Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Professional Quality of Life Among Professionals Working with People with Eating Disorders: The Interplay Between Meaning in Work, Optimism, and Career Duration
Authors Hamama-Raz Y ![]() , Mazor S
, Mazor S
Received 1 August 2023
Accepted for publication 11 October 2023
Published 2 November 2023 Volume 2023:16 Pages 3249—3259
DOI https://doi.org/10.2147/JMDH.S433458
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Yaira Hamama-Raz, Shachar Mazor
School of Social Work, Ariel University, Ariel, Israel
Correspondence: Yaira Hamama-Raz, School of Social Work, Ariel University, Ariel, Israel, Tel +972-77-40020824, Email [email protected]
Purpose: Scientific literature findings reflect the challenges experienced by healthcare professionals (HCPs) whose work is dedicated to helping clients with eating disorders (EDs) in various treatment centers (wards). These challenges can affect the professional quality of life (comprised of compassion satisfaction, burnout, and secondary traumatic stress) of HCPs. The present study delved into this relationship and explored the moderating role of dispositional optimism and the role of career duration in ED wards in the link between meaning in work and professional quality of life.
Methods: Two hundred HCPs working in ED wards in Israel were recruited through their professional social networks. Participants completed self-report questionnaires related to socio-demographic and work data, professional quality of life, meaning in work, and dispositional optimism.
Results: Career duration in ED wards was negatively associated with secondary traumatic stress, while dispositional optimism and meaning in work were positively associated with compassion satisfaction and negatively associated with burnout and secondary traumatic stress. With respect to the moderation effect of dispositional optimism and EDs ward career duration, the findings revealed that the positive relationship between meaning in work and compassion satisfaction weakened as dispositional optimism scores increased. Additionally, the negative relationship between meaning in life and burnout was significant only when the career duration in EDs wards was less than 12.31 years.
Conclusion: HCPs working in ED wards could draw on the findings to improve their professional quality of life, especially through enhancing meaning in work. Attention should be paid especially toward HCPs with many years (> 12.31) of experience in the ED wards.
Keywords: healthcare professionals, eating disorder, professional quality of life, meaning in work, optimism, career duration
Introduction
Individuals with eating disorders (EDs) have high levels of risk, relapse, and treatment resistance.1–3 Therefore, healthcare professionals (HCPs) in this field can experience professional challenges. In a recent meta-ethnography on HCPs’ lived experiences of working with people with EDs, Graham et al4 revealed a key concept of “coping with caring without curing”. This concept described how those working in ED services are limited in their capacity to help, which creates a painful dissonance that can impact the enjoyment of the job, the perceptions of service providers, and work alliances.4
The challenges of working with people with EDs go beyond the HCPs. These challenges have been found to impact the clinician–client alliance and, consequently, the treatment outcomes themselves.5 The confluence of these findings pointed the way to the present study. This study aimed to focus on professional quality of life among HCPs working with people with EDs to benefit both HCPs and their relationship with their clients.
There are two aspects of professional quality of life.6 The positive aspect relates to compassion satisfaction: the pleasure one derives from being able to do one’s work well, feeling positively disposed toward colleagues, and being able to contribute to the work environment. The negative aspect relates to compassion fatigue: the physical and psychological burden felt by those helping others in distress. According to Stamm,6 compassion fatigue is comprised of burnout and secondary traumatic stress. Thus, HCPs who experience poor professional quality of life may indicate a low level of compassion satisfaction and a high level of compassion fatigue, including high levels of burnout and secondary traumatic stress.
It was found that poor professional quality of life diminished the provision of quality care and professional services to patients/clients.7,8 Likewise, poor professional quality of life was found to increase employee turnover.9 The factors that positively and negatively influenced professional quality of life were found to be both sociodemographic- and work-related.10
Following the scientific literature on professional quality of life, we aimed to explore and discover the contributions of specific variables to professional quality of life among HCPs working with people with EDs. The first of these variables is meaning in one’s work. The second variable is dispositional optimism as an internal personality variable. The third variable is career duration in the profession with people with eating disorders. Career duration is the cumulative amount of time in years an HCP has worked in EDs treatment centers (called wards or ED wards) caring for patients with EDs. These three variables have each been the focus of previous studies, but their interplay has not yet been examined.
Meaning in Work
Meaning in work was found to be associated with greater well-being,11 reduced levels of stress and depression,12 and higher job satisfaction.13 In the self-perspective, meaning in work was found to encompass perceiving one’s work as meaningful to the extent that it brings personal benefits to the employee and endows a sense of development and accomplishment of important goals.14 Martela and Pessi15 found that three elements define meaning in work: the subjective experience of the work as intrinsically significant and worth doing; the self-realization that one is able to experience through the work (ie, a sense of autonomy, authenticity and self-expression at work); and the conception that the work serves some greater good or prosocial goal.
Interestingly, the direct relationship between meaning in work and professional quality of life has not yet been studied. However, previous studies have stressed the negative relationship between meaning in work and burnout, which is one of the components of compassion fatigue (clinicians dealing with genetic therapies;16 clinicians who treat abused children;17 medical professionals18). Lee19 noted that meaning in work can help professionals better evaluate their work environment and thereby help prevent burnout. In this particular scholarly context, it was revealed by Hamama-Raz et al20 that the relationship between posttraumatic growth and both secondary traumatization and burnout were moderated by the presence of meaning in the work. Regarding this direct link (namely, the negative link between posttraumatic growth and burnout) the link became stronger as meaning in work increased.20 The present study was designed in light of the gap of research into the direct relationship between meaning in work and professional quality of life among HCPs working with people with EDs.
