Back to Journals » Risk Management and Healthcare Policy » Volume 19
Professional Compromise and Its Association with Burnout, Job Satisfaction, and Patient Satisfaction Among Physicians in a Chinese Tertiary Hospital
Received 24 February 2026
Accepted for publication 24 April 2026
Published 16 June 2026 Volume 2026:19 601873
DOI https://doi.org/10.2147/RMHP.S601873
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gulsum Kaya
Yulin Zeng,1 Ping Han1,2
1The School of Management, Xi’an Jiaotong University, Xi’an City, 710049, People’s Republic of China; 2The Key Laboratory of the Ministry of Education for Process Management & Efficiency Engineering, Xi’an, 710049, People’s Republic of China
Correspondence: Ping Han, Email [email protected]
Background: Physician burnout poses a global challenge to healthcare systems. Professional compromise—pressure on physicians to deviate from clinical judgment or professional standards due to systemic constraints—may contribute to burnout, yet evidence from non-Western settings remains limited. This study examined the prevalence of professional compromise among physicians at a Chinese tertiary hospital and its associations with burnout, job satisfaction, turnover intention, and departmental patient satisfaction.
Methods: A cross-sectional survey was conducted between January and March 2025 at a tertiary hospital in Zhejiang Province, China (n=120 physicians; 10 clinical departments; response rate 80.0%). Professional compromise was measured with a validated five-item instrument adapted from the Measure of Moral Distress for Healthcare Professionals; burnout was assessed using the Emotional Exhaustion subscale of the Maslach Burnout Inventory (licensed from Mind Garden, Inc). Pearson correlations, independent t-tests, and chi-square tests examined associations; effect sizes were quantified using Cohen’s d and odds ratios.
Results: The mean professional compromise score was 3.85 (SD 0.55) on a 1– 5 scale, with 50.0% of physicians reporting frequent compromise (score ≥ 4). Obstetrics and Gynaecology and Emergency Medicine departments exhibited the highest compromise rates. Professional compromise correlated positively with burnout (r=0.587, p< 0.001) and negatively with job satisfaction (r=− 0.347, p< 0.001). High-compromise physicians had substantially higher burnout (Cohen’s d=0.97), lower job satisfaction (Cohen’s d=0.57), and greater turnover intention (55.0% vs. 28.3%; OR=3.09, 95% CI 1.41– 6.77). At the department level (n=10), professional compromise correlated negatively with patient satisfaction (r=− 0.929, p< 0.001).
Conclusion: Professional compromise was prevalent and robustly associated with adverse clinician outcomes. These findings suggest that systemic contributors to professional compromise warrant attention in strategies to improve clinician well-being and healthcare quality. Longitudinal multi-site research is needed to confirm these associations and evaluate targeted interventions.
Keywords: professional compromise, moral distress, physician burnout, job satisfaction, patient satisfaction, healthcare workforce
Background
Physician burnout has emerged as a pressing concern for healthcare systems globally. Prevalence estimates range from 40% to over 60% by specialty and region, with occurrences documented across high-, middle-, and low-income economies.1–3 In China, the combination of rapid healthcare expansion, high patient volumes, and short consultation times has fostered conditions for elevated burnout. Recent national surveys indicate over 65% of hospital-affiliated physicians in China experience burnout, with disproportionately high rates in tertiary regional referral hospitals.4,5
Burnout is characterized by three core dimensions: emotional exhaustion, depersonalization, and diminished personal accomplishment.6 Beyond individual distress, physician burnout affects patient care quality, safety, and satisfaction. Systematic reviews and meta-analyses have established associations between burnout and increased medical adverse events, reduced adherence to clinical guidelines, lower patient satisfaction, and higher turnover intentions.7–9 These findings have led to the recognition of physician well-being as a healthcare quality indicator and calls for systemic interventions targeting burnout’s root causes.10,11
An understudied contributor to burnout is professional compromise, defined as physicians facing systemic, organizational, or administrative pressures to act against their clinical judgment, professional standards, or ethical values.12,13 Examples include abbreviating consultations to meet throughput targets, adhering to resource-driven treatment protocols inconsistent with individualized optimal care, complying with administrative mandates conflicting with clinical priorities, or administering family-requested treatments contrary to patient preferences.
Professional compromise shares conceptual overlap with moral distress—originally described in nursing as knowing the ethically appropriate action but being constrained from pursuing it.14,15 Recurrent moral distress may accumulate as “moral residue,” a persistent psychological burden contributing to burnout and attrition.15 It also aligns with moral injury, a military psychology-derived term describing cumulative harm from repeated violations of one’s moral code.12,16
Empirical research linking moral distress to adverse clinician outcomes has grown substantially in recent years. A meta-analysis by Lamiani et al (30 studies) reported pooled correlations of 0.42 (moral distress-burnout), 0.38 (moral distress-turnover intention), and 0.45 (moral distress-psychological distress).17 Qualitative studies in the US, UK, and Israel have linked administrative burdens, misaligned managerial-clinical priorities, and resource scarcity to physician dissatisfaction and career reconsideration.18,19 The COVID-19 pandemic amplified attention to these issues, with studies documenting heightened moral distress among frontline workers facing resource shortages, triage dilemmas, and ethical conflicts.20,21
Despite this, quantitative research on physician professional compromise in non-Western contexts remains scarce. Chinese tertiary hospitals have unique structural features (daily outpatient volumes of 3000–5000, 3–5 minute consultations, hierarchical cultures, and resource-expectation mismatches) that may shape professional compromise’s prevalence and consequences.22,23 These systemic pressures are hypothesized to frequently compel physicians to compromise professional standards. These challenges are not unique to China; similar patterns of constrained clinical autonomy and moral distress have been documented among healthcare professionals in European and other Eurasian healthcare systems,24 underscoring the international relevance of this research agenda.
Investigating associations between professional compromise and organizational outcomes (eg., patient satisfaction) is particularly relevant to healthcare administrators and policymakers. Higher department-level professional compromise may correlate with lower patient satisfaction, suggesting its consequences extend beyond individual well-being to organizational performance. While non-causal, such evidence could inform hospital management and policy on resource allocation and workflow optimization.
Accordingly, this study had two main objectives: (1) to quantify professional compromise prevalence among physicians in a Chinese tertiary hospital; (2) to examine its associations with burnout, job satisfaction, turnover intention, and departmental patient satisfaction. We hypothesized higher professional compromise would correlate positively with burnout and turnover intention, and negatively with job satisfaction and departmental patient satisfaction.
Methods
Study Design and Setting
This cross-sectional observational study was conducted between January and March 2025 at a tertiary general hospital located in a medium-sized city in Zhejiang Province, eastern China. The hospital serves as the regional referral centre for the surrounding counties and districts, with approximately 1,500 inpatient beds, more than 2,800 employees including approximately 800 physicians, and a comprehensive range of medical and surgical specialties. The institution handles approximately 4,200 outpatient visits and 150 emergency department visits daily. These characteristics are typical of prefecture-level tertiary hospitals in eastern China.
The study protocol received ethical approval from the hospital’s Institutional Review Board prior to commencement of data collection. All study procedures were conducted in compliance with the principles of the Declaration of Helsinki. Participation was voluntary, and all respondents provided written informed consent before completing study questionnaires.
Participants
Physicians from 10 clinical departments were eligible for participation: internal medicine, general surgery, paediatrics, obstetrics and gynaecology, emergency medicine, anaesthesiology, intensive care unit (ICU), neurology, oncology, and orthopaedics. These departments were purposively selected to represent diverse clinical environments, patient populations, acuity levels, and practice patterns within the hospital.
Stratified proportional sampling was employed to ensure adequate representation across departments. Approximately 12 physicians were recruited from each department, with the exact number adjusted slightly based on departmental size. Within each department, eligible physicians were invited to participate during scheduled departmental meetings.
Inclusion criteria were: (1) full-time employment as a licensed physician at the study hospital; (2) at least one year of continuous clinical experience at the institution; and (3) active engagement in direct patient care during the study period. Exclusion criteria were: (1) positions that were purely administrative without clinical patient care responsibilities; (2) extended leave (defined as greater than three months) during the study period, including sick leave, parental leave, or sabbatical; and (3) participation in the pilot-testing phase of the study instruments.
Of 150 physicians meeting eligibility criteria who were invited to participate, 124 agreed and returned questionnaires (participation rate: 82.7%). After exclusion of four questionnaires with excessive missing data (defined as more than 20% of items incomplete), 120 physicians were included in the final analysis, yielding an effective response rate of 80.0%.
