")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Pro-Neurotensin as a Potential Novel Diagnostic Biomarker for Detection of Nonalcoholic Fatty Liver Disease
Authors Mohamed AA, Abo-Elmatty DM, Ezzat O, Mesbah NM, Ali NS, Abd El Fatah AS, Alsayed E , Hamada M , Hassnine AA, Abd-Elsalam S , Abdelghani A , Hassan MB , Fattah SA
Received 5 March 2022
Accepted for publication 27 May 2022
Published 22 June 2022 Volume 2022:15 Pages 1935—1943
DOI https://doi.org/10.2147/DMSO.S365147
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Ming-Hui Zou
Amal A Mohamed,1 Dina M Abo-Elmatty,2 Omnia Ezzat,3 Noha M Mesbah,2 Nada S Ali,3 Aliaa Sayed Abd El Fatah,4 Eman Alsayed,5 Mahmoud Hamada,6 Alshymaa A Hassnine,7 Sherief Abd-Elsalam,8 Ahmed Abdelghani,9 Mohamed Badr Hassan,9 Shaimaa A Fattah2
1Biochemistry and Molecular Biology Department, National Hepatology and Tropical Medicine Research Institute, Cairo, Egypt; 2Biochemistry Department, Faculty of Pharmacy, Suez Canal University, Ismailia, Egypt; 3Biochemistry Department, Faculty of Pharmacy, Egyptian Russian University, Cairo, Egypt; 4Internal Medicine Department, Faculty of Medicine, Minia University, Minia, Egypt; 5Department of Clinical Pathology, Minia University Hospital, Minia, Egypt; 6Internal Medicine Department, Faculty of Medicine, Benha University, Benha, Egypt; 7Department of Gastroenterology and Tropical Medicine, Faculty of Medicine, Minia University, Minia, Egypt; 8Tropical Medicine Department, Tanta University, Tanta, Egypt; 9Internal Medicine Department, Faculty of Medicine, Cairo University, Cairo, Egypt
Correspondence: Sherief Abd-Elsalam, Department of Tropical Medicine, Faculty of Medicine, Tanta University, El-Bahr Street, Tanta, Egypt, Tel +201147773440, Email [email protected]
Background and Aims: Currently, liver biopsy is the gold standard method for diagnosis of non-alcoholic fatty liver severity. It is critical to develop non-invasive diagnostic method to diagnose nonalcoholic fatty liver rather than invasive techniques. Our case–control study was to address the value of circulating miRNA-122 and serum pro-neurotensin as a potential non-invasive biomarker for the diagnosis of non-alcoholic fatty acid diseases.
Methods: Clinical assessment, laboratory investigations, and anthropometric measurements were reported for 157 patients with proven NAFLD. Apparently, healthy participants (n=100) were enrolled as a control group. Serum samples were tested for micro-RNAs− 122 and pro-neurotensin.
Results: Compared with the control subjects, both mi-RNA-122 and serum proneurotensin levels were increased in NAFLD (p< 0.001) and at a cut-off ≥ 6.83, mi-RNA-122 had 51.0% sensitivity, 70.0% specificity to differentiate NAFLD from healthy controls, while serum proneurotensin had 80.0% sensitivity and 80.0% specificity at a cutoff ≥ 108.
Conclusion: The circulating pro-neurotensin might be used as a novel biomarker for diagnosis of patients with NAFLD, wherefore the integration of a circulating mi-RNA-122 and serum pro-neurotensin could be beneficial to diagnose NAFLD cases. Large-scale studies are needed to investigate the possible role of mi-RNA-122 and pro-neurotensin in the development, progression, and prognosis of NAFLD and NASH.
Keywords: nonalcoholic fatty liver disease, NAFLD, metabolic associated fatty liver disease, MAFLD, biomarker, proneurotensin, micro-RNA-122, noninvasive, diagnosis, fatty liver
Introduction
Nonalcoholic fatty liver disease (NAFLD) is considered one of the health problems with great burden on the liver that may end with liver cirrhosis and hepatocellular carcinoma.1 Universally, nonalcoholic fatty liver disease (NAFLD) has a prevalence of 24% and is considered as a high risk of liver-related morbidity and mortality,2 which has been described as the most important precursor to hepatocellular carcinoma (HCC).3 NAFLD is characterized by the macrovesicular accumulation of triglycerides in the liver cells, leading to necro-inflammation and fibrosis, and may progress to cirrhosis and hepatocellular carcinoma. HCC is considered the fifth most abundant type of tumor worldwide and the third most lethal cancer, causing 600,000 deaths each year.4,5 Ultrasound is the most widely used imaging test for NAFLD diagnosis, but its sensitivity decreases if <30% of the liver is affected by steatosis. Additionally, computed tomography (CT scan) is accurate for diagnosing moderate-to-severe liver steatosis; however, it is not accurate for detecting mild steatosis.6
Liver biopsy is the gold standard invasive procedure for diagnosis of non-alcoholic fatty liver disease.7 And so it is critical to develop non-invasive diagnostic method to diagnose nonalcoholic fatty liver rather than invasive techniques. MicroRNAs (miRNAs) are small non-coding RNAs that have been discovered to play a vital role in transcriptional control mechanisms and guiding metabolic homeostasis.8 Mi-RNAs are detectable in almost all body fluids like serum, plasma, and urine. They are resistant to extreme conditions, such as low or high pH, extreme temperature, and RNAs activity.9,10 They have been suggested as diagnostic biomarkers for non-invasive assessment of the pathological state of their origin organ from peripheral blood.11 MicroRNA-122 is involved in hepatocyte proliferation and maturation by stimulating the expression of some specific genes. In addition, it interacts with numerous target genes involved in lipid and cholesterol metabolism.12 Mi-RNA-122 is implicated in NASH development, such as fatty acid synthase (FAS), 3-hydroxy-3-methylglutaryl-CoA reductase (HMGCR), sterol regulatory element-binding protein-1c (SREBP-1c), and sterol regulatory element-binding protein 2 (SREBP-2).13 The circulating levels of miR-122 correlate with alanine aminotransferase (ALT) and aspartate aminotransferase (AST) levels in patients with NAFLD compared with the classic liver function markers.12