Dispositional Optimism
Dispositional optimism is generally seen as a personality trait, which serves as an effective resource for coping with adversity and challenges.21 Previous studies have demonstrated that dispositional optimism is associated with a broad range of positive constructs and with well-being.22,23 In reference to professional quality of life, dispositional optimism was found to be positively associated with compassion satisfaction and negatively correlated with burnout and secondary trauma among school counselors.24 Some scholars examined the association between dispositional optimism and professional quality of life mainly by referring to specific aspects of the constructs of professional quality of life. Specifically, dispositional optimism was negatively correlated with burnout among medical residents,25 and low dispositional optimism was related to higher compassion fatigue risk in genetic counselors.26 In the context of this study, exploring the relations between dispositional optimism and professional quality of life among HCPs working with people with EDs seems to be important, given the challenges that arise among this client group. In addition, we sought to assess the moderator role of dispositional optimism in the link between meaning in work and professional quality of life.
EDs-Career Duration
The third and final work-related variable we aimed to explore was the association between EDs-career duration and professional quality of life. Previous studies showed that compassion satisfaction correlated positively with years of work experience while burnout correlated negatively with years of work experience (nurses in an emergency room;27 dentists28). Also, Yu et al29 revealed among oncology nurses a positive association between increased duration of nursing experience and higher levels of compassion fatigue and burnout. In contrast, however, Ruiz-Fernández et al30 showed that among hospital emergency nurses in Spain, the levels of compassion satisfaction were significantly higher in professionals with less work experience (<10 years). Ruiz-Fernández et al30 claimed that at the beginning of one’s career, professionals enjoy a high level of energy, but with the passage of time and continued work in these services, compassion satisfaction may decline. Thus, career duration in working with people with EDs might be an important component related to both meaning in work and professional quality of life suggesting a moderating role in this association.
The Current Study
Taken together, the aim of the present study was to develop and explore a comprehensive model by which one could examine the moderating role of optimism and career duration among HCPs working with people with EDs in reference to the link between meaning in work and professional quality of life. The following hypotheses were postulated:
H1. EDs-career duration will be associated positively with compassion satisfaction and negatively associated with burnout and secondary traumatic stress; H2. Dispositional optimism will be associated positively with compassion satisfaction and negatively with burnout and secondary traumatic stress; H3. Meaning in work will be associated positively with compassion satisfaction and negatively with burnout and secondary traumatic stress; H4. The association between meaning in work and professional quality of life will be moderated by EDs-career duration and by dispositional optimism.
Materials and Methods
The study protocol was approved by Ariel University’s Institutional Review Board committee (No. AU-SOC-YHR-20210709). Participants were recruited through social networks (eg, WhatsApp, Facebook) related to healthcare professionals who specialized within the eating disorder field in various treatment services: hospitals, outpatient clinics, community rehabilitation homes, and Health Maintenance Organization (HMO) clinics for eating disorders. Participants were informed that participation was entirely voluntary, and that data obtained from the survey would be analyzed in an anonymous format. In addition, a request was made to the Israeli Association of Eating Disorders (ISED) to distribute the link among their members. Data collection took place between August 2021 and January 2022. All participants gave written informed consent for participation in the study.
Participants
Two hundred HCPs working only with people with EDs (inclusion criteria) gave their consent and agreed to fill out the questionnaires. Of the participants, 22% (n = 44) were nutritionists/dieticians, 20% (n = 40) were psychologists, 16.5% (n = 33) social workers, 15.5% (n = 31) rehabilitation instructors, 13.5% (n = 27) nurses, 8% (n = 16) medical doctors, and 4.5% (n = 9) art therapists. Their ages ranged from 20 to 79 years (M = 39.94, SD = 11.42), and most were women (85.0%, n = 170). The majority were native Israelis (87%, n = 174) and were currently married or in a relationship (62.0%, n = 124). Most of the participants described themselves as secular (68.5%, n = 137); 21.5% (n = 43) were traditional and 10% (n = 20) were religious. Regarding the participants’ work environment: the overall professional career duration ranged from 0 to 45 years (M = 12.01, SD = 10.03), the years of EDs career duration ranged from six months to 30 years (M = 7.97, SD = 7.61), and the participants’ part-time employment ranged from 10% to full time (100%) (M = 73.80, SD = 24.45).
Measures
Participants completed the following self-report questionnaires:
Personal data – gender, age, country of birth, marital status, education, and degree of religiosity. In addition, participants were asked to indicate the duration of their professional experience, career duration of employment in eating disorders wards, and if their employment was part- or full-time.
Professional quality of life – was assessed with the Professional Quality of Life Scale (ProQOL) developed by Stamm.6 The ProQOL consists of 30 items with a Likert-type scale of 5 points ranging from 1 (never) to 5 (very often). This scale is composed of three subscales: compassion satisfaction which evaluates positive treatment outcomes (eg, “I get satisfaction from being able to help people”), burnout (eg, “I feel overwhelmed because my workload seems endless”), and secondary traumatic stress (eg, “I think that I might have been affected by the traumatic stress of those I help”). In the current study, we used the translated and validated Hebrew version.31 The participants were directed to specify the frequency of their experiences of each item within the past 30 days. For each 10-item subscale, the summed responses were utilized to determine the scores, with higher values reflecting increased levels of compassion satisfaction, secondary traumatic stress, and burnout. Scores from each of the subscales ranged from 0 to 50, and cut-off rates can be categorized into low = 22 or less, average = 23–41 and high = 42 or more.6 Then, scores were converted with t scores (M = 50, SD = 10). ProQOL-5 has a Cronbach’s alpha of 0.88 for compassion satisfaction, 0.81 for secondary traumatic stress, and 0.75 for burnout.6 The Cronbach’s alpha of the current study was 0.89 for compassion satisfaction, 0.90 for secondary traumatic stress, and 0.73 for burnout.
Meaning in work – was assessed through the questionnaire Personal Meaning in Patient Care developed by Geller et al16 using the Hebrew version that has been used in previous Israeli studies.20,32 The scale is unidimensional and consists of 6-items (eg, “Feeling deep connections with my patients”) using a 4-point scale (from 1 = “never” to 4 = “very much”). The questionnaire was scored by summing the item responses for each 6 items, with a higher score indicating a greater level of ‘finding personal meaning in patient care.’ Its Cronbach’s alpha internal reliability value was 0.82. In the current study, Cronbach’s alpha was α = 0.80.
