Back to Journals » International Journal of Women's Health » Volume 15
Process Evaluation of Facility Delivery Services in Northwest Ethiopia: In the Case of Public Health Centers
Authors Tafere TZ ![]() , Aschalew AY, Tsehay CT
, Aschalew AY, Tsehay CT ![]() , Gebremedhin T
, Gebremedhin T ![]()
Received 31 August 2022
Accepted for publication 3 February 2023
Published 13 February 2023 Volume 2023:15 Pages 235—253
DOI https://doi.org/10.2147/IJWH.S388153
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Tesfahun Zemene Tafere, Andualem Yalew Aschalew, Chalie Tadie Tsehay, Tsegaye Gebremedhin
Department of Health Systems and Policy, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Tesfahun Zemene Tafere, Department of Health Systems and Policy, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, P.O. Box: 196, Gondar, Ethiopia, Email [email protected]
Background: Even if giving birth at health facility is vital for both the mothers and their newborns, the coverage of institutional delivery in Ethiopia is very low (50%). In that regard, several studies have shown the possible factors of low delivery service uptake from the patients’ side, but evidences on delivery services at the health centers are meagre. This study aimed to evaluate the process of delivery services in public health centers of northwest Ethiopia.
Methods: A case study evaluation design with an embedded mixed-method was used to evaluate institutional delivery in public health centers of Gondar city. Dimensions from the access (availability, accommodation, and acceptability) and implementation fidelity (compliance) frameworks were used. A total of 363 mothers, 32 document reviews, 32 direct observations, and 17 key informants were included. The qualitative data were transcribed, translated, coded, and analysed using a thematic analysis approach. The overall process of institutional delivery services was measured based on pre-determined judgmental criteria.
Results: The overall facility delivery process was 75.1%, judged by availability (78.5%), compliance (70.6%), accommodation (68.8%), and acceptability (80.2%) of services. Essential medicines in some of the health centers were stockout, insufficient delivery rooms and inadequate training of health workers on obstetric and newborn care were observed. Using partograph and examining vulval-perineal region for possible laceration during intrapartum period were less practiced. Residence (AOR: 0.13, 95% CI: 0.06– 0.30), ANC 1 to 3 visits (AOR: 2.65, 95% CI: 1.05– 6.74) and ANC4+ (AOR: 5.57, 95% CI: 2.09, 14.84) were factors affected acceptability of delivery services.
Conclusion: Major constraints were in the accommodation of delivery services which needs a holistic effort from all stakeholders. Therefore, implementors with other stakeholders shall improve delivery rooms, facilitate training, and provide parenteral drugs as part of the obstetric and newborn care to improve the facility delivery services in Ethiopia.
Keywords: acceptability, accommodation, availability, compliance, institutional delivery, evaluation
Background
Women comprise a large proportion of any society, and many of them live having increased preventable risk of morbidity and mortality substantially during childbirth.1 One of the interventions that is believed to reduce this excess risk is institutional delivery which means giving births in health institutions under the supervision of trained health professionals.2
The World Health Organization (WHO) promotes institutional delivery at every birth.3 As a result, 63.1% of births were attended by skilled health-care workers across the globe. Its respective coverage among the high-income countries was 100%, whereas the corresponding figure in developing countries is 59.1%.4 According to the 2019 mini Ethiopian Demographic and Health Survey (mEDHS) report, skilled birth attendance in Ethiopia was 50%.5
Socio-cultural factors, inadequate availability of resources such as drugs, human resources, medical equipment, low compliance of health-care providers, and mothers’ attitudes towards the service are delivery process-related attributes reported to impact the utilisation of institutional delivery service.6,13
To overcome the gap, the Ethiopian Ministry of Health has adopted various public health policy initiatives to strengthen the institutional delivery care services such as community mobilization for behavioral and cultural barriers, establishing maternity waiting homes for distance barriers, and exemption of maternal health services for financial or cost barriers.7 Regardless of the efforts, the quality of labor and delivery service process falls below WHO’s standards8 that could prevent 44% of stillbirths, 73% newborn deaths, and 61% of maternal deaths.9 The linkage of the program components of the delivery services in the health centers can be explained by the program logic model in (Figure 1). Health center is a health facility within the primary health-care system that provides promotive, preventive, curative and rehabilitative outpatient care including basic laboratory and pharmacy services through health-care professionals.10,11
 |
Figure 1 Logic model of delivery services. |
Previous studies in Ethiopia focused on the magnitude of institutional delivery. However, the implementation of the program organized by its components-inputs, activities and outputs12 and the barriers and facilitators for the process are not well addressed yet. Therefore, this evaluation will generate a comprehensive evidence on the program process and the barriers and facilitators of the process for decision-making.13–17 Moreover, the findings of the evaluation are expected to produce valuable information for policymakers and program managers in improving the implementation of this vital area of maternal health-care service.
Methods
Evaluation Design and Settings
A case-study design with an embedded mixed-method evaluation was used in this evaluation. The evaluation was conducted in Gondar city. The city has six sub-cities and an estimated population of 344,046.18 According to the information obtained from city administration’s health department office, there is one comprehensive specialised teaching hospital, eight health centers (HCs), and 14 health posts in the city. Maternal, newborn and child health service provisions are integrated with other health services at the health center level. An estimated number of 11,594 pregnant women were served in the HCs in the year 2020.18 The study participants were (a) mothers who received labour and delivery services, (b) health-care providers working in the labour and delivery units, (c) heads of HCs, (d) maternal reproductive health officer of Gondar administrative city, and (e) delivery services documents (partograph, and delivering mothers registration book).
Evaluation Approach and Dimensions
A formative evaluation approach was used that focused on the process theory of institutional delivery. The program process theory consists of the program organisational and services utilization plan.19 Accordingly, the program’s organisational plan was articulated from the perspective of program management that encompasses both the functions and activities the program is expected to perform and the resources required for that performance. Whereas the service utilization plan focused on the critical assumptions about how and why the intended recipients of delivery service were become engaged with the program and follow through to the point of receiving sufficient services to initiate the change process represented in the program impact theory.
This evaluation used a total of four dimensions – three (availability, accommodation and acceptability) from the access framework20 and one (compliance) from the implementation fidelity framework.21
Variables and Measurements
Evaluation dimensions are measurable aspects of program performance that an evaluation intends to examine.19 The compliance domain was assessed using 12 items which measured the health-care providers’ adherence level with the national obstetrics management protocol. Availability refers to the physical presence of services, the supply of drugs, equipment, skilled health professionals, and guidelines, registers, and infrastructures.20 The availability of resources was measured using 12 indicators to determine whether essential drugs, medical equipment, and infrastructures required for the services were available or not. Compliance is the practice of delivery service activities based on the national obstetrics management protocol guideline.21 Accommodation refers to the setup of the organization to accept clients, the clients’ convenience of its appropriateness, and the ability to accommodate organizational factors.20 Likewise, the accommodation of delivery services was measured using eight indicators, each with a 5-point Likert scale (1 = highly dissatisfied to 5 = highly satisfied). Then, highly dissatisfied, dissatisfied, and neutrals were classified as dissatisfied, else as satisfied with the delivery service’s accommodation. Acceptability is the relationship of clients’ attitudes about the personal and practice of providers to the actual characteristics of existing providers.20 Moreover, delivery services acceptability was assessed using 10 indicators with 5-point Likert scales (0 = strongly disagree to 5 = strongly agree). Then the acceptability was dichotomised based on a threshold score. The threshold score for acceptability was determined using the demarcation threshold formula.22

Accordingly, respondents who scored above 60 on the acceptability questions were considered as accepted otherwise not accepted. The indicators were adapted after reviewing different literatures.13,23–25 Stakeholders determined indicators’ weights during the evaluability assessment stage which were calculated using the formula:
 26 (Table 1). Then, judgment parameter was seated; >85, 70–85, 50–69.9, and <50% as very good, good, fair, and poor, respectively, for each dimension and also for the overall program process.