Neurotensin (NT) is an amino acid peptide secreted mainly by neuroendocrine cells in the small intestine.14 It plays an important role in regulating food ingestion and fat absorption.15 An acute increase in intestinal NT release occurs shortly after food ingestion.16 Many studies have described the role of NT in facilitating lipid digestion and fat absorption in the small intestine.17,18 Recently, Li et al reported reduced intestinal fat absorption, along with protection from obesity and NAFLD, in NT-deficient mice fed with a high-fat diet. Moreover, the authors demonstrated that higher plasma pro-NT levels in humans; were associated with insulin resistance and a higher risk of developing obesity later in life in non-obese individuals.19 There were no previous studies on serum proneurotensin level in NAFLD and so, to our knowledge, our current study is considered the first study on this issue. The aim of this study was to assess the expression of serum mi-RNA-122 and detection of serum proneurotensin status in a group of Egyptian patients with nonalcoholic fatty liver disease.
Patients and Methods
This case–control study was conducted on 157 patients with proven NAFLD Patients who were recruited from the outpatient clinic of the Faculty of Medicine, Minia University and Cairo Universities between October 2020 and September 2021. NAFLD diagnosis was proven by abdominal ultrasonography and laboratory investigations. Detailed history and complete laboratory examination were done for all participants including a patient history: name, age, history of smoking, drug history, and family history of any chronic diseases, complete clinical examination and anthropometric measurements that were performed to all patients and controls, the body mass index (BMI) was calculated as weight (in kilograms) divided by height squared (meters squared), liver function tests (alanine transaminase [ALT], aspartate transaminase [AST], gamma-glutamyltransferase [GGT], alkaline phosphatase [ALP], albumin), INR, CRP, Hb, total bilirubin, and total leukocytic count, lipid profiles (triglycerides [TG], high-density lipoprotein [HDL], low-density lipoprotein [LDL] cholesterol) and Alpha-feto protein [AFP].
Nonalcoholic fatty liver disease is characterized by excessive fat accumulation in the liver. It is associated with insulin resistance, central adiposity, increased BMI, hypertension, and hyperlipidemia, which collectively are features of metabolic syndrome. Diagnosis is usually made after an incidental discovery of unexplained elevation of liver enzyme levels or when steatosis is noted on imaging (eg, ultrasonography). Patients are often asymptomatic, and the physical examination is often unremarkable. Not a single laboratory test is diagnostic, but tests of liver function, tests for metabolic syndrome, and tests to exclude other causes of abnormal liver enzyme levels are routinely performed. Imaging studies, such as ultrasonography, computed tomography, and magnetic resonance imaging, can assess hepatic fat, measure liver and spleen size, and exclude other diseases.20 We excluded patients with history of viral hepatitis (hepatitis B virus and hepatitis C virus), autoimmune hepatitis, hepatocellular carcinoma, alcohol consumption, liver cirrhosis, diabetes mellitus, Wilson’s disease, secondary cause of hepatitis, drug-induced hepatitis, or obstructive biliary disease. One-hundred apparently healthy subjects with normal laboratory investigations and abdominal ultrasound were included as a control group.
A written informed consent was taken from all subjects, and the study was approved by the Research Ethics Committee. This study was performed in compliance with the ethics principles of the declaration of Helsinki for Good Clinical Practice guidelines.
Blood Sampling
Venous blood (10 mL) was drawn from participants after an 8–12 h fast. A 3-mL portion was collected into dry sterile vacutainer tubes and used for serum separation was left to clot at room temperature, and then centrifuged at 3000 ×g for 10 min at 4°C. Another 3-mL tube used for sera separation for the detection of micro 122 and pro-neurotensin was stored at −80°C until use. Liver function tests (alanine transaminase [ALT], aspartate transaminase [AST], gamma-glutamyltransferase [GGT], alkaline phosphatase [ALP], albumin), and lipid profiles (triglycerides [TG], and high-density lipoprotein [HDL] and low-density lipoprotein [LDL] cholesterol) creatinine were assayed in sera by Beckman automated biochemistry analyzer. The 2-mL tubes containing EDTA for complete blood picture by phoenix 3300 and 2 mL were collected in tubes containing sodium citrate for INR detection.
