Back to Journals » International Journal of General Medicine » Volume 13
Prioritizing Factors Affecting Deceased Organ Donation in Malaysia: Is a New Organ Donation System Required?
Authors Naghavi N ![]() , Mubarik MS, Rasiah R
, Mubarik MS, Rasiah R ![]() , Sharif Nia H
, Sharif Nia H
Received 11 March 2020
Accepted for publication 26 August 2020
Published 17 September 2020 Volume 2020:13 Pages 641—651
DOI https://doi.org/10.2147/IJGM.S253372
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Navaz Naghavi,1 Muhammad Shujaat Mubarik,2 Rajah Rasiah,3 Hamid Sharif Nia4
1Faculty of Business & Law, Taylor’s Business School, Taylor’s University, Lakeside Campus, Subang Jaya 47500, Selangor, Malaysia; 2Faculty of Business Administration & Social Sciences, Mohammad Ali Jinnah University, Karachi 7500, Pakistan; 3Asia-Europe Institute, University of Malaya, 50603 Kuala Lumpur, Malaysia; 4Department of Nursing, Mazandaran University of Medical Science, Sari, Iran
Correspondence: Hamid Sharif Nia
Department of Nursing, Mazandaran University of Medical Science, Sari, Iran
Tel +989111275093
Email [email protected]
Purpose: The gap between the demand and the supply of human organs for transplantation is on the rise in Malaysia, despite the efforts of governments to promote donor registration. Factors affecting willingness to donate are contextual and vary from country to country. This research mainly focuses on the selection of most suitable organ donation system through factors affecting willingness to donate in Malaysia. The objectives of this study are to prioritize those factors acting as the pillars of the organ donation system and further to select the most suitable organ donation system for Malaysia.
Patients and Methods: The data were collected from 35 experts by using a bipolar questionnaire. The study applied an analytical hierarchal process (AHP) for prioritization factors contributing to willingness to donate and then selection of a suitable organ donation system based on prioritized factors.
Results: Based on the AHP results, it is evident that donation perception (0.36) has the highest priority in influencing organ donation rates, followed by socioeconomic status (0.32), demographic factors (0.23), and financial incentives (0.09). Further, our results challenge the existing opt-in donation system in Malaysia and present a presumptive approach as a suitable system for increasing deceased donation rate in Malaysia. Presumptive approach promotes the role of health-care professionals in securing the family consent.
Conclusion: This approach is a person-oriented rather than process-oriented strategy and it relies on designated requesters’ skills to evoke altruism among bereaved families. Based on results, the authors recommended that relevant government agencies focus on training nurses to discuss donation with bereaved families and raising public awareness.
Keywords: analytical hierarchal process, AHP, deceased organ donation, presumptive approach, willingness to donate, WTD
Introduction
Ever seen the bumper sticker, “Don’t take your organs to Heaven, Heaven knows we need them here!”? Whether or not we believe in God, the question arises why we are taking our organs to the crematorium, or graveyard, when they could be potentially used to save someone’s life.1
Transplantation technologies are considered one of the most efficacious medical advancements of the twenty-first century. Having an organ transplant can be more cost effective than alternative therapies.2,3 However, the current supply of transplantable organs is much lower than the need for them. This widening gap between the number of organ donors and recipients is a serious challenge for governments worldwide.4 Despite the fact that one deceased donor can save an incredible eight lives, the deceased donation rates in Asia are disproportionately lower than those in Western countries.5 Similarly, regardless of serious efforts of the Malaysian government to increase deceased organ donation, the donation rate currently stands at 0.19 donor per one million population.6 In January 2017, there were 21,513 individuals on the waiting lists of organ recipient candidates.7 Although the statistics related to donation pledges indicate an increase in the last six years (in January 2017, 385,173 donor pledges were recorded in Malaysia), there were only 71 actual donors throughout the country in 2016.8 While 521,500 of deaths due to road accidents were recorded in 2016 in Malaysia,9 this precious source of organ procurement is not exploited due to low awareness and limited consent among people. These facts indicate that the current Malaysian organ donation (OD) system should be revised.
Three types of donation systems are commonly adopted to procure deceased organs, namely opt-out (presumed consent), opt-in, and presumptive approach. Different countries have varying levels of success in applying these systems. It is opined that the high donation rate in Spain is a result of the opt-out system in place in this country. Successful implementation of the so-called “Spanish model” in Latin American countries such as Uruguay and Argentina provides further support for the efficiency of the opt-out model for raising deceased organ donation rates. In general, countries that have adopted the opt-in system (with the exception of Germany and Denmark) have struggled to bridge the gap between the organ supply and the demand for viable organs. Further, Wales (part of the UK) has successfully raised the organ donation rates by adopting the presumed consent system. As a result of adopting the opt-in system, Malaysia has been among the countries with the lowest deceased organ donation rates.
The aforementioned findings imply that the effectiveness of any of the discussed OD systems (opt-in, opt-out, and presumptive approach) largely depends upon the way they address the factors affecting willingness to donate (WTD). Due to educational, cultural, and societal circumstances, the relative importance of such factors may differ by country. For example, in a society where altruistic deeds are highly valued and widely recognized, whereas forced donations are considered intrusion in human autonomy, the opt-in donation system seems more suitable. In this vein, extensive research has been conducted to identify the factors influencing donation rates in Malaysia.4,10,11 However, current literature does not provide sufficient evidence to allow informed examination of each OD system with respect to these factors. Similarly, numerous researchers have attempted to identify the most suitable donation system for different countries.12–14 However, they have not provided guidelines for choosing the most appropriate organ donation policy on the basis of importance of factors affecting donation in each culture. The donation criteria vary from country to country and are highly contextual, which has prompted the present investigation. Its aim is to prioritize the factors affecting willingness to donate organs and their usage in selecting a particular donation system, which could be a vital contribution to the existing OD literature and practice. Against this backdrop, the objective of this study is to identify the important factors acting as the pillars of the three most prevalent OD systems and prioritize these factors with respect to Malaysia. Finally, after examining their importance in each OD system, the most suitable OD system for Malaysia is proposed.
