Back to Journals » Infection and Drug Resistance » Volume 19
Profile of Biofilm Formation and Antimicrobial Susceptibility Patterns of Escherichia coli Isolated from Adult Patients Presenting with Urinary Tract Infections at Ruhengeri Level Two Teaching Hospital, Rwanda
Authors Mukashema H ![]() , Yadufashije C
, Yadufashije C ![]() , Tuyishimire A, Imurinde Y, Rugira Niyonkuru B
, Tuyishimire A, Imurinde Y, Rugira Niyonkuru B ![]() , Muhimpundu L, Nshimiyimana A, Musabyumuremyi C, Muhizi E
, Muhimpundu L, Nshimiyimana A, Musabyumuremyi C, Muhizi E ![]() , Muhire P, Habyarimana T
, Muhire P, Habyarimana T
Received 10 August 2025
Accepted for publication 26 January 2026
Published 18 February 2026 Volume 2026:19 559490
DOI https://doi.org/10.2147/IDR.S559490
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sandip Patil
Hyacinthe Mukashema,1 Callixte Yadufashije,1 Aphrodice Tuyishimire,2 Yoranda Imurinde,1 Bruno Rugira Niyonkuru,1 Liliane Muhimpundu,3 Alex Nshimiyimana,1 Celestin Musabyumuremyi,1 Epaphrodite Muhizi,4 Philbert Muhire,4 Thierry Habyarimana1
1Department of Biomedical Laboratory Sciences, INES-Ruhengeri, Musanze, Rwanda; 2Department of Public Health, ICAP at Columbia University, Kigali, Rwanda; 3Department of Medical Microbiology, Jomo Kenyatta University of Agriculture and Technology, Nairobi, Kenya; 4Department of Internal Medicine, Ruhengeri Level Two Teaching Hospital, Musanze, Rwanda
Correspondence: Hyacinthe Mukashema, Department of Biomedical Laboratory Sciences, INES-Ruhengeri, P.O. Box 155, Musanze, Rwanda, Tel +250785007620, Email [email protected]
Background: Urinary tract infections (UTIs) are a public health concern worldwide, with Escherichia coli (E. coli) being the primary cause. Biofilm-forming E. coli increases bacterial resistance to antibiotics, leading to significant morbidity and mortality among patients with UTIs. This study was conducted to determine biofilm formation potential and assess antimicrobial susceptibility patterns of E. coli isolated from adults with suspected UTIs attending Ruhengeri Level Two Teaching Hospital (RLTTH), Rwanda.
Methods: A cross-sectional laboratory-based study was conducted between April and June 2025 on 151 adults with suspected UTIs. A questionnaire was used to record sociodemographic characteristics and risk factors contributing to UTIs among the participants. Midstream urine samples were collected, cultured, and biochemically analyzed to identify E. coli in urine samples. Antimicrobial susceptibility profiles were determined using the disc diffusion method. Biofilm production in E. coli isolates was detected using Congo Red Agar (CRA) method.
Results: Of 151 adults, 64.2% were female and 35.8% male, and the majority of participants were in the age group of 29– 39 years (34.4%). E. coli accounted for 37/151 (24.5%) isolates, of which 16 (43.2%) were confirmed biofilm producers. High resistance was observed for amoxicillin (100%), trimethoprim-sulfamethoxazole (93.8%), nitrofurantoin (87.5%), ampicillin (87.5%), cefixime (56.2%), gentamycin (50%), and ceftazidime (37.5%). Ciprofloxacin and meropenem were effective. Age was the only risk factor associated with biofilm production by E. coli in the study population (p = 0.000).
Conclusion: This study highlights the critical role of E. coli in biofilm production in adults with UTI at RLTTH. A high prevalence of drug resistance was observed among biofilm-producing strains. Intervention strategies, such as frequent biofilm screening, continuous surveillance, and enhanced antimicrobial stewardship programs, are needed.
Keywords: UTIs, E. coli, biofilm-producing strains, antimicrobial resistance, Rwanda
Introduction
Urinary tract infections (UTIs) affect approximately 150 million people globally each year, ranking among the most common infections in primary care.1 UTIs occur when pathogenic bacteria invade and multiply in the urinary tract, disrupting normal kidney and urinary function.2 Although they affect individuals of all ages and sexes, women are disproportionately affected due to anatomical differences such as a shorter urethra.3 Multiple risk factors have been identified, including age, sex, race, circumcision status, HIV, diabetes, catheterization, anatomical abnormalities, pregnancy, and hospitalization.4
Bacteria associated UTI is the second leading cause of illness and the most prevalent worldwide.2 Between 20% and 50% of patients present repeated infections, while between 50% and 80% of people, particularly women, get UTIs at some point in their life every year, almost 150 million people globally receive a UTI diagnosis, which costs more than 6 billion dollars across all age categories.5 Globally, according to estimates, UTIs cause up to 8.3 million visits to outpatient treatment centers, 1 million to emergency department, and 100,000 hospital admissions yearly.6
In developing countries, the study done in Uganda revealed a prevalence rate of UTIs at 32.2% with E. coli being the most prevalent bacterial uropathogen at 41.9%.7 The overall incidence of UTIs considering a study carried in Ethiopia was 90.1% and the mostly isolated uropathogen being E. coli (39.3%).8 Another research carried out in Kenya indicated a prevalence of UTIs that was 54.1%.9
E. coli, a gram-negative enteric bacterium, is the predominant uropathogen accounting for 80–90% of community-acquired and 30–50% of hospital-acquired UTIs.10 Uropathogenic Escherichia coli (UPEC) causes bladder infections by attaching and entering epithelial cells through type 1 and P pili, thus obtaining the property of resisting urine flow and host mechanisms of defence. The UPEC adherence may then build biofilms and intracellular bacterial communities that protect them from the effects of antibiotics and the immune response leading to recurrent or chronic infections.11 In addition, the bacteria produce capsules, siderophores and a variety of toxins all of which assist them in causing tissue injury, obtaining nutrients and survival in the urinary tract. Finally, many UPEC also carry antibiotic resistance genes which complicate therapy and increase recurrence rates.12
One of the most troubling factors relevant to UTI management has been the rising reports of antimicrobial resistance (AMR) from uropathogens.13 One way E. coli can resist antibiotics is by using biofilm formation as a survival mechanism; biofilms protect bacteria within an extracellular matrix and allow them to escape immune responses and antibiotics.14,15 Biofilms are highly organized, three-dimensional communities of microorganisms encased in a self-produced extracellular polymeric substance (EPS) matrix, able to stick to both inert surfaces and biological tissues.16 Biofilm EPS physically limits antibiotic penetration and creates microenvironments including nutrient/oxygen gradients that drive slower growth and phenotypic tolerance (persister cells), which protects bacteria from host defenses and antibiotics thereby contributing to therapeutic failure.17 Moreover, biofilms enhance co-selection of resistance integrons, plasmids, and horizontal gene transfer, contributing to the sustained spread of antimicrobial resistance in UPEC.18 Biofilm-embedded bacteria can have resistance 100–1000 times higher than their free-living counterparts.16 This resistance leads to persistent and recurrent infections, making E. coli an important target for UTI control.10,19