Detection of Serum Pro-Neurotensin
Serum pro-neurotensin was determined by enzyme linked immunosorbent assay (ELISA) using kits obtained from science and technology company (Bioassay Technology Laboratory SH. China), according to manufacturer’s instructions the test was done.
Detection of Micro 122
Total RNA extraction and purification was done using a miRNeasy Mini Kit; cat no: 217004 (Qiagen, Hilden, Germany) according to the manufacturer’s protocol. cDNA was synthesized by reverse transcription reaction using TaqMan MicroRNA Reverse Transcription Kit; cat no: 4366596 (Applied Biosystems, Foster City, USA) and the thermal cycler (Quanta Biotech). The quantification of miR-122 level was amplified from cDNA using TaqMan universal Master Mix and TaqMan assay (has-miR-122; Catalog no: 4427975; Assay ID: 002245). The RNU49 was used as housekeeper gene (RNU49; Cat no: PN4427975; ID: 001005). All the samples were analyzed using the 5 plex Rotor-Gene PCR Analyzer (Qiagen, Germany). The 2ΔΔCt method was conducted for the analysis of gene expression levels using TaqMan microRNA Control Assays RNU49as an endogenous reference control for normalization purposes.20
Statistical Analysis
Data were entered and cleaned using Excel and exported to IBM SPSS software, version 21.0 for Statistical analysis. Descriptive statistics such as mean, median, SDs and percentage were used to describe the patients’ characteristics and barriers to access to care. The relationships between patient characteristics and follow-up status were done by proper statistical test (the Chi-Square test and Fisher’s exact test). All significant relationships with a p value <0.05 were considered for further analysis in binary logistics regression models. Of all statistical tests used, P-values less than 0.05 are considered significant.
Results
Our study included 157 patients with NAFLD (86 males and 71 females) with a median age of 56 years. Healthy controls were 100 subjects (57 males and 43 females) with a median age of 38 years. There was a statistically significant increase in the BMI, ALT, AST, ALP, GGT, total bilirubin, and serum albumin, INR, and AFP in NAFLD patients compared to the control group, while serum creatinine, hemoglobin and total leucocytic count showed non-significant differences between both groups (Table 1). NAFLD patients had a higher significant level of serum triglycerides, total cholesterol, HDL-cholesterol, and LDL-cholesterol compared to the controls (Table 1).
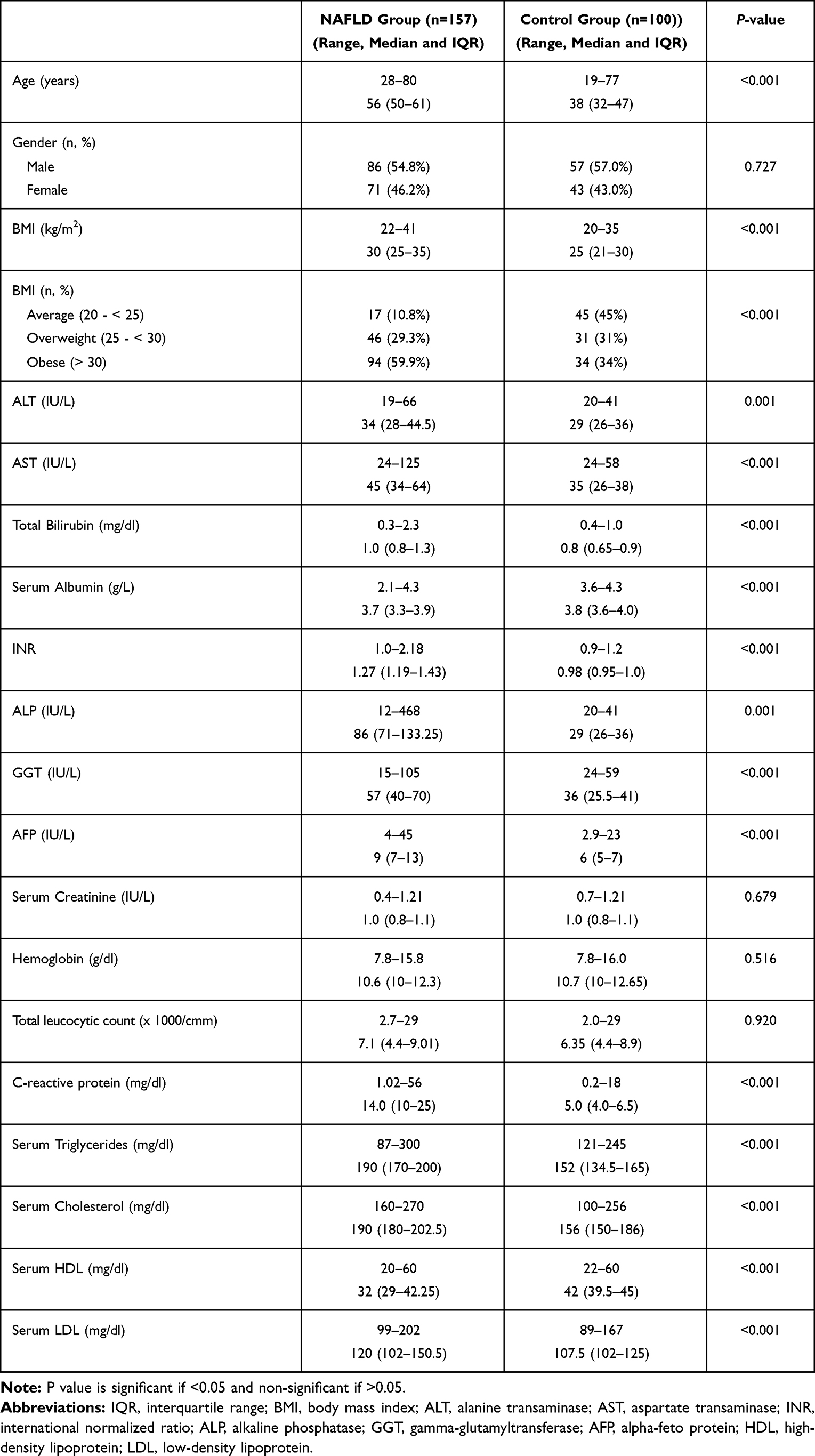 |
Table 1 Demographic and Biochemical Parameters Between NAFLD Patients and Controls |