Dispositional optimism – was assessed with the revised version of the Life Orientation Test (LOT-R33). The Hebrew version of LOT-R has been used in previous Israeli studies.34,35 The scale consists of a 10-items measure of optimism versus pessimism (eg, “Overall, I expect more good things to happen to me than bad”), using a 5-point scale (from 0 = strongly disagree to 4 = strongly agree). The scores are distributed along a continuum of 0 to 24, with elevated scores indicating a greater degree of dispositional optimism and lower scores indicating lower dispositional optimism, which is commonly referred to as pessimism. LOT-R has a Cronbach’s alpha of 82.31 The Cronbach’s alpha of the current study was 89.
Data Analysis
First, data were described using means, standard deviation, skewness, and kurtosis values. Then, associations between continuous variables were examined via zero-order correlations (Hypotheses 1–3). Point-biserial correlations were conducted for associations between dichotomous and continuous variables. Moderation analyses were performed using hierarchical multiple regression models in two steps (Hypothesis 4). In step 1, EDs-career duration, dispositional optimism and meaning in work were entered. In step 2, the interaction terms of meaning in work with dispositional optimism and EDs-career duration were entered. ProQOL measures served as the outcomes. In order to make the results more interpretable, meaning in work, dispositional optimism, and EDs-career duration were centered prior to the analyses.36 Lastly, probing and visualizing the significant interactions were conducted with the Johnson–Neyman method via PROCESS macro for SPSS (Model 1).37 The Johnson–Neyman method designates region (or regions) of significance according to the value (or values) of the moderator, where the conditional effect of the predictor shifts between statistically significant to not statistically significant.38 Note that variance inflation factor (VIF) values were examined in order to rule out multicollinearity issues (ie, VIF >10).39 Moreover, the moderation analyses were examined twice: with and without controlling for age. Since the results were not substantially different, they were reported without controlling for age.
Data were analyzed using IBM SPSS statistics version 28 with an alpha level set to 0.05 for all statistical tests.
Results
Table 1 presents descriptive statistics and correlations between background and study variables. As can be seen from the table, all values of skewness and kurtosis were within the normal range. Dispositional optimism was slightly above the mid-range (on a 0–4 scale), and meaning in work was high (on a 14–24 scale). According to the cut-off rates, compassion satisfaction was categorized as average, with 79 participants (39.5%), 119 (59.5%), and 2 (1.0%) exhibiting high, average, and low