Sample size considerations were informed by two analytic goals. For correlation analyses, a sample of 120 provides approximately 80% power to detect correlations of r≥0.25 at a two-tailed α level of 0.05. For group comparisons with balanced groups (n=60 per group), this sample provides approximately 80% power to detect effect sizes of d≥0.52.
Measures
Professional compromise was measured using a five-item instrument adapted from the Measure of Moral Distress for Healthcare Professionals (MMD-HP) developed by Epstein et al25 The original MMD-HP is a 27-item instrument designed to assess both the frequency and intensity of situations in which healthcare professionals experience constraints on taking ethically appropriate action. The instrument has demonstrated good psychometric properties in North American samples and is publicly available for research use with appropriate attribution.25
For the present study, we adapted the MMD-HP for use in the Chinese tertiary hospital context through a systematic process. First, two bilingual researchers—one physician with clinical experience in Chinese hospitals and one health services researcher with expertise in cross-cultural measurement—independently reviewed all 27 original items and identified those most relevant to the Chinese hospital environment. Second, we employed forward-backward translation methodology consistent with published guidelines for cross-cultural instrument adaptation.26 The selected items were independently translated from English to Mandarin Chinese by two translators; discrepancies were resolved through discussion. A third translator, blinded to the original English version, back-translated the Chinese version to English; the back-translation was compared with the original for conceptual equivalence.
Third, a five-member expert panel comprising two internists, one surgeon, one nurse manager, and one medical ethicist evaluated content validity and cultural appropriateness of the candidate items. Panel members rated each item for relevance (1–4 scale) and clarity (1–4 scale); items with content validity index scores below 0.80 were revised or eliminated. Fourth, cognitive interviews were conducted with 10 physicians (not included in the main sample) to assess item comprehension and response processes. Finally, a pilot study (n=30 physicians) assessed preliminary psychometric properties.
The final instrument comprised five items addressing: (1) providing care perceived as lower quality than desired owing to time constraints; (2) following institutional policies that conflicted with clinical judgment; (3) delivering treatments inconsistent with patient preferences due to pressure from family members; (4) accepting resource allocation decisions that compromised the quality of care one could provide; and (5) acting against professional standards to meet administrative requirements or performance metrics. Each item was rated on a five-point Likert scale with anchors: 1 (never), 2 (rarely), 3 (sometimes), 4 (often), and 5 (very often). Scores were averaged across the five items, with higher scores indicating more frequent professional compromise.
In the present sample, the adapted instrument demonstrated acceptable internal consistency (Cronbach’s α=0.86). Exploratory factor analysis supported a unidimensional structure, with a single factor accounting for 62.4% of item variance and all factor loadings exceeding 0.65. Confirmatory factor analysis yielded adequate fit indices: comparative fit index (CFI)=0.95; Tucker-Lewis index (TLI)=0.92; root mean square error of approximation (RMSEA)=0.06 (90% CI 0.02–0.10); and standardised root mean square residual (SRMR)=0.04. The Chinese-language version of the instrument is available from the corresponding author for research purposes.
Burnout was assessed using the Emotional Exhaustion (EE) subscale of the Maslach Burnout Inventory–Human Services Survey (MBI-HSS).6 The MBI-HSS is the most widely used measure of burnout in healthcare settings and has been employed in hundreds of studies across diverse populations and countries. The complete MBI-HSS comprises three subscales measuring emotional exhaustion, depersonalization, and personal accomplishment; we focused on the emotional exhaustion subscale because it is considered the core component of burnout and has shown the strongest and most consistent associations with work-related outcomes in prior research.27
The Emotional Exhaustion subscale comprises nine items measuring the frequency of feelings such as emotional depletion, fatigue, frustration, and strain related to one’s work. Each item is rated on a seven-point frequency scale from 0 (never) to 6 (every day), yielding total scores ranging from 0 to 54, with higher scores indicating greater emotional exhaustion. Established cutoff values published in the MBI manual categorise scores as: low burnout (<17), moderate burnout (17–26), and high burnout (>26).6
The MBI is a copyrighted instrument published by Mind Garden, Inc. (Menlo Park, California, USA). Research use requires purchase of a licence; a licence permitting use in the present study was obtained. We used the validated Chinese-language version of the MBI-HSS, which has demonstrated acceptable psychometric properties in prior studies of Chinese healthcare workers including physicians, nurses, and other clinical staff.28,29 In the present sample, internal consistency of the Emotional Exhaustion subscale was excellent (Cronbach’s α=0.89).
Job satisfaction was assessed using a single-item global measure with the stem: “Overall, how satisfied are you with your job?” Responses were provided on a five-point scale with anchors: 1 (very dissatisfied), 2 (dissatisfied), 3 (neither satisfied nor dissatisfied), 4 (satisfied), and 5 (very satisfied).
Single-item measures of job satisfaction have demonstrated acceptable validity compared with multi-item scales in multiple studies, including research specifically examining physician populations.30,31 Meta-analytic evidence indicates that single-item and multi-item measures of overall job satisfaction yield similar correlations with theoretically related constructs.30 Single-item measures also offer practical advantages including reduced respondent burden, which is particularly relevant in surveys incorporating multiple constructs and administered to busy clinical populations.
Turnover intention was assessed using a single dichotomous item: “In the past 12 months, have you seriously considered leaving your current position?” (response options: yes/no). This approach is consistent with methods employed in prior physician workforce studies in the United States and internationally.1,32 Turnover intention measured in this manner has demonstrated predictive validity for actual turnover behaviour in longitudinal studies.33
Departmental patient satisfaction data were obtained from the hospital’s Quality Management Office. Patient satisfaction scores, expressed as the percentage of patients indicating satisfaction or high satisfaction with the care received, were extracted from routine post-discharge surveys conducted during the study period (January–March 2025).
These surveys employed the standardised patient experience questionnaire mandated by China’s National Health Commission for all tertiary hospitals as part of the national healthcare quality monitoring programme.34 The questionnaire assesses multiple dimensions of patient experience including communication with physicians, responsiveness of staff, pain management, discharge information, and overall satisfaction. For the present analysis, we used the overall satisfaction item, which asked patients to rate their overall satisfaction with the care received on a five-point scale; scores were aggregated as the percentage of respondents selecting “satisfied” or “very satisfied.”
Patient satisfaction surveys were administered by hospital quality management staff who were not involved in the research study and were blinded to study hypotheses. Data were extracted by administrative personnel and linked to departments using department identifiers; no individual patient data were accessed by the research team.
Participants reported their age (in years), sex (male/female), professional title (resident physician, attending physician, or senior consultant), years of clinical experience, and primary department affiliation.
Data Collection Procedures
Paper-based questionnaires were distributed during scheduled departmental meetings by trained research assistants who were not affiliated with the participating departments. Participants were allocated approximately 15 minutes to complete the questionnaire independently. To maintain confidentiality, completed questionnaires were placed in sealed envelopes and returned directly to the research assistants rather than to departmental supervisors. No identifying information beyond department affiliation was collected on the questionnaires.
Data entry was performed independently by two research assistants using double-entry verification. Discrepancies between the two entries were resolved by reference to the original paper questionnaires. Data were stored on a password-protected computer accessible only to the research team.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics version 27.0 (IBM Corp., Armonk, NY, USA) and R version 4.5.2 (R Foundation for Statistical Computing, Vienna, Austria). A two-sided p-value less than 0.05 was considered statistically significant for all tests.
Continuous variables were summarised using means with standard deviations (SD) and ranges; categorical variables were presented as frequencies and percentages. Distributions of continuous variables were assessed for normality using Shapiro–Wilk tests and visual inspection of histograms and quantile-quantile (Q-Q) plots. All key continuous variables (professional compromise, burnout, job satisfaction, age, years of experience) approximated normal distributions, supporting the use of parametric statistical tests.
For between-group comparisons, physicians were classified into two categories based on their professional compromise scores: low-compromise (mean score <4.00) and high-compromise (mean score ≥4.00). This threshold was selected based on semantic interpretation of the response scale anchors—a score of 4 corresponds to “often” and a score of 5 to “very often,” so scores ≥4.00 identify physicians who report experiencing professional compromise frequently or habitually. This threshold also approximates the sample median (50th percentile), yielding balanced groups for comparison. We acknowledge that dichotomisation of continuous variables entails loss of statistical information and power; however, this approach facilitates clinical interpretation and enables comparison of findings with prior studies that have employed similar categorisation strategies.