Table 2 and Figure 1 show that the median levels of serum proneurotensin and miRNA-122 were significantly higher in NAFLD patients compared to the control group, MI all the laboratory parameters and all histological findings. The level of miRNA-122 had a significant positive correlation with ALT, AST, total bilirubin, CRP, total leucocytic count, AFP, INR, ALP, and total cholesterol, whereas it showed negative correlation with HDL-cholesterol. In contrast, the level of serum proneurotensin showed positive correlation with hemoglobin and negative correlation with total leucocytic count (Table 3).
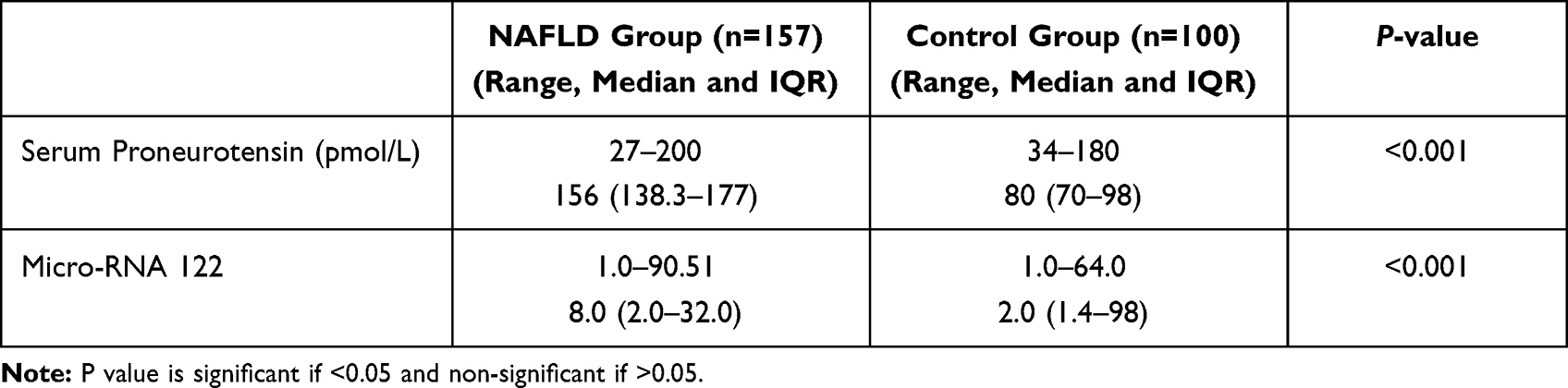 |
Table 2 Difference Between Groups Regarding Serum Proneurotensin and Micro-RNA-122 Assay |
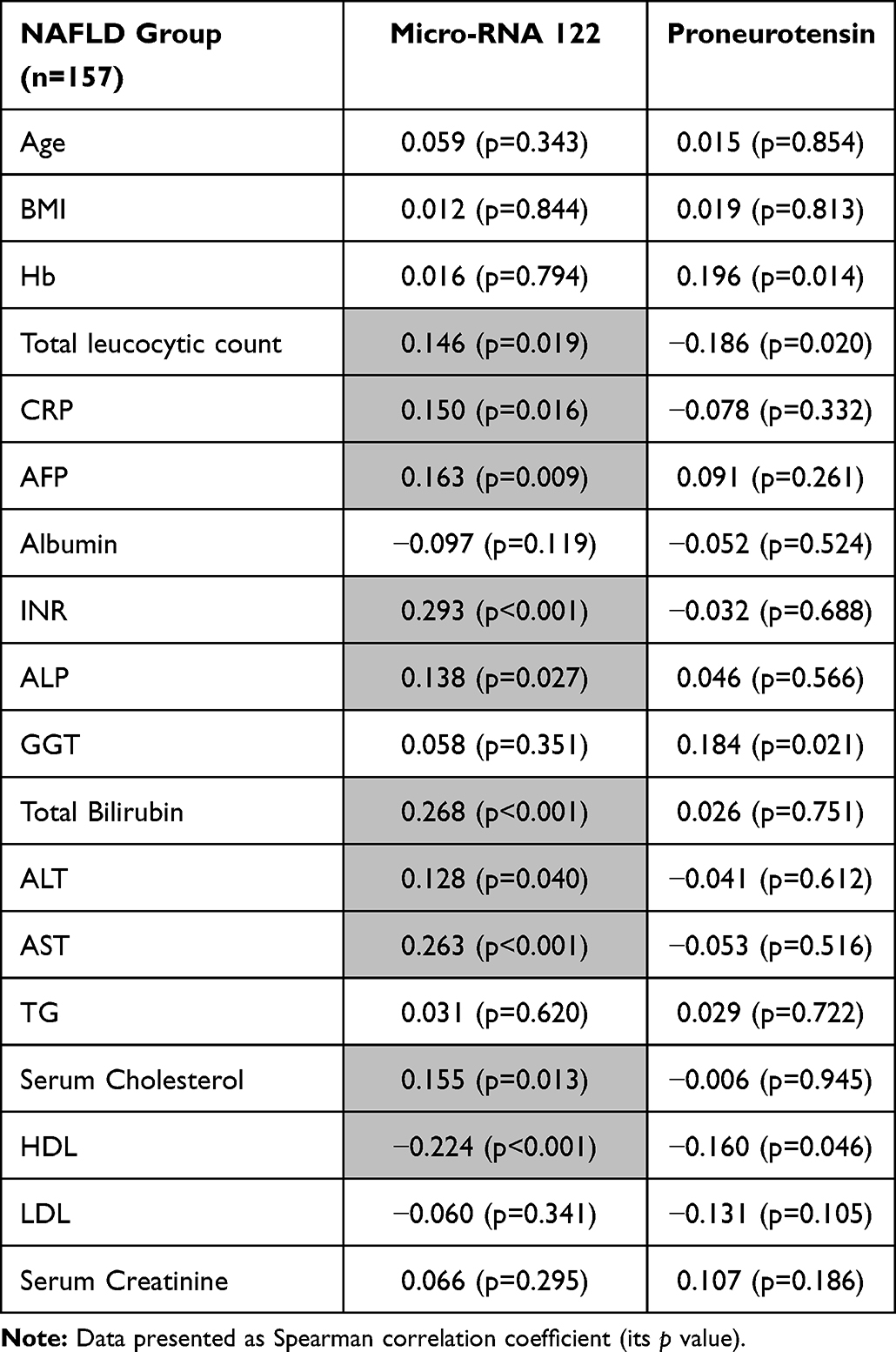 |
Table 3 Correlation Between Each of Serum Proneurotensin and Micro-RNA-122 and Other Measured Variables in NAFLD Group |
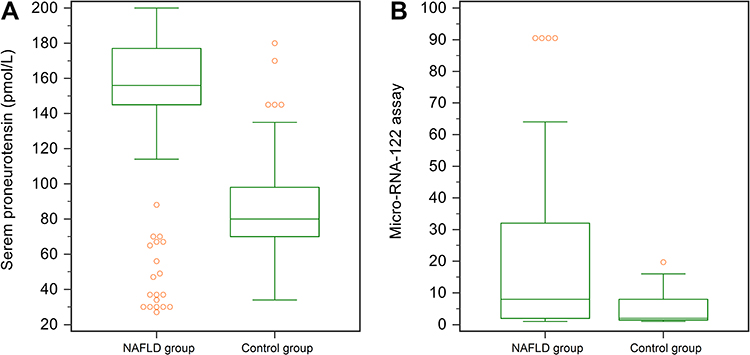 |
Figure 1 Box-and-whisker plot chart showing difference between groups regarding: (A) serum proneurotensin, (B) serum micro-RNA-122. |
The ROC curve demonstrated that serum proneurotensin and mi-RNA-122 can differentiate between NAFLD patients and healthy controls at a cut-off ≥108, ≥6.83 respectively. The AUC for serum proneurotensin was 0.811 with a sensitivity (80.0%) and specificity (80.0%) followed by mi- RNA-122 with AUC = 0.654 and a sensitivity (51.0%) and a specificity (70.0%) (Table 4, Figure 2).