levels, respectively. Burnout was categorized as low, with 85 participants (42.5%), and 115 participants (57.5%) exhibiting average and low levels, respectively. Secondary traumatic stress was also categorized as low, 2 participants (1.0%), 75 (37.5%), and 123 (61.5%) exhibiting high, average, and low levels, respectively. Most of the associations between the study variables were significant, whereas the associations between the background and study variables were mostly non-significant. Specifically, career duration was negatively associated only with secondary traumatic stress (Hypothesis 1). Dispositional optimism and meaning in work were positively associated with compassion satisfaction and negatively associated with burnout and secondary traumatic stress (Hypotheses 2 and 3, respectively).
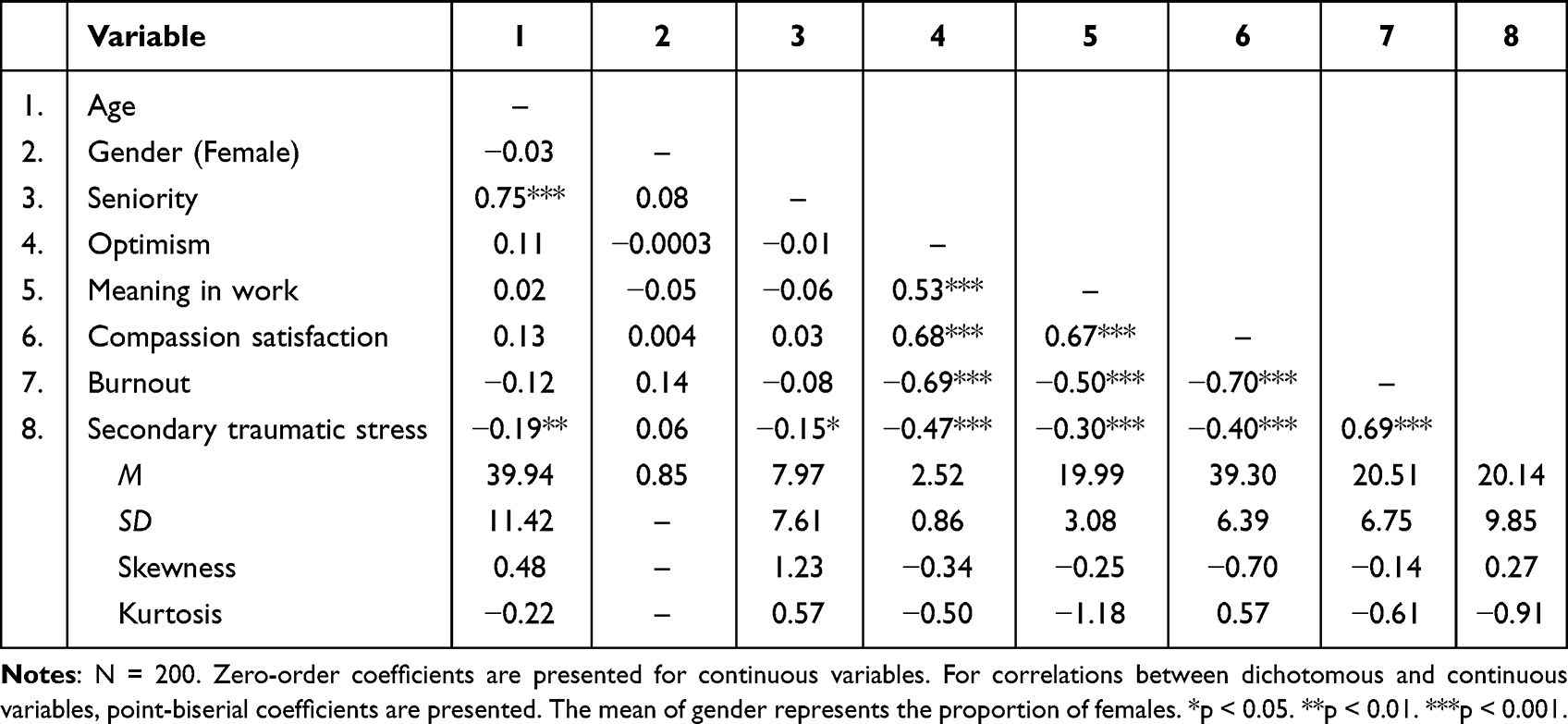 |
Table 1 Means, Standard Deviations, Skewness, Kurtosis, and Correlations Between Background and Study Variables |
Table 2 presents results for the moderation hypothesis (Hypothesis 4). In all analyses, there were no issues of multicollinearity (all VIF values <1.42). In the analysis predicting compassion satisfaction, Step 1 was significant, F(3, 196) = 98.37, p < 0.001, R2 = 0.60, with dispositional optimism and meaning in work positively predicting compassion satisfaction. Adding the interactions in Step 2 yielded significant results, ΔF(2, 194) = 4.69, p = 0.010, ΔR2 = 0.02, with only meaning in life × dispositional optimism significantly predicting compassion satisfaction. The Johnson–Neyman method showed that the positive relationship between meaning in life and compassion satisfaction weakened as dispositional optimism scores were higher and that the relationship remained significant for any value of dispositional optimism (Figure 1).
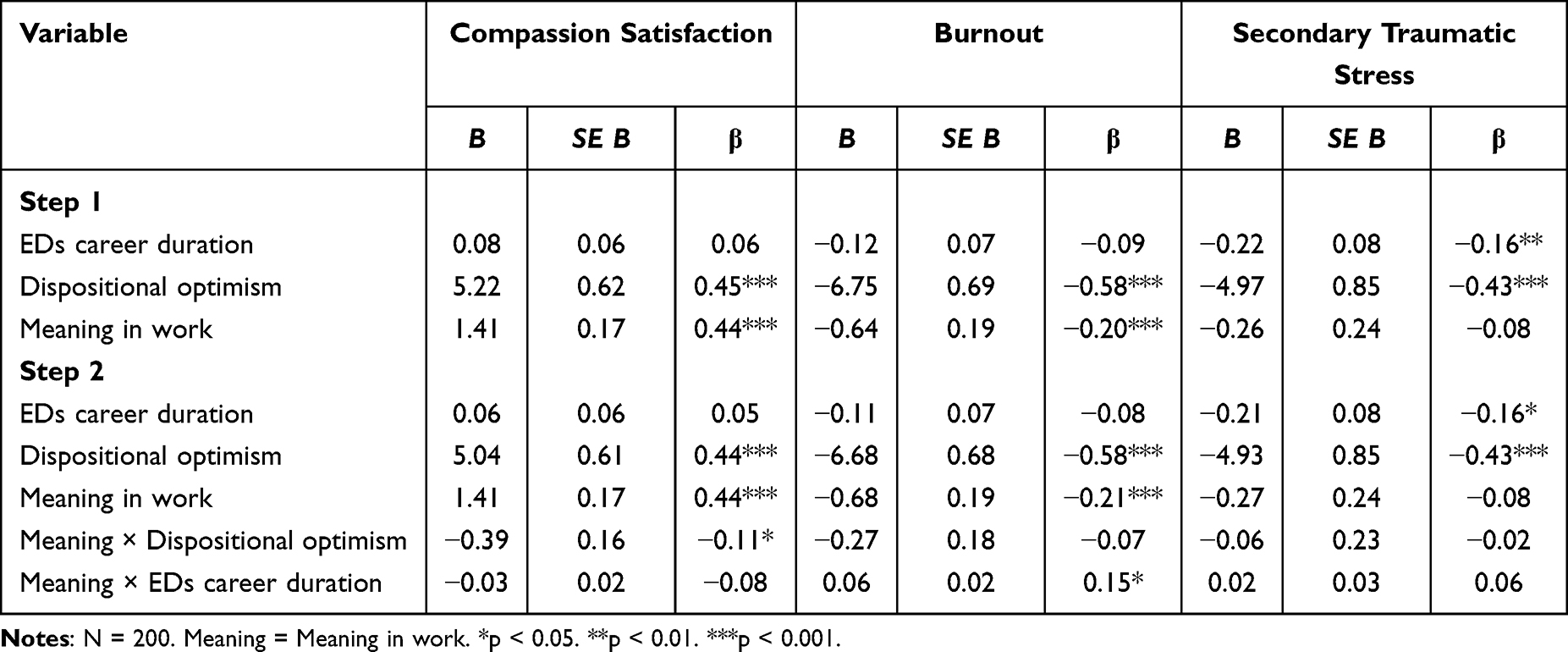 |
Table 2 Results of Hierarchical Multiple Regression Analyses Predicting Professional Quality of Life Measures |
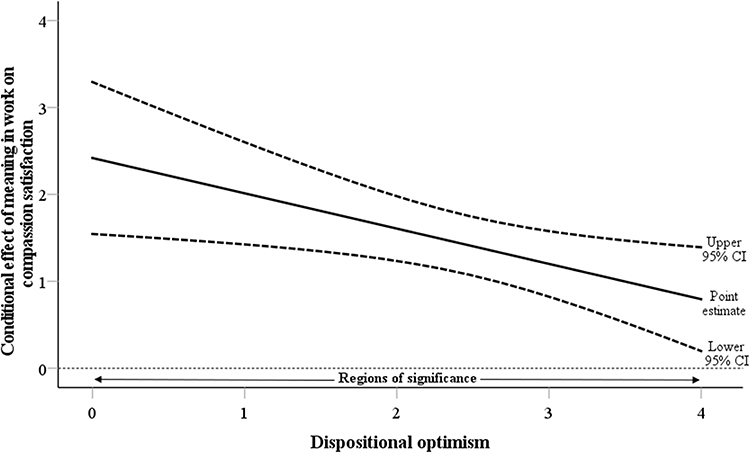 |
Figure 1 Johnson–Neyman method for plotting the regions of significance of the meaning in life × dispositional optimism interaction on compassion fatigue. Notes: N = 200. Non-centered values are presented for dispositional optimism. |
The analysis predicting burnout yielded significant results for Step 1, F(3, 196) = 66.86, p < 0.001, R2 = 0.51, with dispositional optimism and meaning in work negatively predicting burnout. The addition of the interactions in Step 2 was significant, ΔF(2, 194) = 5.23, p = 0.006, ΔR2 = 0.02, with only meaning in life × in the career duration in EDs significantly predicting burnout. The Johnson–Neyman method showed that the negative relationship between meaning in life and burnout was significant when EDs-career duration was less than 12.31 years (78.0% of the participants) but not significant when values were higher (Figure 2).
