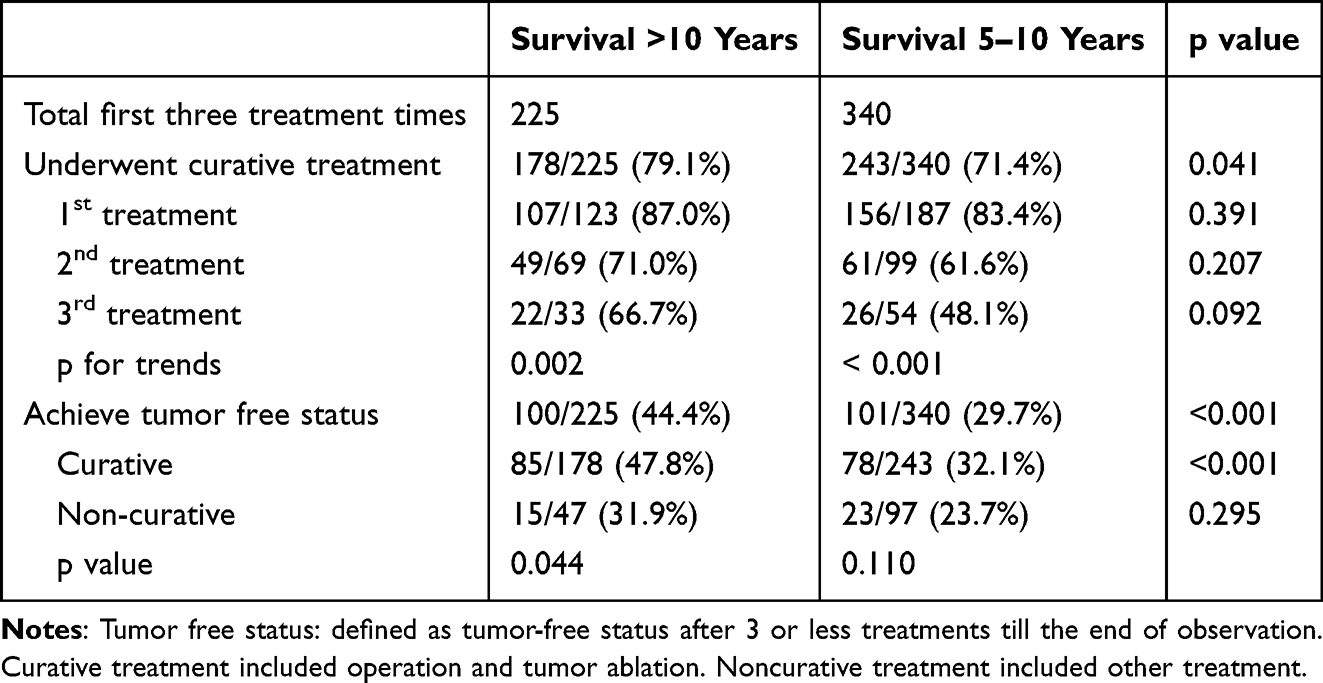 |
Table 5 Patients with Early-Stage Liver Cancer Who Received the First Three Treatments Based on Tumor Free Status and Treatment Types, the Patients Were Divided into Two Groups: Over 10 Years and Survival 5–10 Years |
In survival over 10 years group, there were 100 patients with TFS in total 225 first three sessions treatment. A total of 101 patients achieved TFS in total 340 first three sessions treatment in survival 5–10 years group. Compared to the tumor-free status ratio, patients in survival over 10 years group had better ratio (44.4% vs 29.7%) with statistical significance (P<0.001). In the >10-year group, 85 patients achieved TFS with 178 curative sessions, and 15 achieved TFS with 47 non-curative sessions. Curative treatments were significantly associated with better TFS rates (p = 0.044).