Differences between low-compromise and high-compromise groups in continuous outcomes (burnout score, job satisfaction score) were examined using independent samples t-tests. Equality of variances was assessed using Levene’s test; where the assumption of equal variances was violated, Welch’s t-test with adjusted degrees of freedom was employed. Differences in categorical outcomes (turnover intention) were examined using Pearson’s chi-square test. Effect sizes were calculated to quantify the magnitude of between-group differences: Cohen’s d for continuous variables, interpreted according to conventional benchmarks as small (approximately 0.2), medium (approximately 0.5), and large (approximately 0.8);35 and odds ratios (OR) with 95% confidence intervals (CI) for categorical variables.
Pearson correlation coefficients (r) were calculated to quantify bivariate associations between continuous variables at the individual level (n=120). Correlations were interpreted according to conventional guidelines: small (r≈0.10), medium (r≈0.30), and large (r≈0.50).35 The 95% confidence intervals for correlations were calculated using Fisher’s z-transformation.
At the department level (n=10 departments), Pearson correlations examined the association between departmental mean professional compromise scores (aggregated from individual physician scores) and departmental patient satisfaction percentages. Given the small number of departments, these analyses should be regarded as exploratory and hypothesis-generating rather than confirmatory.
We emphasise that the cross-sectional study design permits identification of associations but does not permit causal inference. Throughout the presentation of findings, we describe relationships in terms of associations and correlations rather than effects or impacts, and we refrain from language implying causation.
Reporting Guidelines
This study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies.36 The completed STROBE checklist is provided as Additional File 1.
Results
Participant Characteristics
A total of 120 physicians from 10 clinical departments completed the survey and were included in the final analysis. Table 1 presents the demographic and professional characteristics of the study sample. The mean age of participants was 38.46 years (SD 7.34; range 26–60), and 69 participants (57.5%) were male. The distribution of professional titles was as follows: resident physicians, 40 (33.3%); attending physicians, 56 (46.7%); and senior consultants, 24 (20.0%). The mean duration of clinical experience was 12.45 years (SD 6.56; range 2–28).
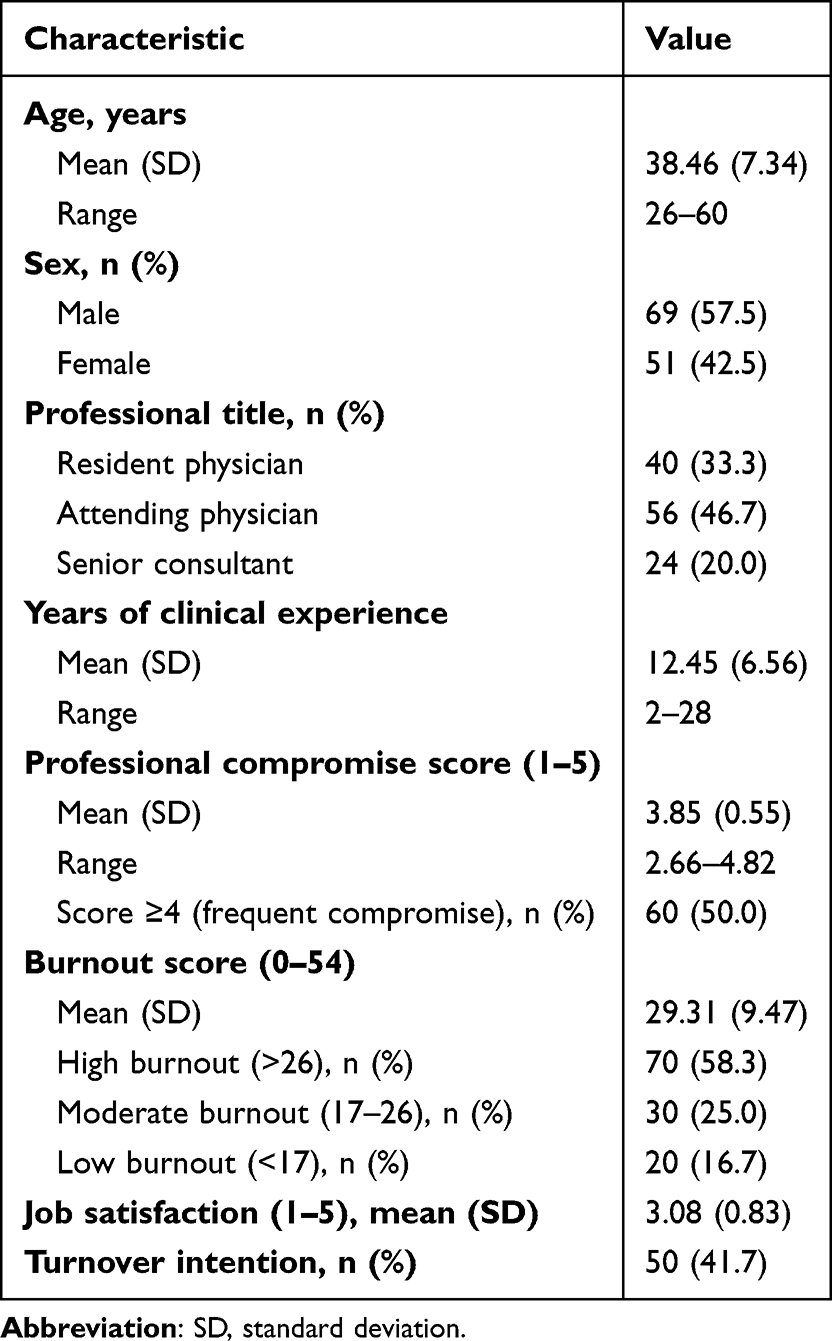 |
Table 1 Characteristics of Participating Physicians (N=120) |
Prevalence of Professional Compromise
The mean professional compromise score across all participants was 3.85 (SD 0.55) on the 1–5 scale, corresponding to a response pattern between “sometimes” (3) and “often” (4). Individual scores ranged from 2.66 to 4.82. The distribution of professional compromise scores approximated normality (Shapiro–Wilk W=0.98, p=0.11), with slight negative skewness indicating a tendency toward higher scores.
Applying the pre-specified threshold, exactly half of the participating physicians (n=60, 50.0%) scored 4.00 or above on the professional compromise scale, indicating that they experienced professional compromise frequently or very frequently. This prevalence suggests that professional compromise is a common rather than exceptional phenomenon among physicians at this institution.
Burnout, Job Satisfaction, and Turnover Intention
The mean burnout score on the Emotional Exhaustion subscale was 29.31 (SD 9.47; range 9–52). Applying the conventional threshold values established in the MBI manual, the distribution of physicians across burnout categories was as follows: high burnout (score >26), 70 physicians (58.3%); moderate burnout (score 17–26), 30 physicians (25.0%); and low burnout (score <17), 20 physicians (16.7%). Thus, nearly three in five participating physicians scored in the high burnout range.
The mean job satisfaction score was 3.08 (SD 0.83) on the 1–5 scale, corresponding approximately to “neither satisfied nor dissatisfied.” Scores ranged from 1 to 5, with the distribution approximately symmetric around the mean.
Turnover intention—operationalised as having seriously considered leaving one’s current position within the past 12 months—was reported by 50 physicians (41.7%). This indicates that more than two in five participating physicians had recently contemplated departure from their positions.
Association Between Professional Compromise and Burnout
At the individual level (N=120), professional compromise demonstrated a strong positive correlation with burnout (Pearson r=0.587, 95% CI 0.45–0.70, p<0.001). This correlation indicates that higher professional compromise scores were associated with higher burnout scores, and that approximately 34.5% of the variance in burnout scores was shared with professional compromise scores (r2=0.345).
Figure 1 displays the scatter plot illustrating the relationship between professional compromise scores (x-axis) and burnout scores (y-axis) among the 120 physicians. Each point represents one physician. The data points demonstrate a clear positive linear trend, with burnout scores increasing as professional compromise scores increase. The fitted linear regression line (burnout = −8.45 + 9.82 × compromise) indicates that each one-unit increase in professional compromise score was associated with an increase of approximately 10 points in burnout score. The shaded band surrounding the regression line represents the 95% confidence interval, demonstrating that this relationship was estimated with reasonable precision.