26 (Table 1). Then, judgment parameter was seated; >85, 70–85, 50–69.9, and <50% as very good, good, fair, and poor, respectively, for each dimension and also for the overall program process.
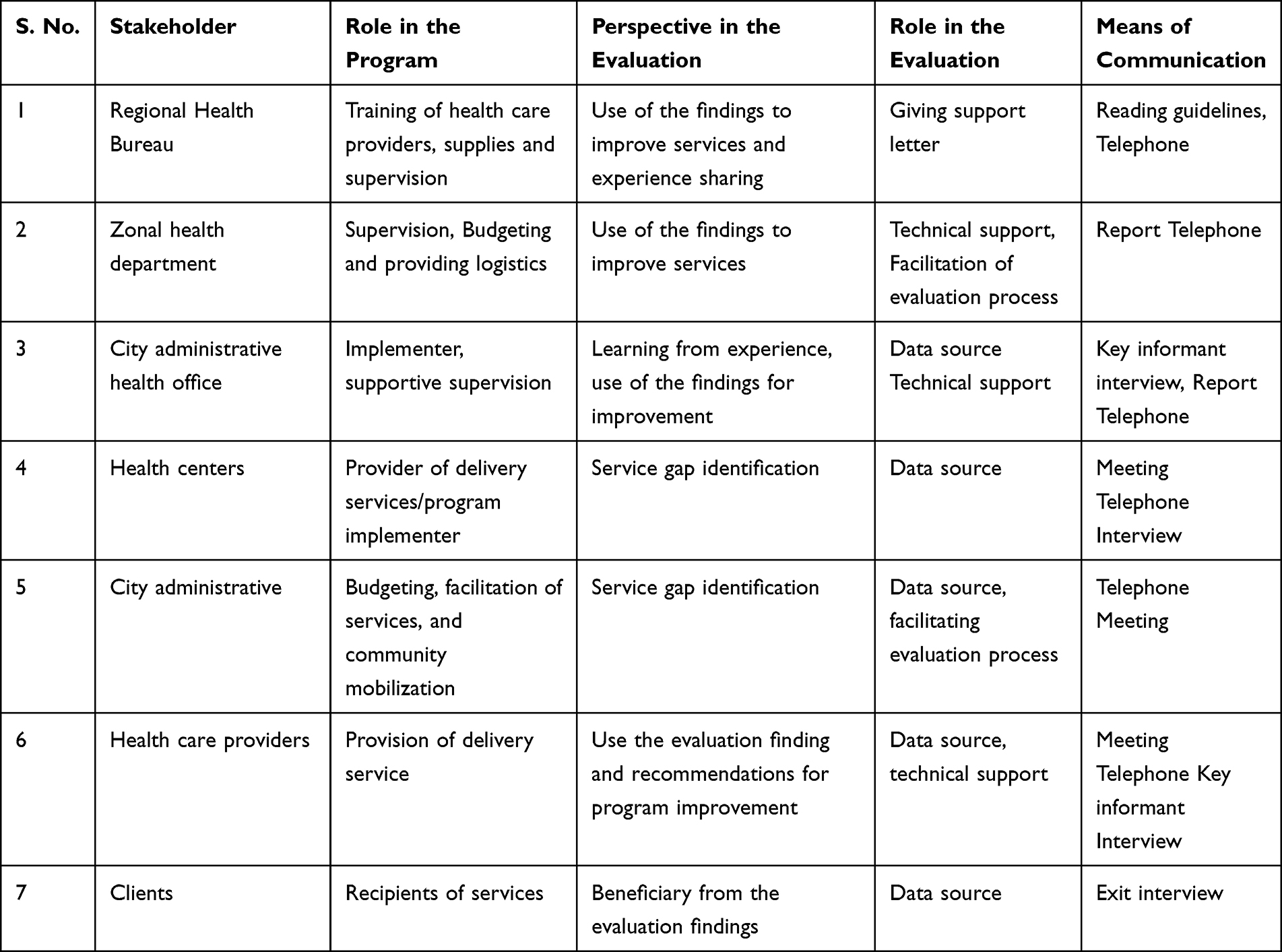 |
Table 1 Stakeholders’ Identification and Analysis Matrix for Delivery Service in Gondar City Health Centers, Northwest Ethiopia, 2020 |
Sample Size and Sampling Procedures
Eight health centers were inventoried for the measurements of availability. A total of 32 non-participatory direct observation sessions were conducted, and all mothers’ medical records were reviewed for measuring the compliance of health-care providers with the national guideline. Further, purposefully selected 17 health workers were involved in the key informant interviews. Accordingly, the head of the delivery room from each health center and coordinator of maternal reproductive health at the health office were selected purposively.
The sample size for the accommodation and acceptability was calculated using a single population proportion formula: 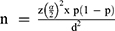 with the assumption of 5% margin of error (d), 95% confidence level, p = 31.3%,27 and 10% non-response rate which yields the final sample size of 363.
with the assumption of 5% margin of error (d), 95% confidence level, p = 31.3%,27 and 10% non-response rate which yields the final sample size of 363.
The proportional sample size allocation was done to each health center based on the prior two months of delivery. Then, participants were selected using a systematic sampling technique. Mothers who gave birth at Gondar city HCs during the data collection period, heads of the delivery room, heads of the health center, and health-care providers who were worked at the facilities at least for six months were included in this evaluation. Mothers who were severely ill and unable to communicate were excluded from the exit interview.
Data Collection Tools and Procedures
Resource inventory checklists, direct observation checklists, document review, structured and semi-structured questionnaires were used for data collection. The resource inventory checklists used for measuring the availability of resources were adapted from the Ethiopian national standard health center requirement guideline and other literature.24,25 The observation checklists and document review used for measuring the compliance of health-care providers to labour and delivery guideline were adapted from the Ethiopian national obstetrics management protocol23 which is similar to WHO guideline (Pregnancy, Childbirth, Postpartum, and Newborn Care: A guide for essential practice).28 A structured questionnaire for exit interviews was adapted from transforming health-care quality in Ethiopia guides and other related literature.29–31 A semi-structured questionnaire for key informant interviews was also adapted from the WHO quality of care for mothers and newborn babies assessment tool and other literature.29,30 These tools were first developed in English and translated to the local language (Amharic), and back to English to ensure consistency. Eight female diploma midwives and two male BSC degree graduate midwives were recruited for data collection and supervision, respectively. A day of training was given on basic data collection and client handling techniques.