In the sections that follow, a detailed literature review is provided, followed by the research methodology, analyses, results, and their discussion. The paper closes with the main conclusions resulting from this study, along with some policy implications.
Literature Review
Organ Donation Systems
As noted previously, some researchers emphasize the opt-in approach as the most ethical OD policy, even though this strategy has failed to provide sufficient number of donated organs.15 Others claim that the opt-out system disregards patient’s autonomy,16–20 even though it can be effective in increasing donation rates.14 Thus, the presumptive approach is introduced as most suitable alternative. Historically, in an opt-in system, donation is requested in an unbiased manner and requesters remained neutral when approaching families to seek consent. In this system, organ-procurement coordinators do not brief families about the altruistic deed of donation that how it can be life savor for potential recipients. Donation process, generally, remains unclear to families and neutral manner of requestors do not help to clarify doubts. In contrast, the goal of the presumptive approach is to focus on obtaining the permission and systematically overcome the family’s objections. Therefore, it embeds a change in the language used by a requestor when approaching the family of a potential donor. Rodrigue et al21 claim that the interpersonal skills of the requestor is one of the factors affecting families’ donation decisions. Organ-procurement coordinators are encouraged to introduce themselves to families as members of the “medical team” or as “grief counselors,” without necessarily disclosing their role.22 The presumptive approach seeks to balance human freedoms with the growing medical demand for deceased organs. It thus refocuses the conversation about consent from one that has been process driven to a person-centered approach, where the benefits of donation and the opportunity to save lives are emphasized. In a recent study, Shah et al23 revealed that techniques employed when approaching families can play a significant role in increasing authorization for donation. Decoupling is one such strategy employed by organ procurement organizations (OPOs) as a way to approach grieving family members. Conceptually, this involves separating the declaration of death to the family from the request for organ donation. It requires providing emotional support to the families.24 Shah et al clearly demonstrated that, when this technique is employed, a significantly higher deceased donation rate is attained.23
Nonetheless, it must be emphasized that the selection of the most optimal donation system for any country must be driven by the major factors affecting willingness to donate deceased organs in that society. Therefore, a brief discussion on such factors is important when designing an organ donation framework. Consequently, in the section that follows, the main factors influencing willingness to donate deceased organs are discussed.
Factors Affecting Willingness to Donate Deceased Organs
The complexity of human nature, sociocultural influences, and the interplay between personal and social conscience represent important determinants shaping beliefs and general opinions on donation.25 According to Irving et al26 and Rasiah et al,4 the role of socioeconomic status (SES), mostly determined by one’s education and income, is of particular importance in this sphere. Empirical evidence indicates that increasing education levels are significantly associated with increased OD rates.23,27 In the same vein, potential donors residing in countries with higher poverty rates are significantly less likely to donate. It is not surprising that higher poverty levels usually correlate with lower educational attainment and high unemployment, as well as low earning potential. However, the evidence on the relationship between income and donation remains inconclusive. Most authors point to the disparities in religious affiliations, family perspectives, age, and other characteristics when explaining the lack of definite relationship between income and deceased donation. Irrespective of donation policy (opt-in or opt-out), in deceased donation, family involvement is inevitable. Therefore, educating families can play a decisive role in raising OD rates in a country.28
Further, financial incentives are recognized as an important determinant of WTD. Those striving to increase OD rates call for the abolishment of regulated markets with “lump sums of cash” and are instead suggesting that potential donors be offered benefits, a tuition voucher for the bereaved family, partial payment of the donors’ funeral expenses, contributions to a charity specified by the donor or his/her family, or financing the donor’s dependent family.29 For instance, the Nuffield Council on Bioethics suggested a pilot funeral payment scheme to incentivize people to register for deceased OD in the UK.30 Nevertheless, use of financial incentives to raise OD remains debatable. On the one hand, proponents of financial incentives opine that appealing only to potential donors’ altruistic motivations is limiting and may foreclose a broad range of programs that also might motivate organ donation.31,32 On the other hand, opponents argue that diluting the altruistic intent of donating organs might undermine important social values.33 Some even claim that it may paradoxically lead to relatives imputing a weaker preference for OD34,35 or result in exploitation of the financial vulnerability of a deceased individual’s family.29,36 Thus, the critics advocate for re-culturing societal thinking to embrace a communitarian spirit of giving and altruism, where people actively want to donate their organs.37 Therefore, the decision to include financial incentives into any strategy for raising deceased OD rates needs to be carefully evaluated.