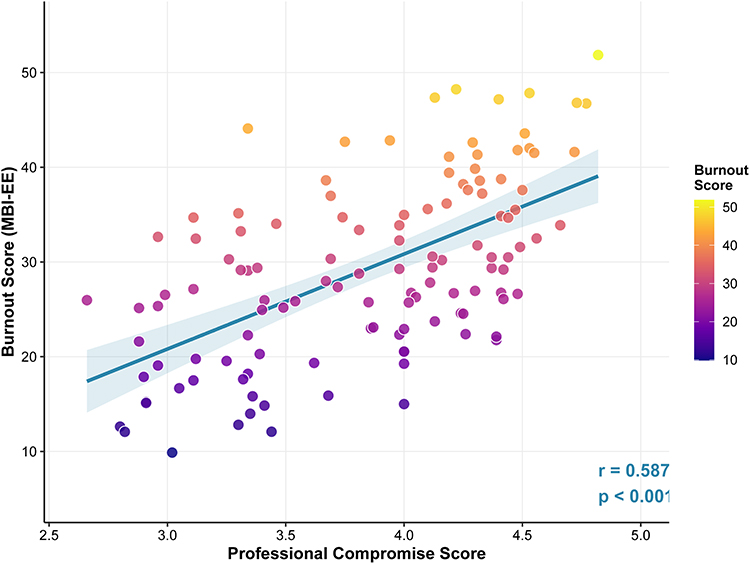 |
Figure 1 Association between professional compromise and burnout among physicians (N=120). Scatter plot displaying the relationship between professional compromise scores (x-axis, scale 1–5) and burnout scores (y-axis, Emotional Exhaustion subscale, scale 0–54) for 120 individual physicians. Each point represents one physician. The solid diagonal line represents the fitted linear regression line (burnout = −8.45 + 9.82 × compromise), indicating that each one-unit increase in professional compromise score was associated with an approximately 10-point increase in burnout score. The shaded band represents the 95% confidence interval around the regression line. Points are colour-coded by burnout level according to the legend, with darker colours indicating higher burnout scores. The Pearson correlation coefficient was r=0.587 (p<0.001), indicating a strong positive association. |
Visual inspection of Figure 1 reveals additional patterns of interest. Physicians with professional compromise scores above 4.0 (the high-compromise group) clustered predominantly in the upper portion of the burnout distribution, with the majority exhibiting burnout scores above 30. In contrast, physicians with lower compromise scores showed greater variability in burnout levels, with scores spanning the full range from low to high burnout. This pattern suggests that while low professional compromise does not guarantee low burnout (other factors also contribute), high professional compromise appears consistently associated with elevated burnout.
Association Between Professional Compromise and Job Satisfaction
Professional compromise was negatively correlated with job satisfaction at the individual level (r=−0.347, 95% CI −0.49 to −0.18, p<0.001). This correlation, while statistically significant and of medium magnitude, was weaker than the correlation between professional compromise and burnout. Approximately 12.0% of the variance in job satisfaction scores was shared with professional compromise scores (r2=0.120).
Additional Correlational Findings
Burnout and job satisfaction were negatively correlated with each other (r=−0.412, p<0.001), a finding consistent with extensive prior literature documenting that emotional exhaustion is associated with reduced work satisfaction.
Neither age nor years of clinical experience correlated significantly with professional compromise (age: r=0.08, p=0.39; years of experience: r=0.11, p=0.24). These null findings suggest that professional compromise was not confined to physicians at particular career stages; rather, it appeared to affect physicians across the spectrum from early-career residents to senior consultants with decades of experience.
Comparison Between Low-Compromise and High-Compromise Groups
Table 2 presents comparisons of outcomes between physicians classified into low-compromise (professional compromise score <4.00; n=60) and high-compromise (score ≥4.00; n=60) groups. The two groups were comparable in demographic and professional characteristics: age (mean 38.2 vs. 38.7 years; t=0.42, p=0.68), sex distribution (55.0% vs. 60.0% male; χ2=0.32, p=0.57), and years of clinical experience (mean 12.1 vs. 12.8 years; t=0.63, p=0.53). This similarity in background characteristics increases confidence that observed differences in outcomes are attributable to professional compromise rather than to demographic confounders.
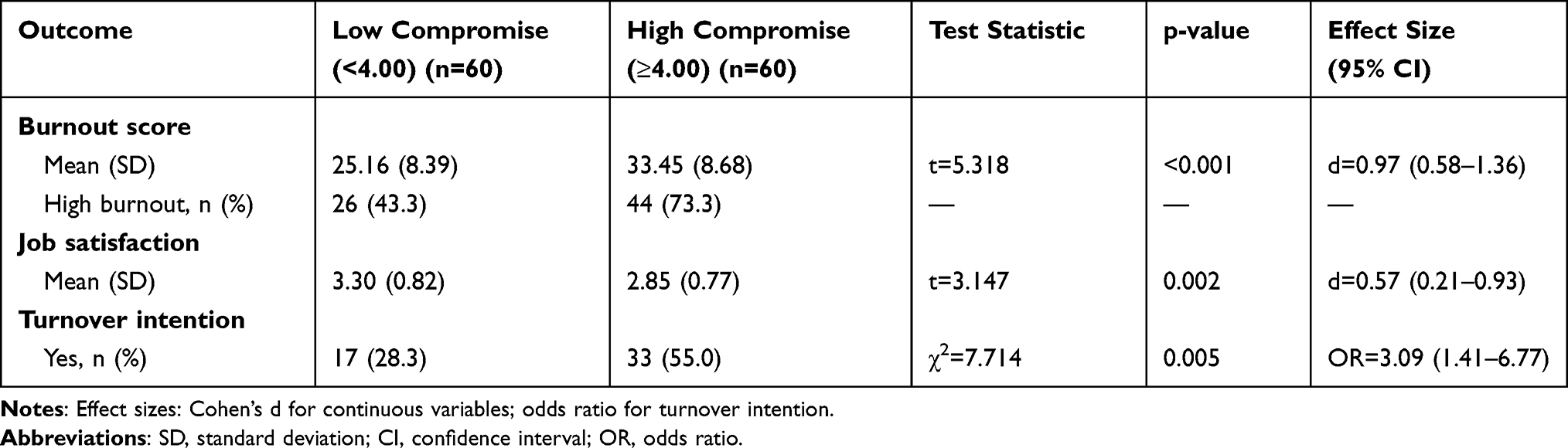 |
Table 2 Comparison of Outcomes Between Low-Compromise and High-Compromise Groups |
Burnout. High-compromise physicians exhibited substantially higher burnout scores than low-compromise physicians (mean 33.45, SD 8.68 vs. mean 25.16, SD 8.39; t=5.318, p<0.001). The magnitude of this difference was large according to conventional benchmarks (Cohen’s d=0.97, 95% CI 0.58–1.36), indicating that the mean burnout score of the high-compromise group was approximately one standard deviation higher than that of the low-compromise group. In practical terms, this translates to a difference of 8.3 points on the 54-point Emotional Exhaustion scale.
The clinical significance of this difference is further illustrated by examining the distribution across burnout categories. Among high-compromise physicians, 44 (73.3%) scored in the high burnout range (>26) compared with only 26 (43.3%) of low-compromise physicians. Conversely, only 5 (8.3%) high-compromise physicians scored in the low burnout range (<17) compared with 15 (25.0%) of low-compromise physicians.
Job satisfaction. Job satisfaction was significantly lower among high-compromise physicians (mean 2.85, SD 0.77) than among low-compromise physicians (mean 3.30, SD 0.82; t=3.147, p=0.002). The effect size was medium (Cohen’s d=0.57, 95% CI 0.21–0.93), indicating a clinically meaningful though more modest difference than observed for burnout.
Turnover intention. Turnover intention was substantially more prevalent among high-compromise physicians (33 of 60, 55.0%) than among low-compromise physicians (17 of 60, 28.3%; χ2=7.714, p=0.005). The odds of reporting turnover intention were approximately three times higher in the high-compromise group than in the low-compromise group (OR=3.09, 95% CI 1.41–6.77).
Visual summary of group comparisons. Figure 2 provides a comprehensive visual summary of the differences between low-compromise and high-compromise groups across the three outcomes using raincloud plots. This visualisation approach combines density distributions (showing the shape of each group’s data), box plots (showing medians and interquartile ranges), and individual data points (showing raw data values), enabling readers to appreciate both summary statistics and underlying data distributions.