 |
Table 4 Cut off Value of Pro-Neurotensin and microRNA 122 in Diagnosis of NAFLD |
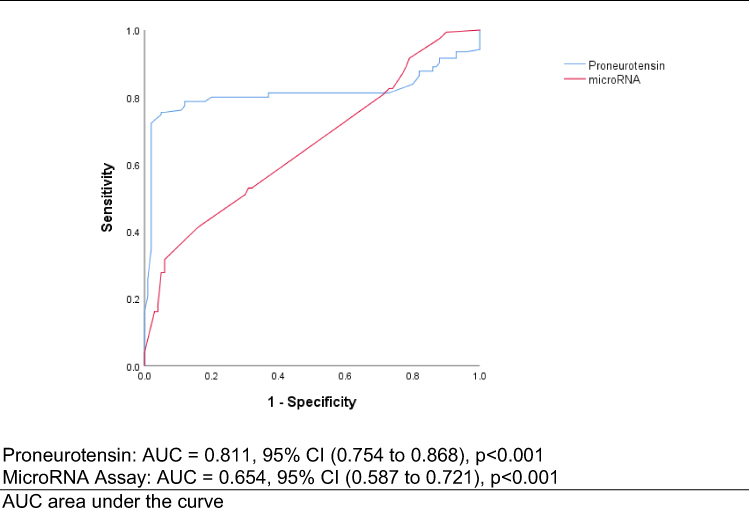 |
Figure 2 ROC curve for diagnosis of pro-neurotensin and microRNA 122 assay in NAFLD patients. |
Discussion
Liver biopsy is the gold standard invasive procedure that takes very small samples from different areas within the liver tissue to investigate the number of liver cells containing fat droplets (steatosis), the degree of liver cell damage, inflammation and the degree of liver fibrosis.21 It can help in the diagnosis of NAFLD severity by providing information about grading, staging, and prognosis. However, it is an invasive procedure with several limitations.22 Many non-invasive tests are available and may reduce the need for liver biopsy but are not specific to NAFLD, such as alpha-fetoprotein and many other nonspecific markers. AFP is a glycoprotein that is normally generated during conception by the fetal liver. In clinical practice, AFP levels are elevated in many clinical situations such as hepatocellular carcinoma, acute or chronic viral hepatitis, chronic liver disease, and gonadal tumors.23–39
Mi-RNAs play an important role in many liver diseases such as viral hepatitis, cancer, and liver fibrosis.24 MicroRNA-122 is the most abundant hepatic miRNA; it represents 70% of the total hepatic miRNAs.12 A large number of studies are interested in the identification and validation of a simpler, non-invasive biomarker for the detection of NAFLD.
Our study showed a significant increase in the level of mi-RNA-122 in NAFLD patients compared to healthy controls. This comes in accordance with several studies who reported that mi-RNA-122 is significantly increased in the serum of NAFLD patients.22,26 Pirola et al reported that miR-122 levels are 7.2 times higher in patients with NASH compared to healthy subjects, suggesting it as an extrahepatic NASH marker.12 On the contrary, Cheung et al found that mi-RNA-122 expression was significantly decreased in NASH patients. The authors confer its downregulation to the alteration of hepatic lipid metabolism genes.27
We found that the levels of mi-RNA-122 were positively correlated with the serum levels of AST, ALT, and ALP. These findings were in agreement with Waidmann et al who found that there is a highly significant correlation between serum miR-122 levels and alanine aminotransferase (ALT), aspartate aminotransferase (AST), γ-glutamyltransferase (GGT) and alkaline phosphatase (ALP). Therefore, miRNA-122 may behave as a biomarker for hepatic injury.28
Although we found that the serum miRNA-122 expression in NAFLD was significantly associated with high levels of total bilirubin, the international normalized ratio (INR), and C-reactive protein (CRP), Waidmann et al reported that miRNA-122 has a negative correlation with the international normalized ratio (INR), total bilirubin, and total protein levels.28 Additionally, the current study showed that there is a positive relationship between over-expression of miRNA-122 and elevated serum of cholesterol, TG, and LDL. This is comparable to Gao et al, who found that the plasma levels of miR-122 was increased in patients with hyperlipidemia, and positively correlated with cholesterol, TG, and LDL-C levels, suggesting that the circulating miR-122 might be used as a target biomarker for hyperlipidemia.29
The association between altered expression of serum NT and pathophysiology of NAFLD and whether there is a relation between susceptibility and NASH is largely unknown. Previous studies found an association between higher pro-NT and the development of obesity and cardiometabolic diseases.30,31 We observed that the circulating level of serum pro-neurotensin is significantly higher in patients with NAFLD. In addition, Barchetta et al observed a linear association between pro-NT, hepatic damage in NASH, and parameters related to glucose metabolism impairment. The authors assume that increased pro-NT levels help the absorption of fatty acids from the small intestine, leading to fat accumulation at specific sites, such as the liver.32
Regarding the diagnostic value, the AUC for serum proneurotensin was 0.811 with a sensitivity (80.0%) and specificity (80.0%) followed by mi- RNA-122 with AUC = 0.654 and a sensitivity (51.0%) and a specificity (70.0%) (p<0.001). Taking into account that a diagnostic tool is good if the AUROC is >0.8 and excellent if the AUROC is > 0.933 therefore, the serum pro-NT may have a better diagnostic value and serve as a good predictor for NAFLD diagnosis compared to mi-RNA −122. The current study is the first to investigate the circulating level of serum pro-neurotensin in the patients with NAFLD, and the results showed that the median serum proneurotensin was significantly higher in group I [NAFLD Group] when compared to group II [Control Group]. Although the median micro-RNA-122 was significantly higher in group I, it was considered statistically lower when compared with the serum pro-neurotensin level elevation, suggesting that circulating pro-neurotensin might be used as a novel biomarker for patients with NAFLD.
Conclusion
In conclusion, we found that the levels of serum pro-NT may help as a non-invasive biomarker for NAFLD prediction and diagnosis. In addition, increased serum level of micro-RNA-122 may identify the presence of NAFLD. Large scale studies are warranted to investigate the possible role of mi-RNA-122 and pro-NT in the development, progression, and prognosis of NAFLD and NASH.