Moreover, a pre-test was done on 18 mothers before the actual data collection and the internal consistency of the questionnaires was demonstrated through the reliability analysis of Cronbach alpha value of 0.93. Daily supervision was done throughout the evaluation process. Furthermore, the first three observations were dropped to minimize the possible hawthorn effects. The qualitative data quality was controlled by taking daily notes on the in-depth information gained from the key informants.
Data Management and Analysis
The quantitative data were checked for completeness, edited, coded, and entered into Epi-data version 4.6 and exported to STATA version 14 software for analysis. Descriptive statistics were computed and results were presented using tables and narrations. A binary logistic regression model was fitted to identify factors associated with the acceptability of services, and in the final model, a p-value of <0.05 and adjusted odds ratio (AOR) with 95% confidence intervals (CI) were used. Qualitative data were gathered, audio records of key informant interviews were transcribed into the text format of the local language, translated into English, and then coded and categorized by using a thematic analysis approach under the dimensions that supplemented the quantitative findings. Weight for the dimensions and the respective indicators were given depending on their level of relevance to the program. Finally, the dimensions were judged based on the pre-determined judgmental criteria.
Results
A total of 363 women who had their newborns recently for the survey, eight health centers for resource inventory, 32 direct observation sessions and document reviews, and 17 health-care providers for key informant interviews were involved in this evaluation.
Availability of Resources
There were a total of 133 skilled birth attendants in the health centers, of whom 63.2% were nurses, 21.0% were mid-wives, and 15.8% were health officers. Five health centers have recommended (3 and more) midwives.
The key informant interview results indicated that there was a shortage and an unequal deployment of midwives in the HCs; some HCs have more than the minimum required standards, whereas some have less than the standards.
There is a shortage of midwives in this HC. There are only two midwives currently working in the HC whom both of them are diploma midwives. During training or day off work, when either of them is absent in the HC, we always operate the delivery unit by one midwife only. This makes providing the necessary care to labour and delivery clients difficult. [mid forty years old male HC head]
There was a high turnover of midwives. Midwives who were trained on different kinds of training regarding delivery care services were turned over to other HCs, and fresh midwives filled the vacant position. Giving training about the delivery care activities and socialisation of them are challenges that results interruption of the implementation of delivery service activities and contribute for the poor quality of the service. [male delivery service coordinator midwife nurse]
Regarding the availability of basic infrastructure, one-fourth of the HCs had three separate rooms per national guideline (labouring, delivering, and postnatal units), and 87.5% of HCs had curtains and functional autoclave. Moreover, 62.5% HCs had a clean toilet with hand washing basin.
There is only one room with one bed for labour, delivery, and postpartum. One day, I remember that the situation that we were forced to give delivery services in the dressing room. As a result, we face problems when more than one labouring mother come to the HC. [male HC head]
Since there is only one room with one delivery couch for maternal health activities (labor, delivery, and postpartum), I was forced many times to transfer laboring clients to University of Gondar hospital when more than one laboring mothers come at the same time. Consequently, there is an unnecessary referral, which is one reason for low coverage of delivery service [female midwife-nurse delivery service coordinator].
The availability of continuous electric and water supply was limited in the majority of HCs. However, the Ethiopian national guideline of health center requirement recommends that adequate water and power supply should be secured 24 hours a day in the HC.
There is an interruption of electric power supply for the last five months, including this month. We are facing a problem to make delivery kits sterilized. We tried to overcome this problem by sterilizing in the nearby HC. We also provide delivery care service by using movable solar light while interruption of electric power supply. [Female delivery service coordinator midwife nurse]
The limitation in the availability of continuous water supply in this HC has affected our routine delivery care service activity. We do not find the required water supply as the desired amount. During the interruption, the water is provided by jerrican outside the HC. [mid-twenty-five-year-old female delivery service coordinator midwife nurse]
In all HCs, there was drug stockout like adrenaline, lidocaine, TTC eye ointment, and parenteral IV infusion (ringer lactate and normal saline). Around 37.5% of HCs were with stockout of magnesium sulfate and hydralazine for the last three months. Additionally, metronidazole parenteral antibiotic was stockout at 50% of HCs for the last three months. Furthermore, parenteral oxytocin was stockout in an HC and vitamin K was stockout for one-fourth of HCs since February 2020 (Table 2).
We have requested magnesium sulfate, hydralazine, oxytocin, and vitamin K but they would not be available from pharmaceutical fund and supply agency, especially vitamin k and magnesium sulfate were stockout many times in the market [mid thirty years old male HC head].
 |
Table 2 Availability of Drugs for Delivery Service in Gondar City HCs, Northwest Ethiopia, 2020 (n = 8) |
Regarding medical equipment and supplies, all HCs had medical equipment used for delivery services like delivery couches, stethoscope, sphygmomanometer, fetoscope, baby weighing scale, episiotomy set, newborn resuscitation set, and delivery forceps.
Moreover, personal protective equipment (surgical glove, goggle, apron) and national delivery care guidelines were available in all HCs (Table 3). According to the results indicated by key informant interviews, the personal protective equipment was not being utilised well despite their presence in the HCs.
No shortage of PPE in this HC. But midwives are reluctant the utilization of these PPE for every labor and delivery care service. They usually use them when more than one delivery clients come at a time. This is because of the negligence that midwives have towards using these PP”. [late twenty years old male HC head]
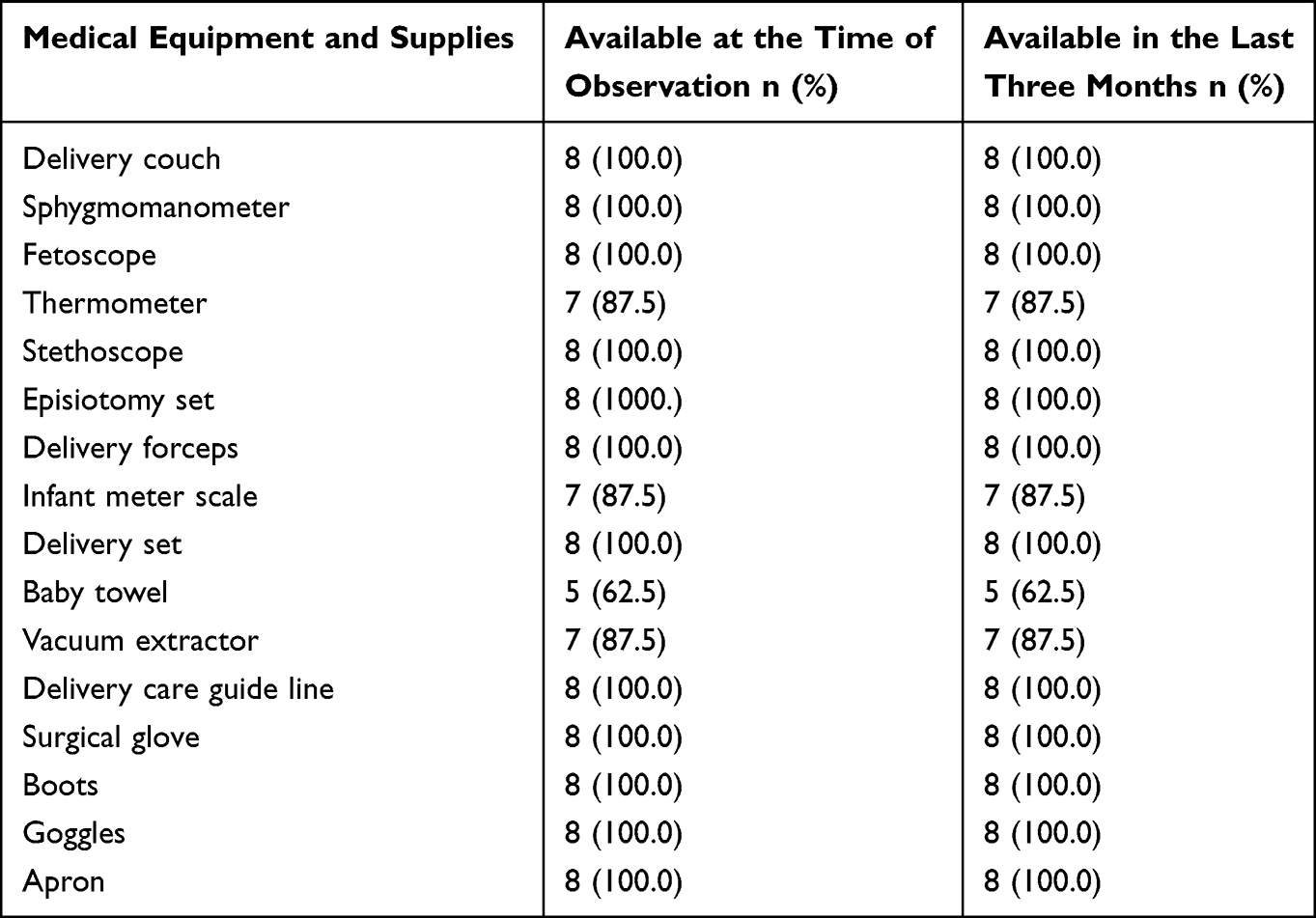 |
Table 3 Availability of Medical Equipment and Supplies of Delivery Service in Gondar City HCs, Northwest Ethiopia, 2020 (n = 8) |
The overall availability score of the delivery service was 78.5%. Medical equipment items, parenteral IV infusions, and delivery care guidelines were 100.0% available in all HCs, whereas the availability of rooms for laboring, delivery, and postpartum per national standard was only in one-fourths of HCs (Table 4).