Discussion
A review of previous literature review reveals that many studies have focused on whether initial treatment influences long-term prognosis in patients with hepatocellular carcinoma,7–9 or have investigated which patient characteristics are best suited for specific initial treatment modalities.10,11 Additionally, prognostic factor analyses frequently identify variables such as liver function reserve, BCLC stage, and tumor biomarkers, though these are largely non-modifiable factors. Therefore, there is growing interest in identifying modifiable factors that could guide adjustments in therapeutic strategies.12 Notably, few studies have explored the role of serial treatment strategies in early-stage HCC. Therefore, our study focuses on the prognostic factors change and serial treatment strategies in long term survival early-stage HCC patients. Patients with early HCC in this study was 1144 number. Two hundred and sixty patients in BCLC 0 with five-year survival rate of 9.0 years, and 884 patients in BCLC A with five-year survival rate of 6.4 years, which met the international standard.13 Although our study population was relatively limited in size, the sample was significant to enable detailed, case-by-case chart reviews, allowing for delicate clinical insights.
In Table 1, based on published references,14 it examined the interplay among multiple prognostic variables, revealing that not all traditionally poor prognostic factors remain significant in long-term survivors. Through these analyses, we gained insight into the relative importance of each variable and were thus able to streamline our selection process, focusing on the most clinically relevant predictors for inclusion in further modeling and interpretation. These prognostic factors included age, viral etiology, liver function reserve (Child-Pugh classification), biomarker (AFP), and tumor numbers. The results are consistent with previous studies.15,16 This study added treatment which represented whether receiving curative treatment. This prognostic factor is a modifiable prognostic factor different from the others. In overall early-stage patients, age >65 years, multiple tumors, non-HBV etiology, Child-Pugh class B, AFP >400 ng/mL, and non-curative treatment were all associated with poorer survival outcomes. However, in multivariate analysis, multiple tumors did not remain a significant factor, and it possibly indicated that effective treatment strategies can overcome the prognostic impact of limited tumor multiplicity. When analysis was limited to patients who survived more than five years (Table 2), both univariate and multivariate analyses showed that multiple tumors and AFP >400 ng/mL were no longer significant prognostic factors. It is also possible that patients with an initial AFP >400 ng/mL who survived beyond five years had favorable treatment responses, thereby mitigating the adverse prognostic effect typically associated with elevated AFP levels. To further explore the impact of these variables, we analyzed the changes in patient proportions and hazard ratios (HRs) for each factor before and after the five-year mark. Prognostic factors associated with both a high patient proportion and a high hazard ratio warrant greater clinical attention. Among poor prognostic factors in this study, in Table 1, the most prevalent were non-HBV hepatitis (74.2%), age >65 years (52.4%), multiple tumors (28.0%), non-curative treatment (13.2%), AFP > 400 ng/mL (12.4%), and Child-Pugh class B (5.6%). Among these, non-HBV etiology, Child-Pugh B, and non-curative treatment had HRs >2, indicated higher risk. Non-HBV hepatitis was both high prevalent and associated with high risk. Age >65 years and multiple tumors were prevalent but had relatively lower risk. Child-Pugh B and non-curative treatment were less frequent but had high risk. AFP > 400 ng/mL was neither prevalent nor strongly predictive of poor outcome in the long term. Because the 5-year survival rates for BCLC stage 0 and A exceed 50%,17 we conducted an analysis and comparison of prognostic factors among patients who were in the early stages and survived more than five years.
As shown in Tables 2 and 6, among patients who survived more than five years, the proportions of several established risk factors declined across all categories.