Individual perceptions about donating organs, donation perception, are widely acknowledged in literature as the major determinant of WTD. Perception is gauged by three major strands, namely, trust, attitude, and awareness.4 Symvoulakis et al25 were of view that distorted beliefs, negative or ambivalent attitudes, and lack of knowledge and trust in health-care systems are often more harmful than chronic diseases, and potentially cost human lives. Better knowledge about organ donation may ultimately translate into the act of donation.38 In a study conducted by Shaw et al,39 the right to overrule for the bereaved family and its impact on one’s trust in donation procedure is investigated. Authors found that “overrule right” for the family of a deceased individual could jeopardize the trust in the donation system. In a country where a deceased individual’s wish is allowed to be overruled by the bereaved family, potential donors’ confidence in the system will be precarious. In this situation, the individual has no confidence that their wish will be respected by the donation authorities. Therefore, a solid and transparent procedure is necessary to ensure trust and increase donation rates. Likewise, ample body of evidence2,40–42 confirms a profound influence of attitudes on donors’ WTD. However, few authors have highlighted the need of an effective policy for converting people’s positive attitudes to actual donations. For example, Zhang et al43 in a survey revealed that the majority of Chinese were favorably inclined toward organ donation, yet their actual donation rates were quite poor. The authors ascribed this disparity to policy weaknesses. Shah et al44 in their research work mention a study conducted by the US Agency for Healthcare Research and Quality (AHRQ) that people often do not have all the information they need to make decisions about donating a family member’s organs, nor do they have a clear understanding of the donation process. Individuals who receive regular information about organ donation or remain in frequent contact with health-care providers are more likely to donate an organ.45 Similarly, awareness can be instrumental in reducing the negative perceptions of organ removal. Johal et al46 highlighted lack of awareness as one of the significant barriers to organ donation. Alghanim47 and Bail48 similarly stressed the role of social media as an effective tool for disseminating knowledge regarding OD.
The demographic factors—namely religion, age, and ethnicity—are also frequently cited in OD literature as instrumental in raising OD rates. Members of the same religious group may have differing and often conflicting opinions in their own interpretation of how their religion encourages/discourages organ donation and transplantation. For example, Padela and Zaganjor49 found that Arabs in their study sample held more positive attitude towards deceased OD than did South Asian or African American Muslims. If religious teachings are interpreted incorrectly, those with greater religious affiliation may reject donation and transplantation due to considering this process against their religious values. Such issues can be fatal in countries where religious teachings are the prevalent source of societal and moral norms. Similarly, ethnicity is also considered an important influencer of WTD. In pertinent literature, various ethnic groups are shown to exhibit differing attitudes toward OD4,46,50–52 According to Moore et al53 low donation rates among ethnic minorities are associated with their religious beliefs and misperceptions, distrust of the medical community, fear of premature declaration of death after signing a donor card, and fear of racism. A microscopic analysis of such results can highlight the ethnicities that should be targeted in the strategies aimed at increasing WTD. Age is also considered to affect willingness to donate organs. According to Naqvi et al54 in Pakistan, youth has a positive perception about OD, as well as greater willingness to donate. However, Dundar et al55 reported that families are reluctant to give consent for OD if the patient has been relatively young. For family members of patients who died at a very young age, emotional attitudes are very important in the OD decision. Contrarily, in an international congress organized by the World Health Organization, Contarovich56 mentioned that the refusal rate among potential donors aged 60 and above is higher than in the 18−35 age group. These findings indicate that true identification of the tendency to donate among various religious and ethnic groups, as well as age categories, can help policymakers devise a focused strategy.
From the discussion presented above, socioeconomic status, financial incentives, donation perception, and demographic factors can be identified as the four main pillars for designating OD systems in a country. In other words, choosing appropriate OD system for a country (opt-in, opt-out, or presumptive approach) should be based on the major factors affecting WTD in other words, an OD system proven successful in one country cannot be simply replicated elsewhere.