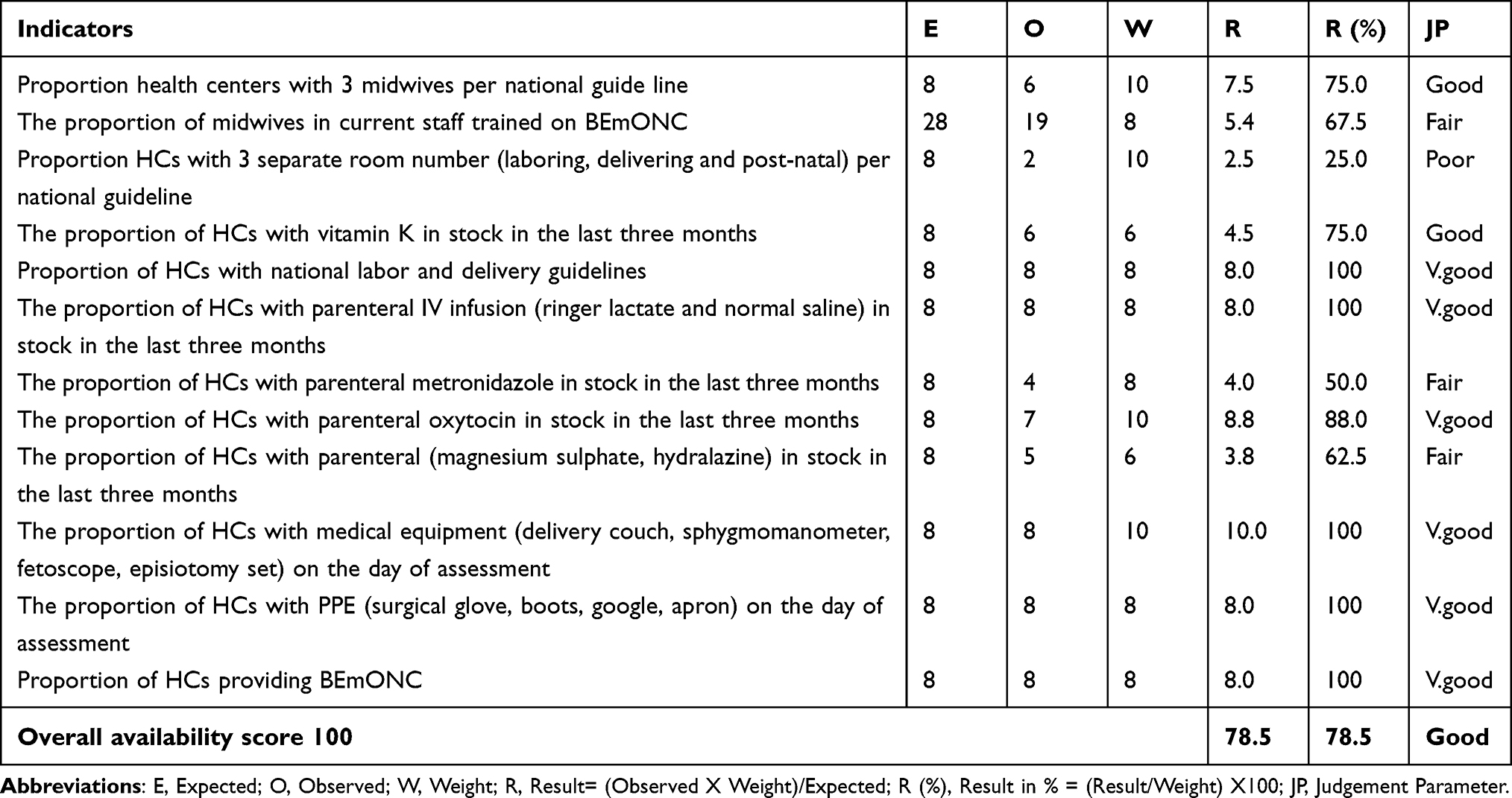 |
Table 4 Judgment Analysis Matrix of Availability Dimension for Evaluation of the Process of Delivery Service in Gondar City Health Centers, Northwest Ethiopia, 2020 |
Compliance of Delivery Service to the Guideline
In the client’s medical record review, a history of present pregnancy like gravida, parity, and ANC visits was recorded for 87.5% of mothers. About abdominal examinations such as fundal height, fetal position, fetal descent, and fetal heartbeat were recorded for 62.5%, 46.9%, 56.3%, and 65.6% of mothers, respectively. Furthermore, vaginal examination at the initial assessment; status of the membrane (68.8%), cervical dilation (81.3%), and fetal presentations (78.1%) were documented. Additionally, some recording files were not safely kept to be easily accessed whenever necessary; they were not also stapled together and had no folders. During the direct observation, monitoring of labor using partograph such as plotting cervical dilation and maternal blood pressure every four hours were observed to be practised for 72.0% and 65.6% of mothers, respectively.
The use of partograph for all mothers admitted in labor is recommended. But midwives do not plot findings on the partograph throughout the labor process. This is because of both the negligence and lack of refreshment training of health workers on partograph utilisation. [male HC head]
Furthermore, the health-care providers had washed hands during delivery preparation and used sterile gloves for 50% and 96.9% of births, respectively.