The prevalence rate of E. coli-related UTIs varies between 20% and 40% globally. In Africa, strains often show high levels of biofilm production and antibiotic resistance, with multidrug resistance (MDR) rates ranging from 50% to 80%.20 In Eastern Africa, challenges such as limited diagnostic capacities and inconsistent antibiotic stewardship further complicate the management. For instance, a study in Tanzania reported E. coli in 47% UTI cases, with over 85% of isolates resistant to ampicillin and co-trimoxazole, and 51.5% exhibiting a biofilm-forming ability.21 Similarly, research in Uganda revealed that 62.5% of uropathogenic E. coli were biofilm producers, with 78% showing MDR, especially against amoxicillin, trimethoprim-sulfamethoxazole, and gentamicin.19 In Rwanda, reports on antimicrobial resistance trends show that resistant pathogens are becoming a bigger problem in the nation.22 According to recent studies, AMR, especially in Gram-negative bacteria like E. coli and Klebsiella species, is a growing public health concern in Rwanda. Available evidence shows that Rwanda has a significant AMR burden with patterns comparable to neighboring East African countries however comparisons are limited by heterogenous surveillance coverage, variable study settings and methodologies.23 Most of these infections are still susceptible to amikacin and carbapenems, but they frequently show resistance to fluoroquinolones and third-generation cephalosporins. Between 2020 and 2024, hospital-based surveillance found a significant frequency of isolates that produced extended-spectrum β-lactamase (ESBL) and were resistant to many drugs, making empirical therapy more difficult.24 In response, Rwanda has put its National Action strategy on AMR (2020–2024) into action and has created a new strategy for 2025–2029 that focuses on boosting laboratory capacity, One Health surveillance, and antibiotic stewardship. Effective AMR management is still hampered by inadequate diagnostic infrastructure and unreliable reporting.25 However, to the best of our knowledge, the relationship with biofilm production has not yet been investigated. This study aimed to assess the biofilm formation potential and antimicrobial susceptibility profiles of E. coli isolated from adults with suspected UTIs attending the Ruhengeri Level Two Teaching Hospital (RLTTH), Rwanda.
Materials and Methods
Study Design and Study Population
This cross-sectional study was conducted between April and June 2025 at RLTTH, located in Musanze City, Northern Province, Rwanda. RLTTH is a major referral and training health facility that serves several hundred thousand people in Musanze and neighboring districts around. The hospital started in 1939 and has 320 beds though it is continuously growing at an unprecedented rate to attain 550 beds. It provides comprehensive medical, surgical, maternity, and teaching services. Using convenience sampling method, a total of 151 participants above 18 years of age who were suspected of having UTIs experiencing UTI-like symptoms, such as back pain, frequent urination, abdominal pain or a burning sensation when urinating were recruited. All participants, including hospitalized and non-hospitalized patients, provided signed informed consent and midstream urine specimens were collected from each consenting participant. Participants who had undergone antibiotic treatment were excluded from the study. This study was approved by both INES-Ruhengeri and RLTTH (Ref 369/ RL2TH/ DG/2025). However, Data confidentiality and right to privacy were respected in compliance with the declaration of Helsinki.
Urine Culture and Bacterial Identification
Approximately 10 μL of urine samples were inoculated on MacConkey agar and Cystine lactose electrolytedeficient (CLED) agar media using a sterile calibrated plastic loop and incubated for 18–24 hours at 37°C. Based on colony characteristics, MacConkey agar plates revealed smooth round pink (lactose fermenting) colonies while yellow, spherical, smooth and moist colonies were observed on CLED agar plates with a colony count of bacterial growth greater than 105 Colony Forming Units (CFU)/mL considered as significant UTI cases. Microscopic identification after Gram staining showed short gram negative (red) rods, and biochemical tests including Triple sugar Iron (TSI) test, citrate utilization test, Sulfide Indole Motility (SIM) test, urease test, Methyl Red (MR) test, Voges-Proskauer (VP) test were performed for identification and confirmation of bacterial isolates.26
Detection of Biofilm Formation and Antimicrobial Susceptibility Testing
Phenotypic biofilm production was assessed using the Congo Red Agar (CRA) method. CRA medium was prepared using brain-heart infusion (BHI) agar (52 g/L), sucrose (50 g/L), and Congo Red (8 g/L). The CRA medium was prepared by mixing BHI agar with sucrose in 800 mL of distilled water in one container, and Congo red stain was prepared in another container as a concentrated aqueous solution (8 g in 200 mL of distilled water) and autoclaved (121°C for 15 minutes) separately from the other medium constituents. It was later added to BHI medium mixed with sucrose after cooling at 55°C, pooled into sterile Petri dishes, and allowed to solidify. The prepared CRA plates were later inoculated with E. coli isolates and incubated at 37°C for 24 hours under aerobic conditions. E. coli colonies showing a black dry crystal-like consistency were considered biofilm-formers. Colonies that retained a smooth red color were identified as non-biofilm- formers. E. coli ATCC 25922 and Staphylococcus aureus ATCC 25932 were used as the positive and negative controls, respectively. In addition, results were interpreted independently by multiple observers.
Antibiotic sensitivity tests were performed on pure isolates following the Kirby-Bauer disc diffusion method on Mueller Hinton agar as suggested by Clinical Laboratory Standards Institute (CLSI) guidelines. Antibiotics tested for included the commonly used antimicrobial agents: cefixime (5µg), ceftazidime (30µg), amoxicillin (25µg), ciprofloxacin (5µg), amoxicillin/clavulanic acid (30 µg), meropenem (10µg), nitrofurantoin (100µg), trimethoprim-sulfamethoxazole (25 µg), gentamycin (10 μg), and ampicillin (10 µg).19 E. coli ATCC 25922 was used as a positive reference strain and susceptibility interpretations were carried out following CLSI guidelines. Raw data for demographic characteristics, bacterial isolates, antimicrobial susceptibility and biofilm formation results are provided in Supplementary Table S1.