As discussed above, the donation criteria vary from country to country and are highly contextual. In the present study, the authors seek to assign weights to the main factors affecting donation and propose their usage in selecting a donation system, which could be a vital contribution to the existing OD literature. Further, relevant literature in this field focuses on either qualitative or quantitative discussions, while both types are rarely employed when developing a model. In this study, we combine tangible and intangible factors in order to propose a general and practical methodology. We thus adopt a MCDM model using analytic hierarchical process (AHP) approach to prioritize factors affecting deceased OD. By creating a balance between efficiency and ethics, the objective of this study is to first prioritize factors affecting WTD as the pillars of OD systems (ie, financial incentives, socioeconomic status, donation perception, and demographic factors) in the Malaysian context. Subsequently, we examine their importance in each particular OD system for selecting the most suitable system for Malaysia.
Patients and Methods
Data
The data were provided by experts who completed a bipolar questionnaire. The authors used expert sampling, a subcategory of purposive sampling, for data collection. It involves consolidation of a sample of individuals with some definitive experience and expertise in a particular field. The first step in expert sampling is identifying the meaning of the term “expert“. We divided experts into four categories, namely doctors, hospital medical staff, health-care professionals, and government policy advisers who deal with organ donation process/policies. All these experts had at least 10 years of experience in the relevant field. The 35 participating experts were briefed about the survey conducted by academics and there was no attempt to influence the selection process (please see more details in Table 1). In the second step and in order to conduct pair comparison, a bipolar questionnaire is designed and distributed among the respondents to rank their individual judgements of the best policy of organ donation as well as the most important factors and subfactors affecting each policy. The scale ranges from one to nine where one indicates the equally important factors vs nine showing one factor is extremely more important than the other one in a pairwise matrix. Samples of AHP questionnaires for prioritizing the factors and subfactors are provided in the appendix. The importance value attributed to each number are illustrated in Table 2
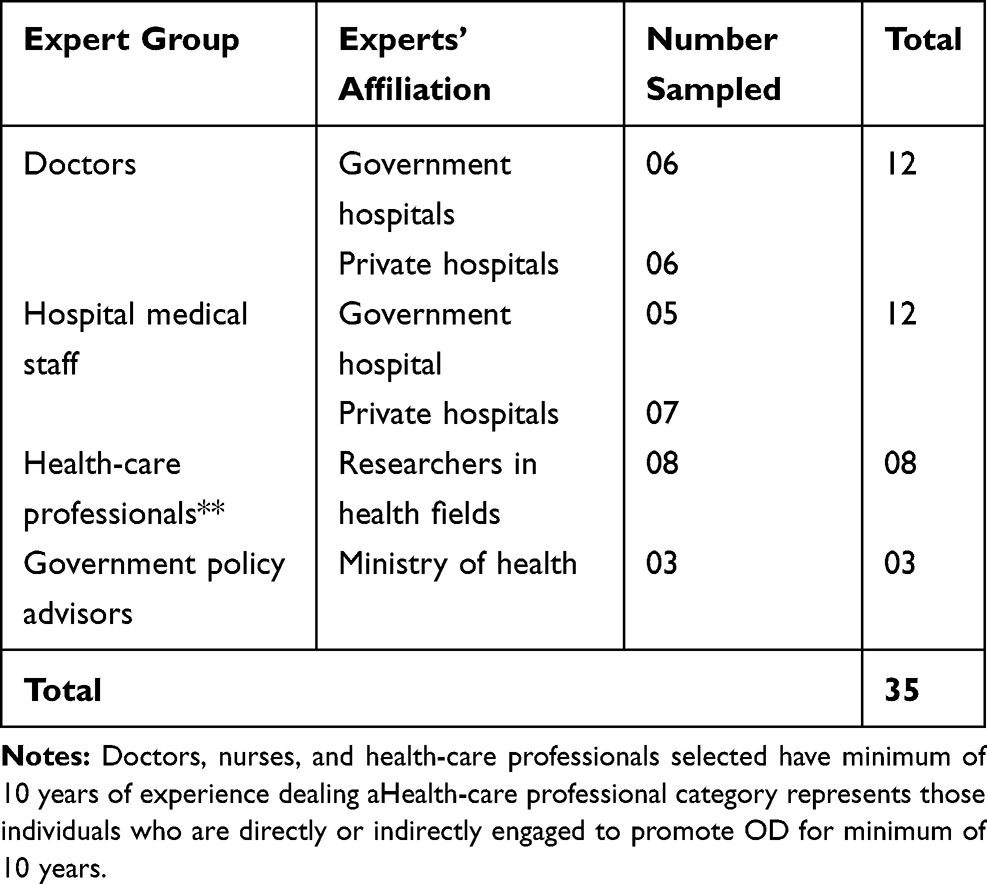 |
Table 1 Experts Sampled |
 |
Table 2 Scores for the Importance of Variables |
Method
In order to assign weights to the factors and subfactors affecting WTD for selecting the most suitable policy for Malaysia, in the present study, an AHP was applied. AHP was first introduced by Saaty57 and is a technique for measuring the qualitative and quantitative factors in decision-making. It facilitates decision-making based on judgments and experience that may influence the decision-making process at multilevel hierarchy structures.58 The advantages of AHP include its ability to reconcile differences (inconsistencies) in the data, and the existence of easy to use commercial software Expert Choice that performs all mathematical calculations required in accordance with multicriteria decision-making. In technical AHP language, factors and subfactors are called criteria and subcriteria, respectively. The AHP, as a theory of measurement through pairwise comparisons, relies on the judgments of experts to derive priority scales, which are then used to measure intangibles in relative terms. The first step in the AHP process is to convert a problem into hierarchy, consisting of goal (selection of best policy), criteria (donor perceptions, socioeconomic status, and demographic factors), subcriteria, and alternatives (opt-in, opt-out, and presumptive approach). The AHP hierarchy is shown in Figure 1 below.
 |
Figure 1 A hierarchical model for policy selection. |
 |
Figure 2 Global weights of subfactors towards goal. |
After establishing the hierarchy, a questionnaire consisting of bipolar questions using Saaty’s scale comprising of criteria and subcriteria affecting WTD was designed to collect the pairwise comparison judgments from the respondents. Table 1 shows the characteristics of the 35 experts that participated in the survey. These experts expressed their judgement on a nine-point scale, anchored at 1=equally important and 9=“extremely important. These preferences were subsequently quantified by applying Saaty’s 1−9 scale and a pairwise comparison matrix was structured using Expert Choice software. Further, the experts’ responses were processed to construct the corresponding pairwise comparison judgment matrices (PCJM), as well as establish the normalized weights. In other words, the importance of each factor in each level is assessed with respect to their parent element by pairwise comparison between peer nodes. For example, in the PCJM of criteria, donor perception is compared to socioeconomic status, and demographic factors with respect to the goal of selection of the best policy. Determining priorities within the levels of the hierarchy help to derive the overall priorities. Reason for using the bipolar comparison underlies the psychological attitude that comparing two options at the same time is easier than comparing all options simultaneously and leads to more accuracy.59 Subsequently, each of these matrices was then converted into the largest eigenvalue problem and was solved to find the normalized and unique priority weights for each criterion. In simple words, the values in the PCJM basically express how many times or how strongly more important a criteria/its indicator (subcriteria) is than the other criteria/subcriteria. In this study, the pairwise comparison will be conducted on three levels, including selection of the best policy, prioritizing the factors (criteria) and subfactors (subcriteria).