Washing before and after every L&D care procedure is essential for the mothers and ourselves to prevent infections. But we sometimes attain delivery care without washing hands, simply by wearing gloves. Because we do not have access to water near to the delivery room since there is no hand washing basin in the delivery room [female midwife-nurse delivery service coordinator].
Likewise, health-care providers were observed to be adhered to checking the completeness of the placenta and contraction of the uterus after the delivery of the placenta for 81.3% and 65.6% of delivering mothers, respectively. On the other hand, 71.9% of births were recorded in the medical record and 75.0% of newborn babies have started breastfeeding within an hour. Moreover, 53.0% of delivering mothers were checked for blood pressure every 15 minutes after the complete delivery of the placenta (Table 5).
 |
Table 5 Chart Reviews and Direct Observation Results of Labor and Delivery Care in Gondar City HCs, Northwest Ethiopia, 2020 (n = 32) |
The overall score of the compliance dimension was found to be 70.6%. Moreover, the proportion of clients who were checked for completeness of placenta was 81.3% which was the highest score and the proportion of delivering clients checked for vaginal bleeding every 15 minutes in the first hour after delivery of the placenta were 59.0% rated as the lowest score under the compliance dimension (Table 6).
 |
Table 6 Judgment Analysis Matrix of Compliance Dimension for Evaluation of the Process of Delivery Service in Gondar City Health Centers, Northwest Ethiopia, 2020 |
Accommodation and Acceptability of Delivery Service
Socio-Demographic Characteristics of Participants
A total of 363 mothers participated in this study. One hundred thirty-two (36.4%) of mothers were aged 25–29 years; the mean age was 26.6 (SD: ±4.8) years. Religious preference for 80.4% was Orthodox; 80.4% were urban dwellers. About 88.2% of them were married; 32.2% went to secondary school (Table 7).
 |
Table 7 Socio-Demographic Characteristics of Participants in Gondar City Health Centers, Northwest Ethiopia, 2020 (n = 363) |
Obstetric Characteristics of Participants
Nearly 12% of mothers’ recent pregnancy was unplanned. Fifty-eight percent of mothers had ANC visit four times and above, 59.0% of mothers were multigravida and 56.7% had two or more deliveries. Seven percent of the mothers ever had a history of abortion. On the other hand, 3% of mothers ever had a history of stillbirth. Moreover, 96.4% of mother had spontaneous vaginal delivery (SVD) which was the predominant mode of delivery and 2 (0.6%) of delivery ended with newborn death (Table 8).
 |
Table 8 Obstetrics Characteristics of Participants in Gondar City HCs, Northwest Ethiopia, 2020 (n = 363) |
Accommodation of Delivery Service
Out of the respondents, 65.6% were perceived that the waiting area was convenient. Nearly two-thirds of mothers were satisfied with the cleanliness of the delivery room. The majority (93.3%) of delivering mothers were satisfied with the delivery room’s light and air condition. About 72.5% of delivering mothers were satisfied with the waiting time; 85.0% were satisfied with the delivery room’s silence and 48.6% were satisfied with the appropriateness of proximity of the toilet.
There is only one toilet in the HC. The toilet has no hand washing basin and it doesn’t get clean regularly because of shortage of water accessibility in the HC. We have informed the head of the HC to discuss different stake holders on the possibilities of building additional toilets and water accessing full days. [female midwife-nurse]
Further, the level of mothers’ satisfaction regarding the accommodation of delivery service structure was 68.8% (Table 9).
 |
Table 9 Judgment Matrix Analysis of Accommodation Dimension for the Evaluation of Delivery Service in Gondar City HCs, Northwest Ethiopia, 2020 |
Acceptability of Delivery Service
The finding of the evaluation showed that the overall acceptability level of delivery service was 80.2%. Of this, 80.4% of mothers responded that health-care providers answered their questions and concerns during delivery care service, and 67.0% accepted the information given by health-care providers about the benefit and side effects of medical treatments and procedures. About 77.7% of mothers accepted the courtesy of health-care providers. The evaluation also showed that 83.8% of mothers were informed about the procedures of the L&D care. Moreover, 94.2% of mothers were responded to recommend the HC’s delivery service for friends and families (Table 10).
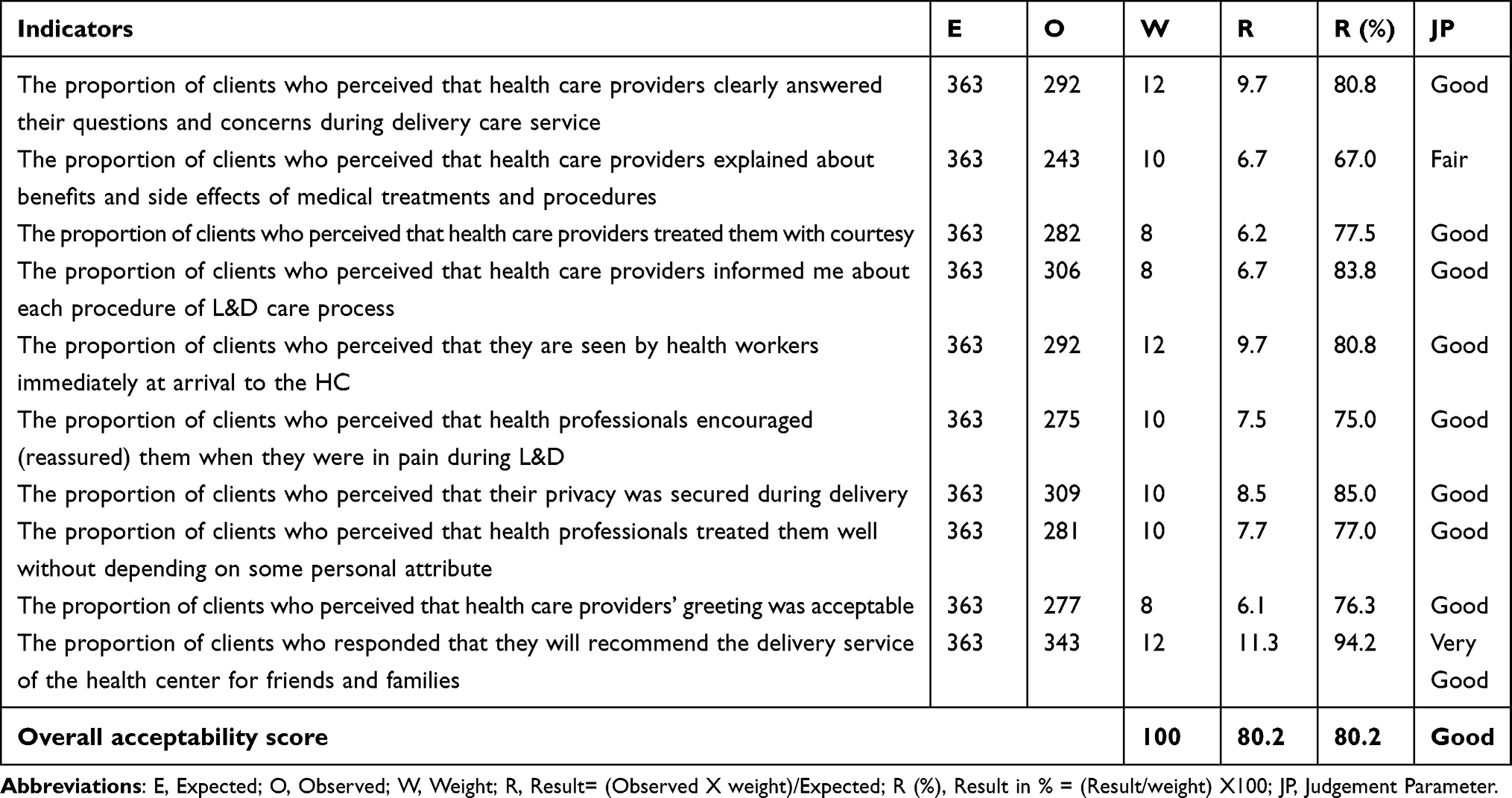 |
Table 10 Judgment Analysis Matrix of Acceptability Dimension for the Evaluation of Delivery Service in Gondar City HCs, Northwest Ethiopia, 2020 |
Factors Associated with the Acceptance of Delivery Service
In our analysis, residence and having ANC during the recent pregnancy were the factors that affect the delivery services. Accordingly, the odds of acceptance of delivery services by rural dweller mothers is significantly lower compared to mothers from urban areas (AOR: 0.13; 95% CI: 0.06–0.30). Mothers who had ANC visits of 1 to 3 compared to mothers who never had any ANC visit (AOR: 2.65; 95% CI: 1.05–6.74) and mothers who had ANC4 or more visits compared to who never had any ANC visit (AOR: 5.57; 95% CI: 2.09–14.84) had significantly higher odds to acceptance delivery services (Table 11).