Human and Animal Rights
No animals were used in this research. All human research procedures were followed in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
Standards for Reporting
STROBE guidelines were followed for this case–control study.
Data Sharing Statement
Data are available upon reasonable request from the corresponding author.
Ethics Approval and Consent to Participate
The study was approved by the Research Ethics Committee of Minia University.
Consent for Publication
Informed consent was signed by every patient before enrolment in the study.
Funding
There is no funding to report.
Disclosure
The authors declare no conflict of interest, financial or otherwise.
References
1. Ahmed AM, Ghany MA, Hakeem GLA, et al. Assessment of vitamin D status in a group of Egyptian children with nonalcoholic fatty liver disease. Nutr Metab. 2016;13(1):1–6.
2. Younossi Z, Anstee QM, Marietti M, et al. Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol. 2018;15:11–20. doi:10.1038/nrgastro.2017.109
3. Mohamed AA, Elsaid OM, Amer EA, et al. Clinical significance of SNP (rs2596542) in histocompatibility complex class I-related gene A promoter region among hepatitis C virus related hepatocellular carcinoma cases. J Adv Res. 2017;8(4):343–349. doi:10.1016/j.jare.2017.03.004
4. Starley BQ, Calcagno CJ, Harrison SA. Nonalcoholic fatty liver dis- ease and hepatocellular carcinoma: a weighty connection. Hepatology. 2010;51(5):1820–1832. doi:10.1002/hep.23594
5. Mohamed AA, Ahmed HH, ElSadek SM, et al. A study of leptin and its gene 2548 G/A Rs7799039 single-nucleotide polymorphisms in Egyptian children, a single-center experience. Clin Res Hepatol Gastroenterol. 2021;45:101724. doi:10.1016/j.clinre.2021.101724
6. Ferreira DM, Simao AL, Rodrigues CM, Castro RE. Revisiting the metabolic syndrome and paving the way for microRNAs in non-alcoholic fatty liver disease. FEBS J. 2014;281(11):2503–2524. doi:10.1111/febs.12806
7. Arab JP, Barrera F, Arrese M. The evolving role of liver biopsy in non-alcoholic fatty liver disease. Ann Hepatol. 2018;17(6):899–902. doi:10.5604/01.3001.0012.7188
8. Ardekani AM, Naeini MM. The role of microRNAs in human diseases. Avicenna J Med Biotechnol. 2010;2(4):161–179.
9. Lee RC, Ambros V. An extensive class of small RNAs in Caenorhabditis elegans. Science. 2001;294(5543):862–864. doi:10.1126/science.1065329
10. Ambros V. The functions of animal microRNAs. Nature. 2004;431(7006):350–355. doi:10.1038/nature02871
11. Weiland M, Gao XH, Zhou L, Mi QS. Small RNAs have a large impact: circulating microRNAs as biomarkers for human diseases. RNA Biol. 2012;9(6):850–859. doi:10.4161/rna.20378
12. Pirola CJ, Fernández Gianotti T, Castaño GO, et al. Circulating microRNA signature in non-alcoholic fatty liver disease: from serum non-coding RNAs to liver histology and disease pathogenesis. Gut. 2015;64(5):800–812; PMID: 24973316; PMCID: PMC4277726. doi: 10.1136/gutjnl-2014-306996
13. Gori M, Arciello M, Balsano C. MicroRNAs in nonalcoholic fatty liver disease: novel biomarkers and prognostic tools during the tran- sition from steatosis to hepatocarcinoma. Biomed Res Int. 2014;2014:741465. doi:10.1155/2014/741465
14. Goedert M, Emson PC. The regional distribution of neurotensin like immunoreactivity in central and peripheral tissues of the cat. Brain Res. 1983;272(2):291–297. doi:10.1016/0006-8993(83)90576-0
15. Ferris CF, Hammer RA, Leeman SE. Elevation of plasma neurotensin during lipid perfusion of rat small intestine. Peptides. 1981;2(Suppl 2):263–266. doi:10.1016/0196-9781(81)90042-5
16. Leeman SE, Carraway RE. Neurotensin: discovery, isolation, characterization, synthesis and possible physiological roles. Ann N Y Acad Sci. 1982;400(1):1–16. doi:10.1111/j.1749-6632.1982.tb31557.x
17. Gui X, Carraway RE. Enhancement of jejunal absorption of conjugated bile acid by neurotensin in rats. Gastroenterology. 2001;120(1):151–160. doi:10.1053/gast.2001.20876
18. Gui X, Dobner PR, Carraway RE. Endogenous neurotensin facilitates enterohepatic bile acid circulation by enhancing intestinal uptake in rats. Am J Physiol Gastrointest Liver Physiol. 2001;281(6):G1413–G1422. doi:10.1152/ajpgi.2001.281.6.G1413
19. Li J, Song J, Zaytseva YY, et al. An obligatory role for neurotensin in high-fat diet-induced obesity. Nature. 2016;533(7603):411–415. doi:10.1038/nature17662