Results
First, we calculated PCJM and developed a consolidated PCJM (CPCJM). In the first step, it is important to find the consistency ratio (CR), as it explains the extent to which the respondents have been consistent while ranking one dimension relative to the other. The results reported in Table 3 reveal that the CR of each of the CPCJM is well below the rule of thumb with the CR value of 0.10. This clearly shows the consistent behavior of evaluators when making comparisons.
 |
Table 3 Consistency Ratio |
Tables 4 and 5 present the CPCJM computed by consolidating experts’ responses.
 |
Table 4 Pairwise Comparison Judgment Matrices of Factors |
 |
Table 5 Pairwise Comparison Judgment Matrices of Sub-Factors |
Table 5 reports the local and global weights assigned to the criteria and subcriteria. Local weights represent the weightings of each subcriterion specific to its criterion, whereas global weights represent weightings assigned to a criterion/subcriterion with respect to the goal. Based on the global weights, it is evident that donation perception (0.36) has the highest priority, followed by socioeconomic status (0.32), demographic factors (0.23), and financial incentives (0.09). Further, according to the local weights of the donation perception subcriteria, awareness (0.39) is given the highest importance followed by attitudes (0.32) and trust (0.29). Among local weights pertaining to the socioeconomic status subcriterion, education (0.58) appears to be the most important factor, outweighing both occupation (0.24) and income (0.18). Likewise, among the examined demographic factors, religion (0.34) was rated the highest by the experts, followed by ethnicity (0.45) and age (0.21). Lastly, for financial incentives, bereaved family support (0.50) possesses the local weighting equal to the combined local weighting of cash incentives (0.25) and financing funeral (0.25). In addition, comparison of global weights assigned to each subcriterion shows that awareness, education, attitudes, and trust are the most important factors in shaping WTD (Table 5).
After discussing the global and local weightings assigned to each criterion and subcriterion, three policy alternatives were examined with respect to their capacity to accommodate the above discussed findings. Table 6 provides detailed insights on the extent to which these three approaches incorporate the main factors affecting WTD. For example, the results reported in Table 7 show that the presumptive approach has the highest potential to cater for donation perception (0.36). Likewise, both socioeconomic status (0.32) and demographic factors (0.23) are best accommodated by the presumptive approach. Only for financial incentives, the least important factor based on global weights, the opt-in approach seems more favorable. However, owing to the low weighting of the financial incentives in the overall criterion assessment (0.09), as shown in Table 7), this does not give any significant distinction to the opt-in approach over the other two. Thus, presumptive approach has emerged as the most optimal strategy for raising WTD in the Malaysian context.
 |
Table 6 Comparison of OD Systems Based on Individual Criteria |
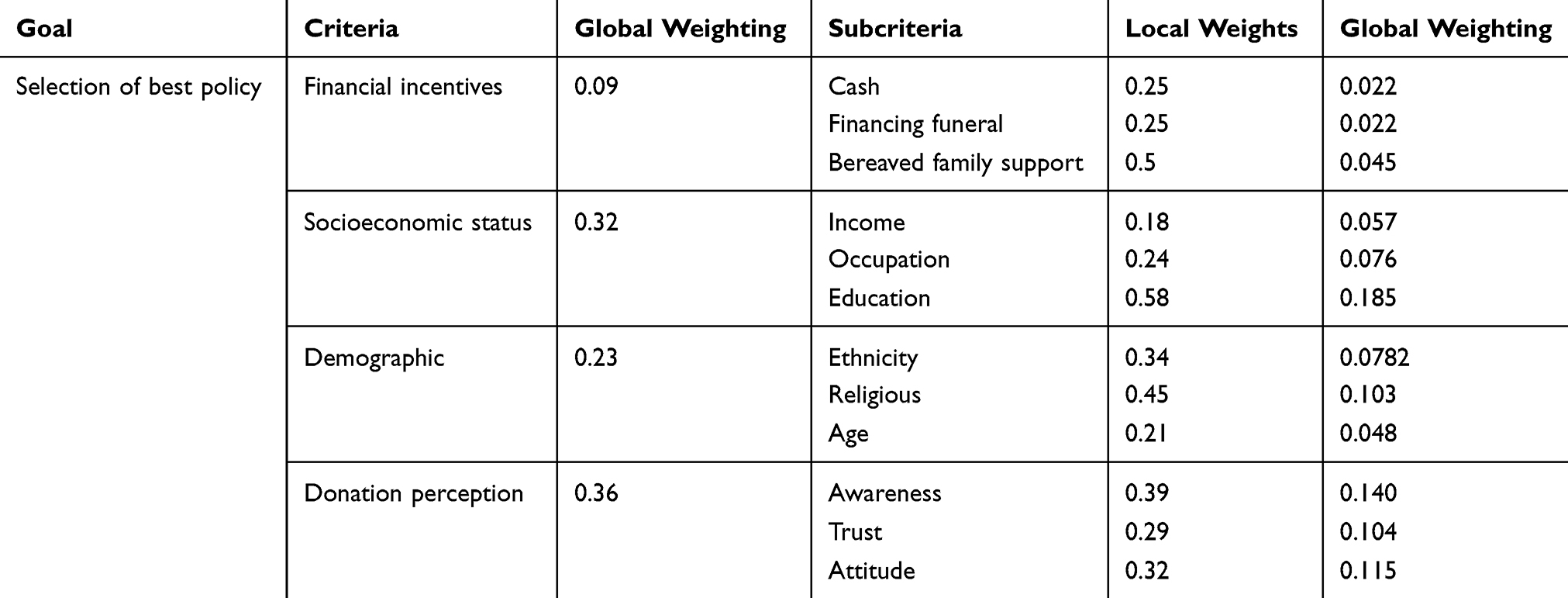 |
Table 7 Prioritization in Context of Malaysia |
In order to assess the stability of these results, we performeda sensitivity analysis, where despite of drastic change in the priorities of criterion factors, presumptive approach remained the most suited policy option. Among three approaches, ability of opt-out approach to accommodate the main factors affecting WTD appeared to be the lowest. In particular, this approach assigned the least importance to donation perception, which had the highest priority in criterion factors, due to which it was ranked the least favorable approach among the three. Figure 3 gives a holistic overview of the results reported in Table 7, demonstrating how various approaches accommodate the factors affecting WTD.
 |
Figure 3 Comparison of organ donation policies based on factors affecting willingness to donate. |
Discussion and Conclusion
The primary objective of this work was to identify the most suitable OD system for Malaysia. We first prioritized the factors influencing WTD in the Malaysian context. Then, on the basis of this prioritization, we determined the most optimal policy option for raising OD rates in Malaysia. Our analysis revealed that four dimensions of socioeconomic status and donation perception—education, awareness, attitude, and trust—are the major subfactors affecting WTD. Any donation system that accounts for these subfactors is thus suitable for the country.