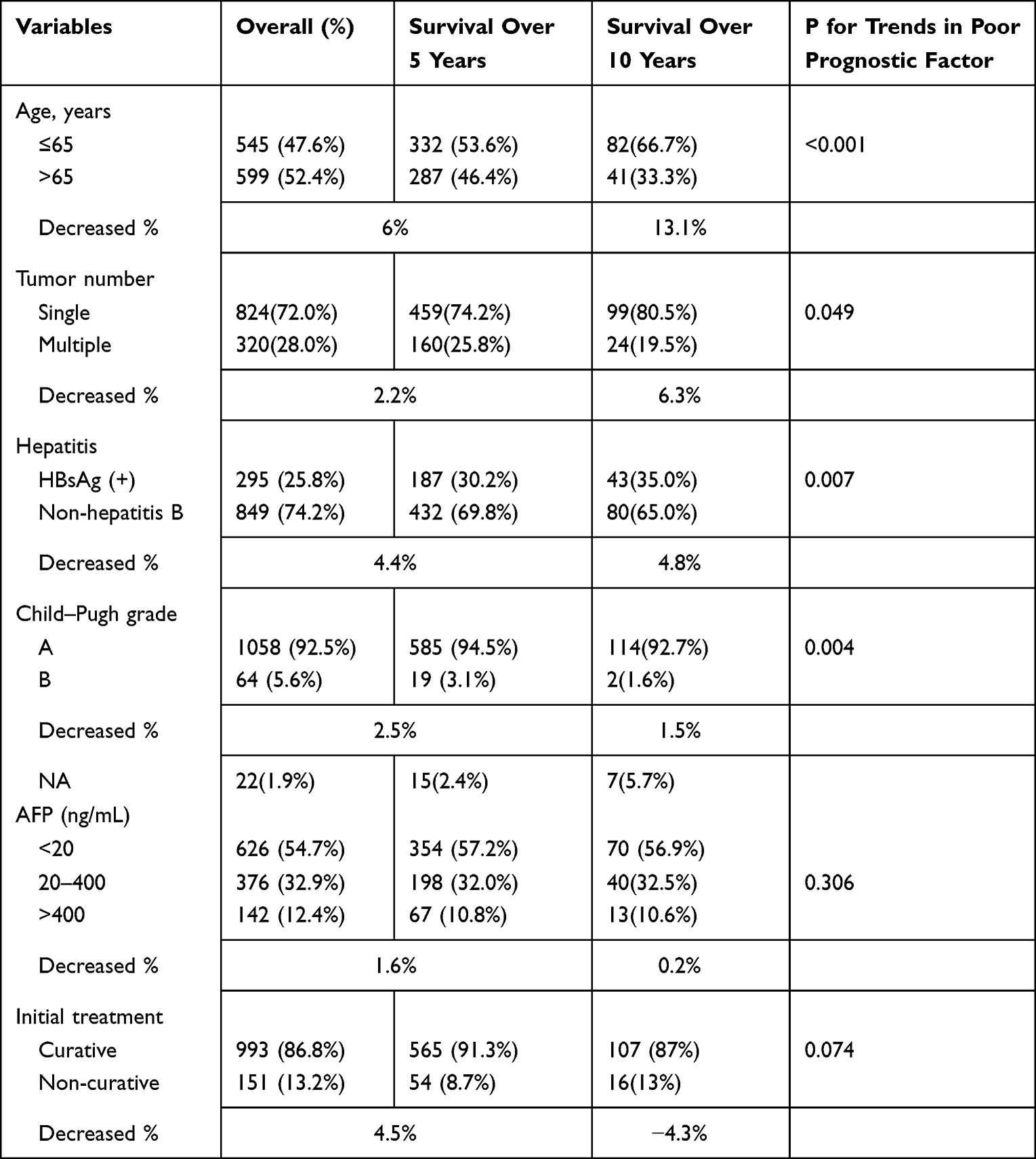 |
Table 6 The Significant Prognostic Factors Were Summarized by the Proportions of Patients from Tables 1–3, Categorized into Three Groups: the Overall Patient, Those Who Survived More Than Five Years, and Those Who Survived More Than Ten Years |
In patients who survived beyond five years, the prevalence of several poor prognostic factors decreased across all categories, with the most notable reductions observed in Child-Pugh B (−44.6%) and non-curative treatment (−34.1%). Although modest declines were also noted in AFP > 400 ng/mL, multiple tumors, and advanced age, age >65 years and non-HBV etiology remained relatively common, suggesting their sustained impact on long-term prognosis.