20. Chen C, Tan R, Wong L, Fekete R, Halsey J. Quantitation of microRNAs by real-time RT-qPCR. In: Park DJ, editor. Vol. 687. Methods. Totowa, NJ: Humana Press; 2011:113–134. Doi:10.1007/978-1-60761-944-4_8
21. Salvoza NC, Klinzing DC, Gopez-Cervantes J, Baclig MO. Association of circulating serum mi-RNA-34a and mi-RNA-122 with dyslipidemia among patients with non-alcoholic fatty liver disease. PLoS One. 2019;11(4):e0153497. doi:10.1371/journal
22. Cermelli S, Ruggieri A, Marrero JA, Ioannou GN, Beretta L. Circulating microRNAs in patients with chronic hepatitis C and non-alcoholic fatty liver disease. PLoS One. 2011;6(8):e23937. doi:10.1371/journal.pone.0023937
23. Tryndyak VP, Latendresse JR, Montgomery B, et al. Plasma microRNAs are sensitive indicators of inter-strain differences in the severity of liver injury induced in mice by a choline- and folate-deficient diet. Toxicol Appl Pharmacol. 2012;262(1):52–59. doi:10.1016/j.taap.2012.04.018
24. Becker PP, Rau M, Schmitt J, et al. Performance of serum microRNAs −122, −192 and −21 as biomarkers in patients with non-alcoholic Steatohepatitis. PLoS One. 2015;10:e0142661. doi:10.1371/journal.pone.0142661
25. Auguet T, Aragonès G, Berlanga A, et al. miR33a/miR33b* and miR122 as possible contributors to hepatic lipid metabolism in obese women with nonalcoholic fatty liver disease. Int J Mol Sci. 2016;17:1620. doi:10.3390/ijms17101620
26. Jampoka K, Muangpaisarn P, Khongnomnan K, Treeprasertsuk S, Tangkijvanich P, Payungporn S. Serum mi-RNA-29a and mi-RNA- 122 as potential biomarkers for Non-Alcoholic Fatty Liver Disease (NAFLD). Microrna. 2018;7(3):215–222. doi:10.2174/2211536607666180531093302
27. Cheung O, Puri P, Eicken C, et al. Nonalcoholic steatohepatitis is associated with altered hepatic microRNA expression. Hepatology. 2008;48(6):1810–1820. doi:10.1002/hep.22569
28. Waidmann O, Köberle V, Brunner F, Zeuzem S, Piiper A, Kronenberger B. Serum microRNA-122 predicts survival in patients with liver cirrhosis. PLoS One. 2012;7(9):e45652. doi:10.1371/journal.pone.0045652
29. Gao Y, He Y, Ding J, et al. An insertion/deletion polymorphism at miRNA-122 binding site in the interleukin-1a 3′untranslated region confers risk for hepatocellular carcinoma. Carcinogenesis. 2009;30:2064–2069. doi:10.1093/carcin/bgp283
30. Melander O, Maisel AS, Almgren P, et al. Plasma proneurotensin and incidence of diabetes, cardiovascular disease, breast cancer, and mortality. JAMA. 2012;308(14):1469–1475. doi:10.1001/jama.2012.12998
31. Januzzi JL
32. Barchetta I, Cimini FA, Leonetti F, et al. Increased plasma proneurotensin levels identify NAFLD in adults with and without type 2 diabetes. J Clin Endocrinol Metab. 2018;103(6):2253–2260. PMID: 29590379. doi:10.1210/jc.2017-02751
33. Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology. 1982;143:29–36. doi:10.1148/radiology.143.1.7063747
34. Abdelfattah AAM, Rizk F, Hawash N, Hanafy A, El-Kalla F, Abd-Elsalam S. Randomized trial of preoperative administration of oral pregabalin for postoperative analgesia in patients scheduled for radiofrequency ablation of focal lesions in the liver. Int J Hyperthermia. 2018;34(8):1367–1371. doi:10.1080/02656736.2018.1424946
35. Wasfy E, Elkassas G, Elnawasany S, et al. Predicting esophageal varices in cirrhotic hepatitis C virus patients using noninvasive measurement of insulin resistance variables. Endocr Metab Immune Disord Drug Targets. 2018;18(6):573–580. PMID: 30073932. doi:10.2174/1871530318666180803120428
36. Mohamed AA, El-Toukhy NER, Said EM, et al. Hepatitis C virus: efficacy of new DAAs regimens. Infect Disord Drug Targets. 2020;20(2):143–149. PMID: 30663575. doi:10.2174/1871526519666190121114003
37. Soliman H, Ziada D, Salama M, et al. Predictors for fibrosis regression in chronic HCV patients after the treatment with DAAS: results of a real-world cohort study. Endocr Metab Immune Disord Drug Targets. 2019;19:1–8. PMID: 31448717. doi:10.2174/187153031901181217112442
38. El-Gebaly F, Abou-Saif S, Elkadeem M, et al. Study of serum soluble programmed death ligand 1 as a prognostic factor in hepatocellular carcinoma in Egyptian patients. Curr Cancer Drug Targets. 2019;19(11):896–905. doi:10.2174/1568009619666190718141647
39. Watany M, Badawi R, Elkhalawany W, Abd-Elsalam S. Study of dickkopf-1 (DKK-1) gene expression in hepatocellular carcinoma patients. J Clin Diagn Res. 2017;11(2):OC32–OC34. doi:10.7860/JCDR/2017/23095.9450
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.