Statistical Analysis
Clinical and demographic information was obtained using a data collection questionnaire. Data were analyzed using SPSS version 21. The chi-square statistical test was used to determine the association of risk factors with biofilm production status, with significance set at p < 0.05.
Results
Demographic Characteristics of Study Participants
As shown in Table 1, the majority of participants were in the age category of 29–39 (34.4%), and female participants (64.2%) were more prevalent than males (35.8%). A large number of study participants had primary education (36.4%), and the majority of study participants were married (69.5%).
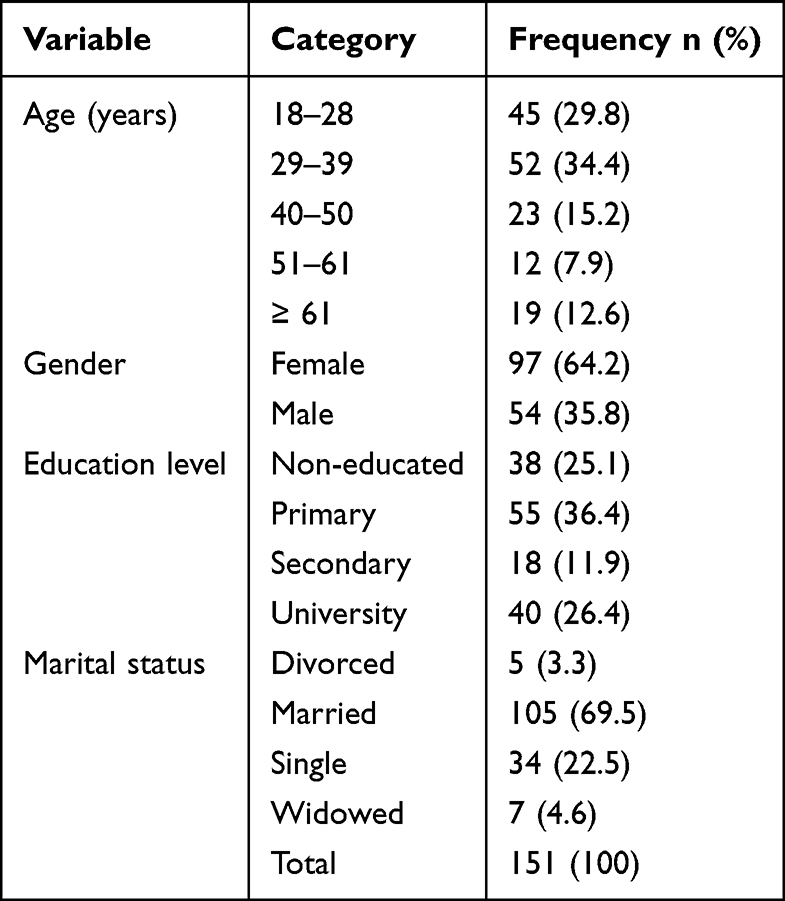 |
Table 1 Socio-Demographic Characteristics of Study Participants |
E. Coli Biofilm Production Rate
Out of 151 examined urine specimens, 37 (24.5%) had E. coli, 94 (62.25%) had no growth, while other bacteria formed the remaining 20 (13.24%). The identified 37 (24.5%) E. coli were then subjected to biofilm production detection using the CRA method. Nearly half (43.2%) of the E. coli isolates were able to form biofilms (Table 2).
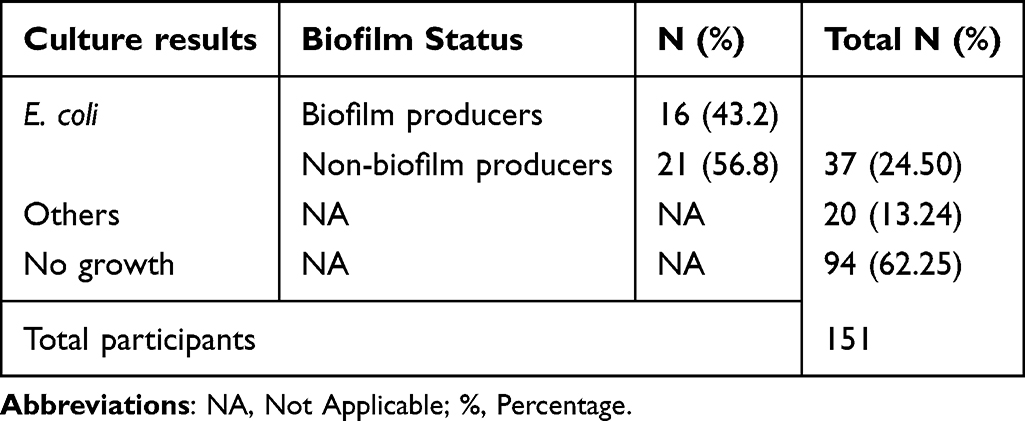 |
Table 2 Biofilm Production Rate of E. Coli Isolated from Patients at RLTTH |
Antimicrobial Susceptibility Profile of Biofilm and Non-Biofilm Producing E. Coli
In this study, antimicrobial susceptibility testing was performed on all 37 E. coli isolates by using antibiotic discs, as shown in Figure 1. Biofilm producing isolates showed very high resistance rates to commonly used antibiotics, including amoxicillin (100%), trimethoprim-sulfamethoxazole (93.8%), ampicillin (87.5%), and nitrofurantoin (87.5%), compared with non-biofilm-forming strains, with 76.19%, 47.61%, 76.19%, and 66.66%, respectively. Meropenem as well as ciprofloxacin showed 100% susceptibility in both biofilm and non-biofilm groups, highlighting their effectiveness in UTI treatments.