In patients who survived beyond 10 years, the prevalence of several poor prognostic factors also decreased across all categories. However, the rate of initial non-curative treatment did not decrease as expected. Since treatment modality is a modifiable factor, not only the initial therapy but also the choice and effectiveness of subsequent treatments can continue to influence survival outcomes.
Each variable is discussed in detail below:
Specifically, age >65 years decreased by 6% (a relative reduction of 11.5%). Age >65 years is inherently non-modifiable. Its adverse effect on long-term survival persisted in the extended follow-up cohort and may even become more pronounced due to age-related comorbidities and functional decline.
Non-HBV etiology by 4.4% (5.9% reduction), and it also remained a significant poor prognostic factor. Although antiviral therapy for HBV is now widely available in Taiwan and has improved outcomes for these patients, those with non-HBV-related liver disease—such as alcohol-related liver disease or non-alcoholic fatty liver disease (NAFLD)—often lack disease-modifying therapies. Once such conditions progress to hepatic fibrosis, the associated poor prognosis becomes difficult to reverse.
Multiple tumors decreased by 2.2% (7.9% reduction) and AFP >400 ng/mL decreased by 1.6% (14.6% reduction). These two prognostic factors appeared to lose their prognostic relevance in the long-term survivor subgroup. In early-stage HCC, tumor multiplicity typically remains within three nodules and can be effectively managed through appropriate curative treatment strategies. Likewise, although AFP >400 ng/mL was a significant prognostic marker in the overall cohort, it became non-significant after five years. It was indicated that some patients with high AFP levels can still achieve curative outcomes. Therefore, in patients who survive beyond five years, baseline high AFP level may not be a reliable predictor of long-term survival. Notably, only 1.6% of the long-term survivors had baseline AFP levels exceeding 400 ng/mL.
Child-Pugh class B decreased by 2.5% (44.6% reduction), and it was the indicator of impaired liver function. It remained a strong predictor of poor prognosis despite its low initial prevalence (5.6%). Its proportion further decreased among long-term survivors, suggesting that patients with decompensated liver function were less likely to achieve extended survival, either due to disease progression or limited treatment tolerance. Patients with Child-Pugh class B may have the potential for improvement following treatment, although the likelihood is relatively low. Since liver function can deteriorate following HCC treatment, the variable needs close monitoring in therapeutic planning.
Among all variables, non-curative treatment was the only modifiable prognostic factor. It was consistently associated with worse outcomes in both the overall cohort and the long-term survivor group. Although only 13.2% of patients initially received non-curative treatment, the notable reduction in its prevalence among those surviving beyond five years underscores its substantial impact on survival. Initial treatment alone is insufficient to fully reflect the impact of therapeutic intervention or prediction in long term survival patient, but subsequent treatments can still influence survival outcomes. These findings highlight a critical area for clinical improvement, emphasizing the importance of prioritizing curative strategies whenever feasible in early-stage HCC.
Age over 65, Child-Pugh class B liver function, and non-curative treatment remained consistent adverse prognostic factors in both the overall and long-term survival analyses, suggesting that these variables have a stable impact on long-term outcomes.
Therefore, in the focus of long-term prognosis for early-stage hepatocellular carcinoma, curative treatment should be a priority, and careful monitoring of liver function is essential when evaluating treatment strategies to avoid progression to Child-Pugh class B. Additionally, patients with hepatitis B virus (HBV) infection were found to have relatively better outcomes, likely reflecting the benefits of early antiviral intervention and widespread access to treatment.
As shown in Table 3, patients who survived over ten years were generally younger and had a higher prevalence of hepatitis B virus (HBV) infection compared to those who survived for 5–10 years. These characteristics suggest that this subgroup may have benefited from earlier detection of HBV carrier status, leading to more aggressive interventions, regular monitoring, and early screening.