 |
Table 11 Bivariable and Multivariable Logistic Regression Analysis for the Factors Associated with Acceptability of Delivery Services in Gondar City, Northwest Ethiopia, 2020 (n = 363) |
Discussion
We used an indicator-driven evaluation to evaluate the process of institutional delivery services, and we found the process was judged as good. Moreover, availability, accommodation, and acceptability dimensions were judged as good whereas the compliance was judged as fair based on a predetermined judgement parameter. Pertinent parenteral IV infusions like ringer lactate and normal saline were fully available in the HCs. Likewise, essential drugs such as adrenaline, lidocaine, and TTC eye ointment were in stock in the last 3 months. This finding is in line with the Ethiopian national guideline of health sector transformation in quality.31
The availability of parenteral antibiotic drugs like metronidazole and gentamycin were stockout, in the 40.0% of HCs in the last three months. This finding is lower than a study in Pakistan which reported that more than 90.0% of health facilities were stocked for these drugs.32 This great difference might be because of the existence of differences in the health system and service delivery.
Health centers had parenteral anticonvulsants; magnesium sulfate was 62.5% and diazepam was 37.5%. This finding was relatively consistent with the other study done in Guinea where 57.0% of health facilities were with parenteral anticonvulsants.33 This consistency might be due to the similarity of the health-care delivery system.
In a significant number of HCs, there was a stockout of parenteral antihypertensive drugs such as hydralazine and methyldopa for the last three months. The key informant interview showed that the reason was the shortage of drugs in the pharmaceutical center. This implies that the quality of delivery services in these HCs is likely to be compromised for delivering mothers with obstetric complications.
Medical equipment; baby towel and vacuum extractor were available in 62.5%, and 87.5% of health centers, respectively, which are below the expected standard in the evaluation. The finding is incongruent with the recommended standard of HC requirements guidelines24 and the recommendation of WHO guidelines.28 The possible reason might be the insufficient allocation of finances for the health centers to buy these equipments. The availability of midwives in 40% of HCs was below the national guideline recommendation (3 midwives per HC) which affects the skill birth attendance coverage in the city. The finding from key informants also indicated the insufficient number of midwives has made the necessary care for delivering mothers difficult. The finding is consistent with a study in northern Ethiopia where half of the health facilities had fulfilled three midwives per HC. The shortage of midwives might be explained by either the limited availability in the market or a high turnover. Thus, emphasis needs to be given to increasing the number of midwives.
The proportion of HCs having separate rooms to accommodate delivering mothers was observed to be 25.0%. This finding is far from the Ethiopian standard health center requirements guideline (3 separate rooms).24 This implies limited health-care managers involved in building rooms and ensuring the safety of delivering mothers.
This evaluation showed that 70.6% of the delivery care services were implemented according to the national standards. This finding was higher than an evaluation conducted in southern Ethiopia, which showed that the compliance dimension’s average result was 46.9%.13 This may be due to the existence of differences in the availability of delivery care guidelines and differences in health-care providers’ tendency towards using labour and delivery care guidelines. For the majority (96.9%) of the mothers, health-care providers were wearing a surgical glove during labour and delivery care procedures. This encouraging finding reflected that health-care providers in Gondar city HCs have relatively adhered to the recommended infection prevention practice during childbirth care.
As an initial assessment task, fetal heartbeat was assessed for 65.6% and fetal presentation for 78.1% as per the guideline. Conducting a complete initial assessment of the laboring mother informs the decision about whether she needs extra care or referral. This finding is relatively better than the finding of the study conducted in Bishoftu town, Ethiopia.8 The difference may be explained by differences that health-care providers adhere to the documentation of initial assessment task done and attention given for timely identification of the mothers.
The finding of this evaluation also showed that partograph used for 72.0% of mothers to monitor the progress of labor for cervical dilation and maternal blood pressure plotting was done for 65.6% of mothers. This finding contrasts the Ethiopian national obstetrics management protocol guideline, which recommends that all mothers in labour be monitored by partograph.23 This inconsistency might be due to a lack of refreshment training on partograph utilisation, which implies relatively poor compliance of health-care providers to the recommended protocol.
Seventy-five percent of the newborn were started breastfeeding within an hour of delivery. This finding was comparable with the study conducted in Northern Ethiopia where 70.4% of newborn babies were early initiated for breastfeeding within an hour34 and was higher than the study conducted in Cotedivoire, in which less than 10% of babies have started breastfeeding within an hour.35 This difference shown during immediate newborn care practice might be due to the difference of knowledge and attitude of the two countries’ health-care providers towards the importance of early initiation of breastfeeding in the prevention of newborn infections.
In this evaluation, 71.9% of mothers were administered with oxytocin 10 IU IM within 1 minute after the birth of the baby. This finding was lower than a study conducted in the Oromia region, Ethiopia, which revealed that 100% of delivering mothers were administered oxytocin.8 The result might be due to the limitation of oxytocin from the pharmaceutical fund and supply agency that supplies the HCs and the inability of health-care providers to adhere to the recommended protocol.
In this evaluation, the satisfaction of delivering mothers with the convenience of waiting area, clean lines of the room, and waiting time was 65.8%, 63.3%, and 72.5%, respectively. These findings were lower than that of a study conducted in northwest Ethiopia, which reported that 95.9%, 88.7% and 95.6% of mothers were satisfied with the waiting area, cleanliness of the room, and waiting for time, respectively.2 This variation might be due to the availability of different structural set up to accommodate delivering mothers. This evaluation demonstrated that 48.6% of mothers were satisfied by the proximity of the toilet. This finding was higher than that of study findings in Gamo Gofa, southwest Ethiopia resulted in 35.5% of mothers were satisfied with the clean lines and access of the toilet36 but lower than the study conducted in Debre Markose, northwest Ethiopia where 83.3% of mothers were satisfied.2 This discrepancy might be due to differences in the accessibility of the toilet for delivering mothers near to the delivery room.