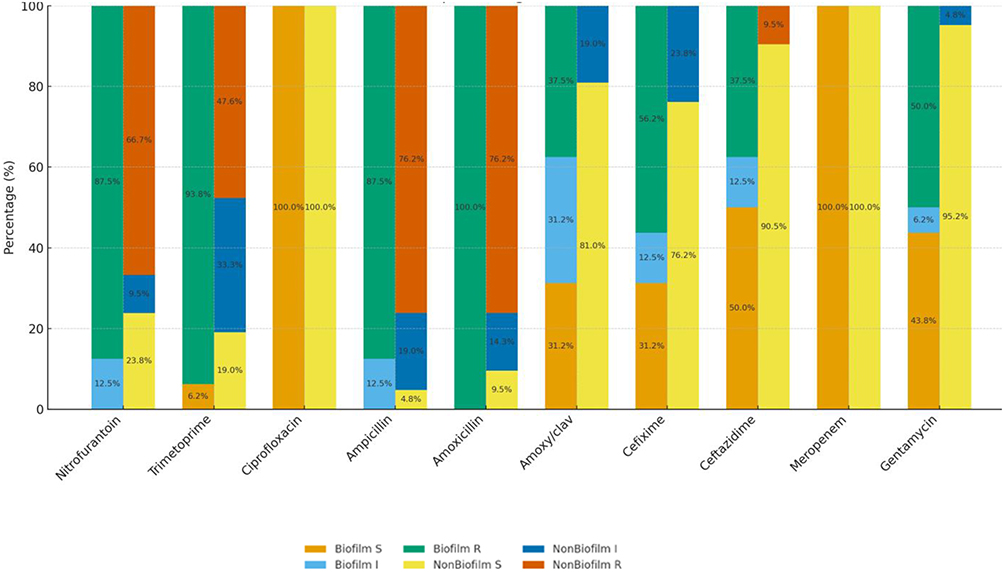 |
Figure 1 Antimicrobial susceptibility profile of biofilm and non-biofilm producing E. coli. Abbreviations: I, Intermediate; R, Resistant; S, Sensitive. |
Risk Factors Associated with Biofilm-Production in E. Coli Among Patients at RLTTH
Biofilm formation in E. coli among patients with UTI was evaluated in relation to demographic and clinical factors, including age, sex, marital status, previous history of UTIs, underlying (chronic) conditions, hospitalization, catheter use, use of antiseptics in genital organs, and pregnancy. As shown in Table 3, the association between biofilm formation by E. coli and various patient-related risk factors revealed that only age (p = 0.000) showed a statistically significant association with biofilm formation, suggesting a demographic influence on the prevalence of biofilm-producing strains. Adult patients ≥62 years had the highest proportion of biofilm producing infections (43.75%), compared to only 14.28% in the same group without biofilm production. The majority of factors did not show any statistical significance, but some trends were noteworthy because patients with a history of UTIs, for instance, had a higher percentage of biofilm-positive cases (31.25%) than biofilm-negative cases (14.28%).
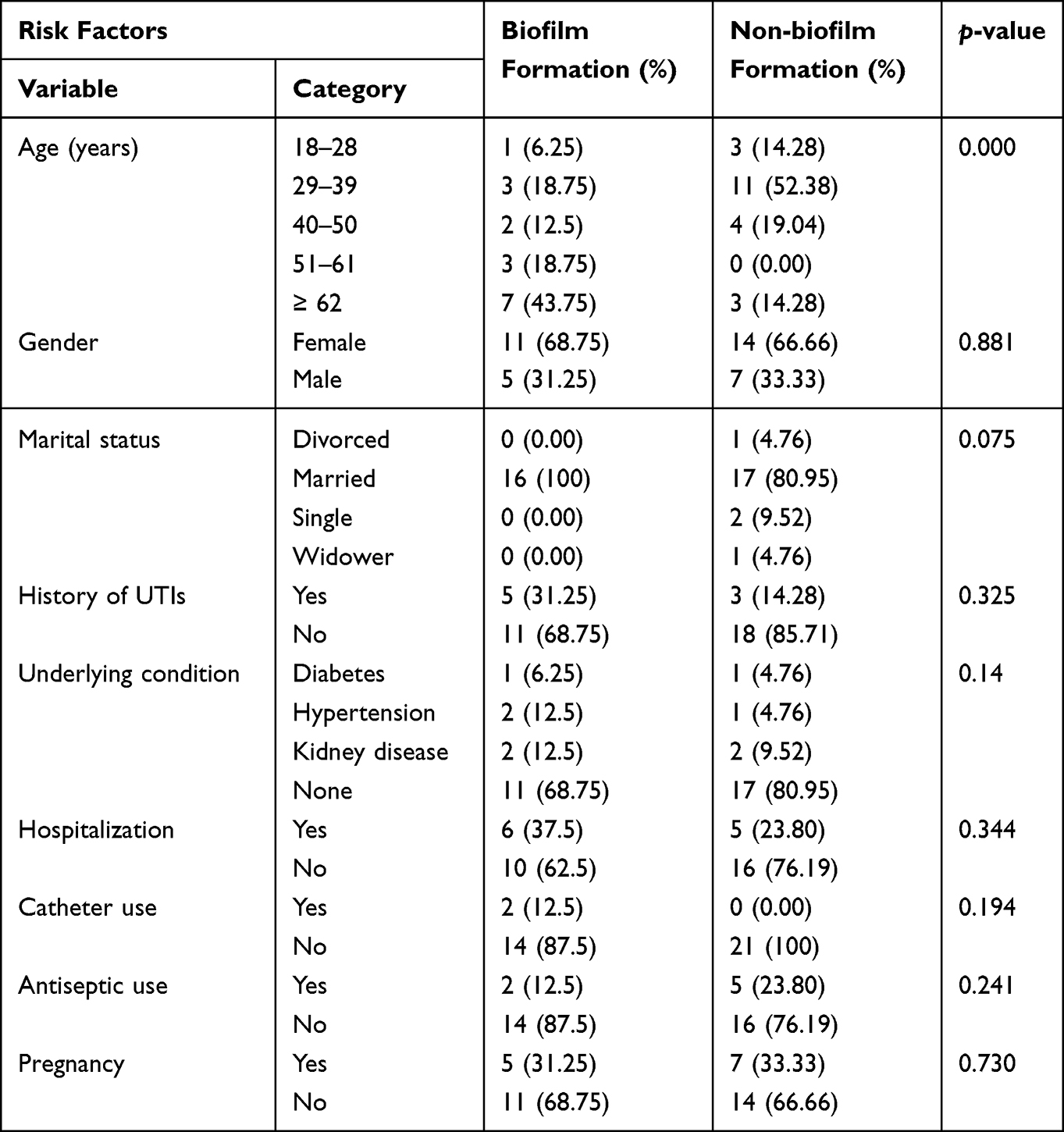 |
Table 3 Risk Factors Associated with Biofilm-Production in E. Coli Among Adult Patients |
Discussion
Biofilm-forming bacteria are a predominant cause of complicated and recurrent UTIs, which are associated with MDR microorganisms.19 E. coli is one of the species most commonly implicated in biofilm-associated infections and plays a significant role in UTIs. The emergence and spread of antimicrobial resistance, particularly in bacteria, are currently regarded as a major global health risk. Bacteria living in biofilms can resist antibiotics up to several times compared to their free-living counterparts and can evade the host’s immune response. Treatment of biofilm-related infections is therefore extremely challenging.16 To our knowledge, this is the first study in Rwanda to assess the profile of biofilm formation and antimicrobial susceptibility patterns of E. coli among adults with suspected UTI.