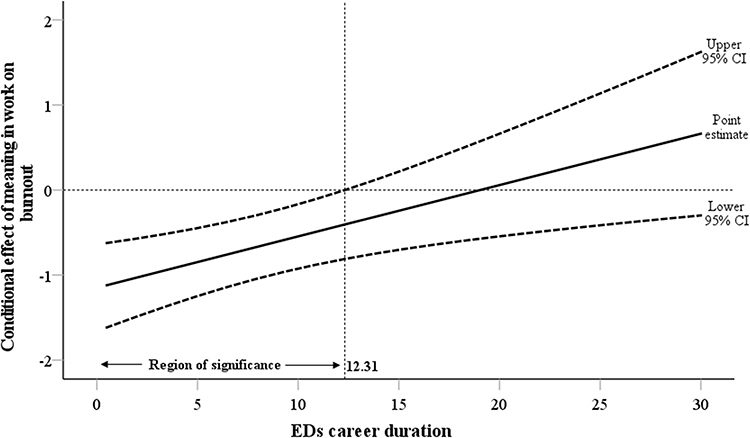 |
Figure 2 Johnson–Neyman method for plotting the region of significance of the meaning in life × eating disorder career duration interaction on burnout. Notes: N = 200. Non-centered values are presented for eating disorder career duration. |
Lastly, predicting secondary traumatic stress yielded significant results for Step 1, F(3, 196) = 21.88, p < 0.001, R2 = 0.25, with EDs-career duration and dispositional optimism negatively predicting secondary traumatic stress. However, the addition of the interactions in Step 2 was non-significant, ΔF(2, 194) = 0.41, p = 0.663, ΔR2 = 0.003.
Discussion
The present study focused on professional quality of life among HCPs working with people with EDs in relation to meaning in work, dispositional optimism, and EDs-career duration. Our findings revealed that in reference to the professional quality of life scores among HCPs working with people with EDs, the majority of HCPs experienced average levels of compassion satisfaction (59.5%), low levels of burnout (57.5%), and levels of secondary traumatic stress (61.5%). High levels of compassion satisfaction and low levels of burnout and secondary traumatic stress result in enhanced professional quality of life, suggesting that HCPs in the present study have satisfactory professional quality of life. To date, no other scholars investigated professional quality of life scores among HCPs working with EDs; thus, our results cannot be compared to other findings. Research into characterizing professional quality of life scores by HCPs working with EDs is necessary to confirm this finding.
With regard to the negative association between EDs-career duration and secondary traumatic stress, our results confirmed previous studies conducted among intensive care and oncology nursing units,40 trauma nurses,41 and healthcare workers including clinicians, nurses, and medical teachers.42 A possible explanation may be that HCPs with lower EDs-career duration have not yet acquired professional tools relevant to the field of EDs, and as such they may be more vulnerable to complex situations that arise in caregiving for patients who are coping EDs.43 Moreover, according to the Conservation of Resources (COR) theory,44 professional career duration (ie, seniority) is included among the “condition” resources. Condition resources can protect against resource loss and allow the individual to recover from losses and to gain resources. Thus, it is reasonable to assume that HCPs with lower career duration in ED wards, are less trained in empirically supported methods, safety management, and treatment resistance with ED patients, and as such may experience more stress, which, in turn, may lead to secondary traumatic stress.
Another finding relates to the association between dispositional optimism and the three components of professional quality of life. That is, dispositional optimism is positively associated with compassion satisfaction and negatively associated with burnout and secondary traumatic stress. Our results support previous studies conducted among teachers,24 medical residents,25 and among residential childcare,45 and veterinary professionals.46 Indeed, Carver et al21 noted that optimistic people face problems and demands in a healthier manner and are more resistant to the biological and psychological effects of stress. In line with this notion, Garrosa et al47 found among nurses that dispositional optimism was a factor that staves off emotional exhaustion. It follows from those studies’ findings that for optimistic HCPs, compassion satisfaction will be higher, while burnout and secondary traumatic stress will be reduced.