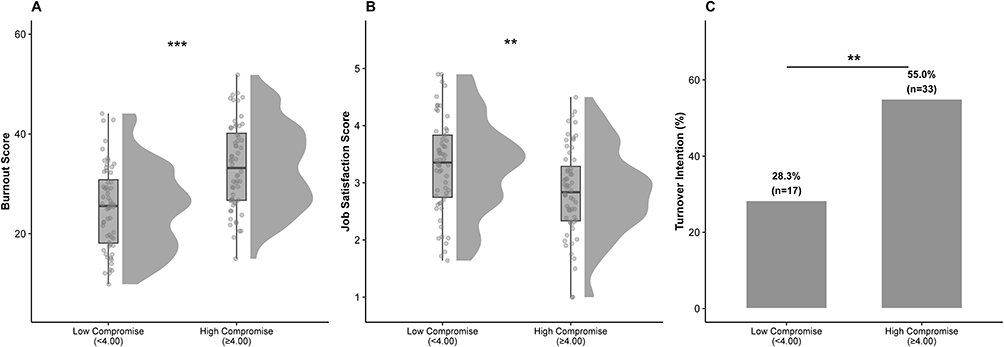 |
Figure 2 Comparison of outcomes between low-compromise and high-compromise physician groups. Raincloud plots displaying distributions of outcomes for low-compromise (professional compromise score <4.00; n=60) and high-compromise (score ≥4.00; n=60) groups. Each panel combines a density curve (showing distribution shape), a box plot (showing median and interquartile range), and individual data points (showing raw values). (A) Burnout scores. The high-compromise group showed a distribution shifted substantially toward higher burnout values compared with the low-compromise group (mean 33.45 vs. 25.16; t=5.318; p<0.001; Cohen’s d=0.97). (B) Job satisfaction scores. The high-compromise group showed lower job satisfaction than the low-compromise group (mean 2.85 vs. 3.30; t=3.147; p=0.002; Cohen’s d=0.57). (C) Turnover intention. Bar heights indicate the percentage of physicians reporting turnover intention in each group. Turnover intention was more prevalent in the high-compromise group (55.0%) than in the low-compromise group (28.3%; χ2=7.714; p=0.005; OR=3.09). Significance annotations: **p<0.01; ***p<0.001. |
Panel A of Figure 2 displays the distribution of burnout scores in each group. The density curve for the high-compromise group is shifted substantially to the right (toward higher burnout values) compared with the low-compromise group. The median burnout score (indicated by the horizontal line within each box) is clearly higher for the high-compromise group. Individual data points reveal that while some overlap exists between groups, the high-compromise group contains few physicians with low burnout scores.
Panel B displays job satisfaction scores. The density distribution for the high-compromise group is shifted to the left (toward lower satisfaction values), and the median is lower than for the low-compromise group. The difference between groups, while significant, is visually less pronounced than for burnout, consistent with the smaller effect size.
Panel C presents turnover intention as percentages with bar height indicating the proportion of physicians reporting turnover intention in each group. The high-compromise group shows a turnover intention rate nearly double that of the low-compromise group (55.0% vs. 28.3%). Statistical significance annotations indicate p<0.01 for job satisfaction and turnover intention comparisons, and p<0.001 for the burnout comparison.
Department-Level Association Between Professional Compromise and Patient Satisfaction
Table 3 presents descriptive statistics for each of the 10 participating departments, including the number of physicians sampled, mean professional compromise score, mean burnout score, and patient satisfaction percentage. Each department contributed 12 physicians to the sample.
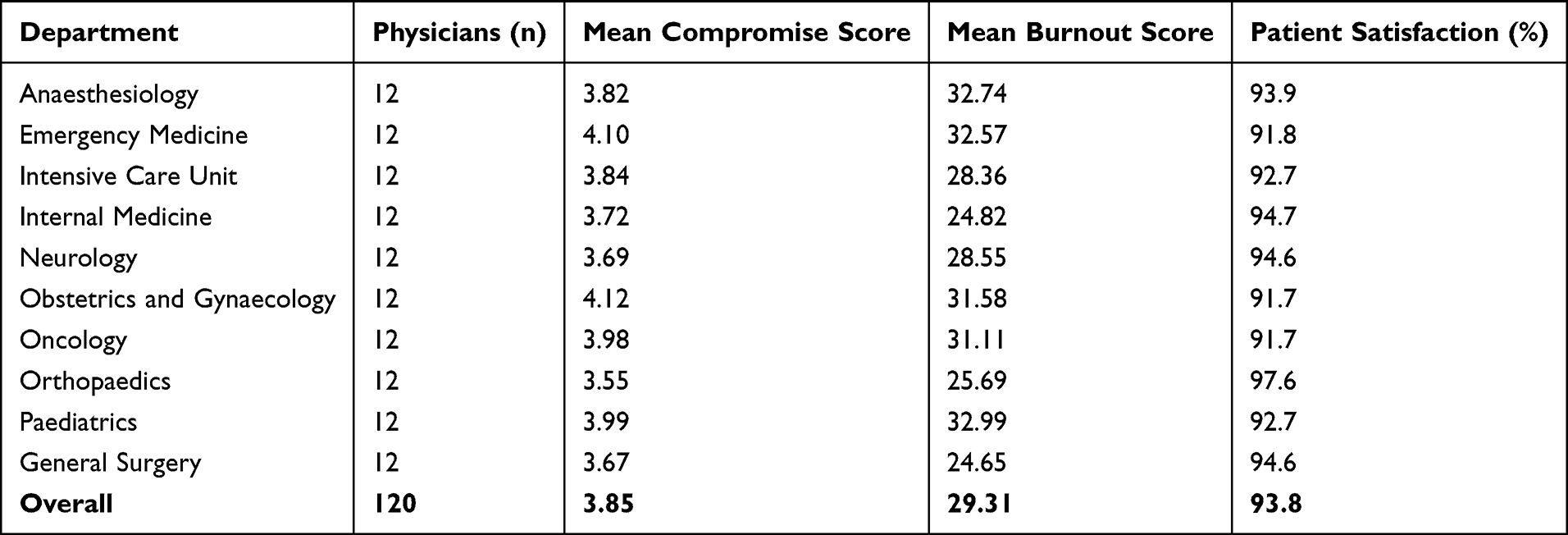 |
Table 3 Departmental Characteristics and Patient Satisfaction (n=10 Departments) |
Considerable variation existed across departments. Departmental mean professional compromise scores ranged from 3.55 (Orthopaedics, indicating the lowest average frequency of compromise) to 4.12 (Obstetrics and Gynaecology, indicating the highest average frequency). Departmental mean burnout scores ranged from 24.65 (General Surgery) to 32.99 (Paediatrics). Patient satisfaction ranged from 91.7% (Oncology, Obstetrics and Gynaecology) to 97.6% (Orthopaedics), with an overall mean across departments of 93.8% (SD 1.9%).
At the department level (n=10), the Pearson correlation between mean professional compromise and patient satisfaction was strongly negative (r=−0.929, p<0.001). This indicates that departments with higher average levels of professional compromise among their physicians tended to have lower patient satisfaction scores.
Figure 3 displays this relationship in a scatter plot, with each point representing one department. The x-axis shows the departmental mean professional compromise score; the y-axis shows the patient satisfaction percentage. Point size is proportional to the number of physicians in each department (all departments had 12 physicians in this study, so points are of equal size). Department labels identify each data point.
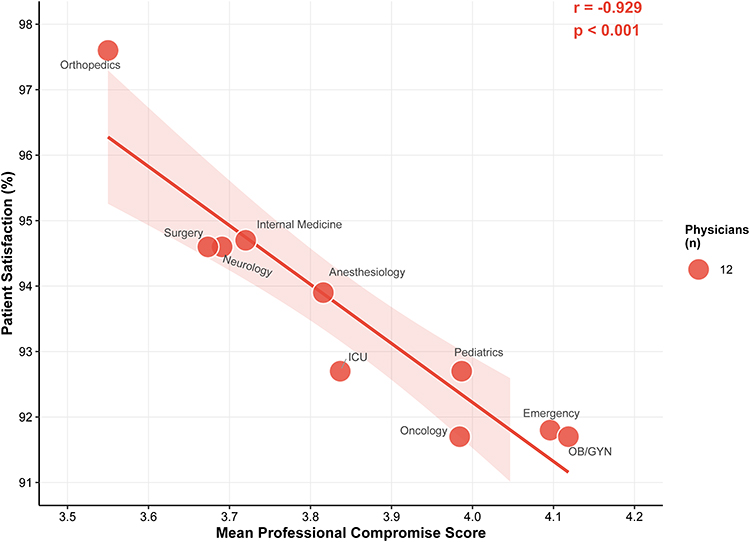 |
Figure 3 Association between departmental mean professional compromise and patient satisfaction (n=10 departments). Scatter plot displaying the relationship between departmental mean professional compromise scores (x-axis) and patient satisfaction percentages (y-axis) across 10 clinical departments. Each point represents one department and is labelled with the department name. The solid line represents the linear regression fit; the shaded band indicates the 95% confidence interval. The Pearson correlation coefficient was r=−0.929 (p<0.001), indicating a strong negative association at the department level. Departments with lower mean professional compromise (e.g., Orthopaedics, 3.55) tended to have higher patient satisfaction (e.g., 97.6%), while departments with higher mean compromise (e.g., Obstetrics and Gynaecology, 4.12) tended to have lower patient satisfaction (e.g., 91.7%). Note: Given the small number of departments (n=10), this finding should be interpreted as exploratory; the ecological nature of the analysis does not permit inference to individual-level relationships. |
The linear regression line demonstrates a steep negative slope, indicating that as departmental mean professional compromise increases, patient satisfaction decreases. The 95% confidence band around the regression line is relatively wide, reflecting uncertainty associated with the small sample of departments. Specific patterns are noteworthy: the Orthopaedics department, which had the lowest mean compromise score (3.55), exhibited the highest patient satisfaction (97.6%). At the other extreme, the Obstetrics and Gynaecology department and the Emergency Medicine department, with mean compromise scores exceeding 4.0, had patient satisfaction percentages below 92%. The Oncology department also showed relatively low patient satisfaction (91.7%) despite a mean compromise score (3.98) slightly below the 4.0 threshold.