In this study, the majority of participants were in the age category of 29–39 (34.4%). This age group is frequently linked to increased UTI risk because of increased sexual activity and reproductive health factors.7,27 Adults ≥61 years (12.6%) are less common but still clinically significant because comorbidities like diabetes, hypertension and kidney diseases can alter UTI presentation and outcomes.
Nearly two-thirds (64.2%) of participants were female (Table 3), which is in line with findings from Al-Gasha’a et al,28 and related literature reflects the well-established greater UTI susceptibility in women associated with anatomical and behavioral factors. Studies have emphasized the contribution of social determinants in UTIs.29 The varied education profile (primary 36.4%), university (26.4%), and non-educated (25.1%) indicates varying levels of hygiene awareness, health-seeking behavior, and antibiotic use.
While the single (22.5%) and widowed (4.6%) groups offer comparative strata for behavioral and exposure differences, the vast majority were married (69.5%), which is in line with a study showing that sexual activity within stable marriages was linked to UTI risk.30 Overall, the demographic profile supports prior research showing that UTI risk is influenced by age, female gender, education, and marital/behavioral characteristics in a variety of contexts.31,32
The study results indicated that E. coli was responsible for 37 (24.50%) of the UTIs observed among adult patients at RLTTH, which supports the worldwide finding that E. coli remains the most common causative organism of UTIs. The prevalence of E. coli noted in this study was higher than the 13.3% reported by Chelangat et al18 but lower than the 33.33% and 47% reported by Al-Gasha’a et al17 and Mlugu et al,12 respectively. Such variability could be due to differences in the local healthcare systems, diagnostic methods, and populations. Odoki et al16 and Gbadamosi15 mentioned that its prevalence was also dependent on age, sex, catheter use, diabetes, and poor hygiene.
The observed high “No growth” rate could be due to previous antibiotic use, low bacterial loads, or non-bacterial causes, factors which can lower culture positivity. Despite these variations, E. coli continues to be the most common cause of UTIs because of its virulence characteristics, including biofilm formation and resistance to host defenses, which enhance its survival and colonization of the urinary tract.19
Biofilm formation in E. coli among UTI patients is still a major clinical concern, and there is high variation in biofilm production worldwide. Among 37 isolated E. coli subjected to biofilm production, 16 (43.2%) of them were biofilm producers and 21 (56.8%) were non-biofilm producers. This showed that nearly half of the E. coli isolates could form biofilms, underscoring the importance of biofilm formation as a major virulence factor in UTIs. The biofilm production rate in this study was lower compared to that reported in other regions, such as the studies done in Egypt33 and Uganda,19 with 58.5% and 62.5%, respectively.
This finding is also relatively lower than the results reported in Indonesia,34 Iran,26 and Ethiopia,35,36 with 83.3%, 72.8%, and 85.3%, respectively. These differences across studies may be due to population demographics, variation in biofilm detection methods, sample size or the geographical location of the clinical settings.
When compared to similar studies, the biofilm production rate of 43.2% in this present study is consistent with findings from global reports, which indicates that Uropathogenic E. coli (UPEC) biofilm production varies globally between 13.3% and 99%.33 These results are in line with a study done in India which showed a biofilm production proportion of 49%.37 Similar results were obtained in Egypt,38 Hungary39 and Tanzania,21 with 45.5%, 47,6% and 51.5%, respectively.
The discovery of antibiotics was crucial in the twentieth century for the treatment of microbial diseases, and, in recent decades, antimicrobial resistance brought on by the wide range of antibiotics available for use as well as their abuse and overuse has posed a global public health concern for health systems.1 In this study, the antimicrobial susceptibility profile of all E. coli isolates was carried out on biofilm-producing and non-biofilm-producing E. coli. The biofilm-producing isolates exhibited higher resistance rates to amoxicillin (100%), trimethoprim-sulfamethoxazole (93.75%), nitrofurantoin (87.5%), and ampicillin (87.5%), with no susceptible strains, followed by cefixime (56.25%), gentamycin (50%), ceftazidime (37.50%), and amoxicillin/clavulanic acid (37.50%). This study emphasizes the role of biofilm formation in antimicrobial resistance.
Similar findings were reported in Tanzania where all isolated strains had maximum resistance to cotrimoxazole and ampicillin; indicating that the medications may be less effective at treating UTIs and should be given less consideration in the treatment plan.21 By generating protective extracellular matrices that prevent antibiotic penetration and host immunological clearance, biofilm development increases E. coli’s ability to survive in harsh environments, such as bladder epithelium and urinary catheters.14 This is consistent with the widely accepted theory that biofilms serve as a barrier of defense, preventing the penetration of antibiotics and promoting horizontal gene transfer.21
While remaining resistant, non-biofilm strains showed partial susceptibility to certain treatments (19.04% to trimethoprim, 23.8% to nitrofurantoin), indicating reduced but not completely lost of treatment options. The reduced susceptibility of non-biofilm strains may be due to the availability of resistance markers other than biofilms, such as Extended Beta-lactamase enzymes. Additionally, biofilm-producing UPEC showed significantly lower susceptibility rates to cephalosporins, such as cefixime, ceftazidime, and β-lactam/β-lactamase inhibitor combinations (amoxicillin/clavulanic acid) than non-biofilm strains, which is in line with the findings of Alshaikh et al38 and Abo-alella et al,33 who suggested that the decreased cephalosporin efficacy against E. coli embedded in biofilms is probably due to modified porin expression or beta-lactamase concentration in the biofilm matrix.