Our results imply that deceased donation rates can be increased by educating people and promoting altruism. Albertsen60 claimed that, without the effort to increase public knowledge about the donation system, even the success on opt-out system would not be warranted.
Presently, an opt-in system is in place in Malaysia. Our results indicate that it is not the most optimal for the Malaysian context, as presumptive approach would be more likely to increase OD rates. While opt-out has been recognized as the most efficient system for procuring deceased organs, the current study shows that, in Malaysia, it is not consistent with the main factors affecting people’s willingness to donate. Therefore, implementation of the opt-out system in this country, where donation perception is the most influential factor in determining WTD, might cause backlash.
As mentioned in pertinent literature61–63 presumptive approach promotes the role of health-care professionals in securing the family consent. Therefore, we can conclude that educating the bereaved family is considered one of the built-in characteristics of this approach. Presumptive approach is a person-oriented rather than process-oriented strategy. This means that this approach relies on designated requesters’ skills to evoke altruism among bereaved families, instead of focusing on the clinical dissection process, which might bring discomfort.
Interestingly, even though presumptive approach is in many ways similar to the opt-in system, it primarily emphasizes the language used by the health-care providers when attempting to acquire family consent. Unlike the shift from the opt-in to the opt-out framework, which is a legislative change to the donation system, the transition towards presumptive approach is viewed as institutional change within the implemented system in a country. In other words, some minor institutional changes in the way that bereaved families should be approached and convinced empathetically can raise donation rates. Our results in favor of the presumptive approach as a means of raising donation rates are in line with those reported by Zink and Wertlieb,64 who proposed the presumptive approach as a solution for the growing organ shortage. Critical care nurses are encouraged to openly support OD, and a value-neutral position is no longer expected. In the same vain, Schulz et al65 posited that donor cards might trigger family communication and ease the physicians’ approach to family about donation.
To the best of the authors’ knowledge, OD policy in each country is contextual and interrelated with the factors affecting people’s perceptions about OD in general, and the donation process in place in that country in particular. As was shown by Mattew-King,66 in Wales, where the opt-out approach was introduced in 2015, OD rates have failed to increase. Thus, the author recommended that ministers focus on factors that have been proven to work, such as training nurses to discuss donation with bereaved families and raising public awareness.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gwynne K. How the organ transplant system is stacked against the most needy and why you should be a donor; 2011. Available from: http://www.alternet.org/story/152074/how_the_organ_transplant_system_is_stacked_against_the_most_needy,_and_why_you_should_be_a_donor.
2. Agwu NP, Awosan KJ, Ukwuani SI, Oyibo EU, Makusidi MA, Ajala RA. Awareness and attitude to deceased kidney donation among health-care workers in Sokoto, Nigeria. Ann Afr Med. 2018;17(2):75–81. doi:10.4103/aam.aam_52_17
3. Ozcan H, Yucel A, Avşar UZ, et al. Kidney transplantation is superior to hemodialysis and peritoneal dialysis in terms of cognitive function, anxiety, and depression symptoms in chronic kidney disease. Transplant Proc. 2015;47(5):1348–1351. doi:10.1016/j.transproceed.2015.04.032
4. Rasiah R, Manikam R, Chandrasekaran SK, et al. Deceased donor organs: what can be done to raise donation rates using evidence from Malaysia? Am J Transplant. 2016;16(5):1540–1547. doi:10.1111/ajt.13603
5. Lo CM. Deceased donation in Asia: challenges and opportunities. Liver Transpl. 2012;18(S2):S5–S7. doi:10.1002/lt.23545
6. International Registry in Organ Donation and Transplantation. Malaysia deceased organ donor evolution. IRODaT – DTI Foundation (Spain); 2018. Available from: http://www.irodat.org/?p=database&c=ES#data.
7. National Transplant Registry. Transplantation unit & national transplant resource centre. Transplant waiting list & allocation. National transplant registry, Dermaorgan Malaysia; 2017. Available from: http://www.dermaorgan.gov.my/en/allocation-waiting-list.
8. TheSundaily. 17 organ donations made this year: NTRC. TheSundaily; 2017. Available from: http://www.thesundaily.my/news/2017/10/08/17-organ-donations-made-year-ntrc.
9. The Statistics Portal. Number of Road Accidents in Malaysia from 2012 to 2016 (In 1000). 2018.
10. Rasiah R, Manikam R, Chandarsekaran SK, Thangiah G, Puspharajan S, Swaminathan D. The influence of socioeconomic and demographic variables on willingness to donate cadaveric human organs in Malaysia. Medicine. 2014;93(23):e126. doi:10.1097/md.0000000000000126
11. Tumin M, Noh A, Jajri I, Chong CS, Manikam R, Abdullah N. Factors that hinder organ donation: religio-cultural or lack of information and trust. Exp Clin Transplant. 2013;11(3):207–210. doi:10.6002/ect.2012.0194
12. Hulme W, Allen J, Manara AR, Murphy PG, Gardiner D, Poppitt E. Factors influencing the family consent rate for organ donation in the UK. Anaesthesia. 2016;71(9):1053–1063. doi:10.1111/anae.13535
13. Etheredge H, Penn C, Watermeyer J. Opt-in or opt-out to increase organ donation in South Africa? Appraising proposed strategies using an empirical ethics analysis. Dev World Bioeth. 2018;18(2):119–125. doi:10.1111/dewb.12154
14. Fan R, Chan H. Opt-in or opt-out: that is not the question. Hong Kong Med J. 2017;23(6):658–660. doi:10.12809/hkmj177022
15. Shepherd L, O’Carroll RE, Ferguson E. An international comparison of deceased and living organ donation/transplant rates in opt-in and opt-out systems: a panel study. BMC Med. 2014;12. doi:10.1186/s12916-014-0131-4
16. MacKay D. Opt-out and consent. J Med Ethics. 2015;41(10):832–835. doi:10.1136/medethics-2015-102775
17. Organ donation for transplantation. Improving Donor Identification and Consent Rates for Deceased Organ Donation (Clinical Guidance) [Database on the Internet]. National Institute for Health and Care Excellence (NICE); 2011.