In >10-year survival group, analysis revealed a significant association between curative treatment and the achievement of tumor-free status (TFS) within the first three treatment sessions. Specifically, 81.3% of patients in the >10-year survival group achieved TFS, significantly higher than the 54% observed in the survival for 5–10-year survival group. Initiation of curative treatment within three sessions led to a 27.3% increase in the 10-year tumor-free survival rate. Regarding stage progression, the 5–10-year survival group had a significantly higher incidence of progression compared to the >10-year survival group. This may be explained by the relatively lower curative treatment rates in the first three sessions among patients in the 5–10-year survival group. These findings suggest that achieving a higher TFS rate and lower stage progression rate are indicated to prolonged survival.
Among patients who achieved TFS within three sessions, the >10-year survival group consistently showed a slightly higher proportion of curative treatment in each session, the differences were not statistically significant. However, the total number of curative treatments over the first three sessions remained higher in the >10-year survival group, indicating that sustained application of curative strategies across treatment sessions—rather than relying on any single treatment—may be critical for achieving long-term survival.
Furthermore, both groups exhibited a decreasing trend in the use of curative treatments with each successive treatment session (p for trend 0.002 and <0.001), suggesting challenges in maintaining curative options over time.
In the >10-year survival group, 44.4% achieved tumor-free status (TFS), which was significantly higher than the 29.7% observed in the 5–10-year survival group. In the >10-year survival group, the cumulative TFS was predominantly achieved within the first two treatment sessions, with the third session contributing only an additional ~10%, suggesting that the success of treatment during the initial two sessions may be more critical for achieving long-term tumor control.
Moreover, within the >10-year group, curative treatments were more effective than non-curative treatments in achieving TFS, with rates of 47.8% versus 31.9%, respectively (p = 0.041). These findings highlight the importance of consistently selecting curative treatment strategies, even in the setting of repeated recurrences in early-stage HCC, as such approaches significantly increase the likelihood of achieving and sustaining tumor-free status.
This study has several limitations. First, it was a retrospective, single-center analysis, which may introduce selection bias and limit the generalizability of the findings. Second, although all cases were carefully reviewed, a proportion of patients with incomplete follow-up data were excluded, which may also affect the results. Third, as our data were collected from 2011 to 2020, the potential era bias should be acknowledged because novel systemic therapies such as immune checkpoint inhibitors were not yet widely implemented during this period, and the outcomes observed may not fully reflect those under current treatment paradigms.
Conclusion
The survival outcomes of the study population were generally consistent with those expected for early-stage hepatocellular carcinoma (HCC). However, our findings indicate that the prognostic factors associated with long-term survival differ in part from those influencing overall survival, particularly in variables that can be modified through clinical intervention. Analysis of subgroup proportions and hazard ratios revealed that younger age and HBV-related HCC were consistently associated with favorable prognosis in both short- and long-term contexts. In contrast, Child-Pugh class B remained a strong negative prognostic factor, albeit with low prevalence. Notably, the initial presence of multiple tumors (1 vs 2–3 nodules) and elevated AFP (>400 ng/mL) appeared to lose prognostic significance in long-term survivors, suggesting that effective treatment may change their adverse impact. In the prognostic factor of curative treatment, this study selected two clinical course indicators for treatment evaluation analysis: achievement of tumor-free status (TFS) within three treatment sessions and the occurrence of stage progression during those sessions. Both indicators showed significant differences between the comparison groups. Furthermore, in patients without stage progression, the use of curative treatments—whether as initial or subsequent interventions—was consistently associated with better outcomes.
These findings suggest that, in addition to baseline patient characteristics that are non-modifiable at the time of diagnosis, several modifiable factors—including the choice of treatment modality, therapeutic efficacy, and early detection of recurrence—play a critical role in determining long-term prognosis. These are areas in which clinical decision-making and treatment strategies can meaningfully influence patient outcomes.
Data Sharing Statement
All analyzed data are included in this published article. The original data are available upon reasonable request from the corresponding author.
Statement of Ethics
This retrospective cohort study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (IRB) of Chang Gung Memorial Hospital, Chiayi Branch (IRB No.: 202500300B0). The study protocol involved analysis of anonymized medical records collected through routine clinical care, without direct patient contact or intervention. Based on the IRB’s assessment, the study qualified for expedited review and was granted a waiver of informed consent due to its retrospective nature and minimal risk to participants. The IRB confirmed that no identifiable patient information would be disclosed and that the confidentiality of the data was strictly protected throughout the study.