Interpretive cautions. This department-level finding must be interpreted with considerable caution for several methodological reasons. First, the analysis included only 10 departments, providing limited statistical power and preventing statistical adjustment for potential confounding variables such as case complexity, patient demographic characteristics, departmental staffing ratios, or resource availability. Second, the ecological nature of this analysis—correlating aggregate characteristics across units—does not permit inference to individual-level relationships. The observed association at the department level may not reflect causal processes operating between individual physicians’ experiences of professional compromise and individual patients’ satisfaction; this represents a form of ecological fallacy. Third, the magnitude of the correlation (r=−0.929) is unusually strong and may be partly attributable to the small sample size; smaller samples tend to produce more extreme correlations (both positive and negative) by chance. Fourth, unmeasured common causes may drive both high professional compromise and low patient satisfaction in certain departments—for example, departments facing severe resource constraints or handling particularly complex cases may simultaneously generate both phenomena without a direct causal pathway between them.
Given these limitations, we regard the department-level finding as exploratory and hypothesis-generating rather than confirmatory. Replication in larger samples using multilevel modelling approaches that can simultaneously examine individual-level and contextual effects is essential before drawing firm conclusions about associations between aggregate professional compromise and patient outcomes.
Summary of Key Findings
To summarise the principal findings: professional compromise was prevalent among physicians in this tertiary hospital, with 50% reporting frequent compromise experiences (score ≥4). Professional compromise was strongly correlated with burnout (r=0.587) and moderately correlated with lower job satisfaction (r=−0.347). Comparison of high-compromise and low-compromise groups revealed that high-compromise physicians had substantially higher burnout (Cohen’s d=0.97), lower job satisfaction (Cohen’s d=0.57), and greater turnover intention (OR=3.09) compared with their low-compromise counterparts. At the exploratory department level, mean professional compromise was inversely associated with patient satisfaction (r=−0.929), though this finding requires cautious interpretation and replication in larger samples.
Discussion
Summary of Findings
This study provides, to our knowledge, the first quantitative assessment of professional compromise among physicians at a Chinese tertiary hospital and examines its associations with clinician well-being indicators and organisational outcomes. Three principal findings emerged from our analysis.
First, professional compromise was prevalent. Exactly half of participating physicians (50%) reported experiencing professional compromise frequently, defined as a mean score of 4 or higher on our adapted instrument. The overall mean score of 3.85 fell between “sometimes” and “often,” suggesting that the majority of physicians encountered situations requiring deviation from their professional standards or clinical judgment with some regularity. These findings indicate that professional compromise is a common rather than exceptional phenomenon in the study setting.
Second, professional compromise was robustly associated with adverse clinician outcomes. The correlation between professional compromise and burnout (r=0.587) was strong, and group comparisons revealed that high-compromise physicians scored nearly one standard deviation higher on the burnout measure than low-compromise physicians (Cohen’s d=0.97). Professional compromise was also associated with lower job satisfaction (d=0.57) and substantially higher odds of turnover intention (OR=3.09). These associations persisted despite demographic similarity between comparison groups.
Third, at the exploratory department level, mean professional compromise correlated inversely with patient satisfaction (r=−0.929, p<0.001). Obstetrics and Gynaecology and Emergency Medicine departments exhibited both the highest compromise scores and the lowest patient satisfaction ratings—a pattern of potential organisational relevance that warrants replication.
Comparison with Prior Research
The positive association between professional compromise and burnout observed in this study is consistent with, and somewhat stronger than, associations reported in prior research from Western healthcare settings. The systematic review by Lamiani et al17 reported a pooled correlation between moral distress and burnout of approximately 0.42 across 30 studies encompassing diverse healthcare professional populations. Our observed correlation of 0.587 exceeds this pooled estimate, though direct comparison is complicated by differences in measurement instruments and study populations.
Several factors may account for the relatively strong association observed in our study. First, the structural characteristics of Chinese tertiary hospitals—exceptionally high patient volumes, brief consultation times, hierarchical organisational cultures—may create particularly intense and frequent experiences of professional compromise. Second, our study focused specifically on physicians rather than mixed samples including nurses, social workers, and other healthcare professionals; the nature and consequences of professional compromise may differ across professional groups. Third, measurement approach may play a role; our adapted instrument focused on frequency of compromise experiences, whereas some prior studies have measured intensity or examined both dimensions.
The magnitude of the effect sizes for group comparisons deserves emphasis. A Cohen’s d of 0.97 for the burnout comparison indicates that high-compromise and low-compromise groups differed by approximately one full standard deviation—a substantial and clinically meaningful difference. For perspective, effect sizes of this magnitude are rarely observed in studies of workplace factors and psychological outcomes. The threefold increase in odds of turnover intention among high-compromise physicians (OR=3.09) also represents a substantial difference with practical implications for workforce planning.
Our finding that neither age nor years of experience correlated with professional compromise is noteworthy. Some prior studies from Western contexts have reported that younger healthcare professionals experience higher moral distress, possibly reflecting idealism that diminishes with experience or accumulated coping mechanisms among more senior staff.17 Our null findings suggest that in the Chinese tertiary hospital context, professional compromise may be pervasive across career stages—affecting residents and senior consultants alike. This pattern could reflect the universality of systemic pressures in these high-volume environments.
Potential Mechanisms
Although our cross-sectional design precludes causal inference, consideration of potential mechanisms linking professional compromise to adverse outcomes may inform future research and intervention development.
Theoretical frameworks from organisational psychology and bioethics suggest several pathways. First, repeated experiences of professional compromise may generate moral residue—persistent psychological distress arising from unresolved ethical conflicts that accumulates over time.15 This accumulated burden may deplete emotional resources, contributing directly to the emotional exhaustion component of burnout. Second, professional compromise may threaten physicians’ sense of professional identity and self-efficacy; when external constraints prevent clinicians from practising according to their training and values, their core sense of professional purpose may be undermined.12,13 Third, self-determination theory posits that autonomy is a fundamental psychological need; systematic violations of professional autonomy through imposed compromise may erode intrinsic motivation and work satisfaction.37
The observed association between departmental professional compromise and patient satisfaction, while requiring replication, suggests possible organisational-level mechanisms. Departments characterised by high levels of professional compromise may face systemic pressures—inadequate staffing, excessive patient volumes, resource constraints—that simultaneously affect both physician experiences and patient care quality. Alternatively, compromised physicians experiencing burnout and emotional exhaustion may engage less fully with patients, compromising communication quality, empathic connection, and the therapeutic relationship. High turnover in departments with elevated compromise could disrupt care continuity, potentially affecting patient experiences. These possibilities are not mutually exclusive and may operate concurrently.
The department-level data highlight Obstetrics and Gynaecology as a particularly vulnerable clinical environment, exhibiting the highest mean professional compromise score (4.12) alongside one of the lowest patient satisfaction rates (91.7%) in the study. The distinct pressures of high-stakes obstetric and gynaecological care—time-sensitive decision-making under resource constraints, navigating family–patient conflicts in reproductive health contexts, and managing ethical tensions in complex deliveries—may amplify both the frequency and consequences of professional compromise. Comparative evidence from a multivariate analysis of gynaecological patient satisfaction in Almaty, Kazakhstan, identified physician–patient communication quality (β=0.30) and care environment (β=0.25) as the strongest predictors of satisfaction,38 suggesting that communication deterioration associated with professional compromise may be particularly consequential in this specialty. These findings underscore the need for targeted, department-specific interventions rather than uniform hospital-wide approaches to workforce well-being.