18. Kluge EH. Improving organ retrieval rates: various proposals and their ethical validity. Health Care Anal. 2000;8(3):279–295. doi:10.1023/a:1009496002775
19. Taskforce OD. Organs for Transplants: A Report from the Organ Donation Taskforce. London, UK: Department of Health, In partnership with Health, Social service and public safety; 2008.
20. Brown S-J. The legal justification for donor optimisation procedures. Clin Ethics. 2016;11(4):122–129. doi:10.1177/1477750916657665
21. Rodrigue JR, Cornell DL, Howard RJ. Organ donation decision: comparison of donor and nondonor families. Am J Transplant. 2006;6(1):190–198. doi:10.1111/j.1600-6143.2005.01130.x
22. Truog RD, Miller FG, Halpern SD. The dead-donor rule and the future of organ donation. N Engl J Med. 2013;369(14):1287–1289. doi:10.1056/NEJMp1307220
23. Shah MB, Vilchez V, Goble A, et al. Socioeconomic factors as predictors of organ donation. J Surg Res. 2018;221:88–94. doi:10.1016/j.jss.2017.08.020
24. Jacoby L, Jaccard J. Perceived support among families deciding about organ donation for their loved ones: donor vs nondonor next of kin. Am J Crit Care. 2010;19(5):e52–61. doi:10.4037/ajcc2010396
25. Symvoulakis EK, Komninos ID, Antonakis N, et al. Attitudes to kidney donation among primary care patients in rural Crete, Greece. BMC Public Health. 2009;9(1):54. doi:10.1186/1471-2458-9-54
26. Irving MJ, Tong A, Jan S, et al. Factors that influence the decision to be an organ donor: a systematic review of the qualitative literature. Nephrol Dial Transplant. 2012;27(6):2526–2533. doi:10.1093/ndt/gfr683
27. Regalia K, Zheng P, Sillau S, et al. Demographic factors affect willingness to register as an organ donor more than a personal relationship with a transplant candidate. Dig Dis Sci. 2014;59(7):1386–1391. doi:10.1007/s10620-014-3053-2
28. Ozer A, Ekerbicer HC, Celik M, Nacar M. Knowledge attitudes, and behaviors of officials of religion about organ donation in kahramanmaras, an eastern mediterranean City of Turkey. Transplant Proc. 2010;42(9):3363–3367. doi:10.1016/j.transproceed.2010.08.035
29. Delmonico FL, Martin D, Dominguez-Gil B, et al. Living and deceased organ donation should be financially neutral acts. Am J Transplant. 2015;15(5):1187–1191. doi:10.1111/ajt.13232
30. Nuffieldbioethics. Nuffield council on bioethics. Human bodies: donation for medicine and research; 2011. Available from: http://nuffieldbioethics.org/wp-content/uploads/2014/07/Donation_full_report.pdf.
31. Becker GS, Elías JJ. Introducing incentives in the market for live and cadaveric organ donations. J Econ Perspect. 2007;21(3):3–24. doi:10.1257/jep.21.3.3
32. Taub S, Maixner AH, Morin K, Sade RM. Council ethical judicial affairs a. cadaveric organ donation: encouraging the study of motivation. Transplantation. 2003;76(4):748–751. doi:10.1097/01.tp.0000086885.76994.e0
33. Voo TC. Altruism and reward: motivational compatibility in deceased organ donation. Bioethics. 2015;29(3):190–202. doi:10.1111/bioe.12078
34. Chong JL. Policy options for increasing the supply of transplantable kidneys in Singapore. Singapore Med J. 2016;57(10):530–532. doi:10.11622/smedj.2016163
35. Roth AE. Repugnance as a constraint on markets. J Econ Perspect. 2007;21(3):37–58. doi:10.1257/jep.21.3.37
36. Epstein M, Martin D, Danovitch G. Caution: deceased donor organ commercialism! Transpl Int. 2011;24(9):958–964. doi:10.1111/j.1432-2277.2011.01294.x
37. Etzioni A. Organ donation: a communitarian approach. Kennedy Inst Ethics J. 2003;13(1):1–18. doi:10.1353/ken.2003.0004
38. Saleem T, Ishaque S, Habib N, et al. Knowledge, attitudes and practices survey on organ donation among a selected adult population of Pakistan. BMC Med Ethics. 2009;10(1):1–12. doi:10.1186/1472-6939-10-5
39. Shaw D, Georgieva D, Haase B, et al. Family over rules? An ethical analysis of allowing families to overrule donation intentions. Transplantation. 2017;101(3):482–487. doi:10.1097/tp.0000000000001536
40. Bastami S, Matthes O, Krones T, Biller-Andorno N. Systematic review of attitudes toward donation after cardiac death among healthcare providers and the general public. Crit Care Med. 2013;41(3):897–905. doi:10.1097/CCM.0b013e31827585fe
41. Wakefield CE, Watts KJ, Homewood J, Meiser B, Siminoff LA. Attitudes toward organ donation and donor behavior: a review of the international literature. Prog Transplant. 2010;20(4):380–391. doi:10.1177/152692481002000412
42. Balwani MR, Gumber MR, Shah PR, et al. Attitude and awareness towards organ donation in western India. Ren Fail. 2015;37(4):582–588. doi:10.3109/0886022x.2015.1007820
43. Zhang QX, Xie JF, Zhou JD, et al. Impact factors and attitudes toward organ donation among transplantation patients and their caregivers in China. Transplant Proc. 2017;49(9):1975–1981. doi:10.1016/j.transproceed.2017.09.022
44. Shah R, Patel A, Ramanuj V, Solanki N. Knowledge and attitudes about organ donation among commerce college students. Natl J Community Med. 2015;6(4):533–535.