The study findings also indicate that meaning in work is positively associated with compassion satisfaction and negatively associated with burnout and secondary traumatic stress. This finding may be explained through Steger’s48 claim that meaning in work can be experienced when individuals are able to identify significance in their actions, and that their work reflects personal values and beliefs. Health professionals with high meaning in work may manage to tolerate frustrations occurring in their daily practice in the pursuit of a highly valued work-associated purpose.49 Similarly, Tei et al18 noted that medical professionals with an enhanced sense of meaning might recognize the greater purpose of their work, thus finding critical situations (eg, alleviating patients’ suffering) more fulfilling than distressing. Indeed, recent findings49 lend support to the role of high meaning in work in compensating for the negative affective experiences among physicians and nurses working with multiple sclerosis. In reference to the HCPs in this study, those practitioners with higher work meaning may view their treatment challenges as manageable,4 thus minimizing the risk for burnout and secondary traumatic stress while reinforcing compassion satisfaction.
With respect to the moderation analysis, the finding shows that the positive relationship between meaning in work and compassion satisfaction weakened as optimism scores strengthened and grew higher (for any value of dispositional optimism). A possible explanation may stem from the notion of dispositional optimism as a psychological strength that remains constant over the course of life.21 Specifically, according to Carver and Scheier,50 optimistic individuals generally have a sense of confidence that difficulties can be handled successfully and that goals may be achieved in different ways. Thus, it might be that its presence is a personal resource that assists in coping21,44 and is a dominant trait in the achieving of compassion satisfaction. In line with this reasoning, Liu et al22 showed that dispositional optimism correlated positively with general self-efficacy, satisfaction with life, and positive affect and correlated negatively with negative affect.
Finally, in reference to the moderating role of EDs-career duration, the result shows that the negative relationship between meaning in life and burnout was significant only when EDs-career duration was less than 12.31 years. A possible explanation for this finding may be related to HCPs’ cumulative experience with EDs treatments and rate of recovery over the years. Specifically, according to Wonderlich et al,51 approximately half of patients with EDs will not recover following an adequate treatment course, and their illness’ duration continues. In addition, Hay et al52 stressed that as a result of repeated treatment failures “both the clinician and patient often share the experience of hopelessness and despair about the likelihood of meaningful change” (p. 996). Indeed, in a recent study related to patients with EDs, it was found that the most frequent reason for terminating treatment by the staff was patients’ failure to meet pre-agreed weight gain goals.53 Thus, it might be that those HCPs who work with patients with EDs for more than 12.31 years ultimately accumulate negative experiences concerning recovery and cure, and as such, meaning in work is not a sufficient resource to correlate with burnout.
Limitations
Several limitations of the present study should be noted. First, the cross-sectional design of the study does not allow any inferences regarding causal relationships. Thus, a longitudinal design would provide more reliable indications regarding the stability of the links between meaning in work, dispositional optimism, EDs-career duration, and professional quality of life over time. Such a design would also allow replication of the present study within different medical contexts (eg, oncology, palliative care). Second, the questionnaires were filled out during the Covid-19 pandemic, which may have affected the complexity of the patients with ED treatment and, accordingly, increased the challenge to the professional, beyond the professional’s personal coping during this period. Third, the data collected did not assess the severity of ED patients or the diversity of diagnoses. As such, caution in interpreting the findings is warranted. Fourth, the study findings rely on a convenience sample with self-report measures and with no data concerning responder rates or the number of non-completers. This may limit the ability to generalize the findings. Finally, the sample used here was relatively small, with a wide range of clinical disciplines and with unequal numbers of representatives of the various disciplines that work with people with EDs, which limited the interpretation of the results. Furthermore, the sample was comprised mostly of women, which is consistent with the predominance of women in the healthcare profession in Israel54 but may not be true elsewhere. As such, the potential generalizability of the results is limited. Future studies are invited to recruit larger samples, with each profession represented in equal number, which may allow the potential generalization of results.
Clinical Implications
In light of the current findings that meaning in work is associated positively with compassion satisfaction and negatively associated with burnout and secondary traumatic stress, it is recommended that care centers of people with EDs implement periodic evaluations of personal meaning in patient care among their HCPs. This may enable the identification of those who might be at risk of burnout.16 In line with this notion, designing interventions that aim to promote meaningful work through recognizing the four dimensions of meaningful work (ie, relationships with each other and with the patients, a commitment to compassionate caring, personal identification with the profession, and mentorship they received as students)55 may be recommended. Another avenue of clinical application relates to EDs-career duration. Continuing supervision and reflective spaces among HCPs with many years in the ED ward (>12.31) may reduce the risk for their burnout and will provide a way to maintain their sense of meaning in work.
Conclusions
This study explores professional quality of life comprised compassion satisfaction, burnout, and secondary traumatic stress among HCPs working with people with EDs. This study found this subject group’s professional quality of life to be satisfying in general. Our findings indicate that dispositional optimism and career duration in EDs wards are central factors in the association between meaning in work and the professional quality of life and its constructs. In respect to these findings, it seems that maintaining professional quality of life of HCPs working with people with EDs via these factors may contribute to a stronger and more satisfying HCPs-to-patient alliance.
Abbreviations
EDs, eating disorders; HCPs, healthcare professionals.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Informed Consent
This study was approved by Ariel University’s Institutional Review Board Committee (AU-SOC-YHR-20210709). Written informed consent was given by each participant.
Author Contributions
Both authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was not funded.