Implications for Practice and Policy
While our findings are cross-sectional and do not establish causation, they suggest several considerations for practice and policy pending confirmation from longitudinal research.
At the individual level, recognition that professional compromise is associated with burnout may inform physician wellness programmes. Assessment of professional compromise could be incorporated into wellness surveillance alongside established measures of burnout and job satisfaction, potentially identifying individuals or groups at elevated risk. Individual-level interventions such as reflective practice groups, ethics consultation services, or peer support programmes might help physicians process and cope with experiences of professional compromise.39
At the organisational level, our findings suggest that attention to systemic factors generating professional compromise may be warranted. These factors might include patient volume and scheduling practices, administrative burden, clinical decision support systems, resource allocation policies, and organisational culture regarding clinical autonomy. While evidence for the effectiveness of specific organisational interventions remains limited,40,41 addressing root causes of professional compromise rather than downstream symptoms aligns with emerging frameworks emphasising system-level approaches to healthcare workforce sustainability.11
At the policy level, our findings carry direct risk-management implications for the journal readership. Physician overwork—a proximate driver of professional compromise—has been shown to impair patient satisfaction through physician–nurse collaboration deficits and heightened patient risk perception in Chinese hospitals.42 Hospital work conditions and burnout have been identified as mediators of adverse event reporting,43 suggesting that professional compromise may indirectly heighten institutional risk by deepening emotional exhaustion. Evidence from Chinese public hospital reform contexts indicates that targeted staff-oriented institutional changes can measurably improve staff satisfaction,44 providing a policy template for addressing the systemic roots of professional compromise. From a risk management perspective, integrating professional compromise monitoring into hospital quality management frameworks—alongside established patient safety indicators—may offer a proactive strategy for simultaneously safeguarding clinician well-being and organisational performance. Policies that inadvertently increase compromise (eg., productivity targets that conflict with quality care) may incur hidden costs in workforce attrition and patient experience decline.
Strengths and Limitations
This study has several strengths. It provides novel quantitative data on professional compromise among Chinese physicians, addressing a gap in the literature regarding non-Western healthcare settings. The use of validated instruments for key constructs—including licensed use of the MBI with appropriate permissions—strengthens measurement quality. The systematic adaptation process for the professional compromise instrument followed established guidelines for cross-cultural instrument development. The sampling strategy ensured representation across diverse clinical departments. The response rate (80.0%) was acceptable for survey research in busy clinical settings.
Several limitations warrant careful consideration. First and most importantly, the cross-sectional design precludes causal inference. We cannot determine whether professional compromise contributes to burnout and other adverse outcomes, whether burnout leads to heightened perception of compromise, or whether both arise from unmeasured common causes. Longitudinal cohort studies tracking physicians over time are necessary to examine temporal relationships and establish the direction of associations.
Second, the single-centre design limits generalisability. Chinese hospitals vary substantially by geographic region, institutional tier (primary, secondary, tertiary), ownership structure (public, private), and patient population. The prevalence and consequences of professional compromise may differ in community hospitals, private institutions, or hospitals in other regions. Multi-centre studies sampling diverse healthcare settings are needed to assess the robustness and generalisability of our findings.
Third, although we employed rigorous adaptation procedures, the professional compromise instrument was derived from measures developed in Western healthcare contexts and may not fully capture culturally specific manifestations of professional compromise in China. Scenarios particularly relevant to Chinese healthcare—such as conflicts with patient families who play prominent roles in medical decision-making, expectations regarding informal payments, or pressures related to hierarchical relationships—may warrant development of indigenous measurement approaches.
Fourth, the department-level analysis included only 10 units, providing limited statistical power, preventing adjustment for confounders, and producing estimates with considerable uncertainty. The striking correlation (r=−0.929) should be regarded as preliminary and potentially influenced by the small sample. Larger studies employing multilevel modelling approaches are essential for robust examination of contextual associations.
Fifth, all physician-reported variables were collected from the same respondents at the same time using similar self-report methods, introducing potential common method bias. Correlations among self-reported constructs may be inflated by shared method variance, respondent tendencies (such as positive or negative affectivity), or transient factors affecting responses. Future research should incorporate objective measures (such as administrative data on productivity, patient outcomes, or physiological stress markers) and multi-source data (such as colleague ratings or patient assessments) to mitigate this concern.
Directions for Future Research
Several directions for future research emerge from this study. Longitudinal cohort studies tracking physicians over time—ideally from the beginning of their careers—would permit examination of temporal relationships between professional compromise, burnout, and other outcomes. Such studies could assess whether professional compromise precedes and predicts subsequent burnout, whether accumulated compromise has dose-response effects, and whether the relationship is bidirectional.
Intervention studies represent an important research priority. Randomised or quasi-experimental studies examining organisational interventions intended to reduce professional compromise—such as workload modifications, enhanced clinical autonomy, or improved resource allocation—could provide evidence regarding causality and inform practice. The field would benefit from rigorous evaluation of both individual-level interventions (such as resilience training or ethics support) and system-level interventions (such as workflow redesign or staffing optimisation).
Qualitative research exploring the lived experience of professional compromise among Chinese physicians would provide contextual depth complementing quantitative findings. Understanding how physicians perceive, interpret, and cope with professional compromise—and how these experiences vary across career stages, specialties, and institutional contexts—could inform intervention development.
Cross-cultural comparative studies might illuminate how healthcare system characteristics shape the prevalence and consequences of professional compromise. Comparison across countries with different healthcare financing models, organisational structures, and cultural contexts could identify system-level factors that protect against or exacerbate professional compromise.
Finally, development and validation of measures specifically designed for the Chinese healthcare context—capturing culturally specific scenarios and using culturally appropriate language—would strengthen future research in this population.
Conclusions
Professional compromise was prevalent among physicians at this Chinese tertiary hospital, with half reporting frequent experiences of acting against their professional standards or clinical judgment owing to systemic constraints. Professional compromise was associated with substantially higher burnout, lower job satisfaction, and greater turnover intention. At the exploratory department level, mean professional compromise correlated inversely with patient satisfaction. While the cross-sectional design precludes causal conclusions, these findings suggest that professional compromise warrants attention as a potentially modifiable risk factor in clinician well-being and healthcare quality. A non-compromised clinical workflow in high-volume tertiary settings might incorporate protected time for ethical reflection, specialty-specific ethics consultation for high-acuity departments such as Obstetrics and Gynaecology, revised performance metrics that balance throughput with care quality, and staffing ratios permitting adequate consultation time. Addressing systemic factors that generate professional compromise may hold promise for improving both the working lives of physicians and the care experiences of patients. Longitudinal and multi-centre research is needed to confirm these associations, examine causal mechanisms, and evaluate targeted interventions.
Abbreviations
CFI, Comparative fit index; CI, Confidence interval; EE, Emotional exhaustion; ICU, Intensive care unit; MBI, Maslach Burnout Inventory; MBI-HSS, Maslach Burnout Inventory–Human Services Survey; MMD-HP, Measure of Moral Distress for Healthcare Professionals; OR, Odds ratio; RMSEA, Root mean square error of approximation; SD, Standard deviation; SRMR, Standardised root mean square residual; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology; TLI, Tucker-Lewis index.
Data Sharing Statement
The datasets generated and analysed during the current study are not publicly available due to institutional data governance policies but are available from the corresponding author on reasonable request and with permission from the hospital’s research ethics committee.
Ethics Approval and Consent to Participate
The study protocol was reviewed and approved by the Institutional Review Board of the Affiliated Hospital of Xi’an Jiaotong University prior to commencement of data collection (2025-044-01). All study procedures were conducted in compliance with the principles of the Declaration of Helsinki. Participation was voluntary, and all respondents provided written informed consent before completing study questionnaires.
Consent for Publication
Not applicable. This manuscript does not contain any individual person’s data in any form.
Acknowledgments
The authors gratefully acknowledge the physicians who participated in this study for their time and candour in completing study questionnaires. We thank the staff of the Quality Management Office for extracting and providing departmental patient satisfaction data. We acknowledge the members of the expert panel who contributed to the adaptation and validation of the professional compromise instrument.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This project is funded by the National Natural Science Foundation of China (Grant No.72271196).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Shanafelt TD, West CP, Sinsky C. et al. Changes in burnout and satisfaction with work-life integration in physicians and the general US working population between 2011 and 2020. Mayo Clin Proc. 2022;97(3):491–17. doi:10.1016/j.mayocp.2021.11.021
2. West CP, Dyrbye LN, Shanafelt TD. Physician burnout: contributors, consequences and solutions. J Intern Med. 2018;283(6):516–529. doi:10.1111/joim.12752
3. Rotenstein LS, Torre M, Ramos MA, et al. Prevalence of burnout among physicians: a systematic review. JAMA. 2018;320(11):1131–1150. doi:10.1001/jama.2018.12777
4. Zhang Y, Liu J, Wang L, et al. Prevalence and determinants of burnout among physicians in China: a systematic review and meta-analysis. BMJ Open. 2024;14:e078456.