45. Simpkin AL, Robertson LC, Barber VS, Young JD. Modifiable factors influencing relatives’ decision to offer organ donation: systematic review. BMJ. 2009;338. doi:10.1136/bmj.b991
46. Johal J, Bains H, Churchward D, Brand S, Malik S. Quantitative study of the beliefs and attitudes to organ donation and the “opt out” system amongst the Sikh community in UK. Transplant Proc. 2018;50(10):2939–2945. doi:10.1016/j.transproceed.2018.03.014
47. Alghanim SA. Knowledge and attitudes toward organ donation: a community-based study comparing rural and urban populations. Saudi J Kidney Dis Transpl. 2010;21(1):23–30.
48. Bail CA. Cultural carrying capacity: organ donation advocacy, discursive framing, and social media engagement. Soc Sci Med. 2016;165:280–288. doi:10.1016/j.socscimed.2016.01.049
49. Padela AI, Zaganjor H. Relationships between islamic religiosity and attitude toward deceased organ donation among American muslims: a pilot study. Transplantation. 2014;97(12):1292–1299. doi:10.1097/01.tp.0000441874.43007.81
50. Dunkel A, Nakamoto K, Schulz PJ. Micro-cultural customization of organ donation propagation messages. Patient Educ Couns. 2017. doi:10.1016/j.pec.2017.12.019
51. Ríos A, López-Gómez S, López-Navas AI, et al. Approach of social groups with little sensitization to organ donation: pilot study in the gypsy population to assess the best approach to determine the attitude toward organ donation for transplantation. Transplant Proc. 2018;50(2):338–340. doi:10.1016/j.transproceed.2017.12.051
52. Wong LP. Knowledge, attitudes, practices and behaviors regarding deceased organ donation and transplantation in Malaysia’s multi-ethnic society. Int J Behav Med. 2010;17:244.
53. Moore SAMD, Myers OP, Comfort DRRTC, Lu SWMD, Tawil IMDF, West SDMD. Effects of ethnicity on deceased organ donation in a minority-majority state*. Crit Care Med. 2014;42(6):1386–1391. doi:10.1097/CCM.0000000000000215
54. Naqvi SAA, Ali B, Mazhar F, Zafar MN, Rizvi SAH. A socioeconomic survey of kidney vendors in Pakistan. Transpl Int. 2007;20(11):934–939. doi:10.1111/j.1432-2277.2007.00529.x
55. Dundar HZ, Oflaz R, Cinar YS, Sarkut P, Kaya E. Is donor age an important factor in cadaveric organ donation? Transplantation. 2017;101(8S–2):S139. doi:10.1097/01.tp.0000525201.06663.03
56. Contarovich F. Organ Donation and a New Message for All Ages: Our Body is a Source of Life to Be Shared. Societal-Public Policy. TTS International Congress the Transplantation Society (TTS), NGO in Official Relation with World Health Organization (WHO). 2010:708.
57. Saaty TL. A scaling method for priorities in hierarchical structures. J Math Psychol. 1977;15(3):234–281. doi:10.1016/0022-2496(77)90033-5
58. Bayazit O. Use of AHP in decision-making for flexible manufacturing systems. J Manuf Technol Manag. 2005;16(7):808–819. doi:10.1108/17410380510626204
59. Ishizaka A, Labib A. Analytic hierarchy process and expert choice: benefits and limitations. OR Insight. 2009;22(4):201–220. doi:10.1057/ori.2009.10
60. Albertsen A. Deemed consent: assessing the new opt-out approach to organ procurement in Wales. J Med Ethics. 2018;44(5):314–318. doi:10.1136/medethics-2017-104475
61. Salim A, Berry C, Ley EJ, et al. In-house coordinator programs improve conversion rates for organ donation. J Trauma. 2011;71(3):733–736. doi:10.1097/TA.0b013e31820500e6
62. Sanner MA. Two perspectives on organ donation: experiences of potential donor families and intensive care physicians of the same event. J Crit Care. 2007;22(4):296–304. doi:10.1016/j.jcrc.2007.03.002
63. Morgan SE, Miller JK. Beyond the organ donor card: the effect of knowledge, attitudes, and values on willingness to communicate about organ donation to family members. Health Commun. 2002;14(1):121–134. doi:10.1207/S15327027HC1401_6
64. Zink S, Wertlieb S. A study of the presumptive approach to consent for organ donation: a new solution to an old problem. Crit Care Nurse. 2006;26(2):129–136. doi:10.4037/ccn2006.26.2.129
65. Schulz PJ, van Ackere A, Hartung U, Dunkel A. Prior family communication and consent to organ donation: using intensive care physicians’ perception to model decision processes. J Public Health Res. 2012;1(2):130–136. doi:10.4081/jphr.2012.e19
66. Mattew-King A. Radical New Law Making Everyone an Organ Donor Unless They Opt-Out Could Save 700 per Year, Government Says. Independent. 2018.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.