Interestingly, both biofilm and non-biofilm isolates were 100% susceptible to ciprofloxacin and meropenem, regardless of biofilm status showing that fluoroquinolones and carbapenems remain highly efficient against these isolates. This could be attributed to their ability to penetrate biofilms or to target active bacterial functions. However, care must be taken because biofilms can promote biofilm-specific resistance that does not always correlate with planktonic minimum inhibitory concentration (MIC) values, according to Ballén et al16 and Behzadi et al,39 whose studies highlighted that biofilm-mediated protection may still result in treatment failure.
In comparison to non-biofilm strain’s susceptibility (95.25%), gentamicin was significantly less effective against biofilm isolates (43.75% susceptibility). This is consistent with findings on biofilm-induced aminoglycoside resistance.40,41 These results underline the necessity for cautious antibiotic selection and resistance monitoring as well as the obstacle biofilms present in the successful treatment of UTIs. Although most isolates have significant levels of resistance to several antibiotics, biofilm-forming organisms had higher MDR rates (defined as resistance to at least three antibiotics of different classes) than non-biofilm-forming organisms. These findings were consistent with the hypothesis that biofilms are associated with increased antibiotic resistance. These findings are in line with a study carried out in Australia that noted that biofilm forming UPEC strains exhibited higher levels of drug resistance than non-biofilm isolates.42 Similar findings were reported in Uganda, where resistance to various antibiotics was observed among E. coli isolates; biofilm producing strains appeared to have more MDR (64%) compared to non-biofilm producers.19
The present study demonstrated that biofilm formation by E. coli is significantly associated with age (p = 0.000), emphasizing the influence of advanced age on the prevalence of biofilm production. Patients ≥62 years of age had the highest rate of biofilm-positive infections (43.75%) compared to 14.28% in the biofilm-negative group. This is in line with the studies of Abo-alella et al33 and Ballén et al,16 which indicates that comorbidities, frequent hospital exposure, and age-related immunosenescence make advanced age a risk factor for biofilm-forming E. coli. Gunardi et al34 further highlighted that older patients are at a higher risk of biofilm formation because they are more likely to require longer hospital stays, repeated antibiotic exposure, and catheterization.
Females were more frequently affected in both the biofilm and non-biofilm formation groups, which is consistent with global epidemiological reports.2,43 However, sex was not significantly associated (p = 0.881). The shorter female urethra makes it easier for germs to ascend and facilitates colonization. Marital status revealed that all biofilm-positive patients were married despite the non-significant association (p = 0.075). As Demir et al44 noted in their social determinant discussions, this may reveal socio-behavioral or co-habitation hygiene behaviors impacting UTI exposure, although the direct biological link is not well known.
Although their greater proportions in the biofilm-positive group suggest potential therapeutic relevance, the history of UTIs and the presence of underlying diseases such as diabetes, hypertension, and renal disease were not statistically significant. Diabetes and renal impairments have been shown to compromise immunological defenses, increasing bacterial survival and biofilm development.35,39
The study did not show any statistically significant association between hospitalization and catheter use (p = 0.344 and p = 0.194, respectively) and biofilm formation; however, they were more prevalent in the group that produced biofilms. This is clinically significant given that biofilm formation is frequently linked to nosocomial infections and foreign body insertion. According to Abo-alella et al33 and Katongole et al19 catheter-associated UTIs are particularly susceptible to biofilm-forming E. coli, making them more difficult to treat and frequently multidrug-resistant.
Patients in the biofilm-negative group were more likely to use antiseptics (23.80%) than those in the biofilm-positive group (12.5%) (p = 0.241), which may indicate that antiseptic hygiene helps prevent the production of biofilms. This confirms the results of studies demonstrating that good hygiene practices lower the risk of resistance development and chronic colonization.14,38
Pregnancy is a known risk factor for UTIs, although biofilm-specific connections are still unknown and may be influenced by immunological modulation and gestational age.45,46 There was no significant difference in pregnancy (p = 0.730), but the proportions in the biofilm and non-biofilm groups were comparable.
Conclusion
The current study showed that E. coli was significantly present (24.5%) in adults with UTI at RLTTH, and nearly half (43.2%) of the isolates had the ability to form biofilms. The high prevalence of drug resistance to amoxicillin, trimethoprim-sulfamethoxazole, nitrofurantoin, ampicillin, cefixime, gentamycin, ceftazidime, and amoxicillin/clavulanic acid makes the treatment of these infections challenging, especially among biofilm producers. Age and biofilm production were significantly correlated, indicating that certain age groups were more vulnerable to chronic or difficult-to-treat UTIs. These results have significant implications for regional and local infection control highlighting the critical and immediate need for age-specific intervention strategies, implementation of appropriate antibiotic stewardship initiatives and regular biofilm screening protocols in laboratory workflows where capacity allows so as to tackle effectively antimicrobial resistance issues.
Of important note, this study was limited to the use of CRA only as a biofilm detection method which is simple, less sensitive and prone to subjectivity but cost-effective and suitable for resource-limited laboratory settings compared to highly sensitive and quantitative methods such as Microtiter plate assays and molecular detection methods that could come up with much more significant results. On the other side, the small sample size may have affected the statistical power leading to lack of statistical significance in some variables. Future studies with larger sample sizes and improved methodologies are recommended.
Data Sharing Statement
The original data for this study are available from the corresponding author upon request and will be freely accessible to scientists who may need to use them for non-commercial reasons, without violating the confidentiality of the participants.
Acknowledgments
We express our sincere gratitude to the staff of INES-Ruhengeri and RLTTH for their valuable support and collaboration. We also express our sincere gratitude to each study participant for their agreement to participate. Their assistance was crucial for the conclusions of this study.
Disclosure
The authors declare that there is no conflict of interest in this study.