Disclosure
The authors declare that there are no conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Le LK, Barendregt JJ, Hay P, Mihalopoulos C. Prevention of eating disorders: a systematic review and meta-analysis. Clin Psychol Rev. 2017;53:46–58. doi:10.1016/j.cpr.2017.02.001
2. Seah XY, Tham XC, Kamaruzaman NR, Yobas PK. Knowledge, attitudes and challenges of healthcare professionals managing people with eating disorders: a literature review. Arch Psychiatr Nurs. 2017;31(1):125–136. doi:10.1016/j.apnu.2016.09.002
3. Zaitsoff S, Pullmer R, Cyr M, Aime H. The role of the therapeutic alliance in eating disorder treatment outcomes: a systematic review. Eat Disord. 2015;23(2):99–114. doi:10.1080/10640266.2014.964623
4. Graham MR, Tierney S, Chisholm A, Fox JRE. The lived experience of working with people with eating disorders: a meta-ethnography. Int J Eat Disord. 2020;53(3):422–441. doi:10.1002/eat.23215
5. Graves TA, Tabri N, Thompson-Brenner H, et al. A meta-analysis of the relation between therapeutic alliance and treatment outcome in eating disorders. Int J Eat Disord. 2017;50(4):323–340. doi:10.1002/eat.22672
6. Stamm BH. The Concise ProQOL Manual.
7. Adimando A. Preventing and alleviating compassion fatigue through self-care: an educational workshop for nurses. J Holist Nurs. 2018;36(4):304–317. doi:10.1177/0898010117721581
8. Garcia CL, Abreu LC, Ramos JLS, et al. Influence of burnout on patient safety: systematic review and meta-analysis. Medicina. 2019;55(9):553. doi:10.3390/medicina55090553
9. Pang Y, Dan H, Jung H, Bae N, Kim O. Depressive symptoms, professional quality of life and turnover intention in Korean nurses. Int Nurs Rev. 2020;67(3):387–394. doi:10.1111/inr.12600
10. Yilmaz G, Üstün B. Professional quality of life in nurses: compassion satisfaction and compassion fatigue. J Psychiatr Nurs. 2018;9(3):205–211. doi:10.14744/phd.2018.86648
11. Arnold KA, Turner N, Barling J, Kelloway EK, McKee MC. Transformational leadership and psychological well-being: the mediating role of meaningful work. J Occup Health Psychol. 2007;12(3):193–203. doi:10.1037/1076-8998.12.3.193
12. Daniel JL. Workplace spirituality and stress: evidence from Mexico and US. Manag Res Rev. 2015;38:29–43. doi:10.1108/MRR-07-2013-0169
13. Kamdron T. Work motivation: relationships with job satisfaction, locus of control and motivation orientation. Int J Arts and Soc Sci. 2015;3(6):125–148.
14. Puchalska-Kamińska M, Czerw A, Roczniewska M. Work meaning in self and world perspective: a new outlook on the WAMI Scale. Soc Psychol Bull. 2019;14(1):1–29. doi:10.32872/spb.v14i1.30207
15. Martela F, Pessi AB. Significant work is about self-realization and broader purpose: defining the key dimensions of meaningful work. Front Psychol. 2018;9:363. doi:10.3389/fpsyg.2018.00363
16. Geller G, Bernhardt BA, Carrese J, Rushton CH, Kolodner K. What do clinicians derive from partnering with their patients? A reliable and valid measure of “personal meaning in patient care”. Patient Educ Couns. 2008;72(2):293–300. doi:10.1016/j.pec.2008.03.025
17. Passmore S, Hemming E, McIntosh HC, Hellman CM. The relationship between hope, meaning in work, secondary traumatic stress, and burnout among child abuse pediatric clinicians. Perm J. 2020;24:
18. Tei S, Becker C, Sugihara G, et al. Sense of meaning in work and risk of burnout among medical professionals. Psychiatry Clin Neurosci. 2015;69(2):123–124. doi:10.1111/pcn.12217
19. Lee S. A concept analysis of ‘Meaning in work’ and its implications for nursing. J Adv Nurs. 2015;71(10):2258–2267. doi:10.1111/jan.12695
20. Hamama-Raz Y, Hamama L, Pat-Horenczyk R, Stokar YN, Zilberstein T, Bron-Harlev E. Posttraumatic growth and burnout in pediatric nurses: the mediating role of secondary traumatization and the moderating role of meaning in work. Stress Health. 2021;37(3):442–453. doi:10.1002/smi.3007
21. Carver CS, Scheier MF, Segerstrom SC. Optimism. Clin Psychol Rev. 2010;30(7):879–889. doi:10.1016/j.cpr.2010.01.006
22. Liu C, Cheng Y, Hsu ASC, Chen C, Liu J, Yu G. Optimism and self-efficacy mediate the association between shyness and subjective well-being among Chinese working adults. PLoS One. 2018;13(4):e0194559. doi:10.1371/journal.pone.0194559
23. Satici B. Testing a model of subjective well-being: the roles of optimism, psychological vulnerability, and shyness. Health Psychol Open. 2019;6(2):2055102919884290. doi:10.1177/2055102919884290
24. Levkovich I, Ricon T. Understanding compassion fatigue, optimism and emotional distress among Israeli school counsellors. Asia Pac J Couns Psychother. 2020;11(2):159–180. doi:10.1080/21507686.2020.1799829
25. Fowler JB, Fiani B, Kiessling JW, et al. The correlation of burnout and optimism among medical residents. Cureus. 2020;12(2):e6860. doi:10.7759/cureus.6860
26. Injeyan MC, Shuman C, Shugar A, Chitayat D, Atenafu EG, Kaiser A. Personality traits associated with genetic counselor compassion fatigue: the roles of dispositional optimism and locus of control. J Genet Couns. 2011;20(5):526–540. doi:10.1007/s10897-011-9379-4
27. Hunsaker S, Chen HC, Maughan D, Heaston S. Factors that influence the development of compassion fatigue, burnout, and compassion satisfaction in emergency department nurses. J Nurs Scholarsh. 2015;47(2):186–194. doi:10.1111/jnu.12122
28. Meyerson J, Gelkopf M, Eli I, Uziel N. Burnout and professional quality of life among Israeli dentists: the role of sensory processing sensitivity. Int Dent J. 2020;70(1):29–37. doi:10.1111/idj.12523
29. Yu H, Jiang A, Shen J. Prevalence and predictors of compassion fatigue, burnout and compassion satisfaction among oncology nurses: a cross-sectional survey. Int J Nurs Stud. 2016;57:28–38. doi:10.1016/j.ijnurstu.2016.01.012
30. Ruiz-Fernández MD, Pérez-García E, Ortega-Galán ÁM. Quality of life in nursing professionals: burnout, fatigue, and compassion satisfaction. Int J Environ Res Public Health. 2020;17(4):1253. doi:10.3390/ijerph17041253
31. Samson T, Iecovich E, Shvartzman P. Psychometric characteristics of the Hebrew version of the professional quality-of-life scale. J Pain Symptom Manage. 2016;52(4):575–581.e1. doi:10.1016/j.jpainsymman.2016.03.019
32. Stokar YN, Pat-Horenczyk R. Themes of end-of-life care in memorable cases of medical health professionals: a mixed methods approach. Curr Psychol. 2023;42:13721–13732. doi:10.1007/s12144-021-02566-x
33. Scheier MF, Carver CS, Bridges MW. Distinguishing optimism from neuroticism (and trait anxiety, self-mastery, and self-esteem): a reevaluation of the life orientation test. J Pers Soc Psychol. 1994;67(6):1063–1078. doi:10.1037//0022-3514.67.6.1063
34. Weinberg M, Besser A, Zeigler-Hill V, Neria Y. Dispositional optimism and self-esteem as competing predictors of acute symptoms of generalized anxiety disorders and dissociative experiences among civilians exposed to war trauma. Psychol Trauma. 2015;7(1):34–42. doi:10.1037/a0035170
35. Pe’er A, Slone M. Media exposure to armed conflict: dispositional optimism and self-mastery moderate distress and post-traumatic symptoms among adolescents. Int J Environ Res Public Health. 2022;19(18):11216. doi:10.3390/ijerph191811216
36. Darlington RB, Hayes AF. Regression Analysis and Linear Models: Concepts, Applications, and Implementation. The Guilford Press: New York; 2017.