Moreover, mothers’ satisfaction with the accommodation of delivery service structural set up in Gondar city HCs was 68.8%. This finding has briefed that more than 30% of mothers were not satisfied with the delivery service structure’s accommodation. This might be due to the delivery service structure’s accommodation that might not be well structured to be convenient for delivering mothers.
The finding of the evaluation showed that 80.2% of mothers were accepted the delivery service which was judged as good. Furthermore, about 94.0% of delivering mothers had accepted the delivery service and will recommend the HCs to their families and friends for the future. This indicates that the mothers’ knowledge, attitude, and personal character of health-care providers caring for delivering mothers might be as desired.
In this evaluation, mothers’ acceptance of delivery service was associated with the residence and having ANC follow up. Those delivering mothers from rural communities were more likely to be associated with non-acceptance compared to urban residents. This finding is consistent with another study conducted in Gondar, Ethiopia27 but contrasts with the study conducted in Addis Ababa, Ethiopia.37 This might be because most rural mothers live in relatively different socio-cultural circumstances, and most of them are in a low level of educational status and they are new to the HCs environment which makes communication and understanding with health-care providers difficult and causes poor acceptance.
Moreover, mothers who had ANC1 to 3 visits had accepted the delivery service two times higher than those mothers who never had any ANC visits. Likewise, mothers who had ANC4 or more visits were five times more likely to accept delivery service than mothers who had no ANC follow-up. This finding supports the study conducted in Oromia, Ethiopia.38
Strengths and Limitations of the Evaluation
The strength of this evaluation was that the evaluation used four dimensions to evaluate the process of delivery service to address a wide area of performance aspects. Moreover, the evaluation employed both qualitative and quantitative methods to get more accurate and detailed results and covered all HCs in Gondar city to make them representative of the findings.
The limitations of this evaluation were that since the evaluation was facility-based and conducted in the health institutions, there might be a social desirability bias like showing gratitude to the health-care providers who saved their lives. This might result in relatively high levels of satisfaction and acceptance towards the service. To minimize it, intensive training of the data collectors on proper interview techniques and interviewing clients in a separate room were the strategies taken. Hawthorn’s effect during the direct observation was the other possible limitation of the evaluation, which might have contributed to the relatively high-performance scores of observant on delivering care process practices. Dropping the first three observations is recommended to minimize it.39 Because after the third session, the observant will return to his/her actual behavior. So, in this evaluation, the first 3 observations were dropped from each observant per facility.
Conclusions
The evaluation findings revealed that the overall process of the delivery service in the evaluation area was good. The availability of resources was also good. But there was insufficient manpower for delivery service; the number of midwives was sub-standard. The training status of health-care workers on BEmONC was relatively insufficient. Parenteral IV Infusions, HIV test kit, surgical gloves, and medical equipment were stock-in. However, the majority of basic parenteral signal functions were not found to be adequately provided to the HCs. Parenteral signal functions were stockout.
The delivery service’s compliance to the guideline was relatively good; however, clinical practices were not found to be adequately practised.
The accommodation of the delivery service structure was judged as poor. Moreover, the acceptability of the delivery service provided in Gondar city HCs was good.
Therefore, it is recommended that the city administrative health office should recruit midwives to the HCs as per national requirements. The HCs should act on providing BEmONC parenteral signal functions. Moreover, health workers should also comply with the standard of care for delivery service.
Abbreviations
ANC, Antenatal Care; BEmONC, Basic Emergency Management of Obstetric and Newborn Care; EDHS, Ethiopian Demography Health Survey; ETB, Ethiopian Birr; HC, Health Center; L&D, Labour and Delivery; MCH, Maternal and Child Health; MOH, Ministry of Health; MMR, Maternal Mortality Ratio; NGO, Non-Governmental Organisation; MRHO, Maternal Reproductive Health Office; UNICEF, United Nations International Children’s Emergency Fund; WHO, World Health Organization.
Data Sharing Statement
Data will be available upon reasonable request from the corresponding author.
Ethics Approval and Consent to Participate
All the ethical procedures were followed in accordance with the declaration of Helsinki. Ethical clearance was obtained from the ethical review committee of the Institute of Public Health, University of Gondar (Ref. No. IPH/837/6/2012). A permission letter was obtained from the Gondar city administration health office, and permission was assured from the heads of the HCs. Informed written consent was obtained from each participant after a brief explanation of the research objectives and data collection process of the study. Participants were also informed about their right to withdraw at any time or to skip a single question or number of questions. After ensuring their volunteerism, those participants who could read and write signed on the space provided. Whereas, for those who were unable to read and write, a fingermark (finger thumb) was taken. Finally, the confidentiality of the participants was anonymized with no any personal identifiers.
Consent for Publication
All participants provided permission to use their anonymised responses in the manuscript.
Acknowledgments
We are grateful to health office managers, heads of HCs, and heads of the delivery case team in Gondar city for their kindly support throughout this study. We would also extend our appreciation to supervisors, data collectors and study participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declared that they have no competing interests.
References
1. Islam N, Islam MT, Yoshimura Y. Practices and determinants of delivery by skilled birth attendants in Bangladesh. Reprod Health. 2014;11(1):86. doi:10.1186/1742-4755-11-86
2. Mamatha K, Thimmaiah N. Impact of Janani Suraksha Yojana on institutional delivery and infant mortality rate in Karanataka. Int J Res Soc Sci. 2014;4(3):444–454.
3. Bitew K, Ayichiluhm M, Yimam K. Maternal satisfaction on delivery service and its associated factors among mothers who gave birth in public health facilities of Debre Markos Town, Northwest Ethiopia. Biomed Res Int. 2015;2015:1–6. doi:10.1155/2015/460767
4. Fekadu M, Regassa N. Skilled delivery care service utilization in Ethiopia: analysis of rural-urban differentials based on national demographic and health survey (DHS) data. Afr Health Sci. 2014;14(4):974–984. doi:10.4314/ahs.v14i4.29
5. ICF EEMD. Health Survey, 2019. Key Indicators Rockville, Maryland, USA: EPHI and ICF; 2019.
6. Elashoff JD, Lemeshow S. Sample size determination in epidemiologic studies. In: Handbook of Epidemiology. Springer; 2005:559–594.
7. Lee AC, Lawn JE, Cousens S, et al. Linking families and facilities for care at birth: what works to avert intrapartum‐related deaths? Int J Gynecol Obstetr. 2009;107(Supplement):S65–S88. doi:10.1016/j.ijgo.2009.07.012
8. Mekonin T. Assessment of Quality of Delivery Services at Public Health Institutions in Bishoftu Town, Oromia Region, Ethiopia. Addis Ababa University; 2017.
9. Lyndon A, Lee HC, Gilbert WM, Gould JB, Lee KA. Maternal morbidity during childbirth hospitalization in California. J Matern Fetal Neonatal Med. 2012;25(12):2529–2535. doi:10.3109/14767058.2012.710280
10. Mann C, Dessie E, Adugna M, Berman P. Measuring Efficiency of Public Health Centers in Ethiopia. Massachusetts and Addis Ababa, Ethiopia: Harvard TH Chan School of Public Health and Federal Democratic Republic of Ethiopia Ministry of Health Boston; 2016.