References
1. Muhimpundu L, Mabeya S, Mwaniki JN, Miringu G, Ngugi C. Prevalence, antimicrobial resistance patterns and ESBL resistance genotypes of Klebsiella pneumoniae Isolated from patients presenting with urinary tract infections at Mama Lucy Hospital, Kenya. IP Int J Med Microbiol Trop Dis. 2024;10(4):416–11. doi:10.18231/j.ijmmtd.2024.068
2. Zeng Z, Zhan J, Zhang K, Chen H, Cheng S. Global, regional, and national burden of urinary tract infections from 1990 to 2019: an analysis of the global burden of disease study 2019. World J Urol. 2022;40(3):755–763. doi:10.1007/s00345-021-03913-0
3. Kaur R, Kaur R. Symptoms, risk factors, diagnosis and treatment of urinary tract infections. Postgrad Med J. 2021;97(1154):803–812. doi:10.1136/postgradmedj-2020-139090
4. Rozwadowski M, Gawel D. Molecular factors and mechanisms driving multidrug resistance in uropathogenic Escherichia coli—an update. Genes (Basel). 2022;13(8):1397. doi:10.3390/genes13081397
5. Zhao F, Yang H, Bi D, Khaledi A, Qiao M. A systematic review and meta-analysis of antibiotic resistance patterns, and the correlation between biofilm formation with virulence factors in uropathogenic E. coli isolated from urinary tract infections. Microb Pathog. 2020;144(April):104196. doi:10.1016/j.micpath.2020.104196
6. John AS, Mboto CI, Agbo B. A review on the prevalence and predisposing factors responsible for urinary tract infection among adults. Euro J Exp Bio. 2016;6(4):7–11.
7. Odoki M, Aliero AA, Tibyangye J, et al. Prevalence of bacterial urinary tract infections and associated factors among patients attending hospitals in Bushenyi District, Uganda. Int J Microbiol. 2019;2019:1–8. doi:10.1155/2019/4246780
8. Seifu WD, Gebissa AD. Prevalence and antibiotic susceptibility of Uropathogens from cases of urinary tract infections (UTI) in Shashemene referral hospital, Ethiopia. BMC Infect Dis. 2018;18(1):1–9. doi:10.1186/s12879-017-2911-x
9. Kiiru S, Maina J, Katana J, et al. Bacterial etiology of urinary tract infections in patients treated at Kenyan health facilities and their resistance towards commonly used antibiotics. PLoS One. 2023;18(5 May):1–14. doi:10.1371/journal.pone.0277279
10. Ramírez Castillo FY, Guerrero Barrera AL, Harel J, et al. Biofilm formation by Escherichia coli isolated from urinary tract infections from Aguascalientes, Mexico. Microorganisms. 2023;11(12):1–18. doi:10.3390/microorganisms11122858
11. Nasi GI, Georgakopoulou KI, Theodoropoulou MK, et al. Bacterial Lectin FimH and its aggregation hot-spots: an alternative strategy against uropathogenic Escherichia coli. Pharmaceutics. 2023;15(3):1018. doi:10.3390/pharmaceutics15031018
12. Li ZP, Li J, Li TL, Song ZY, Gong X. Uropathogenic Escherichia coli infection: innate immune disorder, bladder damage, and Tailin Fang II. Front Cell Infect Microbiol. 2024;(April):1–16. doi:10.3389/fcimb.2024.1322119
13. Bunduki GK, Heinz E, Phiri VS, Noah P, Feasey N, Musaya J. Virulence factors and antimicrobial resistance of uropathogenic Escherichia coli (UPEC) isolated from urinary tract infections: a systematic review and meta-analysis. BMC Infect Dis. 2021;21(1):1–13. doi:10.1186/s12879-021-06435-7
14. Qian W, Li X, Yang M, et al. Relationship between antibiotic resistance, biofilm formation, and biofilm-specific resistance in Escherichia coli isolates from Ningbo, China. Infect Drug Resist. 2022;15:2865–2878. doi:10.2147/IDR.S363652
15. Wang X, Liu M, Yu C, Li J, Zhou X. Biofilm formation: mechanistic insights and therapeutic targets. Mol Biomed. 2023;4(1). doi:10.1186/s43556-023-00164-w
16. Ballén V, Cepas V, Ratia C, Gabasa Y, Soto SM. Clinical Escherichia coli: from biofilm formation to new antibiofilm strategies. Microorganisms. 2022;10(6):1103. doi:10.3390/microorganisms10061103
17. Kwak Y, Kim HG, Seok J, Kim S, Kim EM, Kim A. The critical role of intracellular bacterial communities in uncomplicated recurrent urinary cystitis: a comprehensive review of detection methods and diagnostic potential. Int Neurourol J. 2024;28(1):4–10. doi:10.5213/inj.2448066.033
18. Whelan S, Lucey B, Finn K. Uropathogenic Escherichia coli (UPEC) -associated urinary tract infections: the molecular basis for challenges to effective treatment. Microorganisms. 2023.
19. Katongole P, Nalubega F, Florence NC, Asiimwe B, Andia I. Biofilm formation, antimicrobial susceptibility and virulence genes of uropathogenic Escherichia coli isolated from clinical isolates in Uganda. BMC Infect Dis. 2020;20(1):1–6. doi:10.1186/s12879-020-05186-1
20. Maldonado-Barragán A, Mshana SE, Keenan K, et al. Predominance of multidrug-resistant bacteria causing urinary tract infections among symptomatic patients in East Africa: a call for action. JAC-Antimicrobial Resist. 2024;6(1):1–36. doi:10.1093/jacamr/dlae019
21. Mlugu EM, Mohamedi JA, Sangeda RZ, Mwambete KD. Prevalence of urinary tract infection and antimicrobial resistance patterns of uropathogens with biofilm forming capacity among outpatients in morogoro, Tanzania: a cross-sectional study. BMC Infect Dis. 2023;1–9.
22. Bizimungu O, Crook P, Babane JF, Bitunguhari L. The prevalence and clinical context of antimicrobial resistance amongst medical inpatients at a referral hospital in Rwanda: a cohort study. Antimicrob Resist Infect Control. 2024;13(1):1–8. doi:10.1186/s13756-024-01384-7
23. Osena G, Kapoor G, Kalanxhi E, Ouassa T. Antimicrobial resistance in Africa: a retrospective analysis of data from 14 countries, 2016 – 2019. PLoS Med. 2025;832:2016–2019. doi:10.1371/journal.pmed.1004638
24. Gashegu M, Ndahindwa V, Rwagasore E, et al. Diversity, distribution, and resistance profiles of bacterial bloodstream infections in Three Tertiary Referral Hospitals in Rwanda between 2020 and 2022. Antibiotics. 2024;13(11):1084. doi:10.3390/antibiotics13111084
25. Carroll M, Rangaiahagari A, Musabeyezu E, Singer D, Ogbuagu O. Five-year antimicrobial susceptibility trends among bacterial isolates from a Tertiary Health-Care Facility in Kigali, Rwanda. American JTrop Med Hyg. 2016;95(6):1277–1283. doi:10.4269/ajtmh.16-0392
26. Mahshouri P, Alikhani MY, Momtaz HE, Doosti-Irani A, Shokoohizadeh L. Analysis of phylogroups, biofilm formation, virulence factors, antibiotic resistance and molecular typing of uropathogenic Escherichia coli strains isolated from patients with recurrent and non-recurrent urinary tract infections. BMC Infect Dis. 2025;25(1). doi:10.1186/s12879-025-10635-w