37. Hayes AF. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach.
38. Hayes AF, Rockwood NJ. Regression-based statistical mediation and moderation analysis in clinical research: observations, recommendations, and implementation. Behav Res Ther. 2017;98:39–57. doi:10.1016/j.brat.2016.11.001
39. Hair JF, Black WC, Babin BJ, et al. Multivariate Data Analysis.
40. Mooney C, Fetter K, Gross BW, Rinehart C, Lynch C, Rogers FB. A preliminary analysis of compassion satisfaction and compassion fatigue with considerations for nursing unit specialization and demographic factors. J Trauma Nurs. 2017;24(3):158–163. doi:10.1097/JTN.0000000000000284
41. Von Rueden KT, Hinderer KA, McQuillan KA, et al. Secondary traumatic stress in trauma nurses: prevalence and exposure, coping, and personal/environmental characteristics. J Trauma Nurs. 2010;17(4):191–200. doi:10.1097/JTN.0b013e3181ff2607
42. Maroof N, Sikandar MZ, Nawaz H, Shah SIA. Professional quality of life and its association with work experience and income among healthcare worker: quality of life among healthcare workers. J Aziz Fatm Med Den College. 2019;1(2):55–59. doi:10.55279/jafmdc.v1i2.50
43. Thompson-Brenner H, Satir DA, Franko DL, Herzog DB. Clinician reactions to patients with eating disorders: a review of the literature. Psychiatr Serv. 2012;63(1):73–78. doi:10.1176/appi.ps.201100050
44. Hobfoll SE. Conservation of resources. A new attempt at conceptualizing stress. Am Psychol. 1989;44(3):513–524. doi:10.1037//0003-066x.44.3.513
45. Zerach G. Compassion fatigue and compassion satisfaction among residential child care workers: the role of personality resources. Resid Treat Child Youth. 2013;30(1):72–91. doi:10.1080/0886571X.2012.761515
46. Rohlf VI, Scotney R, Monaghan H, Bennett P. Predictors of professional quality of life in veterinary professionals. J Vet Med Educ. 2022;49(3):372–381. doi:10.3138/jvme-2020-0144
47. Garrosa E, Moreno-Jiménez B, Rodríguez-Muñoz A, Rodríguez-Carvajal R. Role stress and personal resources in nursing: a cross-sectional study of burnout and engagement. Int J Nurs Stud. 2011;48(4):479–489. doi:10.1016/j.ijnurstu.2010.08.004
48. Steger M. Creating meaning and purpose at work. In: Oades LG, Steger M, Delle Fave A, Passmore J, editors. The Wiley Blackwell Handbook of the Psychology of Positivity and Strengths-Based Approaches at Work. Wiley & Sons; 2017:60–81.
49. Negri L, Cilia S, Falautano M, et al. Job satisfaction among physicians and nurses involved in the management of multiple sclerosis: the role of happiness and meaning at work. Neurol Sci. 2022;43(3):1903–1910. doi:10.1007/s10072-021-05520-8
50. Carver CS, Scheier MF. The hopeful optimist. Psychol Inq. 2002;13(4):288–290.
51. Wonderlich S, Mitchell JE, Crosby RD, et al. Minimizing and treating chronicity in the eating disorders: a clinical overview. Int J Eat Disord. 2012;45(4):467–475. doi:10.1002/eat.20978
52. Hay P, Chinn D, Forbes D, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the treatment of eating disorders. Aust N Z J Psychiatry. 2014;48(11):977–1008. doi:10.1177/0004867414555814
53. Thaler L, Booij L, Burnham N, et al. Predictors of non-completion of a day treatment program for adults with eating disorders. Eur Eat Disord Rev. 2022;30(2):146–155. doi:10.1002/erv.2879
54. Israel Ministry of Health. Health ministry report: the manpower in the health professions; 2021. Available from: https://www.gov.il/BlobFolder/reports/health-professions-manpower/he/files_publications_units_info_manpower2021.pdf.
55. Malloy DC, Sevigny P, Hadjistavropoulos T, et al. Perceptions of the effectiveness of ethical guidelines: an international study of physicians. Med Health Care Philos. 2009;12(4):373–383. doi:10.1007/s11019-009-9212-0
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.