5. Li Y, Zhang X, Wang J, et al. Physician burnout in China: current status, trends, and determinants—a national cross-sectional survey. Lancet Reg Health West Pac. 2025;44:101023.
6. Maslach C, Jackson SE, Leiter MP. Maslach Burnout Inventory Manual.
7. Tawfik DS, Scheid A, Profit J, et al. Physician burnout, safety-net status, and clinical outcomes. Pediatrics. 2023;152(2):e2023060451.
8. Panagioti M, Geraghty K, Johnson J, et al. Association between physician burnout and patient safety, professionalism, and patient satisfaction: a systematic review and meta-analysis. JAMA Intern Med. 2018;178(10):1317–1331. doi:10.1001/jamainternmed.2018.3713
9. Hall LH, Johnson J, watt I, Tsipa A, O’Connor DB. Healthcare staff wellbeing, burnout, and patient safety: a systematic review. PLoS One. 2016;11(7):e0159015. doi:10.1371/journal.pone.0159015
10. Wallace JE, Lemaire JB, Ghali WA. Physician wellness: a missing quality indicator. Lancet. 2009;374(9702):1714–1721. doi:10.1016/S0140-6736(09)61424-0
11. Bodenheimer T, Sinsky C. From triple to quadruple aim: care of the patient requires care of the provider. Ann Fam Med. 2014;12(6):573–576. doi:10.1370/afm.1713
12. Dean W, Talbot S, Dean A. Reframing clinician distress: moral injury not burnout. Fed Pract. 2019;36(9):400–402.
13. Rushton CH, Thomas TA, Antonsdottir IM, et al. Moral injury and moral resilience in health care workers. JAMA. 2022;327(18):1827–1828.
14. Jameton A. Nursing Practice: The Ethical Issues. Englewood Cliffs, NJ: Prentice-Hall; 1984.
15. Epstein EG, Hamric AB. Moral distress, moral residue, and the crescendo effect. J Clin Ethics. 2009;20(4):330–342. doi:10.1086/JCE200920406
16. Kopacz MS, Lockman J, Lusk J, et al. Moral injury in healthcare: a scoping review. J Clin Psychol Med Settings. 2023;30:639–654.
17. Lamiani G, Dordoni P, Argentero P. A systematic review and meta-analysis of moral distress and its correlates in healthcare professionals. J Health Psychol. 2024;29(1):3–21. doi:10.1177/13591053231175809
18. Shapiro J, Galowitz P, McCue JD. Teaching medical students to recognize moral injury in healthcare. Med Teach. 2023;45(8):876–882.
19. Ofri D. When We Do Harm: A Doctor Confronts Medical Error. Boston: Beacon Press; 2023.
20. Miljeteig I, Førde R, Hurst S, et al. Moral distress among healthcare professionals during COVID-19: a multi-country study. Nurs Ethics. 2021;28(7–8):1372–1383.
21. Dzeng E, Dohan D, Curtis JR, et al. Homing in on the social: system-level influences on physician moral distress. J Gen Intern Med. 2024;39(1):127–134. doi:10.1007/s11606-023-08474-z
22. Pan J, Wang P, Wu Y, Zhao H, Chen Y, Meng Q. Job satisfaction among Chinese doctors: a multilevel analysis of hospital characteristics. BMC Health Serv Res. 2022;22:1089.
23. Wang X, Liu Y, Chen Z, Li H, Zhang W, Ma X. Work environment and physician satisfaction in Chinese public hospitals. Int J Health Plann Manage. 2024;39(2):456–471.
24. Mellides González M, Losa Iglesias ME, Corral-Liria I, et al. Moral distress healthcare providers in Spain: observational study. Risk Manag Healthc Policy. 2024;17:1493–1501. doi:10.2147/RMHP.S460360
25. Epstein EG, Whitehead PB, Prompahakul C, Thacker LR, Hamric AB. Enhancing understanding of moral distress: the measure of moral distress for health care professionals. AJOB Empir Bioeth. 2019;10(2):113–124. doi:10.1080/23294515.2019.1586008
26. Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. 2000;25(24):3186–3191. doi:10.1097/00007632-200012150-00014
27. Lee RT, Ashforth BE. A meta-analytic examination of the correlates of the three dimensions of job burnout. J Appl Psychol. 1996;81(2):123–133. doi:10.1037/0021-9010.81.2.123
28. Li X, Guan L, Chang H, Zhang B. Core self-evaluation and burnout among nurses: the mediating role of coping styles. PLoS One. 2014;9(12):e115799. doi:10.1371/journal.pone.0115799
29. Zhang W, Meng H, Yang S, Liu D. Job burnout and its influencing factors among village doctors in China: a cross-sectional survey. BMC Prim Care. 2023;24:45. doi:10.1186/s12875-023-01998-7
30. Wanous JP, Reichers AE, Hudy MJ. Overall job satisfaction: how good are single-item measures? J Appl Psychol. 1997;82(2):247–252. doi:10.1037/0021-9010.82.2.247
31. Dolbier CL, Webster JA, McCalister KT, Mallon MW, Steinhardt MA. Reliability and validity of a single-item measure of job satisfaction. Am J Health Promot. 2005;19(3):194–198. doi:10.4278/0890-1171-19.3.194
32. Dyrbye LN, West CP, Sinsky CA, Goebert D, Satele DV, Shanafelt TD. Physicians’ experiences with mistreatment and discrimination by patients, families, and visitors and association with burnout. JAMA Netw Open. 2022;5(5):e2213080. doi:10.1001/jamanetworkopen.2022.13080
33. Griffeth RW, Hom PW, Gaertner S. A meta-analysis of antecedents and correlates of employee turnover: update, moderator tests, and research implications for the next millennium. J Manage. 2000;26(3):463–488.
34. National Health Commission of the People’s Republic of China. Technical guidelines for patient experience monitoring in medical institution. China Health Policy. 2022;(4):1–12. [in Chinese].
35. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
36. von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–1457. doi:10.1016/S0140-6736(07)61602-X
37. Deci EL, Ryan RM. The “what” and “why” of goal pursuits: human needs and the self-determination of behavior. Psychol Inq. 2000;11(4):227–268. doi:10.1207/S15327965PLI1104_01
38. Aliyeva S, Atabayeva AK, Ansatbayeva TN, Kokayeva EA, Sagalbayeva UY, Tsigengagel OP. Key predictors of satisfaction among gynecological patients in Almaty, Kazakhstan: a multivariate analysis. Reprod Med. 2025;(1):49–56. doi:10.37800/RM.1.2025.472
39. Rushton CH, Caldwell M, Kurtz M. CE: moral distress: a catalyst in building moral resilience. Am J Nurs. 2016;116(7):40–49. doi:10.1097/01.NAJ.0000484933.40476.5b
40. Panagioti M, Panagopoulou E, Bower P, et al. Controlled interventions to reduce burnout in physicians: a systematic review and meta-analysis. JAMA Intern Med. 2017;177(2):195–205. doi:10.1001/jamainternmed.2016.7674
41. West CP, Dyrbye LN, Erwin PJ, Shanafelt TD. Interventions to prevent and reduce physician burnout: a systematic review and meta-analysis. Lancet. 2016;388(10057):2272–2281. doi:10.1016/S0140-6736(16)31279-X
42. Zhou K, Xin Y, Li M, Chen L. Physicians’ overwork impacts patient satisfaction via physician–nurse collaboration and patients’ medical risk perception in China. Risk Manag Healthc Policy. 2025;18:3633–3645. doi:10.2147/RMHP.S537903
43. Jarrar M, Al-Bsheish M, Albaker W, et al. Hospital work conditions and the mediation role of burnout: residents and practicing physicians reporting adverse events. Risk Manag Healthc Policy. 2023;16:1–13. doi:10.2147/RMHP.S392523
44. Tao S, Jiao Z, Xie J, Wang Q. Satisfaction with public hospital reform and associated factors among medical staff: a cross-sectional survey in Wuhan, China. Risk Manag Healthc Policy. 2021;14:5071–5080. doi:10.2147/RMHP.S335988
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.