11. Eziawdres D, Worku W, Taye M. Maternal satisfaction with delivery services and its associated factors among mothers who gave birth at public health centers in Yeka Sub City, Addis Ababa, Ethiopia. Health Services Insights. 2021;14:11786329211050722. doi:10.1177/11786329211050722
12. Sedoro T, Ejajo T, Abute L, Kedir T, Erchafo B. Process evaluation of skilled delivery service in Hadiya Zone in Southern Nations, Nationalities, and Peoples Region, Ethiopia. J Environ Public Health. 2020;2020:4717520.
13. Alemi Kebede KH, Teklehaymanot AN, Hassen K. Factors associated with institutional delivery service utilization in Ethiopia. Int J Women's Health. 2016;8:463. doi:10.2147/IJWH.S109498
14. Hagos S, Shaweno D, Assegid M, Mekonnen A, Afework MF, Ahmed S. Utilization of institutional delivery service at Wukro and Butajera districts in the Northern and South Central Ethiopia. BMC Pregnancy Childbirth. 2014;14(1):178. doi:10.1186/1471-2393-14-178
15. Worku A, Jemal M, Gedefaw A. Institutional delivery service utilization in Woldia, Ethiopia. Sci J Public Health. 2013;1(1):18–23. doi:10.11648/j.sjph.20130101.13
16. Amano A, Gebeyehu A, Birhanu Z. Institutional delivery service utilization in Munisa Woreda, South East Ethiopia: a community based cross-sectional study. BMC Pregnancy Childbirth. 2012;12(1):105. doi:10.1186/1471-2393-12-105
17. Tadele N, Lamaro T. Utilization of institutional delivery service and associated factors in Bench Maji zone, Southwest Ethiopia: community based, cross sectional study. BMC Health Serv Res. 2017;17(1):101. doi:10.1186/s12913-017-2057-y
18. Venkatachalam J, Kumar D, Gupta M, Aggarwal AK. Knowledge and skills of primary health care workers trained on integrated management of neonatal and childhood illness: follow-up assessment 3 years after the training. Indian J Public Health. 2011;55(4):298. doi:10.4103/0019-557X.92410
19. Rossi PH, Lipsey MW, Freeman HE. Evaluation: A Systematic Approach. SAGE Publications; 2003.
20. Penchansky R, Thomas JW. The concept of access: definition and relationship to consumer satisfaction. Med Care. 1981;19:127–140. doi:10.1097/00005650-198102000-00001
21. Carroll C, Patterson M, Wood S, Booth A, Rick J, Balain S. A conceptual framework for implementation fidelity. Implement Sci. 2007;2(1):1–9. doi:10.1186/1748-5908-2-40
22. Tadesse BH, Bayou NB, Nebeb GT. Mothers’ satisfaction with institutional delivery service in public health facilities of Omo Nada District, Jimma Zone. Clin Med Res. 2017;6(1):23–30. doi:10.11648/j.cmr.20170601.13
23. Health FMo. Management Protocol on Selected Obstetrics Topics. Federal Democratic Republic of Ethiopia. Health FMo; 2010.
24. EMOH. ETHIOPIAN STANDARD Health Center-Requirements ES 3611:2012.
25. Bayou NB. Quality of birthing care in low income settings: the case of Ethiopia. 2019.
26. Gebremedhin T, Daka DW, Alemayehu YK, Yitbarek K, Debie A. Process evaluation of the community-based newborn care program implementation in Geze Gofa district, south Ethiopia: a case study evaluation design. BMC Pregnancy Childbirth. 2019;19(1):1–13. doi:10.1186/s12884-019-2616-9
27. Gashaye KT, Tsegaye AT, Shiferaw G, Worku AG, Abebe SM. Client satisfaction with existing labor and delivery care and associated factors among mothers who gave birth in university of Gondar teaching hospital; Northwest Ethiopia: institution based cross-sectional study. PLoS One. 2019;14(2):e0210693. doi:10.1371/journal.pone.0210693
28. Word Health Organization. Pregnancy, Childbirth, Postpartum and Newborn Care. A Guide for Essential Practice.
29. Word Health Organization. Making Pregnancy Safer: Assessment Tool for the Quality of Hospital Care for Mothers and Newborn Babies. Copenhagen: WHO Regional Office for Europe; 2009.
30. Word Health Organization. Care in Normal Birth: A Practical Guide: Report of a Technical Working Group: Maternal and Newborn Health/Safe Motherhood Unit, Family and Reproductive. Word Health Organization; 1996.
31. Rudan I, Tomaskovic L, Boschi-Pinto C, Campbell H. Global estimate of the incidence of clinical pneumonia among children under five years of age. Bull World Health Organ. 2004;82:895–903.
32. Kumar R, Ahmed J, Anwar F, Somrongthong R. Availability of emergency obstetric and newborn care services at public health facilities of Sindh province in Pakistan. BMC Health Serv Res. 2019;19(1):968. doi:10.1186/s12913-019-4830-6
33. Baguiya A, Meda IB, Millogo T, Kourouma M, Mouniri H, Kouanda S. Availability and utilization of obstetric and newborn care in Guinea: a national needs assessment. Int J Gynecol Obstetr. 2016;135(S1):S2–S6. doi:10.1016/j.ijgo.2016.09.004
34. Fisseha G, Berhane Y, Worku A. Quality of intrapartum and newborn care in Tigray, Northern Ethiopia. BMC Pregnancy Childbirth. 2019;19(1):1–8. doi:10.1186/s12884-019-2184-z
35. Delvaux T, Ake-Tano O, Gohou-Kouassi V, Bosso P, Collin S, Ronsmans C. Quality of normal delivery care in Côte d’Ivoire. Afr J Reprod Health. 2007;11(1):22–32. doi:10.2307/30032485
36. Tesfaye R, Worku A, Godana W, Lindtjorn B. Client satisfaction with delivery care service and associated factors in the public health facilities of Gamo Gofa Zone, Southwest Ethiopia: in a resource limited setting. Obstet Gynecol Int. 2016;2016:1–7. doi:10.1155/2016/5798068
37. Melese T, Gebrehiwot Y, Bisetegne D, Habte D. Assessment of client satisfaction in labor and delivery services at a maternity referral hospital in Ethiopia. Pan Afr Med J. 2014;17:154.
38. Amdemichael R, Tafa M, Fekadu H. Maternal satisfaction with the delivery services in Assela Hospital, Arsi zone, Oromia region. Gynecol Obstet. 2014;4(257):2161.
39. Newcomer KE, Hatry HP, Wholey JS. Handbook of Practical Program Evaluation. Wiley Online Library; 2015.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Implementation Evaluation of HIV/AIDS Voluntary Counseling and Testing (VCT) Service at Public Health Facilities of Akaki Kality Sub-City, Addis Ababa, Ethiopia
Masrie A, Shawel S, Tamire A, Mandefro M, Gebru T, Ergiba Seboka M, Getachew M
HIV/AIDS - Research and Palliative Care 2023, 15:503-518
Published Date: 4 September 2023