27. Gbadamosi MA. JOURNAL OF PHARMACEUTICAL ANALYSIS author guide.pdf. 2023:119–135.
28. Al-Gasha’a FAS, Al-Baker SM, Obiad JM, Alrobiai FA. Prevalence of urinary tract infections and associated risk factors among patients attending medical city hospital in Baghdad City, Iraq. Rev Bras Gest e Desenvolv Reg. 2020;16(2):77–84. doi:10.3844/ajidsp.2020.77.84
29. Keenan K, Papathomas M, Mshana SE, et al. Intersecting social and environmental determinants of multidrug-resistant urinary tract infections in East Africa beyond antibiotic use. Nat Commun. 2024;15(1). doi:10.1038/s41467-024-53253-x
30. Chelangat S, Ngugi C, Song E, Mwaniki JN, Chelangat S. Prevalence of uropathogenic E. Coli, antimicrobial susceptibility profiles and carriage of extended-spectrum beta-lactamases genes at Mama Lucy Hospital, Kenya. Glob J Health Sci. 2025;10(1):14–37.
31. Jagtap S, Harikumar S, Vinayagamoorthy V, Mukhopadhyay S, Dongre A. Comprehensive assessment of holding urine as a behavioral risk factor for UTI in women and reasons for delayed voiding. BMC Infect Dis. 2022;22(1):1–11. doi:10.1186/s12879-022-07501-4
32. Seid M, Markos M, Aklilu A, et al. Community-acquired urinary tract infection among sexually active women: risk factors, bacterial profile and their antimicrobial susceptibility patterns, Arba Minch, Southern Ethiopia. Infect Drug Resist. 2023;16(April):2297–2310. doi:10.2147/IDR.S407092
33. Abo-alella D, Abdelmoniem W, Tantawy E, Asaad A. Biofilm-producing and carbapenems-resistant Escherichia coli nosocomial uropathogens: a cross-sectional study. Int Microbiol. 2024;27(6):1633–1640. doi:10.1007/s10123-024-00495-w
34. Gunardi WD, Karuniawati A, Umbas R, et al. Biofilm-producing bacteria and risk factors (gender and duration of catheterization) characterized as catheter-associated biofilm formation. Int J Microbiol. 2021;2021:1–10. doi:10.1155/2021/8869275
35. Gebremariam T, Eguale T, Belay T, Kalayu AA, Abula T. Antibiotic resistance, and biofilm forming characteristics of Escherichia coli clinical isolates at a hospital in Tigray, Northern Ethiopia. Cureus. 2024;16(11). doi:10.7759/cureus.73569
36. Zhao A, Sun J, Liu Y. Understanding bacterial biofilms: from definition to treatment strategies. Front Cell Infect Microbiol. 2023;13(April):1–23. doi:10.3389/fcimb.2023.1137947
37. Karigoudar RM, Karigoudar MH, Wavare SM, Mangalgi SS. Detection of biofilm among uropathogenic Escherichia coli and its correlation with antibiotic resistance pattern. J Lab Physicians. 2019;11(01):017–022. doi:10.4103/jlp.jlp_98_18
38. Alshaikh SA, El-banna T, Sonbol F, Farghali MH. Correlation between antimicrobial resistance, biofilm formation, and virulence determinants in uropathogenic Escherichia coli from Egyptian hospital. Ann Clin Microbiol Antimicrob. 2024;23(1):1–22. doi:10.1186/s12941-024-00679-2
39. Behzadi P, Urbán E, Gajdács M. Association between biofilm-production and antibiotic resistance in uropathogenic Escherichia coli (UPEC): an in vitro study. Diseases. 2020;8(2):1–11. doi:10.3390/diseases8020017
40. Cepas V, López Y, Muñoz E, et al. Relationship between biofilm formation and antimicrobial resistance in gram-negative bacteria. Microb Drug Resist. 2019;25(1):72–79. doi:10.1089/mdr.2018.0027
41. Algburi A, Comito N, Kashtanov D, Dicks LMT, Chikindas ML. Control of biofilm formation: antibiotics and beyond. Appl Environ Microbiol. 2017;83(3). doi:10.1128/AEM.02508-16
42. Patterns AS. Antibiotic susceptibility patterns and biofilm production by uropathogenic Escherichia coli from reproductive age women in a region of NSW. J Infect Dis Epidemiol. 2022;8(9):1–10. doi:10.23937/2474-3658/1510280
43. Öztürk R, Murt A. Epidemiology of urological infections: a global burden. World J Urol. 2020;38(11):2669–2679. doi:10.1007/s00345-019-03071-4
44. Demir İ, Öztürk GZ, Uzun A. Analyzing the relationship between genital hygiene behaviors in women and urinary tract infection in any period of life. Ankara Med J. 2020;20(4):982–992. doi:10.5505/amj.2020.37640
45. Mohamed FY, Dahie HA, Mohamoud JH, Adam MH, Dirie HM. Prevalence, antimicrobial susceptibility profile, and associated risk factors of uropathogenic Escherichia coli among pregnant women attending Dr. Sumait Hospital Mogadishu, Somalia. Front Public Health. 2023;11(January):1–9. doi:10.3389/fpubh.2023.1203913
46. Tegegne KD, Wagaw GB, Gebeyehu NA, Yirdaw LT, Shewangashaw NE, Kassaw MW. Prevalence of urinary tract infections and risk factors among diabetic patients in Ethiopia, a systematic review and meta-analysis. PLoS One. 2023;18(1 January):1–19. doi:10.1371/journal.pone.0278028
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Antibiogram of Escherichia coli Isolated from Dairy Cattle and in-Contact Humans in Selected Areas of Central Ethiopia
Tadesse T, Alemayehu H, Medhin G, Akalu A, Eguale T
Veterinary Medicine: Research and Reports 2024, 15:117-127
Published Date: 10 April 2024