Acknowledgments
We sincerely thank the Cancer Center, Chiayi Chang Gung Memorial Hospital, for their support and assistance in this study.
Funding
This study was not supported by any sponsor or funder.
Disclosure
The authors declare no competing interests.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
2. Ministry of Health and Welfare. Cancer Registry Annual Report; 2023. Available from: https://www.mohw.gov.tw/cp-16-79055-1.html.
3. Sangro B, Argemi J, Ronot M, et al. EASL clinical practice guidelines on the management of hepatocellular carcinoma. J Hepatol. 2024. doi:10.1016/j.jhep.2024.08.028
4. Tandon P, Garcia‐Tsao G. Prognostic indicators in hepatocellular carcinoma: a systematic review of 72 studies. Liver Int. 2009;29(4):502–510. doi:10.1111/j.1478-3231.2008.01957.x
5. Kuo MJ, Mo LR, Chen CL. Factors predicting long-term outcomes of early-stage hepatocellular carcinoma after primary curative treatment: the role of surgical or nonsurgical methods. BMC Cancer. 2021;21:1–14. doi:10.1186/s12885-021-07948-9
6. Sarveazad A, Agah S, Babahajian A, Amini N, Bahardoust M. Predictors of 5 year survival rate in hepatocellular carcinoma patients. J Res Med Sci. 2019;24(1):86. doi:10.4103/jrms.JRMS_1017_18
7. Zhu S-L, Yang K, Peng Y-C, et al. Comparison of long-term survival of patients with solitary large hepatocellular carcinoma of BCLC stage A after liver resection or transarterial chemoembolization: a propensity score analysis. PLoS One. 2014;9(12):e115834. doi:10.1371/journal.pone.0115834
8. Sempokuya T, Wong LL. Ten-year survival and recurrence of hepatocellular cancer. Hepatoma Res. 2019;5(38). doi:10.13105/wjma.v11.i2.47
9. Wu K-T, Wang C-C, Lu L-G, et al. Hepatocellular carcinoma: clinical study of long-term survival and choice of treatment modalities. World J Gastroenterol. 2013;19(23):3649. doi:10.3748/wjg.v19.i23.3649
10. Yang W, Yan K, Nahum Goldberg S, et al. Ten-year survival of hepatocellular carcinoma patients undergoing radiofrequency ablation as a first-line treatment. World J Gastroenterol. 2016;22(10):2993. doi:10.3748/wjg.v22.i10.2993
11. Farinati F, Sergio A, Baldan A, et al. Early and very early hepatocellular carcinoma: when and how much do staging and choice of treatment really matter? A multi-center study. BMC Cancer. 2009;9:1–12. doi:10.1186/1471-2407-9-33
12. Yeh J-H, Hung C-H, Wang J-H, et al. Modifiable prognostic factors of hepatocellular carcinoma in patients with non-surgical treatment. PLoS One. 2015;10(12):e0144893. doi:10.1371/journal.pone.0144893
13. Galle PR, Forner A, Llovet JM, et al. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236.
14. Changchien C-S, Chen C-L, Yen Y-H, et al. Analysis of 6381 hepatocellular carcinoma patients in southern Taiwan: prognostic features, treatment outcome, and survival. J Gastroenterol. 2008;43:159–170. doi:10.1007/s00535-007-2134-9
15. Kew MC. Hepatocellular carcinoma: epidemiology and risk factors. J Hepatocell Carcinoma. 2014;1:115–125. doi:10.2147/JHC.S44381
16. Hartke J, Johnson M, Ghabril M. The diagnosis and treatment of hepatocellular carcinoma. Semin Diagn Pathol. 2017;34(2). doi:10.1053/j.semdp.2016.12.011
17. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. doi:10.1016/j.jhep.2021.11.018
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.